Psychotherapeutic Agents
1 Name and describe the three categories of functional disorders discussed in this chapter.
2 Outline some basic precautions that the dental health care professional should keep in mind when treating patients with psychiatric disorders.
3 Summarize the basic mechanism of action, pharmacologic effects, adverse reactions, drug interactions, and uses of the antipsychotic agents.
4 Describe the mechanism of action, pharmacologic effects, adverse reactions, drug interactions, uses, and dental implications of the tricyclic antidepressants.
5 Describe the mechanism of action, pharmacologic effects, adverse reactions, drug interactions, uses, and dental implications of the selective serotonin reuptake inhibitors.
Many drugs have the ability to affect mental activity. Some of these drugs are used in the treatment of psychiatric disorders. The dental health care worker is most likely to encounter the use of these agents in dental patients who have had them prescribed by psychiatrists or other physicians. Because these agents are so widely prescribed and can alter the patient’s dental treatment, the dental health care worker must understand their pharmacologic effects, adverse reactions, and dental implications.
Agents used in the treatment of the major psychiatric disorders are discussed in this chapter. Those used to treat anxiety are discussed in Chapter 11. The anticonvulsants used as “mood stabilizers” are discussed in Chapter 16. Because the psychotherapeutic drugs are classified by their therapeutic use, a brief discussion of the common psychiatric illnesses follows.
PSYCHIATRIC DISORDERS
There are many psychiatric disorders. They may be divided into types such as organic and functional or primary and secondary, depending on their suspected cause. Organic illness is congenital or caused by an injury or a disease. Functional disorders are partially of psychogenic origin, without evidence (yet) of structural or biochemical abnormality (Figure 17-1). The naming and categorization of different mental disorders changes as more information becomes available. Functional disorders include the following categories:
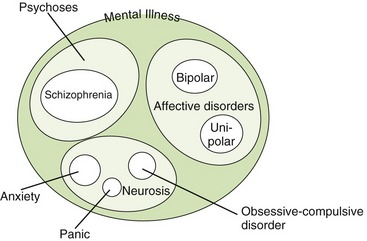
The psychoses are discussed first. Schizophrenia, the most common type of psychosis, is an extensive disturbance of the patient’s personality function with a loss of perception of reality. Schizophrenia is derived from the word meaning “splitting,” and in context it refers to patients splitting from reality (not into multiple personalities). The patient’s ability to function in society is impaired because of altered thinking. The impaired thinking of these patients may be so detached from reality and their delusions or paranoia (e.g., someone is out to get me) so severe that their illness could lead to committing serious crimes, including assassination attempts or murders. Patients may suffer from hallucinations, delusions, or agitation. The positive symptoms of psychosis include agitation, extrapyramidal symptoms, and auditory hallucinations. Other patients may be introspective and uninvolved. The negative effects of psychosis include flat affect and apathy (Box 17-1).
The etiology of schizophrenia is not specifically known, but a familial pattern is often seen. The biochemical actions of the brain and even brain anatomy have been demonstrated to be different from findings in normal individuals in some patients with schizophrenia.
Affective disorders include endogenous and exogenous unipolar depression and bipolar depression (mania). The condition in patients who exhibit only depression is termed unipolar depression. Endogenous (involutional) depression seems to be unrelated to external events, whereas exogenous (reactive) depression appears to be related to specific external events. Whether there are actually two types of depression separated by circumstances of occurrence is questionable. Theories for several different types of depression based on the biochemical situation in the brain have been hypothesized, but no one has been able to show different groups. Patients who exhibit alternating periods of depression and excitation (mania, elation) have bipolar (bi, two) depression, also known as manic-depressive disorder.
Neuroses are less severe than psychoses but can also be helped by drug therapy. Examples include anxiety, panic disorder, phobias, and obsessive-compulsive disorder. Psychophysiologic (somatic) disorders are those that have an emotional origin but manifest by physiologic symptoms. Personality disorders include sexual deviation, alcoholism, and drug dependence. Although many of these conditions are managed using the antidepressants and/or antipsychotics, the anxiety-related problems sometimes require the use of the benzodiazepines. Divisions of these different mental disorders have been and are continually changing to reflect either an increased knowledge or a political or “fad” perspective. (What is “normal” anyway?)
This presentation is an oversimplification of the classifications of psychiatric disorders. The drug groups discussed in this chapter include antipsychotic agents, used to treat psychoses; antidepressant agents, used to treat affective disorders; and lithium, used to treat bipolar disorder. The benzodiazepines, used to treat anxiety and panic disorders, are discussed in Chapter 11.
Before the antipsychotic drugs were introduced into the management of psychiatric disorders, many physical methods were used to treat patients. Only electroconvulsive therapy (ECT, shock therapy) is still used in the treatment of depression. With the use of neuromuscular blocking agents, the use of ECT therapy has become much safer. ECT produces the fastest results of any treatment for depression. It is reserved for patients who are refractive to antidepressants. Some memory loss occurs during the treatment (several sessions).
When treating patients with mental disorders, the following general precautions should be observed by the dental health care worker:
• Communication: Patients with various mental disorders may perceive comments or movement from dental health care workers as threatening. Even normal office discussions may be perceived differently than they are intended. For example, small talk with a peer may be interpreted as a conspiracy by the patient. What you say around and to the patient should be carefully monitored. (I once asked a patient “How are you?” and the patient replied with a loud and angry voice, “Why are you asking me that question?”)
• Compliance: Patients undergoing drug therapy for the treatment of psychoses often do not take their medication as prescribed. A thorough health history including the patient’s medication and its dosage should be obtained.
• Suicide: Depressed patients may attempt suicide. Therefore the amount of any drug prescribed at one time should not exceed the amount required for a lethal dose (usually a 1-week supply). When patients are severely depressed, they have no motivation and usually do not act on any irrational thoughts of suicide. After beginning to take an antidepressant, partial improvement gives them the motivation to attempt suicide before the full antidepressant effects have developed. Children and teens appear to be at a higher risk for suicide with antidepressant therapy, especially with the newer class of drugs. In a suicide attempt, drugs are often combined. For example, a patient may mix an opioid analgesic given for the relief of a toothache, a sedative-hypnotic prescribed for dental anxiety, and an antidepressant medication prescribed by the patient’s physician.
ANTIPSYCHOTIC AGENTS
The antipsychotic agents are divided into two major groups depending on their ability to target both the positive and negative symptoms of schizophrenia. Until the past few years, the conventional antipsychotics were the most often used group of antipsychotics. Table 17-1 lists the conventional antipsychotics and their usual adult daily dose for outpatient treatment. More patients are now being treated with the newer antipsychotics referred to as the “atypical” antipsychotics.
TABLE 17-1
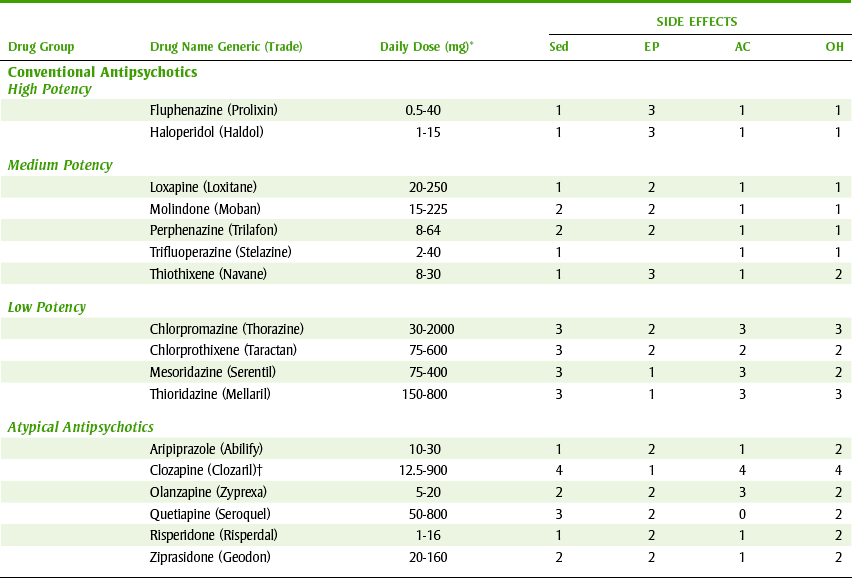
AC, Anticholinergic; EP, extrapyramidal; OH, orthostatic hypotension; Sed, sedation; O, nonexistent; 1, very low; 2, low; 3, moderate; 4, high.
*Usual oral dose for outpatient treatment in milligrams/day.
†Agranulocytosis; weekly white blood cell (WBC) count needed.
The atypical antipsychotics—so named because they were unlike the conventional antipsychotics—have different receptor activities and adverse reaction profiles. As a group, these agents have more nausea and less anticholinergic and sedative effects than occur with the conventional antipsychotics.
The actions of the antipsychotic agents are diverse. Of the conventional antipsychotics, no single agent is clearly superior in its antipsychotic action. However, with the advent of the atypical antipsychotics, patients who were previously resistant to conventional antipsychotic agents have been adequately managed with these new drugs. Antipsychotics that act on several receptors have a broader range of action and can be used in more difficult cases. Clinical judgment and the drug’s side effect profile in a particular patient determine which agent is used. In general, the lower potency agents such as chlorpromazine (klor-PROE-ma-zeen) (Thorazine) have more sedation, more peripheral side effects, and more autonomic effects (e.g., dry mouth), whereas the higher-potency agents such as haloperidol (ha-loe-PER-i-dol) have more extrapyramidal effects and less sedation. Other common phenothiazines include thioridazine (thye-oh-RID-a-zeen) (Mellaril) and trifluoperazine (trye-floo-oh-PAIR-a-zeen) (Stelazine).
Pharmacologic Effects
When conventional antipsychotics are used for treatment of psychoses, any effects other than the antipsychotic effect could be considered an adverse reaction. When used as an antiemetic, other actions would be adverse reactions such as sedation. The pharmacologic effects of the conventional antipsychotic agents include the following.
Antipsychotic Effect: All conventional antipsychotics possess antipsychotic effects associated with slowing of the psychomotor activity in an agitated patient and calming of emotion with suppression of hallucinations and delusions. These agents are active against the positive effects of psychosis but have little effect on the negative effects. Atypical antipsychotics differ in that they are effective against both the positive and negative symptoms of schizophrenia.
Antiemetic Effect: The conventional antipsychotic’s antiemetic effect is a result of depression of the chemoreceptor trigger zone, an area in the brain that causes nausea and vomiting. These agents are useful in the symptomatic treatment of certain types of nausea and vomiting. Historically, prochlorperazine (Compazine) has been used for this effect.
 ATYPICAL ANTIPSYCHOTIC AGENTS
ATYPICAL ANTIPSYCHOTIC AGENTS
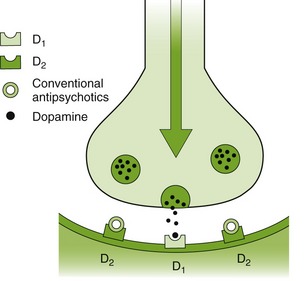
There are several differences between the conventional antipsychotic agents and the newest, or atypical, antipsychotic agents. The conventional antipsychotic agents were primarily dopamine antagonists (Figure 17-2). The atypical agents have action at more than one receptor, for example, the dopamine, serotonin (5-HT), and norepinephrine (NE) receptors, which results in the improved efficacy of these agents. The side effects of the atypical antipsychotics are less than the conventional antipsychotics. Like the conventional antipsychotics, the atypical antipsychotics are effective against the positive effects associated with psychoses. However, unlike the conventional antipsychotics, the atypical antipsychotic agents are effective against the negative effects. Table 17-1 lists the conventional and atypical antipsychotics.
Adverse Reactions
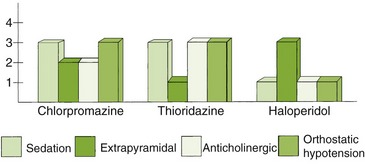
Table 17-1 lists the side effects of the conventional and atypical antipsychotic agents, and Figure 17-3 demonstrates the relative side effects of several conventional antipsychotic agents. Management of patients taking these agents involves minimizing the troubling side effects in each patient.
SEDATION
Conventional antipsychotics differ in the degree of sedation and drowsiness they produce. The degree of sedation is one factor that determines which antipsychotic agent is prescribed. In contrast to the sedative-hypnotic agents, with higher doses the conventional antipsychotics do not produce anesthesia and the patient is easily aroused. Tolerance develops to the sedative effect but not to the antipsychotic effect.
EXTRAPYRAMIDAL EFFECTS
The most common type of adverse reactions associated with these agents results from stimulation of the extrapyramidal system. All conventional antipsychotics produce this effect, although the incidence of the reaction varies. The following types of extrapyramidal effects can occur:
• Acute dystonia consisting of muscle spasms of the face, tongue, neck, and back
• Parkinsonism with symptoms of resting tremor, rigidity, and akinesia
• Akathisia, or increased compulsive motor activity
• Tardive dyskinesia, an irreversible dyskinesia involving the tongue, lips, face, and jaw
Tardive dyskinesia is typically seen in women patients who are older than 40 years and have been taking large doses of the phenothiazines for a minimum of 6 months to 2 years or as long as 20 years. The onset is gradual and the movements are coordinated and rhythmic. This effect is exacerbated by drug withdrawal. The involuntary movements, especially those involving the face, jaw, and tongue, can make home care difficult if not impossible. Performing oral prophylaxis is difficult because of the strength of the oral facial and tongue muscles.
The dental health care worker should discuss the patient’s side effects with his or her physician if oral prophylaxis cannot be performed. A dosage or drug change may be instituted by the patient’s psychiatrist. With the availability of the atypical agents, extrapyramidal side effects can be greatly minimized.
The extrapyramidal side effects of conventional antipsychotics can cause severe intermittent pain in the region of the temporomandibular joint (TMJ). This pain is produced by a spasm of the muscles of mastication. In an acute attack, it becomes difficult or impossible to open or close the jaw. Should muscle spasm be present, force should not be exerted to open the patient’s mouth for dental treatment because dislocations of the mandible can occur.
Treatment of an acute spasm of the mandible must be undertaken after consultation with the patient’s prescribing physician. Alternatives may include decreasing the dose of the patient’s medication, adding an anticholinergic medication to counteract the spasm, or changing the patient’s antipsychotic medication to one that produces fewer extrapyramidal effects. The anticholinergics used to counteract the extrapyramidal side effects of the antipsychotics include benztropine (Cogentin) and trihexyphenidyl (Artane).
ORTHOSTATIC HYPOTENSION
Because these agents depress the central sympathetic outflow and block the peripheral adrenergic receptors (α-sympathetic blockers), they can produce orthostatic hypotension that is additive with other CNS depressants. When a patient rises rapidly from the supine position, a compensatory tachycardia can accompany the orthostatic hypotension.
OTHER CARDIOVASCULAR EFFECTS
These agents have also been reported to cause tachycardia. Ziprasidone significantly prolongs the QT/QTc interval. Periodic electrocardiograms (ECGs) should be performed on patients receiving ziprasidone.
SEIZURES
Because conventional antipsychotics lower the convulsion threshold, seizures may be more easily precipitated in a patient taking these agents, especially if a previous history of epilepsy exists. Bupropion (Wellbutrin, Zyban) can produce seizures, and therefore patients on conventional antipsychotics may not be candidates for its use. Consultation with the patient’s psychiatrist would be warranted.
ANTICHOLINERGIC EFFECTS
The anticholinergic effects of conventional antipsychotics produce blurred vision, xerostomia, and constipation. This is especially significant because the anticholinergic effects of other medications the patient may be taking are additive. The anticholinergics, such as benztropine, used to treat the extrapyramidal symptoms are additive, too. The dental health care worker should be aware of the presence of xerostomia and question patients regarding their method of managing this problem.
OTHER EFFECTS
As previously mentioned, conventional antipsychotics have many adverse effects, including blood dyscrasias, cholestatic jaundice, skin eruptions, and photosensitivity reactions that are exaggerated by sunlight or even by the light from the dental unit.
AGRANULOCYTOSIS
The atypical antipsychotic, clozapine (KLOE-za-peen) (Clozaril), is useful in treating patients with treatment-resistant schizophrenia. Because it produces potentially life-threatening agranulocytosis, clozapine should be tried only after several trials of other agents have failed. Frequent white blood cell counts with differential are required during therapy. With the release of newer atypical antipsychotic agents, use of this agent has decreased.
Drug Interactions
CENTRAL NERVOUS SYSTEM DEPRESSANTS
Conventional antipsychotics interact in an additive or even potentiating fashion with all CNS depressants, including barbiturates, alcohol, general anesthetics, and opioid analgesics. Sedation and respiratory depression can occur.
EPINEPHRINE
Epinephrine, used as a vasoconstrictor in local anesthetic solutions, can be safely used in patients taking conventional antipsychotics. However, because the conventional antipsychotics are α-adrenergic blockers, epinephrine should not be used to treat vasomotor collapse (acute drop in blood pressure) because it could cause a further decrease in blood pressure. This occurs because of the predominant β-agonist (vasodilating) activity of epinephrine in the presence of the conventional antipsychotics (α-blockers). However, using epinephrine-containing local anesthetics in patients taking antipsychotics is acceptable in dentistry.
ANTICHOLINERGIC AGENTS
To control excessive extrapyramidal stimulation, conventional antipsychotic therapy often must be combined with antiparkinson medication of the anticholinergic type, for example, benztropine (Cogentin). This combination is bound to exacerbate antimuscarinic peripheral effects such as xerostomia, urinary retention, constipation, blurred vision, and inhibition of sweating.
Uses
Antipsychotics are the drugs of choice for treatment of schizophrenia. Long-acting injectable conventional antipsychotics, such as fluphenazine (Prolixin) and haloperidol (Haldol), are available for patients with schizophrenia who fail to take their oral medication.
Dental Implications
The dental management of patients taking antipsychotics is summarized in Box 17-2.
SEDATION
Sedation, an adverse reaction of the conventional antipsychotics, is additive with that of other sedating agents.
ANTICHOLINERGIC EFFECTS
Conventional antipsychotics are additive with other agents with atropine-like effects; this combination can lead to toxic reactions, including tachycardia, urinary retention, blurred vision, constipation, and xerostomia. The dental health care worker should be aware that patients may use sugar-containing candy to counteract xerostomia. Use of sugarless products or artificial saliva (Orex, Xero-Lube, Moi-Stir) should be encouraged. Patients should be encouraged to stay away from caffeine-containing beverages because they can exacerbate dry mouth. They should also avoid alcohol-containing mouth rinses because alcohol can also exacerbate dry mouth.
ORTHOSTATIC HYPOTENSION
Orthostatic hypotension effect can be minimized by raising the dental chair slowly and assisting the patient’s first few steps.
EPINEPHRINE
Epinephrine should be avoided in the management of an acute hypotensive crisis in patients taking antipsychotics. It may be safely used in local anesthetic solutions for dental patients.
ANTIDEPRESSANT AGENTS
Antidepressant agents are used not only to manage depression but also for a variety of other uses such as chronic pain adjuvant or migraine headache prophylaxis. One should question the patient to determine the indication for which a tricyclic antidepressant is being prescribed. The dental professional should not assume that the patient is being treated for depression. Until the late 1950s, there was no widely accepted pharmacologic treatment for depression. Forms of mild depression were treated with psychotherapy, and severe depression was treated with ECT. Several classes of antidepressants are currently available, including tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs). Several new, atypical antidepressants, some with unique properties, have been recently released. ECT is still used in the treatment of severely suicidal patients and those resistant to antidepressants. In the case of suicidal thoughts, ECT works faster than any antidepressant drug.
The antidepressants may block NE and/or serotonin (5-HT) reuptake (Table 17-2 and Figure 17-4), produce sedation, and have anticholinergic side effects. One theory of their mechanism of action involves blocking reuptake of NE and/or 5-HT. Another involves downregulation of the β-adrenergic receptors.
TABLE 17-2

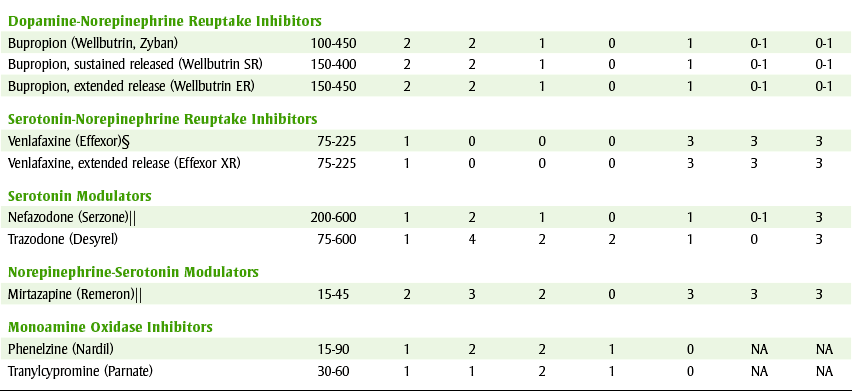
0, Nonexistent; 1, very low; 2, low; 3, moderate; 4, high; AC, anticholinergic; NA, not applicable; N, D, nausea and diarrhea; NE, norepinephrine reuptake inhibitors; OH, orthostatic hypotension; SED, sedation; SERT, serotonin reuptake inhibitors; Wt+, weight gain.
*Usual adult daily dose (mg).
†Used for obsessive-compulsive disorder (OCD).
‡Used primarily for OCD.
§In divided doses.
¶Antagonizes α2-adrenergic receptors.
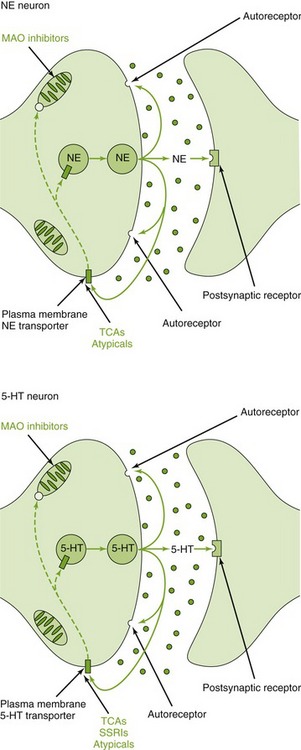
FIGURE 17-4 A noradrenergic and serotonergic synapse and sites at which antidepressants may exert their actions. TCAs, SSRIs, and some atypical antidepressants inhibit the reuptake transporter for NE and/or 5-HT. Monoamine oxidase, which is targeted by MAO inhibitors, is localized at the outer mitochondrial membrane. (From Minneman KP, Wecker L: Brody’s human pharmacology: molecular to clinical, ed 4, Philadelphia, 2005, Mosby.)
Tricyclic Antidepressants
The TCAs are sometimes referred to as the first-generation antidepressants because they were developed and marketed before the second-generation agents. Table 17-2 lists the antidepressants with their usual adult outpatient daily dose in milligrams. All TCAs are similar in their antidepressant effectiveness, differing only in their side effect profile.
PHARMACOLOGIC EFFECTS
The action of TCAs on normal and depressed patients is somewhat different. In the normal patient, an undesirable sedation and fatigue and strong atropine-like side effects are noted. In the depressed patient, a feeling of well-being, elevation of mood, and a dulling of depressive ideation are noted. Sedation occurs often, but tolerance to this effect often develops. Increased ability to concentrate and improvement in sleep is seen with the TCAs. It can take up to 6 weeks for the patient to experience the full pharmacologic effects of the antidepressant.
ADVERSE REACTIONS
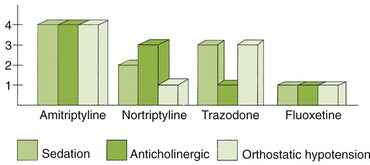
Some of the widely diverse adverse reactions associated with the TCAs resemble those of the antipsychotic agents (Figure 17-5; see Table 17-2).
Central Nervous System Effects: Almost all of the TCAs induce some degree of sedation. Patients should develop tolerance to this sedation.
Autonomic Nervous System Effects: The peripheral effects of TCAs are primarily on the autonomic nervous system. These agents possess distinct anticholinergic effects resulting in xerostomia, blurred vision, tachycardia, constipation, and urinary retention. Some tolerance can develop with continued use. Although TCAs initially produce orthostatic hypotension like the conventional antipsychotics, tolerance to this effect occurs.
Cardiac Effects: The most serious peripheral side effect associated with the TCAs is cardiac toxicity. Myocardial infarction and congestive heart failure have occurred during the course of treatment. Arrhythmias and episodes of tachycardia can be caused by the antimuscarinic (anticholinergic, atropine-like) effects of the TCAs. New antidepressants do not cause this reaction.
DRUG INTERACTIONS
TCAs potentiate the behavioral actions of the amphetamines and other CNS stimulants. TCAs potentiate the pressor effect of injected sympathomimetics. These agents also interact with monoamine oxidase inhibitors, resulting in severe toxic reactions. TCAs may be displaced from plasma protein binding sites by phenytoin. TCAs may be metabolized more quickly because of induction of hepatic microsomal enzymes by barbiturates, carbamazepine, and cigarette smoking. They may interfere with the antihypertensive effects of guanethidine and clonidine. Additive anticholinergic effects are seen if they are administered with other agents with anticholinergic action.
POISONING
Accidental poisoning with TCAs has become more common, and such an overdose can be lethal. The effects of acute poisoning are severe hypertension, cardiac arrhythmias, hyperpyrexia, convulsions, coma, and respiratory failure. Survivors may have permanent myocardial damage. The treatment is symptomatic and should be conservative in view of the interactions with other CNS vasopressor agents. Activated charcoal or gastric lavage may be helpful. Physostigmine has been reported to be effective in treating mild poisoning by tricyclic antidepressants.
USES
TCAs can be used alone or in combination with antipsychotics or ECT in the treatment of depression. In patients who are suicide risks, the long onset of action of the TCAs (several weeks) requires the use of ECT during the initial phase of drug treatment. These agents, which are allowed after several weeks for the development of their effects, can prevent relapse and thus provide long-term control of depression.
When sedation is desired, amitriptyline (a-mee-TRIP-ti-leen) (Elavil) is used. When less sedation is needed, nortriptyline (nor-TRIP-ti-leen) (Pamelor, Aventyl) or protriptyline (proe-TRIP-ti-leen) (Vivactil) can be tried. However, the use of TCAs has decreased because of their less than desirable adverse effect profile and because of the continuing development of newer antidepressants.
TCAs are often combined with one of the antipsychotics (usually an atypical because of the more tolerable side effect profile) in the treatment of patients with both psychoses and depression. Comments relating to the dental implications of both TCAs and antipsychotics apply to patients taking this type of product. Certain antidepressants are used for specific indications. For example, imipramine (im-IP-ra-meen) (Tofranil) is used to control nocturnal enuresis (incontinence) in children. Clomipramine (cloe-MIP-ra-meen) (Anafranil) is used only in the treatment of obsessive-compulsive disorder. Patients with obsessive-compulsive disorder repeatedly perform certain rituals such as hand washing. Doxepin (DOX-e-pin) (Adapin, Sinequan) is used when an antianxiety effect is desired.
DENTAL IMPLICATIONS
The management of dental patients taking antidepressants is summarized in Box 17-3.
Sympathomimetic Amines: Vasoconstricting drugs (sympathomimetic amines) in the local anesthetic solution must be administered with caution to patients taking TCAs. They may potentiate vasopressor (increased blood pressure) response to epinephrine. In the usual cardiac dose (0.04 mg), the sympathomimetic amines present in a local anesthetic solution can be safely administered to patients without preexisting arrhythmias.
Xerostomia: The anticholinergic effect of sympathomimetic amines is additive with that of other agents that produce dry mouth. The dental health care worker should question patients about the products used to alleviate this troublesome side effect and suggest alternatives such as artificial saliva or sugarless gum.
Second-Generation Antidepressants
Second-generation antidepressants (see Table 17-2) are newer antidepressants that possess fewer side effects than the tricyclic antidepressants. For example, they have fewer anticholinergic effects and less cardiotoxicity, and some have less sedation effect. The choice of antidepressant is based on the adverse reaction profile and the individual patient’s response to the agent.
TRAZODONE
Trazodone (TRAZ-oh-done) (Desyrel) is a serotonin modulator antidepressant unrelated chemically to TCAs. It appears to have antidepressant effects equivalent to those of TCAs. Its advantages include that it has fewer anticholinergic effects (e.g., xerostomia) and is less cardiotoxic even in toxic doses. Its disadvantages include that it is highly sedative and has been associated with painful priapism requiring surgical intervention and leaving some patients permanently impotent.
Selective Serotonin Reuptake Inhibitors
A newer group of antidepressants, the SSRIs, have specific action on inhibiting the reuptake of 5-HT. Fluoxetine (floo-OX-uh-teen) (Prozac) was the first member of this group, and others have followed. Sertraline (SER-tral-leen) (Zoloft), paroxetine (pa-ROKS-e-teen) (Paxil), and fluvoxamine (floo-VOX-a-meen) (Luvox) are other members of this group. Their antidepressant action is equivalent to that of TCAs. Their advantage lies in their adverse reaction profile, which differs from that of TCAs (see Table 17-2).
ADVERSE REACTIONS
Central Nervous System Effects: Unlike many of the TCAs, the SSRIs tend to produce CNS stimulation (activation) rather than CNS depression. Headache, dizziness, tremor, agitation, sweating, and insomnia are side effects associated with stimulation. Weight loss or weight stabilization occurs more often than the weight gain that occurs with TCAs. Somnolence and fatigue have also been reported.
Gastrointestinal Effects: Nausea and diarrhea occur in about 15% to 30% of patients. Anorexia, dyspepsia, and constipation have been reported.
Bupropion
Bupropion (byoo-PROE-pee-on) (Wellbutrin [SR]) is a dopamine-NE reuptake inhibitor that has been on the market and then off the market; in 1993 it was back on the market with increased warnings. About 0.4% of patients treated with bupropion have experienced seizures. This incidence may be 4 times greater than with the TCAs and as much as 10 times greater with TCAs at higher doses. Because of its seizure potential, it is reserved for patients who are not responsive to other agents. Gastrointestinal effects, such as constipation, nausea, and vomiting, occur in about 20% of patients. Neurologic effects, such as dry mouth (28%), headache (25%), excessive sweating, and tremors, have been reported. Agitation (32%) and dizziness (22%) occur often. Divided doses, slow titration of doses, and careful patient selection can minimize seizure risk.
Other Antidepressant Agents
Nefazodone (nef-AY-zoe-done) (Serzone), venlafaxine (Effexor), and mirtazapine (Remeron) are examples of newer antidepressants. They are indicated for the treatment of depression. Nefazodone, like trazodone, is a 5-HT modulator, and venlafaxine is a 5-HT-NE reuptake inhibitor. Mirtazapine is a NE-5-HT modulator. The incidence of xerostomia is greater than 10%, and sexual dysfunction often occurs with nefazodone and venlafaxine. Venlafaxine is a weak inhibitor of cytochrome P-450 2D6 isoenzymes. Nefazodone increases the serum levels of alprazolam, triazolam, and digoxin. Nefazodone carries a black box warning regarding its potential to cause life-threatening hepatic failure. Mirtazapine causes somnolence, weight gain, constipation, and dry mouth.
Monoamine Oxidase Inhibitors
Monoamine oxidase inhibitors (MAOIs) include a large variety of drugs that have the ability to inhibit monoamine oxidase. MAOIs possess many adverse effects, and an overdose can lead to a severe toxic reaction. MAOIs interact with many drugs, such as amphetamines, and with foods, such as cheeses, wines, and fish, precipitating a hypertensive crisis and even death. Patients taking MAOIs have detailed food prohibitions because of the chance of drug-food interactions. Because of the potential for life-threatening situations, MAOIs are used as drugs of last choice. Patients taking MAOIs should not be given any drug unless the prescriber has first consulted a reference source on drug interactions.
DRUGS FOR TREATMENT OF BIPOLAR DEPRESSION
Until fairly recently, lithium was the major drug used in the treatment of bipolar depression. Other agents commonly used today include a variety of anticonvulsants, including carbamazepine, valproate, and gabapentin. These agents are often referred to as “mood stabilizers.”
Lithium
Lithium (LITH-ee-um) (Eskalith, Lithobid) is used in the treatment of bipolar (manic) depression, which is characterized by cyclic recurrence of mania alternating with depression. The side effects, which can be minimized by monitoring serum lithium levels, include polyuria; fine hand tremor; thirst; and in more severe cases, slurred speech, ataxia, nausea, vomiting, and diarrhea. Patients undergoing lithium therapy should be observed for signs of overdose toxicity, which may be exhibited by CNS symptoms, including muscle rigidity, hyperactive deep reflexes, excessive tremor, and muscle fasciculations. Because lithium is handled in the body like sodium, changes in sodium levels can affect lithium levels. Salt intake and sweating can also change lithium levels. Some nonsteroidal antiinflammatory drugs (NSAIDs) can decrease lithium clearance, leading to an increase in lithium levels (Box 17-4). A patient’s serum lithium levels before, during, and after taking naproxen are illustrated in Figure 5-10.
Anticonvulsants
In the treatment of bipolar depression (mania), several anticonvulsant agents have been used. The manic phase has been treated with anticonvulsants such as carbamazepine, valproate, and gabapentin. Valproate and carbamazepine are approved by the Food and Drug Administration (FDA) for treating bipolar disorder. Valproate is used more often than lithium because of its more tolerable side effect profile.
CLINICAL SKILLS ASSESSMENT
1. State the major pharmacologic effect of the conventional antipsychotics.
2. State the adverse reactions attributable to the conventional antipsychotics.
3. Explain the drug interactions between epinephrine and the conventional antipsychotics and epinephrine and the tricyclic antidepressants. State which is clinically significant.
4. Describe two advantages of the atypical antipsychotics.
5. List three adverse reactions associated with the tricyclic antidepressants.
6. State the agent used in the treatment of poisoning by tricyclic antidepressants.
7. Name a second-generation antidepressant and describe two advantages and two disadvantages.
8. State the advantages and disadvantages of the SSRIs over the TCAs.
9. Describe two advantages of the atypical antidepressants over the TCAs.
10. Name the agent used to treat bipolar affective disorders and describe its effect on saliva.
 Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.
Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.