The critically ill
Examination of the critically ill patient
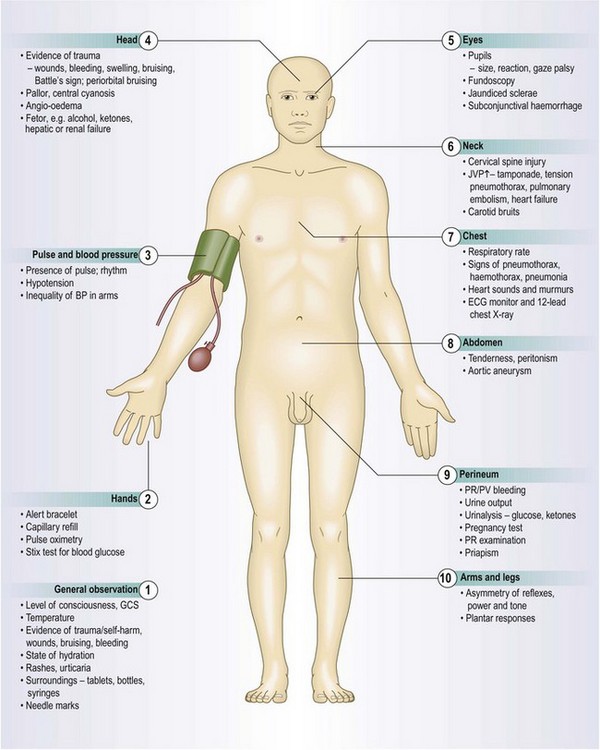
Approach to the critically ill patient
Systematic examination is inappropriate for critically ill patients as immediate intervention may be needed to save life, e.g. in cardiac arrest or tension pneumothorax, or to halt processes which untreated, would lead to death, e.g. hypovolaemic shock. Examination and interventions are often performed simultaneously.
Rapidly identify the main problems affecting the patient and use the resources available to gain control of the situation. Your aim is to stabilise the patient’s condition and address life-threatening problems. This temporary phase should always be followed by a full history and clinical examination when the patient is ‘stable’ to make a full diagnosis, perform specialist investigations and institute definitive therapy.
The clinical manifestations of critical illness (Box 19.1)
Critical illness can present as:
• acute respiratory compromise affecting Airway or Breathing (Box 19.2)
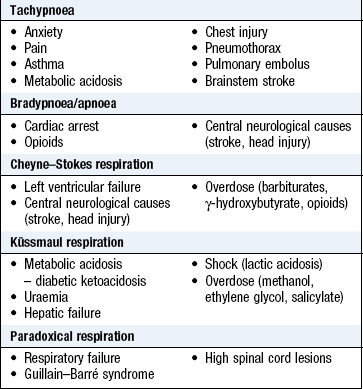
 19.2 Common causes of acute respiratory compromise
19.2 Common causes of acute respiratory compromise
• Altered conscious state (Box 19.4)
• Upper-airway/maxillofacial injury
• Pneumothorax (especially if bilateral or if tension is present)
• Blunt: rib fractures, flail segment, lung contusion
• Penetrating: pneumothorax, open chest wound, major vessel injury with haemothorax
• Acute respiratory distress syndrome (ARDS)
• Exacerbation of chronic obstructive pulmonary disease (COPD)
• acute cardiovascular compromise, detectable as reduced Circulation (Box 19.3)
19.3 Common causes of acute cardiovascular compromise
• Acute myocardial infarction or ischaemia
• Acute valve dysfunction, e.g. endocarditis, mechanical valve failure or obstruction
• Upper: varices, peptic ulcer, tumour, Mallory–Weiss tear, non-steroidal anti-inflammatory drugs (NSAIDs)
• Lower: diverticular disease, angiodysplasia, ischaemic bowel, Meckel’s diverticulum, tumour
• Overt: wounds, especially to scalp, face; long bone or pelvic fractures
• Concealed: chest – haemothorax; abdomen – splenic and/or hepatic injury, retroperitoneal
• Obstetric/gynaecological: placenta praevia, miscarriage, ectopic pregnancy, trauma, tumour
• altered conscious state manifest as neurological Disability (Box 19.4).
19.4 Common causes of altered conscious state
Initially, you may not be aware of events or the timeframe preceding the current state. Concentrating on the system which appears most likely to be causing the problem may be misleading, wastes time and further compromises the patient. Use a simple and safe ABCD approach to address and correct conditions using a logical framework.
The ABCD approach
This has four interlinked phases:
Seek senior, experienced help immediately. If you have to work alone, only proceed to the next item once you have adequately completed the preceding one. A team can deal with the separate elements simultaneously, but the leader should ensure that all components are covered and if a patient’s condition deteriorates, should immediately review the ABCD sequence.
Communicating with others in order to get help requires careful, concise delivery of information that can be difficult in an emotionally charged resuscitation. A useful and widely used format with which to structure your thoughts is SBAR (situation, background, assessment, recommendation: Box 19.5).
 19.5
19.5
SBAR framework for communication
Preparation
Information gathering: The patient may be unable to give a history, so use all possible sources of information (Box 19.6). Include previous primary care or hospital records, relatives, friends, bystanders and emergency or ambulance personnel. Look for diabetic/steroid/anticoagulant cards and medications, and Alert bracelets/necklaces (Fig. 3.3). If possible, contact the patient’s GP, who is often a key source of current and background information.
Managing your resources: Identify your available resources: which staff can help? What is their level of seniority and experience and what can they do? If you have others to help you, identify roles and responsibilities. If you are team leader, communicate your thinking to the whole team clearly and frequently.
Primary survey
The primary survey, investigations and interventions should take 5–10 minutes, unless you have to undertake a life-saving intervention such as tracheal intubation. The patient may be unable to sit up. If this is the case examine him supine throughout.
Examination sequence
 Approach the patient so that he can see you if conscious.
Approach the patient so that he can see you if conscious.
Speak slowly and clearly and assess his response.
If the patient talks to you normally, the airway is clear and there is perfusion of the brain; if his speech is lucid, cerebral function is adequate.
Give a high inspired concentration of oxygen by mask, and move on to B (breathing).
If there is no response to speech, usually because the patient has altered consciousness, perform a more detailed assessment of the airway. Look, listen and feel. Open his mouth and remove secretions, blood, vomit or foreign material by gentle suction with a Yankauer catheter (Fig. 19.1) under direct vision. Leave well-fitting dentures or dental plates in place to maintain the normal airway anatomy. If they are loose or poorly fitting, remove them.

Fig. 19.1 Yankauer suction catheter.
This may have a small hole to control airflow – if present, occlude this with your thumb to generate suction.
Listen for upper airway noises (Box 19.7). Gurgling, snoring or stridor suggests partial airway obstruction. Grunting respiration may be a sign of respiratory muscle fatigue, or an attempt to slow expiration in a patient with a flail segment (see below). Absent breath sounds indicates either complete airway obstruction or absence of breathing.
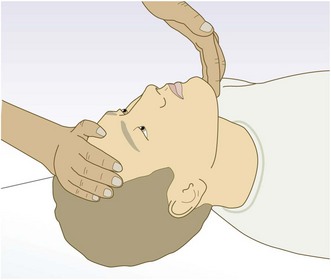
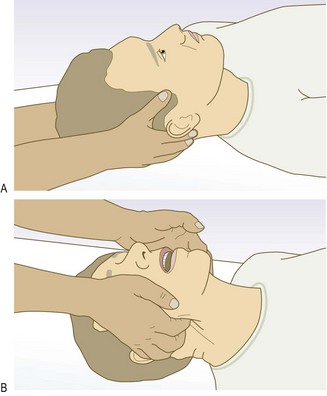
Open the airway by tilting the patient’s head and lifting his chin (Fig. 19.2). If you suspect neck injury, do not move the neck. Control the head and neck by manual in-line control and open the airway using the jaw lift technique (Fig. 19.3). Appropriately sized airway adjuncts, such as nasopharyngeal or oropharyngeal (Guedel) airways, can maintain the airway in patients with altered consciousness (Fig. 19.4). Do not use a nasopharyngeal airway if you suspect a skull base fracture, if epistaxis, nasal trauma or deformity is present, or if the patient is taking anticoagulants. Tracheal intubation may be needed if the patient cannot maintain a patent airway. This should only be performed by an experienced clinician (Box 19.8).
19.8 Principal indications for emergency advanced airway and ventilation techniques

Hypoxia hastens and causes death. Central cyanosis is a late, unreliable sign of hypoxia. Even in critical hypoxia, cyanosis may be absent because of severe anaemia or massive blood loss.
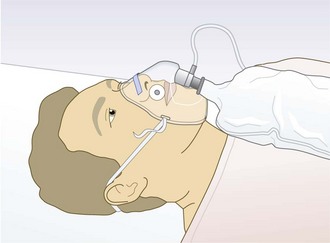
Attach a pulse oximeter probe to a fingertip (Fig. 7.25) or earlobe. Pulse oximetry (SpO2) can non-invasively assess peripheral oxygenation simply (Box 19.9). Use an oxygen mask with reservoir bag and adjust the oxygen flow rate to maintain an SpO2 of 94–98% (Fig. 19.5). If the oxygen mask ‘mists’ on exhalation, the patient has (some) respiratory effort. The only exception to this initial treatment is if you know the patient has chronic obstructive pulmonary disease with CO2 retention (type II respiratory failure). These patients may lose the hypoxic stimulus to breathe if given high concentrations of oxygen. In these patients aim to maintain an SpO2 of 88-92%.
Look for movements of the chest, the accessory muscles and the abdomen. Paradoxical respiration is movement of the abdomen exactly out of phase with that of the chest and indicates respiratory compromise. It is most often due to fatigue of the diaphragm and/or airway obstruction. In patients with chronic airflow obstruction a breathing pattern with abnormal abdominal movements is associated with a much poorer prognosis. Look for other abnormal breathing patterns (Box 19.10).
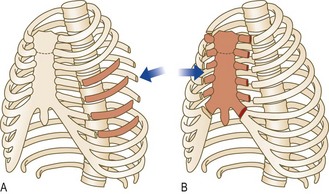
Seek signs of injury (bruising, pattern imprinting, wounds) and of flail segment in trauma patients. In a flail segment the affected area moves paradoxically: it moves outwards from the chest wall during expiration and inwards during inspiration.
Kneel at the patient’s side and look tangentially across the chest. A flail segment is often well localised and, if present, implies that at least three ribs are broken in at least two places (Fig. 19.6). Underlying lung injury is common.
Assess the position of the trachea in the suprasternal notch.
In a trauma patient, systematically and gently palpate the chest to identify any areas of injury. Rib and sternal fractures are associated with localised discomfort. Subcutaneous emphysema feels like ‘crackling’ under your fingers. Examine for consolidation, pneumothorax, pleural effusion and haemothorax (Ch. 7).
Auscultate for breath sounds and added sounds. Critically ill patients may not have the signs you expect. For example, a patient with life-threatening asthma may have little or no wheeze (a silent chest) because airflow into the lungs is poor.
Expose the chest, back, axillae and abdomen. Look for wounds (usually gunshot or stab) producing an open defect in the chest wall (Fig. 19.7). Recognise and treat open pneumothorax or a pneumothorax under tension. An open chest wound equalises pressure between the pleural space and atmosphere, and the affected lung is unable to expand or contract normally with respiration. During inspiration and expiration, you may hear air movement and see a spray of blood at the wound. Cover the wound with a sterile occlusive dressing secured on three sides. A formal tube thoracostomy with underwater seal drainage is then needed.

Suspect tension pneumothorax in any patient who rapidly develops severe respiratory and cardiovascular distress. It occurs when lung injury produces a one-way valve effect (Fig. 19.8). On inspiration air escapes from the lung and accumulates in the pleural space. As the pleural pressure increases, the ipsilateral lung progressively collapses and the increased intrathoracic pressure reduces venous return to the heart, eventually causing cardiac arrest.
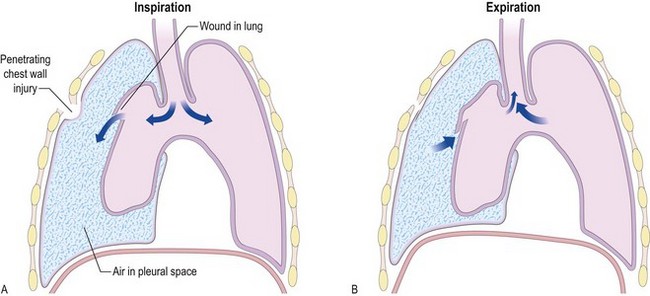
Fig. 19.8 Tension pneumothorax following penetrating injury.
Air enters the pleural cavity via the punctured lung during inspiration. The chest wall and lung defects act as one-way valves. Air cannot escape from the pleural cavity during expiration. The right intrapleural pressure increases, collapsing the right lung, impeding venous return to the heart and occasionally shifting mediastinal structures to the contralateral side.
It occurs most commonly in chest injury, during positive-pressure ventilation or in underlying lung disease (especially when ventilated). The diagnosis is clinical. The patient appears acutely breathless and agitated, has tachycardia and may be cyanosed. Hypotension, bradycardia and altered consciousness are preterminal features. Quickly examine for jugular venous distension, tachycardia and absent breath sounds on the affected side. If the patient is in extremis, insert a large-bore intravenous (IV) cannula through the second intercostal space in the mid-clavicular line on the affected side. Remove the needle from the cannula. A hiss of air, with rapid clinical improvement, confirms the diagnosis. Tube thoracostomy with underwater seal drainage is then required.
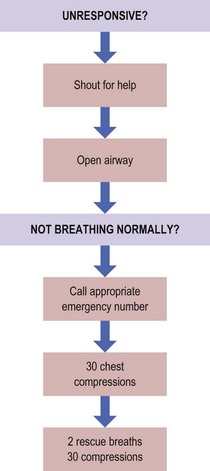
Feel for a central (carotid or femoral) pulse for 10 seconds. If you cannot feel a pulse and the patient is unresponsive, treat as for cardiac arrest (for current guidelines from the International Liaison Committee on Resuscitation on how to manage cardiac arrest, see www.ilcor.org) (Fig. 19.9).
In responsive patients, feel for a peripheral (radial or brachial) pulse. If you cannot palpate a peripheral pulse, this suggests that the patient is significantly hypotensive.
Note the pulse rate, rhythm, volume and character.
Assess peripheral perfusion; press on the fingertip pulp for a few seconds, remove your finger and estimate the capillary refill time (normal <2 seconds).
Attach an ECG monitor to the patient. Note the ventricular rate and the rhythm.
Control external blood losses from wounds or open fractures by direct firm pressure with a sterile dressing placed over the site. Minimise blood loss from long bone fractures (femur, tibia/fibula, humerus and forearm) by splintage.
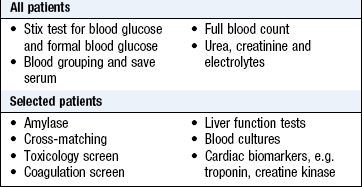
Insert a large-bore (16 FG, 1.7 mm internal diameter or bigger) IV cannula and tape it securely to the skin. In trauma patients and when you suspect hypovolaemia, insert and secure two large-bore cannulae. Take initial blood samples (Box 19.11) from the cannula and then attach an IV fluid-giving set. Commence volume replacement, if needed, with warmed 0.9% saline or Ringer’s solution.
Examine the jugular venous pressure (JVP) (Fig. 6.19). In a sitting or semirecumbent patient, elevation of the JVP in the presence of shock suggests a major problem with the heart’s pumping ability, such as acute heart failure, cardiac tamponade, massive pulmonary embolus, tension pneumothorax or an acute valvular problem.
Check the blood pressure (p. 113).
Examine the precordium and heart, identifying the presence of added heart sounds or murmurs.
Insert a urinary catheter (unless there is evidence of urethral or prostatic injury – blood at the urethral meatus and/or a high-riding, ‘boggy’ prostate on rectal examination) to monitor urine output.
Shock implies that the oxygen and blood supply to an organ or tissue is inadequate for its metabolic requirements. It is recognised clinically by a combination of features (Box 19.12). The extent to which each feature is present depends upon the cause (Box 19.13) and the time course. Signs of shock may be delayed or obscured in athletes, pregnant women, those on vasoactive drugs (beta-blockers, calcium channel blockers, angiotensin-converting enzyme inhibitors), those with pacemakers and the very young and old.
Tachycardia (heart rate >100 bpm) and hypotension (systolic blood pressure <100 mmHg) are not required to diagnose shock: the heart rate may be normal or low in hypoxic shocked patients or those on drugs such as beta-blockers. Blood pressure may be temporarily maintained by sympathetic activity and peripheral vasoconstriction. In critically ill patients non-invasive cuff blood pressure measurements are often inaccurate.
Do not concentrate on absolute figures of systolic or diastolic blood pressure. Readings of 90/50 mmHg are normal in many healthy young women, while 120/70 mmHg indicates significant hypotension in a patient whose pressures are usually 195/115 mmHg. Trends in pulse and blood pressure give far more information than initial or isolated readings. If the patient has a rising pulse rate, with a falling blood pressure and reduced urine output, this strongly implies continuing volume loss and inadequate replacement.
In trauma the most likely cause of shock is blood loss. External blood loss from wounds and compound fractures is usually apparent, but haemorrhage into the abdomen and chest, or from closed long bone or pelvic fractures, is often missed.
Assess the patient’s Glasgow Coma Scale (GCS). Separately record the three components: eye opening, verbal response and motor response (Box 19.14).

 19.14 Glasgow Coma Scale
19.14 Glasgow Coma Scale
| Eye opening | |
| Spontaneous | 4 |
| To speech | 3 |
| To pain | 2 |
| No response | 1 |
| Verbal response | |
| Orientated | 5 |
| Confused: talks in sentences but disorientated | 4 |
| Verbalises: words, not sentences | 3 |
| Vocalises: sounds (groans or grunts), not words | 2 |
| No vocalisation | 1 |
| Motor response | |
| Obeys commands | 6 |
| Localises to pain, e.g. brings hand up beyond chin to supraorbital pain | 5 |
| Flexion withdrawal to pain: no localisation to supraorbital pain but flexes elbow to nail bed pressure | 4 |
| Abnormal flexion to pain | 3 |
| Extension to pain: extends elbow to nail bed pressure | 2 |
| No response | 1 |
| Record the GCS as a total and its three separate components: e.g. GCS 9/15: E3, V2, M4 |
Examine the limbs for localising signs or paraplegia.
Check the pupils for size, reactivity and equal reaction to light. In structural causes of coma (intracranial haemorrhage, infarction) the light reflex is usually absent; in metabolic causes (poisoning, hypoglycaemia, sepsis) it is usually present. A difference in pupil diameters >1 mm suggests a structural cause. The GCS can be misleading in some types of non-traumatic brain injury, for example stroke.
Check the blood glucose using a Stix test (Fig. 19.10). Hypoglycaemia usually causes a global neurological deficit with reduced consciousness, but may present with irritability, erratic or violent behaviour (sometimes mistaken for alcohol or drug intoxication), seizures or focal neurological deficits, e.g. hemiplegia.

If the stix test reading is <3 mmol/l, take a venous sample for formal blood glucose measurement, but treat before you get the result. Give 25–50 ml of 50% dextrose IV. If you cannot obtain venous access rapidly, give 1 mg glucagon by intramuscular (IM) injection. The conscious level should start to improve in 10–20 minutes if hypoglycaemia is the cause of the altered mental state. Repeat the stix test to confirm correction of hypoglycaemia.
Persistent altered consciousness where hypoglycaemia has been adequately corrected implies coexistent pathology, e.g. stroke, or cerebral oedema from prolonged neuroglycopenia. In patients with hypoglycaemia where you suspect chronic alcohol use or withdrawal, or malnutrition, give 100 mg IV thiamine to prevent and treat Wernicke’s encephalopathy (confusion, ataxia and eye signs – nystagmus and conjugate gaze palsies).
If you cannot clearly identify a cause for the patient’s altered conscious state, consider drug overdose. The most common acutely life-threatening drugs are opioids, which cause altered consciousness, respiratory depression (reduced respiratory rate and volume) and small pupils.
Titrate 0.8–2 mg IV naloxone (a specific opioid antagonist) as a diagnostic aid and definitive treatment to any patient with no clear cause for altered consciousness. In opioid intoxication, the patient responds within 30–60 seconds of IV administration. If IV access is difficult, give naloxone IM. If the patient responds, give further doses, as naloxone has a short duration (minutes), while the half-life of most opioids and their active metabolites is hours/days.
Give immediate treatment to stop active focal or generalised seizures. First-line therapy is IV lorazepam (0.5–1 mg/min up to 4 mg) or diazepam (1–2 mg/min up to 10–20 mg). If seizures continue despite this, other agents may be required, e.g. phenytoin.
Manage seizures in pregnancy using the ABCDE approach but consider the fetus as well. Seek senior obstetric and neonatal support immediately. Place women >20 weeks’ gestation in the left lateral position by placing one or two pillows under the right hip. This prevents the gravid uterus from obstructing venous return to the heart with consequent hypotension. Eclamptic seizures in pregnant and postpartum patients are associated with hypertension (diastolic blood pressure >100 mmHg), oedema (usually generalised and often affecting hands and face) and proteinuria. IV magnesium sulphate is a first-line treatment.
If the patient is not already fully undressed, remove remaining clothing. Cover the patient with a gown and warm blankets to prevent hypothermia and maintain dignity. Critically ill patients lose heat rapidly and cannot maintain normal body temperature.
Trauma patients may arrive on a rigid spinal board with neck immobilisation. Remove them from the board to reduce pressure sores and facilitate radiological examination. If the patient is conscious, explain what you are going to do before the patient is ‘log-rolled’ and lifted (Fig. 19.11). The process needs five people. One holds the head/neck and directs the procedure; one removes the spinal board and other debris, and examines the back and spine; the remaining three roll and hold the patient.
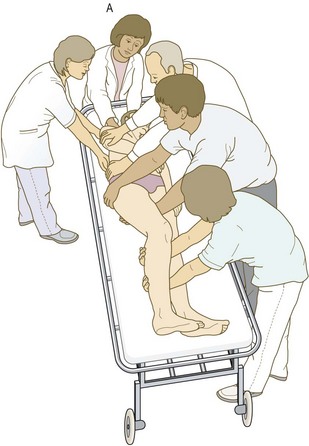
Fig. 19.11 Deployment of personnel and hand positions used when ‘log-rolling’ a patient from the supine to the lateral position.
The person (A) controlling the cervical spine should direct the manoeuvre.
While the patient is rolled, perform a rectal examination, assess anal tone and perianal sensation, and check the core temperature (p. 189).
Examine the patient’s skin surface rapidly but comprehensively. Look for bruises and wounds. In particular, examine the scalp, perineum and axillae. Note open fractures and rashes, e.g. the non-blanching purpuric rash of meningococcal septicaemia (Fig. 17.1) and hyperpigmentation (hypoadrenalism).
Investigations
See Box 19.15.
 19.15 The primary survey
19.15 The primary survey
investigations and interventions
| A | Administer high-flow oxygen |
| B | Measure respiratory rate and SpO2 |
| C | Monitor the electrocardiogram (ECG) continuously and measure blood pressure every 5 minutes |
| Insert and secure large-bore intravenous cannula(e) and take blood samples | |
| D | Record Glasgow Coma Scale |
| Record pupil size and reactivity | |
| Stix test for blood glucose | |
| E | Measure temperature (rectal or tympanic membrane) |
• Arterial blood gas measurement
• Chest X-ray (+ pelvic and cervical spine views in multiply injured)
• Urinary catheter* (and measure urine output hourly)
• Urinalysis (stix test) for blood, protein, glucose, ketones, nitrite, bilirubin and urobilinogen
• Urine pregnancy test in females
• Nasogastric tube†
*Contraindicated if urethral injury is suspected.
†Contraindicated if skull base fracture is suspected.
Secondary survey
The secondary survey reassesses the patient after the primary survey is complete. This is a systematic, detailed top-to-toe examination that fully documents additional signs and identifies injuries in the trauma patient. Only start the secondary survey once you are confident that there is no immediate need for further resuscitation and the patient does not require immediate transfer for definitive care, e.g. to theatre for a patient with a ruptured abdominal aortic aneurysm. Continually re-evaluate to assess the response to treatment. If the patient deteriorates or you are unsure about clinical status, return to the primary survey.
Give adequate analgesia to all patients in pain. There is no ‘standard’ dose. Slowly titrate an opioid drug, e.g. morphine IV in 1–2 mg aliquots to achieve pain relief. The amount needed varies according to the patient’s response and adverse effects, e.g. respiratory depression, hypotension.
Examination sequence
Examine the entire body surface. The skin appearance may suggest an underlying diagnosis, e.g. pallor (blood loss or anaemia), jaundice (hepatic failure), vitiligo or pigmentation in sun-exposed areas, recent scars and skin creases (Addison’s disease).
Look for rashes (in particular, the non-blanching purpuric rash of meningococcal disease) (Fig. 17.1), foci of infection (cellulitis, abscesses, erysipelas), bruising and wounds.
Perform a systematic top-to-toe examination, starting with the head. In a trauma patient palpate the scalp for swelling, and look for wounds which may be hidden in thick or tangled hair.
Look for signs of skull base fracture. These include periorbital bruising (‘raccoon’ or ‘panda’ eyes; Fig. 19.12A), subconjunctival haemorrhage (usually without a posterior margin; Fig. 19.12B), otorrhoea or rhinorrhoea, and most commonly bleeding from the ear or behind the tympanic membrane (haemotympanum). Battle’s sign (bruising over the mastoid process; Fig. 19.12C) may take 1–3 days to develop.

Fig. 19.12 Signs of skull base fracture.
(A) Periorbital bruising (‘raccoon’ or ‘panda’ eyes). (B) Subconjunctival haemorrhage. (C) Battle’s sign.
Examine the eyes for foreign bodies, including retained contact lenses (remove them at this stage), and signs of chronic disease, such as jaundice or anaemia. If you suspect corneal abrasions, stain the eye with fluorescein to identify them (Ch. 12).
Assess the pupils for size, shape, reactivity to light and accommodation.
Examine the eye movements, visual acuity and optic fundi. Urgently refer any patient with penetrating injury, disruption of the globe or loss of vision to a specialist ophthalmologist.
Smell the patient’s breath. The sweet odour of ketones in diabetic ketoacidosis is characteristic, but not everyone can detect it. Severe uraemia causes a ‘fishy’ smell, and hepatic failure a ‘mousy’ smell (fetor hepaticus) due to dimethyl sulphide. Note whether a patient smells of alcohol, but never attribute altered conscious level to alcohol alone.
Look in the mouth for injury to the palate, tongue and teeth.
Check the ears and throat for potential sources of infection.
Assume that the spine and/or spinal cord is injured in all trauma patients, especially those with altered consciousness. Conscious patients may complain of localised neck or back pain, but may be distracted by pain from other injuries. Maintain spinal immobilisation until you can exclude underlying injury. This is rarely possible in the initial assessment period, and many cases require imaging to exclude cord or bony injury.
If there is no history of trauma, ask the patient to flex his neck to touch his chin on his chest. If this causes discomfort, gently flex his neck passively. Meningeal irritation causes spasm of the paraspinal neck muscles with neck stiffness. Meningitis and subarachnoid haemorrhage are common causes and may be associated with photophobia and a positive Kernig’s sign (p. 248). Neck stiffness may be absent early in these conditions or with altered consciousness.
Re-examine the chest and precordium in detail (Chs 6 and 7).
Examine the abdomen, including the pelvis and perineum. Perform a rectal and vaginal examination if necessary. Remove any tampon in a menstruating female and consider toxic shock syndrome as a cause of her symptoms. Rectal examination is mandatory in patients presenting with signs of hypovolaemia, to help identify gastrointestinal bleeding. In trauma patients examine the perineum, rectum and urethral orifice before inserting a urinary catheter.
Check perianal sensation and rectal sphincter tone to assess potential spinal cord injury.
Clinical assessment of pelvis injury is often misleading. Palpation may identify fractures, but do not ‘spring’ the pelvis to assess stability, as this may precipitate further bleeding.
Examine each limb in turn. Look for wounds, swelling and bruising; palpate all bones and joints for tenderness and crepitus, and assess passive and active joint movements. Undisplaced long-bone fractures are easily missed in trauma patients. Always examine the neurovascular integrity of the limb distal to any injury.
Perform a full neurological examination. This is particularly important in patients with altered conscious level or possible spinal injury.
Examine joints for swelling suggesting septic or reactive arthritis (Box 19.16).
 19.16
19.16
Pupil changes and structural intracranial lesions
A dilated pupil (>1 mm in size between the pupils, anisocoria) in a patient with coma strongly suggests a structural intracranial lesion.
Touda Y, Nakazato N, Stein GH. Pupillary evaluation for differential diagnosis of coma. Postgrad Med 2003;79:49–51.
Investigations
Specific investigations will depend upon the presentation involved, e.g. CT for head injury. A 12-lead ECG and chest X-ray are standard and in patients with blunt trauma the initial X-rays should, as a minimum, include views of the cervical spine, chest and pelvis. Perform a urinary pregnancy test in all women of child-bearing age.
Ensure tetanus prophylaxis for all trauma patients who are non-immune. Give IV antibiotic therapy to patients with presumed meningococcal disease, septic shock and open fractures.
Document all investigations, therapy and response to treatment. Stop the assessment process if the patient needs immediate definitive care or investigation. Let the receiving team know exactly which stage of the assessment process you have reached when you hand over care of the patient.
Definitive treatment
Once stable, the patient is moved to a critical care area, theatre, scanning room or another hospital. This is high-risk and there must be sufficiently trained staff accompanying the patient. The critically ill patient needs to be adequately monitored and as ‘stable’ as possible. All relevant documentation and investigation results should accompany the patient, with clear lines of communication between clinicians.
If you discover that the patient is terminally ill and that this crisis is not unexpected, it may not be appropriate for the patient to be given aggressive or ‘heroic’ treatment. It may be difficult to recognise and prepare for a patient’s death but it is essential and humane. Communicate with the family, the GP and the senior clinician previously involved in the patient’s care. Care for the patient in a dignified manner, with the emphasis on analgesia, relief of distressing symptoms and the highest quality of nursing care.