Chapter 12 Using media in health promotion
Overview
Communication of information and advice is central to health promotion strategies. A knowledge of how communication between the sender and receiver of messages takes place and an understanding of the medium through which communication occurs are therefore important tools for the health promoter. Mass media is a powerful agent of communication, reaching large numbers of people. In addition to the traditional media (radio, television, press) new forms of media, most notably the internet, have changed communication patterns and coverage. The mass media now combines the capacity to reach large numbers of people with the capacity to be accessed individually as and when people choose. Mass media has a long history of persuading people to buy a vast array of products and lifestyles which create ill health, such as tobacco, alcohol and fast cars, through both paid advertising and current affairs coverage. Paid advertising and campaigns, unpaid news coverage, social marketing and media advocacy are all used to promote health. Practitioners also use posters, leaflets and other tools to enhance communication with service users. This chapter looks at the potential and limitations of using various media in these different ways to promote health. Readers can find a more detailed discussion of health communication and social marketing in Chapter 8 of our companion volume (Naidoo & Wills 2005).
Introduction
The term mass media includes any communication which reaches large sections of the population. Exam-ples of mass media are television and radio broadcasting and print media such as newspapers, posters and leaflets. The mass media is a ‘broad-spectrum’ intervention, as distinct from ‘narrow-gauge’ personalized interventions tailored to individuals and small groups. The use of public announcements to promote health also has a long history:
 BOX 12.1
BOX 12.1In 1603 James I, King of England, made a public declaration that smoking is:
A custom, lothesome to the eye, hateful to the Nose, harmful to the brain, dangerous to the Lungs and in the black stinking fume thereof, neerest resembling the horrible Stigian smoke of the pit that is bottomelesse … by the immoderate taking of tobacco, the wealth of a great number of people is impaired and their bodies unfit for labour.
More recently, the powerful effects of propaganda during the Second World War were influential in persuading health promoters to adopt a similar strategy. In 1953 John Burton, the editor of the Health Education Journal, stated that:
The first 10 years of our existence could well be called the era of propaganda. Health education has been realised mainly in terms of mass publicity on all fronts. Ad hoc exhortations have been directed at the public following closely the patterns of commercial advertising (Burton, cited in Tones 1993, p. 128).
However, by this time there had already developed a concern that such a strategy was not working and that the role of the mass media in health promotion needed to be redefined:
Many [have come] to feel that mass publicity methods were expensive and relatively ineffective in changing people’s health habits and beliefs, and that health education would have to be planned on a more personal basis (Burton, cited in Tones 1993, p. 128).
 BOX 12.2
BOX 12.2The relationship between the media and the public is complex. In addition to its primary function of informing and entertaining, the media plays a pivotal role in social cohesion, defining what is normal and desirable, and what is not. McQuail (2005) identifies several different roles played by the media:
The mass media is important to health promotion because it is so widely used. Many public health issues, e.g. human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS), alcohol misuse and smoking have been the subject of extensive mass-media campaigns. The aim of such campaigns is usually to raise awareness or present a message advocating healthy lifestyles (Figure 12.1). Beattie (1993) describes the use of the media as ‘health persuasion’, by which he means a top-down conservative method designed to infuse an audience with information.
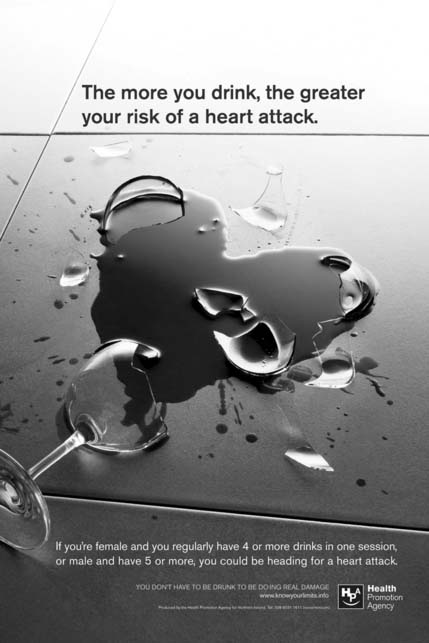
Figure 12.1 Alcohol poster from Health Promotion Agency Northern Ireland. Reproduced with permission from the Health Promotion Agency for Northern Ireland: photography, David Gill.
The media may also be an unhealthy influence, advertising unhealthy products, e.g. fast food, or transmitting unhealthy messages, e.g. that drinking excessively is fun and fashionable. The media also plays a major role in constructing society’s views on health issues and services. What health issues are covered, and the slant the reporting takes, are powerful forces in public discourse around health.
The nature of media effects
The mass media is a distinctive form of communication with specific properties, including:
These characteristics include both strengths and weaknesses when the aim is to promote health. Although a mass audience is guaranteed, with favourable cost implications, ‘correct’ reading, understanding and recall of the intended message by the target audience is by no means certain. A great deal of research is needed to develop suitable messages that will appeal to the target audience and to evaluate their real-life impact. Chapter 8 in our companion volume (Naidoo & Wills 2005) discusses the nature of health promotion messages.
Views on the effects of the mass media have shifted from an early belief that the mass media could produce dramatic changes in attitudes and behaviour to the opposite view that the media has negligible effects (Gatherer et al 1979). Today there is a more tempered view, which regards the media as influential in certain circumstances and in specific ways. For example, a recent systematic review concluded that the use of mass media in promoting the use of health services was effective (Grilli et al 2002). The West Yorkshire Smoking and Health Trial (McVey & Stapleton 2000) demonstrated that a prolonged, heavy-weight, well-resourced mass media campaign can contribute to a significant reduction in smoking prevalence.
Lasswell (1948) presents the following model of mass communication:
Lasswell’s model is useful in flagging up all the key stages of the process of mass communication:
This model was developed with traditional forms of mass media in mind, and its applicability to newer forms of instant and overlapping communication and technologies has been questioned (Chamberlain 1996). The new technologies, such as text messaging or social network sites, are particularly relevant if young people are the target group. Young people are media-literate, i.e. they can access, understand and create communications using a variety of new technologies, including the internet and mobile phones. These new forms of communication may be used to promote health. Text messaging has been successfully used to improve self-management of diabetes (Franklin et al 2006), and has also been used to engage young people in health messages (Dobkin et al 2007). Atkin (2001) has argued that the new interactive and individually tailored communication technologies empower users. Benefits of these new means of communication include relative anonymity, avoidance of stigmatization and marginalization and immediate access wherever people are.
Four main models of how the media affects audiences have been suggested:
Direct effects (linear causal)
This model likens the effects of the mass media to a hypodermic syringe that has an immediate and direct effect on its audience. It assumes a passive audience which can be swayed by manipulative mass media. This view prompted the development of political broadcasts intended to shift voting intentions.
In 1938 Orson Welles broadcast a radio version of H G Wells’ classic science fiction story The War of the Worlds. Thousands of American listeners assumed that the story of an imminent alien invasion from outer space was real and panic spread as people started to flee (Cantril 1958).
This view has since been replaced by an aerosol spray analogy:
Rather than being a hypodermic needle, we now begin to look at mass communication as a sort of aerosol spray. As you spray it on the surface, some of it hits the target: most of it drifts away; and very little of it penetrates (Mendelsohn 1968).
Some people argue that representations of people consuming large quantities of alcohol, being violent or engaging in unsafe sexual activities encourages viewers to do the same. They argue for tighter censorship and controls. Others argue that censorship stifles public debate and different views and opinions, and removes personal freedoms. What do you think?
Two-Step or diffusion of innovation model
This model suggests that mass communication influences key opinion leaders who are active members of the mass-media audience. These opinion leaders then spread ideas to other people through interpersonal means of communication (Katz & Lazarsfeld 1955). The process of diffusing innovation or new ideas through a population is based on the finding that the adoption of new behaviours typically follows an S-shaped trajectory (Rogers & Scott 1997). There is usually a slow initial uptake followed by rapid acceptance, as opinion leaders or early adopters (who are usually from higher socioeconomic groups) communicate the benefits, and then a final slowing as a minority (who tend to be from isolated traditional communities) resist acceptance or change. This suggests that the mass media may be important in raising awareness and communicating basic information, but interpersonal sources, such as friends, peers and known ‘experts’, are most influential in persuading people to make changes.
Uses and gratifications
This model tends to see the audience as more active in selecting and interpreting communications. It suggests that people use the media to meet their own needs, reinforcing existing beliefs or rejecting or reinterpreting communications that do not fit their existing values or beliefs.
Cultural effects
This model sees the media as having a key role in creating beliefs and values about health, medicine, disease and illness. The ways in which these are presented, from the kindly doctor in soap operas, to news bulletins on miracle cures and high-tech interventions, all contribute to people’s understanding of health (see, for example, Lupton 1994). Many studies use discourse analysis to reveal the underlying values, concepts and messages implicit in media portrayals of health and ill health. For example, Joffe & Haarhoff (2002) analyse the ways in which diseases such as Ebola are presented as deadly uncontrollable viruses whilst simultaneously giving the message that such diseases pose little threat to the UK. Harrabin et al (2003) argue that public health is neglected in the media. Public health’s long timescale and basis in numerical data make it unattractive to the mass media. Instead, ‘shock horror’ stories of crisis within the National Health Service (NHS) or the appearance of rare diseases tend to dominate the news headlines.
 BOX 12.5
BOX 12.5Monitor media coverage on television, in magazines, on radio, in broadsheet and tabloid newspapers for items about health over a 1-week period. Use the following categories to allocate coverage by type:
Does the media coverage you monitored fit into these categories?
Which categories were least/most common? What are the implications of this?
How much of the coverage was in entertainment programmes?
Think about and find some examples of how the following are represented in popular media culture:
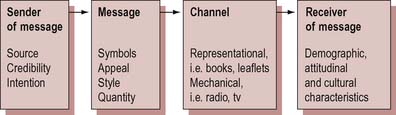
Communication is concerned with the transmission of messages from a sender to a receiver. Messages are coded into signs and symbols which have meaning within specific codes. The message is encoded by the sender, and decoded by the receiver (Figure 12.2). The intention is that messages should be decoded and understood according to the intentions of the sender, but this can be problematic when using the mass media. This is because the mass media targets large audiences simultaneously, and, unlike direct personal communication, there is typically no feedback loop from the receiver back to the sender of the message. This means messages may be interpreted in ways that were not anticipated or intended by the sender. This is one reason why researching the target audience and piloting messages is an important stage in the planned use of the mass media for health promotion.
The role of mass media
Mass communication has been used in health promotion in the following ways:
Planned campaigns
Mass-media campaigns have been used by national health promotion agencies in the UK and worldwide to promote various health messages. Different media, including billboards, press advertisements and radio announcements, have been used, but television is the principal medium because, although it is expensive, it reaches much larger audiences and recall has been shown to be better. The end goal of most media campaigns is to achieve a specific behaviour change, although their ability to achieve such aims is disputed. Harrabin et al (2003) state that members of the public may alter their health related behaviour due in part to the information and advice they get from the media.
Evaluation of mass-media campaigns
These examples suggest that on their own, mass-media campaigns are unreliable in achieving behaviour change. However, used in combination with other strategies, such as personal reinforcement from trusted peers or experts, or policy changes affecting the environment, mass-media campaigns can be effective.
Mass-media campaigns adopt a variety of tactics to communicate their message, including emotional appeals, shock tactics and reassurance. The evidence on whether or not fear is an effective strategy is inconclusive. Early studies showed that people may attend, comprehend and retain information when shocked, but may also become resistant or deny the relevance of the message (Montazeri et al 1998). The use of fear appeals in social marketing has been criticized for its relative ineffectiveness and its unintended negative consequences (e.g. anxiety, complacency and increased social inequity) (Hastings et al 2004). However a review of mass-media antismoking campaigns (Grey et al 2000) concluded that ‘threatening’ and ‘supportive’ approaches could complement each other and contribute to overall effectiveness. What was important was an appeal to the emotions, coupled with supportive messages. It is also important to present a clear action which individuals feel confident they can take (Barth & Bengel 2000).
Extensive reviews of media campaigns now conclude that they may be successful if their goals are reasonable and there is no expectation of immediate results. Tones & Tilford (2001) refer to the hierarchy of communication effects which suggests that simple awareness or market penetration is relatively easy to achieve; to inform or reinforce attitudes is more difficult, and to have any effect on behaviour is even more difficult. They identify certain preconditions for success:
Evaluation of a mass-media campaign to reduce drink-driving could take many forms. Evaluation studies often look at coverage (the percentage of the target population who were exposed to the message), recall (the percentage of the population who could accurately recall the message) or the impact of the campaign on behaviour. Behavioural indicators include statistics relating to the incidence of drink-driving, but the evaluation would probably also examine the incidence of alcohol-related car accidents as this is the main cause for concern and is likely to be better monitored than drink-driving. The evaluation might also include examining the cost-effectiveness of such a campaign (see Example 12.8).
Mass-media campaigns to reduce drink-driving
Two systematic reviews of mass-media campaigns to reduce drink-driving and related car crashes agree that such campaigns are effective. Tay (2005) found that mass-media campaigns significantly reduce drink-driving and alcohol-related crashes and result in large savings. Elder et al (2004) found an average decrease of 13% in alcohol-related crashes following mass-media campaigns, and concluded that the benefits to society outweighed the costs.
Unpaid media coverage
The term ‘unplanned’ is used to describe media coverage that is not specifically paid for as part of a campaign. Health promotion has become increasingly concerned to generate news stories. Campaigns can extend their reach enormously through unpaid coverage.
The mass media has no responsibility to promote health and so if they address such issues it is because the issues are inherently newsworthy, or have been packaged by health promoters to become newsworthy. The tendency to sensationalize means that it is the emotional, the dramatic or the tragic that gets space. Stories tend to relate to individuals, and issues which concern population groups such as older people or the determinants of health thus are ignored. The emphasis on behavioural journalism means that personalities or real-life case studies are also prominent. Newsworthiness depends less on the importance of an issue than on its immediate impact, which is often heightened by being linked to celebrities in emotive ways. For example, the involvement of celebrity Jamie Oliver led to a dramatic increase in media coverage of children’s diets and healthy school meals.
Newsworthiness of health issues
Chapman & Dominello (2001) found that newspaper coverage of tobacco and health issues could be significantly affected and increased through a strategy of proactive press reports. The key to increased media coverage was to use newsworthy aspects, e.g. the use of celebrities, moral panics or medical scares, to contextualize the story. Giving a local spin to general stories will also ensure coverage in regional media.
Although such tactics may increase coverage of the work of health promoters and put across health messages, the ability of the media to distort and sensationalize should always be remembered. An editorial in The Observer newspaper in 1994 commented: ‘There is nothing quite so irresponsible as the media in hot pursuit of a health scare and nothing quite so gullible as the public presented with one’. The editorial had been prompted by a concern about necrotizing fasciitis (a tissue-destroying disease caused by a strain of bacteria) which was neither new nor on the increase, but which had prompted headlines such as ‘Killer bug eats my body’ or ‘Flesh-eater on the move’.
Reid (1996) observes that media interest can be generated by the commissioning of surveys or research reports. However, such reports frequently result in health scares because of poor reporting and misunderstanding of statistics and the concept of risk. An example is the research study linking the measles, mumps and rubella (MMR) vaccine to the development of autism and Crohn’s disease in young children, which led to a drop in MMR uptake immediately following the press reports.
Take a current issue which has received a lot of media coverage, e.g. bovine spongiform encephalitis (BSE), young people’s alcohol and drug use or the rising incidence of obesity, especially amongst children and young people.
Although the generation of unpaid publicity can be effective and at minimal cost, it is difficult to sustain a high level of coverage for more than a few days. Health promoters need persistence and creativity to keep issues prominent in the media. There is also a need for media training for health promoters in skills such as writing press releases, networking and design in order to access and use the media to its full potential.
No Smoking Day (NSD) is an example of a successful ongoing event. NSD is a charity with no budget for advertising, yet it succeeds in generating media coverage of the day as well as increasing the use of quit-smoking helplines. Evaluation of this public awareness campaign, which is supported by local activities, demonstrates its effectiveness. In 2004 an estimated 1 in 7 of UK smokers claimed to have quit or reduced their consumption on NSD. Among those who participated, 11% were still non-smokers 3 months after the event (Owen & Youdan 2006).
Media advocacy
Public policy is rarely a consequence of direct approaches to policy-makers and increasingly there is a recognition that public opinion can influence decisions. Media advocacy is a particular strategy of using the media to try to generate public concern about the ways in which the legislative, economic or environmental context affects public health. Examples include promoting the smoking ban in public places and the debate surrounding food-labelling regulations. Media advocacy is therefore a means of applying pressure for policy change to advance public health objectives (Wallack & Dorfman 1996). Often there is major opposition from established economic interests to the proposed policy change. The conflicting interests in many health-related areas can lead to split loyalties, and there have been calls for media advocacy to be undertaken independently of any official health promotion or public health posts (Regidor et al 2007). Media advocacy objectives are:
Chapman (2004) lists 10 questions that can be used to guide careful planning and lead to positive results, including identifying desired public health objectives and media advocacy objectives, and how to frame the issue in a favourable light, including what sound bites, symbols and words to use, and how it might be personalized. Weinreich (1999) identifies five key stages in media advocacy:
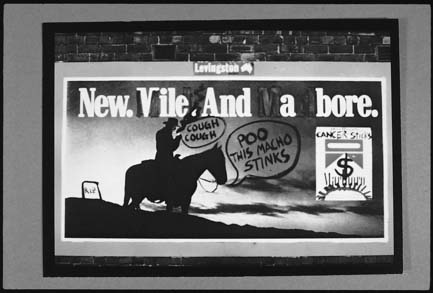
Chapman & Lupton (1994) emphasize the importance of the media in achieving policy change: ‘There are few instances in the recent history of public health where advocacy staged through the news media has not played a pivotal role in effecting the changes sought by public health workers.’ An example of successful media advocacy involving international cooperation was Infact’s Nestlé boycott of the 1970s and 1980s which led to the World Health Organization’s International Code of Marketing for Breast Milk Substitutes (McKee et al 2005). Direct action can also be successful, as evidenced by the Billboard Utilising Graffitists Against Unhealthy Promotions (BUGA-UP), an Australian group which targeted tobacco advertising (Figure 12.3) (McKee et al 2005).
Consider the ways in which mental health issues are reported in the media.
How could the media be actively used to get mental health issues discussed differently?
Stuart (2006) has shown how entertainment and news media provide images of mental illness that emphasize danger, criminality and unpredictability. This kind of coverage has a negative impact on people with mental health problems, leading to further stigmatization.
Social marketing
Just as commercial companies are able to get the public to buy products (even those they may not really need), so health promoters should be able to get people to choose healthy behaviours. Some of the techniques of marketing are now being widely used in health promotion to influence the acceptability of healthy lifestyles so that they seem desirable and easy to adopt. One of the limitations of mass-media campaigns is that they are a one-way communication process and tend to adopt a uniform population message. Increasingly, health promoters are making use of social marketing techniques that allow specific groups to be targeted (Naidoo & Wills 2005). Marketing segments the population into different subgroups based on attitudes and behaviour as well as cruder socioeconomic and demographic variables.
Commercial marketing is based on the idea of ‘exchange’ – that the marketer tries to provide something the consumer wants at an acceptable price. Health promoters are beginning to recognize the importance of formative research, which carefully identifies what people see as the benefits of particular health behaviours, so that these can be incorporated into the campaign message. In a sense this is merely an application of the Health Belief model (see Chapter 9) which suggests that for people to make a change in their health behaviour they need to see the benefits outweighing costs such as time and effort.
Marketing a commercial product is very different from trying to sell health. Advertising typically mobilizes existing predispositions, whereas health promotion typically tries to counter them. For example, advertising associates the product (beer, crisps) with something people desire, such as fun. All too often, health promotion messages are about not indulging, and therefore by implication, not having fun (don’t drink and drive, eat less fat). Advertising is selling things in the here and now, to be consumed and enjoyed immediately. By contrast, health promotion messages are often about forgoing present enjoyment for future benefits.
As we have seen, selling a product is a complex and carefully researched process. The needs of the market have to be identified, messages developed which will appeal to the market segment that is being targeted, and a comparison made of different media channels and their relative effectiveness in reaching a general and the targeted population. Together these aspects make up the marketing mix.
The marketing mix: the four Ps:
Social marketing – the application of marketing principles to ‘sell’ ideas, attitudes and behaviours to benefit the target audience and society in general – poses additional challenges. Additional Ps have been suggested for social marketing, including:
What the mass media can and cannot do
Research and evaluation of the use of the mass media in health promotion have led to a reassessment of its potential and limitations (see particularly Tones & Tilford 2001). It is now accepted that the mass media can:
Factors which enable behaviour change include existing motivation, supportive circumstances and advocating simple one-off behaviour change (e.g. carry a donor card, install a smoke alarm).
Communication tools
A majority of patients actively seek information about how to cope with health problems, of whom three-quarters cite their doctor as the most important source of health information. About a third use the internet and a quarter look for information in leaflets and books (Coulter et al 2006). Leaflets and pamphlets have been used to educate the public since the beginning of the 20th century. When the Central Council for Health Education was established in 1927 it listed the provision of better and cheaper leaflets as its main aim. The greatest use of written material is to support one-to-one interactions with clients and patients. As only 50% of information can be recalled by patients 5 minutes after a consultation, this seems an effective use of leaflets. There is some evidence that written information can not only improve patients’ understanding and recall, but also provide reassurance.
Multimedia tools and other new technologies offer many new opportunities for the dissemination of information. The worldwide web offers the possibility of interactive dialogue and for the public to select the information they require at a time convenient for them. These new forms of media are very popular. A survey in 2001 found that almost 100 million American adults regularly visit health-related websites (Wilson 2002). Telemedicine, including the helpline NHS Direct, offers a two-way dialogue allowing people who are unable to access primary care to ask questions and get feedback about their symptoms. These new technologies offer a simulation of human interaction – conversations, the café, support groups – all of which can be harnessed to link health information with the important element of sociability.
The proliferation of avenues of communication does not necessarily mean that people are better informed about health issues today. Quality control is often absent (e.g. in much of the worldwide web), and even when it exists, the criteria used are often not explicit. Commonly agreed criteria include being up to date, using reliable sources of information and information that is reliable, relevant, accurate and accessible (e.g. as assessed by readability tests) (Shepperd et al 1999; Coulter et al 2006).
Conclusion
The mass media is a significant partner and resource for health, but one that needs to be understood and used according to its own priorities. To expect a mass-media campaign to produce large shifts in behaviour and contribute directly to reduced morbidity and mortality is unrealistic. But the media can work for health by supporting individual and social change.
On an individual level, the mass media can supplement, but not substitute for, one-to-one education and advice. Even with sophisticated marketing and audience research, the mass media remains a fairly blunt instrument with little opportunity for feedback or clarification. However, the media can raise awareness, provide information and motivate people to change if their environment is supportive. The media can also be used to advocate for public health by shifting public opinion and encouraging the formation of healthy public policies. The media can also be used for social marketing, to promote attitudes, beliefs and behaviours that are conducive to health. Other forms of media, such as leaflets and posters, can provide a useful supplementary communication tool to inform, educate and advise people about health issues.