Respiratory and Gastrointestinal Drugs
1 Summarize the two groups of respiratory diseases.
2 Name and describe the mechanisms of action of several types of drugs used to treat respiratory diseases.
3 Discuss the types of drugs used to treat respiratory infections, including the implications to dentistry.
4 Summarize the most common types of gastrointestinal diseases.
5 Name and describe the types of drugs used to treat gastrointestinal diseases, including any implications to dentistry.
Diseases of the respiratory and gastrointestinal tracts are common, so dental health care workers are sure to encounter patients taking drugs for these diseases (Figure 22-1). Because the medications given to treat these diseases can affect dental treatment, the dental health care worker should be aware of the effects of these drugs on the patient and how these drugs can alter the dental treatment plan.
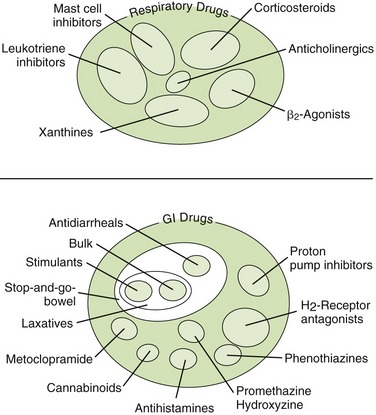
RESPIRATORY DRUGS
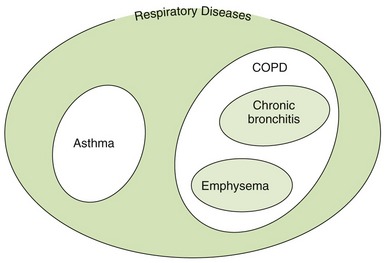
Diseases that are treated with respiratory drugs include asthma, chronic obstructive pulmonary disease (COPD), and upper respiratory tract infections (Figure 22-2). Respiratory drugs come from a wide range of drug groups, from adrenergic drugs for bronchodilation to corticosteroids for reducing inflammation. Drugs that increase expectoration and reduce coughs are also included in this discussion. Many drugs used to treat respiratory problems are administered topically via the lungs by the use of a metered-dose inhaler (MDI).
Respiratory Diseases
Noninfectious respiratory diseases are divided into two groups: (1) asthma and (2) COPD (see Figure 22-2). COPD is further divided into chronic bronchitis and emphysema. Other respiratory problems are related to respiratory infections, such as viral or bacterial.
 ASTHMA
ASTHMA
One common respiratory disease is asthma. It is characterized by reversible airway obstruction and is associated with reduction in expiratory airflow. A few hours later, inflammation occurs, resulting in an increase in secretions in the lungs and swelling in the bronchioles. Asthma is classified as being either intermittent or persistent. Persistent asthma is further categorized as mild, moderate, or severe. Patients with intermittent asthma experience symptoms less than two times a month and the symptoms do not interfere with normal activity. Persistent asthma occurs anywhere from more than twice a week to all day long. Persistent asthma can cause minor limitation of normal activities, and severe persistent asthma can severely limit the patient’s normal activities. When asthma is treated, both components of the disease must be addressed. The National Asthma Education and Prevention Program Expert Panel Report 3, published in October 2007, presents the latest recommendations of the National Heart Lung and Blood Institute regarding asthma therapy. Figure 22-3 reviews the stepwise approach for managing asthma in children older than 12 years of age and adults.
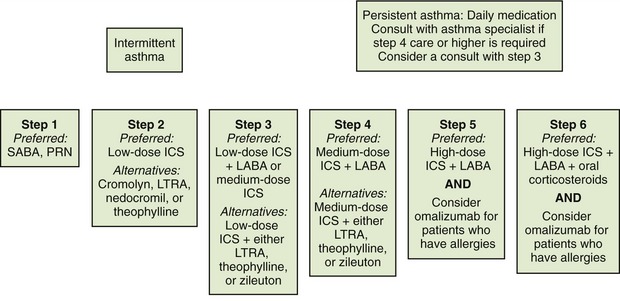
FIGURE 22-3 Stepwise approach for the management of asthma in persons 12 years of age or older. All patients require a rescue SABA inhaler whether they have intermittent or persistent asthma. SABA, Short-acting β2-agonist; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LTRA, leukotriene receptor antagonist. (From National Asthma Education and Prevention Program Expert Panel 3: Guidelines for the diagnosis and management of asthma, Bethesda, Md, 2007 [October], National Heart Lung and Blood Institute, National Institutes of Health, U.S. Department of Health and Human Services.)
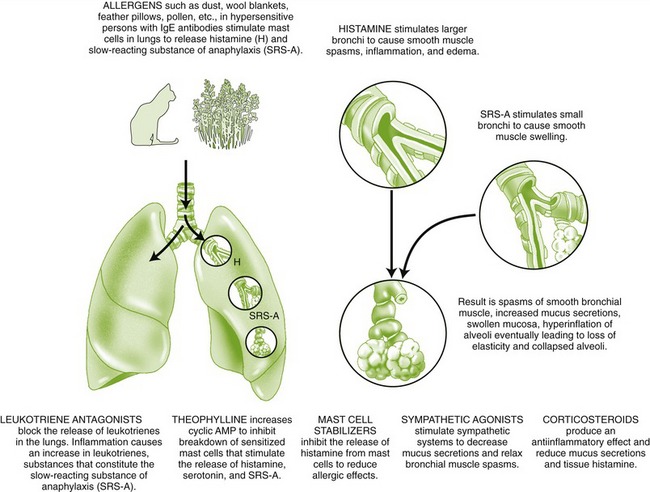
Asthma may be precipitated by allergens, pollution, exercise, stress, or upper respiratory infection (allergic reaction to viruses). In status asthmaticus, patients have persistent life-threatening bronchospasm despite drug therapy. Environmental pollution may also play an important role in the increase in asthma. The dental health care worker should treat dental patients with asthma so that minimal stress is induced. Patients should bring their fast-acting β2-agonist inhalers to be used prophylactically or in the management of an acute asthmatic attack in the dental office. Signs of asthma include shortness of breath and wheezing. Observation and questioning of the patient for asthma control before the dental appointment by the dental health care worker can prevent an acute attack. β-Adrenergic agonists, xanthines, cromolyn, corticosteroids, leukotriene (LT)-altering agents, and anticholinergics are used to treat this disease (Figure 22-4).
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
COPD is characterized by irreversible airway obstruction, which occurs with either chronic bronchitis or emphysema. Smoking is associated with almost all COPD. Chronic bronchitis is a result of chronic inflammation of the airways and excessive sputum production. Emphysema is characterized by alveolar destruction with airspace enlargement and airway collapse. The anticholinergics are the first-line treatment, but β-adrenergic agonists and xanthines are also used to produce bronchodilation in these patients. In many instances patients receive a combination metered dose inhaler with an anticholinergic drug and a β2 agonist. COPD and emphysema are associated with an increase in the incidence of bronchospasm and with fixed airway obstruction. Patients with upper respiratory tract infections often take adrenergic agonists for nasal congestion or bronchoconstriction, antihistamines to reduce secretions, expectorants to thin sputum, and antitussives to control coughing. Each drug group is discussed separately.
In the normal person, the drive for ventilation (breathing) is stimulated by an elevation in the partial pressure of carbon dioxide (Paco2). The partial pressure of oxygen (Pao2) can vary widely without stimulating ventilation in the normal patient. Patients with COPD, because their ventilation is compromised, experience a gradual rise in Paco2 over time. Because this mechanism becomes resistant to changes in Paco2, a new stimulus emerges, the partial pressure of Pao2. The patient’s ventilation is then driven by a decrease in Pao2. If a patient with COPD is given oxygen and the Pao2 rises, the stimulant to breathing is removed, and there is the possibility of inducing apnea. For patients with severe COPD, it is suggested that oxygen be limited to less than 3 L/min. Other literature recommends that in severe COPD, oxygen by nasal cannula be used during a dental appointment, especially if pain or stress is expected (increased oxygen demand).
DRUGS USED TO TREAT RESPIRATORY DISEASES
The MDI (Figure 22-5), developed in the 1950s, provides a useful method to administer certain medications to the respiratory tree. It is the preferred route of delivery for most asthma drugs. Its advantages include the following:
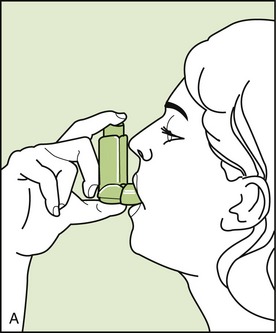
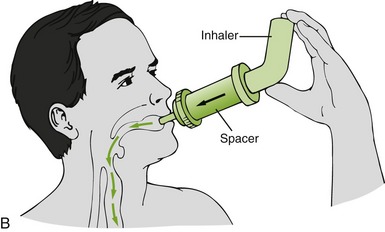
FIGURE 22-5 A, Metered-dose inhaler (MDI) for treatment of respiratory conditions. B, MDI with spacer. (B from Clayton BD, Stock YN, Harroun RD: Basic pharmacology for nurses, ed 14, St Louis, 2007, Mosby.)
• It delivers the medication directly into the bronchioles, thereby keeping the total dose low and side effects minimal.
• The bronchodilator effect is greater than a comparable oral dose.
• The inhaled dose can be accurately measured.
• The onset of action is rapid and predictable (versus unpredictable response with orally administered agents).
• MDIs are compact, portable, and sterile, making them ideal for the ambulatory patient.
Disadvantages of MDIs are that they are difficult to use properly (particularly for children) and they can be abused, with a resultant decrease in response. Additional patient education is required to get the most from this dose form. Often, a “spacer” is placed between the MDI and the mouth to increase the amount of drug delivered to the lungs (see Figure 22-5, B). Medications currently available in MDIs include β-agonists, both specific and nonspecific; corticosteroids; cromolyn; and anticholinergic drugs.
Chlorofluorocarbons (CFCs), which have ozone-depleting properties, have been phased out as propellants in MDIs. Nonchlorinated hydrofluoroalkane (HFA) propellants that do not deplete the ozone layer have replaced the CFCs.
Sympathomimetic Agents
Sympathomimetic or adrenergic agonists produce bronchodilation by stimulation of the β-receptors in the lungs. Chapter 4 discusses the presence of β-receptors in the heart (β1) (tachycardia) and lungs (β2) (bronchodilation). With the development of selective β2-agonists (β2 > β1), bronchodilation with fewer cardiac side effects can be achieved. The selective β2-agonists, used orally, by inhalation, and parenterally, are currently one of the mainstays of respiratory therapy.
SHORT-ACTING β2-AGONISTS
The short-acting β2-agonists have specificity for the respiratory tree. Side effects include nervousness, tachycardia, and insomnia. Short-acting β2-agonists, such as albuterol, may be administered by inhalation (metered dose or nebulization with an air compressor) or orally (tablet or liquid). Table 22-1 lists some short- and long-acting β2-agonists and their routes of administration. The first line of treatment for intermittent asthma is a short-acting β2-agonist (see Figure 22-3). The short-acting β2-agonists are the drugs of choice for the emergency treatment of an acute attack of asthma. Recent studies have found that the overuse of these agents results in airway hyperresponsiveness and a decrease in the lung’s response to them. Therefore these agents should be used primarily for the treatment of acute problems, not for the management of normal breathing function. One major mistake that many asthmatics make is to rely on the albuterol inhaler and omit using the steroid inhaler. The reason this occurs is because the albuterol gives an immediate response.
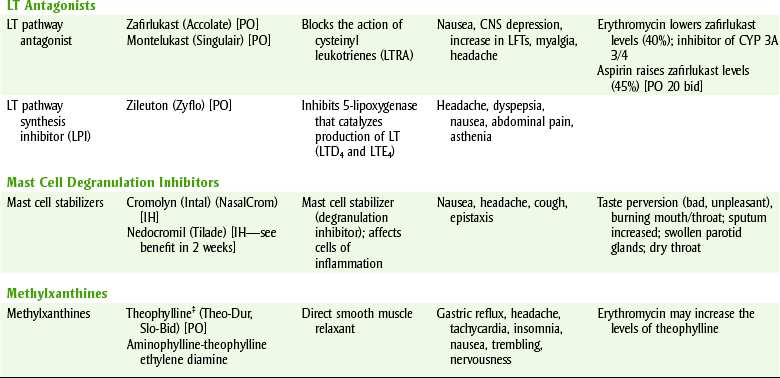
TABLE 22-1
FDA-APPROVED DRUGS USED TO MANAGE ASTHMA
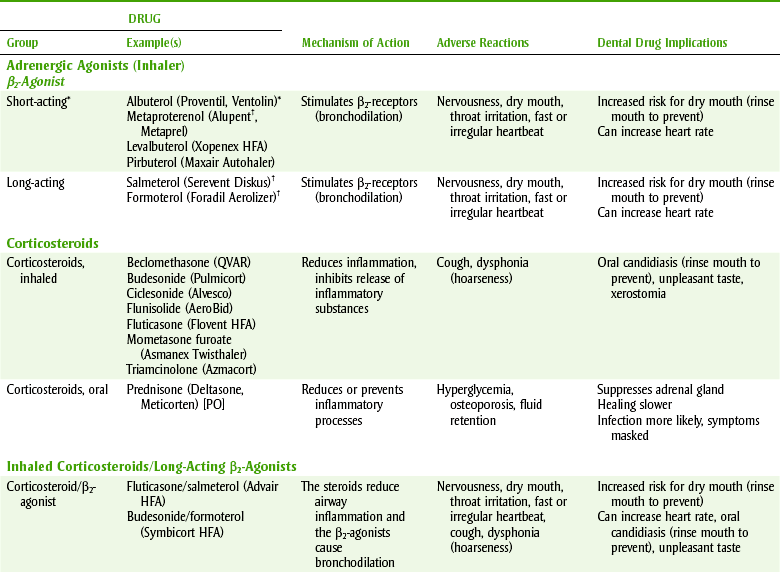
Consideration for asthma patients: avoid morning appointments, more allergenic potential, hypersensitivity to aspirin, NSAIDs, sulfites; more common, especially with nasal polyps.
bid, Twice a day; BP, blood pressure; CNS, central nervous system; IH, inhalation; LFTs, liver function tests; LT, leukotriene; PO, by mouth.
*Use for an acute attack.
†Do not use in an emergency, delayed onset >1 hr, prolonged effect (12 hr).
‡Relative of caffeine found in coffee and cola beverages.
LONG-ACTING β2-AGONISTS
Long-acting β2-agonist inhalers (see Table 22-1 and Figure 22-1) are used in conjunction with low-dose corticosteroids, to treat patients with persistent asthma that are not well-controlled on low-dose inhaled corticosteroids. Long-acting β2-agonists improve lung function, decrease symptoms, and reduce exacerbations and rescue use of short-acting β2-agonists. They are not recommended as monotherapy for asthma. Long-acting β2-agonists carry a black box warning about a higher risk of asthma-related deaths because of a high number of asthma-related deaths reported with salmeterol therapy during a clinical trial. Long-acting β2-agonists are best administered in a fixed-dose combination in the same inhaler with an inhaled corticosteroid (see Table 22-1). Long-acting β2-agonists are combined with corticosteroid inhalers so that two different drugs, at lower doses, can be used to treat persistent asthma.
Corticosteroids
Inhaled corticosteroids are the most effective long-term treatment for control of symptoms in all patients with mild, moderate, or severe persistent asthma (see Table 22-1). Randomized, controlled clinical trials have demonstrated that inhaled corticosteroids are more effective than LT modifiers, long-acting β2-agonists, cromolyn, or theophylline in improving pulmonary function, preventing symptoms and exacerbations, reducing the need for emergency room visits, and decreasing the number of asthma-related deaths. Most patients experience a positive response at relatively low doses. The optimal dose may decrease or increase over time but it should always be tailored to the lowest possible dose. Doses depend on the inhaled corticosteroid and the inhaler device. Common inhalers contain beclomethasone (be-kloe-METH-a-sone), triamcinolone (trye-am-SIN-oh-lone), and fluticasone (Flovent) (see Table 22-1). Patients taking these corticosteroids have a significant improvement in pulmonary function with a decrease in wheezing, tightness, and cough. The orally inhaled corticosteroids are especially useful in reducing inflammation and therefore the secretions and swelling that occur within the lungs after an asthma attack occurs. Although the steroids produce no immediate benefit in an acute asthmatic attack, they hasten recovery and decrease morbidity in these patients. They also reduce hyperreactive airway.
The side effects of steroids vary, depending on the route of administration, frequency of intake, duration of intake, total dose, and preexisting diseases a patient may have.
Chronic oral corticosteroids, such as prednisone, may be necessary in some severely asthmatic patients and even in patients with moderate asthma, especially during respiratory infections. Prolonged systemic use can result in adrenal suppression, poor wound healing, and immunosuppression. Supplemental steroids may need to be considered if adrenal suppression has occurred (see Chapter 19).
Candidiasis of the oral cavity can result from the chronic use of an inhalation corticosteroid. When the dental health professional performs an oral examination of any patient using steroid inhalers, any symptoms of candidiasis should be noted and treated. Patients using oral corticosteroid inhalers should be advised to rinse the mouth and gargle with water after using the inhaler to minimize the chance of candidiasis.
Steroids are also available as sprays for allergies. An example is beclomethasone (Beconase, Vancenase). It reduces the stuffiness by reducing inflammation within the nasal canal.
Leukotriene Modifiers
LTs are synthesized by the enzyme 5-lipoxygenase from arachidonic acid, which also produces prostaglandins (PGs). These LTs are produced by cells of inflammation and produce bronchoconstriction, increased mucus secretion, mucosal edema, and increased bronchial hyperreactivity. The LT pathway inhibitors block the effects of the release of LTs. They are used to manage patients with asthma that is not controlled by β2-agonists and corticosteroid inhalers.
Zileuton (Zyflo) is a 5-lipoxygenase inhibitor that works by preventing the synthesis of the LTs. Zafirlukast (Accolate) and montelukast (Singulair) are LT receptor antagonists (LTRA). They are not as effective as the corticosteroid inhalers. Both are effective when taken orally. Some patients respond better than others, but who will respond cannot be predicted.
The adverse reactions of these agents include irritation of the stomach mucosa, headache, and alteration of liver function tests. Zafirlukast has a drug interaction with erythromycin and aspirin. Zafirlukast increases the effect of warfarin. Caution should be exercised when giving to patients taking drugs metabolized by 2C9 (tolbutamide, phenytoin, and carbamazepine) or 3A3/4 (dihydropyridines, cyclosporin, astemizole, and cisapride) cytochrome P-450 enzymes. Erythromycin lowers the level of zafirlukast by about 40%. Aspirin raises zafirlukast levels by about 50%. Zafirlukast has recently been found to increase the level of theophylline in the blood. This may be explained by the fact that zafirlukast is an inhibitor of cytochrome P-450 3A3/4 isoenzymes and is a substrate for cytochrome P-450 isoenzyme 2C9. Both zafirlukast and zileuton have been reported to cause life-threatening hepatic injury. Alanine aminotransferase levels need to be monitored, and patients should discontinue the drug immediately if abdominal pain, nausea, jaundice, itching, or lethargy occurs. Also, there have been reports of mood changes in patients taking montelukast.
CROMOLYN
An agent that is effective only for the prophylaxis of asthma and not for treatment of an acute attack is cromolyn (KROE-moe-lin) (Intal, Nasalcrom). It has no intrinsic bronchodilator, antihistaminic, or antiinflammatory action. Cromolyn prevents the antigen-induced release of histamine, LTs, and other substances from sensitized mast cells. It appears to do this by preventing the influx of calcium provoked by immunoglobulin E (IgE) antibody-antigen interaction on the mast cell. This effect accounts for the group name that these drugs have been given: mast cell degranulation inhibitors. Cromolyn is the least toxic of all asthma medications. It is currently available in a metered-dose form like the other inhalation agents. Nedocromil (Tilade) is similar in action to cromolyn.
The advantage of cromolyn is its safety. It may be used prophylactically by patients with chronic asthma or taken before exercise-induced asthma. Intranasal cromolyn (Nasalcrom) is available over-the-counter (OTC) for allergic rhinitis.
Methylxanthines
The xanthines and methylxanthines consist of theophylline (thee-OFF-i-leen) (Theo-Dur, Slo-Bid), caffeine, and theobromine. Theophylline, used as a bronchodilator, can be combined with ethylenediamine to produce aminophylline (am-in-OFF-i-leen), which is more soluble. Theophylline is used to treat persistent asthma and the bronchospasm associated with chronic bronchitis and emphysema. Bronchodilation is the major therapeutic effect desired.
Side effects associated with the methylxanthines include central nervous system (CNS) stimulation, cardiac stimulation, increased gastric secretion, and diuresis. Patients often complain of nervousness and insomnia. Erythromycin can increase the serum levels of theophylline, and toxicity may result.
Intravenous aminophylline and rapidly absorbed oral liquid preparations are used to manage acute asthmatic attacks and status asthmaticus. To manage persistent asthma, sustained-release preparations in tablet or capsule form are used. Patients on chronic theophylline may have blood levels drawn to determine if the dose they are taking is appropriate. Current literature suggests that the use of theophylline should be limited to patients whose asthma is not controlled with other agents. When the chance of theophylline toxicity is weighed against the potential therapeutic benefit, theophylline is often omitted from an asthmatic’s therapeutic regimen.
Anticholinergics
Inhaled anticholinergic drugs appear to inhibit vagally mediated reflexes by antagonizing the action of acetylcholine. This then causes bronchodilation. Ipratropium (i-pra-TROE-pee-um) bromide (Atrovent) is a short-acting anticholinergic available for oral inhalation for people with COPD. Tiotropium bromide (Spiriva) is an inhaled long-acting anticholinergic drug used to treat COPD. Side effects, including dry mouth and bad taste, are minimized with administration by inhalation. Both drugs have a cross-hyperreactivity with peanut and soybean allergies. Ipratropium bromide’s bronchodilating effect is additive with that of the β-agonists. It is available as in combination with albuterol sulfate (Combivent) and is used in patients with COPD on a regular aerosol inhalation bronchodilator who continue to have evidence of bronchospasm. Neither ipratropium bromide nor tiotropium bromide are approved by the Food and Drug Administration (FDA) for treating asthma.
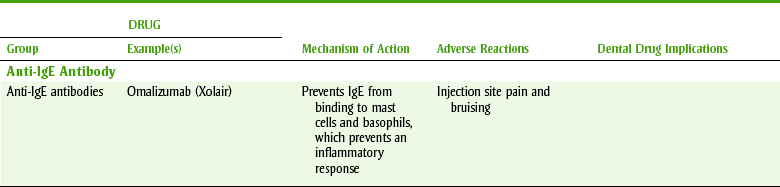
Anti-Immunoglobulin E Antibodies
Omalizumab (Xolair) is the first in a new class of medications introduced to treat asthma due to allergens. It is a recombinant humanized monoclonal antibody that prevents IgE from binding to mast cells and basophils, thereby preventing the release of inflammatory mediators after allergen exposure (see Table 22-1 and Figure 22-3). This drug is FDA-approved for adjunctive use in patients at least 12 years of age, with well-documented specific allergies and moderate-to-severe persistent asthma that is not well-controlled on an inhaled corticosteroid with or without a long-acting β2-agonist. Omalizumab is administered as a subcutaneous injection every 2 to 4 weeks. It is expensive. Adverse effects include injection site pain and bruising. Anaphylaxis can occur within 2 hours of injection but sometimes 4 days later. It is advised that patients be kept under observation for 2 hours after the first 3 injections and for 30 minutes after subsequent injections. Patients are educated about the signs and symptoms of anaphylaxis and when to self-administer injectable epinephrine.
Agents Used to Manage Upper Respiratory Infections
Nasal decongestants are β-adrenergic agonists that act by constricting the blood vessels of the nasal mucous membranes (α effect). Some examples of these include pseudoephedrine (soo-doe-e-FED-rin) (Sudafed, Sucrets, in Actifed) and phenylephrine (fen-ill-EF-rin) (Neo-Synephrine, Sinex, Allerest). Many nasal decongestants are available OTC for both local and systemic use (see also Table 4-5). Chronic topical use of decongestants may result in rebound swelling and congestion. Therefore decongestant nose sprays should not be used for more than a few days. Unwanted side effects of adrenergic stimulation may occur. Phenylephrine (Neo-Synephrine) is used topically as a nasal spray, and phenylpropanolamine is used systemically as a decongestant (α-agonist action). Pseudoephedrine, both an α-adrenergic agonist and a β-adrenergic agonist, is used systemically as a nasal decongestant.
EXPECTORANTS AND MUCOLYTICS
Expectorants are drugs that promote the removal of exudate or mucus from the respiratory passages. Liquefying expectorants are drugs that promote the ejection of mucus by decreasing its viscosity. Mucolytics destroy or dissolve mucus.
Some expectorants act by their ability to cause reflex stimulation of the vagus, which increases bronchial secretions. Guaifenesin (gwye-FEN-e-sin), the most popular expectorant, is contained in a variety of OTC products mixed with other active ingredients. Robitussin is available as guaifenesin alone (Robitussin plain) and mixed with an antitussive agent (Robitussin DM).
Mucolytics are enzymes that are able to digest mucus, decreasing its viscosity. Acetylcysteine (Mucomyst) is a mucolytic used to loosen secretions in pulmonary diseases, including cystic fibrosis. It is also used orally as an antidote for acetaminophen toxicity.
ANTITUSSIVES
Antitussives may be opioids or related agents used for the symptomatic relief of nonproductive cough. Opioids are the most effective, but because of their addicting properties, other agents are often used. Codeine-containing cough preparations are commonly used, but their histamine-releasing properties may precipitate bronchospasm.
Dextromethorphan (dex-troe-meth-OR-fan) (the DM in cough medicines such as Robitussin DM), an opioid-like compound, suppresses the cough reflex by its direct effect on the cough center. It does not cause the release of histamine. It may potentiate the effects of CNS depressants. It is available both alone and in combination with other ingredients. By impairing coughing, dextromethorphan may not allow the secretions to be cleared from the lungs.
Dental Implications of the Respiratory Drugs
About 10% of the population has some pulmonary disease, so patients taking medications for asthma, emphysema, or chronic bronchitis are often encountered. With severe COPD, a patient can develop pulmonary hypertension, increasing the risk for cardiac arrhythmias. Stress should be minimized and adrenal supplementation instituted if the patients are taking certain doses of steroids and the procedure is likely to produce severe stress. Patients prone to developing respiratory failure, if given oxygen (either alone or with nitrous oxide) or CNS depressants, may manifest acute respiratory failure. Aspirin should be avoided in patients with asthma, and erythromycin may alter the metabolism of theophylline (Box 22-1). Emergency equipment and medications should be available when treating these patients (see Table 23-1 and Box 23-3).
GASTROINTESTINAL DRUGS
Many drugs, both OTC and on prescription, are used for gastrointestinal diseases. Some are used to treat specific gastrointestinal diseases, and others are used to provide symptomatic relief.
Gastrointestinal Diseases
Ulcers and gastroesophageal reflux disease are common gastrointestinal tract diseases. With the discovery of the etiology of ulcers, the incidence of ulcers in the population has decreased substantially. Nonspecific complaints of gastroesophageal reflux disease (GERD) include burping, cramps, flatulence, fullness, and congestion in the stomach. The gastrointestinal tract is highly susceptible to emotional changes because it is innervated by the vagus nerve associated with the autonomic nervous system.
GASTROESOPHAGEAL REFLUX DISEASE
GERD, or “heartburn,” is the most prevalent gastrointestinal disease in the U.S. population. In this condition, the stomach contents, including the acid, reflux, or flow backward through the cardiac sphincter, up into the esophagus. Because the esophagus is not designed to endure the stomach’s acid, irritation, inflammation, and erosion can occur. The pain from the inflamed esophagus may be severe and located in the middle of the chest, causing it to be interpreted as a heart attack and trigger an emergency room visit. The main problem is the lack of adequate function of the cardiac sphincter, allowing backflow to occur. The symptoms of GERD are exacerbated by eating large meals (blowing up a balloon [stomach] increases the back pressure) and by assuming the supine position (gravity no longer helping).
Lifestyle changes that can reduce symptoms include avoiding eating for 4 hours before bedtime, eating smaller meals more often, and raising the head of the bed with bricks or using several pillows. If untreated, some patients may have such severe symptoms that they cannot sleep lying down and must sit in a chair.
GERD is treated in two ways: one is to decrease the acid in the stomach and the other is to constrict the cardiac sphincter (the muscle between the stomach and the esophagus). If the sphincter is tighter, it is less likely that the contents will flow back into the esophagus. The H2-blockers and the proton pump inhibitors (PPIs) reduce or eliminate the stomach’s acid. The gastrointestinal stimulants act by increasing the tone in the cardiac sphincter. Sometimes both of these approaches are required to make the patient asymptomatic. Antacids are used for acute relief of symptoms.
ULCERS
Ulcers may occur in the stomach or small intestine. In the past, it was thought that ulcers were caused by “too much acid.” However, in the last decade it has been determined that most ulcers are related in some way to the presence of the organism Helicobacter pylori. Many ulcers can now be cured by using a combination of one or more antibiotics and an H2-blocker or a PPI to reduce the acid in the stomach. Some ulcers, especially in the elderly, are secondary to the chronic use of the nonsteroidal antiinflammatory drugs (NSAIDs). NSAID-induced ulcers occur because NSAIDs inhibit synthesis of PGs, which are cytoprotective to the stomach.
Dental Implications
Box 22-2 summarizes the treatment of dental patients with peptic ulcer disease (PUD) and GERD.
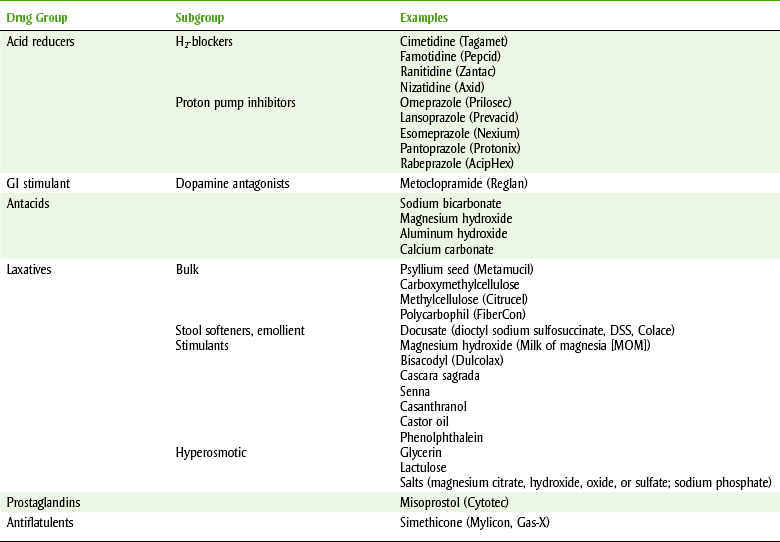
DRUGS USED TO TREAT GASTROINTESTINAL DISEASES
Histamine2 (H2)-receptor antagonists block and inhibit basal and nocturnal gastric acid secretion by competitive inhibition of the action of histamine at the H2-receptors of the parietal cells. They also inhibit gastric acid secretion stimulated by other agents such as food and caffeine. All the members of this group, which are now available OTC, are listed in Table 22-2. Cimetidine (sye-MET-i-deen) (Tagamet) is discussed as the prototype. However, it has largely been replaced by famotidine, ranitidine, and nizatidine because of their more tolerable side effect profiles.
USES
This group is indicated for the treatment of ulcers and the management of the symptoms of ulcers and GERD. Combining H2-blockers with antacids has no therapeutic advantage; in fact, antacids inhibit their absorption and should not be administered within 1 hour of H2-blockers. H2-blockers should be administered with meals and at bedtime. For maintenance, if only one dose is needed daily, the bedtime dose is most effective.
Because smoking increases acid production and reduces the effect of the H2-blockers, smoking cessation assistance should be offered to dental patients who smoke. Cimetidine blocks H2-receptors, which in part are responsible for the inflammatory response in the cutaneous blood vessels of humans.
ADVERSE REACTIONS
The side effects of cimetidine include CNS effects such as slurred speech, delusions, confusion, and headache. Because cimetidine binds with the androgen receptors, it produces antiandrogenic effects such as gynecomastia, reduction in sperm count, and sexual dysfunction (e.g., impotence). Unlike cimetidine, neither ranitidine nor famotidine has been found to possess antiandrogenic activity. Famotidine has been associated with dry mouth and taste alterations. Cimetidine’s hematologic effects include granulocytopenia, thrombocytopenia, and neutropenia. Reversible hepatitis and abnormal liver function tests have been reported with all of the H2-blockers.
Cimetidine inhibits liver microsomal enzymes responsible for the hepatic metabolism of some drugs (cytochrome P-450 oxidase system), resulting in a delay in elimination and an increase in serum levels of some drugs, possibly producing toxicity. Ranitidine inhibits the P-450 enzymes much less than does cimetidine, and the other H2-blockers have no effect on the P-450 enzymes. A few examples of drugs that are metabolized by the P-450 pathway include warfarin, metronidazole, lidocaine, phenytoin, theophylline, diazepam, and carbamazepine.
DENTAL DRUG INTERACTIONS
The metabolism of the following drugs occasionally used in dentistry may be reduced by the administration of cimetidine:
• Ketoconazole and itraconazole: Toxic levels of these antifungal agents may be produced if they are used continuously for the management of chronic fungal infections. H2-receptor antagonists may increase gastrointestinal pH. Concurrent administration with H2-receptor antagonists may result in a marked reduction in absorption of itraconazole or ketoconazole. Patients taking itraconazole or ketoconazole should take H2-receptor antagonists at a different time.
• Alcohol: The blood alcohol levels of persons who have ingested alcoholic beverages may be higher if the patient has been taking cimetidine.
• Benzodiazepines: The metabolism of the benzodiazepines, such as diazepam and midazolam, may be slower. The recovery from use of these drugs might be slower.
The other H2-blockers are unlikely to produce important dental drug interactions.
Proton Pump Inhibitors
Proton pump inhibitors (PPIs) are potent inhibitors of gastric acid secretion that are effective (in combination with the antibiotics) in healing duodenal ulcers, and as monotherapy for the acute treatment and maintenance therapy of GERD. The mechanism of action involves the inhibition of the hydrogen/potassium adenosine triphosphatase (H+/K+ ATPase) enzyme system at the surface of the gastric parietal cell. Currently available PPIs are listed in Table 22-2. PPIs heal ulcers more rapidly than H2-receptor blockers or any other drug. Tolerance does not occur with PPIs because the increased gastric-mediated histamine release cannot overcome proton pump blockade.
Side effects include headache and abdominal pain. In rats, omeprazole produced an increase in gastric carcinoid tumors, but it has now been determined that this is unlikely to occur with use in humans. Therefore the original limit on the duration of use of omeprazole has been lifted. Although it is unknown whether a relationship exists between omeprazole and mucosal atrophy of the tongue and dry mouth, these side effects have been reported. Long-term use of PPIs, particularly at high doses, has been associated with an increased risk of osteoporotic fractures.
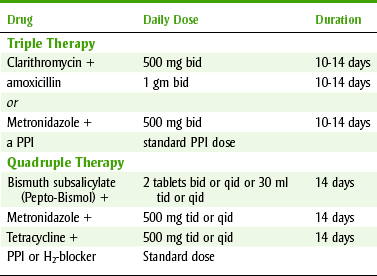
Mixed Antiinfective Therapy for Ulcer Treatment
Ulcers are closely related to the organism H. pylori. To treat ulcers, a combination of two antiinfective agents (tetracycline, metronidazole, clarithromycin, or amoxicillin), an H2-blocker or a PPI, and bismuth subsalicylate (Pepto-Bismol) may be used. Common multidrug regimens are listed in Table 22-3. Newer combinations often use one antibiotic and a PPI such as esomeprazole and clarithromycin. These agents are used for 2 weeks and result in a cure in many patients.
Antacids
Antacids are used to treat a variety of gastric conditions, by both self-medication and recommendation of the patient’s prescriber. Acute gastritis and symptoms of ulcers are sometimes managed with antacids. Acute gastritis, the most common type of gastric distress, is termed heartburn or upset stomach. The symptoms include epigastric discomfort or a burning feeling. The symptoms of gastric ulcers can be managed with antacids.
Antacids are drugs that partially neutralize hydrochloric acid in the stomach. By raising the pH to 3 or 4, the erosive effect of the acid is decreased and pepsin activity is reduced (see Table 22-2).
Sodium bicarbonate rapidly neutralizes gastric acid. Its major disadvantage is that alkalosis can occur. It also contains sodium and is contraindicated in cardiovascular patients who are to minimize sodium intake. For these reasons, it is not recommended, although it is still used by the lay public.
Calcium carbonate, aluminum and magnesium salts, and magnesium-aluminum hydroxide gels are the active ingredients in all other antacids. Calcium salts may result in acid rebound, constipation, or hypercalcemia. Aluminum salts can produce constipation. Magnesium salts produce osmotic diarrhea. Hypermagnesemia has been reported in patients with renal disease. Drug interactions with the antacids include altering the absorption of other drugs from the gastrointestinal tract. Drugs whose absorption is inhibited include tetracyclines, digitalis, iron, chlorpromazine, and indomethacin. Conversely, levodopa’s absorption is increased because stomach emptying time is shortened. By mixing aluminum and magnesium salts in a single preparation, the effects on the bowel can be balanced.
Miscellaneous Gastrointestinal Drugs
Misoprostol (mye-soe-PROST-ole) (Cytotec) is PGE2α and is indicated in the management of NSAID-induced ulcers. Both H2-blockers and PPIs reduce the symptoms of NSAID-induced ulcers but do not prevent the ulcers. Misoprostol increases gastric mucus and inhibits gastric acid secretion. Its side effects include stomach distress and diarrhea (caused by PGs). Its FDA pregnancy category is X because it stimulates uterine contractions and will induce labor.
SUCRALFATE
Sucralfate (soo-KRAL-fate) (Carafate), a complex of aluminum hydroxide and sulfated sucrose (a polysaccharide with antipeptic activity), is used to treat duodenal ulcers. In the stomach, the aluminum ion splits off, leaving an anion that is essentially nonabsorbable. Sucralfate combines with proteins, forming a complex that binds preferentially with the ulcer site. It can be thought of as a “bandage” for ulcers. It inhibits the action of pepsin and absorbs the bile salts. Its acid-neutralizing capacity does not contribute to its antiulcer action. Constipation is the most frequent side effect reported (2.2%). Other side effects (<0.3%) include dry mouth, nausea, rash, and dizziness. It must be taken on an empty stomach and can inhibit the absorption of tetracycline.
METOCLOPRAMIDE
The drug metoclopramide (met-oh-KLOE-pra-mide) (Reglan) is a dopaminergic antagonist. It blocks the action of dopamine and that action facilitates cholinergic effects within the gastrointestinal tract. Metoclopramide stimulates the motility of the upper gastrointestinal tract without stimulating secretions and relaxes smooth muscle innervated by dopamine. It relaxes the pyloric sphincter and increases peristalsis in the duodenum. This results in an accelerated gastric emptying time. It also increases the tone of the lower esophageal sphincter. Its antiemetic property is the result of its antagonism of dopamine receptors both centrally and peripherally.
Metoclopramide is indicated for the relief of symptoms associated with diabetic gastroparesis (gastric stasis) and improves delayed gastric emptying time. Another indication is short-term therapy for gastroesophageal reflux with symptoms. The most common CNS side effects are restlessness, drowsiness, and fatigue, and these occur in 10% to 25% of patients. Parkinson-like reactions can occur in up to 10% of patients. Gastrointestinal side effects include nausea and diarrhea. Additive CNS depression may occur when other CNS depressants are used concomitantly.
Laxatives and Antidiarrheals
Self-medication with laxatives is a common practice among the lay public. Although a few indications for the use of laxatives exist, overuse is common and habituation can result. The myth that “regular” bowel habits are essential has led to this practice. Abuse of these substances occurs in bulimic patients. Short-term, occasional use for constipation and use before diagnostic procedures (barium enema) are legitimate indications. The types of laxatives (Table 22-4) are as follows:
• Bulk laxatives: Bulk laxatives are preferred because they are the safest and act most like the normal physiology of humans. They contain polysaccharides or cellulose derivatives that combine with intestinal fluids to form gels. This increases peristalsis and facilitates movement through the intestine. Patients with problems with constipation can increase their intake of fiber or use any bulk laxative daily without problems.
• Lubricants: Mineral oil, a lubricant that was previously often used, is no longer recommended. It can be absorbed if used over a long period and can interfere with the absorption of the fat-soluble vitamins (A, D, E, and K).
• Stimulants: Stimulant laxatives act by producing local irritation of the intestinal mucosa. Because of their potent effect, intestinal cramping can result. Bisacodyl, a member of this group, is often used before bowel surgery or radiologic examinations but should not be used for simple constipation.
• Stool softeners (emollients): Dioctyl sodium sulfosuccinate, an anionic detergent, wets and softens the stool by accumulating water in the intestine. These agents should be limited to short-term use, although they are nontoxic.
• Osmotic (saline) laxatives: Magnesium sulfate or phosphate produces its laxative effect by osmotically holding water. It should be used with caution in patients with renal impairment.
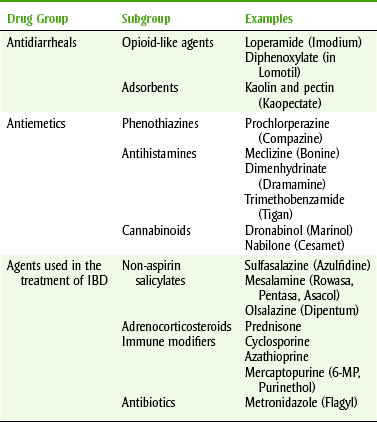
ANTIDIARRHEALS
Drugs used to treat diarrhea are either adsorbents or opioid-like in action. Antidiarrheals are used to minimize fluid and electrolyte imbalances. In certain poisonings or infections, antidiarrheals are contraindicated. The most common adsorbent combination used to treat diarrhea is kaolin and pectin (Kaopectate). The opioids, such as diphenoxylate with atropine (Lomotil) and loperamide (OTC Imodium), are the most effective antidiarrheal agents. They decrease peristalsis by acting directly on the smooth muscle of the gastrointestinal tract.
Antiemetics
Drugs used to induce vomiting and to prevent vomiting are used for certain gastrointestinal tract problems. Vomiting may occur because of a variety of situations such as motion sickness, pregnancy, drugs, infections, or radiation therapy, and many sites within the body can activate the emetic center to produce vomiting (Figure 22-6). Choice of the drug to treat vomiting depends to some extent on the cause of the vomiting.
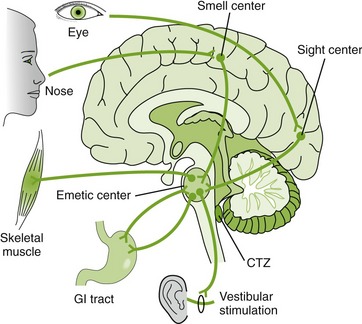
FIGURE 22-6 The chemoreceptor trigger zone (CTZ) and other sites that activate the emetic center. (From McKenry L, Tessier E, Hogan MA: Mosby’s pharmacology in nursing, ed 22, St Louis, 2006, Mosby.)
PHENOTHIAZINES
Phenothiazines (e.g., prochlorperazine [Compazine]) are used to control severe nausea. Their side effects include sedation and extrapyramidal symptoms, including tardive dyskinesia (see Chapter 17). Promethazine (Phenergan), a phenothiazine with antihistaminic and anticholinergic properties, is used in dentistry to treat nausea and vomiting associated with surgery and anesthesia. It also has sedative and antisialagogue action. It is sometimes used concurrently with opioids to minimize the nausea they produce.
ANTICHOLINERGICS
Anticholinergics can be used for the nausea and the vomiting associated with motion sickness and labyrinthitis. Both dimenhydrinate (Dramamine) and meclizine (Bonine) possess antiemetic, antivertigo, and antimotion sickness action. Because they have antihistaminic action, sedation is a side effect. A scopolamine transdermal patch (Transderm-Scop) is placed behind the ear and releases medication over a 3-day period. It is used for motion sickness on ships and boats. It is contraindicated whenever anticholinergics are used (see Chapter 4). Dry mouth, blurred vision, sedation, and dizziness have been reported.
ANTIHISTAMINES
The agent diphenhydramine (Benadryl), an antihistamine with antiemetic properties, commonly produces sedation. Hydroxyzine (Atarax) is used in dentistry as an antiemetic or antianxiety agent.
TRIMETHOBENZAMIDE
The drug trimethobenzamide (Tigan) has an antiemetic effect that is mediated through the chemoreceptor trigger zone. It produces sedation, agitation, headache, and dry mouth. It is available orally or as a suppository that contains 2% benzocaine (avoid in patients allergic to ester local anesthetics).
METOCLOPRAMIDE
Metoclopramide (Reglan) can control the nausea and vomiting of patients receiving cancer chemotherapeutic agents. It acts both centrally (dopamine antagonist) and peripherally (stimulates release of acetylcholine). It is also indicated for the management of gastric motility disorders such as diabetic gastric stasis.
CANNABINOIDS
Dronabinol (droe-NAB-i-nol) (Marinol) and nabilone (NAB-i-lone) (Cesamet) are psychoactive substances derived from Cannabis sativa L. (marijuana). They produce effects similar to those of marijuana. These agents are indicated to treat the nausea and vomiting associated with cancer chemotherapy in patients who have failed to respond to conventional antiemetic therapy. These agents can be abused. Tolerance and both physical and psychologic dependence can occur. Close supervision is required when these agents are administered. Side effects include drowsiness and dizziness. Perceptual difficulties, muddled thinking, and elevation of mood can also occur.
Agents Used to Manage Chronic Inflammatory Bowel Disease
Chronic inflammatory bowel disease (IBD) is divided into two subcategories: ulcerative colitis and Crohn’s disease (Figure 22-7). Although probably multifactorial, an autoimmune response is thought to be associated with ulcerative colitis. Crohn’s disease extends through all layers of the intestinal wall, whereas ulcerative colitis involves only the mucosa. Crohn’s disease can involve the whole intestine, but the colon is most commonly affected. Ulcerative colitis involves the rectum and may involve the distal part of the colon but does not involve the small intestine. Smoking is protective against ulcerative colitis, and smoking cessation may exacerbate the disease. NSAIDs should be used with caution in patients with IBD.
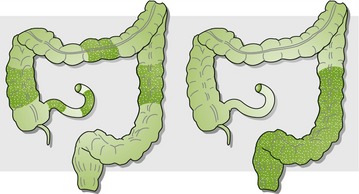
FIGURE 22-7 Crohn’s disease (left) and ulcerative colitis (right). (Modified from Cotran KS, Kumar V, Robbins SI: Robbins and Cotran pathologic basis of disease, ed 7, Philadelphia, 2005, Saunders.)
The drugs used to treat IBD include laxatives, colonic stimulants, and osmotic agents and are indicated for patients that do not respond to fiber supplementation. Loperamide (Imodium) and atropine/diphenoxylate (Lomotil) are antidiarrheal agents that are also used to treat IBD in patients with diarrhea-predominant irritable bowel syndrome (IBS). Antispasmodics, such as hyoscyamine and dicyclomine, are best used on an as-needed basis for acute attacks of abdominal pain or before meals in patients with postprandial symptoms. The newer agents, tegaserod (Zelnorm) and alosetron (Lotronex), are serotonin 5-hydroxytryptamine modulators. They play a major role in the regulation of intestinal motility, secretion, and visceral sensitivity. Tricyclic antidepressants are used when diarrhea-persistent IBS is moderate to severe. These drugs modulate the perception of visceral pain, alter gastrointestinal transit, and treat psychiatric comorbidities.
Infliximab (Remicade) is the newest agent approved by the FDA to treat ulcerative colitis. It works by neutralizing tumor necrosis factor (TNF). Infliximab finds TNF in the bloodstream and removes it before it causes inflammation in the gastrointestinal tract. The drug has been linked to an increased risk of infection, especially tuberculosis, and may increase the risk of blood problems and cancer. Once started, infliximab is often continued as long-term therapy, although its effectiveness may wear off over time.
CLINICAL SKILLS ASSESSMENT
1. What are some of the risk factors of GERD?
2. What is the role of antacids, H2-receptor antagonists, and PPIs in the treatment of GERD?
3. What are the dental concerns associated with the medications used to treat GERD?
4. Compare and contrast the different antacids.
5. What is the role of sucralfate in the treatment of PUD?
6. What are some common adverse effects of antidiarrheals, antiemetics, and laxatives?
7. Discuss different methods of minimizing an asthma attack in the dental office.
8. What is the role of steroids in the treatment of asthma?
9. Why are oral, inhaled steroids the preferred dose form in the treatment of asthma?
10. What is the role of β2-adrenergic agonists in the treatment of asthma?
11. What are the dental concerns associated with β2-adrenergic agonists? What would the dental practitioner tell a patient about them?
 Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.
Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.