Delivering Assistive Technology Services to the Consumer
PRINCIPLES OF ASSISTIVE TECHNOLOGY ASSESSMENT AND INTERVENTION
Assistive Technology Assessment and Intervention Should Consider All Components of the HAAT Model: Human, ctivity, Assistive Technology, and Context
Assistive Technology Intervention Is Enabling
Assistive Technology Assessment Is Continuous and Deliberate
Assistive Technology Assessment and Intervention Require Collaboration and a Consumer-Centered Approach
Assistive Technology Assessment and Intervention Require an Understanding of How to Gather and Interpret Data
Quantitative and Qualitative Measurement
Norm-Referenced and Criterion-Referenced Measurements
Methods for Gathering and Interpreting Information
OVERVIEW OF SERVICE DELIVERY IN ASSISTIVE TECHNOLOGY
Evaluation of Functional Vision
Evaluation of Visual Perception
Evaluation of Tactile Function
Evaluation of Auditory Function
Identifying Potential Anatomical Sites for Control
Selecting Candidate Control Interfaces
Comparative Testing of Candidate Control Interfaces
Matching Electronic Device Characteristics to the User’s Needs and Skills
Evaluating the Match Between Characteristics and the Consumer’s Skills and Needs
Effects of Errors in Assistive Technology Systems
Facilitating Assistive Technology System Performance
EVALUATING THE EFFECTIVENESS OF ASSISTIVE TECHNOLOGY SERVICES AND SYSTEMS
Measuring Clinical and Functional Outcomes
Functional Independence Measure
User Satisfaction as an Outcome Measure
Canadian Occupational Performance Measure
Quebec User Evaluation of Satisfaction With Assistive Technology
Assistive Technology Abandonment
Quality of Life as an Assistive Technology Outcome Measure
Health-Related Quality of Life
Psychosocial Impact of Assistive Devices Scale
Matching Person and Technology Model
Relationship of Outcome Measures to the Human Activity Assistive Technology Model
On completing this chapter, you will be able to do the following:
1 Describe principles related to assessment and intervention in assistive technology service delivery
2 Describe the methods used to gather and analyze information during assistive technology assessment and intervention
3 Understand the relationship between the consumer’s life roles and performance areas and his or her needs for assistive technology
4 Identify and describe each of the steps in assistive technology service delivery
5 Discuss the matching of device characteristics to consumer needs and skills
6 Understand the need for training and how to develop effective programs
7 Define outcomes as related to assistive technology
8 Understand why outcomes in assistive technology need to be measured
9 Discuss the principles of outcome measurement and their relationship to service delivery and system effectiveness
10 Understand how measurement of outcomes in related disciplines can contribute to knowledge and development of assistive technology outcome measurements
11 Understand the unique outcomes measurement needs of the field of assistive technology
12 Describe the primary outcome measurement tools developed for outcome assessment in assistive technology service delivery programs
Service delivery is the provision of hard and soft assistive technologies to the consumer. Chapter 1 delineated the components of the assistive technology industry, which has at its core the consumer and service delivery programs. This chapter describes the process by which the consumer obtains assistive technology devices and services. Chapter 2 described a model that is used as the basis for assistive technology assessment and intervention (human activity assistive technology [HAAT] model) and discussed the principles of assistive technology system design. This chapter builds on the HAAT model by delineating systematic methods of assessment and intervention that help the assistive technology provider (ATP) define the components of the model and integrate them into an effective assistive technology system for each individual consumer. The intrinsic enablers of the human and his or her relationship to the use of assistive technologies, as discussed in Chapter 3, provide the foundation for the discussion of evaluation of consumer skills in this chapter.
To effectively provide these services to the consumer, the ATP should be knowledgeable in the following areas:
1. The principles related to assessment and intervention and methods of gathering and interpreting information
2. The service delivery practices used to determine the consumer’s needs, evaluate his or her skills, recommend a system, and implement the system
3. The measurement of outcomes of the assistive technology system that indicate whether the identified goals have been achieved
4. The identification and attainment of funding for services and equipment
In this chapter and in Chapter 5 general principles and practices related to each of these areas are presented.
PRINCIPLES OF ASSISTIVE TECHNOLOGY ASSESSMENT AND INTERVENTION
The assistive technology intervention begins with an assessment of the consumer. Through this assessment, information about the consumer is gathered and analyzed so that appropriate assistive technologies (hard and soft) can be recommended and a plan for intervention developed. Information is gathered regarding the skills and abilities of the individual, what activities he or she would like to perform, and the contexts in which these activities will be performed. The assessment also yields information regarding the consumer’s ability to use assistive technologies. On the basis of the assessment results, a plan for intervention is developed. This plan includes implementation of the system, follow-up, and follow-along. Basic principles that underlie assessment and intervention in assistive technology service delivery are listed in Box 4-1.
Assistive Technology Assessment and Intervention Should Consider All Components of the HAAT Model: Human, Activity, Assistive Technology, and Context
Often assistive technology assessment focuses on the assistive technology only, which can lead to later rejection or abandonment of the technology. One way to reduce the probability of abandonment or misuse is to consider systematically all four parts of the HAAT model. Needs and goals are often defined by a careful consideration of the activities to be performed by the individual. However, it is rare that the activity will be performed in only one context, so it is important to identify the influence of the physical, sociocultural, and institutional elements in the contexts in which the activities will be performed (see Chapter 2). Thus the careful evaluation of the activities to be performed and the contextual factors under which that performance will occur are key to success. Once the goals have been identified, an assessment of the skills and abilities of the human operator (the consumer) must be identified. Only after consideration of these three components (activity, context, and human) can a clear picture emerge of the assistive technology requirements and characteristics. The assessment process must also include an assessment of the degree to which these characteristics match the consumer’s needs. Chances of success in implementation of an assistive technology system are enhanced by attention to all four parts of the HAAT model during the service delivery process.
Assistive Technology Intervention Is Enabling
The primary purpose of assistive technology intervention is not remediation or rehabilitation of an impairment but provision of hard and soft technologies that enable an individual with a disability to be functional in activities of daily living. This principle places the focus on functional outcomes. Through the application of the HAAT model we can develop goals for the assistive technology intervention, and these goals ultimately are used to measure the functional outcomes of the intervention. Approaching intervention from this perspective requires that the ATP determine the individual’s strengths and capitalize on them instead of focusing on deficits or impairments. For example, in functional activity of typing, in a rehabilitation approach the goal would be to improve hand and finger control sufficiently to allow for typing, with the intervention focusing on exercises and activities for the fingers and hands. From an assistive technology perspective, however, the objective becomes enabling the person to perform the functional activity of typing regardless of how it is done. The impairment in the hands and fingers that causes the disability is not necessarily addressed. The disability of being unable to type is what is addressed in the assistive technology approach. Through the use of assistive technology, alternative approaches to using the fingers for typing are considered, such as using a mouthstick, head pointer, or a speech recognition system instead of the hands.
This focus on function does not mean an individual’s potential for improvement is ignored. The parallel interventions model (Angelo and Smith, 1989; Smith, 1991) demonstrates how technology can be used to promote the dual objectives of enabling function and improving an individual’s skill level. In one track, assistive technologies are provided that are based on the consumer’s current skills and needs and that maximize function. Simultaneously, a second track provides intervention that focuses on improving skill level to minimize the reliance on technology. Some individuals who have a severe physical disability may never have had the opportunity to develop their motor skills, and training to develop these skills can take months or years (Cook, 1991). A common example is an individual whose evaluation shows that he or she is able to use the head to activate a single switch to make simple choices on a computer. With training and a period of experience in using this switch, head control may improve to the point where the individual can use a light beam positioned on the head to make direct choices with a dedicated communication device. The latter means of control would more quickly provide access to choices on a device and would be much less demanding cognitively.
Assistive Technology Assessment Is Continuous and Deliberate
Although assessment is typically considered a discrete event in the direct service delivery process, it is actually a continuous process. Assistive technology assessment entails a series of activities linked together and undertaken over time. The activities that occur and the decisions that are made during the intervention are deliberate rather than haphazard. Information is gathered and decisions are made from the moment of the initial intake referral through follow-along.
The ATP re-evaluates progress toward the goals of the intervention plan and makes necessary revisions. For example, during training, observation may reveal that the consumer can access the control interface more effectively if it is positioned at an angle instead of flat. As decisions are implemented, their influence is continuously assessed and revisions are made to the intervention. The ideas of client-centered practice (Canadian Association of Occupational Therapists, 2002) highlight the importance of involving the client at all stages of assessment, from the initial framing of the activities in which the client wishes to engage to the recommendation of an assistive technology system. The client refers to the individual and others in the environment such as family and caregivers (Canadian Association of Occupational Therapists, 2002). Assessment continues not only while the consumer is actively involved in the service delivery process but also potentially throughout the consumer’s life. Because many individuals have life-long disabilities, they will be in need of assistive technology throughout their lives. It is important not only to recommend assistive technology that enables the individual today but also to predict the technology that will be necessary to enable the individual in the future. The components of the HAAT model change over each individual’s lifetime. Changes may occur in the individual’s skills and abilities, life roles, and goals; the capabilities of technology; and the context in which the assistive technologies are used. By using the HAAT model as a framework, the ATP can predict some of these changes and plan for the consumer’s future technology needs.
Assistive Technology Assessment and Intervention Require Collaboration and a Consumer-Centered Approach
Given the nature of assistive technology and its influence on the consumer’s activities of daily living, it is essential that the assessment and intervention be a collaborative process. McNaughton (1993) defines a collaborator as “one who works with another toward a common goal” (p. 8). Furthermore, she states that collaboration requires that (1) all participants be equal partners, (2) a problem-solving attitude be shared by all participants, (3) there be mutual respect for each other’s knowledge and the contributions each person can make as opposed to the titles he or she holds, and (4) each participant have available the information necessary to carry out his or her role (McNaughton, 1993).
Frequently, assistive technology services are provided through consultation, in which the ATP is called into a situation on a limited basis to specifically address the assistive technology needs of the consumer. There may be several people already involved with the consumer, including family members, teachers, vocational counselors, employers, therapists, and representatives from the funding source. The assistive technology assessment and intervention is more successful when these significant others are identified and involved at the beginning of the process.
There is a delicate balance between the opinion and “expertise” of the ATP (based on technical knowledge and experience with a variety of people) and the opinion and “expertise” of the consumer and family relating to the specific needs and goals of the person. The role of the ATP is to educate the consumer of the choices available so that the consumer can make decisions related to the assistive technology in an informed manner. The challenge for the ATP is to do this without unduly influencing the client’s choice. The value of this approach is that the consumer and the ATP inform each other throughout the process and develop a shared responsibility for the outcome. This approach has been referred to as the “educational model” of intervention (as opposed to the “expert” and “consumer-driven” models, which take one extreme position or the other). Lysack and Kaufert (1999) describe this process and its benefits.
The ATP should initiate the collaborative process by identifying significant others as a part of the intake referral phase. For example, Jerry, who has a developmental disability, lives in a small group home. During the intake, the ATP discovers there are several key people who need to be involved in the assistive technology intervention for Jerry: staff at his home, staff at the day program he attends, an occupational therapist who consults with his residential program, his caseworker at the department of developmental services, and his parents, who live out of town. Each of these individuals is invited to participate in the initial assessment and decision-making process. Different participants will be working with the consumer to accomplish different goals. Communication among the collaborators regarding their respective goals for the consumer is critical. It is important to identify the ways in which the goals of the assistive technology intervention can be accomplished without interfering with other goals. Sometimes compromises need to be reached. For example, two professionals working with the consumer may be focusing on different goals, and compromises may need to be made by all parties in working toward these interdependent goals. One therapist may be working with a child on improving the strength in his or her neck muscles to improve head control, whereas the ATP’s goal may be to support and position the head in an upright position to prevent deformity and allow optimal position for functional activities. The success of the assistive technology system depends on coordination and teamwork among all the individuals involved with the consumer.
Beukleman and Mirenda (1998) discuss the importance of building consensus among the user, family members, and other team members. Negative consequences, such as a lack of vital information for intervention, lack of “ownership” of the intervention resulting in poor follow-through with the recommendations, and distrust of the service provider, may result if the process of consensus building is not begun during the initial assessment. Initiating this process early helps to avoid problems in the future with regard to the acceptance and use of a device.
Assistive Technology Assessment and Intervention Require an Understanding of How to Gather and Interpret Data
It is both possible and desirable to measure human performance, and much of what is described in this chapter is directed toward that end. In assistive technology service delivery we need to be careful that we know what we are measuring. In some cases, as in determining the effectiveness of our service delivery process and outcomes, we want to measure the performance of the entire assistive technology system. Because this system has been defined to be the four components of the HAAT model (human, activity, context, and assistive technology), measurements and outcomes that apply to the entire system must be developed. In other cases (e.g., during an initial assessment) human performance rather than system performance needs to be measured. Measuring human performance can be general or task specific (Sprigle and Abdelhamied, 1998). An individual’s general abilities are measured when separate components of the sensory, perceptual, physical, and cognitive systems, such as range of motion, sensation, strength, tone, or memory, are evaluated. Task-specific measurement involves the evaluation of the individual’s functional skills. The ability of the person to complete a functional task, such as entering text into a computer document, requires a level of skill that combines physical, sensory, and cognitive abilities. In this case clear objectives must be established for each task, a clinical standard to be applied must be developed, and then measures that evaluate the performance must be developed.
In this section we focus on the principles associated with measurement in assistive technology service delivery. These include the purposes, types, standards, and methods of measurement.
Quantitative and Qualitative Measurement.
Information gathered by the ATP throughout the assistive technology intervention can be by either quantitative measurement or qualitative measurement. The philosophies of qualitative measures and quantitative measures are quite different. Quantitative measures assign a number to an attribute, trait, or characteristic (Nunnally and Bernstein, 1994). The assumption of quantitative measures is that the construct of interest can be measured in some meaningful way. For example, a test can be constructed that measures the joint range of motion (the construct) that an individual has available to control a computer access device. Joint range is expressed as degrees of motion and a common understanding exists regarding what is meant when a specific joint range of motion is described. Here the construct can be assigned a number that is meaningful to individuals using and interpreting the test. Alternatively, a test can be constructed that intends to measure boredom. It is possible to develop a scale and have individuals rate their boredom on a four-point scale (for example). But what does a score of 4 mean on such a scale? We can assign a number on a scale but it is difficult to interpret the meaning of that number.
Qualitative assessments assume that each individual has a different experience and that it is important to provide the opportunity to capture that experience. There is no attempt to measure a particular construct. Rather, the purpose is to describe and understand the user’s experience with the technology. Qualitative assessments may include observation, either directly or by videotape or interview with the client and others. Qualitative assessments often capture those experiences that cannot be directly quantified or for which quantification holds little meaning. They provide the client with the opportunity to identify issues, experiences, or goals that may not be previously identified on a quantitative measure.
Both qualitative and quantitative assessment formats are important in the AT assessment process and for evaluation of the outcomes of AT use. Quantitative measures allow comparison of experiences of a large number of individuals and a well-constructed instrument is essential in building evidence to support the efficacy of AT use. Qualitative methods provide a rich description of the experiences of AT use, which may not be readily apparent from the use of quantitative instruments alone. Together these methods can provide strong support for AT use, both on an individual and collective basis.
Norm-Referenced and Criterion-Referenced Measurements.
Two commonly used standards are available for measuring performance (for both the human and the total system): norm referenced and criterion referenced. In norm-referenced measurements the performance of the individual or system is ranked according to a sample of scores others have achieved on the task. Norm-referenced measures usually produce a percentile rank, a standardized score, or a grade equivalent that indicates where the individual stands relative to others in the representative sample (Witt and Cavell, 1986). When selecting a norm-referenced test for use, it is important to review how the norms were developed. Norms need to be relevant to the population for which the instrument is being used. They need to be recent and representative (Wiersma and Jurs, 1990). In other words, the characteristics of the sample used to develop the norms must be similar to those of the client group for which the assessment is being used. The items that form the instrument need to be relevant to the client group. For example, assessing visual-perceptual skills by using blocks is not relevant for most adults. Similarly, use of outdated questions or materials will not give an accurate picture of the client’s abilities. For example, testing keyboarding skills on a typewriter will give some information on keyboarding skills but does not cover the full range of skills required to use a computer (Miller Polgar, 2003). An alternative way to assess human or system performance is to rate the performance according to a specified criterion or level of mastery, which is referred to as criterion-referenced measurement, and the person’s own skill level in using the system is used as the standard. As an example of this approach, Jagacinski and Monk (1985) evaluated joystick and head pointer use by young adult nondisabled subjects. They found that skill in using these devices is acquired with some difficulty over many trials. The criterion used was whether the individual’s performance (time to move to target) did not change by more than 3% over a period of 4 consecutive days (Figure 4-1). In Figure 4-1, the horizontal axis represents the elapsed practice time and the vertical axis represents how quickly the person has been able to use the joystick or head pointer to move to a target. The horizontal dotted line is the final level of performance and serves as the criterion of performance. Using this criterion, they found that joystick use required 6 to 18 days and head pointer use required 7 to 29 days of practice to reach the criterion level of performance.
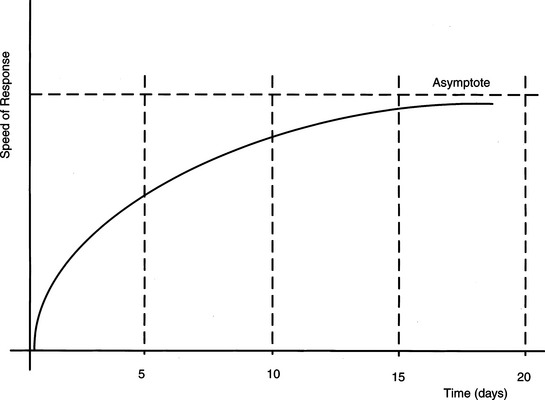
Figure 4-1 Speed of response to reach a target as a function of days of training. The horizontal axis is days of training. The vertical axis represents the speed to reach the target. The dotted horizontal line is the speed as performance levels off. This is used as the criterion for performance.
When the criterion-referenced approach to measurement is used, two desirable goals are accomplished. First, the assessment of progress is based on the person’s unique set of skills and there is no attempt to relate this performance to a normalized standard. In this example, the two alternative ways of accomplishing the same task (joystick and head pointer) are compared to determine which method is likely to result in a higher skill level. The second goal is accomplished by using the person’s own performance as a standard for measuring progress. Goal attainment scaling (King et al, 1999) is one standardized process of developing criteria that are specific to the client and task that are then applied to evaluate outcomes.
Methods for Gathering and Interpreting Information.
There are several methods used to gather and interpret quantitative and qualitative information about the consumer: (1) collection of the initial database, (2) interview procedures, (3) clinical assessment, and (4) formal assessment procedures (Dunn, 1991). Often, more than one method is used to gather information about the same aspect of a consumer’s skills, the context, the activity, or the use of assistive technology. For example, information on an individual’s hand function can be collected through each of these methods. The use of multiple sources of information is illustrated by Sam, a 22-year-old man with quadriplegia secondary to a complete C6 lesion of the spinal cord, who is being evaluated for his ability to access a computer.
Information collected for the initial database may include the reason for referral, medical diagnosis, and educational and vocational background information. This information is collected during the referral and intake phase of the service delivery process; its purpose is to provide preliminary data for planning the assessment. Sam’s medical diagnosis is complete quadriplegia at the C6 level. If we refer to a text describing the effects of spinal cord injury at the C6 level on arm function (see Table 3-8), we expect Sam to have scapular movements, shoulder flexion, elbow flexion, and wrist extension but to lack finger flexion and extension. Most medical histories do not provide information on the consumer’s assets and functional abilities. In some cases we may unintentionally limit the consumer’s potential if we fail to look beyond the expectations we have acquired on the basis of the medical diagnosis. As Christiansen (1991) points out, a medical diagnosis may provide guidelines for the assessment and expectations regarding the nature of the consumer’s impairments, but it is inadequate for planning intervention.
The interview, another way to collect information, can occur at different points in the service delivery process. Typically, an initial interview takes place during the needs identification phase as a means of gathering information regarding the consumer and his or her needs. It is important that the consumer, family members, rehabilitation or education professionals, and other care providers be interviewed. In Sam’s case, during the initial interview his goals and his particular needs related to using a computer are determined. The tasks with which he has difficulty performing are identified. Finding out whether Sam currently uses any adaptive equipment, or has in the past, to complete functional tasks also provides valuable information about his hand function. For example, Sam is able to sign his name by using an adapted splint to assist with grasping the pen, but it is difficult for him to write and he tires quickly. This difficulty has led him to pursue the use of a computer to facilitate taking notes at school and completing homework assignments. Another stage in which the interview is important is follow-up. At this stage, interviewing the consumer or caregivers provides valuable information on whether the device is being used and how. It is important that the ATP develop the ability to conduct interviews so that useful information is gathered.
Formal assessment procedures are administered in a prescribed way and have set methods of scoring and interpretation. Therefore, they can be duplicated and analyzed. Through formal assessment procedures, Sam’s arm and hand abilities can be quantified. For example, Sam’s muscle strength in his upper extremities can be evaluated by performing a manual muscle test (Daniels and Worthingham, 1986). Formal assessments should use standardized tests whenever possible. The ATP who uses such tests should evaluate the instrument development and psychometric properties to determine whether they are applicable to the client population and that the interpretation of the scores will be meaningful. Frameworks exist that guide a clinician’s critique of an evaluation (e.g., Miller Polgar and Barlow, 2002). These frameworks identify aspects of test construction, psychometrics, and clinical utility that are important considerations of an instrument’s usefulness in a given situation. Clinical assessment techniques involve skilled observation of the consumer and are used throughout the assessment and intervention process. The ATP may structure these techniques so that a series of steps is followed to determine specific skills or they may be intentionally left unstructured to see what takes place. Observation can be done during a simulated task in a clinic setting or in a context familiar to the consumer (e.g., classroom or workplace). Through skilled observation during the structured task of a series of typing tests, it may be observed that Sam’s typing speed and accuracy improve when he stabilizes himself with his left forearm and types with his right hand. Observation complements information obtained from standardized tests.
All these considerations lead to one very important conclusion: In the application of assistive technology systems, success is largely the result of the combined efforts of knowledgeable and competent clinicians who, in collaboration with informed consumers and caregivers, make decisions on the basis of both specific knowledge and experience. The complexity of the total system, including the diversity of the individual and of disabilities, technologies, and contexts of use, dictates that, when an assistive technology device is designed, best practice is often a matter of using clinical reasoning combined with results of established assessments.
OVERVIEW OF SERVICE DELIVERY IN ASSISTIVE TECHNOLOGY
Regardless of the type of service delivery model (see Chapter 1), there is a basic process by which delivery of services to the consumer occurs. Figure 4-2 illustrates the steps involved in this intervention process. The first step is referral and intake. At this point, the consumer, or someone close to him or her, has identified a need for which assistive technology intervention may be indicated and contacts an ATP to make a referral. The service provider gathers basic information and determines whether there is a match between the type of services he or she provides and the identified needs of the consumer. Funding for the services to be provided is also identified and secured at this stage. Once the criteria for intake have been met, the evaluation phase begins. A more detailed specification of the consumer’s assistive technology needs is the first step in this phase, which is referred to as needs identification. After a thorough identification of the consumer’s needs, the consumer’s sensory, physical, and cognitive skills are evaluated. Technologies that match the needs and skills of the consumer are identified, and a trial evaluation of these technologies takes place. The evaluation results are summarized and recommendations for technologies are made on the basis of consensus among those involved. These findings are summarized in a written report, which is used to justify funding for the purchase of the assistive technology system.
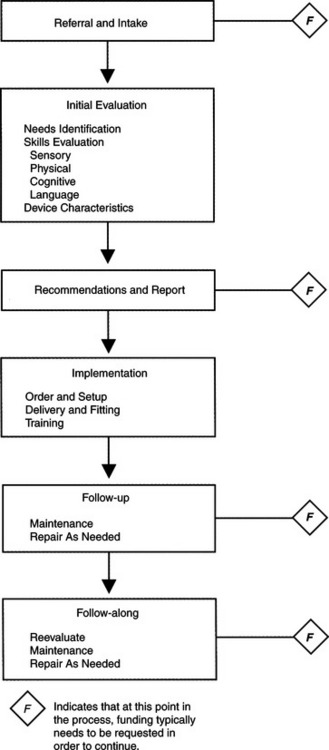
When funding is secured, the consumer proceeds with the intervention in the implementation phase. At this phase, the equipment that has been recommended is ordered, modified, and fabricated as necessary, set up, and delivered to the consumer. Initial training on the basic operation of the device and continuing training of strategies for using the device also take place during this phase.
Once the device has been delivered and training has been completed, whether the system as a whole is functioning effectively must be determined. This step normally occurs during the follow-up phase, in which it is determined whether the consumer is satisfied with the system and whether the goals that have been identified are being met. The follow-up phase actually closes the loop by putting in place a mechanism by which regular contact is made with the consumer to see whether further assistive technology services are indicated. When further AT services are required, the referral, intake, and implementation phases are repeated. Building this final phase into the service delivery process ensures that the consumer’s needs are considered throughout the life span. A more in-depth look at each of these steps follows.
Referral and Intake
The purpose of the referral and intake phase is to (1) gather preliminary information on the consumer, (2) determine whether there is a match between the needs of the consumer and the services that can be provided by the ATP, and (3) tentatively identify services to be provided (Gaster, 1992).
The consumer, or the person making the referral on the consumer’s behalf, recognizes a need for assistive technology services or devices, which triggers the referral to the ATP. These identified needs are called criteria for service, and they define the objectives for the intervention. A third party involved in the referral, such as a state vocational rehabilitation agency, will have a set of policies and procedures that governs who is eligible to seek assistive technology intervention and what devices and services they cover. Langton and Hughes (1992) describe a framework called “tech points” for inclusion of assistive technology in the vocational rehabilitation case management process. They identify key points during the consumer’s vocational rehabilitation at which technology should be considered. This approach is valuable because it includes a mechanism through which the vocational case manager can monitor whether a criterion for assistive technology services exists for individuals in his or her caseload. Depending on the policies of the ATP, referrals are accepted from a variety of sources. These sources include the consumer, a family member or care provider, a rehabilitation or educational professional, or a physician. At this time, information regarding the consumer’s background and perceived assistive technology needs is gathered for the initial database. This information includes personal data (e.g., age, place of residence), medical diagnosis and health information, and educational or vocational background. Information related to the individual’s medical diagnosis and health information that may guide the assessment includes whether the condition is expected to remain stable, improve, or decline. The appropriateness of the referral is viewed from the perspective of both the ATP and the referral or funding source. When exchanging information about the consumer’s needs and the services provided by the ATP, each party can determine whether there is a match. One outcome is that the needs of the consumer do not match the services provided by the ATP. For the consumer’s benefit, this mismatch should be acknowledged and the consumer referred to another source that can more appropriately address his or her needs. The assistive technology provider should have, within the organization’s mission statement, a policy that establishes what services are provided and who is eligible to receive services. For example, some assistive technology service providers specialize in certain disabilities (e.g., visual impairment), and others focus on specific technologies (e.g., seating technologies). Professional codes of ethics and standards of practice (see Chapter 1) require that ATPs practice within their specialization and not try to provide services outside of this realm.
The other outcome is that there is a match between the needs of the consumer and the services provided by the ATP. In this case, funding is sought and plans are made to move forward with the initial evaluation, starting with a thorough identification of the consumer’s needs. From the information provided, the ATP also determines the level of service that would be most beneficial to the consumer. There are a number of scenarios. First is the individual who has never used or been evaluated for assistive technologies, which could be an individual who is newly disabled or someone with a long-standing disability. An individual with a long-standing disability who may not have previously been a candidate for assistive technology services may now be able to access assistive devices because of recent advances in technologies. In this situation an in-depth assessment is warranted. Referrals may also be received from consumers who have used technology for some time and would like to evaluate current commercially available technologies. If this person’s functional status has remained stable, it may not be necessary to conduct a complete evaluation. In some cases the assistive technology is not working or has been abandoned by the consumer and he is seeking a referral to see if modifications to the system can aid in making it more functional. Sometimes the consumer may only require further training or re-evaluation of how he or she is using the current system to see whether training in new strategies would be beneficial. Similarly, there may be a new care provider who needs training or technical assistance.
Initial Evaluation
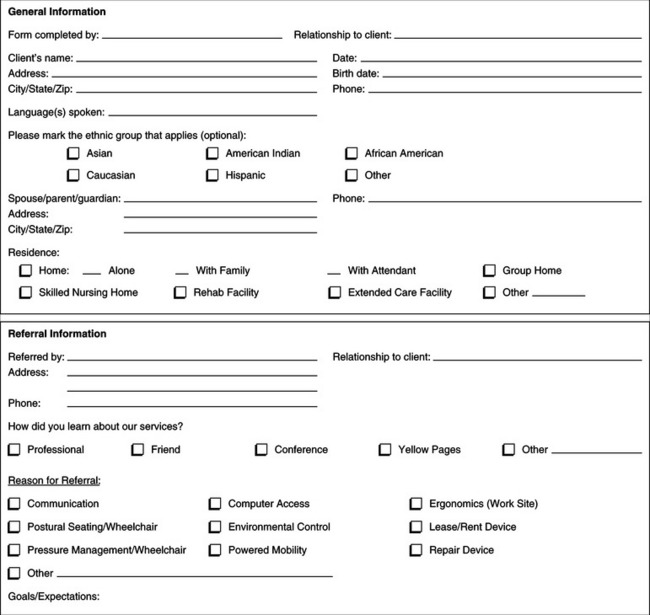
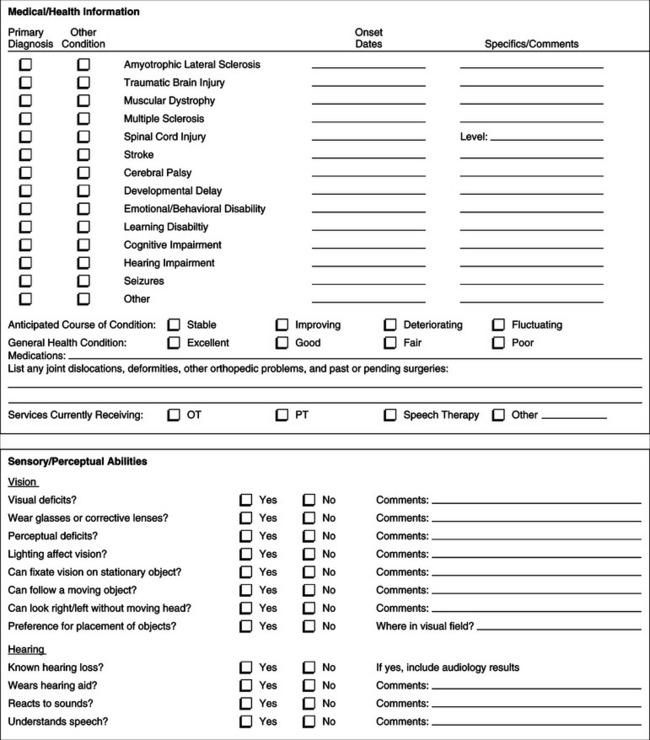
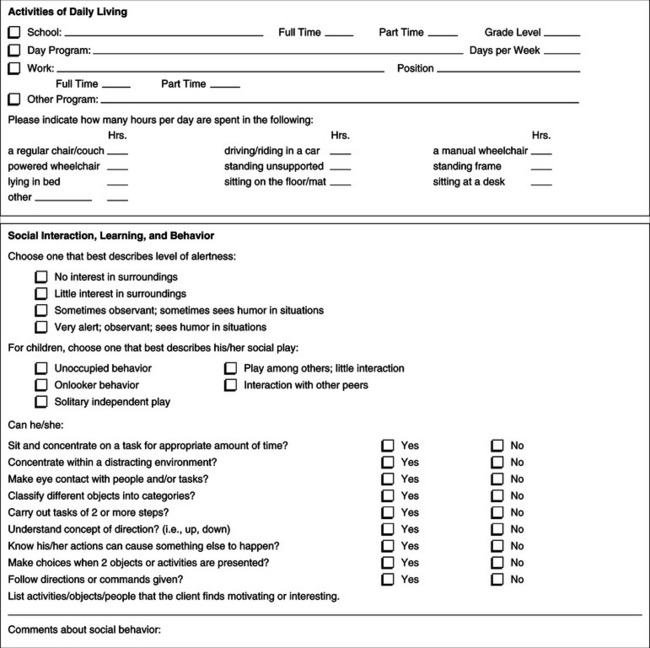
Through a systematic evaluation, the ATP gathers information and facilitates decisions related to eventual device use. Because of the cost of the assistive technology to the consumer (or third-party funding source), it is essential that the ATP be able to assist the consumer in making informed decisions in the selection of a device. Current knowledge of the available technology and use of a systematic process facilitate the ATP’s ability to make such decisions. This section focuses on the type of information gathered and the procedures used during the evaluation. Examples of assessment forms that capture most of the data discussed here are included in Appendices 4-1A and 4-1B.
Needs Identification
Through the needs identification process, the individual’s needs and goals, which provide the basis for the assistive technology intervention, are determined. Identifying the needs of the consumer is the most critical component of the service delivery process and it is completed at the onset of evaluation. The information collected during needs identification is the cornerstone for measuring the effectiveness of the final outcome. Therefore, it is important to take this step seriously and ensure that there is a consensus among those involved as to the nature and scope of the problem to be addressed by the assistive technology intervention and the goals identified to target these problem areas.
Information gathered during needs identification is also used by the ATP to justify purchase of services and equipment. Third-party payers who fund services and equipment want to know what the problem or need is and how the equipment is going to address the need. Finally, the needs identification process results in the development of a plan for completing the remainder of the evaluation, which includes composition of the evaluation team, determination of needed evaluation tools and devices, and identification of further information required (either through evaluation of the consumer or by request from outside sources).
Figure 4-3 provides a model for gathering and analyzing information regarding the person’s life roles, performance areas, related activities, and tasks. The consumer’s life role at the time influences his or her needs and goals. Is the individual a child or an adult? What are his or her life roles? Life roles include student, parent, employee, volunteer, and so on. It is important to note that, as the individual’s life roles change over time, so may the technology that is needed. Changing life roles, and therefore technology needs, is one of the reasons that consumers may return after a time to be re-evaluated.
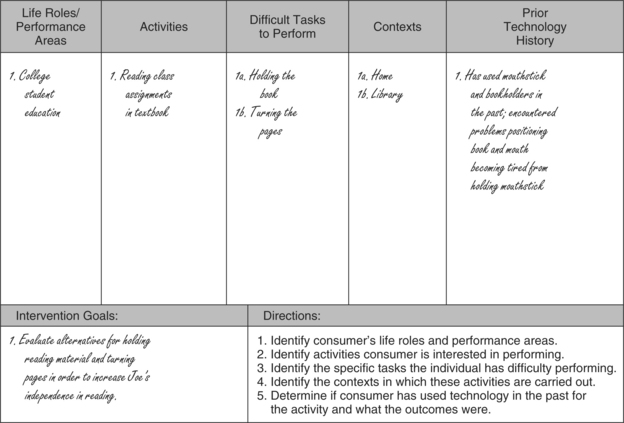
In relation to the consumer’s life roles, there are performance areas (self-care, work, school, play, leisure) in which activities are accomplished. Identifying these performance areas helps the ATP to define the activities for which the consumer needs assistance. For example, play (performance area) is very important for a young child (life role), and a child with a disability may be precluded from manipulating toys (activity). Identifying the context in which the consumer will perform these activities is also critical. In Figure 4-3 we show needs identification for a student who is attending college. A major activity for this student is reading the material assigned from the textbook. The major part of this activity will take place at home for him, but he will also need to do some reading at school.
A task analysis of the skills required to complete the activity is conducted. The consumer and others identify to the best of their ability which tasks the consumer can likely perform himself or herself and which tasks may need to be assisted with technology. This information may be unknown in some cases, and the evaluation can determine which tasks the individual needs assistance with. In our example the activity of reading is broken down further into small tasks. If the student has a physical inability to hold the book and turn the pages, resulting in the need for manipulation of reading material, we identify this inability as a need in the third column. Another student who may have difficulty with the activity of reading because of a visual impairment will require different technologies to meet this need.
The consumer’s prior history with technology should also be discussed as part of the needs identification. Useful information can be gathered from the consumer’s previous success or failure with using assistive technology. Has he or she had experience in using technology before, and if so, what technology was used and was the experience successful? If not, why? In our example the student had attempted to turn the pages of different books with the use of a mouthstick, which turned out to be unsuccessful. It is important to identify and discuss reasons why the mouthstick did not work for the individual. Perhaps the mouthstick was cumbersome and uncomfortable to use for any extended period, or perhaps the individual could physically perform the task with the mouthstick but did not like the esthetics of it.
Beukelman and Mirenda (1998) discuss the need to identify actual or potential “opportunity barriers” and “access barriers” for the consumer. Although their model specifically targets consumers with augmentative communication needs, it also holds true for other areas of assistive technology. Opportunity barriers are imposed by individuals or situations that are not under the consumer’s control. Generally the provision of assistive technology does not result in the elimination of these barriers. Beukelman and Mirenda (1998) identify five types of opportunity barriers: policy barriers, practice barriers, attitude barriers, knowledge barriers, and skill barriers. Policy barriers are legislative, regulative, or agency policies that govern situations in which consumers find themselves. For example, there are regulations in some school districts that restrict the use of school-purchased assistive technology to use in the school, preventing it from being taken home. Practice barriers refer to routine activities that are not dictated by policy but that constrain the use of assistive technologies. If the school’s policy does not require that the device stay in the school, but the local teacher or principal has the practice of keeping the devices in the school, the result is the same as if it were a policy. Attitude, knowledge, and skill barriers all apply to those individuals with whom the consumer interacts and on whom the effective use of the device depends. If the consumer’s job supervisor has a negative attitude regarding the use of automatic speech recognition because it is distracting to other workers, it is an attitude barrier that prevents the consumer’s participation in that job. Alternatively, the supervisor may have insufficient knowledge or skill regarding automatic speech recognition to ensure that it is effectively installed and made available to the consumer. The approach taken by the ATP to overcome opportunity barriers is very different depending on the type of barrier. It may involve training (for skills or knowledge), lobbying (for policy, attitude, or practice barriers), or a combination of the two.
Access barriers are barriers related to the abilities, attitudes, and resource limitations of the consumer or his or her support system (Beukelmen and Mirenda, 1998). During the needs assessment before an augmentative communication evaluation, for example, all the consumer’s current ways of communicating can be identified. Known constraints related to user and family preferences and the attitudes of communication partners are other access barriers that should be identified. A potential barrier to accessing technology, one commonly seen during augmentative communication assessments, is resistance on the part of parents to pursue an augmentative communication device because they are worried that the use of such a device will inhibit the child’s development of natural speech. As discussed later in this chapter, the ability to find funding for assistive technology systems and services may also pose a barrier. Identifying potential and actual barriers (both opportunity and access) during needs assessment will help the ATP formulate strategies for assessment and intervention.
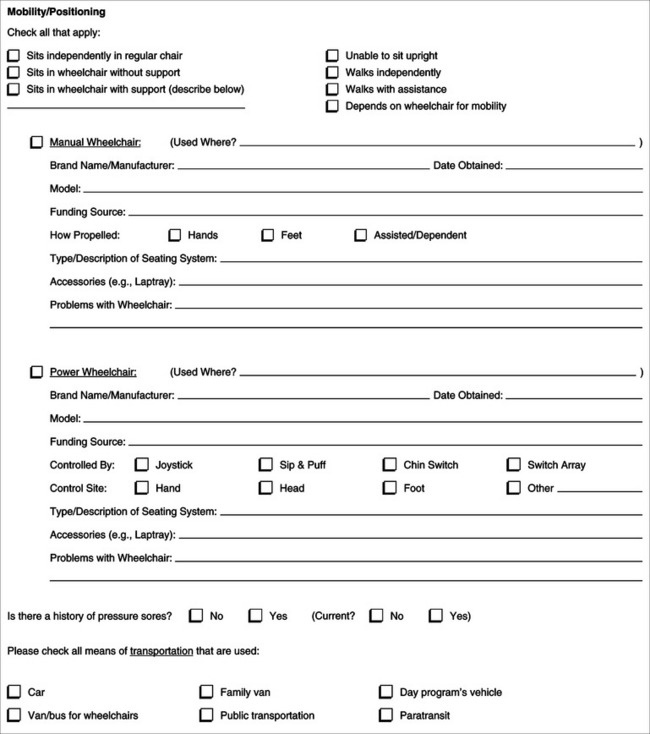
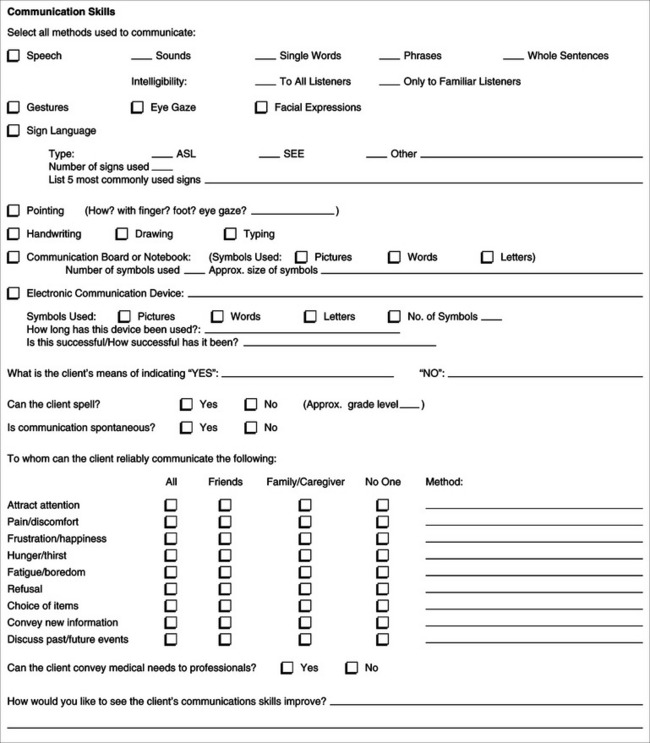
The information for the needs assessment can be derived from an interview or through a written questionnaire completed by the consumer or his representative. In Appendix 4-1A we provide one example of a questionnaire. Instruments such as the Matching Person and Technology Assessments (Scherer, 1998) can also be used by the ATP to identify the areas of the individual’s needs and his or her predisposition to use assistive technology. If the information is gathered through a written questionnaire before the ATP actually meets the consumer, it should be reviewed at the time of the first meeting with the consumer. The purpose of reviewing this material at the first meeting is to ensure that all the necessary information has been provided and to analyze the information to develop the goals. The total team should also be present at this meeting, and everyone’s input regarding the needs and goals of the consumer can be discussed and a consensus reached.
Skills Evaluation: Sensory
As discussed in Chapter 3, auditory, tactile, and visual senses all play a role in the use of assistive technology. In recommending assistive technologies, the ATP needs to be aware of the consumer’s sensory abilities and limitations. The ATP is not expected to diagnose sensory impairments such as hearing loss or visual impairments. Consumers who have sensory impairments have usually undergone evaluation by a specialist (e.g., audiologist, ophthalmologist, or optometrist) and are able to provide the ATP with a report that details the degree of impairment. If this testing has not occurred, the ATP should make a referral to an appropriate source before proceeding.
The ATP needs to be able to identify sensory functions that are available. If the primary disability is sensory, an alternative sensory pathway may need to be used, so the ATP needs to know what the consumer’s sensory capabilities are. For example, in the case of a consumer who is blind and who needs to read, the ATP must evaluate tactile and auditory skills that can substitute for vision during reading (see Chapter 8). In other cases a consumer may have a sensory disability resulting from either a physical or a cognitive limitation. For example, if a consumer is hard of hearing, the ATP needs to know how this will affect interaction with technology. This includes everything from hearing warning beeps when a computer error is made to understanding voice synthesis on a communication device.
Evaluation of Functional Vision.
The most critical visual skills needed for assistive technology use are sufficient acuity to see the symbols used in the system of choice or to identify small objects in the environment; adequate visual field to allow input of information from a display (e.g., the keyboard or the monitor) or the environment; and sufficient visual tracking ability (e.g., for reading or tracking a moving cursor). During the initial interview, known visual problems should have been identified, but a visual screening may also identify previously undetected deficits. The ATP can evaluate the effect of these deficits related to the use of technologies.
Identifying any visual field deficits a consumer may have is extremely important in the application of assistive technology. Visual field is commonly assessed by having the consumer look straight ahead and then indicate when he or she first sees a moving stimulus appear in the peripheral visual field. The stimulus is held approximately 18 inches away and moved in an arc toward the consumer’s midline. This testing is typically done for the right and left peripheral fields and the upper and lower fields. Peripheral field vision is considered intact if the stimulus is seen when it is parallel to the person’s cheek and impaired if the individual does not indicate that he or she sees the object as it approaches the center of his or her face (Dunn, 1991).
In some cases it is difficult to identify the effects of visual field limitations on assistive technology use. For example, individuals with a visual field deficit may make errors in typing because they do not see the whole keyboard. If the ATP is not careful, this performance may be interpreted as a physical limitation instead of a visual field deficit. If motor limitations were assumed, the keys may have been made larger so that the consumer could hit them more easily, an expensive and unnecessary step.
Visual tracking is the ability to follow a moving object. This skill is necessary for many assistive technology tasks, such as following a moving cursor on a screen, following the rotation of a plate with food in a feeder, or following objects in the environment while driving a wheelchair. Visual tracking is usually tested by having the consumer follow a moving object with the eyes. The object is held approximately 18 inches in front of the consumer and moved horizontally, vertically, and diagonally. The ATP notes whether the two eyes track together, whether the eye pursuits are smooth or jerky, whether there is a delay in the tracking, and whether the eyes can track without head movement.
Limitations in visual tracking ability may significantly reduce the options for specifying and designing an assistive technology system. In particular, these results have implications for the use of scanning augmentative communication systems in which the cursor moves left, right, up, and down (four-way directional scanning). It may be that an individual with a disability is able to track more easily to the right and down than to the left and up. In this case, two-way directional scanning, right and down, is preferable to using all four directions. When the cursor gets to the extreme right of the display, it automatically wraps around and begins from the left side again. Similarly, when it gets to the bottom, it wraps around to the top.
Visual scanning differs from visual tracking in that the object does not move; instead the eyes are moved to view different parts of a scene to find a desired object or location. This skill is used, for example, to locate obstacles during mobility and to scan a keyboard to find a specific key. The eye movements used in visual scanning are the same as those used in tracking. We often assess this capability by presenting arrays of pictures, symbols, words, or letters and asking the consumer to choose one item from the array. In Chapter 3 we described visual accommodation as the ability of the eyes to adjust to objects near and far. This component is impaired in many persons with disabilities, and it is important to be aware of possible accommodative insufficiency during the assessment process. A visual accommodation impairment may be observed by changing the visual focus between a monitor and keyboard. If the monitor and keyboard are far apart, the person may have more difficulty than if these objects are visually close. An individual’s ability to see objects (visual acuity) is affected by (1) the size of the object, (2) the contrast between the object and the background, and (3) the spacing between the object and surrounding background objects. These three considerations apply to symbols as well as to objects. For testing of visual acuity, actual objects, photographs, line drawings, orthographic symbols, letters, and words are used. It is helpful to have a set of materials that includes objects of 3 to 4 inches high; large letters, pictures, and symbols 1 to 2 inches high; and letters and words down to the size of standard typewritten letters (an eighth of an inch) (Cook, 1988). Information gathered from the initial interview can guide the ATP as to the type and size of symbol to start with. The goal is to find the smallest size of symbol that can be seen well by the consumer and that results in accurate selections, which are tested by presenting two items of the selected size and symbol type at a time to the consumer. The individual is asked to identify one of the two items using the manner in which he or she usually indicates a choice (e.g., eye gaze, pointing, yes/no). Three trials of each size and symbol are completed before proceeding to the next smaller size, until the individual is no longer able to identify the item successfully. It is desirable for the consumer to be able to see a small size for a number of reasons. First, the smaller the size, the larger a given array of symbols can be. Second, this allows greater options in hardware and software, including standard keyboards and software that have been developed for the nondisabled population.
If the consumer is able to read but appears to have difficulty seeing words, the effects of various foreground-background combinations (to improve contrast) and letter spacing can be assessed by using computer displays and software designed for this purpose (see Chapter 7). For example, most word processing software allows alteration in the background and foreground (letters) colors. Special software designed for persons with visual impairments also adds size variation to these capabilities. For computer applications, these features can improve performance.
We can improve visual performance by using enlarged graphics or text and by designing control panels with dark backgrounds and light lettering or controls. Identifying switches or keys with colors more distinguishable to the individual may be helpful. Switches can be light colored and placed on a dark background to improve recognition, and language board arrays can have bold dark letters or pictures on a white background, or vice versa. Likewise, video screens and the input array need to be carefully planned so that the amount of information presented is not cluttered.
Evaluation of Visual Perception.
As discussed in Chapter 3, visual perception is the process of giving meaning to visual information. Visual perceptual skills that need to be considered during assessment include depth perception, spatial relationships, form recognition or constancy, and figure-ground discrimination. Visual perception is an important consideration when considering the client’s ability to interpret information presented in a visual display or to safely navigate a mobility device in the environment. Formal testing of the consumer’s visual perception may have been completed before the assistive technology assessment, and results of this evaluation can be gathered during the initial interview. It is necessary to observe the consumer during functional tasks and note any apparent perceptual problems. If there is still some concern regarding the exact nature of the problems, a formal evaluation such as the Motor Free Visual Perception Test (Colarusso and Hammill, 1972) can be used.
Evaluation of Tactile Function.
There are three particular circumstances in which attention needs to be paid to the evaluation of tactile sensation. These occur during seating and positioning assessments, when evaluating tactile input for the use of control interfaces, and when considering the use of tactile alternatives to vision or hearing.
Somatosensory input is necessary for detecting forces or pressures exerted on the surface of the skin. Individuals who lack sensation may sit for prolonged periods without shifting position, which can result in skin breakdown. The ATP needs to be aware of an individual’s sensory status in these situations and be able to evaluate pressure on the sitting surface. Dunn (1991) presents a specific testing protocol for tactile response. Additionally, observation and monitoring of the skin surface is necessary. Tactile functions that are included in a somatosensory protocol include one-two point discrimination, perception of light touch versus deep pressure, perception of temperature, joint position sense, and localization of tactile stimulation. Somatosensory function is responsible for providing information regarding the location of a control interface, the movements required to activate it, and whether it is successfully activated. Lack of ability to receive appropriate sensory input (e.g., because of Hansen’s disease, nerve injuries, or sensory loss from aging) can severely limit the effective use of control interfaces. The initial interview generally reveals whether somatosensory deficits are present. During functional tasks, the ATP’s skilled observation can identify limitations caused by sensory deficits. Dunn’s (1991) sensory testing protocol can also be applied in this situation. In the case of decreased tactile sensation, the control interface needs to provide adequate feedback so that it compensates for the loss of sensory function (see Chapter 7). When visual or auditory function is inadequate for the input of information, we often use tactile substitutes (see Chapters 8 and 9). To determine whether this alternative sensory input is viable for an individual, tactile function must be evaluated. In particular, the skin response on one or more fingers is evaluated by using two-point discrimination and similar tests. This evaluation is necessary because certain diseases (e.g., diabetes) that result in loss of vision also cause reduced tactile sensation.
Evaluation of Auditory Function.
The ATP, through the initial interview and observation during functional tasks, should be aware of any significant auditory impairments that may affect device use. In cases of suspected hearing loss, a formal evaluation by an audiologist should be requested. Basic information sought by the ATP should include whether the individual responds to auditory stimuli, is distracted by some or all sounds, recognizes specific auditory stimuli (e.g., someone calling his or her name), and responds appropriately to auditory stimuli (Dunn, 1991). For example, many augmentative communication devices emit a beep when a selection is made. For some individuals, this cueing is helpful; however, for others the beep may produce a startle reflex that interferes with the succeeding motor movement. The individual may eventually habituate to the beep, but it is important to consider a device that has the option of disabling it.
Skills Evaluation: Physical
The overall goal of the physical skills evaluation is to determine the most functional position for the individual and evaluate his or her ability to access a device physically. At a very basic level, physical skills include range of motion, muscle strength, muscle tone and the presence of obligatory movements. Many protocols exist for evaluation of range of motion. Both passive and active ranges of motion are assessed. Range of motion is important in consideration of positioning needs for function and the amount of movement available to access a device or perform a task. Related to range of motion is muscle strength. Again, many protocols are available for testing muscle strength. Muscle strength is graded in a range from unable to move independently, moves with gravity eliminated, able to move against gravity, and moves against different degrees of resistance. It is important to note that the presence of a neurological disorder such as cerebral palsy, stroke, or traumatic brain injury will affect both range of motion and muscle strength. Typical protocols for testing these components are not generally useful for these populations because the position of the individual affects muscle tone and subsequently range of motion and muscle strength. For example, a child with cerebral palsy may seem to have limited flexion range of motion in the lower extremities when lying in supine. However, when turned on the side, the ability to flex the legs is much easier. In supine, the influence of the tonic labyrinthine reflex increases extensor tone. This influence is not present in side lying, making flexion much easier.
Muscle tone and the presence of obligatory movements are important considerations for individuals with neurological disorders. As described above, the position of the individual affects the available movement. Muscle tone is assessed in various functional positions, particularly prone, supine, sitting, and standing. Obligatory movements, or reflexes, are assessed to determine how they might affect function. Key reflexes or obligatory movements include the asymmetrical and symmetrical tonic neck reflexes, tonic labyrinthine, extensor thrust, bite, and grasp reflexes. The ability to right the head when moved out of a vertical alignment, either lateral or in the anterior-posterior plane is another component. Postural control is a related component that refers to the ability to maintain the trunk in a vertical alignment. When completing an assessment to determine function in various positions, it is important to handle the client and to challenge his or her balance and postural control to determine the degree of support he or she will need to work in a given position and the movement available in that position.
Sitting and standing balance are additional considerations. The ability to maintain balance in these positions is determined through observation of the ability to maintain the position independently and the response to challenges to balance in these positions. Sitting balance is described as hands free, where the individual can maintain balance and function without using hands to support himself or herself; hands dependent, where he or she needs to support himself or herself with one or both hands to maintain sitting; and propped or dependent sitting, where he or she cannot sit without external support. Sitting balance is an important component of a seating and mobility assessment (Chapters 6 and 12).
Gross and fine motor assessments generally test higher-level motor skills. Gross motor skills include balance on one foot, performing symmetrical and asymmetrical movements of the upper and lower extremities, coordinating one side of the body, lifting and carrying objects, rapidly alternating movements, and running, skipping, and hopping. Fine motor assessment includes rapidly alternating finger movements, performance of isolated finger movements, manipulation of objects of different sizes, and performance of specific fine motor tasks. The Bruinicks-Oseretsky Test of Motor Proficiency (Bruininks, 1978) and the Movement ABC (Henderson and Sugden, 1992) are two examples of comprehensive motor evaluations appropriate for children. The Gross Motor Function Test (Russell et al, 2002) is designed specifically for children with neurological impairments. Once again, if a neurological condition is present, it is important to remember that function is dependent on the client’s position.
Identifying Potential Anatomical Sites for Control.
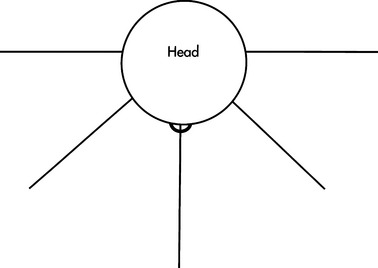
In Chapter 3 we identify the control sites that can potentially be used by the consumer to operate a device (see Figure 3-10) and describe the various movements that each control site is capable of performing.
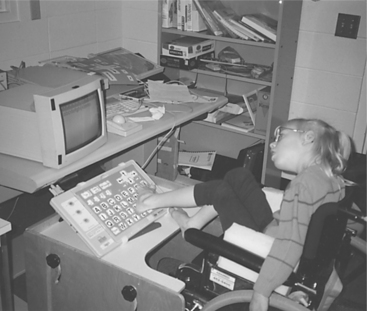
When individuals with physical disabilities are evaluated, it helps to keep in mind the movement capabilities of each of these anatomical sites and the hierarchy in which these sites are considered. The hands and the fingers are the preferred control sites because they are naturally used during manipulation tasks and finer resolution can be achieved. If the hands are not an option for control, the head and mouth are considered next. With the use of mouthsticks, head pointers, or light beams, it is possible to achieve the fine resolution and range needed to control a device. The next option to consider is the foot. Some individuals are able to develop fine control of the foot for typing (Figure 4-4); however, problems with positioning the device so that the user can see it make this site less desirable than the hands or the head. The least desirable sites are the legs or the arms because they are controlled by larger muscle groups, so the movements of these sites are gross in nature compared with the fine movements of smaller muscles (Cook, 1988).
Simulation of functional tasks is used to evaluate the types and quality of movement an individual possesses. Functional tasks are chosen for evaluation because they are often more meaningful to the consumer than physical performance components such as strength and joint range of motion. They also provide the ATP with an opportunity to gather qualitative information regarding the consumer’s movements, and results of such tasks are more likely to reflect the consumer’s true abilities.
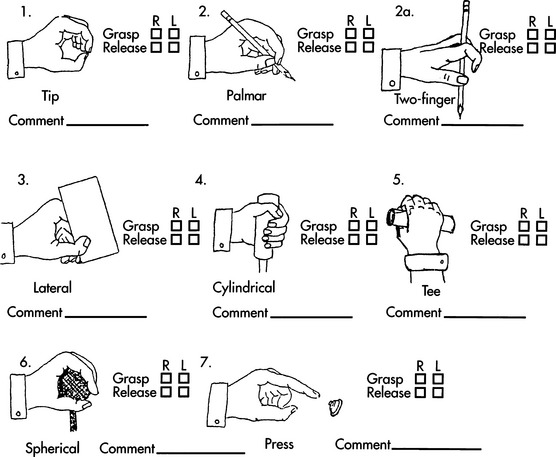
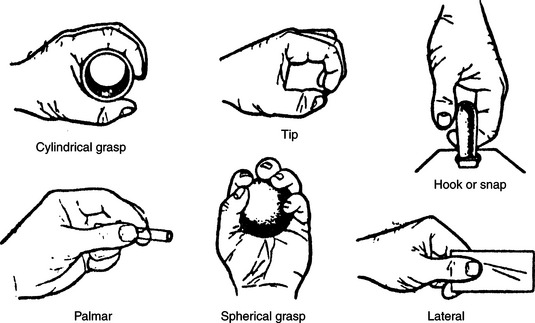
We present a model based on clinical experience to determine the best anatomical site for accessing a control interface. The hands, being the control site of choice, are the first to be assessed. Basic hand function can be observed and rated by using a “grasp module” (Figure 4-5), which includes a total of seven functional grasp patterns. The consumer’s ability to complete each grasp pattern is rated (unable, poor, fair, or good). Notations are also made regarding how the consumer completed the movement and the factors that made it successful or not. For example, did the object need to be positioned in a particular way for the consumer to grasp it? Was there a delay in initiating the movement? Did the consumer have difficulty releasing the object? Was the movement pattern isolated or synergistic in nature? Did the consumer appear to have problems with depth perception when reaching for the object?
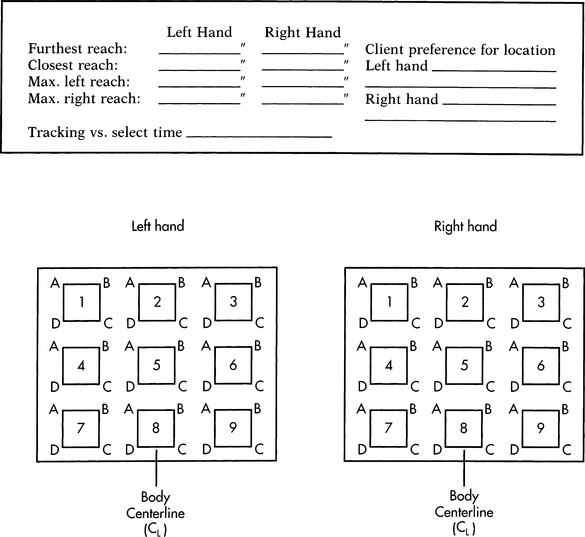
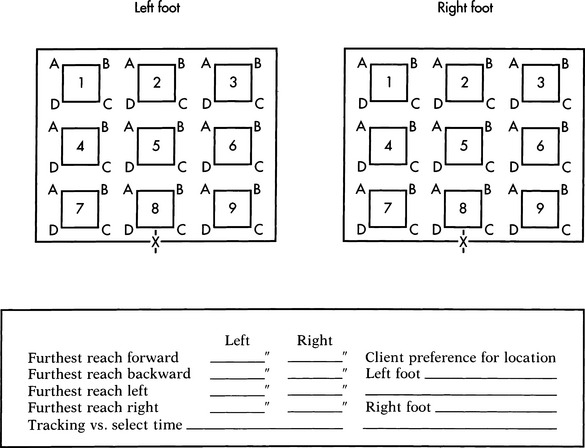
If the consumer has the potential for hand use, it is then necessary to determine the minimal and maximal arm range within a workspace and the resolution in hitting a target. A range and resolution board, as shown in Figure 4-6, can be used to measure both of these. If possible, the consumer is asked to use the thumb or a finger to point to each corner of each numbered square. If the consumer is unable to point to the corners, he or she is asked to touch each square with the whole hand. This provides information regarding the approximate size of the workspace and the best locations for a control interface and a rough measure of accuracy of movement. Both arms are evaluated as appropriate.
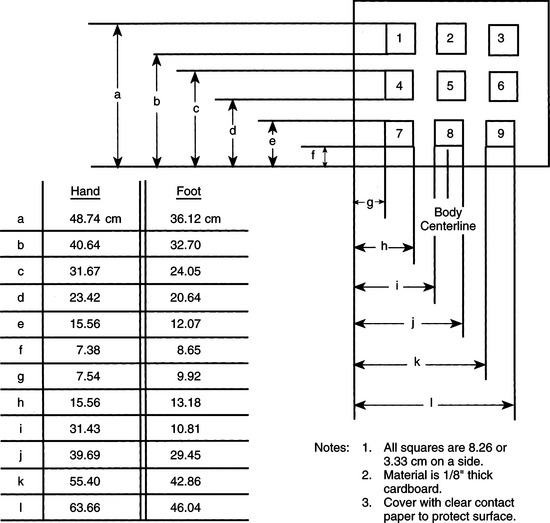
Figure 4-6 Range and resolution board used for evaluating the ability to hit a target using a given control site.
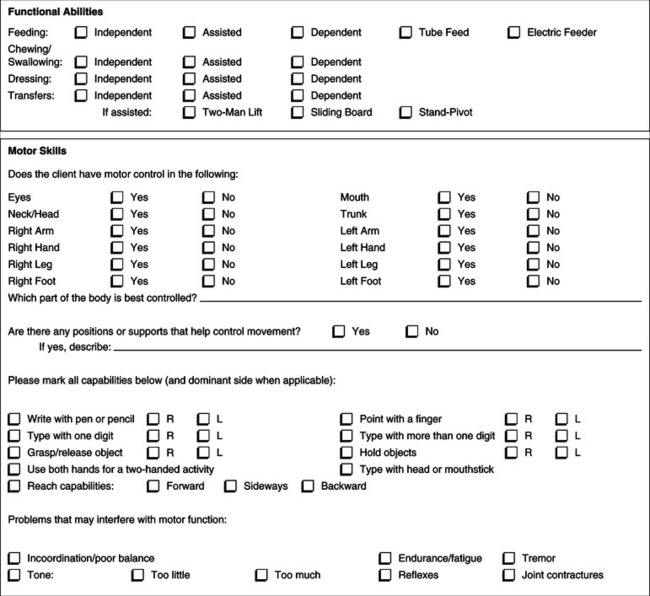
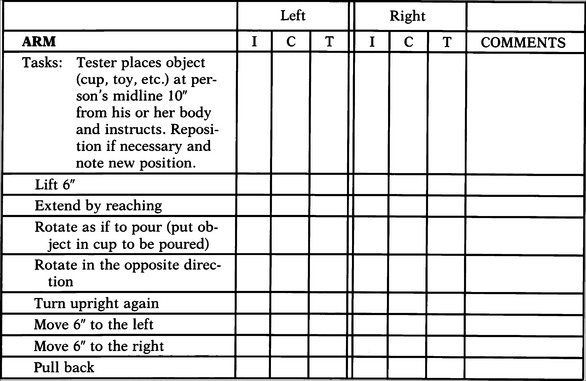
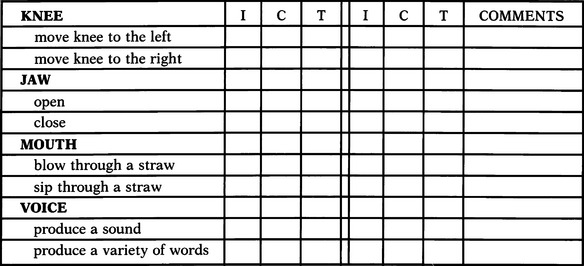
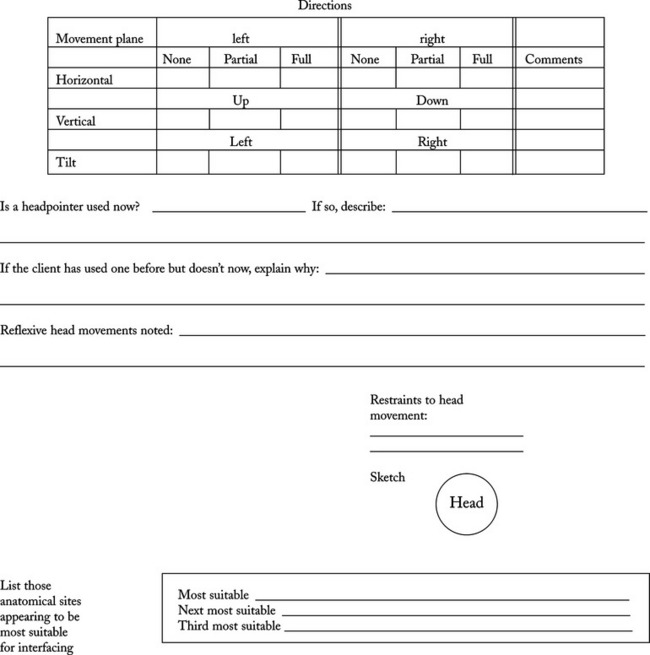
If the hands are eliminated as a control site, other anatomical sites must be considered. For example, we can also measure range and resolution for the foot and head. With a range and resolution board of smaller dimensions, the same task can be used to evaluate foot range and targeting skills and the consumer’s range and resolution with a mouthstick, light pointer, or head pointer. Appendix 4-1B shows a sample assessment form for documenting the information gathered during the physical skills evaluation. After completion of this component of the skills evaluation, the ATP should have a good idea of the user’s physical skills and the anatomical sites that can best be used to control an interface.
Selecting Candidate Control Interfaces.
Once the ATP has identified anatomical sites that the consumer can potentially use, the next step in the process is to select control interfaces that have potential to be used successfully by the consumer. In Chapter 7 we present a set of control interface characteristics that are useful in selecting interfaces that most closely match the consumer’s available anatomical sites.
Comparative Testing of Candidate Control Interfaces.
Once potential anatomical sites and candidate control interfaces have been chosen, next the consumer’s ability to use these interfaces is measured. Comparative testing provides the ATP with data on the consumer’s speed and accuracy in using particular control interfaces. These data can be used to compare different interfaces operated with a given site. If a control enhancer (e.g., mouthstick, head pointer) or modification (e.g., keyguard) is being considered, its use should also be evaluated (Chapter 7). This is one area where gathering quantitative information on the person’s ability to use the control interface is extremely valuable and can assist the ATP in making decisions regarding the selection of a control site and interface. It is also important to note the consumer’s preferences during this process.
During the assessment process, speed of response is often used to compare control interfaces. Speed of response is a temporal (time-based) measurement that can be quantified. Because these measurements are typically made in the controlled setting of the clinic, they must be carefully applied to contexts outside the clinic. Another measure used to compare control interfaces is accuracy of response. This is often based on moving to the correct position, and it is therefore a spatial measurement, rather than a temporal (time-based) measure. Measurement of accuracy requires a standard of performance. This is usually the number of correct responses out of the total number of trials. Speed of response and accuracy are generally inversely proportional to each other for novice users.
When these two basic parameters are defined, methods for measuring them can be described. The selected control interface is first placed in a position where the consumer can activate it. It may be necessary to try different locations for the control interface before finding the position at which the consumer has the greatest control. The consumer’s time to move from a rest position to target the control interface can be measured with a stopwatch.
Computer-assisted assessment provides several useful features. First, data collection and analysis can be automated, relieving the clinician of tedious record keeping. Performance measures for each possible control site/interface pair can be obtained. The effects of different positions for the control interface or the use of control enhancers and modifications can also be measured. Because several different control site/interface combinations can be evaluated, this data collection process can facilitate the choice of interfaces on the basis of measured results. Second, the computer can provide a variety of contingent results (including graphics, sound, and speech) when the control interface is activated. This variety of results not only makes the task more interesting, but it also can allow assessment of visual and auditory capabilities.
Skills Evaluation: Cognitive
Chapter 3 describes the major cognitive skills associated with assistive technology use. Although there are standardized test batteries that are used for cognitive assessment (Duchek, 1991), in general we do not use them for evaluating consumer’s cognitive skills related to assistive technologies. Instead, clinical observation is the major strategy used for the collection of information regarding a consumer’s cognitive function. Clinical observation yields information that is often not provided by standard tests. For example, by observing a consumer using a switch-activated program on the computer, the ATP can obtain an indication of the consumer’s level of attention, understanding of cause and effect, degree of motivation, and ability to follow directions. Assessment of cognitive skills is important when determining whether the client will be able to learn how to use the technology and whether he or she has the capacity to use it effectively in the long term.
All three types of memory discussed in Chapter 3 (sensory, short-term, and long-term) are important for the use of assistive technologies. Memory tasks related to assistive technology can be evaluated by structured clinical observations. For example, the ATP can have the consumer memorize a group of codes and then note the consumer’s ability to remember these codes during an encoding task.
Problem solving can also be measured during functional tasks. For example, when an electric feeder is used, it is necessary to rotate the plate to position the food so that the spoon can pick it up. Proper use of this technology requires a high degree of problem-solving skills. If the person lacks these skills, use of the device becomes frustrating and an alternative should be considered. The value of this type of cognitive assessment is that it occurs during completion of a functional task, which may be predictive of assistive technology system use.
Skills Evaluation: Language
The evaluation of language skills required for the use of assistive technology devices focuses on both expressive and receptive abilities. In addition, the ability to sequence items, use symbol systems, combine language elements into complex thoughts, and use codes is important in operating various types of assistive technologies. Although the most extensive language evaluation is carried out for augmentative communication system recommendations (see Chapter 11), language skills and use are also important in using other assistive devices such as mobility systems (see Chapter 12) or systems for manipulation (see Chapter 14). Also, language and hearing are closely coupled, and assistive technologies intended for persons with hearing impairments must address language and auditory skills (see Chapter 9).
Specific areas that are evaluated include categorization, sequencing, matching, social communicative skills (e.g., degree of interaction), receptive language skills (e.g., recognition of words or symbols, understanding of simple commands), motor speech skills, and pragmatic language skills. Advanced language capabilities (e.g., syntax and semantics) are also evaluated when possible. The evaluation of these skills for augmentative communication device use is discussed in Chapter 11.
Matching Electronic Device Characteristics to the User’s Needs and Skills
The assessment process to this point provides the basis by which the ATP and the rest of the assistive technology service delivery team carefully define the goals to be accomplished and determine the skills the consumer has available for assistive technology system use. It is necessary to systematically transform these goals and skills into characteristics of assistive technology devices. In this section those aspects that are specific to the characteristics of electronic devices are considered. The term device characteristics refers to general properties of the technology. A feature is a particular implementation of a characteristic. Characteristics of automobiles include, for example, engine, color, size, performance (acceleration, gas mileage), and doors. Features for these same characteristics might include four-cylinder engine, blue color, compact size, 35 miles per gallon, and two doors. Consumers have certain needs, and they match those needs to general characteristics to select specific features of interest. They also have skills that apply to the selection. For example, a consumer may not be able to use a standard manual transmission and chooses only automatic transmission cars for consideration. Life roles also play a part in the selection decision. For instance, parents with small children may choose a minivan rather than a compact car.
In assistive technology service delivery, a similar matching process can be used to choose features that match the consumer’s needs and skills. This systematic approach is superior to using trial and error with all the possible devices that may work and then trying to pick one. To use this approach, however, a set of characteristics to be considered must be defined. A generic set of assistive technology device characteristics is listed in Box 4-2. The categories in this box parallel those used in Figure 2-5 to describe the components of the assistive technology portion of the HAAT model. In the following chapters more specific characteristics are considered for certain areas of assistive technologies: seating systems, control interfaces, computer adaptations, augmentative communication systems, mobility devices, manipulation devices, and sensory aids.
Human/Technology Interface.
The human/technology interface is the portion of the device with which the consumer directly interacts. The most general human/technology characteristics, which apply to all devices, are the physical properties. These include the force exerted by the human/technology interface on the person and the force exerted by the person on the interface, the size and weight of the interface, and its texture and hardness. A seating system may be too hard or soft to be effective, and this feature can be related to the needs of the individual consumer. All human/technology interfaces must be attached either to the person, to a wheelchair, or to a stable work surface. Consideration of this “mountablilty” characteristic can often mean the difference between success and failure of the human/technology interface. For example, if a consumer has very limited range of arm movement, a switch must be positioned within this range.
Just as the human user exerts forces on the human/technology interface, the human/technology interface provides feedback to the user. This may be as a direct consequence of the interface. For example, a seat cushion exerts a certain force, depending on its materials, design, and construction. In other cases the user feedback is a separate component, such as a flashing light indicator on a television control or a tactile display on a reading device for a person with total visual impairment. Human/technology user feedback sources can be described in terms of the characteristics of magnitude, type, and origin. These characteristics can be matched to the consumer’s needs. For example, the magnitude of a visual display is the brightness of the light. The types of human/technology interface feedback are other characteristics and include visual, auditory, and tactile varieties. Each of these can be matched to the corresponding user skill. The origin refers to the source of the feedback, such as that provided by a seat cushion or the voice output provided from the screen reader.
The next three characteristics listed in Box 4-2 apply to human/technology interfaces used with electronic assistive devices (including power mobility). The number of inputs required to operate any device is a characteristic. This characteristic is referred to as the size of the input domain (see Chapter 7). There are many types of control interfaces available, with varying numbers of inputs and requiring different physical skills for activation. The most appropriate control interface for any given consumer is largely determined by the physical and interface assessments that are described here and in Chapter 7.
Depending on the size of the input domain related to the consumer’s needs and skills, a selection method can be chosen. In Chapter 7 two basic selection methods are described: direct and indirect. In direct selection, all the choices are presented to the user at one time and the user has the physical ability to choose any one element directly. With indirect selection, there are intermediate steps required for the user to make a selection. If the number of input signals required (on the basis of needs) is greater than the number the consumer can control (on the basis of physical skills), then some form of indirect selection must be used. Individual devices may have both these methods or they may be restricted to only one method. Direct selection requires greater physical skill than indirect selection; however, indirect selection requires greater cognitive, visual, perceptual, and possibly auditory abilities. The consumer’s skills must be taken into account when specific device features are chosen.
Selections are made from a selection set consisting of the choices available to the consumer. Features of this set include size, number of choices, format (e.g., print, tactile), and type of symbol (real objects, pictures, computer icons, line drawings, traditional orthography, or symbols used to represent an idea). The type of symbol system that is most appropriate to a given individual is determined during the language assessment. The question of symbol system type is obviously essential for augmentative communication devices, but it is also important in other applications. For example, in electronic aids to daily living (EADL), the devices to be controlled must be labeled, and often symbols are used rather than words to make the systems available to persons who have difficulty in reading. Speech labels, generated by synthetic speech, are also used in the selection set for individuals who have either visual or cognitive limitations. Along with determining the type of symbols used in the selection set, the size of the selection set is also determined. The number of choices required is often dictated by the consumer’s needs and by other factors such as how many will fit on a display given the consumer’s visual acuity. The choice of these features for a consumer is based on his or her skills in several areas, including sensory, cognitive, and language.
The Processor.
Recall that the processor is the element of the assistive technology device that relates the human/technology interface to the other components. Sometimes this is simply a mechanical linkage (e.g., in a reacher), and in such cases there are not many choices in characteristics. However, processors for electronic devices have several characteristics that must be carefully matched to the consumer’s needs and skills. The first of these is the basic set of commands that are necessary to operate the device. It is important to ensure that the consumer can use these so that the system will be functional for the consumer. For example, in a powered wheelchair system the basic commands are forward, backward, left, and right. In a communication device, some basic commands include printing a document and speaking. In an EADL the commands may include lights on and off, TV channel selection, and telephone dialing. These are essential for operation. The greater the number of commands, the more flexible the system is to the user. For example, an EADL that can control the television with three functions (power, volume, and channel), turn three appliances on and off (lights, drapes, and door lock), dial a telephone (three commands), and access an emergency message machine has 10 functions. The more commands included, the more confusing the system can become. The consumer, family, care providers, and ATP need to evaluate the effect of a specific command size during the assessment.
A second characteristic of the processor is the control parameters. In contrast to commands, control parameters allow adjustments to be made to the system; they are nice to have but not always essential. Control parameters include such things as variable speed for forward and reverse or indoor and outdoor speed levels in a powered wheelchair. In an augmentative communication device, control parameters adjust the voice synthesizer pitch, voice type, and rate to affect the way the speech output sounds. A control parameter also provides the ability to switch between different applications for multiple activity outputs. For example, it is possible to operate an EADL, communication device, and computer access system from a powered wheelchair controller. Individual control parameters need to be presented to the consumer for the systems being considered, and both the consumer and the ATP need to evaluate their effectiveness.
The final general processor characteristic is data or information processing. In this case the device is internally processing information rather than dealing with commands or control signals. One example, used in augmentative communication systems and screen readers for the blind, is the generation of spoken output from text using software programs. By listening to several speech systems, the consumer can determine the intelligibility of each and identify which one is preferred.
Another type of information processing is word prediction, in which the software program guesses at the desired word on the basis of the entries the consumer makes. This type of application can also adapt to the user by learning his or her most frequently used words. Encoding involves the use of a symbol (e.g., number, letter, mnemonic, color) to represent a vocabulary item or a command (e.g., TV ON in an EADL). The user selects the code instead of directly selecting the element, which can increase the user’s rate of data entry. Encoding schemes can be cognitively difficult, and the consumer should try them during the assessment. The consumer may indicate a preference of one encoding method over another after having a chance to try several.
Information processing is also used in sensory systems to convert the input from the environmental sensor to a form that can be presented to the user. For example, a hearing aid uses a microphone to detect voices, amplifies them (data processing), and presents the amplified signal to the ear (see Chapter 9). Different hearing aids have different data processing, and the consumer can evaluate this characteristic.
Environmental Interface.
As discussed in Chapters 2, 8, and 9, the environmental interface is that portion of the assistive technology system that is used to take in information from the external world for use in a sensory substitution system. For example, when the person has a visual limitation, we use a camera, and when a person has an auditory impairment, we use a microphone. Characteristics that apply to this element include the range of the input signal (i.e., how big or small the signal can be and still be detected). The smallest signal that can be discerned from background noise is the threshold. As an example of how these characteristics can be applied, consider the two problems of reading and mobility for persons with severe visual impairments. For reading, the device needs very little range because only one letter or line of text needs to be viewed at a time. However, for mobility the environmental sensor needs to take in a variety of sizes (e.g., from a dish to a tree). For reading, the threshold is low (a letter in fine print), but for mobility the threshold can be much higher.
Activity Output.
The activity output is what the system accomplishes for the consumer (e.g., communication, mobility, manipulation). The first characteristic that describes the activity output is its magnitude. This includes the volume for a speech synthesis system, the force or torque generated by a powered wheelchair, and the brightness of a video screen display. Precision is a measure of how accurately the system performs the functions and how exactly it accomplishes its task. For example, a reacher may be able to pick up a cup but not a button. If the consumer needs to pick up the button, then this particular reacher has insufficient precision to accomplish the task. If an output can be used in different contexts or can be used to accomplish different goals for the consumer, we would say that it is flexible. Flexibility can be an important factor when the consumer has many tasks to perform. Careful consideration of context must also be included in choosing specific activity output features.
Physical Construction.
The final category of characteristics is physical construction. No matter how well a system works in an assessment session, it will not be effective in everyday use unless the person has access to it at all times. This is determined primarily by the mountability of the system. Special consideration must be given to both the mounting of the system (or placement on a desk) and the attachment of any components to a wheelchair. For example, mounting of a communication system to a wheelchair must be considered during the assessment to ensure that the chosen system is compatible with the consumer’s wheelchair.
Portability is a measure of the degree to which the device can be moved from place to place. This characteristic includes a consideration of size, weight, and power source. For electronic devices, portability often requires that the device be battery operated and that it be small and lightweight enough to be carried or attached to a wheelchair. If the person is ambulatory, his or her ability to carry the device needs to be assessed. There are differences in batteries (e.g., life may be a few hours or a few days between charges) and size and weight. For mobility devices, the ability to transport the wheelchair in the trunk of a car may need to be considered. Some wheelchairs fold so that they can be transported in a car trunk, whereas others, such as powered wheelchairs, do not typically fold.
Generally consideration of the characteristics of color, shape, and overall design are done last when a recommendation for assistive technologies is developed for a consumer. We refer to these as packaging characteristics. Consideration of the consumer’s preferences in this area can contribute to motivation to use the system and to overall user satisfaction. However, the consumer’s packaging preferences cannot always be integrated into the system (e.g., the wheelchair may not come in bright orange). All these features should be discussed with the consumer and others to ensure that the device selected will meet the consumer’s needs.
Evaluating the Match Between Characteristics and the Consumer’s Skills and Needs.
It is our premise that a large part of the assessment up to this point is best completed without the introduction of specific devices. The focus of the assessment remains on the functional results to be achieved by the technology instead of on the secondary features of technology, such as color, size, and design. Once the basic functional characteristics have been determined, differences in the secondary factors of size, weight, color, and overall design become important, and they may be the basis for a final decision. After the assessment phases described earlier, one or more devices that have the potential to meet the consumer’s skills and needs are identified for the consumer to evaluate. There are two primary ways in which the ATP can evaluate specific technologies for use by the consumer: (1) trial using the actual device and (2) simulation of device characteristics.
Ideally the consumer will have the opportunity to try the devices being considered and evaluate their usefulness before a recommendation is made. However, because of the expense, it is not always possible for the ATP to have access to every available device, nor is it a prerequisite for conducting a skilled assessment. It is desirable that the ATP have available a set of devices that represents a broad range of characteristics. A service delivery program can carefully choose equipment to be used for evaluations, making it possible to address the major characteristics of devices during consumer assessment. Sometimes a short trial during a one-time assessment is not adequate and it is necessary to have the consumer use the device for an extended period. In some cases a local manufacturer’s representative might loan a device to the ATP for a consumer trial. Other manufacturers and service delivery programs lease devices for this purpose. If these devices are available, it is helpful to demonstrate the various features to the consumer and have the consumer try them. There may be two or three devices being considered, and, if possible, each device should be tried and evaluated by the consumer. In lieu of having the actual device available, the ATP can simulate device characteristics. Simulation requires that the ATP be knowledgeable about the characteristics and features available for specific assistive technologies. For computer-based products, the assistive technology adaptations are often software based, and demonstration disks can be obtained from manufacturers or downloaded from a manufacturer’s Web site. These demonstration programs illustrate the essential features of the software, but they are not fully functional and their use is time limited.
To position a control interface for simulation during assessment, universal mounting systems that can be adjusted and placed in various positions can be used. This step is important to ensure that the control interface is in a functional position for the consumer and that it remains stable during the assessment.
Effects of Errors in Assistive Technology Systems.
An important operational characteristic of assistive technology systems is the way in which they deal with errors. Two types of errors are of concern. Random errors are infrequent and are generally chance occurrences. An example of a random error is the consumer’s inability to understand a voice synthesizer because of high amounts of ambient noise. If the noise is not present, there is no error, and even if there is noise it may not lead to an error in interpretation. It is only the random co-occurrence of the need to use the voice synthesizer, the presence of noise, and a listener who does not understand the output that creates the error. Random errors may recur, but they are not consistently present in the system. We can do very little to avoid this type of error in the assistive technology system design process.
Of greater concern are periodic, or regular, errors, which occur under predictable conditions. These errors may also be infrequent, but they are foreseeable. As an example, many letter-to-speech software programs make mistakes in pronunciation when used with voice synthesizers. The mispronunciation always occurs whenever the particular word is entered. This type of error can be dealt with in the design process. For our example of mispronunciation, exception tables are typically used so that the utterance sounds correct although the letter-to-speech rule makes an error. There are several effects of errors on assistive technology system performance, including loss of information, injury, and embarrassment. All three of these can occur in the same system, and they may be due to the human, the activity, the context, the assistive technology, or the interaction of all of these components. For example, a power wheelchair will not function if the user does not regularly charge the batteries. The user must somehow cause the action that results in the batteries maintaining a charge, and the power wheelchair system must provide accurate information about the degree to which the batteries are charged. Error-free function here relies on the successful integration of the human with the technology. Loss of information is a common effect associated with augmentative communication systems (see Chapter 11) and sensory aids (see Chapters 8 and 9). Loss of information refers to an interruption in the output of the system, whether it is auditory or visual, as in a voice output communication aid, or physical, as in the power to propel an electrically powered wheelchair. It can occur because the human operator makes an error in motor, sensory, or cognitive performance or as a result of a device error. Although the net effect on system performance of either of these errors (human or device) may be the same, it is important to distinguish between them to correct the problem.
When the human operator makes the errors, the distinction needs to be made as to whether the cause is lack of capacity (e.g., inability to control excessive tremor resulting in erroneous selections or visual limitations in reading a display) or lack of skill (inadequate experience or practice in using the device). If the problem is the capacity of the user, then modifications must be made in the system (e.g., using a keyguard to prevent erroneous entries or an enlarged display screen to improve visibility). If the problem is one of skill, training may help reduce the number of errors.
Physical injury is a more serious effect of a system error. This type of error can occur in a mobility system (see Chapter 12) if, for example, a braking system fails or a motor fails to turn off. Consideration of this type of error leads us to the concept of “fail-safe” design. This approach attempts to anticipate the types of errors (termed failures when caused by the device) and to ensure that, if they do occur, the probability of injury is minimized. For example, if a power wheelchair controller fails, it should fail in the off state. If it fails in the on state, the user may be injured because the chair cannot be controlled. Similar to loss of information, the capacity or the skill of the user can cause physical injury. A final general effect of assistive technology system errors is embarrassment. This effect is somewhat unique to assistive technologies, and it is a direct result of the role that assistive technology systems play in the daily life of the user who has a disability. Because the tasks being performed cannot be accomplished without the system, its use is continuous throughout the day. Over a long period, system errors leading to embarrassment are inevitable. The embarrassment may be relatively minor, such as a manipulation system dropping a spoonful of food. In other contexts, it may be much more significant. For example, an augmentative communication device may fail and produce the wrong utterance. If the context is a presentation in an important meeting and the mistaken utterance is an obscenity, the consequences are potentially very negative. To place the importance of this type of error in perspective, recall that the device is often perceived by both the user and other people as being a part of the user. Thus, the user is held responsible for an inappropriate utterance just as if he or she had used his or her own voice to produce it.
The errors and their resulting effects may arise from any of the components of the assistive technology system or their interaction. The human error may be related to capacity or skill. The device may malfunction, in which case the error is related to the design. The context may cause an error. For example, the pressure relief properties of a wheelchair cushion may be impaired if the cushion is exposed to extremely cold environments for a prolonged time and the cushion materials freeze. An example of an error that is caused by the interaction of the components of the HAAT model relates to devices that have many functions, with complex commands required for successful activation. In part, the error is caused by the capacity of the user to learn how to operate the device. It is also caused by the design of the device that requires complex actions for successful operation. Some of the concepts related to human factors that were discussed in Chapter 2 are relevant here.
It is clear from this discussion that identification and reduction of errors can occur at several points in the assistive technology process. Initially, incorporating a design and accompanying soft technologies that are congruent with universal design principles can minimize errors. Errors can be identified and possibly corrected through use of a thorough evaluation that leads to a suitable device recommendation, coupled with a trial period. Finally, errors in the assistive technology system are identified and reduced through follow-up with individual users and after market research into the effectiveness of the system.
Decision Making.
To propose a set of candidate assistive technology devices for a consumer, it is necessary to choose characteristics of these systems that will meet the needs and be consistent with the skills possessed by the consumer. The most important principle in this process is the relationship between the tasks the assistive technology device must accomplish for a person (embodied in the consumer’s goals) and the characteristics that must be contained in the device for those tasks to be accomplished. Each goal may be accomplished only if a set of essential characteristics is included in the assistive technology system. For example, the goal may be mobility, and the characteristics of the type of cushion, wheelchair type, and color all contribute to the accomplishment of this goal.
Many characteristic-goal relationships are subtler, however, and generic characteristics of devices are not always equivalent to specific features of commercially available assistive technologies. For example, a generic characteristic of all EADLs is turning lights on and off. However, different manufacturers of EADLs may accomplish this function in different ways. Developing recommendations and a plan for implementation should be based on the consideration of device characteristics that have been evaluated by the consumer.
Computer-based expert systems that assist in the decision-making process for assistive technologies are being developed. Depending on the expert system, collection and interpretation of data are incorporated. Expert systems use artificial intelligence to guide the ATP through the assessment and decision-making process. Expert systems attempt to mimic the skills of an ATP by using software programs that are capable of making decisions much like humans do. In assistive technologies, several preliminary systems have been developed. Garrett et al (1990) have developed an expert system called VOCAselect for use in selecting augmentative communication systems for specific consumers. Their system is based on 17 features that are determined during the assessment process. In addition to features related to consumer performance (e.g., input method, vocabulary size), they include physical construction (e.g., portability) and information regarding available support services (e.g., acceptable price range, training availability). These factors are then related to specific features of each available communication device. The expert system matches the specific requirements of the user, on the basis of goals and needs and on assessment of skills, to appropriate devices. By including the weight of factors (e.g., characteristic A is twice as important as characteristic B) and a scale of responses (e.g., priority for speech output is nine out of 10), this type of expert system can focus on specific options even more closely. Garrett et al report that preliminary trials indicate exact agreement in device selection between the expert system and a speech-language pathologist.
Stapelton and Garrett (1995) carried out an evaluation of this system. Respondents to a survey indicated strongly (greater than 79%) that this system would be of value in making recommendations for augmentative communication systems. They also present an example of the use of this program for a specific case. Stapelton et al (1995) extended the VOCAselect concept to the selection of computer adaptations (see Chapter 7). This computer program is similar to VOCAselect, but it is built on characteristics of devices and software used to make computers accessible to individuals who cannot use a keyboard or mouse for entry or the standard screen for output. In operation this software is functionally identical to VOCAselect. Stapelton et al (1995) present an example of the use of this system.
Regardless of whether an expert system is used, the process we have described is highly effective in defining the features of a recommended system. It is important to recognize that the features that are most limiting must be considered first, followed by those that are less restrictive. For example, in an augmentative communication system, the type of symbol system is often the most limiting characteristic. If a consumer requires pictures as a symbol, many devices are eliminated immediately. In contrast, spoken output as a characteristic is not as limiting because most devices use similar speech synthesizers. For each type of assistive technology, it is important for the ATP to identify a set of general characteristics that fit within the categories of Box 4-2. These are presented in later chapters. If the characteristics are generic, then specific features can be selected in sequence to define the final assistive technology system. The major advantage of the assessment methods described here is that they are based first on a consideration of the consumer’s goals and skills and second on a consideration of assistive technology system characteristics. Thus the system is matched to the consumer (within the limits of current technology) rather than the consumer being forced to adapt to the system. Without a structured approach such as the one presented here, however, it is very difficult to meet consumer’s goals.
It is clear that many characteristics of devices should be considered, and the features (and their costs) will differ from one system to the next. In addition to specific features of the device, other important factors include the contexts of use, the amount of training required before the device can be used effectively, cost, availability of a family member or caregiver to support and facilitate the training and implementation of the device, and ease of use of the device.
Recommendations and Report
The recommendations summarize the information gathered during the evaluation and suggest a design for the assistive technology system. At the conclusion of the assessment, everyone involved should sit down to review it and come to a consensus regarding the final recommendation. A written report is prepared that details the assessment and recommendations for an assistive technology system. The written report synthesizes the assessment process, and it starts out by defining the needs and goals that have been addressed. A summary of the consumer’s skills applicable to device use is provided, with a description of generic characteristics to be incorporated into a device. This summary is followed by specific recommendations for equipment, including descriptions, part numbers if applicable, manufacturer’s name, any modifications that need to be made, and cost. Recommendations for soft technologies are also included in the written report. These may include recommendations for developing skills that are necessary before purchase of a device, training once the device has been purchased, and strategies for incorporating the technology into the individual’s context. Finally, a plan for implementation of the recommendations is provided. This includes logistics such as seeking funding from the appropriate sources and who will take responsibility for implementing the recommendations.
Often the written report is aimed at various individuals, thus presenting a unique challenge for the ATP writing it. The report, first of all, needs to be geared toward the consumer, who may not be familiar with medical or technical jargon. Rehabilitation or educational professionals working with the consumer may also be receiving the report and its recommendations. These professionals typically need information on what the consumer’s skills have been in using the technology and what skill areas they may need to address to facilitate the use of the device. Some of these professionals may be very knowledgeable in assistive technology, but for others this may be their first experience with it. The contact person for the funding source will also be reading the report, and his or her interest is typically in the “bottom line,” or what it is going to cost. This person wants evidence that the system recommended is going to meet the consumer’s needs at the lowest possible cost. In the section on funding in this chapter, we describe how to write a report to a third-party payer to justify the purchase of an assistive technology system.
IMPLEMENTATION
Once the recommendations have been made and funding is obtained, the implementation phase begins. This aspect of the delivery process consists of ordering specified equipment, obtaining commercially available equipment or fabricating custom equipment, making needed modifications, assembling or setting up equipment, thoroughly checking it as a system, fitting the device to the consumer, and training the consumer and caregivers in its use.
Ordering and Setup
Many recommended interventions have components from several manufacturers, and these must be integrated into a total system. Some of these may be standard commercially available components and others may be commercial assistive technologies. These devices are ordered from the manufacturer or equipment supplier and may take up to 6 weeks to be received after ordering. The recommendation may have also included a custom device or devices that require an adaptation. Examples of custom modifications include mounting a switch to a wheelchair or table, making a cable for connecting two devices together (e.g., a communication device and an EADL), programming a device for unique vocabulary, and adapting a battery-powered toy so that it can be controlled with one switch. The design and fabrication of these system components can occur during the waiting time for the delivery of the commercially available technologies. Once all the individual devices and adaptations are available, it is necessary to assemble them into a total package. For example, a wheelchair obtained from one source and a seating system from another will need to be interfaced to each other. The complexity of this assembly process varies widely, and some systems require much more effort than others.
Delivery and Fitting
Once the equipment is obtained, modified, or adapted as necessary and integrated into a system, the system is ready to be delivered to the consumer. This may occur in a clinic setting, in a school or at a job site, or in the consumer’s living setting. The choice of locations depends on the nature of the equipment, the ease of transport of the consumer, and the complexity of the system (i.e., what support services of technicians and tools are required). We refer to all system deliveries as a “fitting” because we are interfacing the human (consumer) with the rest of the system. In some cases, such as custom seating systems, the process resembles a fitting for an orthotic or prosthetic device. In other cases the fitting focuses on installation of the system, mounting the control interface and the device to a wheelchair, and interconnection of the various components. The fitting phase may also include some amount of assessment as adjustments are made to optimize the consumer’s ability to use the system. An example of this is the use of head switches to control a power wheelchair. The head switches must be attached to the wheelchair and wired into the controller unit. This is done before the fitting, and during the fitting, the location of the head switches (e.g., how close they are to the consumer’s head) is adjusted to maximize performance.
The complexity of many assistive technology systems may require more than one session to obtain all the proper adjustments, mountings, and fittings. The ATP must be prepared to continue making adjustments and adaptations in the system until the consumer’s goals and needs are met. This phase of the delivery process often involves some reassessment, but its success is directly related to the quality of the initial assessment and recommendations, and difficulties experienced at this time can often be traced to incomplete or inaccurate assessments.
Facilitating Assistive Technology System Performance
A major concern of everyone involved in the delivery of assistive technology services is whether the device recommended is going to meet the stated goals. It cannot be assumed that intervention ends with the delivery of the device. Most users of technology, even those with previous technology experience, require assistance in facilitating their performance with the device. The ATP, as the designer of the system, is responsible for providing the means to facilitate human performance. The soft technology described in Chapter 1 is relevant here.
Bailey (1989) identifies three methods that facilitate human performance: written instructions, performance aids, and training. He describes the major difference among each of these facilitators as “the time that elapses between when information is presented and when the performance takes place” (Bailey, 1989, p. 325). A performance aid is used immediately and written instructions are read and also used fairly quickly, but information presented during a training session may not be used until months later. In designing performance facilitators for individual users, the ATP should keep this difference in mind. The ATP also needs to know how to provide a balance among these facilitators. For example, many manufacturers of augmentative communication devices develop an abundance of written instructions. Even if the user were to read all this information, most of it would be forgotten. It has been found that when workers on a job site need information that can be found in similar documents, they either take a guess at the solution or ask someone else (Bailey, 1989). The same thing happens with assistive technology users. An example of this is a person who is hard of hearing and obtains a hearing aid. It may work fine for a relatively long period; then the batteries are discharged and need to be replaced. Often the user merely puts the hearing aid in a drawer because it “doesn’t work anymore” instead of replacing the batteries. If the user does replace the batteries, it is generally because he asked someone else what to do or was instructed in the process when the aid was sold to him, not because he looked it up in the user’s manual. Bailey admits that there are few guidelines to help the ATP determine when to use performance aids, written instructions, or training but emphasizes that “the best decisions are made when as much as possible is known about the potential users, the activity to be performed, and the context in which the performance will take place” (p. 326). As applicable, each of the following chapters has a section on specific training ideas.
Training.
Bailey (1989) defines training as “the acquisition of skills, knowledge, and attitudes that will lead to an acceptable level of human performance on a specific activity in a given context” (p. 387), which is referred to as performance-based training. In the field of assistive technology, prior authorization from the funding source to conduct training is usually required. For a funding source to authorize training, an estimate of the amount of time that will be needed is typically required, with the result that training becomes time based rather than performance based. Time-based training is completed within a specified period, regardless of whether the user achieves a level of skill. Without adequate training, there is an increased likelihood that the device will be abandoned. The training process is facilitated if the ATP starts out by developing a set of well-defined, measurable objectives for training. These objectives help focus the training sessions and serve as an indicator for termination of training. It is also important that there be one person affiliated with the consumer who takes on the role of the facilitator and learns the operation of the device and basic concepts so that he or she can assist with the use of the device as needed.
Training oriented toward establishing operational competence is initiated at the delivery and fitting (Pallin, 1991). This phase of training is intended to make it possible for the user of the technology, his or her care providers and family, and any other support person to begin using the assistive technology system. Examples of considerations included in training for operational competency for the consumer are (1) how to turn an electronic device on and off, (2) making adjustments in operational parameters (e.g., adjusting a scanning rate), (3) loading an initial vocabulary in an augmentative communication system, (4) explaining basic maintenance (e.g., battery charging, cleaning), (5) introducing basic functions and how they work (e.g., choosing what to say on a communication device, using an adapted telephone dialer), and (6) basic troubleshooting so that the consumer and others have some strategies to use if problems develop with the system. It is important to present information in small doses to avoid overwhelming the consumer and others, particularly for a complex system. At the initial fitting session it is only necessary to present enough information so that the consumer can begin to use the system. Subsequent training addresses the acquisition of the necessary skills for more advanced operations.
In addition to basic operational competence, it is necessary for the consumer to develop strategies that maximize the effectiveness of the system. To facilitate this, the ATP provides training for strategic competence. The training focuses on the application of the system rather than on basic operation. As this phase of training progresses, the consumer begins to develop his or her own set of strategies. For example, the person using a manual wheelchair will develop strategies for navigating curbs or inclines and the user of an augmentative and alternative communication (AAC) device will develop strategies for communicating in a noisy restaurant.
Performance Aids.
A document or device containing information that an individual uses to assist in the completion of an activity is called a performance aid. By decreasing the amount of information to be remembered, the performance aid reduces the amount of cognitive processing required to complete an activity. With a performance aid, the user does not have to rely as much on long-term memory, which results in reduced errors, increased speed for certain tasks, and a reduced amount of training required. Performance aids do not necessarily have to be written; picture symbols can also be effective for individuals who cannot read. Bailey (1989) describes five quality standards for performance aids: (1) accessibility, (2) accuracy, (3) clarity, (4) completeness and conciseness, and (5) legibility.
Performance aids are commonly used with individuals who have memory deficits as a result of damage to the brain. One type of performance aid is simple step-by-step instructions that assist the user in carrying out a sequence of tasks. For example, Tim is a young man who has sustained a head injury. He uses a computer to complete school assignments but has problems remembering the sequence of steps to get into his computer word processing program. The steps to do this have been simply written and are posted next to his computer. Because Tim also has visual acuity problems, the instructions are printed in large, bold letters. For Tim, this simple performance aid has meant the difference between success and failure in using his computer.
Another type of performance aid assists in remembering several items of information. An example of this type of aid is a printed list of codes with their meanings, which an individual may have stored in his or her augmentative communication system. Often such a list such is attached to the side of the device so the user can view it easily as needed. Sometimes codes and their meanings are built into software programs and presented on the screen each time the user selects a letter.
Written Instructions.
Written instructions should be considered an integral part of the system and be available to the user at the time of the system delivery. Instructions are helpful when step-by-step directions with detailed information are required or when graphic information needs to be presented. Written instructions may be compiled and presented in the form of user manuals, handbooks, or computer software. The ATP must not assume that the instructions provided by the manufacturer are going to be adequate. Written instructions provided by the manufacturer of the system may include too little or too much information or they may be difficult to follow by the user. It is recommended that instructions from the manufacturer be reviewed and supplemented as needed. When the manufacturer’s documentation is overwhelming, the ATP can review the documentation and condense it into a quick reference sheet that provides simplified and frequently used information.
Bailey (1989) provides detailed guidelines for developing the various types of written documents, including software documentation. It is important to remember to keep the audience in mind and to write the instructions for the people who will use them. For example, if the primary person facilitating the performance is the parent, the instructions may be different from those generated if the facilitator is a teacher. In the field of assistive technology, this may mean a new or revised set of instructions for each individual consumer, even for use of the same device.
FOLLOW-UP AND FOLLOW-ALONG
Once the system has been implemented, it is tempting to think that the intervention has been completed. This perception, however, is totally false; the delivery of the system marks the beginning of the time of use, and it therefore signals the beginning of the evaluation of system effectiveness. The term follow-up refers to activities that occur during the period immediately after delivery of an assistive technology system and that address the effectiveness of the device, training, and user strategies. The term follow-along is used to describe those activities that take place over a longer period. This phase addresses factors such as changes in needs or goals, availability of new devices, and other concerns.
A formal follow-up phase is included in the delivery process for several reasons: (1) assistive devices can seldom be used right out of the box without ever needing to be adjusted, (2) electronic devices are not 100% reliable, and a significant portion of them require repair during the first year of use, (3) training programs seldom proceed flawlessly, and questions arise during the initial period of use, and (4) perceived device failures are often the result of operator error caused by a lack of device understanding. A carefully developed follow-up program will identify these problems easily and address them quickly.
Repair and maintenance are often conducted during the follow-up phase. Repair refers to action taken to correct a problem in a system. Maintenance, on the other hand, is a systematic set of procedures that is aimed at keeping the device in working order. Examples of maintenance functions are proper battery charging, cleaning, tightening mounting hardware, and lubrication of moving mechanical parts. A regular schedule will ensure that necessary maintenance takes place. Assistive technology system failures result in a major disruption of the consumer’s life. For example, a consumer depends on a power wheelchair for mobility. If it fails, he or she may have a manual wheelchair as a backup, but the consumer’s independence may be significantly reduced. Repair of assistive technologies is most often carried out either through manufacturer’s representatives or directly through the manufacturer. In the latter case, the device must be returned to the factory for repair, and the consumer may be without it for several days or even longer. Prompt attention to repair needs of consumers is an important part of follow-up.
As part of a formal follow-up program, contacts with the consumer (by telephone, on the job site, in the home, or in the clinic) are scheduled on a regular basis, such as at 1, 3, 6, and 12 months after delivery. These contacts occur regardless of whether there is a perceived problem, and they are in addition to other activities such as training or repair. This regularly scheduled contact is important because there may be unnoticed problems, or more often there are underused features that are discovered during the follow-up sessions. Mortola, Kohn, and LeBlanc (1992) found in a follow-up study that, because of mechanical reasons, 63% of 196 assistive devices delivered by their center were not being. In most of these cases the consumer had not informed the ATP of the device failure.
As we have defined it, follow-along has a much longer time frame than follow-up does. Although follow-up typically covers the first year of operation of an assistive technology system, follow-along is carried out over the individual’s lifetime. Consumers may return for service after a period of years for several reasons. They may have found that the device is not working as they would like and is not meeting their functional goals. Another reason is to obtain information about advances in technology since they obtained the device. In other cases the consumer may have changed in significant ways. This change is often seen in children who have grown significantly and need a revision in their seating system. Change can also be the result of a degenerative condition such as amyotrophic lateral sclerosis, and in these cases the device may need to be altered to accommodate decreased physical function. In other cases the change in consumer condition is a result of the development of new skills that make it possible to consider new device features. For example, a consumer who has had a traumatic brain injury may initially receive a communication device that is based on very simple replay of sentences. As he or she recovers, the ability to spell effectively may improve and a device with this capability should be considered.
There are other reasons for follow-along. One of the most important of these is a change in the life roles and context of the consumer. For example, Martin, who has severe cerebral palsy and has used an AAC device for several years, decides to move into an apartment on his own. The success of this transition could depend heavily on the availability of assistive technologies. An EADL would allow him to control lights and appliances, answer and dial the telephone, and control the television, DVD, and other entertainment devices. This re-evaluation is dictated not by changes in his condition but by changes in his life roles and the context in which he will be using his technology.
As opposed to follow-up, follow-along is often initiated by the consumer rather than by the ATP. This is because the ATP is not aware of the changing physical, sensory, and cognitive conditions in the consumer. On the other hand, the consumer cannot possibly be aware of changes in technology. For this reason, it is important that the ATP develop a mechanism to maintain contact with consumers to inform them of changes in technology. This mechanism should empower each consumer to take personal responsibility for his or her long-term assistive technology needs. One frequently used method for doing this is a regular newsletter that is sent to consumers by the ATP.
Another reason for both follow-up and follow-along is to evaluate the effectiveness of the assistive technology system by measuring outcomes. This evaluation provides a measure of how well the system meets the original needs identified during the assessment. The next section describes the measurement of outcomes.
EVALUATING THE EFFECTIVENESS OF ASSISTIVE TECHNOLOGY SERVICES AND SYSTEMS
Measuring the outcomes of assistive technology services is a primary focus in the industry today and will continue to be in the forefront of assistive technology service delivery. Consumers want measures that reflect their needs for improved function and quality of life. Payers seek efficient provision of services using the fewest possible resources, and providers seek information on how to deliver efficient and effective assistive technology services. To provide evidence of the effectiveness of assistive technology services and systems, well-developed and sound outcome measures are required.
Fuhrer et al (2003) suggest that a comprehensive conceptual framework will guide the development of useful outcome measures. They describe a model that will help researchers and clinicians identify assumptions, variables, and populations when developing, considering, and implementing assistive technology outcome measures. Outcome of device use is considered to be the frequency and duration of device use.
The model considers different time frames when evaluation is important: initial procurement of the device and the introductory period leading to short- and long-term outcomes. Three aspects are considered when a device is obtained: (1) the need for the device, (2) the type of device, including its intrinsic and extrinsic properties, and (3) the services involved when obtaining the device (Fuhrer et al, 2003). A number of constructs are considered in evaluating short- and long-term outcomes, including effectiveness, efficiency, satisfaction with the device, psychological function, and subjective opinion of the contribution of the device to the client’s well-being (Fuhrer et al, 2003). If the user is not satisfied with the device, it may be abandoned in either the short or the long term. The constructs related to the International Classification of Functioning, Disability, and Health (ICF) (World Health Organization [WHO], 2001) are mediating factors in the short and long term. This classification is described in Chapter 1.
When outcome measures for assistive technology systems are considered, the ATP needs to develop measures and standards of performance that allow a careful determination of the effectiveness of such systems. For instance, a child who is evaluated for a power wheelchair (see Chapter 12) will have a level of accuracy, speed, and reliability that can be measured. Speed of response and accuracy are both used to assess power wheelchair performance. The speed of response is important in describing how quickly a disabled consumer reacts to obstacles, and accuracy is a measure of how well the consumer can navigate a specific course. If this is used as the baseline performance, progress over time can de determined by comparing performance with this baseline. In a clinic or laboratory setting, these measures can be used to select a control interface (see Chapter 7) and to determine such things as the feasibility of safe powered mobility. However, to determine the success of the desired functional outcome (independent mobility), measures must be made in the intended context. This requirement raises several additional questions, such as what is the standard for accuracy of power wheelchair use in a shopping mall? Is it a minimal number of collisions with people and objects? If so, how many are acceptable? Is it being able to successfully negotiate a crowded store? If so, what is being measured to assess success (e.g., minimal breakage, no collisions, how fast the user gets to the door)? Obviously, measuring and assessing assistive technology system performance in the real world is not an easy task. In the remainder of this chapter the focus is primarily on the measurement of outcomes of the use of assistive technology devices and the provision of services.
Overview
The effectiveness of assistive technology systems in meeting the needs of consumers is related to many factors. Sackett (1980) identifies four types of evaluation to consider: effectiveness, efficacy, availability, and efficiency. These can each be related to different questions and to different assessment instruments. For evaluating effectiveness we ask the question, does it work? Effectiveness is measured in terms of the impact of the product on the consumer’s life and needs. Therefore the outcome measurements that we collect must begin with and focus on the consumer and the results of the assistive technology intervention. These outcomes allow us to determine the efficacy of the service delivery structure and process. Efficacy is the ability to produce a desired result or effect; the question to be asked is, can it work? This aspect is what is measured in evaluation of a service delivery structure and process. It provides useful information on how services are being delivered so that necessary revisions can be made.
The entire assistive technology industry is evaluated by the success of service delivery and assistive technology system use by the consumer. As described above, the consumer and the delivery of assistive technology services are at the core of the assistive technology industry (see Figure 1-2). Gathering information on outcomes should be included as a regular part of the service delivery process so that this information can be used as feedback to the rest of the industry. For example, a manufacturer could be determined to have good manufacturing practices and meet all industry standards; however, the most meaningful standard is the effectiveness of the equipment for consumers. Likewise, the effectiveness of the equipment is only as good as the service provider who delivers it. If, as a whole, there are problems with consumer use of assistive technology, all the industry will be affected. This aspect is related to evaluation of availability, which asks the question, is it reaching those who need it (Sackett, 1980)?
Finally, the question, is it worth doing? needs to be answered. This addresses the relative importance of the service being provided by comparing it with other programs that could be purchased with the same resources. This evaluation measure is referred to as efficiency. Third-party payers want to know that the assistive technology services and devices are worth paying for. It is the ATP’s responsibility to provide this justification.
A wide range of outcome data needs to be collected, and determinations need to be made regarding what measures will be used, how many measures are needed, and how focused the measures need to be (Smith, 1996). When outcome measures are developed for assistive technology devices and services, it is important to be clear about who the stakeholders are in this process (DeRuyter, 1995). This is not as obvious a question as it first seems. If outcome measures are used to inform funding sources, are these funding sources consumers of the outcome results or stakeholders in the process? Likewise, providers may be considered either consumers or stakeholders, depending on the type of outcome measure used and the implications for its implementation. If user satisfaction is to be used as an outcome measure, is that a measure that relates to the provider, the funding source, or the user? Certainly the user of the technology is a consumer, but not all outcome measures are user centered. In the remainder of this section those measures that have been demonstrated to have reliability and validity in the measurement of outcomes at several levels are discussed.
Structure, process, and outcome measures in assistive technology delivery can be distinguished among. The structure of the delivery system refers to aspects such as the staffing, staff expertise, equipment on hand, budget, and range of services provided. The process of assistive technology delivery includes the stages of assessment and intervention described in this chapter. Process measures ascertain whether these stages have occurred and whether the procedures meet an acceptable standard. Outcome measures evaluate the end result of the assistive technology intervention. Figure 4-7 illustrates the interrelationships among the assistive technology system, the service delivery process, and their outcomes.
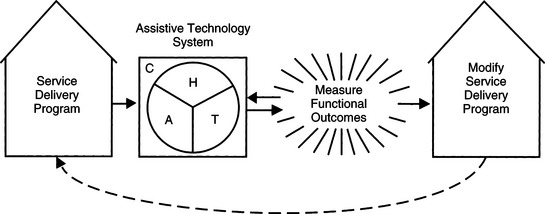
Figure 4-7 Interrelationship among the assistive technology system, the service delivery process and structure, and their outcomes. H, Human; A, activity; C, context; T, assistive technology.
There are a number of different levels at which we can evaluate the effectiveness of both devices and services by measuring outcomes. Traditionally, at the clinical level the question being asked is, did the intervention remediate the individual’s impairment? This is the impairment level of the ICF classification of the WHO (see Chapter 1). In the provision of assistive technologies, this level is seldom the major focus, but it is important because assistive technologies can lead to improvement in impairment and thus in function. The parallel interventions model (Angelo and Smith, 1989; Smith, 1991) described earlier in this chapter illustrates how intervention to affect the level of impairment is related to the use of assistive technologies. The next level is the functional level, when the question is, can the individual accomplish tasks that he or she could not do without the assistive technology? This is the activity level of the ICF classification of the WHO. In this case, functional performance measures are typically used to determine effectiveness.
When services were primarily clinical and delivered in institutional settings, measures of impairment and functional measures were the focus of outcome evaluation. However, over the past decade there has been a move toward community-based services in rehabilitation. This has been driven by rising costs of institutional care and is being addressed by shortening stays and transferring more care to the community. As described in this chapter, many services, including most of assistive technology services, are more appropriately delivered in the community where they will be used.
Community-based services are also being driven by an emerging alliance between the largely institution-based rehabilitation establishment and the largely community-based disability community. This alliance has implications for responsibility for care, including responsibility for choices of assistive technology devices and services (Lysack and Kaufert, 1999). As described in Chapter 1 and in this chapter, consumers play a larger role in decision making regarding what they receive and the evaluation of the quality of both the devices and services. The question being asked by the consumer at this level is, do the assistive technology services and devices provided meet my needs? To answer this question, user satisfaction measures related to assistive technology services and devices have been developed.
As discussed in Chapter 1, the classification of disability over the past 20 years has begun to focus on its social dimensions (Fougeyrollas and Gray, 1998). This social model, now incorporated into the WHO ICF classification (WHO, 2001), provides a richer and more complete view of both disability and the role of assistive technologies in the lives of people who have disabilities. It is no longer important to achieve success only in the clinic or laboratory. The real test is in daily community use of the technologies. The question being asked at this level is, what is the impact of this assistive technology device or service on quality of life? The primary outcome measures used for assessing the effectiveness of assistive technology devices and services in this broader social context are quality-of-life measures.
Each of these primary types of measurement of assistive technology device and service outcomes is discussed in the following sections.
Measuring Clinical and Functional Outcomes
In the past, health care and rehabilitation quality of service was measured by looking at factors such as timeliness and the completeness of the services provided (e.g., whether a discharge summary was completed for the consumer within 1 week of discharge). These are actually process measures, and they do not reflect outcomes of the assistive technology intervention. Within the past decade or so, rehabilitation service providers have begun to focus more on the functional outcomes achieved by the consumer as a result of intervention. Because the focus of assistive technology practitioners is on reducing disability and maximizing an individual’s functional status, it is only natural that one of the factors to measure is functional outcome related to assistive device use.
There are a number of tools that have been developed and studied that measure functional outcomes of individuals who have been through the rehabilitation process. Examples of functional outcome measures include the Barthel Index (Mahoney and Barthel, 1965), the Klein-Bell ADL Scale (Klein and Bell, 1979), and the Functional Independence Measure™ (FIM) (Uniform Data System for Medical Rehabilitation, 1997).
Unfortunately, many of these traditional tools used in the field of rehabilitation do not document the efficacy of technological intervention (Christiansen, Schwartz, and Barnes, 1988; Smith, 1996). As Smith (1996) points out, many instruments are limited in their scope in three ways: (1) they tend to be developed for a particular population, such as individuals who have sustained a stroke, (2) many instruments are developed for a particular health care setting, such as long-term care or acute rehabilitation settings, and (3) they frequently focus on a specific functional area, such as hand function or self-care.
Functional Independence Measure.
The FIM (Instrument is an example of one functional outcome measure. We have chosen the FIM(as an example because it is widely used in assessing the outcomes of rehabilitation interventions. The FIM(is based on a medical model of assessment that places importance on cure (Smith, 1996). The FIM measures the individual’s performance on 18 items under the categories of self-care, bowel and bladder management, transfers, locomotion, communication, and cognition (Uniform Data System for Medical Rehabilitation, 1997). The scoring of the FIM(is on a seven-point scale. The individual only obtains the full seven points if he or she does not require any assistance or assistive device to perform a function. Thus the FIM(is not directly applicable to assistive device outcome measurement because its maximal score in any category can only be obtained if the person does not use any technology. Use of technology automatically implies that the person is not totally functionally independent. This appraisal of functional independence is inconsistent with the current view that an individual is independent if he or she can manage his or her own life (Smith, 1996). Another concern regarding the FIM(and other tools that measure function is that they do not impart information regarding the impact of assistive devices on the quality of life of the user (Jutai et al, 1996).
User Satisfaction as an Outcome Measure
Any discussion of assistive technology effectiveness must consider the recommended system and how well it meets the consumer’s needs. Therefore, the measures must be consumer oriented, which means that the factors used to evaluate the effectiveness of assistive technology systems must be based on criteria that are important to the consumer. User satisfaction is the consumer’s perception of the degree to which the assistive technology system achieves the desired goal. This is a multidimensional phenomenon that requires qualitative measures (Demers, Weiss-Lambrou, and Ska, 1996). In addition, general user satisfaction scales are global, and they do not take into account various factors that affect a person’s use or nonuse of assistive technologies. In assistive technology applications, on the other hand, rating scales that address specific aspects of use are used (see Brooks, 1990, for example). For a large sample of users, these surveys can be statistically analyzed to determine the most important factors in achieving user satisfaction. These group statistics may indicate a significant lack of satisfaction, and this information can be used to make changes in the service delivery structure and process to improve user satisfaction. For any individual assistive technology system, satisfaction is one parameter to be evaluated during the follow-up and follow-along processes. One limitation with satisfaction survey instruments is that they often “top out”; that is, individuals use either the highest or lowest score, and the range of a scale is lost. For example, assume that a five-point scale is used, with levels of “very dissatisfied,” “dissatisfied,” “neutral,” “satisfied,” and “very satisfied.” Most individuals will reduce this to a three-point scale, using the two ends and “neutral.” This is especially true if several parameters are measured with the same scale. Also, user satisfaction scales are one dimensional, measuring only satisfaction. Multidimensional scales can be more informative (Jutai, personal communication, 2001).
Canadian Occupational Performance Measure.
The Canadian Occupational Performance Measure (COPM) (Law et al, 1998) assesses the client’s perception of the importance of self-identified occupational performance goals and his or her satisfaction with that performance. The measure uses an interview format to identify goals in the areas of self-care, productivity, and leisure. The client rates the importance of each of these goals and their satisfaction. The instrument can be used before and after intervention. It is quite flexible because it allows the user to adapt the instrument for a specific purpose. The user can ask the client to think specifically of self-care, productivity, and leisure activities that he or she wants or needs to do when using a particular type of assistive technology. Miller Polgar and Barlow (2002) used this instrument as an outcome of seating and mobility intervention. Its utility was somewhat limited unless the client was asked to think about goals that specifically involved the use of assistive technology. This instrument has been used with many different client populations. Once the client becomes comfortable with identifying his or her own goals, the COPM is a very useful outcome measure.
Quebec User Evaluation of Satisfaction With Assistive Technology.
Five criteria were used in the development of the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) (Demers, Weiss-Lambrou, and Ska, 1996). The first is the recognition that user satisfaction is a multidimensional phenomenon that includes a broad range of variables, each of which can affect the user’s satisfaction with assistive technology. The second criterion relates to the inclusion of three types of variables: those involving the environment (context in the HAAT model), pertinent features of the person’s personality (the human), and the characteristics of the assistive technology itself. The third criterion is the recognition that the user should determine the relative importance of the satisfaction variable. This reflects the highly subjective nature of the user satisfaction measure. The fourth criterion provides for the user to express his or her opinion freely within the constraints of an interview context. Finally, the QUEST was designed to be simple to understand and easy to use by ATPs when evaluating satisfaction. The QUEST requires approximately 30 minutes to administer and is guided by a three-part form.
The first part of the instrument is the general information questionnaire. This form is designed to determine the context in which the user’s satisfaction or dissatisfaction developed. It consists of 18 open-ended questions designed to include the three domains of environment (context [e.g., living arrangements, social supports, funding considerations]), user characteristics (human [e.g., sex, age, nature of disability, types of functional problems]), and assistive technology characteristics (e.g., when the device was acquired, frequency and patterns of use or nonuse, number and types of assistive technologies used).
The second part of the QUEST instrument is an assessment of satisfaction. This includes a set of 27 variables that represents the factors most likely to affect user satisfaction with assistive technologies. Each of the variables represents a specific category, but they are randomly ordered in the presentation to the user. This ensures that the user’s answers are not artificially influenced by the category of the question. Three tasks are used in this part of the evaluation. In the first task, the person is asked the degree of importance that he or she attributes to each variable. Each of the variables is printed on a card. There is a board for classifying the variable from very important (a score of 3) to no importance (0). The evaluator asks the user where he or she would like each card placed and then circles the response on the form. After completing the 27 variables, the user is given an opportunity to add other satisfaction variables that he or she feels are important. This task personalizes the assessment in terms of the individual’s preferences. The second task requires that the evaluator reorganize the variables according to the three categories, and only the variables selected as being quite or very important (scores of 2 or 3) are included. For this task, a six-point scale (0 [very dissatisfied] to 5 [very satisfied]) portrayed on a semicircular dial is used. For each of the variables included from Task 1, the user is asked to indicate his or her satisfaction by moving the dial or instructing the evaluator where to place it. The evaluator then circles the result on the summary form. Finally, the user is asked to express a global satisfaction score for the device. This task, as in Task 1, personalizes the assessment to the individual user. The third and final part of the QUEST requires that the evaluator reorganize the results from Part 2 into the three global categories (environment, person, and assistive technology). Only the values for those variables rated as quite or very important in Task 1 are included. The summary sheet then serves to facilitate the interpretation and use of the data in assessing satisfaction and addressing those areas in which satisfaction is low.
Weiss-Lambrou et al (1999) used the QUEST to determine satisfaction of consumers with seating aids. They describe the application of QUEST to this situation with a group of 24 subjects who used modular seating aids (see Chapter 6). They found that the most important variable (user comfort) was also rated as the least satisfying. This study illustrates the value and importance of a consumer-driven measure of user satisfaction. Weiss-Lambrou et al describe the application of QUEST in this context in detail.
Assistive Technology Abandonment.
One of the most tangible indicators of lack of consumer satisfaction is when the consumer stops using a device although the need for which the device was obtained still exists. This situation is called technology abandonment, and it is useful to look at some of the factors that lead to it. Phillips and Zhao (1993) surveyed more than 200 users of assistive technologies and identified four factors that were significantly related to the abandonment of assistive technologies: (1) failure of providers to take consumers’ opinions into account, (2) easy device procurement, (3) poor device performance, and (4) changes in consumers’ needs or priorities.
More recent research examined personal and social factors that predict assistive technology abandonment. Pape, Kim, and Weiner (2002) conducted a review of the literature related to assistive technology abandonment to look at how the personal meaning attributed to assistive devices influences their integration into the user’s daily life. They found that psychosocial and cultural variables were primary factors in determining the meaning individuals assigned to assistive technology. In particular, their expectations of how the device would function, the social costs of using the device (i.e., cost/benefit of device use), and an outlook that disability did not define the user as a person were the primary factors that contributed to whether a person integrated assistive technology into his or her life (Pape, Kim, and Weiner, 2002). Reimer-Weiss and Wacker (2000) examined factors that predicated assistive technology use in individuals with disability. They found that the relative advantage of the assistive technology in the user’s life and the user’s involvement in the device selection process were predictors of device use or discontinuance.
Scherer et al (2005) have developed a group of measures that help determine the match between the individual and technology. The Matching Person and Technology assessment is described shortly. A recent study examined the validity of the assumptions that guided the development of this instrument. The results of the study supported these assumptions, specifically that personal characteristics related to mood, self-esteem, self-determination and motivation, and psychosocial characteristics related to friend and family support (as examples) were significant predictors of device use (Scherer et al, 2005). Collectively, the earlier studies of Phillips and Zhao (1993) and the more recent work of Pape et al (2002), Reimer-Weiss and Wacker (2000), and Scherer et al (2005) provide evidence that characteristics of the device, the person, and their environment predict whether the client will use a device or abandon it.
Quality of Life as an Assistive Technology Outcome Measure
ATPs, assistive technology suppliers, and assistive technology manufacturers often claim that their services or devices “improve the quality of life” of the consumer. This is an appealing concept. Who wouldn’t want to do this? There are, however, several difficulties with this concept when there is an attempt to actually measure it. In fact, the term quality of life is itself controversial and subject to misuse (Wolfensberger, 1994). Despite these limitations, it is tempting to want to measure quality of life. It is being applied with increasing frequency to outcomes measurement in medicine and rehabilitation (Oldridge, 1996). In a medical service context, quality of life is often related to life expectancy and optimal life quality during the time a person is alive. In rehabilitation the concept of quality of life takes on a bit of a different meaning because the goal is not “repair” or cure but rather maximizing function and independence for the individual. In both cases the concept of health is important. The WHO defines health as “a state of complete physical, mental and social well-being, not merely the absence of disease” (WHO, 1948). Assistive technologies can certainly contribute to both quality of life and a healthy life. Measures designed to assess the degree to which this goal is achieved have begun to emerge over the past decade, and we are in a position to evaluate the assertion that a service or device actually does improve a consumer’s quality of life. Several measures of quality of life are discussed in this section.
Health-Related Quality of Life.
The concept of health-related quality of life (HRQL) refers to the impact of health services on the overall quality of life of individuals, and it represents the functional effect of an illness and its consequent therapy on an individual as perceived by the person receiving the therapy (Oldridge, 1996). It measures one dimension of quality of life. Others are independence, income, adequate housing, and a safe environment. The definition of HRQL is “the value assigned to duration of life as modified by impairment, functional states, perceptions and social opportunities that are influenced by disease, injury, treatment or policy” (Patrick and Erickson, 1993; quoted by Oldridge, 1996). Rehabilitation in general, and assistive technologies in particular, addresses the long-term effects of disease and injury. Therefore both rehabilitation and assistive technology affect HRQL as defined here. However, as Oldridge points out, there are many instruments that have been developed to measure HRQL. Many of these are medically oriented and unsuited to assistive technology outcomes measurement. However, the general concepts underlying HRQL do have relevance to assistive technology outcomes measurement, and there is a need to develop new instruments that are more sensitive to the impact of assistive technologies on HRQL. Oldridge (1996) describes the types of HRQL measurements, their application, and the underlying principles on which this construct is based.
Psychosocial Impact of Assistive Devices Scale.
To address the need for quality of life–related measures in assessing assistive technology outcomes, Day and Jutai (1996) developed the Psychosocial Impact of Assistive Devices Scale (PIADS). The development of the PIADS was based on information obtained through focus groups on the experiences of users of assistive technology (Day and Jutai, 1996). The initial set of constructs was developed and evaluated by a set of users. The scales were modified to include both positive and negative impacts on quality of life of assistive technology users by defining a scale from −3 (maximal negative impact) to +3 (maximal positive impact). The final version of the PIADS is a 26-item self-rating scale intended to measure the impact of rehabilitative technologies and assistive devices on the quality of life of the users of these products. Three subscales are included in the PIADS. These are competence (the effects of a device on functional independence, performance, and productivity), adaptability (the enabling and liberating effects of a device), and self-esteem (the extent to which a device has affected self-confidence, self-esteem, and emotional well-being). This multidimensional aspect of the PIADS contributes to its reliability and validity as a measure of the psychosocial impact of assistive technologies on the consumer.
The PIADS has been applied to measurement of outcomes with a variety of assistive technologies. The original study focused on eyeglass and contact lens wearers (Day and Jutai, 1996). In subsequent studies it has been demonstrated that the subscales of the PIADS remain consistent over populations and types of disabilities (stroke, amyotrophic lateral sclerosis, cerebral palsy) or types of assistive technologies. For example, Jutai et al (2000) used the PIADS to evaluate the psychosocial impact of EADLs (see Chapter 14). The goal of this study was to determine the perceived benefit of EADLs to the consumer’s quality of life. Two groups were included: users of EADLs and those for whom EADLs were appropriate but who had not yet received them. Users’ perceptions were measured at two points 6 to 9 months apart to determine the stability of the perception of psychosocial impact. Jutai et al found that EADLs produced similar degrees of positive impact on users and positive perceptions of anticipated impact on those without EADLs. The two measures of those using EADLs indicated that the psychosocial impact was stable over the time frame used. This study demonstrated the utility of the PIADS as an instrument for quantifying the psychosocial impact of assistive technologies.
Jutai et al (1996) discuss the use of instruments such as the PIADS to evaluate the outcomes of service provision in assistive technologies. The importance of quality-of-life outcome measures, in addition to clinical, functional, and user satisfaction assessments, is demonstrated through a series of case studies related to ease of implementation, clear definition of the desired outcomes, ethical considerations, and responsibility to the user of the assistive technology.
Matching Person and Technology Model.
The Matching Person and Technology (MPT) model and assessment instruments have been developed to allow consumers to prioritize their own outcomes in relation to measurable changes in the perceived quality of life as opposed to the absence of disease or sickness or functional ability (Galvin and Scherer, 1996). This instrument has much in common with the QUEST and PIADS. The developers of the QUEST used the MPT as one of the theoretical bases for their work (Demers, Weiss-Lambrou, and Ska, 1996). As in these other measures, the MPT is a multidimensional instrument that taps domains related to overall impact on quality of life. Three domains are included in the MPT (Galvin and Scherer, 1996). The milieu dimension assesses characteristics of the environment and psychosocial setting in which the assistive technology is to be used. The personality dimension focuses on the individual’s personality, temperament, and preferences. Finally, the technology component addresses characteristics of the assistive technology itself. Like the QUEST and PIADS, the MPT is designed to be applied across a wide range of disabilities and assistive technology types. The multidimensional nature of the MPT makes it possible to separate influences of the technology, environment, and personal preferences. For example, a consumer may have characteristics (goals, skills, and abilities) typically associated with assistive technology nonuse as measured by the milieu/environment variable but may appear to be an optimal user according to characteristics identified for personality and technology. In this case the milieu/environment influences may need to be addressed before the consumer can gain maximal benefit and satisfaction from the use of the assistive technology. Galvin and Scherer (1996) describe the MPT instrument and its application in detail. The MPT has been shown to have reliability and validity in determining the factors related to device abandonment and in assessing the impact on quality of life of assistive technology use.
Relationship of Outcome Measures to the Human Activity Assistive Technology Model
The framework used throughout this text is the HAAT model. This framework is useful in placing the various outcome measures described in an overall structure. Each HAAT element can be related to outcome measures. The activity defines the consumer goals to be achieved on the basis of a consideration of life roles, performance areas, and tasks. There may be several goals for one consumer because he or she has several different life roles (e.g., worker, parent, husband or wife). Goals that are defined form the basis for a consumer-driven outcome assessment. Important questions to be addressed in this domain include (1) was the goal achieved? how well was it achieved? (outcome measures) and (2) were the needs adequately addressed during the assessment to allow definition of goals? (process measure).
Constraints that are placed on the achievement of goals are defined by the HAAT context. This is directly related to the milieu of the MPT and the environment of the QUEST and the adaptability subscale of the PIADS. Outcome measures arising from the context include whether the system is able to function in the required contexts and how well. These may relate to the physical context (e.g., heat or cold, bright light, noisy environment), settings (e.g., home versus employment), or social factors. The inclusion of social factors links the process to society as a whole through cultural considerations (see Chapter 2). One aspect of culture is the funding priorities that are mandated by society’s attitudes toward persons with disabilities. Society as a whole determines funding priorities. If the consumer obtains a system purchased though a particular source, he or she is obligated to comply with the mandate of that funding source. For example, vocational rehabilitation agencies fund services and devices if they are related to employment, and a consumer who receives a computer from this source is obligated to use it for employment rather than for recreation. However, if a consumer uses his or her own money to buy the services or system, he or she can use them as she sees fit. Thus the funding source is linked to the assistive technology system through the social context. The area of funding is discussed further in Chapter 5.
The human component of the HAAT model is directly related to the personality dimension of the MPT, the self-esteem and competence subscales of the PIADS, and the personality feature of the QUEST. Each of these instruments taps a slightly different perspective on the human element of the HAAT model and relates to the overall perception of consumer satisfaction and improvement in quality of life as a result of the acquisition of an assistive technology system.
The desired assistive technology characteristics, the final element of the HAAT model, are defined by the combination of consumer skills, goals, personality, and contextual constraints. The QUEST addresses these through its assistive technology characteristics criterion, the MPT through the technology dimension, and the PIADS through the adaptability subscale. These characteristics are based on the consumer tasks that must be accomplished; the personality, perceptual, and motivational characteristics; and the characteristics of the assistive technology relevant to device use or nonuse. Questions of importance that can be addressed by the various outcome instruments include (1) were the skills accurately determined? (2) were these characteristics able to accommodate for contextual constraints? (3) were the characteristics and associated tasks consistent with the consumer’s skills? and (4) if the identified tasks are successfully completed, is the goal achieved?
Process and structure can also be evaluated by determining how well the needs and goals; human skills, perceptions, and motivation; and contextual constraints described by the HAAT model are identified. The assessment determines the human skills available to meet the goals. One typical process measure is how accurately these skills were determined. An example outcome measure is the degree to which these skills apply to the use of assistive technologies. For example, assume that it is determined during the assessment that a consumer can use a standard keyboard (see Chapter 7). By evaluation of his or her success in performing functional daily tasks with the keyboard, both the outcome and the process can be measured. If the consumer is physically unable to use the keyboard, then the assessment procedures must be reviewed to see whether the assessment process is sound. If the process is all right but an error in ATP judgment was made, then the structure needs to be altered by providing more staff training to increase the likelihood that correct recommendations will be made. When the effectiveness of training is being considered, a process goal, such as the degree to which the consumer has moved from novice to expert status with a given system, can be measured. Alternatively, the consumer may be able to use the keyboard physically, but the total system may not meet his or her needs, so the consumer may be dissatisfied with the overall result. This outcome will have an impact on process and structure as well, but it also may require revision in the system to make it functional.
Conclusions
The effectiveness of the assistive technology system and the efficacy of the ATP to provide services are both measured by their ability to meet the needs of the consumer. Obviously this is appropriate. However, it is easy to lose sight of this emphasis if a program is built from a perspective of “experts” providing a service for consumers rather than collaborating with the consumer, family, and others to meet a goal. The collaborative approach releases the ATP from the burden of having all the answers and accepting total responsibility. Responsibility for successful outcomes is shared with the consumer and others. This avoids the paternalistic protection of the consumer and empowers him or her to take responsibility for the outcome. Each member of the team becomes 100% responsible for success. This encourages cooperation, communication, and interaction, all factors that are essential for effective use of the system. The most effective service is operated from the point of view of establishing desired outcomes and then developing the structure and process to realize them. Too often ATPs and other professionals tend to protect their services from scrutiny rather than welcoming evaluation and its implications for improvement.
The development of appropriate process and outcome measures for assistive technology service delivery is still at an early stage. Since the mid 1990s, however, a number of new tools have been developed and validated and are now available for the ATP to use in evaluating the effectiveness of assistive technology systems. The outcome measures described in this chapter have been developed to allow determination of skills, abilities, and motivation; functional performance requirements and skill levels; consumer satisfaction with the recommended system; and overall impact on the quality of life of the consumer and significant others. Each of these measures has been developed and validated to focus on different aspects of assistive technology outcomes. As demonstrated, several of these have common characteristics. Work is under way to relate three measures, the PIADS, QUEST, and MPT, to each other and to develop a common understanding of the important variables leading to successful assistive device application and use (Jutai, 2001). Continued research and development, particularly on the psychosocial aspects of assistive technology use and nonuse, will continue to inform our assessment of outcome measures and the development of assistive technologies that are more effective in meeting the needs of consumers.
SUMMARY
This chapter describes the principles of assessment and intervention and the service delivery process to the consumer. The steps in the process include referral intake, needs assessment, evaluation, recommendation, implementation, follow-up, and follow-along. The current state of outcome measurement in the field of assistive technology is also discussed.
Study Questions
1. Describe the five principles for assistive technology assessment and intervention.
2. Distinguish between quantitative and qualitative assessment procedures.
3. What are the four methods of gathering assessment information?
4. What is the difference between clinical and formal assessment procedures?
5. What is the meaning of the term criteria for service as used in assistive technology referral?
6. List the steps involved in assistive technology service delivery and write a brief description of each one. Which of these steps is the most important? Justify your choice.
7. Describe the difference between opportunity barriers and access barriers. Give an example of each.
8. List three types of opportunity barriers and how they can be addressed during the assessment process.
9. What consumer skills do we evaluate during the assistive technology skills assessment?
10. Describe the ideal relationship between the consumer and the assistive technology practitioner in the assessment and recommendation process for assistive technologies.
11. What visual functions do we measure during the sensory assessment, and how does each of these apply to the use of assistive technologies?
12. Describe the major components of a physical evaluation.
13. What are the major areas that are assessed in the cognitive evaluation for assistive technologies? Why do you think these areas were chosen?
14. Why is a separate “device characteristics” section included in the assessment? What are the outcomes of this portion of the evaluation?
15. Who are the audiences for the written assessment report? What challenges does this present?
16. Describe the major steps in implementation of an assistive technology system.
17. What are the major types of performance facilitators? When is each type used? What is the role played by each?
18. What are the major goals of a follow-up program, and how does this differ from follow-along?
19. What is the difference between repair and maintenance?
20. What are the three major domains in which outcome measures are used in assistive technology service delivery?
21. How do the three measurement domains of Question 20 relate to an improvement in the service delivery process?
22. What are the limitations in the use of the Functional Independence Measure(Instrument for assessing the outcome of assistive technology interventions?
23. What are the strengths of the COPM in relation to determination of consumer needs and satisfaction?
24. Describe the major features of the QUEST and how it is used to assess user satisfaction.
25. What are the most common reasons that consumers abandon technology?
26. What is the HRQL, and how is it related to assistive technology outcome measures?
27. What are the three subscales of the PIADS? Why does the inclusion of these three scales increase the usefulness and validity of the PIADS?
28. Describe the relationship of the four HAAT model components to the outcome measures described in this chapter.
29. What are the roles and responsibilities of the ATP in determining the effectiveness of assistive technology services and devices?