Chapter 8 Reorienting health services
Overview
Many agencies, services and practitioners contribute to the promotion of health and this chapter outlines the role of these stakeholders and different occupational groups. A reorientation of health services towards prevention was one of the key action areas of the Ottawa Charter (World Health Organization 1986), yet it is the least successfully applied. Health promotion poses several ambitious challenges for the health care sector: to extend the core business of health services from clinical outcomes to quality of life; to extend the focus from patients and relatives to staff and the wider community; and to integrate prevention into care and cure practices. To do so can only be achieved through organizational and funding changes. This chapter discusses these challenges, the practitioners and agencies involved in promoting health, and how their contribution to health promotion can be mainstreamed and validated. The provision of health and social care services differs widely from country to country, and this chapter focuses on the UK experience.
Introduction
Historically the cure and treatment of illness have taken precedence over the prevention of ill health, or the promotion of positive health in the organization. Most people thinking of health services think of hospitals and family doctors, a focus on treatment, developments in surgery and new techniques and more effective medicines. There is widespread acceptance that prevention is better than cure and it is the only rational way forward for public health. Yet a recent review claims that 1.5 million pounds sterling is spent on prevention and health promotion in the UK each year, which is the sum spent on the National Health Service (NHS) in a day and a half (Wanless et al 2007). Part of the reluctance to invest in prevention is because the benefits accrue over time and so with limited resources and a pressure to demonstrate results, the focus of health services becomes skewed towards care.
Whilst the contribution of health services to longevity is clear, as we saw in Chapter 2 many factors unconnected with health services have a profound impact on health. For many health promotion practitioners, the contribution of health care services in addressing the determinants of health is marginal (Wise & Nutbeam 2007). However health services do have a unique and significant contribution to make towards population health. This chapter argues that health services, defined as ‘all the activities whose primary purpose is to promote, restore, or maintain health’ (World Health Organization 2000) are critically important in progressing health and human development.
 BOX 8.1
BOX 8.1The Commission on the Social Determinants of Health (World Health Organization 2007, p. viii) has considered the contribution of health systems to equity. In pairs, decide to be A or B and develop some examples and argument to support the statements below:
What these statements illustrate is that, whilst health services may be a trusted focal point for any society, they may inadvertently contribute to inequity. In Chapter 4 we outlined the case made for health promotion by the Ottawa Charter of 1986 which stated that health care should encompass traditional education, disease prevention and rehabilitation services but also ‘health enhancement by empowering patients, relatives and employees … enabling people to increase control over, and to improve, their health’. Not only would this involve ‘open[ing] channels between the health sector and broader social, political, economic and physical environmental components’, but it would also demand a ‘change of attitude and organization of health services which refocuses on the total needs of the individual as a whole person’.
 BOX 8.2
BOX 8.2Reorienting health services is the least successfully applied of the Ottawa Charter’s key action areas (Wise & Nutbeam 2007). What might be the reasons behind this? Is there a case for continued or enhanced action to reorient services?
Resistance to reorienting health services is primarily due to the organizational tradition and culture, particularly within the state-funded NHS, of providing treatment and care. This acute-care paradigm means that all too frequently health practitioners view their role as patching people up and sending them home. Prevention is seen as ‘helping people to get better by doing what is good for them’, with patient compliance as an important objective. Patients who do not take advice may be seen as demanding and, in some cases, refused treatment if they do not follow recommended behaviour change. In countries funded by social contributions, practitioners who are paid by a fee for service have little incentive for prevention and activities such as managing chronic disease or health education which are time-consuming and bring no financial reward.
Yet there is some evidence of change and a recognition of the need to move towards a national health service and away from being a sickness service (Department of Health 2005, p. 119). The focus has shifted from treatment for acute conditions to the management of chronic conditions and the maintenance of optimum health. In recent years, ‘self-management’, ‘collaborative’ care, ‘shared decision-making’ and ‘the expert patient’ have become integrated into the management of chronic lifestyle conditions such as diabetes. Our companion volume Public Health and Health Promotion: Developing Practice (Naidoo & Wills 2005) discusses these moves to involvement and participation by patients and the public in health service planning and delivery in Chapter 6.
A major incentive for the reorientation of health services is economics. Increased longevity and expectations coupled with the rising costs of health services have led to a concern with the cost-effectiveness of services. There is growing evidence of the economic case for shifting focus from treatment to health promotion. A major UK review to examine health care funding needs (Wanless 2002) concluded that the ‘fully engaged scenario’, in which people self-manage their health and the NHS embraces prevention, is the most cost-effective.
Promoting health in and through the health sector
In addition to its obvious role of providing health care services, the health sector plays a major role in promoting health through being:
The NHS is a social setting just like a school or workplace. It has its own organizational procedures, values and ethos and cultural norms. For it to embrace health (rather than the treatment of disease) as its goal requires a change in all these elements.
The health service is an important setting for health promotion because it offers a range of health professionals the opportunity to integrate health promotion into their practice, and thus to fulfil the early promise of a comprehensive and health-promoting health service.
There are several unique characteristics of the health service setting that make it ideal for promoting health. Use of health services is universal, so that everyone at some point in their lives comes into contact with health service providers. For many more vulnerable groups, such as people with long-standing limiting illness, contact is long-term and frequent. In the UK 97% of the population is registered with a general practitioner (GP) and 70% consult their GP at least once a year. Health practitioners enjoy high levels of trust and credibility amongst the general population and thus have the ability to affect people’s knowledge, attitudes and beliefs. The NHS is the country’s largest single employer and therefore workplace initiatives may affect a significant percentage of the workforce and their families. All these factors provide good reasons for prioritizing the health services as a setting for health promotion. Chapter 16 discusses the hospital as a health-promoting setting.
Primary health care and health promotion
The 1978 Alma Ata declaration (World Health Organization 1978) defined primary care:
Primary health care seeks to extend the first level of the health system from sick care to the development of health. It seeks to protect and prevent the problems at an early stage. Primary health care services involve continuity of care, health promotion and education, integration of prevention with sick care, a concern for population as well as individual health, community involvement and the use of appropriate technology.
Primary care is often used interchangeably with primary medical care as its focus is on clinical services provided predominantly by GPs, as well as by practice nurses, primary/community health care nurses, early childhood nurses and community pharmacists.
Primary health care (PHC) incorporates primary care, but has a broader focus through providing a comprehensive range of generalist services by multidisciplinary teams that include not only GPs and nurses but also allied health professionals and other health workers. PHC services also operate at the level of communities. The Royal College of General Practitioners (www.rcgp.org.uk) identifies the functions of the PHC team as:
There are 60 000 primary care physicians in France, about 1.7 per 1000 people, which is double the number in the UK. There are just over two primary care nurses, including health visitors, per doctor in France, which is about half the ratio of the UK.
In many countries, such as France, there has been a move away from PHC in favour of a centralized hospital system. Community care is delivered by medical practitioners with much less involvement in providing a broad PHC with health promotion at its core.
Primary health care principles
The PHC approach is characterized by the following principles:
Primary health care: strategies
PHC strategies need to be consistent with the underlying philosophy of health promotion. In Chapter 5 we discussed various approaches to promoting health, of which education is one approach. Through education, communities and individuals gain understanding of the factors influencing their health and can work to gain control over health problems. The term empowerment is often used to describe patient education or any communication with a patient that is client-centred in its orientation. Yet empowering approaches necessitate organizational and environmental change. Figure 8.1 shows how empowerment and health gain can be built into nurse–client contacts.
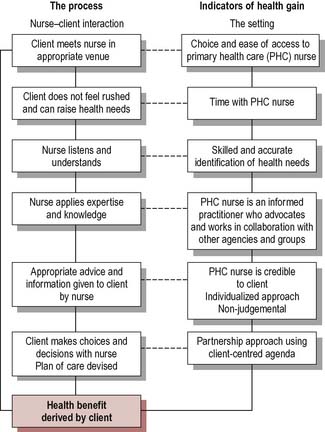
What factors might make it difficult for primary care nurses to act in ways which empower their clients?
Much of the health promotion practised in PHC settings is carried out by nurses. Much of this is opportunistic. A client has a consultation or is referred to a member of the PHC team and is identified as ‘at risk’. The practitioner takes the opportunity to offer advice, information or a further referral on a health-related issue. In some cases, the practitioner may start a series of brief interventions using motivational interviewing to identify the client’s readiness to change (see Chapter 9).
How many advantages and disadvantages of opportunistic health promotion can you identify?
You may have included some of the following:
The emphasis of recent policy has been on developing more planned and proactive health promotion activities. The need for a risk assessment becomes a key skill enabling PHC practitioners to target health promotion better. For example, only a minority of those at risk of a sexually transmitted infection (STI) attend genitourinary medicine (GUM) clinics, whereas the great majority of adults will access primary care in any one year. Matthews & Fletcher (2001) suggest therefore that GPs are likely to encounter patients from across the risk spectrum for STIs and should develop planned ways of raising the issue of sexual health risks with all patients.
Primary health care: service provision
PHC is the first level of health care which is directly accessible to individuals and communities. This means that effective PHC must be locally based, in proximity to the places where people live and work, easy to access and free at the point of delivery. As the first level of health care services, PHC services need to be well integrated with the secondary and tertiary health care sectors, in order to provide prompt assessment, response, referral and continuity of care for people throughout all levels of the health care system. There is an increasing burden of chronic and complex health conditions, including the frail aged, that will demand care in the community.
The following examples of PHC services describe the Peckham experiment of the 1930s and the recent proposals to reorganize London’s health care around polyclinics.
Do you see any similarities in the following description of two forms of PHC?
The Peckham experiment
The Pioneer Health Centre was started in the 1930s by two doctors concerned about the health of poor people living in south London. The Health Centre tried to address health in a holistic way and incorporated a fitness club, theatre, gym, swimming pool, billiards table, children’s nursery, a cafeteria serving healthy, cheap food, a library and medical consulting rooms. For one shilling (5p) a week per family, all of the Centre’s facilities could be used. In 1938, 600 families belonged. It closed during the Second World War, reopening in 1946 when it added a nursery school, youth club, marriage advisory service, Citizen’s Advice Bureau and child guidance. It closed in 1950 because it did not fit into the structure of the emerging NHS. The Centre has been revived as Pulse Health and Leisure – a partnership between Southwark Council and Lambeth, Lewisham and Southwark health authorities funded by £3.2 million of lottery money. Its aim is ‘to provide a unique leisure, health and fitness resource that encourages local people to invest in their own health and well-being’. The new partnership thus puts the responsibility for health squarely with the individual.
Polyclinics
Polyclinics will offer not just GP services, but also ‘antenatal and postnatal care, healthy living information and services, community mental health services, community care, social care and specialist advice all in one place. They will provide the infrastructure (such as diagnostics and consulting rooms for outpatients) to allow a shift of services out of hospital settings. They will be where the majority of urgent care centres will be located. And they will provide the integrated, one-stop-shop care that we want for people with long-term conditions’ (Darzi 2007, p. 11, para. 22). The staff in each centre will include GPs, consultant specialists, nurses, dentists, opticians, therapists, emergency care practitioners, mental health workers, midwives, health visitors and social workers (Darzi 2007, p. 92, main table). The shift of much health care out of hospital settings means that in the future ‘the bulk of healthcare activity will take place in polyclinics’ (Darzi 2007, p. 107, para. 71).
Behind both forms of provision is the notion that health care needs to be closer to home and include the wide range of services that promote health. Whilst the Peckham experiment had a holistic view of individual and community health needs, the polyclinic is firmly rooted in a medical model of care. Whereas the Peckham centre was rooted within its community, inevitably a polyclinic provides centralized services further away and more difficult to access from the disadvantaged communities who use and need PHC the most.
One common argument is that adequate provision of PHC services will mean that more specialized hospital-based services are unnecessary. For example, proper management and monitoring of chronic conditions such as diabetes and asthma should help prevent the development of crises which require hospitalization. As stays in hospital become shorter, the role of the primary health team becomes more important.
Traditional models of PHC that assumed the family doctor would build up a detailed knowledge of patients over time and visit in their own homes are changing, however, and may not be relevant for transient and culturally diverse populations. Consultations in general practice in the UK tend to be short (8–9 minutes) compared to other countries and unable to address adequately the wide range of psychosocial problems experienced by disadvantaged population groups. GP’s awareness of possible referral options in the locality is also limited (Popay et al 2007), although innovative ‘social prescribing’ projects exist such as the one in Stockport, in which a GP may refer to arts, gardening schemes, learning or a self-help library.
Participation, collaboration, empowerment and equity are core health promotion principles.
Participation
It is now accepted that the public have the right to be consulted and to have a say in the policy-making process (the drivers towards patient and public involvement are discussed in our companion volume in Chapter 6 (Naidoo & Wills 2005)). However, the means of public consultation range from formal to informal; one-off events to ongoing contact; and reactive to proactive. Any of the following activities undertaken to increase public participation and involvement could be said to be public health work:
Equity
As we saw in Chapter 2, there is a strong argument for advocating greater social and economic equity as a means of promoting health. This refers to equity of both material resources and power (the ability to achieve desired goals). Equity, or being fair and just, is not the same as equality, which is the state of being equal. Whilst equality may be impossible to achieve, providing equal services for people with equal needs and working to reduce known inequalities in health are realistic goals.
Most practitioners see the promotion of equity as a political task beyond their role or competence. However, even small steps contribute to greater equity. For example, ensuring clients know their benefit entitlement and claim it, helping clients to fill out the necessary forms or supporting the case for a welfare benefits advisory service to receive health authority funding are all aspects of working for equity to improve material circumstances. Identifying inequities in local services, such as people not registered with general practices, and supporting such groups to gain access to services, is also working for equity. Targeting areas of deprivation for more intensive interventions is another example which is frequently found. The arguments and evidence in favour of targeting small areas or population groups are discussed in more detail in our companion volume (Naidoo & Wills 2005).
Collaboration
Collaboration or partnership working is the third health promotion principle. Collaboration means working together with others on shared projects. Collaboration is necessary because of the many different factors affecting public health, which means that any one agency or organization can have only a limited impact on health. By working together, more fundamental changes can be put into place, with a greater potential to promote health. Government has stressed the need for local authorities to consult widely with their local communities and to work alongside the NHS to promote health. Coterminous boundaries, joint appointments for Directors of Public Health, statutory requirements for joint strategic plans such as local area agreements, and a framework for commissioning services for health and well-being are ways in which this collaboration has moved forward. (Information about current government strategy for health services and local authorities can be found on the websites of the Department of Health at www.dh.gov.uk; the local government authorities at www.idea.gov.uk; or the NHS confederation at www.nhsconfed.org.)
Our companion volume Public Health and Health Promotion: Developing Practice (Naidoo & Wills 2005) discusses some of the challenges associated with partnership working across organizational boundaries, such as differences in priorities, organizational ethos, funding arrangements, competition for contracts and geographical boundaries. Enabling factors identified include committed individuals, joint funding and pooling of resources, shared education and training opportunities and existing projects which span different agencies.
Think of an intervention in your health promotion practice concerning the health promotion of a service user.
Reflect on why you did what you did.
Could you have done something different?
Would other health promoters have done the same as you?
If you adopted a public health approach to your work, what aspects of this intervention would change?
NHS Health Scotland has developed a framework to support the development of a health-promoting service, as shown in Figure 8.2.
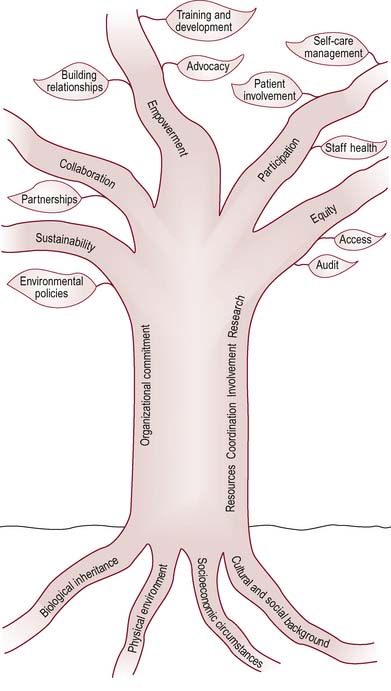
The roots of the tree suggest the necessity of understanding the underlying conditions that determine health and ill health:
This understanding of who, when and where is affected enables possible interventions to be identified. The trunk of the tree illustrates the importance of organizational commitment to improving health. The branches describe key areas for health promotion activity and those elements of the setting that contribute to health, e.g. organizational policy and the physical environment.
To reduce the financial burden on health services there are a number of possible initiatives which aim to prevent ill-health. What are the advantages and disadvantages of each?
All the above suggestions have been adopted. Most reflect the view that there needs to be incentivization through financing mechanisms or performance management in order for health care organizations to adopt health promotion strategies. As the requirement standard for public health simply requires plans to be in place for disease prevention and health promotion with regard to obesity, smoking, substance misuse and STIs (Department of Health 2004), actions may be interpreted very differently from routine health education to rehabilitation therapy.
Obesity, for example, is a public health priority. Although primary care may offer potential for health promotion, there are numerous barriers to effective health promotion in primary care. Maryon-Davis (2005, p. 97) describes obesity as a frequently intransigent problem for primary care. He cites:
Maryon-Davis (2005) suggests the following as ways of overcoming these difficulties in the case of obesity. However these strategies may also be applied to other problems:
Who promotes health?
‘Health is a state of complete physical, social and mental well-being, not merely the absence of disease or infirmity’ (World Health Organization 1946). Using this well-known definition of health, make a list of who is involved in promoting and protecting the nation’s health.
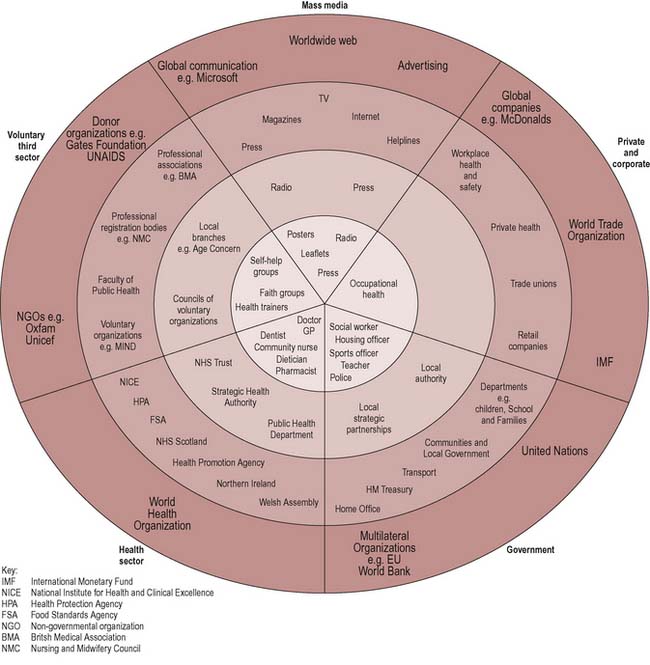
Identifying who promotes health depends on how it is defined. If you adopt a fairly narrow medical model of health, you may have included a range of health sector professionals such as GPs and health visitors. If, however, your definition is wider and health is seen as socially and economically determined, then a much wider range of partners can be seen to promote health. Figure 8.3 illustrates the sectors and range of agencies that can be involved in promoting health. These span international and global interests, national, regional and local levels. Many of these agencies would not regard health as their core business but their activities can make a significant contribution to the promotion of good health in society. Reorienting the work of such agencies and organizations would mean making explicit their health goals and impact.
International
Numerous international organizations such as the World Health Organization have health promotion as a core function. Other organizations, such as the World Trade Organization, responsible for free trade and investment agreements between nations, can have an impact on resource consumption and environmental stress, and on wage rates and thereby the efforts of countries to reduce inequities. The World Bank provides financial assistance to low-income countries and is a major funder of health projects, including mass immunization campaigns and antimalaria projects.
 BOX 8.14
BOX 8.14War and public health
Increasing global interdependence has meant that wars are more likely to affect countries geographically far removed from the conflict, through economic repercussions, emigration patterns and even by direct forms of action such as terrorism. Almost all wars since the Second World War have been fought in developing countries, which has allowed the west to consider war as an exceptional event rather than a mainstream concern for public health. This is despite the fact that in 1990 war was the 16th cause of global burden of disease (Murray & Lopez 1997) and predictions were that by 2020 it would take eighth place, putting it ahead of human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS). Wars have also dramatically shaped the spending of the countries of the developing world, which buys approximately 85% of world arms and weaponry. Many of these countries spend more on arms and weapons than on education or health (Levy & Sidel 2002). The five major developed powers (China, France, Russia, the USA and the UK) produce 90% of the world’s arms and the arms trade has a role in the perpetuation of conflict (Bunton & Wills 2005).
National
A range of government departments have an influence on health and the government is committed to ‘joined-up’ policy. The appointment of a Minister for Public Health in England in 1997 was intended to ensure coordination of health policy across government. Health impact assessments are intended to ensure that the health consequences of a range of policies will be considered during their development stage.
A range of agencies within government have a remit for aspects of health, e.g.:
In England, following the disbandment of the Health Development Agency, there is no lead agency for health promotion. Health Scotland, the Welsh Assembly and the Health Promotion Agency for Northern Ireland take on this role in the other UK countries. In other countries there are national centres which may coordinate research and knowledge, contribute to policy advocacy and provide a voice for public health and health promotion practitioners, e.g. Public Health Agency for Canada.
Increasingly the corporate sector is recognizing the potential of health as a commodity. In recent years, there has been a huge expansion in gym membership, exercise equipment, organic foods and farmers’ markets. Supermarkets promote foodstuffs on the basis of their health-giving potential. The impact of the corporate sector on health through labour market policies and environmental degradation is increasingly recognized (see Chapter 11 on how public policy is being oriented to health).
Local
Authorities and trusts are the different types of organizations that run the NHS at a local level. The whole of England is currently split into 10 strategic health authorities (SHAs). These organizations were set up in 2002 to develop plans for improving health services in their local area and to make sure their local NHS organizations were performing well. The NHS website (http://www.nhs.uk/aboutnhs/HowtheNHSworks/) provides details on the current structure of the NHS which includes acute trusts that provide hospital-based care; ambulance trusts providing emergency care; mental health trusts and primary care trusts (PCTs).
PCTs are now at the centre of the NHS and control 80% of the NHS budget. They are local organizations with a remit to identify local needs and any problems of equity and commission for the provision of corresponding services. The role of a PCT is to:
All NHS bodies have a legal duty to involve and consult the public. Patient and public involvement (PPI) forums were set up in every NHS trust and PCT area to gather views about local health services and provide dialogue with the NHS. Local involvement networks (LINks) will be established for every local authority (LA) area that has social services provision. They will support local people in taking part in planning, developing and making decisions about local services, including monitoring and making their views known about how services are delivered. A health overview and scrutiny committee may review and scrutinize any matter relating to the planning, provision and operation of health services within a local area.
Key functions that have an impact on health, such as housing, transport and sport and leisure, are all LA responsibilities. Prior to the 1970s the public health function was located in LAs but was transferred to the NHS in 1974. Increasingly, LAs and PCTs are now required to work together in planning and providing services. In some areas the Director of Public Health may be jointly appointed by the PCT and the LA. The Local Government and Public Involvement in Health Bill (2006) requires the production of a joint ‘strategic assessment’ of the health and social care needs of the local population. LAs must produce a community plan to improve well-being in the area informed by a local strategic partnership (LSP) which brings together organizations from public, private, community and the voluntary sector. A local area agreement (LAA) is a 3-year agreement – informed by the community strategy – setting out the priorities for a local area. LAAs cover four basic themes:
Public health and health promotion workforce
PHC services require balance between health promotion, preventive care and illness treatment. This is best achieved through the use of a team drawn from a variety of disciplines, including not only medical and nursing health professionals but also community workers, public health information workers and educators.
The Report of the Chief Medical Officer’s Project to Strengthen the Public Health Function (Department of Health 2001) provided a framework for assessing the contribution of the broader public health workforce to the public health function. In particular the document referred to three main categories of employees:
Reorienting the workforce means identifying health promotion opportunities and also encouraging a way of working which is empowering and enables people to take control over health issues.
Wider contributors
Wider contributors are professionals who have an impact on public health as part of their work, but who may not recognize this, e.g. teachers and social services employees. This part of the workforce is important because they can reach people who are not in contact with the health service and refer them on to sources of advice and support. In order to maximize their contribution, the public health aspects of their work need to be recognized and foregrounded. Teachers provide an example of this failure to recognize the importance of public health and health promotion – although schools are seen as key settings for health promotion in many countries with national standards and with key roles to strengthen the social and emotional well-being of both pupils and staff, health promotion is not part of initial teacher education in many countries (Chapter 13).
There is also a huge informal workforce that contributes to health. Voluntary organizations or non-governmental organizations (NGOs) act as service providers, self-help groups, pressure groups and as sources of education and information. They are involved in statutory structures such as local strategic partnerships and in planning and consultation exercises, such as the community plans. Voluntary organizations are important in providing specialized information, and being close to the community and isolated and vulnerable groups. They can reflect people’s experience of a service and give an indication of other needs, acting as a catalyst for change. The precarious funding of many voluntary organizations means they have to expend a great deal of time and effort securing grants and funding, which can make long-term planning difficult and lead to low morale.
Practitioners
Practitioners are a smaller group of professionals who spend most, or all, of their time in public health practice. Changing contracts and more specific definitions of roles and competencies mean that job remits in primary and social care are in a state of constant flux. Any account of working practice is in danger of being both context-specific and out of date in the near future. Increasingly roles are becoming generic such as those within ‘the children’s workforce’ where the skills, competence and knowledge required are similar regardless of professional background or role and apply to a very wide range of workers, including personal advisers, health visitors, midwives, youth workers, family workers, substance misuse workers, nursery nurses, educational welfare officers, community children’s nurses, school nurses and support staff such as learning mentors working in schools.
A brief description of some key roles follows. It illustrates the importance of health promotion in many job remits but also the challenges faced and why, for many individual practitioners, health promotion often slips to the bottom of a busy workload.
Specialist community public health nurses
Health promotion is a priority in the role of specialist community public health nurses such as health visitors and school nurses:
Specialist community public health nursing aims to reduce health inequalities by working with individuals, families, and communities promoting health, preventing ill health and in the protection of health. The emphasis is on partnership working that cuts across disciplinary, professional and organisational boundaries that impact on organised social and political policy to influence the determinants of health and promote the health of whole populations (www.nmc-uk.org).
Increasingly, community nurses are expected to adopt a population focus, adopting community development methods (see Chapter 10), identifying local needs and supporting community and voluntary groups. Community nurses are part of the PHC team and should work closely with other community nurses, GPs and social workers. However health promotion may not always be coordinated or prioritized because health and social care workers tend to concentrate on their own case load.
Because community nurses visit people in their own homes, they are able to build a strong relationship with their clients over a period of time. This enables them to carry out much one-to-one education, counselling and opportunistic health education. District nurses, for example, visit people with chronic sickness or disability at home. Much of their work is with older people (1:4 people over 75 are on a district nurse caseload) and they carry out opportunistic health education as well as liaising between people living in the community and other relevant health and welfare workers. The individualized basis of patient care offers opportunities for health promotion but is also a constraint both in limiting time and also separating district nursing from a population perspective. One study reports a district nurse commenting: ‘Public health … it’s like anything isn’t it … we just don’t realise we are doing it … I think maybe we need to be more aware of just what skills we’ve got’ (Arnold et al 2004).
Mental health nurses
Promoting mental health requires a collaborative approach from a diverse and wide-ranging group of stakeholders. Mental health promotion is often associated with psychiatry and the health and social care services involved in delivering care and treatment to people experiencing mental ill health. Whilst treating mental illness is an important component, mental health promotion is concerned with the mental health and well-being of the whole population throughout the life course. Mental health promotion is delivered in a variety of settings, including schools, the workplace, the community at large and within specific communities such as care homes or prisons (see the Wales Mental Health Promotion Network at www.wales.nhs.uk).
School nurses
School nurses are part of the community nursing service but their role varies enormously. Originally, it was to focus on the detection and treatment of poor hygiene, infestations and malnutrition, but it has since evolved to become routine health surveillance and screening. In common with health-visiting practice, the current role for school nurses is to move away from routine surveillance towards identifying needs and targeting support, e.g. support for children with chronic diseases or the provision of education and counselling on specialized topics such as sexual health. Some areas adopt a life course approach, with the school nurse acting as a navigator for children throughout their school journey.
Midwives
Hospital midwives are involved in antenatal education and the delivery of babies. Community midwives visit all new mothers in their area, and provide support and education as well as monitoring the health of mothers and babies.
Midwives are in an ideal position to extend support to expectant and new families and to provide a service which helps parents to access information and use it effectively to nurture the health of their family. However, they also have an important role in bringing public attention to those issues which are beyond the scope of individuals to change, such as social and environmental obstacles (Crafter 1997, p. 3).
General practitioners
General practice has traditionally been a private and personal consultation between doctor and patient. Health promotion consisted of opportunistic advice or information, often limited by time or a concern not to be ‘intrusive’. The contracting of GP services provides additional payments to GPs to carry out preventive work such as immunizations, health checks to identify risk and the giving of advice. Opportunities for planned interventions have increased and there are numerous examples of exercise referral schemes and lifestyle management programmes.
Practice nurses
Practice nurses are directly employed by GPs. Practice nursing is a relatively new profession, although there are now over 25 000 practice nurses in the UK. Their health promotion role has been largely confined to immunization, taking bloods, cytology, lifestyle advice, travel health and health checks, but increasingly they are staffing minor illness centres.
Dentists
There is an increasing emphasis on prevention in dentistry, particularly with children. Dentists receive a capitation fee per child and so have an interest in keeping that child’s teeth healthy. Many practices employ a hygienist who gives advice on dental health. Health authorities also have a community dental service which may offer dental health promotion to schools and residential homes.
Pharmacists
The potential of community pharmacies to promote health has been recognized in a national strategy (Department of Health 2005b). Pharmacy staff advise the public on the safe use of medicines, minor ailments and healthy lifestyles. They may also provide specific public health interventions as part of a broader NHS service, for example, weight loss clinics, specialist smoking cessation advice or drug misuse services. In order to maximize their potential, all pharmacies should have areas set aside where members of the public can consult in private with the pharmacist.
The role of community pharmacists
Examples of health promotion provided in community pharmacies includes education and advice on:
Environmental health
The role of environmental health is particularly wide-ranging, encompassing statutory powers relating to food hygiene and pollution (of noise and air), specialist work on safety in the workplace and places of entertainment, and work on sustainability and recycling. Because environmental health officers have wide-ranging statutory powers, their work in health promotion is mainly advice on legislation and enabling people to fulfil those regulations. Their work may thus involve offering training courses or one-to-one advice in establishments.
Allied health workers
Many other professions allied to medicine, such as speech and language therapists, chiropodists, physiotherapists, radiographers and dietitians, have a part to play in health promotion, especially patient education.
Care workers
Population projections indicate a more rapid ageing of the population. People aged 85 and over will comprise 3.8% of the UK population by 2031 and the majority of these will need residential care. Care workers have a key health promotion role to improve fitness and nutrition and thereby minimize illness and dependence. Care workers also have a role in positive mental health promotion and empowering older people to have a degree of control over their lives. Preventing ill health in the frail aged is also important, e.g. the prevention of falls and pressure sores. Residential care workers liaise with GPs, social workers, physiotherapists, chiropodists and catering staff.
Specialists
Specialist advisers in public health are usually public health consultants and specialists working at a strategic or senior management level. They play a role in developing public health programmes and often have specific scientific expertise and accreditation.
Health promotion departments are part of the health authority and are usually accountable to the Director of Public Health. They vary widely in size, from a handful to 50 staff, and consist of health promotion specialists and several support and clerical staff. They have the lead role in initiating, coordinating and supporting health education and health promotion activity within their areas. Health promotion units may have commissioning or providing functions, or both. Commissioning activities include:
Conclusion
Reorienting health services is a challenging task in which little progress has been made. There are many reasons for the intransigence of the health services to change. PHC is a social system with its own structure and culture which determine the way in which it tackles health and ill health. Its partnerships tend to be client- rather than population-focused, and though based in communities, there may be little work with communities. It is driven by a medical model of health rather than a social model, and evaluation is still often seen in terms of reduced morbidity and mortality, rather than in terms of health gain processes and outcomes. The priority in primary care is treatment, which means that often patient compliance is valued above patient autonomy and participation. Although progress has been made in prioritizing health promotion, it is still ‘bolted on’ to core tasks instead of being integral to everyone’s work and service delivery. Key health promotion activities, such as addressing health inequalities, are replaced by the need to respond to client demands, which may paradoxically have the effect of reinforcing inequalities by providing more services for more educated and articulate patients. Perhaps the biggest barrier is inertia, or the duplication of ways of working that have served in the past.
On the plus side, there is a large pool of potential health promoters, including many practitioners in primary, secondary and tertiary care services. The effective delivery of health promotion would, in the long run, ease the workload of most practitioners, as well as enabling people to enjoy better health and increased longevity. Health promotion underpins many of the activities already being undertaken by practitioners, e.g. collaboration and partnership working. The economic argument for reorienting health services is robust, and provides a compelling case for action. Pulling all these positive factors together is a long-term and daunting task, but many small steps have already been taken. The ongoing challenge is to keep the reorienting health services agenda foregrounded and to identify ongoing strategies to progress this goal.