Introduction and Overview
ASSISTIVE TECHNOLOGIES: A WORKING DEFINITION
Definition of Assistive Technology Devices and Services
Characterization of Assistive Technologies
Assistive Versus Rehabilitative or Educational Technologies
General Versus Specific Technologies
Commercial to Custom Technology
HISTORICAL PERSPECTIVE ON ASSISTIVE TECHNOLOGY DEVICES AND SERVICES
(Very) Early Developments in Assistive Technologies
Evolution of State-of-the-Art Assistive Technology
U.S. Federal Legislation Affecting the Application of Assistive Technologies
Rehabilitation Act of 1973 (Amended)
Americans With Disabilities Act (ADA) of 1990
Individuals With Disabilities Education Act Amendments of 1997 and 2004
Elementary and Secondary Education Act (2001 Reauthorization)
Assistive Technology Act of 1998, as Amended (2004)
Developmental Disabilities Assistance and Bill of Rights Act
ASSISTIVE TECHNOLOGY INDUSTRY TODAY
Consumer and Direct Consumer Services
Characteristics of Direct Consumer Service Programs
Distribution of Hard Technologies
PROFESSIONAL PRACTICE IN ASSISTIVE TECHNOLOGY
Providers of Assistive Technology Services
Ethics and Standards of Practice
Code of Ethics for Assistive Technologies: The RESNA Code of Ethics
Standards for Service Providers
On completing this chapter, you will be able to do the following:
2 Delineate the characteristics of assistive technologies
3 Describe the history of assistive technology practice
4 List the major legislative initiatives that have affected the application of assistive technologies
5 Describe the components of the assistive technology industry
6 Explain the roles of the consumer
7 Identify several distinguishing features of service delivery programs
8 Identify the professionals who may work as assistive technology practitioners
9 Understand the transdisciplinary approach to assistive technology service delivery
10 Discuss the major professional issues in assistive technology practice
In the last 25 to 30 years there has been major growth in the application of technology in ameliorating the problems of persons with disabilities. Until the publication of the first edition of this book in 1994, there was no unified set of principles for this application of technology. This chapter begins by providing an overview of assistive technologies and the industry that supports their development and distribution. A brief historical perspective and a summary of the major United States federal legislation that provides the mandate for assistive technologies are also presented.
ASSISTIVE TECHNOLOGIES: A WORKING DEFINITION
The document International Classification of Functioning, Disability, and Health (ICF) describes a system developed by the World Health Organization (WHO) that is designed to describe and classify health and health-related states. These two domains are described by body factors (body structures and functions) and individual and societal elements (activities and participation) (WHO, 2001). It is a revision of the previous classification system, described in the International Classification of Impairments, Disabilities, and Handicaps (ICIDH) (WHO, 1980). Two primary shifts in philosophy discriminate between the ICIDH and the ICF classification systems: the recognition of the importance of the environment as a mediating factor in the performance of daily function and the use of more positive language (i.e., the construct of function replaces that of disability).
Body structures and function refer to the structural and physiological functions of the body. For example, the classification relating to vision lists the anatomical structures of the eye and the sensory and motor and perceptual elements of vision. Activity and participation are considered to be a single classification. There is much debate on whether it is possible to differentiate between an activity and participation. Something that may be considered participation at one stage in life becomes an activity at a later stage. The ICF defines activities as the “execution of tasks” and participation as “involvement in life situations” (WHO, 2001, p. 10). Examples of the different components of activity and participation include learning and applying knowledge, communication, mobility, self-care, and community, social, and civic life.
The ICF recognizes two contextual factors that modify health and health-related states: environment and personal factors (WHO, 2001). The latter are not classified but merely identified and include age, sex, race, lifestyle habits, and social and cultural backgrounds, among other factors. The inclusion of these factors in the ICF recognizes their ability to influence differentially the outcome of the same impairment in two individuals.
The ICF does classify environmental elements. Assistive technologies are located in this classification, most prominently in the products and technology chapter. They are specifically mentioned related to activities of daily living, mobility, communication, religion, and spirituality and in specific contexts such as education, employment and culture, recreation, and sport (WHO, 2001). Many of the remaining environmental chapters have implications to assistive technology, although it is not mentioned explicitly. These chapters include access to public and private buildings, the natural and built outdoor environments, people and animals that provide physical and emotional support (personal care attendants and health care professionals are identified here; service animals are not), attitudes of individuals and others and services, systems, and policies, that include legislation (WHO, 2001). Scherer and Glueckauf (2005) reviewed the ICF and discussed the implications to provision of assistive technologies. They concluded that the revised classification system puts the onus on the assistive technology provider to demonstrate positive outcomes for assistive technology recommendations and use.
Definition of Assistive Technology Devices and Services
Dictionaries provide the following definition of technology: (1) the science or study of the practical or industrial arts, (2) applied science, and (3) a method, process, and so forth for handling a specific technical problem (Guralnik, 1979; McKechnie, 1983).
Surprisingly, none of these definitions says anything about a “device”; instead the emphasis is on the application of knowledge. This is an important concept, and the term assistive technology will be used to refer to a broad range of devices, services, strategies, and practices that are conceived and applied to ameliorate the problems faced by individuals who have disabilities.
Within this framework there are many ways to define assistive technologies. One widely used definition is that provided in Public Law (PL) 108-364 the Assistive Technology Act of 1998, as amended (2004). The definition of an assistive technology device in this law is as follows:
Any item, piece of equipment or product system whether acquired commercially off the shelf, modified, or customized that is used to increase, maintain or improve functional capabilities of individuals with disabilities.
This definition has several important components, and because it will be used as a working definition throughout this book, these components will be examined in some detail. First, the definition includes commercial, modified, and customized devices. By including all types of devices, the statute encompasses an extremely wide range of applications. Second, this definition emphasizes functional capabilities of individuals with disabilities. Functional outcomes are the only real measure of the success of assistive technology devices, and throughout this text the importance of providing technologies that result in increased functional capability is stressed. Finally, the emphasis on individual persons with disabilities underscores the importance of treating each application of technology as a unique circumstance. No two applications are exactly the same in terms of the needs and skills of the person being served, the activities to be accomplished, and the context in which the application takes place.
PL 108-364 also defines an assistive technology service as any service that directly assists an individual with a disability in the selection, acquisition, or use of an assistive technology device. The law includes several specific examples that further clarify this definition: (1) evaluating needs and skills for assistive technology, (2) acquiring assistive technologies, (3) selecting, designing, repairing, and fabricating assistive technology systems, (4) coordinating services with other therapies, and (5) training both individuals with disabilities and those working with them to use the technologies effectively. This definition demonstrates the broad spectrum of services inherent in the delivery of assistive technologies.
Characterization of Assistive Technologies
In this section a characterization of assistive technologies is presented from several points of view. Each of these is a logical outgrowth of the definitions presented earlier, and each is useful in the process of applying assistive technologies. Box 1-1 shows several classifications used to distinguish different types of assistive technologies.
Assistive Versus Rehabilitative or Educational Technologies.
Technology can serve two major purposes: helping and teaching (Smith, 1991). Technology that helps an individual to carry out a functional activity is termed assistive technology. Our emphasis in this text is on assistive technologies that serve a variety of functional needs. Technology can also be used as part of an educational or rehabilitative process. In this case the technology is usually used as one modality in an overall education or rehabilitation plan. Technology in this sense is used as a tool for remediation or rehabilitation rather than being a part of the person’s daily life and functional activities, and it will be referred to it as rehabilitative or educational technology, depending on the setting. Often rehabilitative or educational technology (e.g., cognitive retraining software) is used to develop skills for the use of assistive technologies, and some of these applications are discussed in later chapters. A benefit of characterizing assistive technologies is that funding programs have targeted goals that require technology to meet specific purposes and items that can be described in a manner consistent with those purposes will be approved for funding.
Low to High Technology.
The next of these distinctions is between low- and high-technology devices. Although this distinction is imprecise, inexpensive devices that are simple to make and easy to obtain are often described as “low” technology and devices that are expensive, more difficult to make, and harder to obtain as “high” technology. According to this distinction, examples of low-technology devices are simple pencil and paper communication boards, modified eating utensils, and simple splints. Wheelchairs, electronic communication devices, and computers are examples of high-technology devices.
Hard and Soft Technologies.
The PL 108-364 definition of an assistive technology device applies primarily to hard technologies as they are defined here. The main distinguishing feature of hard technologies is that they are tangible. Odor (1984) has distinguished between hard technologies and soft technologies. Hard technologies are readily available components that can be purchased and assembled into assistive technology systems. This includes everything from simple mouth sticks to computers and software. On the other hand, soft technologies are the human areas of decision making, strategies, training, concept formation, and service delivery as described earlier in this chapter. Soft technologies are generally captured in one of three forms: (1) people, (2) written, and (3) computer (Bailey, 1996). These aspects of technology, without which the hard technology cannot be successful, are much harder to obtain. Assistive technology services as defined in PL 108-364 are basically soft technologies. Soft technologies are difficult to acquire because they are highly dependent on human knowledge rather than on tangible objects. This knowledge is obtained slowly through formal training, experience, and textbooks such as this one. The development of effective strategies of use also has a major effect on assistive technology system success. Initially the formulation of these strategies may rely heavily on the knowledge, experience, and ingenuity of the assistive technology practitioner. With growing experience, the assistive technology user originates strategies that facilitate successful device use. The roles of both hard and soft technologies as integral portions of assistive technology systems are discussed in the section on activities in Chapter 2.
Appliances Versus Tools.
An appliance is a device that “provides benefits to the individual independent of the individual’s skill level” (Vanderheiden, 1987, p. 705). Tools, on the other hand, require the development of skill for their use. Household appliances such as refrigerators do not require any skill to operate, whereas tools such as a hammer or saw do require skill. This same criterion applies to assistive technologies. The determining factor in distinguishing a tool from an appliance is that the quality of the result obtained using a tool depends on the skill of the user. For example, eyeglasses, splints, a seating system, or a keyguard for a computer are all appliances because the quality of the functional outcome does not depend on the skill of the user. On the other hand, success in maneuvering a powered wheelchair does depend on the skill of the user; therefore the wheelchair is classified as a tool. Examples of assistive technology tools and appliances are shown in Table 1-1.
TABLE 1-1
Examples of Assistive Technology Tools and Appliances
| Topic (Chapter No.) | Appliances | Tools |
| Control interfaces (7) | Keyguards | Joystick |
| Computer access (7) | Enlarging lens | Enlarged keyboard |
| Augmentative communication (11) | — | Alphabet board |
| Manipulation (14) | Environmental control* | Electric feeder |
| Mobility (12) | Wheelchair armrest | Manual wheelchair push rims |
| Sensory (8) | Eyeglasses | Long cane |
*See text; classification depends on electronic aid for daily living and its functions.
In some instances the device may be a tool or an appliance, depending on how it is set up to be used. For example, an electronic aid to daily living (formerly called an environmental control system) that controls lights or appliances (see Chapter 14) requires a relatively complex set of electronic circuits that most would agree are high tech. However, this system can be set up so that the only skill required to operate it is to turn it on or off, in which case it may be considered an appliance. In other instances this system may require the user to learn a sophisticated method of scanning to operate it; the system would then be considered a tool. It is important to note that an appliance that requires user skill because it is poorly designed is not considered a tool.
As Vanderheiden (1987) points out, the successful use of assistive technology tools requires training, strategies, and special skills. These are soft technologies. For example, learning aids that facilitate the use of an assistive device are tools that are used only until the user gains sufficient skill to use the device independently. However, the use of the learning aid requires skill, and this aid is therefore a tool. Strategies for the use of an assistive device require skill and are therefore properly categorized as tools. Both appliances and tools require careful assessment, recommendation, and fitting (see Chapter 4), but only the tool also requires skill development (Vanderheiden, 1987). If training of care providers is included, as well as the consumer of the technology, then training also may be necessary for appliances. For example, when a new seating system is provided (Chapter 6), the care staff must be trained in how to position the person in the seating system. By including soft technologies in our concept of a tool, the importance of developing these skills together with the acquisition of the basic hard technology tool or appliance is emphasized.
Another important point raised by Vanderheiden (1987) is that the tools used by persons with disabilities are often different from those used by the general population, which means that, to develop skill, the assistive technology user often cannot observe someone using the same device. People routinely use observation, such as watching someone using a hammer, as a means of learning how to use a tool. When the person with a disability is the only one in that environment who is using the tool, he or she must rely more heavily on personal experience and formal training to learn to use it effectively. Increasingly, people with disabilities who are expert users of a particular type of assistive technology are serving as mentors to novice users.
Minimal to Maximal Technology.
Assistive technologies are specified and designed to meet a continuum of needs. At one extreme are devices that provide some assistance or that augment the individual’s ability to perform a task. For example, an individual with cerebral palsy may be able to speak, but on occasion his or her speech may be difficult to understand. In those instances the individual may clarify speech by using a letter board to spell out words not understood. Or a person with respiratory problems may be able to ambulate inside the house but, because of low endurance, may require a powered wheelchair to be able to do grocery shopping independently. In fact, many grocery stores now provide powered carts for individuals who need this type of augmented mobility. At the other extreme are maximal assistive technologies that replace significant amounts of ability to generate functional outcomes. For example, some individuals have no verbal communication ability and may require a device to be able to communicate. Likewise, some individuals are totally dependent on a manual or powered wheelchair for personal mobility.
Minimal technologies generally augment rather than replace function. Classically, devices that augment have been termed orthoses or orthotic devices. Although this term originally referred to orthopedic braces of various types, it has been broadened to include all devices that assist or augment function. The term prosthetics or prosthetic device originally was used to describe devices that replaced a body part both structurally and functionally. Now this term has also been broadened to include all devices that provide a functional replacement.
General Versus Specific Technologies.
Assistive technologies are differentiated according to whether they are used in many different applications or whether they are intended for a specific application. General-purpose assistive technologies include (1) seating and positioning systems, (2) control interfaces, and (3) computers. These are classified as general purpose because they are used across a wide range of applications. Body position affects the way an individual uses the assistive technology. Frequently, external support systems, an assistive technology, are necessary to achieve a body position that facilitates functional activities. Control interfaces are the means by which the user interacts with any assistive technology. Examples include the joystick on a powered wheelchair, the keyboard on a computer, or the handle that operates the closing mechanism on a reacher. Virtually every electronic assistive technology has a computer incorporated into it. Computers enhance the flexibility and the breadth of application of these devices. Thus computers are also included as general-purpose technologies.
Specific-purpose assistive technologies facilitate performance in one unique application area. Examples include devices for communication, manual and powered wheelchairs, feeding devices, hearing aids, and mobility aids for persons with visual impairments. Because these devices are intended for a specific use, it is possible to design them to maximize their capabilities to meet a particular need.
Commercial to Custom Technology.
Another distinction shown in Box 1-1 is between commercially available devices and those that are custom made for an individual. There is actually a continuum from commercial devices (designed for the general public and designed for persons with disabilities), to modification of a commercial device, and finally to making a completely customized device.
Figure 1-1 illustrates the progression from commercially available devices to those that are completely customized for an individual. The term commercially available is used to refer to devices that are mass produced. These include commercial devices designed for the general population (standard commercially available devices) and assistive technologies (special commercially available devices), which are mass-produced devices designed for individuals with disabilities. For example, standard personal computers designed for the general population are often used by persons with disabilities. Increasingly, commercial products are being designed according to the principles of universal design: the design of products and environments to be usable by all people, to the greatest extent possible, without the need for adaptation or specialized design (North Carolina State University Center for Universal Design, 2001). In this approach, features that make a product more useful to persons who have disabilities (e.g., larger knobs; a variety of display options—visual, tactile, auditory; alternatives to reading text—icons, pictures) are built into the product. This approach is much less expensive than modifying a product after production to meet the needs of a person with a disability. In some cases (e.g., telecommunications equipment) this universal design approach is mandated by federal regulations. In some countries, universal design is known as “design for all.” The North Carolina State University Center for Universal Design, in conjunction with advocates of universal design, has compiled a set of principles of universal design, shown in Box 1-2. This center also maintains a Web site on universal design (www.design.ncsu.edu/cud).
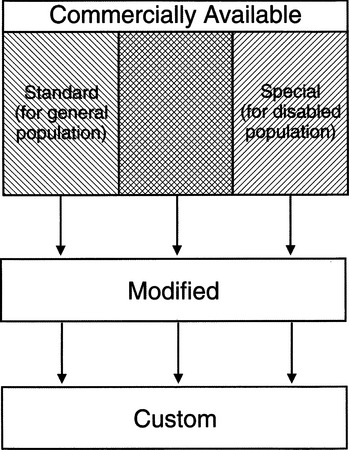
Figure 1-1 The progression from commercially available devices for the general population and commercially available devices for special populations to modified devices and custom devices.
When an individual’s needs for assistive technology cannot be met with a commercial device, special devices that are mass produced and commercially available for persons with disabilities can be attempted. Examples include wheelchairs, augmentative communication systems, and many aids to daily living. In some cases a combination of standard and special-purpose technologies are used; this is represented by the cross-hatched area of Figure 1-1. For example, a standard general-purpose computer may be used with special-purpose software to create an augmentative communication device (see Chapter 11).
If commercially available devices cannot meet an individual’s needs, one may be modified to fit. This modification can vary from simple to very complex. For example, if an individual has difficulty using the keys on a computer keyboard, software that facilitates its use can be purchased. In this case the most expensive and complex part of the system (the computer) is a standard commercial product, and the software is the simplest and least expensive portion of the system. However, the software may have a cost that is much higher than expected relative to its simplicity because it is a special product and all the costs of development must be recovered from the small production run. A special commercially available device may be modified as well. For example, a commercially available augmentative communication device may require modification so that it can be mounted on a user’s wheelchair.
When no commercial device or modification is appropriate, it is necessary to design one specifically for the task at hand. This approach results in a custom device. Because they are mass produced, commercial devices have a lower per unit cost than do custom devices. For example, seating and positioning systems for persons with severe disabilities may be individually contoured to achieve the necessary functional result, which can increase the cost (see Chapter 6).
Another important difference between modified or custom devices and commercial devices is the level of technical support that is available with each. A commercially produced device generally has written documentation and operator’s manuals available. Although the quality of these written materials varies widely, some documentation is better than none, and modified or custom devices often have none. The manufacturer or supplier of commercial equipment provides technical support and repair. Because modified or custom devices are one of a kind, technical support may be hard to obtain, especially if the original designer and builder is no longer available (e.g., if the user moves to a new area).
Summary
Assistive technology can be characterized in many ways. It is useful to realize, however, that yesterday’s high tech is tomorrow’s low tech, custom devices become commercial if more than a few people need them, and appliances often enable the use of tools. Thus no good categorization is perfect or static. As the field advances, there will be new considerations that will further stretch our concepts and force new ways of categorizing and describing assistive technologies.
HISTORICAL PERSPECTIVE ON ASSISTIVE TECHNOLOGY DEVICES AND SERVICES
(Very) Early Developments in Assistive Technologies
Although it is tempting to view assistive technologies and the assistive technology industry as innovations that have occurred over the past 30 years, to really investigate the origins of this field, it is necessary to go back much further in time. Imagine that we are in the Stone Age. Our friend Borg has broken his leg on a hunting expedition. Because there is no plaster yet available, his leg is not placed in a plaster cast, and when it heals he has a decided limp. Determined to continue providing for his clan, he reaches for the nearest stick to assist his walking. Thus one of the first assistive technology devices is conceived, fabricated, and put into use. At that time this custom device is referred to as “high tech” because of its advanced design and its use of state-of-the-art materials. As time moves on, Borg’s descendants begin to realize that assistive technologies can help meet other needs. His great-granddaughter, Myra, now in her later years, discovers that an empty animal horn can be used to make voices louder and help compensate for her fading hearing. One of the first uses of the wheel, a new invention that will be reinvented many times over the years, is to transport people. This key component of the current wheelchair is surprisingly similar to its predecessor. Most important, each version emphasizes function rather than form or style. Borg’s walking stick also bears a strong resemblance to present-day canes and crutches. However, Myra’s animal horn is only functionally related to the modern-day hearing aid. There is little structural relationship between these two devices, which brings us to the next major point in the history of assistive technologies.
Evolution of State-of-the-Art Assistive Technology
Assistive technologies have always been based on the materials and state-of-the-art technology available to the practitioners. In assistive technologies functional outcomes are emphasized above all other considerations. For this reason, some applications have had little change for many years. Borg’s cane is one example; although the structure has remained the same, the materials have changed. However, other applications have only been possible as technologies have advanced.
During the Civil War in the United States, great strides were made in the development of prostheses, especially for the lower limb. Sockets were improved, creating a better fit and more functional outcome. A socket developed by Parmelee in 1863 featured the first suction attachment of a lower limb prosthesis (Murphy, Cook, and Harvey, 1982). This type of socket, still used in modern prostheses, eliminated discomfort caused by pelvic attachment bands and reduced alignment problems and the risk of breakage at the joint. The materials used in 1863, however, bear little resemblance to those used today. Current prostheses use composite metals and plastics, whereas Parmelee’s device was made of wood and leather.
Miniature electronic circuits only available in the past 35 years have replaced Myra’s horn. However, hearing aids were first patented in the 1890s, and the major function of amplifying sound has not changed over the years. What has changed is the structure of these aids. Now they fit into the ear, amplify a wider range of sounds, and are generally more effective (see Chapter 9). In the 1890s these aids were bulky and produced much lower fidelity. It was a long time between Myra’s horn and the first hearing aids in the 1890s, but in the last 100 years the state of the art in this field has changed dramatically.
In some cases, current assistive technology applications were not possible as few as 15 years ago. The well-documented revolution in electronics is the reason for most of these gains, and computers are the vehicle by which the advancements have been made. The single most important change in computer design and construction was the reduction in complexity brought about by the development of the microprocessor electronic circuit “chip.” This innovation, the microprocessor, resulted in reduced size (from a room full of electronics to a typewriter-sized device), reduced cost (affordable by an individual), and greatly increased functional capabilities. Although computers are usually thought of as stand-alone personal systems, microprocessors are built into a large number of devices, from computer printers to microwave ovens and other household appliances. These chips also make possible such important innovations as synthesized speech (see Chapters 8, 10, and 11), robotic aids (see Chapter 14, and computer graphics, all of which play major roles in assistive technology applications. It is difficult to find assistive technology applications in any functional performance area that have not been affected by microcomputer advances. Even in the area of seating and positioning, computer technology is being used for the design and manufacture of custom seat cushions (see Chapter 6). Throughout the remainder of this book the most important of these applications are described.)
U.S. Federal Legislation Affecting the Application of Assistive Technologies
Although industrial advancements and competition have driven the recent development of assistive technology devices, the development of assistive technology services and service delivery in the United States has been affected significantly by federal legislation. In this section only the recent legislation that has most directly affected the development and application of assistive technologies is discussed. Each of the major pieces of legislation that is discussed is summarized in Table 1-2. For the complete text of any federal law, refer to the Library of Congress’s “Thomas” Web site at www.thomas.loc.gov/. Specific information on U.S. legislation related to assistive technologies is available on the Rehabilitation Engineering and Assistive Technology Society of North America (RESNA) Web site at www.resna.org.
TABLE 1-2
Recent Major U.S. Federal Legislation Affecting Assistive Technologies
| Legislation | Major Assistive Technology Impact |
| Rehabilitation Act of 1973, as amended | Mandated reasonable accommodation in all federally funded programs; requires both assistive technology devices and services be included in state vocational rehabilitation services plans and IPE for each client; Section 508 mandates equal access to electronic office equipment for all federal employees; defines rehabilitation technology as rehabilitation engineering and assistive technology devices and services; mandates rehabilitation technology as primary benefit to be included in IPE |
| Individuals with Disabilities Education Act Amendments of 1997 | Recognized the right of every child to a free and appropriate education; included concept that children with disabilities are to be educated with their peers; extended reasonable accommodation, least restrictive environment, and assistive technology devices and services to age 3-21 years; mandated IEP for each child, to include consideration of assistive technologies; also included mandated services for children from birth to 2 years and expanded emphasis on educationally related assistive technologies |
| Assistive Technology Act of 1998, as amended (replaced Technology Related Assistance for Individuals With Disabilities Act of 1988) | First legislation to specifically address expansion of assistive technology devices and services; mandates consumer-driven assistive technology services, capacity building, advocacy activities, and statewide system change; supports grants to expand and administer alternative financing of assistive technology systems |
| Developmental Disabilities Assistance and Bill of Rights Act | Provides grants to states for developmental disabilities councils, university-affiliated programs, and protection and advocacy activities for persons with developmental disabilities; provides training and technical assistance to improve access to assistive technology services for individuals with developmental disabilities |
| Americans With Disabilities Act of 1990 | Prohibits discrimination on the basis of disability in employment, state and local government, public accommodations, commercial facilities, transportation, and telecommunications, all of which affect the application of assistive technology; use of assistive technology affects requirement that Title II entities must communicate effectively with people who have hearing, vision, or speech disabilities; addresses telephone and television access for people with hearing and speech disabilities |
| Medicaid | Income-based (“means-tested”) program; eligibility and services differ from state to state; federal government sets general program requirements and provides financial assistance to the states by matching state expenditures; largest funding source for assistive technology benefits among all funding programs; benefits may vary from state to state for adults; assistive technology for adults must be included in state’s Medicaid plan or waiver program |
| Medicare | Major funding source for assistive technology (durable medical equipment); includes individuals aged 65 years or more and those who are permanently and totally disabled; federally administered with consistent rules for all states |
In the United States, as shown in Table 1-3, statutes can be organized into two groups. The first group is statutes that provide structure to society by prohibiting discrimination and thereby facilitate access to or use of assistive technologies. This group includes Section 504 of the Rehabilitation Act of 1973 and the Americans With Disabilities Act. The second group includes those statutes that provide actual services that may include assistive technologies. This group includes the Individuals With Disabilities Education Act and health programs such as Medicaid and Medicare. Some statues appear in both categories.
TABLE 1-3
Groups of U.S. Legislation Related to Assistive Technologies
| Category | Legislation |
| Statutes that facilitate access to or use of assistive technologies by providing structure to society by prohibiting discrimination | Section 504 of the Rehabilitation Act of 1973 |
| Section 508 of the Rehabilitation Act of 1973 | |
| Americans With Disabilities Act | |
| The Developmental Disabilities Assistance and Bill of Rights Act | |
| Statutes that provide services that may include assistive technologies | Sections of the Rehabilitation Act of 1973 |
| Individuals With Disabilities Education Act | |
| Medicaid and Medicare | |
| The Developmental Disabilities Assistance and Bill of Rights Act |
Rehabilitation Act of 1973 (Amended).
The Rehabilitation Act of 1973 established several important principles on which subsequent legislation has been based. The most far-reaching of these principles are nondiscrimination and reasonable accommodation. Section 504 of the Rehabilitation Act prohibits any activity receiving federal funds from discriminating solely on the basis of disability. To remedy discrimination, federally funded activities and programs must offer reasonable accommodations to facilities, programs, and benefits to ensure that people with disabilities have equal access and equal opportunity to derive benefits. As a result of the wide reach of federal funding, the nondiscrimination provisions of the Rehabilitation Act of 1973 compelled universities—recipients of many different types of federal funding—and local and state governments, and others to make architectural changes to campuses, public buildings, sidewalks, and museums to reduce barriers. Elevators were added to buildings, ramps and curb cuts were made to accommodate wheelchair users, and voice and Braille labels were added to signs (including elevators) to provide access for visually impaired persons. State and local programs that provide medical, social, recreational, and other services also had to make changes to ensure that people with disabilities had equal access to the programs and their benefits. The Rehabilitation Act’s nondiscrimination provisions also extend to the activities of the federal government itself. Many of these efforts to accommodate individuals with disabilities involved the use of assistive technologies.
The Rehabilitation Act amendments of 1998, which are contained in the Workforce Investment Act of 1998 (PL 105-220), are the most recent amendments to the Rehabilitation Act. This act was also amended in 1986 (PL 99-506), 1992 (PL 102-569), and 1993 (PL 103-73). Together they include several provisions involving assistive technology. First the amendments require that each state include within its vocational rehabilitation plan a provision for assistive technology (referred to in PL 99-506 as rehabilitation engineering or technology and in PL 105-220 as rehabilitation technology). PL 99-506 defined rehabilitation engineering as the systematic application of technologies, engineering methods, or scientific principles to meet the needs of and address the barriers confronted by individuals with disabilities in areas that include education, rehabilitation, employment, transportation, independent living, and recreation. The term includes rehabilitation engineering, assistive technology devices, and assistive technology services (29 U.S.C. § 705[30]).
Because this plan is the basis by which states receive federal funding for vocational rehabilitation, there is a strong incentive to provide these technology-related services. The Rehabilitation Act also requires that provision for acquiring appropriate and necessary assistive technology devices and services be included in Individualized Written Rehabilitation Programs (IWRPs), renamed in the 1998 amendments as “Individualized Plans for Employment” (IPE), which are written for individuals with disabilities.
A third Rehabilitation Act provision with important assistive technology implications is Section 508. First added in the 1986 amendments and later strengthened in the 1998 amendments, this section was developed to ensure access to “electronic office equipment” by persons with disabilities who work for the federal government. Although limitation to the federal government may seem to be so restrictive as to severely reduce the impact of the law, the federal government is such a large purchaser of computers and other office technology that any purchasing specifications it makes take on the role of informal standards. This legislation has had a significant influence on the design and manufacture of computers and their accessibility to persons with disabilities. Persons who are blind or have low vision and those with difficulty in accessing the keyboard have benefited from standards derived as a result of Section 508, and several manufacturers have included technology that increases access in the basic designs of their computer systems. Many of these features are discussed further in Chapters 7 and 8.
The major intent of Section 508 is that electronic and information technology developed, procured, maintained, or used by the federal government be accessible to people with disabilities. Section 508 applies to federal departments and agencies. It covers access to electronic office equipment and electronic information services provided to the public by the federal government. This provision includes ensuring that end users with disabilities (1) have access to the same databases and application programs as other end users, (2) are supported in manipulating data and related information resources to attain equivalent end results as other end users, and (3) can transmit and receive messages using the same telecommunication systems as other end users. The U.S. Architectural and Transportation Barriers Compliance Board is now developing standards for Section 508. The guidelines accompanying Section 508 also detail the functional performance specifications for electronic office equipment accessibility. Because of provisions in the former Technology Act, now the Assistive Technology (AT) Act of 1998 (see p. 14), states and territories that receive AT Act funding and all subrecipients must comply with.
Americans With Disabilities Act (ADA) of 1990.
The Americans with Disabilities Act (ADA, PL 101-336) prohibits discrimination on the basis of disability in employment, state and local government, public accommodations, commercial facilities, transportation, and telecommunications. It also applies to the U.S. Congress. To be protected by the ADA, an individual must meet the following ADA definitions of disability: a person who has a physical or mental impairment that substantially limits one or more major life activities, a person who has a history or record of such an impairment, or a person who is perceived by others as having such an impairment. The ADA does not specifically name all the impairments that are covered. The ADA has four main titles: Title I (employment), Title II (state and local government agencies and public transportation), Title III (public accommodations), and Title IV (telecommunications), all of which affect the application of assistive technology.
The prohibition of employment discrimination on the basis of disability stated in Title I of the ADA requires employers with 15 or more employees, including religious entities with 15 or more employees, to provide qualified individuals with disabilities an equal opportunity to benefit from the full range of employment-related opportunities available to others. For example, it prohibits discrimination in recruitment, hiring, promotions, training, pay, fringe benefits, and other privileges of employment. It restricts questions that can be asked about an applicant’s disability before a job offer is made. Many issues of employment involve the use and application of assistive technology because Title I of the ADA requires that employers make reasonable accommodation to the known physical or mental limitations of otherwise qualified individuals with disabilities unless it results in undue hardship. The application of Title I to employee fringe benefits protects employees with disabilities or family members with disabilities from discrimination in the provision of health insurance benefits, which is an important funding source for assistive technologies.
Title II covers all activities of state and local governments regardless of the government entity’s size or receipt of federal funding. Title II requires that state and local governments give people with disabilities an equal opportunity to benefit from all their programs, services, and activities (e.g., public education, employment, transportation, recreation, health care, social services, courts, voting, and town meetings).
State and local governments are required to follow specific architectural standards in the new construction and alteration of their buildings. They also must relocate programs or otherwise provide access in inaccessible older buildings. In addition, the use of assistive technology such as specialized computer software affects the requirement that Title II entities must communicate effectively with people who have hearing, vision, or speech disabilities, which includes screen readers, enlarged computer screens, and augmentative and alternative communication devices. Public entities are not required to take actions that would result in undue financial and administrative burdens. They are required to make reasonable modifications to policies, practices, and procedures where necessary to avoid discrimination unless they can demonstrate that doing so would fundamentally alter the nature of the service, program, or activity being provided.
The transportation provisions of Title II cover public transportation services, such as city buses and public rail transit (e.g., subways, commuter rails, Amtrak). Public transportation authorities may not discriminate against people with disabilities in the provision of their services. They must comply with requirements for accessibility in newly purchased vehicles, make good faith efforts to purchase or lease accessible used buses, remanufacture buses in an accessible manner, and, unless it would result in an undue burden, provide paratransit where they operate fixed-route bus or rail systems. Paratransit is a service in which individuals who are unable to independently use the regular transit system (because of a physical or mental impairment) are picked up and dropped off at their destinations.
Title III covers businesses and nonprofit service providers that are public accommodations, privately operated entities offering certain types of courses and examinations, and privately operated transportation and commercial facilities. Public accommodations are private entities that own, lease, lease to, or operate facilities such as restaurants, retail stores, hotels, and movie theaters; private schools; convention centers; physicians’ offices; homeless shelters; transportation depots; zoos; funeral homes; day care centers; and recreation facilities, including sports stadiums and fitness clubs. Transportation services provided by private entities are also covered by Title III.
Public accommodations must comply with basic nondiscrimination requirements that prohibit exclusion, segregation, and unequal treatment. They also must comply with specific requirements related to architectural standards for new and altered buildings and reasonable modifications to policies, practices, and procedures. In addition, public accommodations must use assistive technology for their requirement to offer effective communication for people with hearing, vision, or speech disabilities as well as other access requirements. Additionally, public accommodations must remove barriers in existing buildings where it is easy to do so without much difficulty or expense, given the public accommodation’s resources.
Courses and examinations related to professional, educational, or trade-related applications, licensing, certifications, or credentialing must be provided in a place and manner accessible to people with disabilities, or alternative accessible arrangements must be offered. For example, courses and examinations given by computer should use appropriate computer assistive technology for people with vision, hearing, or cognitive disabilities.
Title IV addresses telephone and television access for people with hearing and speech disabilities, which has wide assistive technology implications, especially because emerging and developing technologies in the telecommunications and television fields are changing at a rapid pace. Title IV requires common carriers (telephone companies) to establish interstate and intrastate telecommunications relay services (TRS) 24 hours a day, 7 days a week. TRS enables callers with hearing and speech disabilities who use text telephones (TTYs) and callers who use voice telephones to communicate with each other through a third-party communications assistant. The Federal Communications Commission (FCC) has set minimum standards for TRS services. Title IV also requires closed captioning of federally funded public service announcements.
Widely hailed as a major civil rights bill for the disabled, the ADA has the potential of removing many of the barriers that have kept individuals with disabilities from engaging in all aspects of society. Assistive technologies surely play a major role in this process.
Individuals With Disabilities Education Act Amendments of 1997 and 2004.
The Education for All Handicapped Children Act (EAHCA) of 1975, PL 94-142, later amended by the Individuals with Disabilities Education (IDEA) Act of 1990 and the IDEA Amendments of 1997 (IDEA 97), PL 105-17, establish the right of every child with a disability to receive a “free and appropriate public education” (FAPE). Before this law, more than 1 million children with disabilities were excluded from American public schools. Currently there are approximately 6 million children being served under IDEA.
The centerpiece of the IDEA is an individualized education plan (IEP) that describes each student’s current educational performance and outlines the program of specially designed instruction (special education) and supplemental (related) services each child with a disability is to receive as part of his or her FAPE. IEPs also state specific educational goals to be achieved by the student, both short and long term (by the end of the school year). Assistive devices, and training in their use, have long been recognized as components of an FAPE. Indeed, students’ need for and ability to benefit from these devices and services, and schools’ obligations to provide these devices and services as special education or related services, predate the formal inclusion of definitions of assistive technology devices and services in the act. Definitions of those terms, copied from the Technology Act definitions, PL 100-407, were not formally added to the special education lexicon until 1990. A federal policy interpretation makes that clear. It was issued August 10, 1990, and stated that assistive technology devices and services had to be provided when they were necessary for students to receive an FAPE (Goodman, 1990). This policy letter was issued before the Individuals with Disabilities Education Act of 1990 became law. A much earlier policy letter (Desch, 1986) describes the implications of PL 94-142 regarding acquisition of assistive technologies by students with disabilities. In the 1997 IDEA Amendments PL 105-117, schools were directed to consider the assistive technology needs when formulating every IEP for students with disabilities. This provision is retained in the 2004 amendments.
Other important provisions of the EAHCA and IDEA are the requirement that children with disabilities are educated with their nondisabled peers to “the maximum extent appropriate.” This is known as the “least restrictive environment” principle. Children with disabilities are to be removed from the regular class environment “only when the nature or severity of the disability is such that education in regular classes cannot be achieved satisfactorily.”
The influence of this law has been far reaching. Devices ranging from sensory aids (visual and auditory) to augmentative communication devices to specialized computers have been used to provide access to educational programs for children with disabilities. Lack of local services or lack of funds is not a sufficient reason to deny services or devices justified in the IEP. If the IEP goals are not met, or if there are differences over what should be included in the IEP, there is a fair hearing process that may be pursued. The IDEA also mandates that schools begin to plan for the transition of students with disabilities to a wide range of possible post-high-school or adult activities, beginning many years before the student’s anticipated departure from the education programs. When planning for transition, schools are expected to work closely with state vocational rehabilitation programs. Transition planning and programming is an important point for the discussion and provision of assistive technologies.
The focus of IDEA 97 is on improving results for children with disabilities. One major portion of the original act invited states to expand and improve services to infants and toddlers with disabilities and their families (Part H, the Infants and Toddlers with Disabilities Program). In 1997, Part H became Part C of IDEA 97.
Part C of IDEA 97 provides for services to infants and toddlers (birth through age 2 years). More than 177,000 children receive services under Part C, and of those, nearly 10,000 receive assistive technology devices and services. State AT Act projects have been active in promoting the use of assistive technology for the very young and have contributed to building the capacity to provide AT services under Part C. Technology provided includes battery-operated toys with easy-access switches, seating and positioning systems, mobility devices, computers and alternative access aids, communications software, and others. Adapted toys help the child learn the basic concept of cause and effect. Seating and positioning systems provide support and guide the growth of a child’s body. Mobility devices also allow the child to move about in his or her environment. Computers and alternate access aids, such as large keypads and touch screens, can help children use software that develops communication, perceptual skills, fine motor skills, and many other skills. Through annual grants beginning in 1987, financial support is provided to develop, establish, and maintain a statewide system that offers early intervention services to all eligible children. Although participation in Part H (now Part C) was always voluntary, each state has chosen to develop a statewide system and, as of October 1, 1994, has committed to seeing that services are available to every eligible child and his or her family. The U.S. Department of Education, through the Office of Special Education Programs (OSEP), distributes funds under Part C to the states to help them carry out collaborative systems planning, policy development, and implementation of needed services for infants and toddlers who have disabilities.
The number of very young children using assistive technology has increased dramatically over the past 4 years. Besides assistive technology devices and services, states provide a variety of other services to children from birth to 2 years old, such as special education; physical and occupational therapy; nutrition services; audiology; nursing services; speech-language pathology; family training, counseling, and home visits; and vision services. The services to be provided to the child with a disability and the family are documented in an Individualized Family Service Plan (IFSP). Development of the IFSP, as with the IEP, is based on assessments of a child’s capabilities, skills, and needs and is constructed through a team approach that includes family members.
Elementary and Secondary Education Act (2001 Reauthorization).
This act (Public Law 107-110), also known as “No Child Left Behind” (NCLB), requires schools to test at least 95% of students with disabilities. These scores must be reported with other students’ scores and are used in determining whether the school is making adequate yearly progress. School districts must also report the progress of students who receive special education separately as a part of determining adequate yearly progress. Assistive technologies can play an important role in achieving curriculum goals (see Chapter 15) and may assist schools in achieving adequate yearly progress. Some states are developing standards for technology used in education and these are directly related to NCLB as well (Edyburn, Higgins, and Boone, 2005).
Assistive Technology Act of 1998, as Amended (2004).
Designated as PL 108-364, the Assistive Technology Act replaced the Technology-Related Assistance for Individuals with Disabilities Act of 1988 (PL 100-407) and the amendments to that law (PL 103-218) enacted in 1994. The 1986 Vocational Rehabilitation (VR) Amendments predated the Technology Act and it introduced numerous assistive technology provisions into the VR program. The Assistive Technology Act extends funding to the 50 states, the District of Columbia, Puerto Rico, and outlying areas (Guam, American Samoa, U.S. Virgin Islands, and the Commonwealth of the Northern Mariana Islands) that received federal funding under the Technology Act. The purposes of the Assistive Technology Act include the following:
1. Support states in their provision of assistive technology to individuals of all ages with disabilities through statewide programs.
2. Provide financial assistance to states to support their programs that provide access to assistive technology and assistive technology services.
The Assistive Technology Act is divided into three parts: Title I, State Grant Programs; Title II, National Activities; and Title III, Alternative Financing Mechanisms.
Title I provides grants to states to support capacity building and advocacy activities designed to assist the states in maintaining permanent, comprehensive, consumer-responsive, statewide programs of technology-related assistance. These include public awareness, interagency coordination, technical assistance, and training to promote access to assistive technology, and support to community-based organizations that provide assistive technology devices and services or assist individuals in using assistive technology. Title I also provides legal protection and advocacy services; funding for technical assistance, including a national public Internet site; and technical assistance to the states.
Title II provides for increased coordination of federal efforts related to assistive technology and universal design. It authorized funding for multiple grant programs from fiscal years 1999 through 2000, including grants for universal design research, Small Business Innovative Research grants related to assistive technology, grants to commercial or other organizations for research and development related to universal design concepts, grants or other mechanisms to address the unique assistive technology needs of urban and rural areas and of children and the elderly, and grants or other mechanisms to improve training of rehabilitation engineers and technicians.
Title III requires the Secretary of Education to award grants to states and outlying areas to pay for the federal share of the cost of the establishment and administration of, or the expansion and administration of, specified types of alternative financing systems for assistive technology for people with disabilities. These alternative-funding mechanisms may include a low-interest loan fund, an interest buy-down program, a revolving loan fund, a loan guarantee or insurance program, and others (RESNA Technical Assistance Project, 1999).
The primary changes in the 2004 amendment include the repeal of the provision that allows the law to expire on an annual basis. The law is now in force for 6 years. It includes the provision of assistive technology for individuals of all ages and attempts to make the provision of assistive technology and access to assistive technology services more consistent across the states and other U.S. jurisdictions (Association of Assistive Technology Act Programs, 2005).
Developmental Disabilities Assistance and Bill of Rights Act.
The developmental disabilities program was originally enacted as Title I of the Mental Retardation Facilities and Construction Act of 1963 (PL 88-164) and has been amended eight times since then. This program provides grants to states for developmental disabilities councils (DD councils), university-affiliated programs (UAPs), and protection and advocacy activities for persons with developmental disabilities (PADD). Grants to UAPs include grants for training projects with respect to assistive technology services for the purpose of assisting university-affiliated programs in providing training to personnel who provide, or will provide, assistive technology services and devices to individuals with developmental disabilities and their families. Such projects may provide training and technical assistance to improve access to assistive technology services for individuals with developmental disabilities and may include stipends and tuition assistance for training project participants.
Medicaid.
Medicaid is a federal program created in 1965 and codified as Title XIX of the Social Security Act (42 U.S.C. §1396. et. seq.). It is an income, or “means-tested,” program, so eligibility depends on a person’s income level. Medicaid is an example of a program of joint federal and state responsibilities, called “cooperative federalism.” These programs are noted by joint or shared responsibilities for financing and administration. The federal government guarantees no less than 50% funding for state outlays for their Medicaid programs, with the amounts increasing as the relative wealth of the state’s population decreases. States with the poorest populations in the nation receive federal payments of as much as 80% of their total Medicaid outlays. The federal government, through the Centers for Medicare and Medicaid Services (CMS, formerly the Health Care Financing Administration [HCFA]) also establishes a broad outline of the people who must be eligible for Medicaid, the services Medicaid programs must offer, and the way those services must be delivered, but states then have many choices about who is eligible, which services are offered, and how they are delivered. States also are responsible for day-to-day program administration.
Medicaid is not a federally mandated program. Instead, states must elect to participate and express their desire to do so by submitting a “state plan for medical assistance” to CMS. Every state participates in Medicaid. The state plan is an acknowledgement that the state will follow all federally established Medicaid requirements and identifies all the choices the states will make regarding individual eligibility and covered services. The Medicaid program neither provides services directly nor pays cash assistance directly to individuals who need medical care. Rather, the program provides payment to providers (e.g., physicians, pharmacies, hospitals, therapists) for covered supplies and services rendered to qualified recipients.
Medicaid programs are the largest funding source for assistive technologies—both devices and services—in the United States. However, its program vocabulary was established decades before the phrase assistive technology was coined, so reference to assistive technology in Medicaid means access to items of durable medical equipment, or prosthetic devices. Reference to services means access to occupational, physical, or speech-language pathology or audiology services. An individual who seeks Medicaid funding for any of these items or services must generally meet a three-part test: (1) the individual must be eligible for Medicaid, (2) the specific device or service requested must be one that is covered by the Medicaid program, and (3) the individual must establish that the device or service requested is medically necessary.
Among Medicaid services, the broadest, in terms of total benefits covered, is known as Early and Periodic Diagnosis, Screening, and Treatment, or EPSDT. EPSDT is a benefit available to every Medicaid-eligible individual who is younger than age 21 years. Its scope includes every Medicaid service listed in the Medicaid Act, both those that are required by the statute and all the optional services the states are able to elect to include in their state plans. For children, all these services must be available. EPSDT’s primary goal is early identification of health conditions, which is accomplished by mandatory periodic health screenings, and to minimize or eliminate disability by providing access to the broadest possible range of treatment. Any health condition identified in an EPSDT screening that requires treatment is to be treated as long as the intervention can possibly be covered by Medicaid. For children who require assistive technologies, EPSDT ensures access to Medicaid funding for their necessary devices and services (42 U.S.C. §1396[a][4][B]; 42 C.F.R. §441.50-441.62).
The EPSDT benefit is available only to Medicaid recipients who are younger than 21 years. For those who are 21 years or older, a different set of Medicaid benefits may be offered. For adults, Medicaid programs are required to offer a small number of services identified in the federal statute, but then they are given the choice to add to their state plan any combination of approximately three dozen “optional” services. States typically have included approximately two dozen or more of these optional services, some of which are important funding sources for assistive technologies.
The flexibility of the Medicaid program also includes a state option to seek waivers of Medicaid program requirements for specifically identified populations with special needs (e.g., technology-dependent children). “Waivers” are an opportunity for states to extend Medicaid eligibility or expand the scope of Medicaid services in a targeted way to populations that are at risk of institutional care. By extending Medicaid eligibility, waivers provide access to the health services these individuals need to remain in their homes. Or, by providing access to items that do not “fit” within the state’s definition of “durable medical equipment” or “prosthetic devices,” institutional care can be avoided.
As shown in Box 1-3, there are 11 separate Medicaid service categories that have been identified for funding assistive technology or durable medical equipment. Some are mandatory services, meaning they must be included in the state’s plan for medical assistance, whereas others are optional, meaning they can be provided to adults in the state at the option of the state. Each service category is more specifically defined in the federal regulations. For example, 42 C.F.R. §440.70(b)(3) defines medical supplies, equipment, and appliances as mandatory items under home health services; 440.110 defines physical therapy, occupational therapy, and speech, hearing, and language therapy; 440.120(c), prosthetic devices; 440.130(c), preventive services; and 440.130(d), rehabilitation services.
Persons with disabilities who are seeking to use Medicaid as a source of funding for assistive technology must navigate an often cumbersome process that usually requires both their specific conditions and needs to be expressed in language designed to fit program criteria. With very few exceptions, the Medicaid law and its implementing regulations do not identify specific types of treatment or devices that are covered, only broad categories of health care. This situation imposes an interpretive obligation on state program administrators who must decide whether the specific item or service requested “fits” or is “covered” by one of the state’s Medicaid services. Although access to many assistive technologies—both devices and services—is readily provided, these interpretive duties have proved a breeding ground for dispute about coverage and medical need. Many states have sought to avoid these disputes by adopting item- or service-specific clinical or coverage criteria. The most common items that are the subject of these criteria are communication devices and wheelchairs. In general, Medicaid coverage of assistive technologies is so broad because of the total number of people Medicaid serves, its special focus on needs identification and treatment of children, and its general purposes, which are outlined in the federal statute. The primary goal of Medicaid is to provide medical assistance to persons in need and to furnish them with rehabilitation and other services to help them “attain or retain capability for independence or self-care” (42 U.S.C. §1396). The federal regulations provide further that “each service must be sufficient in amount, duration and scope to reasonably achieve its purpose” (42 C.F.R. §440.230[b]).
Medicare.
The Medicaid and Medicare programs, created together in 1965, are codified as Title XVIII of the Social Security Act. Although Medicaid is focused on the needs of those who lack the financial means to meet the costs of necessary health care, Medicare initially was focused on the needs of the elderly, defined as individuals aged 65 years and older. It was believed that this population was less wealthy and less healthy and had access to less health insurance than did younger individuals and therefore needed assistance meeting the costs of their health care needs. Medicare subsequently was expanded to serve individuals with disabilities who are younger than age 65 years. Medicare is administered by the federal government, and the rules are the same for every state in the nation. Medicare is another major funding source for assistive technology. Like Medicaid, however, its program vocabulary characterizes devices as either durable medical equipment or prosthetic devices. It also covers occupational and physical therapy and speech-language pathology services. Medicare is a health insurance program for four groups: (1) individuals aged 65 years or older, (2) people of all ages who meet the standards of disability under the Social Security Act; (3) the disabled children of persons who had been working and who became disabled themselves, died, or retired at age 65 years; and (4) people with end-stage renal disease. It is divided into two parts. Part A, known as “hospital insurance,” covers inpatient services, posthospital care in skilled nursing homes, hospice care, and home health care. Home health care includes durable medical equipment, occupational and physical therapy, and speech-language pathology services. Part B, known as “supplemental medical insurance,” covers physician’s services; laboratory services; durable medical equipment; medical supplies; prosthetic devices; rehabilitation therapy services, including speech-language pathology services; and home health care for beneficiaries not covered by Part A. Access to assistive technologies for Medicare recipients is overwhelmingly through the Part B benefit.
The Medicare program operates like a federally subsidized insurance program. Beneficiary contributions include cash deductions and coinsurance requirements under Parts A and B and monthly premiums for Part B. For individuals who are eligible for Medicare and who are also poor, state Medicaid programs can assume the Medicare cost-sharing requirements for those individuals who qualify for both Medicare and Medicaid. Also, like many insurers, Medicare is a cost reimbursement program, meaning that Medicare recipients must first obtain an item or service, then seek Medicare reimbursement for their outlays.
Some assistive technology devices are covered by Medicare as items of durable medical equipment or as prosthetic devices. Medicare defines durable medical equipment as equipment that (1) can withstand repeated use, (2) is primarily and customarily used to serve a medical purpose, (3) generally is not useful to a person in the absence of illness or injury, and (4) is appropriate for use in the home. Medicare also has a unique limitation among benefits and funding programs that applies to mobility aids. It claims that Congress has directed that it consider only a person’s mobility related activities of daily living that arise in the person’s home, as opposed to all typical mobility needs regardless of environment, which is the generally accepted and long-standing professional standard for mobility aid assessment. Medicare reimbursement for items or services will be based on the same three factors as were stated for Medicaid: individual eligibility, coverage, and medical necessity. Medicare uses the phrase “reasonable and necessary” as a synonym of medical necessity. To be eligible for Medicare reimbursement, a covered item or service must be reasonable and necessary for the treatment of an illness or injury or to improve the functioning of a malformed body member. Medicare guidance further describes the concept of “reasonableness”: although an item may be medically necessary, it may not be reimbursed by Medicare if (1) the cost of the item is disproportionate to the therapeutic benefits derived from its use, (2) the item is more expensive than an appropriate alternative, or (3) the item serves the same purpose as equipment already available to the beneficiary.
Like most insurance policies, Medicare excludes many items for coverage, including hearing aids and eyeglasses. Other exclusions apply to items or services deemed related to “convenience,” “personal comfort,” or “custodial care.” Because these terms are subjective and the general acceptance of certain medical procedures changes over time, Medicare has established procedures for re-examining these conclusions. In 2001, for example, Medicare replaced guidance that called augmentative communication devices “convenience items” with new guidance that recognizes them as covered items of durable medical equipment. Medicare has since become the single largest payer of “speech-generating devices,” a term Medicare staff coined, among all funding programs. (See discussion of history of Medicare policy reform for speech-generating devices at www.aacfundinghelp.com.)
ASSISTIVE TECHNOLOGY INDUSTRY TODAY
Now that assistive technology has been defined and historical and legislative factors affecting the delivery of assistive technology have been reviewed, the structure of the assistive technology industry can be described. Figure 1-2 depicts the components of the assistive technology industry and how they are interrelated. It is important to be aware of the function of each component, its contribution to the industry and the necessary interaction among these components.
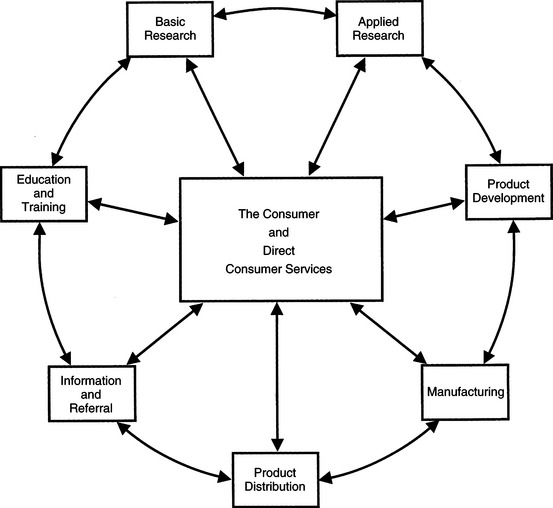
Figure 1-2 The assistive technology industry. The components center around the delivery of devices and services to consumers through direct services. The other industry components are arranged to illustrate their relationships to each other. (Modified from Smith RO: Models of service delivery in rehabilitation technology. In Perlman LG, Enders A, editors: Rehabilitation service delivery: a practical guide, Washington, DC, 1987, RESNA.)
RESNAConsumer and Direct Consumer Services
Without a consumer who uses the assistive technology devices and services, all the components in Figure 1-2 are unnecessary. Likewise, without a delivery system that actually provides the technology to the consumer, the supporting components in Figure 1-2 are ineffective. For this reason, the consumer and direct consumer services are shown at the center of the figure. However, it is important to note that the consumer may be involved in all aspects of the industry.
Direct consumer services is the component in which a consumer’s need for assistive technology is identified, an evaluation is completed, recommendations are made, and the system is implemented. The steps in providing these services are described in Chapter 4.
The Consumer.
The consumer of assistive technologies is viewed primarily as the recipient, or end user, of assistive technology. With this in mind, the industry components should be responsive to the consumer, his or her needs, and recommendations based on utilization of assistive technology services and products. As assistive technology systems are applied in the “real world,” information from the consumer (and direct service providers) flows out to the other components so that changes in products and services can be made. Likewise, the other components interact among themselves and ultimately affect the consumer and the direct consumer service providers through research, new product development, and dissemination of information.
The consumer should not, however, be viewed solely as the recipient of the technology. The consumer must be considered an active participant in the other industry components as well if the application of assistive technologies is to be effective and the industry is to grow. A number of sources recognize the many roles of the consumer in the assistive technology industry. Corthell (1986) used the term consumer as codeveloper to describe a philosophy where the consumer is involved in all aspects of the assistive technology industry. The National Institute on Disability and Rehabilitation Research (NIDRR) furthers this concept by stressing the importance of participatory research in assistive technology. As Graves (1993) points out, it is people with disabilities, their families, and the professionals serving them who are the customers of NIDRR. It is imperative that the research activities be responsive to the needs of these individuals. Therefore projects funded by NIDRR must be participatory in nature and involve individuals who will benefit from the research (e.g., persons with disabilities) in all phases of the project, which includes involvement in designing and conducting, as well as disseminating, the research.
Consumers can also be effective in training others in how to use a particular device and in assistive technology education. For example, the Empowering End Users through Assistive Technology (EUSTAT) project in Europe has developed guidelines for trainers, a set of critical factors for assistive technology training and descriptive information on programs that provide assistive technology training for consumers (http://portale.siva.it/bancadati/biblioteca/SchedaBiblioteca.asp?IDBiblioteca=1). One of the documents developed by EUSTAT is written for consumers of assistive technology services and gives practical guidance regarding how to access these services. Keep in mind, as you read about each component of the assistive technology industry, that there are many ways in which consumers can be and are involved.
Characteristics of Direct Consumer Service Programs.
Assistive technology systems and services are delivered to the consumer through a variety of models and in different types of settings. There are several attributes that set direct consumer service programs apart from one another. The primary distinguishing factor, and the one most commonly used, is the type of administrative setting in which the service delivery program exists (Smith, 1987). On the basis of Smith’s classification, Box 1-4 describes models of service delivery programs according to their administrative settings.
Smith (1987) also identifies several distinguishing features of service delivery programs. The purpose and mission may differ among service delivery programs. The purpose of some programs may be only to provide one-time evaluations, whereas other programs may provide comprehensive assistive technology services. The functional areas, or types of services, provided by assistive technology service delivery programs are other variables. Augmentative communication, seating and mobility, orthotics and prosthetics, sensory aids, computer access, robotics, and driving are some of the functional areas in which services are rendered. One program is unlikely to provide services in all these areas. Programs usually focus on a few of these functional areas.
The type of population served by an assistive technology program may be another distinguishing feature. For example, the United Cerebral Palsy Association (UCPA) supports a number of programs involving assistive technology that serve children and adults with cerebral palsy. The requirement for a military service–connected disability distinguishes the population served by the Department of Veterans Affairs. Service delivery programs also differ depending on the geographical area that they serve. Some programs are community based in that they are set up strictly to serve individuals in the community. Other programs provide specialized evaluation services to a large geographical region. On a larger scale, there are also providers such as national equipment distributors that have offices throughout the nation. Whether the program is in a rural or an urban area is another geographical factor reflected in the types of services provided. For example, programs in rural service delivery areas need to be able to provide services to farmers who have work-related injuries and require adaptation of their farm machinery to continue their livelihood.
To serve consumers who do not live in urban areas, some assistive technology service delivery occurs through telerehabilitation programs. Telerehabilitation refers to the use of telecommunications technologies to capture and transmit visual and audio information, biomedical data (e.g., electroencephalograms, x-ray films, ultrasound data), and consumer information (Kim, 1999). In assistive technology service delivery, telerehabilitation is used for preassessment screening, postassessment training in device use, and the provision of follow-up services. Transmission of telerehabilitation data may be through computer interfaces over the Internet, through telephone lines, or by satellite. For home use there are small units that resemble fax machines (Kim, 1999). These portable units allow follow-up in a consumer’s home. Scheck (1998) describes several examples of the use of telerehabilitation for assistive technology service delivery, one of which is for training in augmentative and alternative communication (AAC) (see Chapter 11). In this application the speech-language pathologist uses a small “document camera” (typically used for projecting images onto a screen or photographing them for transmission) to visualize the symbol display on the AAC device. Another camera focuses on the consumer, and a microphone picks up the synthesized speech produced by his AAC device. The speech-language pathologist can provide both instruction and evaluation from his or her office while the consumer remains at home.
Burns et al (1998) describe four case studies that illustrate the application of telerehabilitation to support the use of assistive technologies in the home. The four cases are (1) seating evaluation (see Chapter 6), (2) setup of a computer access system (see Chapter 7), (3) home accessibility evaluation (see Chapter 4), and (4) training in the use of an augmentative communication system (see Chapter 11). As Burns et al point out, telerehabilitation can overcome some of the difficulties faced by individuals who live at a distance from centers that provide assistive technology services. Low-cost video telephone technology was used in these studies. This technology, which has some limitations for studies involving full motion, was chosen because it depends only on standard telephone lines for implementation. For cases in which a family did not have a phone, cellular telephone transmission was used. Each of the cases described by Burns et al was initiated by the delivery of the telerehabilitation technology to the client’s home (often by mail). The family was then instructed in the use of the equipment (by telephone from the rehabilitation center), and the consultation was conducted remotely. The results that they obtained, although preliminary, are encouraging, and they provide useful information regarding the pros and cons of distance consultation through the use of telerehabilitation technology.
The internal operations of a service delivery program are another characterization. These include the structure of the organization (from large corporation to small, privately owned company), the number and type of professionals employed to provide the services, and whether the consumer must come to the center for services or a van or mobile unit goes to see them.
The final descriptor of service delivery programs is how the services are funded. Some assistive technology service delivery programs are funded under the general overhead of a larger organization, such as programs based within a rehabilitation hospital. Some programs are supported by grant funding, whereas others rely on a fee for service charged to third-party payers. Sources of third-party funding and mechanisms for obtaining funding for individual consumer services and equipment are discussed in detail in Chapter 5.
Basic Research
The major goal of basic research is the generation of new knowledge. Research hypotheses are posed that address fundamental questions regarding physical or biological phenomena. There are basic research questions that underlie the successful application of assistive technologies. For example, basic neuroscience studies that help to describe movement patterns in persons with disabilities provide the fundamental basis on which new control interfaces can be designed (see Chapter 7).
The single most distinguishing feature of basic research in assistive technologies is that the outcomes are not known beforehand, although hypotheses are proposed. Basic research into the effect of disability on functional performance has implications to the design of assistive technology. Throughout this text basic research studies that underlie the successful development and application of assistive technologies are described.
Applied Research
The distinction between basic and applied research is not precise, and there is some overlap. However, in the area of assistive technology application the distinction between these two types of research is clearer than in the general case. There are many types of applied research studies in assistive technology. They can be grouped as follows: (1) testing of assistive devices under various operating conditions to answer a performance question; (2) development of new assistive devices on the basis of clinical need, basic research findings, or both; (3) research on the use of assistive technologies by persons with disabilities; and (4) research studies designed to develop new assessment or training approaches or materials.
An example of the testing of devices is the use of performance standards to test wheelchairs or other devices (e.g., Cooper, Boninger, and Rentschler, 1999). In some cases, such as wheelchairs, there are accepted standards against which devices are tested (see Chapter 12). In other cases, such as augmentative communication systems (Chapter 11), there is no generally accepted standard, but a device or series of devices can be evaluated against operational characteristics developed specifically for the research study (Dahlquist et al, 1981). Another example of an applied or clinical research study related to assistive technology use is the study of the effects of adaptive seating on eating and drinking of disabled children (Hulme et al, 1987). The purpose of this study, and of studies like it, was to determine whether positioning had any effect on the oral-motor functions of children with multiple handicaps. The results also advance the state of the art in adaptive seating systems (see Chapter 6) by providing insight into what these systems must do to facilitate positioning for functional activities.
The development of new devices may occur in a university or other research laboratory setting or in industry. In either case the objective is to design and build at least one copy of a device that will perform a specific function. In general, engineers (electrical or electronic, mechanical, or industrial) create the design and technicians carry out fabrication of the devices. The initial new device that is produced is referred to as a prototype. Consumers are involved in the design process and in trial testing the prototype.
Applied research studies that focus on the use of assistive technologies are abundant. Often these studies involve assistive technologies that rely on user strategies for success. For example, augmentative communication systems used for conversation use many different types of symbol systems. An applied research study might have a goal of comparing the effectiveness of these different symbol systems in facilitating conversation (see, for example, Burroughs et al, 1990). Another example is the use of computer adaptations that replace the keyboard with devices that recognize spoken words, known as automatic speech recognition (ASR). There are several different ways of accomplishing this same function, and applied research studies are carried out to compare them (Snell and Atkinson, 1987). A related example is the study of the effects of ASR on the vocal system (Kambeyana, Singer, and Cronk, 1997). Because ASR systems require abnormal speech patterns for recognition, there is concern that vocal fold damage may result from their use. Studies to determine the actual effects of prolonged usage of ASR systems contribute to both our knowledge of ASR use and to basic speech science.
Finally, some applied research has been carried out to improve the process of assessment, recommendation, and implementation for assistive technologies. Because the assistive technology field is so diverse, individuals from a variety of disciplines may conduct these studies. For example, Lee and Thomas (1990) conducted extensive research on the assessment of individuals for control interfaces suitable for accessing computers and other assistive devices. Their research resulted in an assessment protocol, a set of data collection forms, and a series of case studies usable by others. In another study, Cook and Coleman (1987) developed an assessment protocol for augmentative communication that included a hierarchy for relating the skills and needs of a person with a disability to the characteristics of devices. The research carried out to develop this hierarchy involved assessment and analysis of results from 40 children with disabilities. In both these studies the emphasis was on better application of assistive technologies as a result of improvements in the assessment process.
Product Development
Product development involves the engineering and industrial design that must be applied to a prototype device to convert it to a version that can be fabricated in small quantities and tested with potential users. Testing of this “production prototype” is commonly referred to as alpha testing and is normally conducted in-house by manufacturers. Once the device appears to be functioning properly, several (as few as five or as many as 100) additional replicas are fabricated. There are several goals to be achieved by this procedure. First, by making more than one copy of the same device, the manufacturer can determine what potential problems may develop during the manufacturing phase (see the next section). Second, several individuals simultaneously can engage in more extensive evaluation of this set of prototypes. This phase of evaluation is often referred to as beta testing. Often manufacturers of assistive devices carry out beta testing with clinicians, consumers, and others who can give the preproduction prototypes a thorough evaluation. This accomplishes several things: (1) identification of as many potential product failures as possible, (2) evaluation of product documentation (e.g., user’s manual) to ensure that it is clear and useful, and (3) evaluation of the product with a variety of consumers with disabilities to identify the target population as accurately as possible. The latter is important because new products may be developed because one individual with a disability has an unmet need, and it is not known how widely applicable the device will be. This situation is relatively unique to assistive technologies and is one of the reasons that new product development is slower in this industry than in others, such as consumer electronics.
Manufacturing
Manufacturing is the process by which a working prototype can be converted into a device that is then mass produced. Although, in the case of assistive technologies, “mass production” may mean production runs of only a few hundred units or less, this process is still quite different from producing a few beta-test prototype devices that function correctly. It is at this stage that production techniques become important. There are many fabrication techniques that are suitable for use only when many copies of an item are made. Several of these are based on the fabrication of a mold from which parts are formed. This technique can be used for polymer (plastic), metal, and ceramic materials. The cost of making the mold can often be very high ($50,000 to $200,000 or more) if the part is complex. However, once the mold is made, the individual copies of the item are quite inexpensive (from a few cents to a few dollars). This process is not feasible unless there are large numbers of parts manufactured; the cost of the mold is then amortized over the total number of parts produced. In assistive technologies this process is most often used for low-tech products such as reachers and eating utensils. Certain parts of some high-tech devices, such as wheelchair casters or the cases for augmentative communication devices, are also molded. Because the mold is a one-time cost, the size of the production run determines the cost of each part. The more pieces that are produced, the lower the cost per item. Because the cost of the molds is often very high, changes in design can also be expensive and may not be made until the original cost of the first model is recovered.
When manufacturing parts from molds, the major cost is in the production equipment; labor costs are relatively low. Other types of manufacturing are much more labor intensive. At one extreme are fabrication methods that rely exclusively on hand assembly. For example, most augmentative communication devices are fabricated one at a time by hand. There are no economies of scale in this type of process. Each device requires a certain amount of time to assemble, and the only savings in manufacturing cost are derived from the increased skill and speed of the individual worker doing the assembly. Thus production labor costs are a significant part of the cost of a manufactured item.
Both parts (materials) costs and labor costs are components of any manufacturing process. Savings in materials costs can be made by producing more units, even if they are hand assembled, because many suppliers give volume discounts for a larger order of the same part. In some assistive technologies, production runs are substantially below a level that generates a discount; for others they are much higher.
At the other extreme from hand assembly is a totally automated production process in which all fabrication and assembly are performed by dedicated machines. This ideal situation does not really exist because some human intervention in the process is necessary for all manufacturing. However, many commercial products are produced by use of a great deal of automated manufacturing. Because the automated production machines do not require a salary, the cost per item is reduced as more copies are made, that is, as the production runs get larger. The production runs necessary for true production automation are approximately 100,000 and higher, which rarely occurs in the production of assistive technology devices.
The assistive technology market is broad. The range of disabilities and the effects of those disabilities are extremely large, which result in a diversity of needs that can be served by assistive devices. Unfortunately, the number of people who have exactly the same need, and for whom the same device will meet the need, is small. This leads to small volumes of production and increased costs per device. It also has the effect of making a device seem more expensive because it is less complex but costs the same as a consumer device that is more flexible.
Many of the commercial general-use devices that are used as assistive technologies are produced by these automated manufacturing techniques. For example, personal computers often have production runs of 100,000 or greater. Thus the cost per unit for a system of this type is lower than for a device specifically designed and built for use by persons with disabilities.
Several conclusions can be drawn from this discussion. The volume in which devices are produced is directly related to their cost. This idea is reflected in two ways in assistive technologies. First, there is the direct relationship between cost and volume of production, which is why certain low-tech devices such as mouth sticks may cost in the hundreds of dollars and a high-tech electronic calculator costs less than $20. Second, the difference between devices produced in large volumes and those produced in smaller volumes is sometimes reflected in overall sophistication and capability rather than directly in price. For example, a personal computer that is capable of performing a wide variety of tasks and that uses sophisticated and complex components is often comparable in price to a much less sophisticated but more specialized assistive device. Thus more function for the price is often gained when a device is produced in larger quantities.
Distribution of Hard Technologies
Manufacturing a device is not worthwhile if consumers and service providers are not aware of its existence. Therefore marketing is an important part of the assistive technology distribution process. In contrast to consumer products, assistive technologies must be marketed and distributed to a highly specialized audience of providers (therapists, engineers, vocational rehabilitation counselors) and consumers. Marketing of assistive technologies involves significant costs, which must be recovered from the selling price of the device.
Distribution of manufactured assistive technologies can occur in several different ways. The major distribution options are (1) mail order, (2) direct sales by company representatives, and (3) distribution through a dealer or supplier. The choice of one or more of these is highly dependent on the type of product. For wheelchairs, seating and positioning systems, aids to daily living, and home care products, most distribution is through assistive technology suppliers. Most of these suppliers do not handle communication, environmental control, or computer access technologies.
For many low-tech devices, computer software, and some computer hardware, distribution is by mail order or via the Internet. This system is an advantage in areas where there are no suppliers providing the needed equipment. It is most effective for products for which there is no fitting or need for a prepurchase trial by the consumer. In some cases an evaluation center has devices to try, which can eliminate some limitations. Mail-order or Internet distribution can have significant costs for preparation and distribution of catalogs, for Web-based materials and brochures, and for processing orders. Another limitation to this approach is that maintenance and repair is harder to obtain for high-tech devices, such as computer systems, purchased this way.
Relatively few assistive technology products are distributed through direct company-employed representatives. Some exceptions are augmentative communication systems and aids for persons with visual impairments. Some of these have direct sales staffs, whereas others use dealers who carry several related products. In either case, this distribution network is not adequate to cover all geographical areas equally, and mail-order or Internet sales typically supplement the direct representative network. Electronic products such as augmentative communication systems, environmental control units, and feeders are often outside the range of capabilities of the standard rehabilitation equipment supplier. This situation has led to the development of more direct sales in these product areas.
Information and Referral
The ability to readily obtain current information on assistive technology services and products is essential for both service provider and consumers. The Internet has a large amount of information available in many areas, including assistive technologies. This is the good news; the bad news is that much of this information is not validated by an independent source, so both the quality and accuracy of the information accessed must be carefully evaluated. The Resources section found at the end of this book contains a list of Web sites that is intended to provide some initial information; it is not meant to be all inclusive.
ABLEDATA is the largest and most well known general source of information on products for individuals with disabilities. It contains more than 32,000 listings of devices (of which 21,000 are currently available). The ABLEDATA database also contains information on noncommercial prototypes; customized, one-of-a-kind products; and do-it-yourself designs. The scope of ABLEDATA listings is broad, encompassing sensory and motor aids, low- and high-tech devices, and applications from home care to employment. The ABLEDATA database classifies each assistive technology product by its intended function or any special features it possesses. The products are classified into the 19 areas shown in Table 1-4. Clicking on any of these topics provides a link to the major categories within that topic and then a link to specific product types in each category. Key word or phrase searching is also available. It is possible to search the ABLEDATA Web site in one of four ways: (1) by keyword or phrase, (2) by brand name of an assistive device, (3) by name of manufacturer or distributor, and (4) by Boolean search (specifying multiple features to be included in the search). If Internet access is not available, an ABLEDATA search can be requested from their information specialists by phone, fax, or mail.
TABLE 1-4
ABLEDATA Topics and Categories
| Topics | Major Categories |
| Aids for Daily Living (products to aid in activities of daily living) | Bathing, Carrying, Child Care, Clothing, Dispenser Aids, Dressing, Drinking, Feeding, Grooming/Hygiene, Handle Padding, Health Care, Holding, Reaching, Smoking, Toileting, Transfer |
| Blind and Low Vision (products for people with visual disabilities) | Computers, Educational Aids, Health Care, Information Storage, Kitchen Aids, Labeling, Magnification, Office Equipment, Orientation and Mobility, Reading, Recreation, Sensors, Telephones, Time, Tools, Travel, Typing, Writing (Braille) |
| Communication (products to help people with disabilities related to speech, writing, and other methods of communication) | Alternative and Augmentative Communication, Headwands, Mouthsticks, Signal Systems, Telephones, Typing, Writing |
| Computers (products to allow people with disabilities to use desktop and laptop computers and other kinds of information technology) | Software, Hardware, Computer Accessories |
| Controls (products that provide people with disabilities | Environmental Controls, Control Switches with the ability to start, stop, or adjust electric or electronic devices) |
| Deaf And Hard of Hearing (products for people with hearing disabilities) | Amplification, Driving, Hearing Aids, Recreational Electronics, Signal Switches, Speech Training, Telephones, Time |
| Deaf Blind (products for people who are both deaf and blind) | [no categories listed] |
| Education (products to provide people with disabilities with access to educational materials and instruction in school and in other learning environments) | Classroom, Instructional Materials |
| Environmental Adaptations (products that make the built environment more accessible) | Indoors, Outdoors, Vertical Lift, Houses, Specialties, Lighting, Signs |
| Home Management (products that assist in cooking, cleaning, and other household activities and adapted furniture and appliances) | Food Preparation, Housekeeping, Furniture |
| Orthotics (braces and other products to support or supplement joints or limbs) | Head and Neck, Lower Extremity, Torso, Upper Extremity |
| Prosthetics (products for amputees) | Lower Extremity, Upper Extremity |
| Recreation (products to assist people with disabilities with leisure and athletic activities) | Crafts, Electronics, Gardening, Music, Photography, Sewing, Sports, Toys |
| Safety and Security (products to protect health and home) | Alarm and Security Systems, Child Proof Devices, Electric Cords, Lights, Locks |
| Seating (products that assist people to sit comfortably and safely) | Seating Systems, Cushions, Therapeutic Seats |
| Therapeutic Aids (products that assist in treatment for health problems and therapy and training for certain disabilities) | Ambulation Training, Biofeedback, Evaluation, Exercise, Fine and Gross Motor Skills, Perceptual Motor, Positioning, Pressure/Massage Modality Equipment, Respiratory Aids, Rolls, Sensory Integration, Stimulators, Therapy Furnishings, Thermal/Water Modality Equipment, Traction |
| Transportation (products to enable people with disabilities to drive or ride in cars, vans, trucks and buses) | Mass Transit Vehicles and Facilities, Vehicles, Vehicle Accessories |
| Walking (products to aid people with disabilities who are able to walk or stand with assistance) | Canes, Crutches, Standing, Walkers |
| Wheeled Mobility (products and accessories that enable people with mobility disabilities to move freely indoors and outdoors) | Wheelchairs (Manual, Sport, and Powered), Wheelchair Alternatives (Scooters), Wheelchair Accessories, Carts, Transporters, Stretchers |
| Workplace (products to aid people with disabilities at work) | Agricultural Equipment, Office Equipment, Tools, Vocational Assessment, Vocational Training, Work Stations |
ABLEDATA also publishes Informed Consumer Guides that include information on product selection and purchase of a particular type of device. References to product write-ups, standards, or comparative studies on that product class, linkages to other resources and reference materials, and reports on specific products submitted by consumers are also included. Fact sheets and Informed Consumer Guides can be viewed and downloaded from the ABLEDATA Web site. The Assistive Technology Directory lists companies with products included in the database.
Written publications such as conference proceedings, periodicals, directories, and catalogs are another way to find information on assistive technology services and products. Most manufacturers have catalogs, and it is easy to be placed on their mailing lists so that you receive updated information. In addition to their catalogs, manufacturers may also publish regular newsletters of product updates and applications, and many also have their own Web sites that are updated frequently and provide instant information regarding their products. In some cases it is possible to purchase the product directly through the company Web sites. Many of the centers that provide services in assistive technology publish newsletters and maintain Web sites as well.
Electronic listservs are formed by individuals with common interests. Each user accesses the information from his or her own e-mail system, and all messages are available to all members of the list. There are many listservs that address various areas of assistive technology applications. Some are maintained by professional associations (e.g., RESNA, American Occupational Therapy Association, American Speech-Language Hearing Association, American Physical Therapy Association), whereas others are established and maintained by rehabilitation centers or universities. There are also user- or consumer-oriented listservs, which address either specific issues (e.g., one particular disability) or general issues. These listservs are often useful places to gain information regarding specific assistive technology questions. Four of the most useful U.S.-based conferences (all annual) are the International Conference on Technology and Disability (California State University at Northridge) Conference (held in March in Los Angeles, www.csun.edu/cod/conf/index.html), Closing the Gap (held in October in Minneapolis, www.closingthegap.com), Assistive Technology Industry Association (January, Orlando, Florida, www.atia.org), and RESNA (June, various locations, www.resna.org). International conferences include the Australian Rehabilitation and Assistive Technology Association (even years) (http://www.e-bility.com/arata/sitemap.php), the Association for the Advancement of Assistive Technology in Europe (odd years) (http://www.aaate.net/), and the Japanese conference on the advancement of Assistive and Rehabilitative Technology (odd years) sponsored by the Rehabilitation Engineering society of Japan (http://www.resja.gr.jp/eng/). There are also specialty conferences in specific areas of assistive technology such as the International Association for Augmentative and Alternative communication (even years) (http://www.isaac-online.org/) and the International Seating Symposium (annual) (http://www.iss.pitt.edu/).
Education
As previously stated, the growth of the assistive technology industry has meant an increased availability of devices and services for individuals with disabilities. However, it is necessary that competent professionals be involved in the delivery of these devices and services. It is also necessary that these professionals come from a variety of clinical and technical backgrounds. Many individuals practicing in the area of assistive technologies received their information on the job or through in-service training such as conferences or workshops. Formal training courses or programs as part of undergraduate or graduate educational programs have developed over the past 15 to 20 years.
For professionals currently in practice, in-service educational activities in assistive technologies that supplement the individual’s professional training and experience are available. Typically this type of educational activity is very focused and of short duration. In-service programs have been the major type of formal educational activity for professionals applying these technologies. The variety of in-service opportunities in assistive technology applications is extremely large, and it is growing yearly. Some workshops are offered by industry, and they focus on a specific product or product line. Other workshops or seminars are offered by rehabilitation centers or universities. These workshops may include one area of application (e.g., seating and positioning or augmentative communication), or they may be broader. Often workshops are offered in conjunction with major conferences of professional associations, which can be a convenient way for conference participants to obtain in-service education in a cost-effective manner.
A major source of in-service education is conferences that focus on assistive technologies. These conferences provide a wealth of opportunities for education (see Enders and Hall, 1990). Many are regional, which makes them more financially accessible than the national meetings. Another source of continuing education is professional journals. Some professions have journals that occasionally publish articles on assistive technology; other journals are solely dedicated to assistive technology (see Resources). With the growth of the Internet, there is an increasing number of assistive technology courses and educational programs offered at a distance (including on-line and teleconference formats). These often involve multiple institutions (both rehabilitation centers and universities) and international linkages.
Preservice educational activities are part of professional preparation at the undergraduate or graduate level for practice in specific disciplines such as occupational therapy, physical therapy, recreation therapy, rehabilitation engineering, special education, speech-language pathology, and vocational rehabilitation counseling. In recent years the number of programs that offer instruction in assistive technology topics has increased, particularly in occupational therapy, rehabilitation engineering, and speech-language pathology (focusing on augmentative and alternative communication) programs. The scope of assistive technology instruction in preservice educational programs varies widely. There may be an assistive technology specialization within a rehabilitation discipline (e.g., OT, PT, or SLP), required or elective courses or subjects in assistive technology, assistive technology material included within a broader course, or, at the graduate level, assistive technology projects or theses. The most common programs are those that include some assistive technology material in other courses; the least common are those specializing solely in assistive technology. With the increasing role of technology in the lives of individuals with disabilities, it is crucial that newly trained professionals entering their respective fields have some level of formal training in assistive technology applications.
In rehabilitation engineering, the entry-level degree for professional practice is the master’s degree. There are few universities that offer degrees in rehabilitation engineering at this level. More often, it is a subspecialization within another engineering discipline (e.g., biomedical engineering). In some cases a certificate of completion is presented to the student in addition to the master’s degree in his or her field of specialization.
Rowley, Mitchell, and Weber (1997) described their experience over 6 years with one model master’s level program in rehabilitation engineering. This program’s curriculum has four areas of emphasis for student acquisition of knowledge and skills: (1) disability and technology, (2) major rehabilitation systems, (3) applied skills, and (4) life-long learning.
The major influence of preservice educational programs is that more individuals than ever before are entering practice in their professional field with knowledge of assistive technologies and their application. This development will have a major positive influence on the effectiveness of these technologies, the development of new and innovative devices, and the impact that these systems have on the lives of persons with disabilities.
PROFESSIONAL PRACTICE IN ASSISTIVE TECHNOLOGY
This section describes the person who provides assistive technology and the issues surrounding his or her professional practice. Three broad issues are discussed in this section: (1) ethics of practice, (2) quality assurance, and (3) liability. Each of these has implications both for the individual practitioner and for organizations involved in the assistive technology industry. We begin with a description of the person providing assistive technology services and devices.
Providers of Assistive Technology Services
The assistive technology practitioner (ATP) typically has a professional background in one of several areas, including engineering, occupational therapy, physical therapy, recreation therapy, special education, speech pathology, or vocational rehabilitation counseling. Each professional has a contribution to make to the industry based on his or her unique background. Therefore ATPs should be well grounded in their disciplines. It is equally important for each ATP to have knowledge and skills in assistive technology and familiarity with the scope of the assistive technology industry. RESNA has developed an assistive technology certification program to address this issue; it is discussed further in a later section.
Any of these professionals may be involved in any of the components of the assistive technology industry. For example, occupational or physical therapists with expertise in the area of seating may be found providing direct consumer services, consulting with manufacturers on the use and function of wheelchairs and seating systems, educating others on the prescription of seating systems, or working in research on the effect of certain body positions on functional activities. Likewise, speech pathologists may be involved in augmentative communication as a member of an evaluation team, may function as a representative for a manufacturer’s particular products, or may conduct research on interactions among users of communication devices. These are just some examples of the ways in which ATPs can be involved. A similar variety of roles in the assistive technology industry are available to ATPs from other disciplines.
Having described the ATP’s position in the industry as a whole, let us now look at his or her role in direct service delivery. ATPs are involved in the needs assessment, evaluation, implementation, training, and follow-up of assistive technology services in various functional areas. Examples of these areas are augmentative communication, seating and mobility, orthotics and prosthetics, sensory aids, computer access, robotics, and driving.
Because of the number of factors and the complexity involved in the delivery of assistive technology systems to the consumer, a team approach is desirable. This team may consist of as few as two professionals working together. Each individual team member brings knowledge and skills from his or her area of expertise that can be applied to the assistive technology service delivery process. Although it is tempting to view each functional service area (e.g., augmentative communication, seating, mobility) as being in the domain of one or two specific disciplines, service delivery is most effective when a transdisciplinary team approach is used.
In a transdisciplinary team approach, there is crossing over of professional boundaries and sharing of roles and functions. All individual team members must be well grounded in their profession but also feel comfortable enough to extend their role beyond that profession (Pronsanti, 1991). This blurring of roles can be seen, for example, during an augmentative communication assessment performed by a team consisting of a speech pathologist, an occupational therapist, and a rehabilitation engineer. Traditional roles may dictate that the occupational therapist perform an assessment of the consumer’s ability to reach and point, the speech pathologist evaluate language skills, and the rehabilitation engineer design the mounting of the device. In contrast, with a transdisciplinary team, all three disciplines contribute to identification of a good control site for the individual or to mounting the device in the most appropriate location. A team discussion may also form the basis for the type of vocabulary to include in the augmentative communication device. As a result of this team collaboration, a more thorough assessment of the individual’s needs and skills is likely to occur.
Although some practitioners may feel threatened that the transdisciplinary approach takes away part of their professional identity, Kangas (quoted by Mastrangelo, 1992) points out that her experience has been that this approach improves the assessment process and actually strengthens each person’s professional identity through the giving and confirmation of information. This approach also encourages support, creativity, and honesty among the disciplines (Mastrangelo, 1992).
Ethics and Standards of Practice
Ethics is defined as “the study of standards of conduct and moral judgment…and the system or code of morals of a particular…profession” (McKechnie, 1983, p. 627). When applied to a field of professional endeavor such as assistive technology delivery or a profession such as occupational therapy or rehabilitation engineering, the ethical conduct of practitioners is embodied both in a code (or canons) of ethics and in standards of practice. Each ATP must comply with the code of ethics for his or her discipline (e.g., rehabilitation engineering, occupational or physical therapy, speech-language pathology, or vocational rehabilitation counseling). The code of ethics for a discipline is typically developed by the professional association serving it. As discussed, ATPs have responsibilities in assistive technology service delivery that are not specified by their individual discipline’s code of ethics. For this reason, it is important to have a code of ethics that addresses the specific issues related to the application of assistive technologies. Standards of practice differ from codes of ethics in that they describe more specifically what is and is not considered to be good practice in a given discipline.
Code of Ethics for Assistive Technologies: The RESNA Code of Ethics.
RESNA is an interdisciplinary professional association whose activities focus on assistive technologies. Its members come from many disciplines and a variety of settings, and their activities involve the full scope of assistive technology applications. In 1991 the RESNA Board of Directors adopted the code of ethics shown in Figure 1-3. This code is similar to those of other disciplines involved in rehabilitation and is based on several of them. However, it includes issues related to the provision of technology. It is presented as a reminder of the obligations that a practitioner in the assistive technology industry has to his or her consumers, others who work with and care for them, the general public, and the profession as a whole.
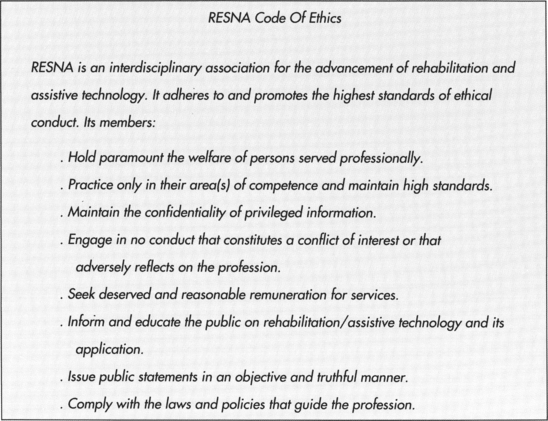
Standards of Practice.
Because each assistive technology practitioner belongs to his or her own discipline, it is important that the standards of practice pertaining to that specialty be adhered to. These standards are often the basis for professional certification programs. RESNA has developed the standards of practice shown in Box 1-5 for assistive technology practitioners and suppliers.
Quality Assurance
Quality assurance is a broad area of fundamental importance to the safe and effective application of assistive technologies. It involves two basic considerations: (1) the quality of the services rendered and (2) the quality of the devices supplied (Enders and Hall, 1990). Quality assurance is closely tied to reimbursement, and as the number of devices and practitioners increases, third-party payers are requiring some indication that the services and devices are necessary, safe, and effective. A comprehensive quality assurance program addresses these issues. The quality of services can be measured and evaluated by certification (of individual practitioners) and accreditation (of facilities and programs). The efficacy of devices is measured by adherence to device performance standards and good manufacturing practices. Ultimately, the quality of assistive technology services and devices is determined by measurement of outcomes resulting from both the provision of the services and devices and the use of the technologies to facilitate functional improvement and quality of life for the individual consumer.
Overview.
Patterson (1989) presented the following overview of quality assurance from the perspective of The Joint Commission (TJC). The consumer, practitioner, and purchaser (of services or devices) each have a unique view of what constitutes quality. The consumer views it from his or her own point of view and, in the case of assistive technologies, judges the quality on how daily activity is improved in the specific areas of application. The practitioner generates measures of performance and then attempts to judge the quality of the services and devices against these measures. The practitioner evaluates both the technologies and the consumer because motivation, amount of effort spent on training, and so on can affect success of any device or service. The purchaser of services or devices asks the most basic of questions: are the services and devices cost-effective? This question also implies the existence of a measurable outcome, and often purchasers require the practitioner to develop such measures before funding is approved.
Patterson cites several reasons why quality assurance programs are necessary. The most important is to ensure that practice is effective and appropriate to the consumer’s needs. A good quality assurance program improves practices and outcomes and consumer satisfaction. In addition, quality assurance programs are necessary to ensure accountability to the public and conformance with codes of ethics.
Quality assurance programs are implemented through both internal and external factors. Organizations that provide assistive technology services and equipment must have a philosophical commitment to quality assurance that is reflected in their mission statements, and there must be internal monitoring and evaluation. External monitoring is also important to ensure objectivity in meeting quality assurance goals. External monitoring can be accomplished through standards required by organizations that accredit the facility (such as TJC); certification of individual practitioners; standards developed by third-party reimbursement organizations; and local, state, or federal legal requirements.
Standards for Service Providers.
Professional certification is a voluntary process in which a professional organization measures and reports the degree of competence of an individual practitioner (Warren, 1991). To establish a certification program, there must be an agreed on body of knowledge unique to the practitioners in the area to be certified. Once the body of knowledge is adequately described, a set of professional competencies must be established and a method for evaluating an individual’s knowledge in these competence areas (usually a written examination) must be developed and implemented. As Warren points out, the examination process must be developed in such a way as to reflect how a person performs on the job, and it must reflect knowledge actually required for satisfactory job performance. Within the assistive technology field, the challenge of establishing a valid and useful certification program is complicated by the great diversity of disciplines involved. RESNA has developed a certification program in assistive technologies that addresses the special requirements of this field and that builds on other disciplines’ certification and licensure, such as registered occupational therapist, registered physical therapist, professional engineer, or certificate of clinical competence–speech pathology. RESNA offers a voluntary credentialing program; on successful passage of an examination, one of two types of credentials is currently awarded. The assistive technology practitioner certificate is intended for service providers primarily involved in analysis of a consumer’s needs and training in the use of a particular device. The assistive technology supplier certificate is intended for service providers involved in the sale and service of commercially available devices. The assistive technology certification focuses on the skills and knowledge required to deliver assistive technologies, assuming that the individual has already established disciplinary competence by certification or licensure. The certification process is further described on the RESNA Web site (www.resna.org).
The National Association of Medical Equipment Suppliers (NAMES), an association of suppliers of rehabilitation and home health care equipment, has established a national registry for rehabilitation technology suppliers. The NAMES National Registry of Rehabilitation Technology Suppliers (NRRTS, www.nrrts.org) has a goal of providing a mechanism for consumers, clinicians, and third-party payers to identify qualified suppliers to ensure provision of high-quality rehabilitation technology and related services to people with physical disabilities. NRRTS defines a rehabilitation technology supplier as one who provides enabling technology in the areas of wheeled mobility, seating and alternative positioning, ambulation assistance, environmental control, and activities of daily living. To become a certified rehabilitation supplier, an individual must first join NRRTS. NRRTS membership confirms that a rehabilitation technology supplier has demonstrated work experience, received recommendations from professional associates, adheres to a stringent code of ethics, and commits to participate in continuing education to remain an NRRTS member. NRRTS awards the Certified Rehabilitation Technology Supplier certificate to a NRRTS member in good standing who has successfully completed the RESNA assistive technology supplier credentialing examination.
Although certification programs address the qualifications of individual practitioners, accreditation addresses the quality of services provided by facilities. The Rehabilitation Accreditation Commission (CARF) (4891 E. Grant Rd., Tucson, AZ 85712, (520) 325-1044, www.carf.org) accredits organizations in the rehabilitation field. This accreditation is based on the results of the organization’s service delivery program, which includes hospitals, home care, mental health, long-term care, and ambulatory care. CARF views its activities as a quality improvement mechanism based on an external, impartial peer observation of current service practice. An organization’s practices are measured against internationally developed and accepted quality indicators that focus on consumer-driven results, stakeholder satisfaction, and quality improvement. A CARF quality audit for accreditation serves as a framework for quality improvement, with a focus on individual consumers’ outcomes and satisfaction. CARF accreditation is widely viewed as a mark of quality achievement. CARF accredits more than 20,000 service programs in the United States and Canada, and this accreditation is accepted or required for rehabilitation organizations in more than 40 states.
CARF includes standards for assistive technologies in both the employment and community services categories of their accreditation program (CARF, 1999). Standards for assistive technology services are included in the “principal standards,” which apply to all types of accredited services and in specific types of community and employment services. Principal CARF standards require that each person served must have access to assistive technologies to meet his or her identified needs. If an organization cannot provide the assistive technologies required, referrals must be made to providers who can meet the needs of the persons who are served by the organization. In addition, each person’s exit report must contain a description of the assistive technology services provided. CARF also has specific standards for employment assistive technology services and community assistive technology services. These services focus on achievement of employment, community access, inclusion, and independence goals. Assistive technology services may include selection, acquisition, or use of assistive technologies; information, referral, or observation of assistive technology; and exploration of alternative assistive technology strategies. CARF standards also emphasize that the accredited organization should clearly tell people what it can and cannot do to help them regarding access to assistive technologies. In addition, the organization’s services should be focused on helping people get and keep a job or on community access, inclusion, and interdependence, as appropriate. Appropriate staff knowledge, training, and experience are also evaluated.
Standards for Devices.
There are several types of standards that can be developed for assistive devices. The manufacture and production of assistive technologies and other medically related equipment are regulated by federal legislation in the United States (PL 94-295). These regulations include specification of good manufacturing practices and classify devices on the basis of the risk of their use.
The Food and Drug Administration (FDA) classifies medical devices in these categories. Class I devices (e.g., wheelchair accessories) are minimal risk. Class II devices require performance standards to be met (e.g., powered wheelchairs, standup wheelchairs, and special grade wheelchairs and motorized three-wheel vehicles). Class III devices require premarket approval (e.g., a stair-climbing wheelchair) (21 C.F.R. 890.3890). The Canadian system for medical devices is almost identical, with the same risk-based classification system, Class I through Class IV.
Two types of submissions may be made to the FDA for medical devices. The premarket approval is the process that the FDA uses to evaluate the safety and efficacy of new products that pose a significant risk to the patient. A 510(k) notification is submitted for a change to an existing device that is already on the market or for a new device that is “substantially equivalent” to a preamendment device. Further information may be obtained from the FDA Web site (www.fda.gov/cdrh).
Most assistive technologies are judged to be minimal risk (Class I or Class II), which reduces the restrictions on their development and testing and on their approval for sale by prescription. However, in addition to paperwork and delays, there are costs associated with obtaining approval for a device at any level of risk, and these costs must be recovered from the sale of the product.
Third-party reimbursement may be refused for a device that is not FDA compliant. Repeated violations can result in fines and even jail for manufacturers who continue to market products after being informed that they needed to undergo FDA review; imported devices are often barred at the border by U.S. Customs officials if they are not cleared. Assistive technology providers and suppliers may also be at risk, from a legal perspective, if they use products that are not approved.
Devices can also be rated by development of compatibility and performance standards. Compatibility standards are developed to ensure that devices from different manufacturers can be used together. In assistive technologies, compatibility standards exist for control interfaces, computer-emulating interfaces, powered wheelchair controllers, and other devices. For example, control interfaces have connectors on the end of their cables that allow them to be plugged into electronic assistive technologies. For a control interface from one manufacturer to be used with a device from another manufacturer, they must both adhere to a compatibility standard that specifies the type of connector, which pins have which functions, and so on. These standards are voluntary, but it is in the best interest of a manufacturer to adhere to them to maximize the use of its products.
Performance standards are also voluntary. These standards specify how a device should perform and provide a set of tests to be used for comparing similar products from different manufacturers (Enders and Hall, 1990). For example, wheelchair performance standards specify durability, maneuverability, dynamic stability, and energy consumption (Axelson and Phillips, 1989). In some cases, such as wheelchairs, the standards become formalized and adopted by the American National Standards Institute or the International Standards Organization. Approval by one or more of these bodies indicates that the standards have received a careful and thorough review, that they embody reasonable expectations of performance, and that they address issues of safety and efficacy. There are also less formal performance standards, which may be developed by an industry or an agency. The Veterans Administration develops standards for their purchase of medical and assistive devices. Because they purchase large quantities of devices, manufacturers adhere to their standards and these purchase specifications serve as informal performance standards.
Whether standards are informal or formal, compatibility or performance, they have an influence on the success of assistive technology use only to the degree that they are voluntarily adopted by industry. The motivation for this adoption is both economic (e.g., increased sales) and altruistic (e.g., concern for safety and functional improvement). Assistive technology practitioners need to work with industry to ensure that standards are meaningful. They also need to insist that products they recommend have met applicable standards. These activities help to ensure that meaningful product standards are developed and used.
Outcomes of Assistive Technology Delivery.
Assistive technologies create unique challenges in quality assurance. For many therapies, a service is provided in a clinical rehabilitation setting and the success of the outcome is based on measures such as functional improvement, reduced hospitalization, or ability to work at average productivity. It is not possible to apply these measures directly to assistive technology services and devices because the goals of the service are different. In assistive technology service delivery, the selection of a device is based on what a person is able to do now, not what he or she will be able to do on completing a program of therapy. A device that is expected to meet the needs of the person is then recommended, and the individual consumer decides whether to use it. The device is used not in a well-controlled clinical environment, but in the larger context of employment, school, and community. To evaluate the effectiveness of this entire process, the focus should not be on the service or device individually, but on the entire assistive technology system, which includes the user, the technology, the activities being carried out, and the context (environment) in which the system is being used. The determination of the “success” of the service delivery process is based on measurement of outcomes related to the success the consumer achieves using the assistive technology system. Outcome measures are objective criteria, usually developed during the assessment and recommendation process, that can be used to judge the effectiveness of both devices and services during the training and follow-up phases of the service delivery process. In Chapter 2 a framework for assistive technologies that provides the basis for outcome measures is developed. In Chapter 4 the development and application of outcome measures for assistive technology services and devices are discussed.
SUMMARY
The definitions, history, legislation, industry, and professional issues presented in this chapter provide the foundation for our discussion of assistive technologies and their application. In the remainder of this text, a set of principles, some of which are general and some of which apply to a specific need, are presented. In addition, the practices that underlie successful application are described in detail. Many specific assistive devices are also characterized in succeeding chapters.
Study Questions
1. How are assistive technologies included within the WHO ICF?
2. What is meant by a “low-tech” and a “high-tech” assistive device? Give an example of each.
3. Distinguish between hard and soft technologies.
4. Give three examples of assistive technology appliances and three examples of assistive technology tools.
5. What is the difference between minimal and maximal technology? Give an example of each.
6. Refer to Figure 1-1. Why are standard commercially available products less expensive than special commercially available products? Why are the latter less expensive than modified or custom-designed devices? Give examples of all four classes.
7. Why do we distinguish assistive technologies from rehabilitative and educational technologies? Can one device play a role in both areas?
8. Distinguish between specific purpose and general purpose technologies.
9. What has been the influence of federal legislation on the availability of assistive technology devices and services?
10. List at least four ways in which U.S. federal legislation has affected the practice of assistive technology service delivery.
11. Compare the situation today regarding assistive technologies with that in 1972.
12. What is at the focal point of the industry of assistive technology? What are the other industry components?
13. Pick any one piece of legislation shown in Table 1-2 and describe its influence on the development and application of assistive technologies.
14. Why should the consumer be considered a “codeveloper”?
15. Assistive technology practitioners may have a background in a variety of disciplines. List some typical disciplines.
16. Define the characteristics of direct consumer service settings in assistive technology.
17. Describe how you would carry out an ABLEDATA search if (1) you know the manufacturer, (2) you know the name of the device, and (3) you only know the general name of a device.
18. Describe the benefits of a transdisciplinary team.
19. Why is it necessary to have codes of ethics?
20. How does a code of ethics differ from standards of practice?
21. What are the major elements of a quality assurance program?
22. Describe how certification and accreditation differ. What is the purpose of each?
23. What are the major features of the CARF standards in assistive technology?
24. What is the difference between a performance standard and a compatibility standard?
25. What are the two kinds of liability with which assistive technology practitioners must be concerned?