Autocoids and Antihistamines
1 Define histamine and discuss its pharmacologic effects, adverse reactions, and uses.
2 Describe the dental implications, pharmacologic effects, adverse reactions, toxicity, and uses of the antihistamines.
3 Name and discuss the mechanism of action of nonsedating H1-receptor antagonists.
4 Categorize the prostaglandins and thromboxanes and outline their pharmacologic effects, uses, and dental implications.
5 List several other types of autocoids and describe how they work.
The term autocoids is derived from the Greek autos (self) and akos (remedy). Although the agents in this class possess widely differing pharmacologic actions, they all occur naturally in the body, are produced by many tissues, and are formed by the tissues on which they act.
The autocoid agonists or antagonists include the H1- and H2-receptor antagonists (H1-RA) or blockers, the eicosanoids (prostaglandins [PGs], thromboxanes [TXs], and leukotrienes [LTs]), serotonin agonists, angiotensin inhibitors, and cytokinins. As research on these agents continues, the agonists and their potential antagonists hold great promise for future therapy in many different areas. In fact, LT antagonists (see Chapter 22) are new drugs used for the management of asthma.
HISTAMINE
Histamine is a ubiquitous biogenic amine. Although many of its peripheral actions are well known, its precise physiologic function, particularly in the central nervous system (CNS), is not clear. The structure of histamine is seen in Figure 18-1.
Almost all mammalian tissues contain or can synthesize histamine. In humans, histamine is stored in the mast cells in the intestinal mucosa and in the CNS. When an allergic reaction occurs, the mast cells degranulate and histamine is released.
Histamine is released from the tissues in the body by normal reactions, abnormal reactions, or the administration of certain drugs. The amount of histamine released in these reactions determines the effects seen in the patient.
Pharmacologic Effects
In humans, histamine causes the following effects:
With the synthesis of agents that can block some of the effects of histamine, new pharmacologic agents have been developed. The histamine receptors are termed H1 and H2. Some evidence of an H3-receptor exists. The H1-receptors are primarily related to vasodilation, increased capillary permeability, bronchoconstriction, and pain or itching at the nerve endings (the first four items on the preceding list). The H2-receptors are responsible for stimulating gastric acid secretion (the last item on the preceding list) and will be reviewed in Chapter 22. The action of the H3-receptor is unknown.
Histamine’s actions are mediated by activation of H1-receptors, H2-receptors, or other receptors. Agents that block or antagonize the effects of histamine at the H1-receptors are referred to as H1-blockers or H1-receptor antagonists (H1-RA), and at the H2-receptors they are H2-blockers or H2-receptor antagonists (H2-RA).
Adverse Reactions
When an allergic reaction occurs, an antigen-antibody reaction causes the release of histamine and other autocoids. Anaphylaxis is a serious and sometimes fatal reaction to a foreign protein or drug introduced into the body. Difficulty in breathing, convulsions, lapses into unconsciousness, and death can ensue. The predominant feature in this syndrome is bronchoconstriction.
In addition to bronchoconstriction, the action of histamine during an anaphylactic reaction includes vasodilation and increased capillary permeability, both of which lead to decreased blood pressure followed by shock and cardiovascular collapse. Other symptoms of anaphylaxis include apprehension, paresthesia, urticaria, edema, choking, cyanosis, coughing, and wheezing. Fever, shock, loss of consciousness, coma, convulsions, and death may result.
Although the treatment of anaphylaxis is described in Chapter 23, it is discussed here in relation to its cause. The drug of choice for anaphylaxis is parenteral epinephrine, a physiologic antagonist (epinephrine dilates bronchioles via the β2-receptors) rather than an antihistamine, which is a pharmacologic antagonist (antihistamine blocks the bronchoconstriction produced by histamine at the same H1-receptor). The reason for this is that antihistamines antagonize only some of the effects of histamine, and they work competitively, whereas epinephrine acts as a direct β2-agonist.
ANTIHISTAMINES (H1-RECEPTOR ANTAGONISTS)
The common term antihistamine refers to agents that are H1-receptor antagonists or H1-blockers. They are widely used drugs, and dental practitioners should be familiar with them for the following reasons:
• Many patients have seasonal allergic reactions (e.g., hay fever) that make dental treatment difficult. The dentist may prescribe, or the patient may self-medicate with antihistamines before a dental procedure to reduce the symptoms of hay fever and make it easier for the patient to breathe.
• A mild allergic reaction to a drug may be treated with antihistamines in the dental office. If the allergic reaction is severe, epinephrine is the drug of choice.
• Patients taking antihistamines may experience side effects, such as xerostomia, but the newer nonsedating antihistamines have less anticholinergic effect.
• Antihistamines interact with many other drug groups and are additive with other CNS depressants.
Pharmacologic Effects
The older H1-receptor antagonists, also called H1-blockers, have several pharmacologic effects, including antihistaminic, anticholinergic, antiserotonergic, and sedative effects. Because they have a chemical structure similar to that of histamine, they can bind with the H1-receptor and prevent or block the action of histamine (if it is released). Table 18-1 gives the chemical groups of various antihistamines, some examples of each group, and the properties of each group.
TABLE 18-1
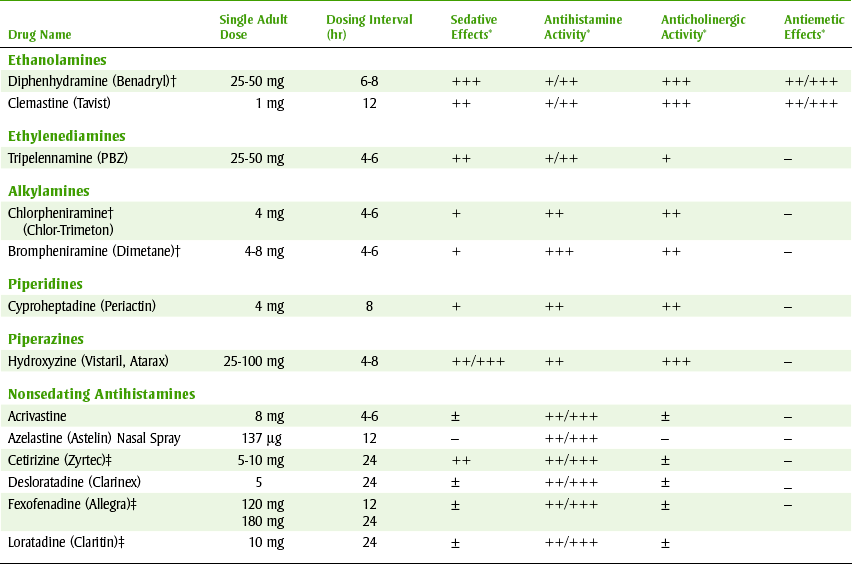
*++++, Very high; +++, high; ++, moderate; +, low; ±, may have some effect; –, no effect.
†Available over-the-counter.
‡Also available in combination with pseudoephedrine.
Figure 18-2 compares the relative sedative, antihistaminic, and anticholinergic effects of five common antihistamines: brompheniramine (brome-fen-EER-a meen) (Dimetane), chlorpheniramine (klor-fen-EER-a-meen) (Chlor-Trimeton), diphenhydramine (dye-fen-HYE-dra-meen) (Benadryl), fexofenadine (feks-oh-FEN-a-deen) (Allegra), and loratadine (lor-A-ti-deen) (Claritin). One should note that some antihistamines are effective for nausea and that some have more anticholinergic effects (more xerostomia).
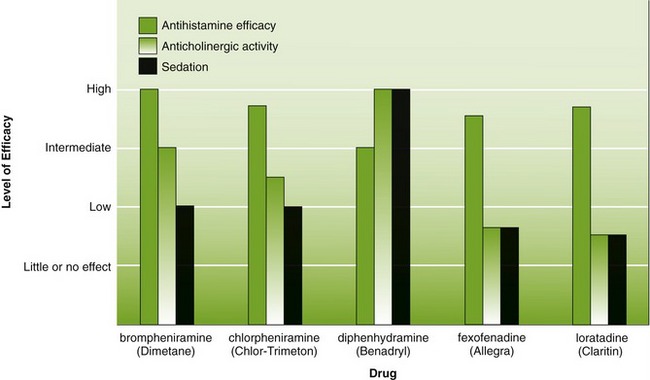
FIGURE 18-2 Comparison of efficacy and adverse effects of selected antihistamines. (From Lilley LL, Harrington S, Snyder JS: Pharmacology and the nursing process, ed 5, St Louis, 2007, Mosby.)
The pharmacologic effects of antihistamines can be divided into those caused by blocking histamine at the H1-receptor and those independent of this effect.
 H1-RECEPTOR BLOCKING EFFECTS
H1-RECEPTOR BLOCKING EFFECTS
Antihistamines, which are H1-antagonists, competitively block or antagonize histamine’s effect at the following sites:
• Capillary permeability: By blocking capillary permeability produced by histamine, less tissue edema occurs from the transport of the serum into the intracellular spaces.
• Vascular smooth muscle (vessels): The antihistamines block the dilation of the vascular smooth muscle that histamine produces.
• Nonvascular (bronchial) smooth muscle: Because other autocoids are also released in an anaphylactic reaction, antihistamines are not effective in counteracting all the bronchoconstriction present during that reaction.
• Nerve endings: Antihistamines can suppress the itching and pain associated with this histamine-mediated reaction at the cutaneous nerve endings.
OTHER EFFECTS (UNRELATED TO H1-BLOCKING EFFECTS)
Central Nervous System Effects: The antihistamines produce varying degrees of CNS depression. Because diphenhydramine produces a high degree of sedation, it is the principal agent used in over-the-counter (OTC) sleep aids (Sominex, Nytol). It is less expensive as an antihistamine than as a sleep aid.
Anticholinergic Effects: An anticholinergic effect (cholinergic blockade), weaker than but similar to that of atropine, can be used to “dry up” secretions when treating the symptoms of certain upper respiratory diseases (allergies, “cold”). A potential disadvantage with the anticholinergic effect is that secretions may be “dried up” and more difficult to clear.
Antiemetic Effects: Some antihistamines, such as meclizine (Dramamine, Bonine), have pronounced antiemetic or anti–motion sickness activity. These agents are also effective in controlling the dizziness, nausea, and vomiting that occurs with vertigo.
Antihistamines with antiemetic effects may be useful in dentistry to manage postoperative nausea and vomiting, especially when opioid agents have been used. The antihistamines that have phenothiazine-like action, such as promethazine, are the most effective antiemetics.
Adverse Reactions
Like the pharmacologic effects of the antihistamines, the adverse reactions vary in relative amounts among the different agents. Figure 18-2 shows how adverse reactions and pharmacologic effects vary among antihistamines.
CENTRAL NERVOUS SYSTEM DEPRESSION
CNS depression can be either a pharmacologic effect (the wanted effect) or an adverse reaction (the unwanted effect), depending on the use. Sedation is the most common side effect associated with the older antihistamines, and it may be accompanied by dizziness, tinnitus, incoordination, blurred vision, and fatigue. Patients who are given antihistamines should be warned against operating a motor vehicle or signing important documents. Sedation with antihistamines is additive with that caused by other CNS depressant drugs.
As with all drugs that depress the CNS, stimulation or excitation can occur in a few cases. Symptoms include restlessness, excitation, and, in severe cases, convulsions. It is more common in children, elderly patients, and those who use a larger dose than prescribed. The newer nonsedating H1-blockers, such as loratadine (Claritin), produce less sedation because they do not penetrate the brain as easily.
When antihistamines are combined with decongestants (adrenergic agents), the antihistamine-related CNS depression is counteracted by the CNS stimulation of the decongestants. The planned result is for each agent’s CNS effects to cancel out the other’s effects.
Many antihistamine-decongestant combinations are marketed for treatment of colds or sinus problems. They are available OTC and by prescription
GASTROINTESTINAL EFFECTS
The gastrointestinal complaints commonly associated with the antihistamines include anorexia, nausea, vomiting, and constipation. Xerostomia is categorized as an anticholinergic adverse reaction. The H2-blockers (see Chapter 22), not the H1-blockers, antagonize histamine’s effect on the secretion of stomach acid.
ANTICHOLINERGIC EFFECTS
The H1-receptor antagonists have varying anticholinergic effects. The importance to the dental health care worker is that anticholinergic effects lead to xerostomia and xerostomia leads to numerous dental problems. Xerostomia can cause an increased caries rate in patients taking antihistamines on a long-term basis. In patients taking chronic antihistamines, the mouth should be observed for symptoms of xerostomia and counseling about techniques to manage it should be presented.
The nonsedating antihistamines have much less anticholinergic effect and are less likely to produce xerostomia. Loratadine (Claritin) is a heavily advertised nonsedating antihistamine.
Toxicity
Antihistamine poisoning has become more common in recent years because of the easy accessibility of the agents in OTC preparations promoted as sleep aids. Excitation predominates in small children, and sedation can occur in adults. Death usually results from coma with cardiovascular and respiratory collapse. The treatment is directed at specific symptoms.
Uses
Certain allergic reactions, such as allergic rhinitis and seasonal hay fever, can be controlled by antihistamines. With continued use, tolerance can develop to the effects of a particular antihistamine. Changing to an agent in another chemical group can often restore the effects desired. These agents are less useful in the treatment of the common cold. Some people like the anticholinergic effect on secretions and want all their secretions to stop.
Acute urticarial attacks can be treated with antihistamines to relieve itching, edema, and erythema. In the treatment of anaphylaxis, the physiologic antagonist epinephrine rather than the antihistamines is indicated first. The xanthines (aminophylline) are also more effective than the antihistamines in producing bronchodilation in acute anaphylaxis. Because antihistamines produce some local anesthetic effect when applied topically, certain painful oral lesions can be treated with topical antihistamines. For example, with discomfort, the patient may swish and swirl diphenhydramine liquid inside the mouth.
NAUSEA AND VOMITING
Because of the antiemetic action of some antihistamines, they are used to prevent and treat motion sickness and to control postoperative vomiting and vomiting induced by radiation therapy. The nausea and vomiting associated with pregnancy should not be treated with antihistamines because of these agents’ alleged potential for fetal harm.
PREOPERATIVE SEDATION
The use of the older H1-antihistamines in dentistry is primarily based on their CNS effects. They are used for preoperative sedation because of their sedative and antiemetic effects. Hydroxyzine and promethazine are useful for this purpose (see Table 18-1). Their antiemetic actions can be helpful to counteract the adverse effect of the opioids.
PERIPHERAL (NONSEDATING) H1-RECEPTOR ANTAGONISTS
Chemically, members of the nonsedating H1-receptor antagonists do not have any common denominator. They are different in origin, chemical structure, solubility, and metabolic effects. They all share the specific blocking action of peripheral H1-receptors. Because they do not cross the blood-brain barrier in usual therapeutic doses, they do not produce sedation (really, they are less likely to produce sedation). Table 18-1 lists the nonsedating antihistamines. Often, both sedating and nonsedating antihistamines are combined with a decongestant to treat nasal congestion along with the signs and symptoms of allergic response.
Peripheral (nonsedating) antihistamines have become valuable adjuncts in the therapy of seasonal and perennial rhinitis and certain forms of urticaria. It is likely that these agents will eventually replace the older H1-receptor antagonists for these conditions. In the treatment of dental patients, however, the place of the older H1-receptor blockers is ensured because these compounds are used as much for their side effects (sedation, potentiation of opioids, reduced nausea) as for their antihistaminic action. Many of them also come as a combination product with a decongestant.
Fexofenadine
Fexofenadine (Allegra) is an active metabolite of terfenadine (Seldane) and was developed by the manufacturer of terfenadine (Seldane) to replace it. Terfenadine was found to be responsible for cardiac arrhythmias and changes in the electrocardiogram (ECG) secondary to other drugs that inhibited its metabolism, and as a result, it was withdrawn from the market.
Because fexofenadine does not cross the blood-brain barrier to any appreciable degree, the potential for sedation is greatly reduced. Side effects include drowsiness and viral infections. It has little of the anticholinergic effects exhibited by the traditional H1-blockers. Both erythromycin and ketoconazole increase the level of fexofenadine (by inhibiting its metabolism), but no clinical manifestations have been noted. Whether interactions will occur with other imidazoles or macrolides (clarithromycin, azithromycin) must be determined. Its onset of action is about 1 hour, and its time to peak serum concentration is 2.6 hours. Its duration of action is at least 12 hours, and its half-life is 14.4 hours. About 20% is metabolized in the liver and excreted in the urine, and 80% is excreted in the feces. Its dose is 60 mg twice a day.
Loratadine
Loratadine (lor-AT-i-deen) (Claritin), another nonsedating antihistamine, has similar action to the other drugs in this group. Its onset is 1 to 3 hours, its peak effect is 8.4 to 28 hours, its duration of action is 24 hours, and its half-life is 12 to 15 hours. It is extensively metabolized to an active metabolite. Adverse reactions include headache, somnolence (less than 10%), fatigue, and xerostomia.
Desloratadine
Desloratadine (Clarinex) is the active metabolite of loratadine and is a nonsedating H1-receptor blocker. It is also dosed once daily. Side effects include fatigue, dry mouth, headache, and gastrointestinal disturbances.
Cetirizine
Cetirizine (se-TI-ra-zeen) (Zyrtec) is another nonsedating H1-receptor blocker. Its onset of action is usually less than  hour, and it peaks in about 1 hour. Its half-life is 8 hours. The intense competition among the companies selling nonsedating antihistamines is brutal. It is also available without a prescription.
hour, and it peaks in about 1 hour. Its half-life is 8 hours. The intense competition among the companies selling nonsedating antihistamines is brutal. It is also available without a prescription.
OTHER AUTOCOIDS
Prostaglandins and Thromboxanes
The prostaglandins (PGs) and thromboxanes (TXs) are members of a group of biologically active agents termed eicosanoids.
Other members of this group include the leukotrienes (LTs), lipoxins, hydroperoxyeicosatetraenoic acids (HPETEs), hydroxyeicosatetraenoic acids (HETEs), and epoxyeicosatetraenoic acids (EETEs). The PGs and TXs have been found in most body tissues and fluids. They are produced in the body in response to many different stimuli, and small quantities produce a large spectrum of effects on many different body systems.
The family of PGs is divided into six main series of agents: A, B, C, D, E, and F, of which the last two (E and F) are predominant. These main groups are further subdivided and give rise to an extensive and complicated series of compounds. The subscript numbers (1, 2, and 3) following the letters indicate the degree of unsaturation. The α or β refers to the spatial configuration of the carbon 9 hydroxyl group (e.g., PGF2α).
Until recently, PGEs and PGFs were the most abundant and most intensively studied PGs. Now, many new PGs (e.g., PGG and PGH), TXs (e.g., TXA and TXB), and prostacyclin (PGI) have become the central interest.
Because the individual PGs have many activities, it is unlikely that they have a single receptor. They are released by mechanical, thermal, chemical, bacterial, or traumatic injuries.
PHARMACOLOGIC EFFECTS
The pharmacologic effects of the PGs encompass many diverse actions. Not only is there a wide spectrum of action, but different PGs have different activities in different tissue. As PG agonists or antagonists are identified, the number and range of actions in the body will be increased. Some currently known effects of the PGs include the following.
Smooth Muscle Effects: Vascular smooth muscle may be either relaxed (vasodilation) or stimulated (vasoconstriction) depending on the specific PGs. The effect of PGs on the gastrointestinal tract is to produce cramping (increased motility). Their effect on the uterus is to cause contraction, especially in the near-term uterus.
Platelets: Another example of the opposing actions of different PGs is TX and PGI. TX, produced by platelets, stimulates platelet aggregation and is a vasoconstrictor, whereas PGI, produced by the vessel walls, inhibits platelet aggregation and is a vasodilator. Fine gradations of action in the body can be elicited using this mechanism in which two different chemicals produce the opposite effect. If secretion of one of the paired autocoids is increased, then the desired action is produced. Conversely, secretion of the other autocoid produces the opposite effect. In addition, antagonists to these autocoids block their normal effects. For adjusting one particular effect, there may be both agonist and antagonist effects for each autocoid. This “system” to modulate adequate coagulation can be modified by adding a drug. Adding of aspirin can alter the clinical outcome. Even altering the dose of aspirin can produce different effects (low dose and high dose).
Effects on Reproductive Organs: PGs are abundant in the semen, but their role is unknown. Both PGE and PGF have oxytocic (uterine contraction) action, making them useful as abortifacients in the second trimester and as inducers of labor at full term.
Central Nervous System Effects: PGs increase body temperature by releasing interleukin-1, which promotes the release and synthesis of PGE. PGEs stimulate the release of hormones such as growth hormone, prolactin, thyroid-stimulating hormone (TSH), adrenocorticotropic hormone (ACTH), follicle-stimulating hormone (FSH), and luteinizing hormone (LH).
DENTAL IMPLICATIONS
The PGs are important in dentistry because they have been implicated in periodontal disease. At least two stages of periodontal disease may involve PGs. The first is the inflammation of the gingiva with its resultant erythema, edema, and increase in gingival exudate. PGs, thought to be mediators of the inflammatory response in oral soft tissues, may be involved in this initial stage of periodontal disease. The second is the resorption of alveolar bone with tooth loss. PGs also prevent the synthesis of new bone by inhibiting osteoblastic activity. This explains the reason the use of nonsteroidal antiinflammatory drugs (NSAIDs) in the management of periodontal disease is being explored.
Newer research concerning the etiology of periodontal disease has discovered more correlations among different factors. Certainly, several autocoids, such as PGs, LTs, and cytokines, have been found to be involved in the production of periodontal disease.
USES
One therapeutic use of the PGs is inducing midtrimester abortions. PGs are administered by intraamniotic injection (a salt of PGF) or vaginal suppository (PGE analog). For very early abortions, PGE analogs are combined with antiprogestins (mifepristone [Mifeprex] or RU-486) in an oral dose form currently available in France and the United States. A PG agonist (misoprostol [Cytotec]) is available for the prevention of NSAID-induced ulcers. PGE is cytoprotective at low doses. Currently, PGs are being studied in the treatment of bronchial asthma and hypertension.
PROSTAGLANDIN ANTAGONISTS
The administration of PG antagonists may prove useful in the treatment of certain pathologic conditions. This seems reasonable in view of the many effects of the PGs in the body. For example, aspirin can inhibit platelet aggregation by blocking TX (which promotes aggregation). Indomethacin, an NSAID, blocks the effect of the PGs on the ductus arteriosus (PGs keep the ductus arteriosus open). After birth, if the ductus arteriosus does not close, indomethacin given intravenously can close the ductus, thereby making open heart surgery unnecessary. There is also some evidence that certain phenolic compounds, such as eugenol (clove oil), dentistry’s poultice, inhibit PG. Because PGs are involved in inflammation, agents that inhibit the PGs may be useful in the treatment of inflammation.
Leukotrienes
LTs are another complex group of autocoids that are also derived from arachidonic acid. They were formerly called slow-reacting substance(s) of anaphylaxis (SRS-A). Although they show considerable species variation, their dominant action in humans is powerful bronchoconstriction. In that effect, LTs are far more potent than histamines. They also contract other smooth muscle such as the uterus and gastrointestinal tract. Extensive research is devoted to these substances, and great progress can be expected, potentially in the treatment of asthma and other forms of bronchoconstriction.
Kinins
Kinins are polypeptides that are distributed in a great variety of body tissues. Two members of this group, kallidin and bradykinin, are found in plasma and may play a role in dental diseases. These agents are formed by the action of certain proteolytic enzymes (kininogenases), such as kallikrein, on their common precursor, kininogen. Other kininogenases include trypsin, plasmin, and certain snake venoms. There are at least two receptors for bradykinin: the B1-receptor and the B2-receptor. The “B” in these receptors stands for bradykinin; they are not to be confused with the β-adrenergic receptors present in the sympathetic autonomic nervous system.
The plasma kinins may be involved in shock and acute or chronic allergic or inflammatory conditions such as anaphylaxis and arthritis. Their effects on the body include vasodilation, increased capillary permeability, edema, pain resulting from action on nerve endings, and contraction or relaxation of nonvascular smooth muscles. The kinins apparently mediate pulpal pain and are implicated in the control of the synthesis of endogenous analgesics, particularly the endorphins, during caries formation. It is possible that inhibitors of kinins may be useful dental therapeutic aids in the future.
Although no specific antagonists of the kinins are yet available, some drugs are known to inhibit kinin-evoked responses. For example, salicylates (aspirin) and glucocorticoids (steroids) inhibit kallikrein activation and may play a role in future therapy.
The synthesis of antagonists to the autocoid kinins and their possible clinical use are currently being investigated.
Substance P
Substance P is a peptide thought to function as a neurotransmitter in the CNS and a local hormone in the gastrointestinal tract. It is a vasodilator and produces hypotension. It increases the action of the intestinal and bronchial smooth muscle. It also causes secretion in the salivary glands and an increase in sodium and water excretion from the kidney. Substance P may be a transmitter that is released from unmyelinated fibers that respond to pain. It is also involved in many other functions because it is present in areas of the brain that are not involved in pain.
CLINICAL SKILLS ASSESSMENT
1. What are first-generation antihistamines and how do they work?
2. What are the pharmacologic effects of first-generation antihistamines?
3. What are the adverse reactions associated with first-generation antihistamines? Can they lead to toxicity?
4. What would the dental practitioner tell a patient about adverse reactions with a special emphasis on those with dental implications?
5. What are the drug interactions associated with first-generation antihistamines that are of dental concern?
6. What is the mechanism of action of second-generation antihistamines?
7. What are the adverse reactions of second-generation antihistamines?
8. What are the advantages of second-generation antihistamines over first-generation antihistamines?
 Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.
Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.