Funding Assistive Technology Services and Systems
U.S. Public Sources of Assistive Technology Funding
Programs for the Developmentally Disabled
Plan for Achieving Self-Sufficiency
Department of Veterans Affairs
Canadian Provincial and Territorial Sources of Assistive Technology Funding
Canadian Federal Sources of Assistive Technology Funding
Health Canada—First Nations and Inuit Health: Uninsured Health Benefits
Opportunities Fund for Persons With Disabilities
Australian State Government Funding Schemes
Australian Commonwealth Funded Schemes for the Older Person
Australian Department of Veterans’ Affairs—Rehabilitation Appliances Program
Australian Motor Vehicle Compulsory Third Party Personal Injury Insurance
Australian Government Education Departments
FUNDING PROCESS AND GUIDELINES FOR PROCURING FUNDING
IDENTIFYING THE FUNDING SOURCE
JUSTIFYING FUNDING FOR ASSISTIVE TECHNOLOGY SERVICES AND DEVICES
BILLING AND CODING FOR SERVICES
APPENDIX 5-1: SAMPLE FORMS FOR DOCUMENTING CONSUMERS’ EQUIPMENT NEEDS
On completing this chapter, you will be able to do the following:
1 Identify the major categories of funding for assistive technology services and equipment
2 Describe the types of assistive technology devices and services covered by each category of funding
3 Distinguish between categories of funding as they relate to specific consumer characteristics
4 Describe the process for procuring funding
5 Describe the process by which funding decisions can be appealed
As discussed in Chapter 1, there is an established assistive technology industry that provides services and devices for individuals with disabilities. Evaluation, implementation, and maintenance and repair of assistive technologies can be costly, and most consumers do not have the financial resources available to purchase the necessary services and equipment. Therefore, funding by third-party sources is necessary for individuals to procure assistive technology services and equipment. Fortunately, funding for many assistive technology services and devices is widely available, and accessing that funding is generally a matter of following a straightforward process. Assisting with the acquisition of this funding is an inherent part of the assistive technology practitioner’s (ATP) role as a service provider.
In most countries assistive technology services and devices are funded by numerous sources rather than by a system solely dedicated to the funding of assistive technology services and equipment. For any given individual, equipment and services may be funded solely from one source or through a combination of sources. Funding for assistive technology is usually rendered through agencies that have been primarily developed for the provision of other types of health, education, or social services programs.
In this chapter funding for assistive technologies in several countries (United States, Australia, and Canada) is described. Funding programs in these countries are representative of those in many other countries with local modifications of elements of the programs. The various funding sources can be categorized as three general types: public, private, and other.
PUBLIC SOURCES OF FUNDING
U.S. Public Sources of Assistive Technology Funding
Public funding sources for assistive technology funding in the United States include federal, state, and local government agencies; several public sources of funding are listed in Box 5-1. There are more than 30 programs established by the U.S. Congress that affect U.S. residents with disabilities and more than 12 agencies on the federal level that oversee these programs (Morris and Golinker, 1991). Typically, Congress authorizes funding through a specific piece of legislation, such as the Medicare Act, and designates a federal agency to determine the scope and criteria for the program. Other programs are examples of a principle called “cooperative federalism.” For them, Congress passes a law that is broadly administered by a federal government agency but administered on a day-to-day basis by the states. These programs also will be jointly funded by the federal and state governments. Medicaid and vocational rehabilitation are examples of cooperative federalism programs. A third model extends the federal presence to local levels of government where day-to-day decision making occurs. The Individuals With Disabilities Education Act (IDEA), which sets standards for the education of children with disabilities by local schools, is an example of this type of program.
Medicare.
Medicare is the health insurance program operated by the federal government. Coverage, benefits, and program operation for this program are described in Chapter 1. Medicare funds durable medical equipment (see Chapter 1 for definition). Some assistive technology equipment, such as speech-generating devices, the full range of mobility aids and accessories, hospital beds, and patient lifts, are covered under Part B as durable medical equipment.
Medicaid.
Medicaid is a public welfare program whose coverage, benefits, and program operation are described in Chapter 1. Assistive technology services and devices are within the scope of each state’s Medicaid program (Golinker and Mistrett, 1997). The federal definitions of the intent and scope of mandated and optional services should be used as a starting point to determine the basis of Medicaid funding for assistive technology. To receive federal funding for Medicaid, all states must comply with these definitions of services. Golinker and Mistrett (1997) identify 11 services among the list of mandatory and optional Medicaid services under which funding for assistive technology and services may qualify (see Box 1-3). These services are early and periodic screening, diagnostic treatment services; home health care services, prosthetic devices; occupational therapy; physical therapy; speech-language pathology; rehabilitative services; preventive services; skilled nursing facility; and services and intermediate care facility services for persons with mental retardation, developmental disabilities, and related conditions. Because assistive technology devices and services are not listed as such in the Medicaid vocabulary, it is recommended that use of these terms be avoided when applying for funding under Medicaid (Golinker and Mistrett, 1997). Instead, the device being requested should be identified by its specific name in all documentation and any descriptive terms used should match those in the definition of one of the Medicaid services listed above.
One of the general criteria for funding of all Medicaid services is that the requested equipment or service be considered a medical necessity. Another general criterion for funding of Medicaid services is that prior approval or authorization is required for nearly all services and equipment. Before commencing any services or purchasing any equipment for a Medicaid beneficiary, the ATP needs to request approval from Medicaid for the purchase of such services or devices. In some states a certain amount of occupational and physical therapy services may be provided without prior authorization. Because the ATP may not know whether this threshold has already been reached, it is generally safer from a reimbursement standpoint to get prior approval for the services to be provided.
Children’s Medical Services.
Medical and related services are provided to children under the age of 21 years who have chronic disabling conditions and who meet income limitations. These services are funded by the federal government under Title V of the Social Security Act. All children are eligible for medical diagnosis and evaluation. In some states, funding of assistive technologies is provided by Children’s Medical Services.
Programs for the Developmentally Disabled.
Within each state, programs for the developmentally disabled provide a range of services, including case management, advocacy, community living, and purchase of other services. Assistive technology services and equipment may be funded from these programs.
Tricare (formerly CHAMPUS).
The Tricare program, formerly known as the Civilian Health and Medical Program of the Uniformed Services (CHAMPUS), is a federally funded program that provides medical benefits to active duty military service members and their dependents and to military retirees and their dependents. Tricare contracts with various health insurance companies to administer this program, which provides medically necessary equipment and assistive technology services.
Education.
As discussed in Chapter 1, the Education for All Handicapped Children Act of 1975, the Handicapped Infant and Toddlers Act of 1986, and the 1991 reauthorization of these statutes through IDEA are vehicles through which assistive technology and related services can be provided to children with disabilities. Children from birth to 2 years of age must have an Individualized Family Service Plan (IFSP), and children 3 years to 21 years old must have a written Individual Education Plan (IEP) (see Chapter 1). Assistive technology must be considered in the development of the child’s IEP. If assistive technology is identified as being necessary for a “free and appropriate public education,” it must be included in the IEP and this service must be provided.
Vocational Rehabilitation.
The federal government provides states with funds to administer programs that help individuals with disabilities to enter, remain in, or return to employment. An Individual Plan for Employment (IPE, formerly called an Individual Written Rehabilitation Plan) that outlines the individual’s vocational objectives and services to be provided is required. Those who need assistive technology to complete training in a vocational rehabilitation program or to obtain or retain employment (competitive, supported, or sheltered) are eligible for funding of assistive technology equipment and services. Statutory amendments to this program create a strong presumption that an employment outcome always is possible, if the right services, including assistive technologies, are provided. For this reason, greater attention is expected to be directed to developing services plans and vocational outcomes for individuals with more severe disabilities. However, staff of vocational rehabilitation programs may not be aware of the benefits of assistive technology, and efforts by ATPs to provide continuing training can increase their awareness regarding assistive technology.
Plan for Achieving Self-Sufficiency.
The Plan for Achieving Self-Sufficiency (PASS) is a program that allows individuals to put aside income for equipment or services that will assist them in achieving a vocational objective. This includes assistive technology services and devices such as augmentative communication devices and adapted computer equipment. The Social Security Administration oversees this program and must approve the PASS before it can go into effect. The Social Security Administration excludes the money earned to pay for the devices from earned income, which allows the consumer to continue to receive applicable benefits. The consumer develops a written plan that identifies needs and feasible occupational goals, with a timetable for attaining these goals.
Department of Veterans Affairs.
The Department of Veterans Affairs (DVA), formerly the Veterans Administration (VA), directly provides assistive technology equipment and related services and contracts with outside programs to provide these services. Individuals who have a service-connected disability are eligible for purchase of assistive technologies by the VA.
Workers’ Compensation.
Expenses incurred as a result of work-related injuries are covered by Workers’ Compensation benefits. Under certain conditions, equipment, home modifications, and services are covered. Workers’ Compensation benefits are financed jointly by individual employers or groups of employers and state governments (Burton, 1996). A designated state agency or board develops the regulations for Workers’ Compensation and private insurance companies typically administer the program.
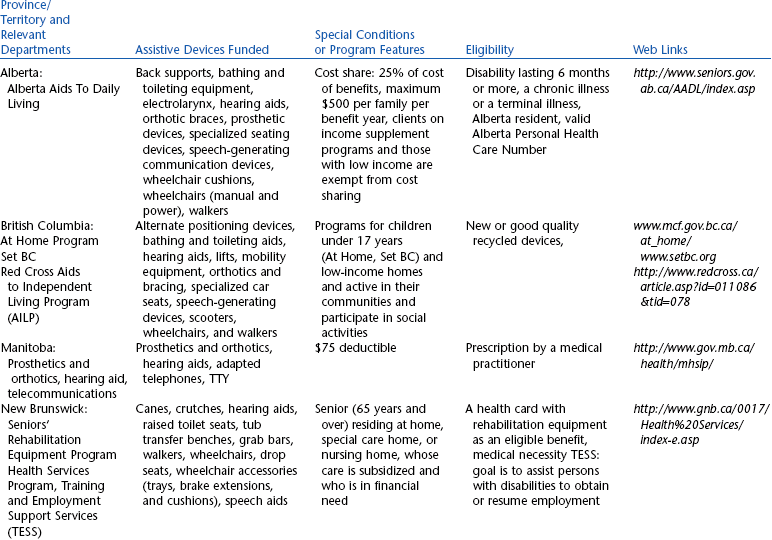
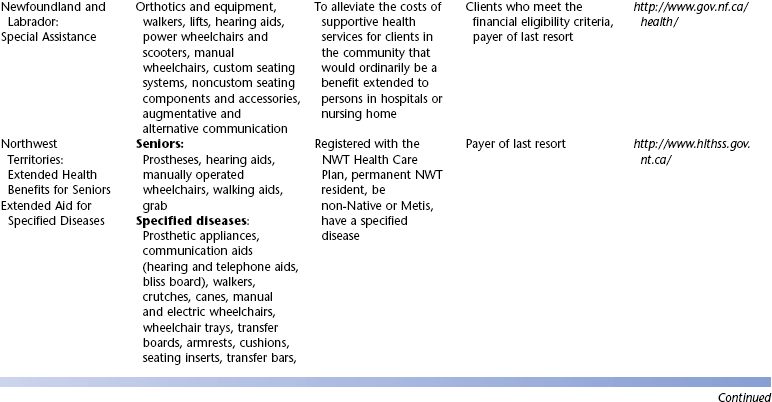
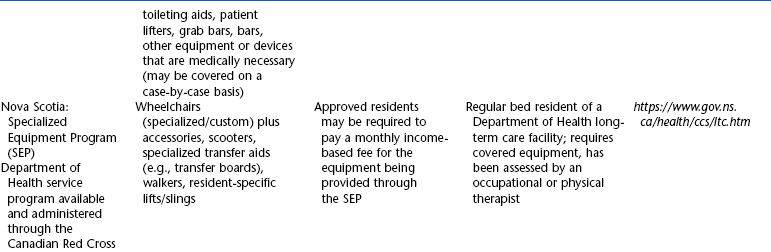
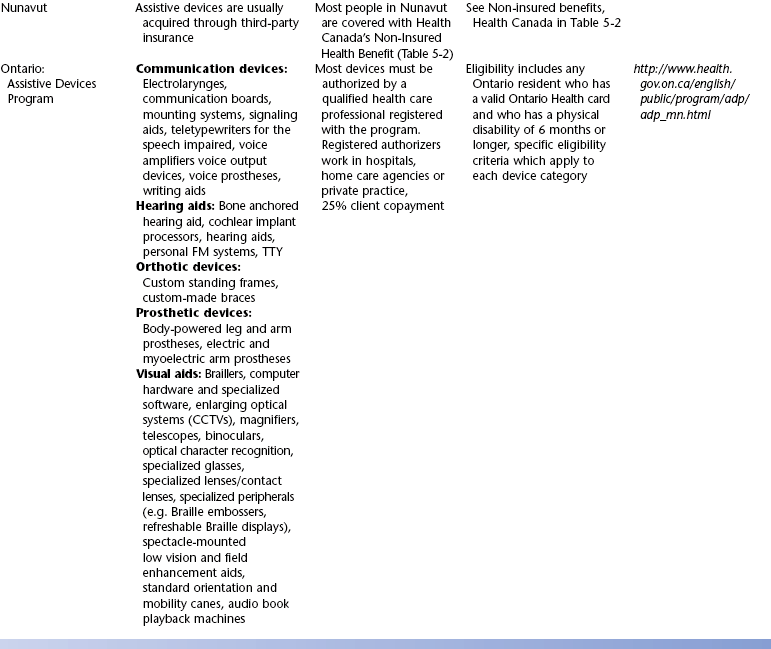
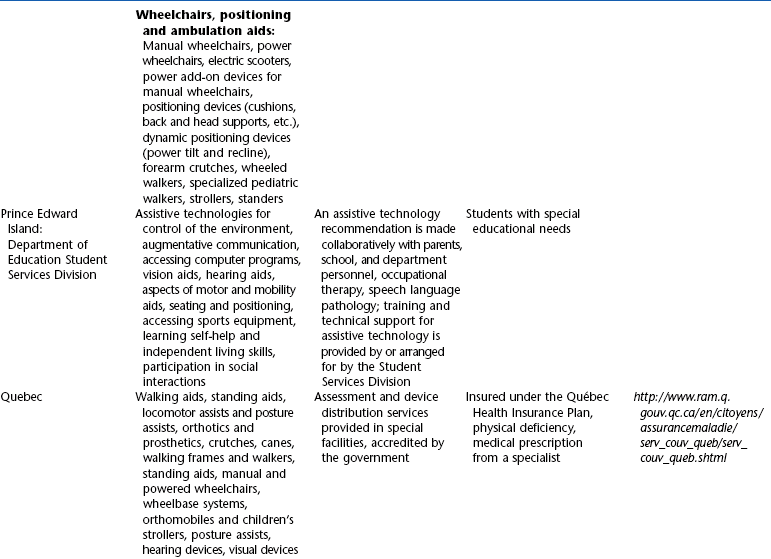
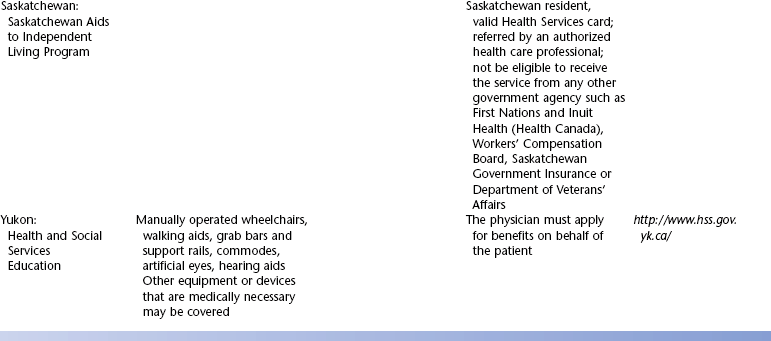
Canadian Provincial and Territorial Sources of Assistive Technology Funding*
In Canada the delivery of health services is the responsibility of the provinces and territories. Although there are federal programs, most assistive technology funding is allocated and managed at the provincial/territorial level. Most federal programs have clauses about funding only what the provinces and territories do not fund. Table 5-1 shows the breakdown of public funding sources for assistive technologies in Canada by jurisdiction. It is clear that there are major differences in programs across the country. In general, funding is provided for children through a children’s services ministry or an education ministry. For older adults, the major funding is for seniors in a social services department or, in some jurisdictions, a senior’s ministry. Table 5-1 lists the covered assistive technologies. This list is not complete in all cases because some jurisdictions list devices as examples and consider each request on the basis of medical necessity. Eligibility for funding is also listed in Table 5-1. Assistive technologies are generally funded only for conditions lasting 6 months or longer. In most cases an approved health provider must make a recommendation or generate a prescription for the appropriate assistive technology. Although this is often a medical doctor, many jurisdictions also accept recommendations from occupational therapists, physical therapists, or speech-language pathologists, depending on the type of technology being recommended. Some jurisdictions recycle assistive technologies. This only applies to technology that can be cleaned, reconditioned, and upgraded (e.g., with new software in an electronic system) to meet current levels of performance. Some communication devices, wheelchairs, and selected types of aids to daily living are routinely recycled. Customized seating systems, prosthetics and orthotics, and aids to daily living used for self-care and eating are not generally recycled.
Canadian Federal Sources of Assistive Technology Funding
Federal or national Canadian programs are listed in Table 5-2. These programs may have slightly different forms in each province.
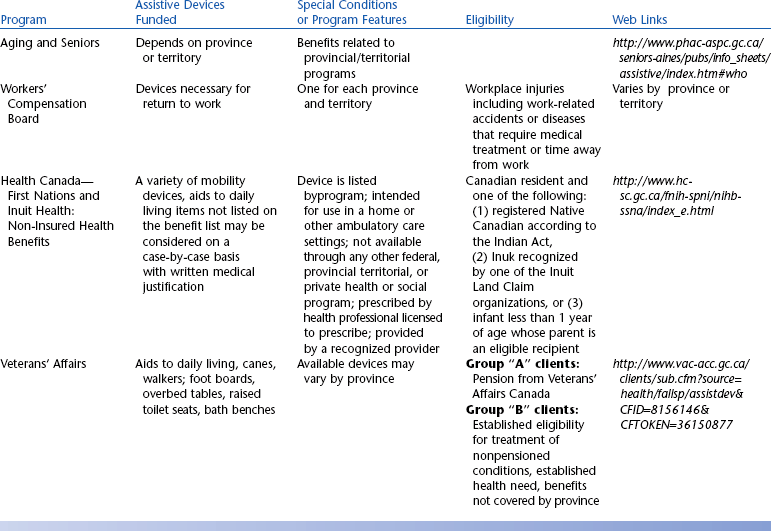
Health Canada—First Nations and Inuit Health: Uninsured Health Benefits.
The Federal Department of Health (Health Canada) provides funding to persons of Native Canadian descent for uninsured provincial or territorial items (http://www.hc-sc.gc.ca/fnih-spni/nihb-ssna/benefit-prestation/2004-2005_rpt_e.html). Under the Canada Health Act, provinces and territories are responsible for delivering health care services. First Nations and Inuit people access these insured services through provincial and territorial governments. There are a number of health-related goods and services, including assistive technologies, that are not insured by provinces and territories or other private insurance plans. Health Canada’s Non-Insured Health Benefits Program supports First Nations people and the Inuit in reaching an overall health status that is comparable to that of other Canadians by providing coverage for a limited range of these goods and services when individuals are not insured elsewhere. Assistive technology devices and services may be funded under this program on a case-by-case basis. A benefit will be considered for coverage when the conditions shown in Table 5-2 are met.
Veterans Independence Program.
The Veterans Independence Program is administered by the DVA. As shown in Table 5-2, this program is available to all veterans who require it for their pensioned conditions, wartime pensioners who are seriously or medium disabled, pensioners with multiple health conditions, war veterans with low income, former prisoners of war, and overseas service veterans waiting for a priority access bed. The program covers the provision of wheelchairs, some activities of daily living (ADL), and other self-care equipment.
Opportunities Fund for Persons With Disabilities.
The Opportunities Fund for Persons With Disabilities has a primary objective of assisting persons with disabilities to prepare for and obtain employment or self-employment and to develop the skills necessary to maintain that new employment. The program works with employers to assist them in making their work setting accessible to persons with disabilities and with individuals to prepare them for work or for starting their own businesses. The program also partners with private sector organizations to develop programs that enhance employability for persons with disabilities. Among the benefits listed are expenses related to university tuition, equipment, transportation, and living expenses while in training.
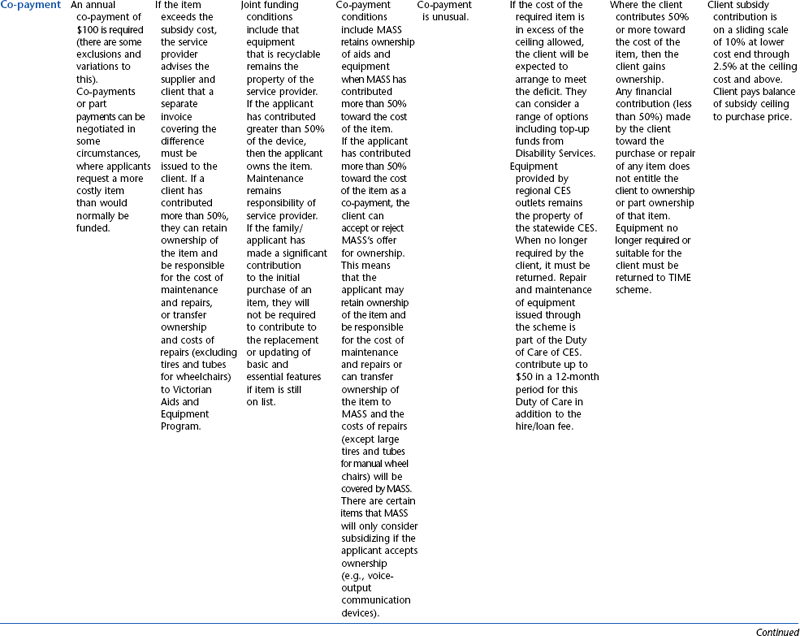
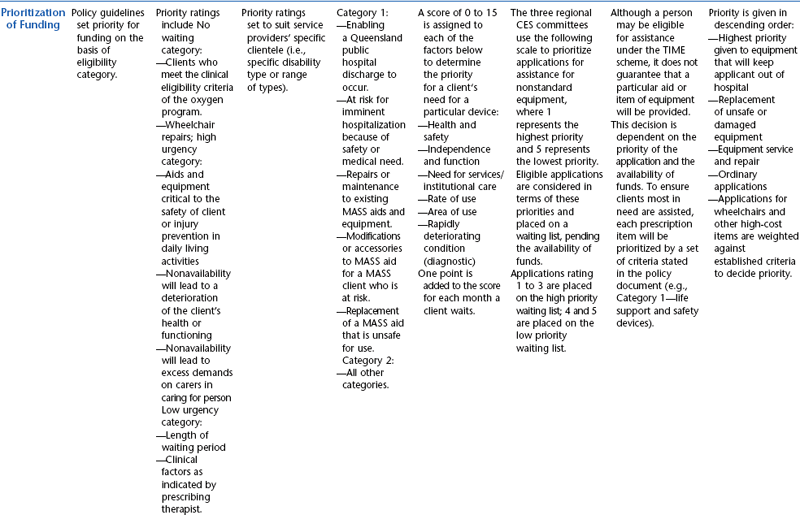
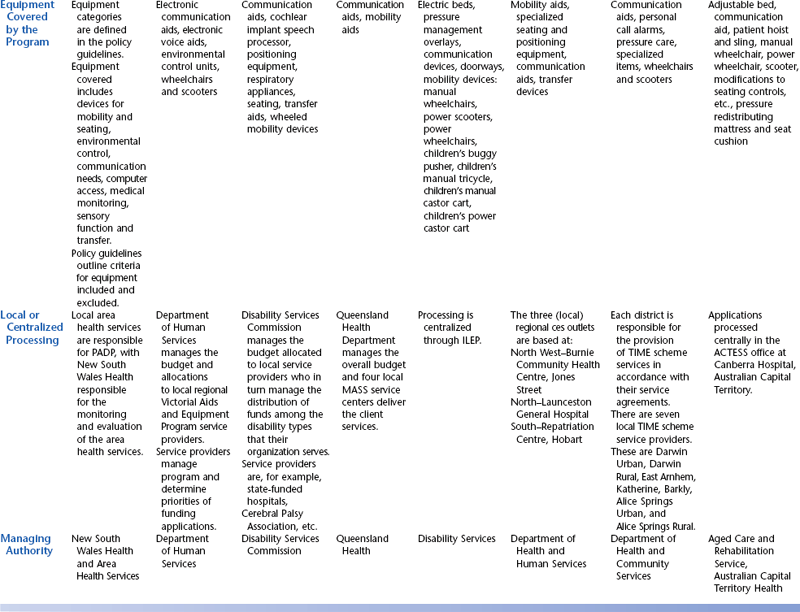
Australian State Government Funding Schemes
The funding programs that are provided through the state governments of Australia have been designed specifically to provide for people with disabilities and include assistive technology in the lists of approved items. The state programs have evolved quite independently in each Australian state or territory and therefore are not uniform. The schemes are administered through various state government departments and are funded from state/territory sources. Although all these programs have similar objectives, there is variation in the level and range of assistance that they provide to people with disabilities. These programs also vary in their level of means testing. The Australian state funding schemes and their Web links are summarized in Table 5-3. Details of Australian public sources of funding for assistive technology devices and services are shown in Table 5-4.
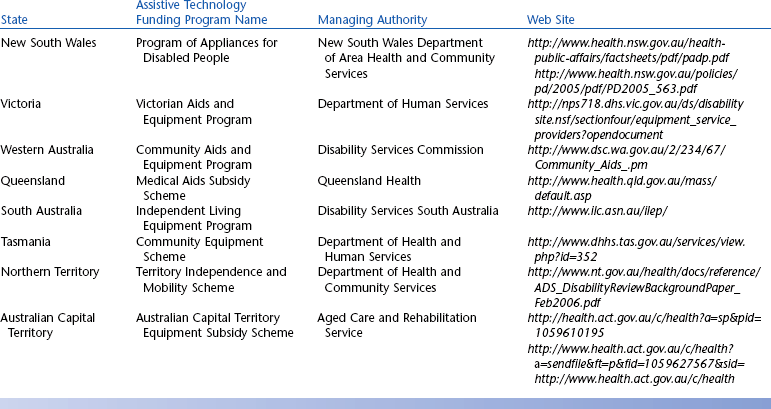
TABLE 5-4
State and Territory Funding Programs for Assistive Technology in Australia
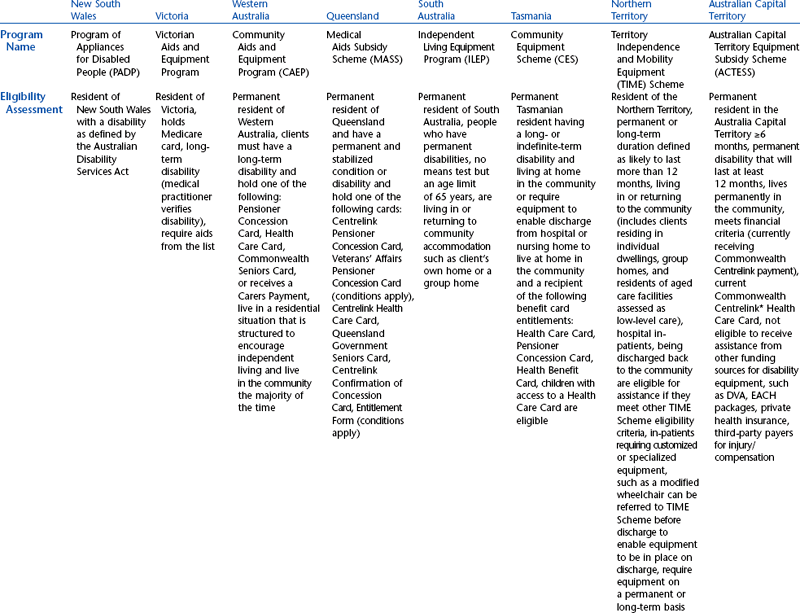
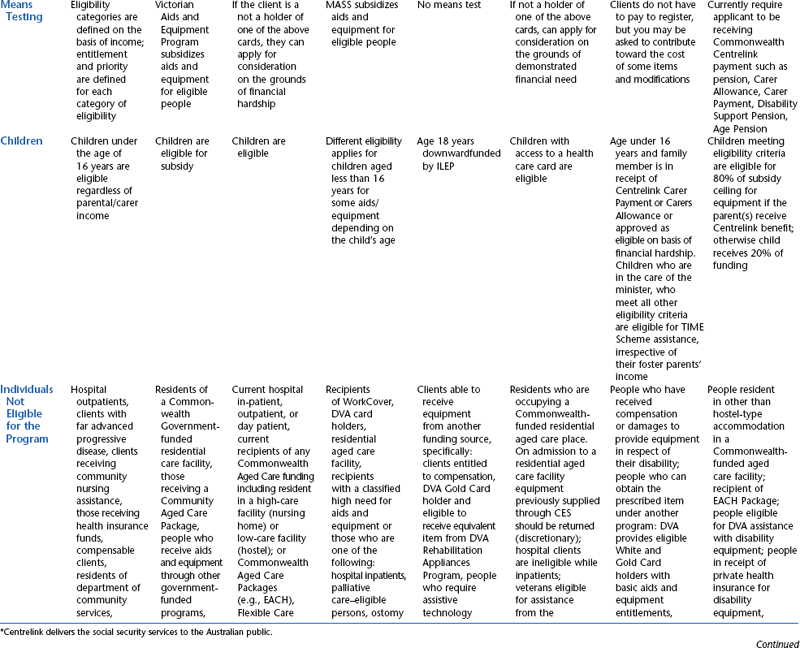
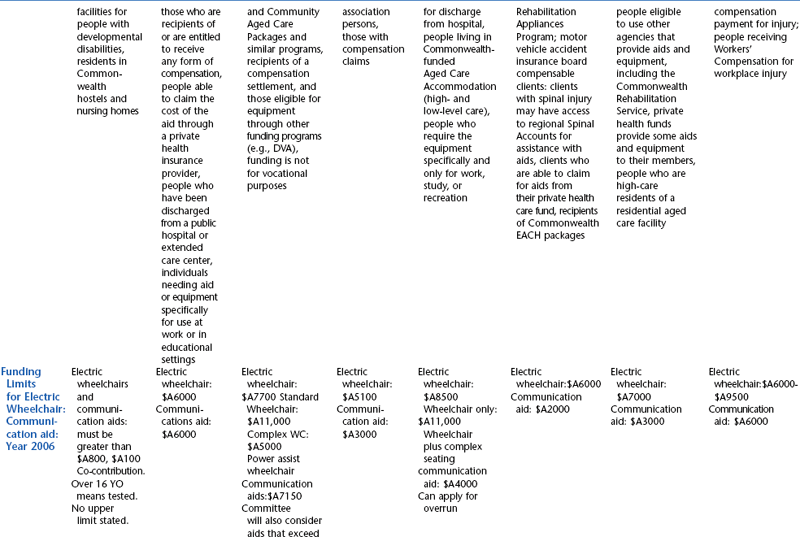
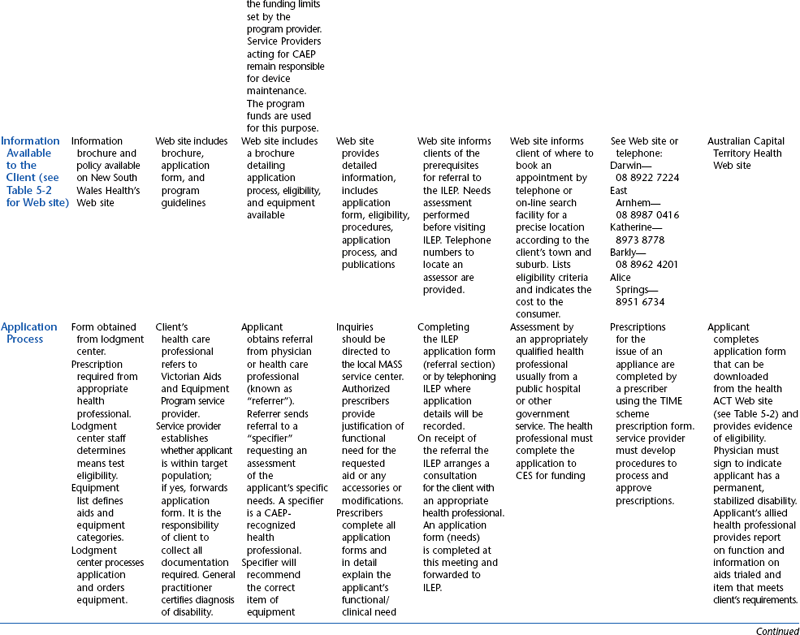
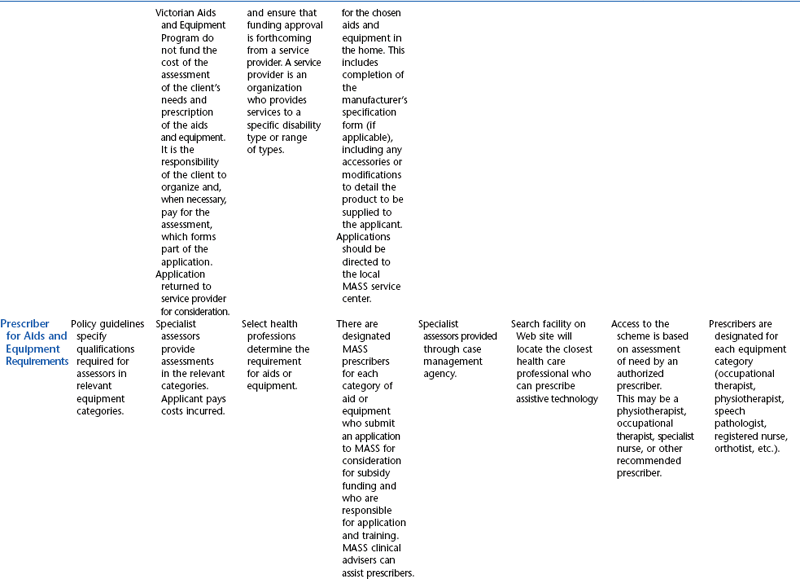
*Centrelink delivers the social security services to the Australian public.
Australian Commonwealth Funded Schemes for the Older Person
The Australian government contributes funding for assistive technology and services for some people with disabilities. The funding is provided through the Department of Health and Ageing (http://www.health.gov.au) and is distributed through schemes that are common to all states and territories throughout Australia. The government-funded schemes are aimed at the frail older person and are generally for the provision of care and accommodation rather than for assistive technology. The eligibility of a person with a disability as distinct from a frail older person to benefit from a funding program is usually an “also” statement grafted on to the definition of a particular scheme.
There are four commonwealth-funded schemes, two that relate to nursing home care and two that relate to funding packages aimed at maintaining frail older people and people with disabilities in the community. Community Aged Care Packages (CACPs) are designed to enable older people who are assessed as eligible for low-level residential (or hostel) care to alternatively remain living in the community. Under the CACP program, a range of services can be provided to the individual, but assistive technology is not included. Extended Aged Care in Home (EACH) packages are similar to CACPs; however, they are targeted at clients who need a high level of care. They were created so that funding can be allocated more efficiently between clients who need high-and low-level care. EACH packages equate to the high-care residential nursing home situation and it is stated in the guidelines that program funds can be used to provide assistive technology.
Australian Department of Veterans’ Affairs—Rehabilitation Appliances Program
The DVA exists to serve members of Australia’s veteran and defense force communities, war widows and widowers, and widows and dependents, through programs of care, compensation, commemoration, and defense support services. The Rehabilitation Appliances Program (RAP) is one of the support services offered by the DVA. It is administered by the DVA and provides aids and appliances to eligible members and their dependents of the veteran community to help them maintain their independence as they grow older. This includes war veterans, members of the Australian Defence Force, former members of the Australian Defence Force, cadets, and war veterans from the United Kingdom and other Australian allies, in some cases. The DVA has major offices in all state capitals and 26 Veterans’ Affairs Network offices throughout Australia. Appliances provided under this program must meet a clinical need and must be the simplest, most effective, and least costly equipment that will suffice. Box 5-2 lists typically funded items under the Australian RAP program. DVA funding for appliances is eligibility tested, and if a person with a disability is eligible for either of the funding schemes the person is generally excluded from using state-based schemes.
Australian Motor Vehicle Compulsory Third Party Personal Injury Insurance
Each state/territory in Australia has a motor vehicle insurance commission designed to provide compensation for people who are injured and become disabled as a result of road accident trauma. Settlements received by people in this situation should be designed with the provision of assistive technology as one of the essential compensatory strategies for the loss of function by the injured person. The insurance commissions or their representatives are listed in Table 5-5, along with the respective Web sites. Australia wide, Motor Vehicle Third Party Personal Injury Insurance is compulsory; it is commonly known as Compulsory Third Party Insurance.
TABLE 5-5
Motor Vehicle Compulsory Third-Party Insurance Funding for Assistive Technologies in Australia
| Jurisdiction | Program | Web Link |
| Western Australia | Insurance Commission of Western Australia | http://www.icwa.wa.gov.au/icwa/ic_menu_list.shtml |
| South Australia | Motor Accident Commission Allianz Australia is the sole claims manager acting on behalf of the Motor Accident Commission of South Australia. | http://www.allianz.com.au/allianz/CICT+SA.html |
| Queensland | Motor Accident Insurance Commission (MAIC)–Allianz Australia is the sole claims manager acting on behalf of the MAIC Queensland. | http://www.allianz.com.au/allianz/CICT+QLD.html |
| Victoria | Transport Accident Commission | http://www.tac.vic.gov.au/jsp/content/NavigationController.do;jsessionid=MGOLMNDPMBIA?areaID=25 |
| NSW | Motor Accidents Authority | http://www.maa.nsw.gov.au/index.aspx |
| Northern Territory | Motor Accidents (Compensation) Act | http://notes.nt.gov.au/dcm/legislat/legislat.nsf/0/960af9d56ee9b5d969256e5c00095824?OpenDocument |
| Tasmania | Motor Accidents Insurance Board | http://www.service.tas.gov.au/Search/PhraseSearch.asp?Task=Applications&DisplayHeading=Motor+vehicle+insurance |
| Australian Capital Territory | Third Party Insurance–Australian Capital Territory | http://www.nrma.com.au/pub/nrma/motor/ctp/act/index.shtml |
Australian Government Education Departments
In Australia, the delivery of education services is a state government responsibility. Education departments in each state provide some assistance to students who need assistive technology to pursue their educations. The programs have tended to develop in isolation and therefore differ in detail from state to state. However, the programs generally concentrate on providing assistive technology that is essential for the student’s education, thus limiting the availability or use of assistive technologies (such as communication aids) more broadly in the community. It is recommended that those interested in pursuing this avenue of funding for assistive technology seek further information from the particular state’s education department.
The Australian Disability Discrimination Act 1991 includes a document entitled “Disability Standards for Education 2005” (http://www.dest.gov.au/sectors/school_education/programmes_funding/forms_guidelines/disability_standards_for_education.htm). This Australian government standard outlines the obligation that educational institutions have to provide equal access to education for a person with a disability. This standard does not directly discuss assistive technology or funding for devices, but it does clearly state the need for the application of both the hard and soft forms of such technologies to ensure access to education for students with disabilities.
PRIVATE SOURCES OF FUNDING
In addition to public funding sources, there are private sources of funding. These vary by country. Examples of U.S. sources are identified in Box 5-1. Private sources of funding in Canada are shown in Table 5-1. Other Australian sources of funding include nongovernment schools, charitable sources (lotteries, service clubs [e.g., Rotary, Lions, Variety]), philanthropic organizations, private health insurance, and worksafe programs. The availability of these programs, the specific coverage, and the eligibility criteria vary across the country.
Self-Funding
Personal sources of funding include out-of-pocket cash paid by the consumer, private trust funds, and loans. Because of the cost of assistive technology equipment and services, paying cash could be a hardship on the consumer. Sometimes this is the only alternative, however. Some individuals have trust funds set up where money received from a legal settlement is kept to provide for the equipment and services they may need, including assistive technologies. Individuals who use personal funds to purchase assistive technology may be eligible for a deduction or credit on their taxes and should consult with a tax accountant.
In the United States and some other countries low-interest loans are also available for the purchase of assistive technology. These programs are a major initiative of the Assistive Technology Act, which sought to broaden the availability of low-interest loan programs throughout the country. In procuring a loan, the consumer shares the responsibility of paying for the equipment, which may increase the consumer’s involvement in the process (Reeb, 1989). The Easter Seal Society has recently set up a national loan fund to help persons with disabilities purchase assistive technologies. The loan fund was made possible by a U.S. Department of Education grant. Up to 75% of the equipment costs can be financed. The maximal amount that can be financed is $3200. Some manufacturers and vendors also provide low-interest loans. A consumer in need of a loan should check with these sources as well.
Private Health Insurance
Private health insurance is the source of approximately 35% of all health expenditures in the United States (government and direct private payments comprise the other sources) (U.S. Dept. of Commerce, Bureau of the Census, Statistical Abstract of the United States, 2006, Table 118, p. 98). Most often, insurance is an employment fringe benefit, although individuals also can purchase an insurance policy on their own. Although insurance policies may vary considerably, benefits such as durable medical equipment are almost always included. Very often, rehabilitation therapies such as occupational therapy, physical therapy, and speech-language pathology services also will be covered. When assisting an individual with insurance, the ATP will have to ensure that the item or service being sought fits within one or more of the covered services of the policy and that no coverage exclusions or limitations apply. This information will be found in the benefits booklet that is provided with the policy, which details the scope of coverage and exclusions as well as co-payments, deductibles, preferred providers, if any, and appeal procedures. As in public health insurance, funding by private health insurance companies is based on a medical diagnosis and justification of medical necessity. Most private forms of health insurance require the use of current procedural terminology (CPT) codes for billing (see section on billing and coding later in this chapter).
Private health insurance is also a potential source for funding assistive technology devices and speech-language pathology and occupational and physical therapy services beyond what is publicly funded in Canada. Private health insurance is often used to “top-up” benefits when funded amounts are inadequate (e.g., too few hours of training for an augmentative communication device) or when there is a co-payment.
OTHER SOURCES OF FUNDING
There are alternative sources for funding that do not fall under the categories of public or private agencies (see Box 5-1). These sources include service clubs, private foundations, and volunteer organizations. There are various community service clubs (e.g., Kiwanis, Rotary Club) that may be a source of funding for a local individual who has no other means of funding. Service clubs are more likely to provide funding if one of their goals is to help certain disability groups or if the consumer is a member of the club or personally knows someone who is a member. Examples are two funds created by the Muscular Dystrophy Association that allow individuals with neurodegenerative diseases such as MD or ALS to receive up to $2000 to facilitate access to a speech-generating device and up to $2000 to facilitate access to a mobility device.
There are foundations related to a specific disability group that directly supply equipment and services to individuals with that particular disability. Other disability-related foundations provide partial funding or assist the consumer in obtaining funding. The American Federation for the Blind provides low-interest loans, for example, to individuals who are visually impaired and need to purchase equipment (Matheis et al, 1991). There are also a number of volunteer organizations (e.g., Telephone Pioneers of America) that may contribute by fabricating a custom device. Usually the labor is provided and the consumer pays for the cost of materials. Similar benefits are provided by the Canadian National Institute for the Blind.
FUNDING PROCESS AND GUIDELINES FOR PROCURING FUNDING
To obtain funding for assistive technology devices services, individuals with disabilities must follow the procedures and guidelines established by each program for which they are eligible and that covers the items being requested. ATPs play a crucial role in this process. Most often it is the ATP who must make the case for funding by conducting assessments, preparing reports, gathering prescriptions and other documentation, and communicating with equipment suppliers and funding program staff. If there is a trial period, the ATP will generally supervise it and report the results to establish the potential benefit of the device. ATPs also are the primary liaison between the client, the supplier, and the funding sources. If funding is denied, ATPs are often called on to coordinate appeals, which may involve representation of the client or soliciting and then working with a professional advocate who will pursue the appeal on the client’s behalf. Although most of these tasks are not compensated, funding has to be pursued, ATPs have to do it, and it has to work for the consumer to receive the services and devices.
A complicating factor is that consumers may be eligible for multiple sources of funding, each of which may have different rules and procedures. This is particularly true because funding and benefits programs have been created to serve very specific purposes, yet health services are able to serve broader goals. Thus, the same services may be covered by multiple programs (e.g., occupational therapy will be covered as a special education–related service and a health benefit within health insurance) or by Medicaid (in the United States). It also is not uncommon for individuals to have multiple sources of health care coverage (e.g., private health insurance and Medicaid or Medicaid and Medicare). Coordinating the benefits of these programs is important to ensure maximum benefit to the consumer.
Over time, the ATP may be called on to seek funding for the same client and for the same item or service multiple times. Funding will be sought to pay for the initial assessment, for purchase of a device, for payment for training and other services; for repairs or modifications to the device; for periodic reassessment of needs; and ultimately for device replacement. Most programs that pay for equipment purchase or rental also will pay for equipment repair and, as necessary, replacement.
Soft technology services such as training are important for many types of assistive technologies, both for the device user and caregivers. Funding for these services, however, is not always covered, even if device purchase is covered. Obviously, the provision of a device without these services can have adverse consequences for the individual. The ATP may be called on to identify alternative sources for these services, such as training offered by supplier sales representatives.
The several points during the service delivery process at which funding may need to be pursued are shown in Figure 4-2. To the novice ATP, funding programs can appear as a dense or even impenetrable web, but the funding process is navigable. Care and attention to detail are required, but this is not different from the general obligations of the ATP in all his or her professional activities.
IDENTIFYING THE FUNDING SOURCE
The various funding sources are described earlier in this chapter and in Chapter 1. This section provides guidelines for navigating the U.S. process of obtaining funding. This process also applies in broad terms to other countries. In general, consumers will know what programs they are eligible for. If they are eligible for Medicaid, Medicare, private insurance, or Tricare, they will possess a wallet card stating their eligibility. (Suppliers may require photocopies of both sides of this card to be submitted along with the other documentation to support a funding request.) Those who are veterans will know they are eligible for DVA services. Children with disabilities are likely to already have been identified and referred to the early intervention or special education systems. The only program where an ATP is likely to be a valuable asset regarding initial program eligibility is vocational rehabilitation. The client’s ability to demonstrate a potential to work may be dependent on access to assistive technology, and it will be the ATP’s evaluation and report that both identifies that need and establishes eligibility for the broader range of vocational rehabilitation services. From this list of potential funding programs, the ATP must begin to coordinate the justification and documentation process. Specific evaluations and reports may be required by each program. Great care must be taken to prepare written reports to ensure that the standard of need for each program or unique program vocabulary is stated. For example, each of the agencies that provide funding for assistive technologies may have a different standard of need. Educational agencies will fund assistive technology that provides a student with access to education. Medicare and Medicaid only fund durable medical equipment that is medically necessary, such as wheelchairs and seat cushions. In state vocational rehabilitation agencies, there is a standard that the assistive technology must significantly contribute to the individual’s ability to be productive at work for it to be funded. The role of the ATP is to know which programs are likely to fund the particular types of services and devices that are required by an individual consumer. These can then be matched to the benefits provided by the programs for which the consumer is eligible. Assistive technology equipment suppliers are aware of the funding sources that can be used for reimbursement of their products, and they can be useful sources of information to the ATP and the consumer. ATP reports describing “needs” must be written with care and written with the expectation the reviewer will be looking for vocabulary that is consistent with the reviewer’s program’s purposes.
Dealing with the multiple public or private agencies is a challenge. Procedures for obtaining funding for assistive technologies, levels of funding, and staff familiarity with the scope of and need for assistive technology and related services vary from agency to agency. For example, some funding agencies require that equipment and services be purchased from an approved list of vendors. Other funding agencies require approval for services and equipment before implementation. It is the responsibility of the consumer and the ATP to locate for each agency the regulations that apply to assistive technology and pursue funding on the basis of those regulations. Another important consideration is the principle of “payer of last resort,” which requires a specific sequencing of multiple benefits or funding programs. The Medicaid program is identified by statute as the payer of last resort in relation to other health benefits programs. For this reason, if a consumer has both Medicaid and Medicare or Medicaid and private health insurance, the procedures related to obtaining payment from Medicare or from the private insurance must be followed first before a claim can be submitted to Medicaid. In general, the procedure for sorting the relationship between multiple funding programs is called “coordination of benefits.” Another characteristic of benefits and funding programs, particularly those that provide health benefits, is that they compartmentalize coverage. Specific services will be provided, such as durable medical equipment, occupational therapy, physical therapy, or speech-language pathology. However, not all these services may be covered. Thus, a program may pay for an item of durable medical equipment but not cover the assessment to establish need for the item or training in its use. These limitations force the ATP to be alert for alternative sources of funding so that all the person’s needs can be met.
As a practical matter, an ATP may not only be interacting with multiple funding programs for the same item or service if a person has dual eligibility and both programs cover the service but also may be working to secure multiple items or services for the client at the same time. The following case study provides an example of a person with multiple funding programs and multiple needs.
To simplify the process of obtaining funding, it is recommended that a funding strategy be developed for each consumer. Beukleman and Mirenda (2005) identify five steps in developing such a strategy:
1. Survey the funding resources that are available to the individual.
2. Identify various funding sources for the various activities of an intervention (i.e., assessment, equipment, and training). The use of a personal funding worksheet such as the one shown in Box 5-3 is helpful.
Funding for Miranda
Miranda is 14 years old and a freshman in high school. She has cerebral palsy and uses a wheelchair for mobility. She is also nonverbal. Her teacher referred her to the assistive technology center for an augmentative communication evaluation. During the needs assessment, it was discovered that Miranda was also in need of a new seating and mobility system. Her mother also expressed a desire for Miranda to be more independent at home and to be able to turn the TV and her stereo system off and on. Miranda has a range of assistive technology needs, and it became apparent to the ATP that funding for Miranda was going to have to come from multiple sources. Given the information that was shared during the needs assessment, the ATP completed a personal funding worksheet for Miranda. The ATP will seek funding from the state Medicaid system for the seating and mobility system, from the school system for an augmentative communication device, and from Miranda’s personal resources for an electronic aid to daily living (EADL) to turn her TV, stereo, and appliances off and on. Her father is also involved in the local Rotary Club and that may be another source of funding for the EADL.
BOX 5-3 Personal Funding Worksheet
Paul H Brookes
Client: __________________________________________________________________________________________________________________
Type of intervention (e.g., augmentative and alternative communication devices, mobility): _______________________________________
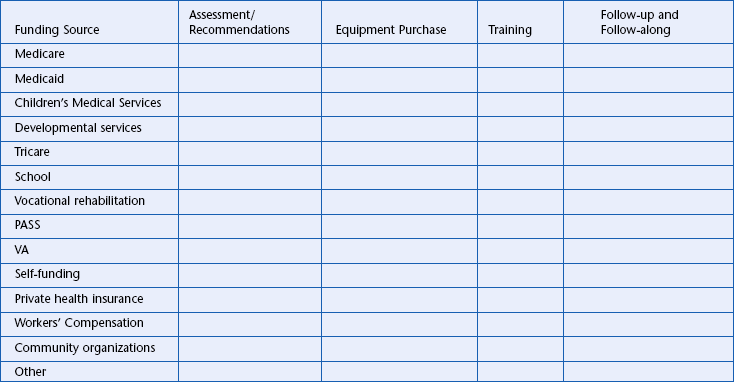
Modified from Beukelman DR, Mirenda P: Augmentative and alternative communication, management of severe communication disorders in children and adults, Baltimore, 2005, Paul H Brookes.
3. Prepare a funding plan with the consumer and the family members.
4. Assign responsibility to specific individuals for pursuing funding for each aspect of the intervention.
5. Prepare necessary documentation for the funding request. Be sure to make all requests in writing so that a written record is available if an appeal is necessary.
Keeping current on funding information is time consuming but absolutely essential for the ATP. Every state has a technology assistance project (see Chapter 1) that disseminates information on funding resources and strategies. For contact information, refer to the Rehabilitation Engineering and Assistive Technology Society of North America Technical Assistance Project Web site (www.resna.org). Assistive Technology: A Funding Workbook (Morris and Golinker, 1991) also provides information on funding resources and strategies. The independent living centers found in each state are another source of funding information and advocacy. Networking with other assistive technology professionals at conferences, by listservs, and over the phone are other invaluable resources.
JUSTIFYING FUNDING FOR ASSISTIVE TECHNOLOGY SERVICES AND DEVICES
Third-party payers require adequate documentation and proof of need before they will approve funding for assistive technology services or equipment. The essential question funding sources want answered is how this technology will improve the individual’s functioning. Whether it is a medical, vocational, or educational need, there are essential components that should be included in any written justification. Golinker and Mistrett (1997) identify components to address when justifying a medical need for a device, but these elements can apply to other justifications as well. These components are summarized as follows:
1. A description of the specific functional limitation that the device and service addresses
2. A detailed description of the device, including features, accessories, and customization
3. A specific description of the effect of the device or service (e.g., how it will alleviate or ameliorate the functional limitation)
4. A description of the evaluation process, how the recommendation was arrived at, and what other alternatives were considered
5. An explanation of why the device being recommended is the least costly equally therapeutically effective solution
6. A description of the expertise of the ATP (or interdisciplinary team) recommending the services or equipment, including general professional experience and specific experience in assistive technology services
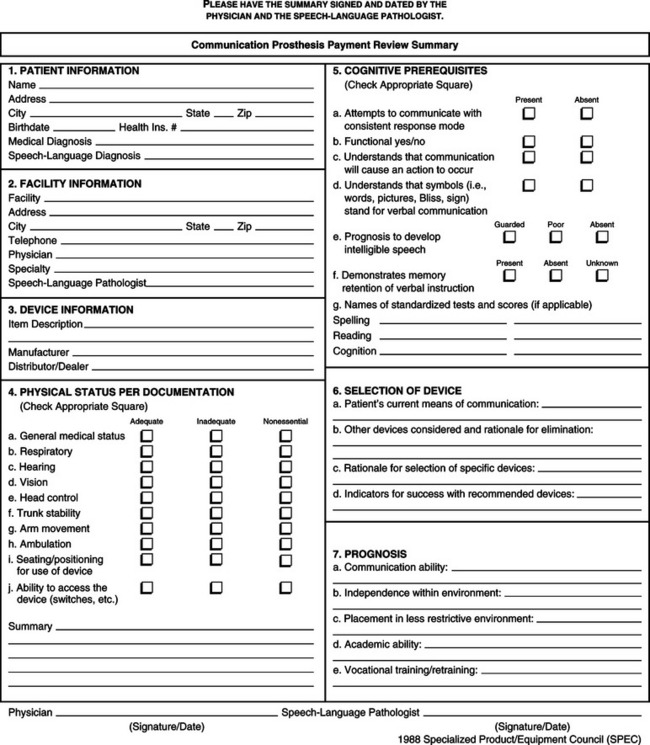
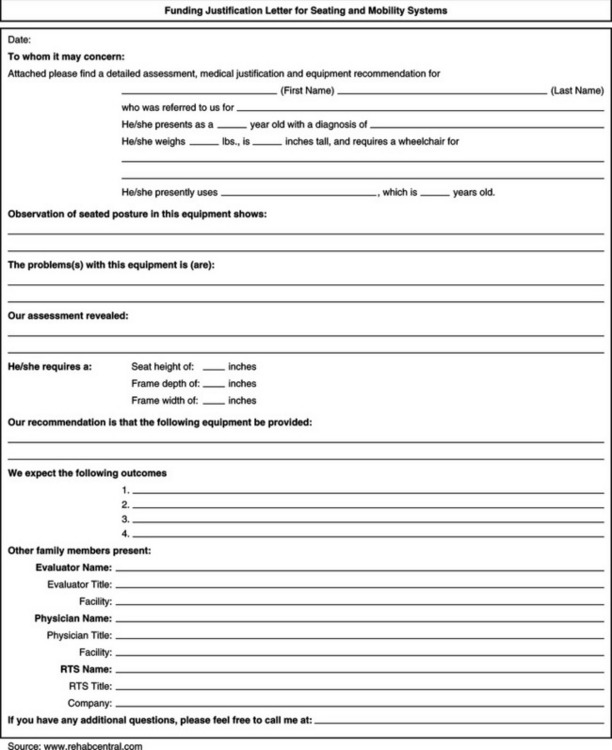
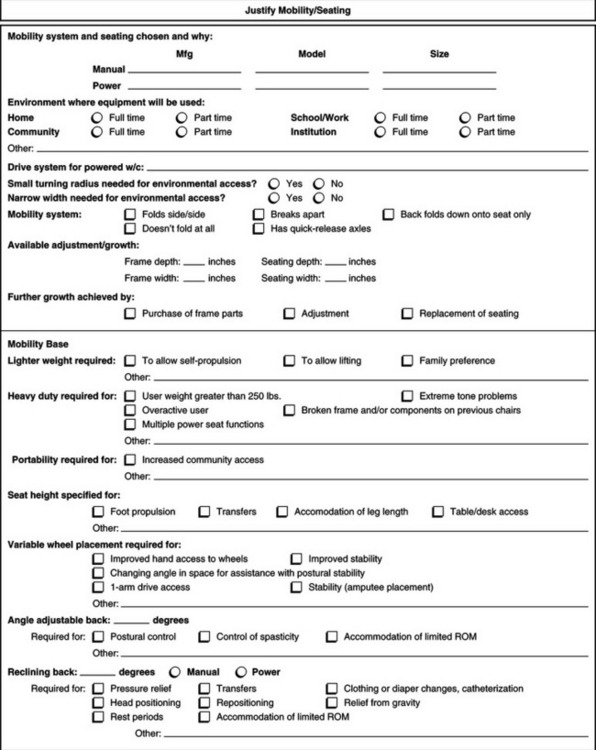
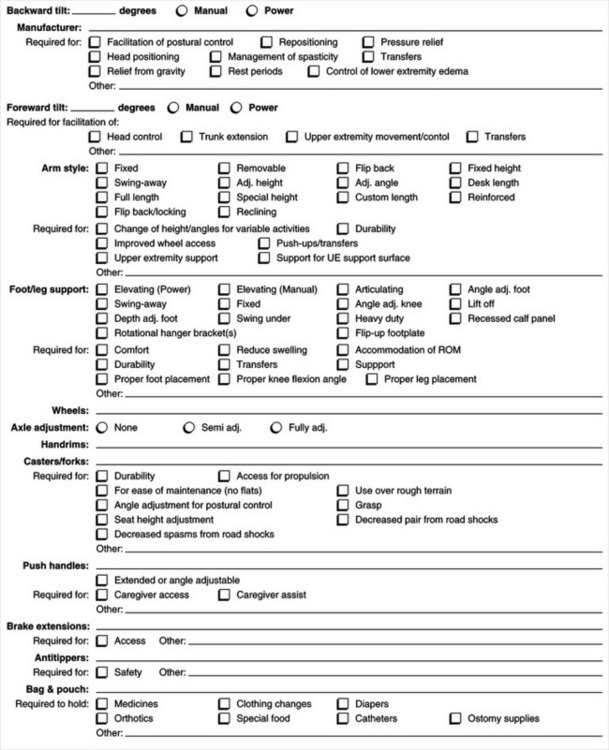
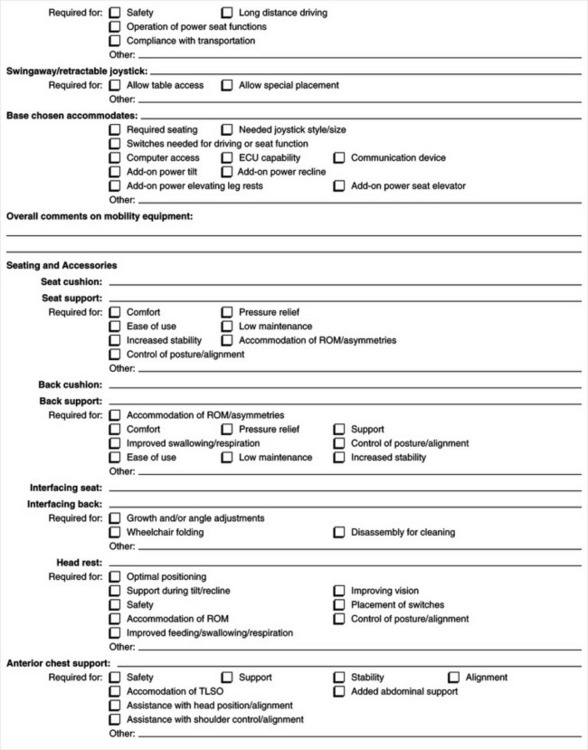
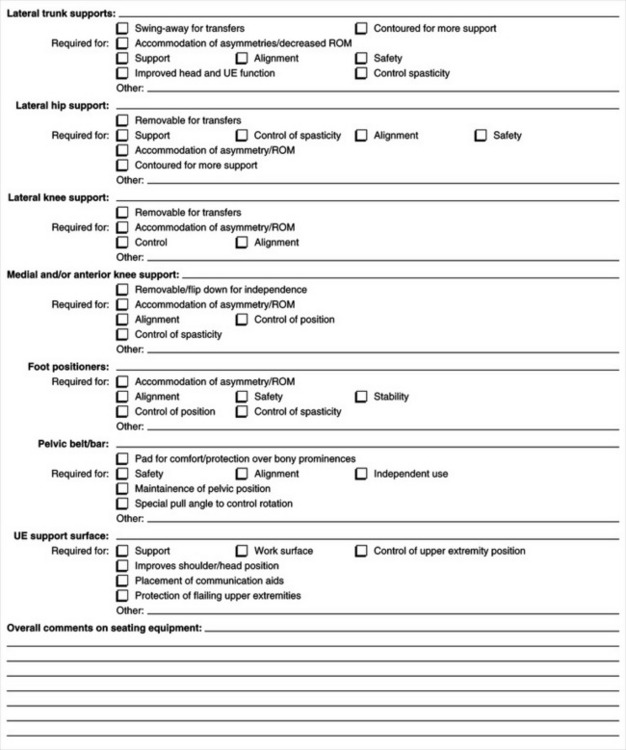
A specific criterion for funding under Medicare, Medicaid, and private health insurance is medical necessity. This requires that the justification include “identification of a medical diagnosis, or condition, that is specifically coupled to the functional impairment being addressed by the device” (Golinker and Mistrett, 1997, p 217). A physician’s prescription is required for devices that are medically necessary. Appendix 5-1A provides an example of a form to use to justify funding for augmentative communication devices and Appendix 5-1B shows an example of a justification form for seating and wheeled mobility systems.
When funding is being pursued through a vocational rehabilitation agency, it is important that the written justification specify how the device will enhance the individual’s ability to function in a work setting. For assistive technology services and equipment to be considered, they need to be part of the consumer’s IPE. Similarly, when funding is being pursued through special education, the justification needs to address how the equipment will give the child access to a free and appropriate education in the “least restrictive environment.” All assistive technology services and equipment must address goals written in the child’s IFSP for children from birth to 2 years old or in the IEP for children aged 3 to 21 years. For children in school, an additional comment is appropriate. Many health services also are school-related services. Typically, schools provide these services. If a child needs more health services than a school offers, health services programs such as Medicaid or insurance will be sought as a supplemental benefit. For Medicaid-eligible children, Medicaid will often pay the school for its provision of certain related services that also are covered by Medicaid, such as audiology, occupational therapy, physical therapy, speech-language pathology, and nursing services.
It is likely that the staff person reading the funding justification has never met the consumer and may not have had any experience with a person with a disability or with assistive technology. It is important that the justification be easily understood and that it clearly depict who this person is, what the needs are, and how the system can help. It may be helpful to include a picture or videotape of the consumer with the system being recommended.
APPEALING THE FUNDING DENIAL
At any point in the funding process, a denial for funding may be received. When requests for funding have been denied, it helps to be persistent and to submit an appeal for the denial. It is through this persistence that funding sources may eventually include assistive technologies as a regular part of the support they provide.
Every funding agency has an appeals process whereby the client, ATP, family member, or a professional advocate can appeal a funding denial. The first step taken is to determine the procedure for an appeal and the time limitations related to appeals. The next step is to find out why the request was denied. Almost all funding programs will provide an explanation to the client in writing. By knowing the reason for denial, all persons working to help the client can develop an appeal plan. It will be based on a comparison of the denial reason to the facts, to the scope of benefits offered by the program, including program definitions and guidance, and wherever possible, to a comparison of the funding program’s past actions when the same item or service was sought. In short, an appeal plan allows for the development of a specific statement of why the denial is wrong and why it should be reversed. It also will allow for identification of any missing information or clarifying statements to supplement what already has been submitted. Implementation of the plan will be an appeal that specifically addresses the denial reason and thus decreases the likelihood of the appeal being denied as well. Sometimes a request is denied because a piece of information was inadvertently omitted, such as a billing code, and resubmission of the request with the necessary information is all that is needed. Or, the denial may have been made because the agency believes that the plan or policy does not include such a benefit, or it may be based on the fact that the provider does not think that the request meets the criteria for funding.
Mendelsohn (1996) discusses typical grounds for appeal and the format that appeals may take. The purpose of an appeal is to convince the funding agency that the denial was erroneous and to have the decision reversed. The appeal should be made in writing to the funding source. It should explain why the denial for funding was inappropriate and provide any additional information that may have been omitted in the initial request (Golinker and Mistrett, 1997). During the appeals process it may be necessary to ask for assistance from a skilled advocacy layperson or an attorney.
BILLING AND CODING FOR SERVICES
Preparing the billing form correctly and using the proper codes on billing forms are necessary to ensure payment. Medical payers require that the provider use diagnosis codes and procedure codes when services are billed. Diagnosis codes are used to describe the person’s condition or the medical reason for the services being requested; it is this condition that is the key to establishing medical necessity. The most widely used diagnosis coding system in the United States is The International Statistical Classification of Diseases and Related Health Problems, tenth revision (World Health Organization, 1992).
In the United States procedure codes are used to describe the services that the provider implemented or the equipment delivered and that are being billed. The Health Care Financing Administration (HCFA) Common Procedure Coding System (HCPCS) is the most commonly used procedure coding system. It has three levels: (1) the American Medical Association’s physician’s CPT is referred to as Level I HCPCS, (2) Level II HCPCSs are the HCFA-developed alphanumerical codes, including codes for durable medical equipment, prosthetics, orthotics, and supplies, and (3) Level III HCPCSs are local codes created as needed by Medicare and other carriers (Acquaviva, 1998). Example CPT codes relevant to assistive technology devices and services are shown in Box 5-4.
The CPT codes are a set of five-digit codes that pertain to the medical service or procedure performed by physicians and other service providers. The CPT Editorial Panel of the American Medical Association establishes the CPT codes, which have become the industry standard for reporting, and updates them on an annual basis. There is a physical medicine and rehabilitation section of the CPT codes under which occupational, physical, and speech therapy can bill for certain procedures that may encompass assistive technology intervention. The codes in this section are defined in 15-minute segments. For example, an occupational therapist who has instructed a consumer with a visual impairment on the use of sensory aids to increase independence in self-care can bill using CPT code 97535 (“Selfcare/Home management training [e.g., ADLs and compensatory training, meal preparation, safety procedures, and instruction in the use of adaptive equipment direct one-on-one contact by provider, each 15 minutes”). Practitioners may use codes in any section of the CPT as long as the service is within the scope of practice for the practitioner (Acquaviva, 1998). A new code specific to assistive technology has been drafted and is in the process of getting approved as an addition to the CPT codes.
PAYMENT PRACTICES
The traditional method of payment for health care has been fee for service. Under this method of payment, providers are paid a certain rate per unit of service (American Occupational Therapy Association [AOTA], 1996). As a result of skyrocketing health care costs in the United States, however, payment practices in the health care field have changed significantly over the last decade. Managed care has emerged as a means of controlling health care costs. The term managed care is used to describe “any method of health care delivery designed to reduce unnecessary utilization of services, and provide for cost containment while ensuring that high quality of care or performance is maintained” (Rognehaugh, 1998, p. 134). Managed care plans are now a major part of private health insurance offerings, as well as part of publicly funded insurance programs such as Medicare, Medicaid, Workers’ Compensation programs, and CHAMPUS.
Several measures are used by managed care plans to limit either provider payments or enrollee use of services. The primary cost-cutting mechanism used in managed care is capitation. Negotiating with providers for a prepaid amount gives providers a direct stake in controlling their costs. In this arrangement the managed care organization (MCO) agrees to pay the provider a set amount of money on a per-member basis in exchange for the provider’s assuming responsibility for furnishing all or certain health services to a patient for a specified period of time (AOTA, 1996). The provider takes the risk that the capitation rate will be sufficient to cover all the costs of care for the members. An enrollee in the MCO’s plan is restricted to using providers that have a contractual agreement with the MCO.
Other measures used by MCOs to control costs include precertification or preauthorization, mandatory second opinions, case management, and use of a third-party administrator (AOTA, 1996). For ATPs, the implications of managed care are many. Primarily it makes it difficult or impossible to get paid for services if the ATP does not have a contract with an MCO or is not part of a group that contracts with an MCO. The ATP also should determine whether the provider requires preauthorization or second opinions before carrying out any services with the consumer. Case managers are being used more often, particularly in situations where the individual has had an injury or accident resulting in a long-term disability. Most case managers in the United States are nurses who may have limited experience with assistive technology. The case manager is a gatekeeper who controls access to the services that are provided to the individual, including assistive technology. One way for ATPs to learn more about case management and conversely to educate case managers about assistive technology is through the Case Management Society of America (CMSA) and its on-line forums, which can be accessed at the CMSA Web site (www.cmsa.org).
Consumers and ATPs need to continually be involved in educating funding sources and advocating for the inclusion of assistive technology equipment and services in agencies’ policies. As discussed in Chapter 4, ATPs need to expand their documentation of the benefits and outcomes of assistive technology. This documentation provides helpful information when advocating for increased allocation of funding by public and private agencies.
SUMMARY
The various sources of funding for assistive technology services and equipment are described in this chapter. Sources of funding for assistive technology are either public or private and include programs such as Medicare, Medicaid, vocational rehabilitation, education, private health insurance, low-interest loans, and grants. The ATP should be knowledgeable about the different funding sources and the process for successfully obtaining funding. This includes identifying the appropriate funding source for the consumer, writing a funding justification, billing and coding for assistive technology, and appealing denials as needed. Furthermore, it is important that the ATP advocate at the public policy level for increased coverage of assistive technology services and equipment.
1. List the major steps in identifying a funding source for a particular assistive technology device or service.
2. What are the major categories of funding for assistive technology devices?
3. What are the major assistive technology funding sources typically available for a child who is in an educational program and needs an augmentative communication device?
4. What are the most likely funding sources for support of assistive technology devices and services for an adult who sustains a head injury at the age of 25 years?
5. Compare funding sources for assistive technologies in the United States, Australia, and Canada. What features are common and which are different?
6. Describe two distinct funding sources and identify at least one criterion that must be met by the consumer to be eligible for funding of assistive technology services from each source.
7. What are the types of personal funding?
8. What restrictions are typically placed on private insurance funding of assistive technology devices and services?
9. What is the source of the benefits available under Workers’ Compensation?
10. What are the major challenges in identifying the most likely funding source for a given situation?
11. Define the term “medical necessity.”
12. When writing a medical justification for a device for a consumer, what elements should be included?
13. What are CPT codes, and how can they be used in securing funding for assistive technology services and devices?
14. List three types of alternative funding sources for assistive technology devices and services.
15. What are the five steps recommended for developing a funding strategy?
16. Describe the two types of billing codes commonly used in health care.
17. What is managed care, and how does it affect assistive technology service delivery?
18. What is meant by the term capitation? What are the implications of capitation for assistive technology service delivery?
19. What are the major steps taken to appeal a funding denial?
20. How can consumers and ATPs work together to inform funding sources of the needs for assistive technology services and devices?
APPENDIX 5-1
Sample Forms for Documenting Consumers′ Equipment Needs
APPENDIX 5-1A
Communication Prosthesis Payment Review Summary
> Name—Patient’s complete name
> Address—Patient’s home address
> Health Insurance Number—Appropriate number for coverage
> Medical Diagnosis—Document medical diagnosis (ICD-9-CM) for the patient
> Speech-Language Diagnosis—Document Speech-Language diagnosis (ASHACS) for patient
> Facility—Wherre the patient is receiving treatment
> Address/Phone Number—Facility address and phone (with area code)
> Item Description—General description of device being recommended
> Manufacturer—Maker of the device
> Distributor/Dealer—Local source of supply, including service and training
> Check the square that characterizes the patient’s current physical condition per medical/clinical documentation or personal observation
> Adequate/inadequate rating related to physical patameters only as they apply to the use of the specific communication device
> Nonessential rating indicates status is not related to the use of the device for this patient.
5. PATIENT’S COGNITIVE PREREQUISTES
> Check the appropriate square that best describes the patient’s current status.
> If applicable, provide the name of the testing instrument and the scores obtained
6. SELECTION OF AUGMENTATIVE COMMUNICATION DEVICE
a. Current Means—Describe how this patient currently communicates and why it is not the best method of choice.
b. Other Devices—List other devices considered for this patient and why they would not be applicable.
c. Rationale—What characteristics of this device influence the determination that it was the best choice, e.g., portability, size, symbols, service, or training.
d. Indicators—Has the patient had an opportunity to use the device? How long? Rental? What was observed, e.g., increased initiation of ADLs
a. Communication Ability—Will the patient’s ability to communicate basic needs, such as health and safety information, be improved?
b. Independence—Will the patient’s independence increase with the use of the device?
c. Placement—Will the community placement be affected? Example: group home vs. nursing home.
d. Academic Ability—Will the patient’s ability to learn and retain new information change?
e. Vocational Training—Will the patient’s ability to advance in vocational rehabilitation improve?
8. COMMENTS—Give any comments unique to this device or what it will offer for this individual that would help in determining payment. Use space provided on the reverse side of the summary form.
References
Acquaviva J, ed. Effective documentation for occupational therapy, ed 2, Bethesda, MD: American Occupational Therapy Association, 1998.
American Occupational Therapy Association Managed Care Project Team. Managed care: an occupational therapy sourcebook. Bethesda, MD: The Association, 1996.
Beukelman, DR, Mirenda, P. Augmentative and alternative communication, management of severe communication disorders in children and adults, ed 3. Baltimore: Paul H Brookes, 2005.
Burton, J. Workers’ compensation, twenty-four-hour coverage, and managed care. Work Comp Mon. 1996;9:11–21.
Golinker, L, Mistrett, SG. Funding. In: Angelo J, ed. Assistive technology for rehabilitation therapists. Philadelphia: FA Davis, 1997.
Matheis, D, et al. The buck starts here … a guide to assistive technology funding in Kentucky. Frankfort, KY: Department of the Blind, 1991.
Mendelsohn, S. Funding assistive technology. In: Galvin JC, Scherer MJ, eds. Evaluating, selecting, and using appropriate assistive technology. Gaithersburg, MD: Aspen Publishers, 1996.
Morris, MW, Golinker, LA. Assistive technology: a funding workbook. Arlington, VA: RESNA Press, 1991.
Reeb, KG. Assistive financing for assistive devices: loan guarantees for purchase of products by persons with disabilities. Washington, DC: Electronic Industries Foundation, 1989.
Rognehaugh, R. The managed care health care dictionary, ed 2. Gaithersburg, MD: Aspen Publishers, 1998.
U.S. Department of Commerce, Bureau of the Census: Statistical abstract of the United States, 2006, Table 118, p. 98.
World Health Organization. The International statistical classification of diseases and related health problems. Geneva: World Health Organization, 1992. [10th revision].