Chapter 9 Developing personal skills
Overview
People’s health behaviour or lifestyles have been regarded as the cause of many modern diseases. Therefore a main focus of health promotion has been on modifying those aspects of behaviour which are known to have an impact on health.
In previous chapters we have argued that such an approach is unlikely to be effective unless it acknowledges how people’s behaviour may be a response to, and maintained by, the environment in which they live. Many health promoters, however, see their role as helping people to live their lives to its best potential, which may involve some change in their health behaviour.
This chapter is concerned with those aspects of health behaviour that people can control. Understanding why people behave in certain ways and how they can be helped to maintain chosen behaviours is central to self-empowerment. This chapter explores the usefulness of social psychology which offers several theoretical models that identify the determinants of behaviour change. This can contribute to, if not the prediction, then at least an understanding of how people make decisions about their health. This can be a useful tool in planning health promotion interventions. The influence of specific factors such as individual self-esteem or people’s perceptions of control over their lives needs to be taken into account by the health promoter in order to offer practical support and positive experiences in making choices.
Empowerment is a term much used in health promotion. It is a complex concept that encompasses various levels of working for change:
Enabling people to change is often assumed by health promoters simply to mean health education. Such programmes are described by Keleher (2007, p. 145) as typically delivered as brief interventions or in a series of sessions covering those things the clinician or health promoter regard as important with compliance as the goal.
Client-centred health education is concerned with a person’s agency in decision-making. Such an approach acknowledges that people can take some control over their lives through knowledge, skills and confidence and it may enable people to identify structural barriers and facilitators to their health. This kind of empowering education was described by Paolo Freire (see Chapter 10) in his description of radical adult literacy pedagogy. Frequently however developing personal skills is equated with helping people to change, drawing on psychological theories of behaviour change, motivation and self-efficacy.
Several theories have attempted to explain the influence of different variables on an individual’s health-related behaviour:
This chapter explores the application of these models of behaviour change to health, and considers how an understanding of cognition and decision-making can be incorporated into empowerment and education strategies.
Definitions
According to social psychology theories of behaviour change, people’s behaviour is partly determined by their attitude to that behaviour. An individual’s attitude to a specific action and the intention to adopt it are influenced by beliefs, motivation which comes from the person’s values, attitudes and drives or instincts, and the influences from social norms.
Beliefs
A belief is based on the information a person has about an object or action. It links the object to some attribute. For example, a person believes that potatoes (object) are fattening (an attribute). Theories of health-related behaviour change are based on the idea that an individual’s behaviour will be based on his or her beliefs. In this example, the person will cut down on potatoes if they wish to lose weight. If this person is encouraged to believe that potatoes are not fattening but a useful bulk food, then he or she may include them in the diet. In other words, that information can influence beliefs which will then, in turn, influence behaviour. This simple model is sometimes referred to as the knowledge–attitudes–behaviour (KAB) model. Of course, behaviour change is never quite as simple as that. Information alone is neither necessary nor sufficient for behaviour change. The health risks of smoking are well known and yet 30% of the population continue to smoke.
Values
These are acquired through socialization and are those emotionally charged beliefs which make up what a person thinks is important. A person’s values will influence a whole range of feelings about family, friendships, career and so on. For example, values relating to sex and gender give rise to a number of attitudes towards motherhood, employment of women, body image, breast-feeding and sexuality.
Attitudes
These are more specific than values and describe relatively stable feelings towards particular issues. There is no clear association between people’s attitudes and their behaviour. Sometimes changing attitudes may stimulate a change in behaviour and sometimes behaviour change may influence attitudes. For example, many people continue to smoke despite a negative attitude to smoking. Yet once the behaviour is stopped, they may develop vehement antismoking views.
People’s attitudes are made up of two components:
Attitudes are very hard to change. They may be changed by providing more or different information, or by increasing a person’s skills. For example, a person’s attitude towards the benefits of exercise might be influenced by providing information about different types of physical activity and their effects on the body. It might also be influenced by improved performance which motivates the person and encourages him or her to think of exercise as enjoyable.
Festinger (1957) used the term cognitive dissonance to describe a person’s mental state when new information is given which is counter to that already held. This prompts the person either to reject the new information (as unreliable or inappropriate) or to adopt attitudes and behaviour which would fit with it.
 BOX 9.1
BOX 9.1Some people may become concerned and change when presented with information about health risks. Others may make some change such as switching to a lower-risk substitute (e.g. low-fat spread). Others may deny their risk, perhaps by underestimating the frequency or amount of their current behaviour.
Drives
The term ‘drive’ is used in the Health Action model (Tones & Tilford 2001) to describe strong motivating factors such as hunger, thirst, sex and pain. It is also used to describe motivations which can become drives, such as addiction. Some studies suggest that addiction is the consequence of frequently repeated acts which become a habit and its base is a psychological fear of withdrawal (Davies 1997). Social learning theory (Bandura 1977) uses the term instinct to describe behaviours which are not learned but are present at birth. Instincts can override attitudes and beliefs. Hunger, for example, can easily override a person’s favourable attitude and intention to diet.
Understanding the impact of people’s beliefs in their behaviour is key to addressing those issues. Take the example of smoking:
What personal skills are needed to take greater control over one’s health? Consider this in relation to a change of behaviour you have made.
Practitioners often prioritize knowledge and information over self-confidence and a belief that change is possible as well as a willingness and motivation to make a change.
The practitioner needs to understand what contributes to people’s decision-making about health and what makes some people more amenable to change than others. The social cognition models which we shall now consider highlight the following as important:
How do you explain consistent findings in many studies that show a gap between knowledge and behaviour change, e.g. 70% of the population know about the importance of 5 a day but only 35% of the population act on it (Scottish Executive 2005)?
Such findings illustrate that knowledge of health benefits is only loosely associated with behaviour change. Although opportunities to change are greatest in most affluent areas, little action is taken. Self-reported motivation is unrelated to propensity to change. Understanding the wider cultural frameworks such as pleasure, comfort and convenience underpinning decision-making is essential to motivating individuals and groups.
The following theoretical models try to unpack the relative importance of these factors, recognizing that what people say is not necessarily a guide to what they will do, and that there are numerous antecedent and situational variables.
The health belief model
The Health Belief model is probably the best-known theoretical model highlighting the function of beliefs in decision-making (Figure 9.1). This model, originally proposed by Rosenstock (1966) and modified by Becker (1974), has been used to predict protective health behaviour, such as screening or vaccination uptake and compliance with medical advice (e.g. Gillam 1991). The model suggests that whether or not people change their behaviour will be influenced by an evaluation of its feasibility and its benefits weighed against its costs. In other words, people considering changing their behaviour engage in a cost–benefit or utility analysis. This may include their beliefs concerning the likelihood of the illness or injury happening to them (their susceptibility); the severity of the illness or injury; and the efficacy of the action and whether it will have some personal benefit, or how likely it is to protect the person from the illness or injury.
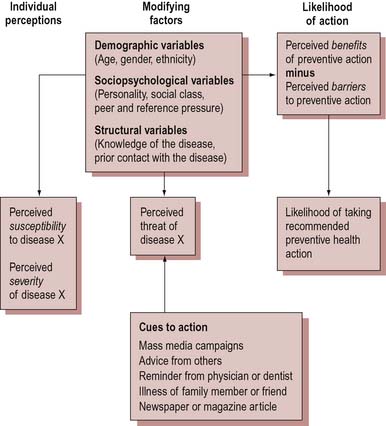
For a behaviour change to take place, individuals:
Consider the following situation and then try to apply the Health Belief model to see if you can predict how the woman might respond.
A mother of three children under 5 receives a card from her GP informing her that her youngest child should receive a Hib injection to protect him from meningitis. The woman works at a local factory as an hourly paid packer. Her mother cares for the children whilst she is at work, but has no transport.
If we are to use the Health Belief model as a model for predicting health behaviour, we would see the mother as a rational problem-solver who would not only be aware of the causes of Hib meningitis but also the risks of contracting it (the child’s susceptibility and severity). We would assume that the mother would have been made aware of the efficacy of the vaccine and be aware of its protection against one type of meningitis only (Haemophilus influenzae B). She would also be aware of any possible side-effects or contraindications. If the mother has had previous children vaccinated with no adverse effects or had this child or other children immunized against other diseases, she is more likely to view this vaccination favourably and have confidence in its effectiveness. In using this model as a predictor of behaviour, we need to take into account the perceived barriers and costs to taking this action. The mother would need to ask her own mother to take the child to the doctor. The child’s grandmother may be unwilling or unable to take three children on public transport. Or the mother would have to take time off work with consequent loss of earnings.
Most learning theories are based on the premise that people’s behaviour is guided by consequences. If these are positive or deemed to be positive, then the person is more likely to engage in that behaviour. These explanations, which see behaviour as a simple response to positive or negative rewards, do not seem to account for the persistence of health behaviours which have apparently negative consequences, such as smoking or drinking and driving. Short-term gratification is a greater incentive than possible long-term harm.
Becker suggests that individuals are influenced by how vulnerable they perceive themselves to be to an illness, injury or danger (their susceptibility) and how serious they consider it to be (severity). People’s perception and assessment of risk are central to the application of this model. Most people make a rough assessment about whether they are at risk. This seems to be influenced by four factors:
Where a situation is not well known however, people have an unrealistic optimism that ‘it won’t happen to me’ (Weinstein 1984).
 BOX 9.5
BOX 9.5There are over 250 000 traffic accidents each year with 30 000 casualties, of which 3400 are fatalities. Excess speed is a contributory factor in a significant number of road accidents. In one survey (Scottish Office 1998) 88% of drivers admitted to driving at 40 mph in a 30 mph zone at least sometimes. The current response to speeding is:
How might an understanding of social cognitions help to target a strategy for safer driving?
Since beliefs may be affected by experience, direct contact with those who have a condition can powerfully affect attitudes exposing stereotypes and prejudice. For example, contact with a person who is human immunodeficiency virus (HIV)-positive or who is living with acquired immunodeficiency syndrome (AIDS) can change beliefs about the fatality of the disease, and about who is affected and how.
Those who work with young people find perceptions of risk are very different. Risk-taking is an important task of adolescence and part of separation from family. It is hard for young people to appreciate the long-term effects of, for example, smoking when 25 can seem old.
Many health education campaigns have attempted to motivate people to change their behaviour through fear or guilt. Drink–drive campaigns at Christmas show the devastating effects on families of road accident fatalities; smoking prevention posters urge parents not to ‘teach your children how to smoke’. Increasingly hard-hitting campaigns are used amongst others to raise awareness of the consequences of binge drinking, smoking and drug use. Whether such campaigns do succeed in shocking people to change their behaviour is the subject of ongoing debate (see, for example, Hill et al 1998). Although fear can encourage a negative attitude and even an intention to change, such feelings tend to disappear over time and when faced with a real decision-making situation. Being very frightened can also lead to denial and an avoidance of the message. Protection Motivation theory (Rogers 1975) suggests that fear only works if the threat is perceived as serious and likely to occur if the person does not follow the recommended advice.
 BOX 9.6
BOX 9.6Questioner: ‘How do you think you’ll be in say 10 years’ time, in terms of health?’K (age 16): ‘Dead!’
T (age 15): ‘I don’t want to think about tomorrow, let alone 10 bloody years.’
The Health Belief model suggests that people need to have some kind of cue to take action to change a behaviour or make a health-related decision. The issue needs to become salient or relevant. The cue could be noticing a change in one’s internal state or appearance. For example, a pregnant woman stops smoking when she feels the baby move. It could be an external trigger, such as a change in circumstance like change in job or income, or the death or illness of someone close. It could be a comment from a ‘significant other’ or a newspaper article. Health care workers can be significant others. For example, GPs’ advice is taken seriously. The GP has expertise, is trustworthy and has authority, leading the patient to desire to comply. The effects of persuasive communications on attitudes are discussed more fully in Chapter 12 on mass media.
According to the 2005 Gay Men’s Sex Survey (Sigma Research 2005), 50% of sexually active gay men had unprotected anal sex in the previous year. A total of 40% of gay men were unaware of their own HIV status.
Consider how the Health Belief model could be used to explain this health behaviour.
What reasons could you offer for individuals not carrying out their intentions to act in ways that are perceived as beneficial?
Factors associated with HIV-positive men having unprotected sex were.
The Health Belief model has been widely criticized. Some of these criticisms relate to its lack of weighting for different factors – all cues to preventive action, for example, are seen as equally salient. It may appear that complex behaviour and actions are informed and chosen via analysis of a set of conceptual components that are isolated from one another. What we have seen so far is that behaviour is far more nuanced with many different interwoven arguments and scripts. The model may not be particularly helpful in predicting behaviour or identifying those elements that are important in influencing people to change, but it does highlight the range and complexity of factors involved.
Theory of Reasoned Action and Theory of Planned Behaviour
According to the Theory of Reasoned Action (Ajzen & Fishbein 1980), behaviour is dependent on two variables:
These two influences combine to form an intention.
Ajzen & Fishbein (1980) acknowledge that people do not necessarily behave consistently with their intentions. The ability to predict behaviour will be influenced by the stability of a person’s belief. Stability is determined by strength of belief, how long it has been held, whether it is reinforced by other groups to which the individual belongs, whether it is related to and integrated with other attitudes and beliefs and how clear or structured it is.
The Theory of Reasoned Action differs from the Health Belief model in that it places importance on social norms as a major influence on behaviour. Figure 9.2 shows the significance of this factor in the Theory of Reasoned Action. Social pressure may be exerted through societal norms (such as those relating to weight and body image), community norms, the peer group and the beliefs of ‘significant others’ (such as parents or partners).
The motivation to comply with perceived social pressure from ‘significant others’ could cause individuals to behave in a way that they believe these other people or groups would think is right. The influence of so-called peer group pressure (even if it does not amount to pressure) can be very powerful within a small group if the individual values membership of that group or wants to belong to it. Young people have many potential social pressures and increased social competition due to internet websites such as MySpace and Facebook, and are exposed to marketing and advertising that may encourage early adoption of a teen lifestyle.
Think of an occasion where social norms have influenced a health-related decision on your part. What was the most powerful aspect of this influence? Consider the following example of conformity with social norms.
‘Bill works in a predominantly male office. At the end of the day, five or six people adjourn to a local bar. The men are eager to establish themselves by buying a round of drinks. Bill waits until everyone has finished before offering to buy a round, by which time someone else has got to the bar. Bill usually only drinks one pint of beer but he stays until everyone has bought a round – six pints.’
The role of modelling has been particularly important in health promotion. Concern has been expressed that indirect modelling of behaviour may come from the media. For example, people on television are able to drink heavily without any apparent ill effects (Hansen 2003). Direct modelling is sometimes assumed to be less influential, but models who have status and credibility, such as musicians and people in sport, have been used to present health promotion messages. If people are influenced by role models, then health promoters may themselves be taken as exemplars.
Should health promoters ‘practise what they preach’?
Think of some examples where practitioners’ behaviour may be at odds with the health improvement they wish to promote.
Some health promotion programmes use the influence of the peer group to promote positive health. The rationale is that peers may be seen as having more credibility, are able to communicate in appropriate ways and are models to follow, although doubts may be expressed about the skills and information that peer educators possess (Wilton et al 1995; Harden et al 1999).
Social norms include peer group or family beliefs, but also what are perceived to be ‘general’ norms as conveyed by, for example, the mass media. What is important is what the individual believes other people do, not the actual extent of the activity. The World Health Organization has identified the importance of formal and informal social networks to support individuals and give people assistance in the pursuit of health (Wilkinson & Marmot 2003). Group techniques, such as those used by Alcoholics Anonymous, appear to have some success by getting clients to identify with the group through personal testimony and a public commitment, which encourages the group to provide support for each other.
Bandura’s (1977) social learning theory suggests that the health choices people make are related to:
Perceptions of self-efficacy are based on people’s assessment of themselves – whether they have the knowledge and skills to make changes in their behaviour and whether external factors such as time and money will allow that change.
How might observing others’ behaviour influence our own? To what extent does believing we can do something enable us to do it? How does thinking influence our behaviour?
Self-efficacy is determined by:
Personal judgement of worth expressed in the attitudes people hold towards themselves is also part of a sense of self-efficacy. We talk of high or low self-esteem in the sense of feeling more or less worthwhile and valued. Self-concept is a global term which refers to all those beliefs which people have about themselves – about their abilities and their attributes. It includes ideas about appearance, intelligence and physical skills. It is built and modified through our perceptions of the way other people behave towards us, how we are accepted and affirmed, or rejected and criticized. It will thus also derive from having a network of social support.
The development of self-concept and self-esteem has been at the centre of work in health education and promotion. It is assumed that people with high self-esteem are likely to feel confident about themselves and have social and life skills which will enhance their feelings of personal efficacy. Because of these feelings of personal effectiveness, the person’s self-esteem is enhanced.
Many health education programmes, particularly those targeted at young people, have been based on the premise that there is a relationship between low self-esteem and health behaviour. However a survey by the Joseph Rowntree Foundation (Perri et al 1997) found that those who had ever tried drugs had similar levels of sociability as young people in general but were more at ease and had a more relaxed attitude to the future. Programmes such as Drug Abuse Resistance Education (DARE) which aim to boost self-esteem by equipping young people with better skills to resist peer pressure and make independent decisions are thus unlikely to prevent drug experimentation.
Intention and behaviour in sexual decision-making
Personal or ‘micro’ factors are played out in many issues of choice and real-life decision-making is often not a rational process.
A study of HIV-positive people and sex (Ridge et al 2007) found that, although they may have the intention to use a condom, ‘irrational feelings’ such as intimacy, trust and desire could all influence perceptions of risk.
Ajzen further developed the Theory of Reasoned Action and recast it as the Theory of Planned Behaviour (Ajzen 1991) (Figure 9.3). This model incorporated another variable – that people’s behaviour is a consequence of their perceived control. People differ in the extent to which they think they can make changes in their lives. Social learning theory suggests that the ways in which people explain the things that happen to them are a product of their childhood experiences. Those who are rewarded for their successes and punished consistently and fairly will come to believe that they are in control of their lives. Those who have inconsistent rewards or punishments irrespective of their behaviour are more likely to see events as a consequence of chance and their own role as irrelevant (Rotter 1954).
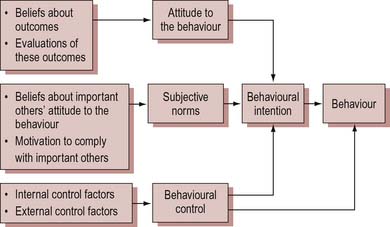
Control in the context of health can be understood in terms of:
What strategies can practitioners use to help build their clients’ confidence so that they feel more able to make changes in their health behaviour?
Research has focused on categorizing attitudes to health by using a locus of control measure such as a multiple-choice inventory. It has been assumed that those who have a strong internal locus of control will see themselves as more coping, and more able to act decisively and capably and will be those people who undertake preventive health actions or change to more healthy behaviours. So far it has generally been found that there is only a weak relationship between feelings of control and specific behaviours, although associations have been found with smoking cessation and weight loss and the propensity to use preventive medical services (Wallston et al 1978). Indeed, a lifestyle survey of 9000 adults found that ‘unhealthy’ kinds of behaviour are more likely to be associated with an internal locus of control (Blaxter 1990). At the same time, those who recorded positive or responsible attitudes to health were also more likely to have a high locus of control. This confirms the argument earlier in this chapter that specific behaviour cannot necessarily be predicted from attitudes.
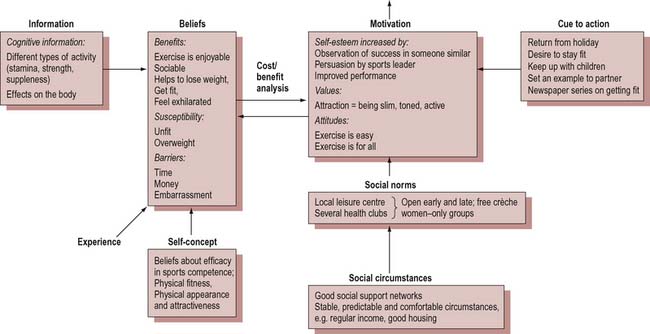
People who register as ‘externals’ on the multidimensional health locus of control scale are those with lower levels of education, and of lower socioeconomic class – in other words, people who have every reason to believe that they do not have much control over their lives or health status. Figure 9.4 is a diagrammatic representation of some of the influences on a person’s decision to take up an exercise programme. It shows how confidence to participate in physical activity could be built through positive attributions such as fitness and weight loss and through successful performance. Social support networks will also be crucial in maintaining commitment.
The Stages of Change model
So far in this chapter we have discussed the factors influencing the decisions people make in relation to their health.
Prochaska & DiClemente’s transtheoretical model (1984, 1986; Prochaska et al 1992) is important in describing the process of change. The model derived from their work on encouraging change in addictive behaviours, although it can be used to show that most people go through stages when trying to change or acquire behaviours.
Many people have had experiences of knowing what they ought to do and not doing it. Most people have tried and failed at some point in their lives to make a change in their health behaviour, such as giving up smoking or losing weight. Think about one of your experiences of failing to make a change. Why do you think the change did not last:
Now think about a change you have managed to make. Why do you think you were able to stick to this decision?
Figure 9.5 illustrates this process and identifies the following stages.
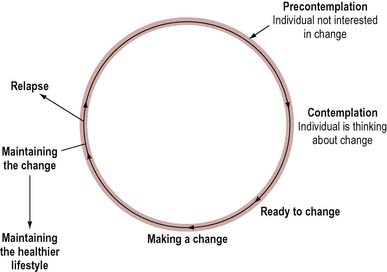
Precontemplation
Those in the precontemplation stage have not considered changing their lifestyle or become aware of any potential risks in their health behaviour. When they become aware of a problem, they may progress to the next stage. Assessing a client’s readiness to change is a key first step.
Contemplation
Although individuals are aware of the benefits of change, they are not yet ready and may be seeking information or help to make that decision. This stage may last a short while or several years. Some people never progress beyond this stage.
Preparing to change
When the perceived benefits seem to outweigh the costs and when the change seems possible as well as worthwhile, the individual may be ready to change, perhaps seeking some extra support.
Making the change
The early days of change require positive decisions by the individual to do things differently. A clear goal, a realistic plan, support and rewards are features of this stage.
Maintenance
The new behaviour is sustained and the person moves into a healthier lifestyle. For some people maintaining the new behaviour is difficult and the person may revert or relapse back to any of the previous stages.
Change is not a smooth process. Whilst few people go through each stage in an orderly way, they will go through each stage. This has proved helpful for many health care workers who find it reassuring that a relapse on the part of their clients is not a failure, but that the individual can go both backwards and forwards through a series of cycles of change – like a revolving door. Thus a smoker may stop smoking many times before finally giving up completely. Nevertheless the client is still aware of the benefits of giving up smoking and health care workers may be able to focus on such small changes, which can provide themselves and their clients with a sense of achievement and identifiable progress.
Whilst individuals may not have an awareness of contemplating, actioning and maintaining change, the intention will be based on individuals deciding that it is in their best interests to change. The key to successful interventions then is for a client to be motivated. Health promoters must bear in mind that their clients may not share their perceptions about the worth of a particular behaviour.
Motivational interviewing is a non-directive client patient-centred counselling style that aims to help clients explore their ambivalence about changing their behaviour. It starts with an exploration of the clients’ readiness to change (in keeping with the transtheoretical model of change) and how important change or the behaviour is to them (Miller & Rollnick 2002). Central to this technique is the view that motivation is enhanced if the client articulates the costs and benefits of change. The client’s confidence that change can happen is bolstered by support, discussion of barriers and negotiated action plans.
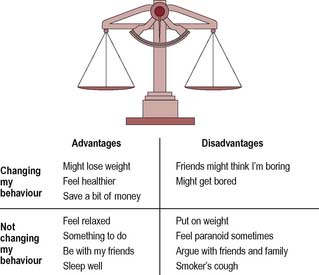
These techniques are widely adopted. Some have much in common with counselling techniques, as summarized in Table 9.1. One of the principles of motivational interviewing is that people feel some ambivalence about their health behaviour. One way of helping a person to become clearer is to use a decision balance matrix in which clients work out the costs and benefits of changing or not changing their behaviour, as illustrated in Figure 9.6 with a person exploring cannabis use.
Table 9.1 Using client-directed counseling techniques
| Do | Don’t |
|---|---|
| Summarize your understanding of the client’s thoughts and feelings | Interrupt or finish sentences |
| Look and sound interested | Advise or tell the client what to do |
| Keep eye contact and use positive body language | Disagree or contradict (raise alternatives) |
| See things from the client’s point of view | Project your own beliefs or feelings on to the client |
| Ask open questions to get more information | Assume your experiences are the same as the client’s |
| Be curious rather than intrusive | Constantly repeat the same paraphrases, e.g. ‘it sounds like’ or ‘you feel like’ |
| Give the client time to think as well as talk | Pretend you understand if you don’t. Ask for more explanation |
| Respond to what the client is saying rather than trying to lead the conversation |
From Michie et al (2006).
Health trainers
The White Paper Choosing Health: Making Healthy Choices Easier (Department of Health 2004) proposed the development of a new role for improving health – health trainers. These are people drawn from local communities and trained to reach those who want to adopt healthier lifestyles but don’t necessarily use local services.
Self-empowerment approaches have at their centre the principle of participation. These techniques allow people to examine their own values and beliefs; explore the factors which affect the choices they make; and develop the skills to act upon their intentions. In addition to techniques such as motivational interviewing and client-centred counselling, educational drama, story-telling, assertiveness and negotiation skills training, and problem-solving may be used.
The Prerequisites of change
All the models of behaviour change discussed in this chapter suggest that people are involved in a rational processing of information when they make a decision. People are not usually so consciously rational, as this study of the health beliefs of working-class mothers in south Wales illustrates:
In the subjects we studied there was little evidence of a rational approach to the personal decision-making process, i.e. a weighing up of the advantages and disadvantages of a particular change followed by a decision to act. Instead any change was a consequence not just of thought but also a mix of emotion, habit, impulse, social influences and bolshie lack of forethought, which is so typically human (Pill & Stott 1990).
Pill & Stott’s study of self-initiated change shows the importance of precipitating life events and the minor part played by health concerns. For example, women who gave up smoking did so to save money and those who took up exercise did so to join in with their children.
The importance of considering the social context and everyday life is brought out clearly by this study, which showed that eventually most women reverted to their original behaviours because of the influence of partners or children, or because it was too difficult to juggle personal and family priorities.
The evidence from people who have changed their health behaviour suggests that there are certain minimum conditions required for that change to take place.
The change must be self-initiated
Some people react adversely or wish to contain any attempt to look at their ‘unhealthy behaviour’. To some people, their behaviour may not seem unhealthy at all but may constitute a clear source of well-being, its benefits far outweighing its risks. There is a clear message here for those health promoters who work with individual clients and who are sometimes accused of ‘telling people what to do’ – people will only change if they want to.
The behaviour must become salient
Most health-related behaviours, including smoking, alcohol use, eating and exercise (or lack of it), are habitual, and built into the flow of everyday life such that the individual does not give them much thought. For a change to occur, that behaviour or habit must be called into question by some other activity or event so that the behaviour becomes salient. For example, a smoker going to live with a non-smoker causes the smoking behaviour to be reappraised. The death of a relative from breast cancer may similarly prompt a woman to go for screening.
The salience of the behaviour must appear over a period of time
The habitual behaviour needs to become difficult to maintain. The new behaviour must, in turn, become part of everyday life. For example, one reason why people on diets often resume their previous eating pattern is because they are made constantly aware of the diet and it is never allowed to become a habit. Similarly, exercise is often not maintained because it requires effort; hence the advice to reluctant ‘couch potatoes’ to build physical activity into their daily life by walking to work or running up stairs rather than going out to exercise at a pool or gym.
The behaviour is not part of the individual’s coping strategies
People have various sources of comfort and solace, and will resist change to these behaviours. It is sometimes possible to enable clients to identify alternative coping strategies. For example, a person who eats chocolate when depressed may be encouraged to become physiologically aroused by taking up jogging.
The individual’s life should not be problematic or uncertain
There is a limit to a person’s capacity to adapt and change. For example, those living on low incomes will be stretched by coping with poverty and its uncertainties. Having to make changes in their health behaviour may be too much to expect for people whose lives are already problematic.
Social support is available
The presence and interest of other people provides reinforcement and keeps the behaviour salient. Changing one’s behaviour can be stressful and individuals need support. The influence of peer group pressure and support is not given sufficient weight in the various psychological theories of change.
Conclusion
What is clear from this outline of psychological theories of behaviour change is that none provides a full explanation. However, the variables identified by these models do appear in people’s accounts of their health behaviour:
Whilst these models may not help to predict who will adopt preventive or protective health practices, they can help to plan programmes of education by making clear those factors which influence decisions.
Elsewhere in this book we argue that a focus on people’s health lifestyles can minimize the structural barriers such as poverty or discrimination that may make choices more difficult for some groups. The client-centred approaches described reflect a shift away from traditional didactic and persuasive methods. Their aim is to enable clients to have the understanding and skills to translate intention into practice. Those most likely to benefit, however, are people with good education and literacy, social support and personal and economic resources. For this reason such approaches must be accompanied by broader programmes that make the healthier choice the easier choice.