Confirming death
Examination to confirm death
Definition
In the UK there is no legal definition of death. It is the clinician’s responsibility to declare when a patient has died. Death is defined by the UK Academy of Medical Royal Colleges as: ‘the irreversible loss of the capacity for consciousness, combined with irreversible loss of the capacity to breathe’. For practical purposes, death has occurred if there is absence of spontaneous cardiac function, respiratory effort and central nervous system activity.
Death used to be synonymous with the sudden and unexpected loss of spontaneous cardiac activity and respiration (cardiopulmonary arrest). Appropriate and prompt treatment can, however, successfully resuscitate some people in this category (Ch. 19).
Timing
The exact timing of death is rarely predictable, but is sometimes anticipated and accepted, e.g. in a patient with advanced metastatic cancer. Some patients with very severe chronic or terminal illness do not wish to have resuscitative efforts performed. In some countries, including the UK, the applicability of a ‘do not attempt resuscitation’ (DNAR) directive may be discussed with the patient and close relatives. The outcome of this discussion should be clearly recorded in the notes, made known to relevant medical and nursing staff and reviewed regularly. The presence of a DNAR order does not in any way imply withdrawal of treatment: it should focus attention on the general care of the patient, including adequate analgesia.
Confirmation
Confirming death has major medicolegal implications and obligations. Your approach and manner should always be professional. Although death may appear obvious, carefully and systematically examine the body. Misdiagnosis is especially likely in situations where vital functions and general metabolism are greatly reduced (Box 20.1).
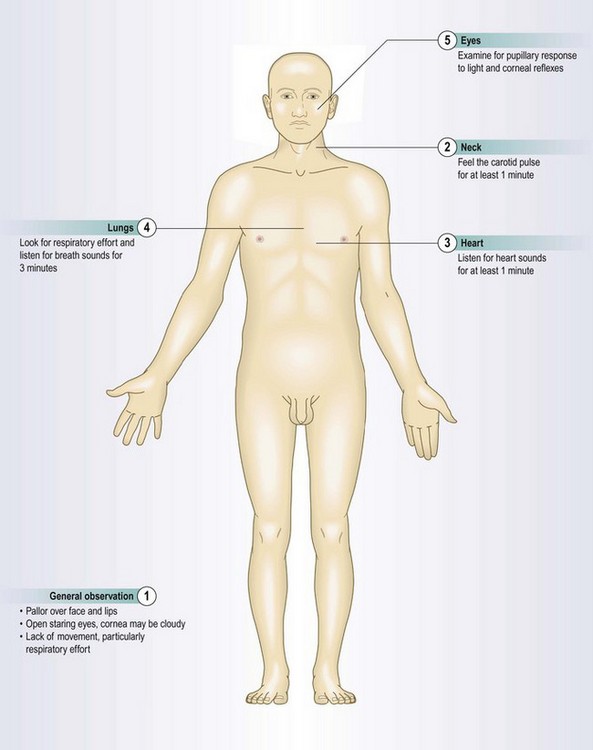
Examination sequence
 Feel for a major (carotid or femoral) pulse for at least 1 minute.
Feel for a major (carotid or femoral) pulse for at least 1 minute.
Listen for heart sounds over the cardiac apex for at least 1 minute.
While you are doing this, watch the chest wall for any movement.
Listen to the chest for breath sounds for 3 minutes.
Watch for any spontaneous movement during your examination.
Press over the supraorbital notch and check there is no response to supraorbital pressure.
Simultaneously retract both eyelids, shine a bright light into each eye in turn and check that both pupils are unreactive.
Check for absence of the corneal reflexes (Fig. 11.6).
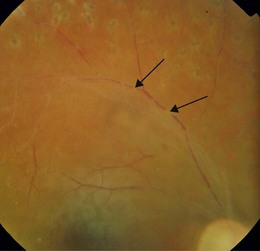
Other clinical features associated with death include unnatural pallor, particularly of the face and lips, relaxation of the facial muscles with drooping of the lower jaw and open staring eyes. Eye changes include cloudiness of the cornea, reduced eyeball tension and, on fundoscopy, segmentation of blood within the retinal veins. This is known as ‘cattle-trucking’, ‘railroading’ or ‘boxcars’ (Fig. 20.1). None of these changes, however, should be used in isolation as a marker of death. Other postmortem changes gradually develop (Box 20.2).
 20.2 Postmortem changes
20.2 Postmortem changes
Dark red/purple skin discoloration in gravity-dependent parts of the body develops within 20–30 minutes of death and becomes ‘fixed’ after about 12 hours
Investigations
In certain situations, additional investigations may be available and confirmatory: for example, an electrocardiograph monitor trace showing asystole, absence of pulsatile flow from an intra-arterial line, or of contractile motion on echocardiography.
Brainstem death
Modern resuscitative devices and techniques can maintain the function of the heart, lungs and visceral organs, even when brainstem function has stopped. Patients receiving mechanical ventilation require additional tests to confirm brainstem death, which should be carried out by two experienced doctors on two occasions 24 hours apart. Prior to such testing establish that the patient has irreversible brain injury of known cause producing deep coma and apnoea requiring artificial ventilation and that excludes potentially reversible causes (Box 20.1).
Examination sequence
There should be no response to any test below to confirm brainstem death.
Apply a painful stimulus, e.g. supraorbital pressure or pinch an earlobe.
Check the corneal reflexes (p. 254).
Apply suction to the trachea to check for a cough or gag reflex. Note any response to the tracheal tube.
Inject 20 ml of ice-cold water into the external auditory meatus and look for eye movements (oculovestibular reflexes/nystagmus).
Stop ventilation long enough to allow PaCO2 to rise to >6.7 kPa. Continue 100% oxygenation, by a cannula in the tracheal tube. Look for any respiratory effort: its absence indicates medullary brainstem failure.
What to do after you have confirmed death
Record the death in the patient’s medical notes, with the date and time at which you pronounced life extinct. If possible, state what you believe to be the cause of death. Sign the notes legibly; include your designation.
Inform the close family or next of kin about the death as soon as possible. Wherever possible, do this in person rather than by telephone. Breaking bad news is difficult: always speak to the bereaved in a quiet and private environment, avoid interruption (ask someone to take your telephone and pager) and, wherever possible, involve a nurse or counsellor to act as a witness and provide future support if required. Relatives need time to understand and accept the situation. Use great care and sensitivity to try to support them. Inform the family doctor as soon as is reasonable. The followers of some faiths have procedures and rituals that should be followed after a death and which require the involvement of an appropriate religious leader.
If appropriate, ask about the deceased’s wishes for organ donation. Some people carry an organ donor card stating their wishes. In the UK there is an organ donor register, which allows people to indicate their wishes for organ donation after death. You can check this register to confirm the deceased’s wishes.
Where the circumstances of death are unexpected or where death has occurred in suspicious or prescribed circumstances, the legal authorities must be informed. Examples include suspected overdose, deaths related to alcohol or after surgery or if there is to be a post mortem examination. Do not give a death certificate until the coroner, procurator fiscal or other authority has agreed that you should do so (Box 20.3).
 20.3 Deaths that may require further enquiry
20.3 Deaths that may require further enquiry
• caused by an accident arising from use of a vehicle, e.g. aircraft, ship, train or car
• due to an industrial disease, e.g. mesothelioma
• where the circumstances suggest suicide
• following abortion or attempted abortion
• thought to be due to sudden infant death syndrome
• of a child in the care of a local authority or on an ‘at risk’ register
• due to a disease, infectious disease or syndrome which poses a serious public health risk, e.g. hepatitis A, B, C or E, food poisoning, legionnaire’s disease, any hospital-acquired infection
• by burning or scalding or as a result of fire or explosion which might have arisen from medical mishap
• occurring in a general practitioner’s surgery or health centre
• where a complaint has been received at the health board about the medical treatment given to the deceased