Chapter 36 Principles of infection control
Cross infection
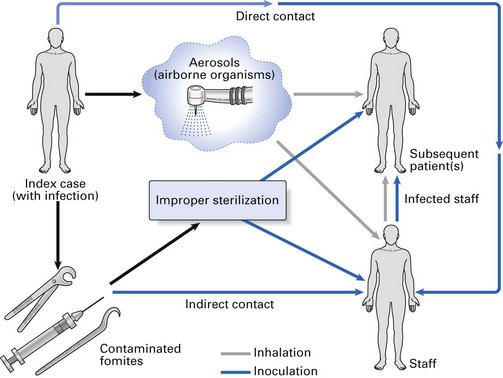
Cross infection may be defined as the transmission of infectious agents between patients and staff within a clinical environment. Transmission may result from person-to-person contact or via contaminated objects (fomites) (Fig. 36.1). Organisms capable of causing cross infection in humans are derived from:
Principles of infection transmission
Transmission of infection from one person to another requires:
Source of infection
The sources of infection in clinical dentistry are mainly human; they include:

Convalescent carriers are those who suffer an illness and apparently recover, although blood and secretions of the individual act as persistent reservoirs of infective organisms. For example, following diphtheria or streptococcal sore throat, the organisms may persist in the throat for some time and infect others or, in the case of hepatitis B patients, may recover fully, although they may carry the infectious agent in the blood for a considerable period. The latter are called chronic carriers.
Asymptomatic carriers give no history of infection as they may have unknowingly had a non-apparent or subclinical infection (recognized merely because of the presence of specific antibodies in the person’s blood). Nevertheless, these individuals may carry infective microbes in the saliva, blood and other body secretions.
Hepatitis B is a classic example of a disease that may manifest with or without symptoms, and thus, the clinician may be faced with either a convalescent or an asymptomatic carrier of hepatitis B virus. Note: a convalescent carrier can be identified from the history of infection, as opposed to an asymptomatic carrier who cannot be diagnosed in this way.
Standard infection control
From the foregoing, it is clear that it is impossible to ascertain whether the patient who attends for dental treatment is a carrier of infectious agents. Therefore, all patients should be treated as if they were reservoirs of pathogens. The infection control procedures involved in such treatment are termed standard precautions (previously termed universal precautions), and all clinical procedures performed on any patient should be conducted using standard infection control. The corollary of this is that no additional infection control precautions should be necessary when a patient who is a carrier of infection such as HIV disease attends the clinic. The importance of this concept cannot be overemphasized and should be noted by all who practise dentistry.
Evolution of universal precautions, standard precautions and additional precautions (or transmission-based precautions)
The first set of recommendations on infection control in dentistry, issued in the late 1980s, focused primarily on the transmission of blood-borne pathogen transmission in dental care and other clinical settings and was termed universal precautions. These recommendations emphasized the need to treat blood and other bodily fluids contaminated with blood from all patients as potentially infectious.
However, the realization that moist body substances are equally important in disease transmission led to the development of standard precautions in the mid-1990s. Thus, standard precautions are similar to universal precautions as they are designed to reduce the risk of infection transmission from both recognized and unrecognized sources of infection to patients and clinicians. Standard precautions apply to contact with:
For the overwhelming majority of infectious diseases, including those possibly encountered routinely in dental settings, the application of standard precautions will arrest disease transmission.
However, in special situations where a known infection with a high transmission potential is suspected or encountered, additional precautions or transmission-based precautions have to be implemented. These include situations dealing with patients either having or suspected to be infected with virulent pathogens that are transmitted through:
These so-called transmission-based precautions include patient isolation, adequate room ventilation, respiratory protection of workers and postponement of non-emergent dental care procedures. It should however be realized that in routine dentistry, application of standard precautions would be the norm and additional precautions have to be implemented in special situations, such as in hospital settings where such patients are treated or during epidemics, such as the outbreak of severe acute respiratory syndrome (SARS).
A note on the management of potential carriers of transmissible spongiform encephalopathy or prion diseases
The regulations in the USA state that standard infection control measures have to be modified when treating such cases as prions cannot be destroyed using the routine sterilization protocol. Hence, when transmissible spongiform encephalopathy (TSE) patients are treated, special sterilization procedures are required, or alternatively all instruments need to be disposable (see Chapter 4). However, according to the British guidelines, special precautions for patients with TSE are not required but strict adherence to standard precautions is adequate.
Mode of transmission
Transmission of infection may occur by:
Some of the infectious agents of concern in dentistry and their possible routes of transmission are given in Table 36.1.
Table 36.1 Some infectious agents of concern in dentistry and their routes of transmission
| Microorganism | Major transmission route |
|---|---|
| Viruses | |
| Cytomegalovirus | Inhalation |
| Hepatitis viruses | |
| Hepatitis B | Inoculation |
| Hepatitis C | Inoculation |
| Delta hepatitis (hepatitis D) | Inoculation |
| Herpes simplex virus types 1 and 2 | Inoculation |
| Human immunodeficiency virus (HIV) | Inoculation |
| Measles and mumps viruses | Inhalation |
| Respiratory viruses | |
| Influenza virus | Inhalation |
| Rhinovirus | Inhalation |
| Adenovirus | Inhalation |
| Rubella virus | Inhalation |
| Bacteria | |
| Neisseria gonorrhoeae | Inoculation |
| Treponema pallidum (syphilis) | Inoculation |
| Mycobacterium tuberculosis | Inoculation/inhalation |
| Streptococcus pyogenes | Inhalation |
Airborne infection
Airborne infective organisms in the form of infectious aerosols may be inhaled, causing diseases such as influenza, the common cold and tuberculosis. When aerosols are created, for example, by high-speed instruments, different sizes of droplets are produced. Their fate depends on their size. Droplets greater than 100 µm in diameter are called spatter and settle very quickly on surfaces as a result of gravitational pull; they contaminate whatever is immediately in front of and below the patient. Small droplets of less than 100 µm in diameter account for the majority of droplets created (Table 36.2). They evaporate instantaneously and remain suspended or entrained in the air for many hours as droplet nuclei, which consist of dried salivary or serum secretions and any organisms they may contain. Eventually, they fall to the ground. In practical terms, this underscores the importance of adequate ventilation of the clinical environment, particularly during the use of aerosol-creating instruments and the routine disinfection of surgery surfaces.
Table 36.2 Characteristics of aerosols produced by high-speed instrumentation
| Particles | Droplet nuclei | |
|---|---|---|
| Diameter | >100 µm | <100 µm |
| Time spent airborne | Minutes | Hours |
| Penetration into respiratory tract | Unlikely | Possible |
| Possible mode of transmission | Direct contact or from dust | Inhalation |
Infection via sharps and needlestick injuries
The major route of cross infection in the dental surgery is through the skin or mucosa due to accidents involving sharps or needlestick injuries (Fig. 36.1). There is evidence that hepatitis B transmission from patient to dentist and vice versa has occurred by this means.
Mode of entry
Transmission of the pathogen to the new host is sometimes by direct contact but is more often an indirect process involving various vehicles of infection, dealt with above. Once the organism has approached the new host, it may gain ingress via a number of portals:
Inhalation, inoculation and, rarely, direct contact are the modes by which the pathogens gain access to the host tissues in the dental clinic environment.
Infection control procedures
From the foregoing, it is evident that the number of infectious diseases that dental personnel may be exposed to during the working day could be fairly substantial. Several measures are available to dental personnel (dentists, dental hygienists, dental surgery assistants, school dental nurses, dental laboratory technicians and radiology technicians) to break this chain of cross infection. These may be categorized as:
These subjects are dealt with in detail in the next chapter.
Key facts
Centers for Disease Control and Prevention. Guidelines for infection control in dental health-care settings. Morbidity and Mortality Weekly Report. 2003;52:1-66.
Cottone J.A., Terezhalmy G.T., Molinari J.A. Practical infection control in dentistry. Philadelphia: Lea & Febiger; 1991.
Kohn W.G., Harte J.A., Malvitz D.M., et al. Guidelines for infection control in dental health care settings. Journal of the American Dental Association. 2004;135:33-47.
Mims C., Playfair J., Roitt I., Wakelin D., Williams R. Hospital infection, sterilization and disinfection, Ch. 34. Medical microbiology, 2nd ed. London: Mosby. 1998.
Samaranayake L.P. Cross infection prevention in dentistry. Part I: General concepts and surgery attire. Dental Update. 1989;16:58-63.
Samaranayake L.P., Scheutz F., Cottone J. Infection control for the dental team. Copenhagen: Munksgaard; 1991.
Review questions (answers on p. 355)
Please indicate which answers are true, and which are false.