CHAPTER 9 Head and dental trauma
A variety of injuries affecting the oral cavity may be encountered in equine practice. Many of these injuries arise from inquisitive or playful interaction of the horse with objects in its environment. Other injuries are the direct result of human action. Oral injuries may involve, in various combinations, the soft tissues, osseous, and/or dental structures of the mouth.
The oral environment and healing of oral injuries
Although wounds within the oral cavity are exposed to food material and a large mixed resident population of obligate and facultative anaerobic and aerobic bacteria, healing generally proceeds far more rapidly than with cutaneous wounds. Even extensive intra-oral injuries to the cheeks or tongue rapidly resolve providing the inciting cause (fractured or displaced tooth, foreign body, or sequestrum) is no longer present. One of the factors responsible for such efficient healing and the limited subsequent formation of scar tissue, is that oral mucosal wounds have a subdued inflammatory response compared to external skin wounds.1,2 In addition, the constant bathing of oral wounds with saliva (rich in protease inhibitors, cytokines and growth factors) also speeds up wound healing. Furthermore, an excellent oral vascular supply ensures that tissue devitalization is minimal.
Given the intrinsic good healing characteristics of the oral mucosa, there is generally little merit in attempting to assist healing by using topical medications, and in any event, there is little objective support for the efficacy of most such treatments. Oral lavage with a saline solution or water may temporarily assist in reducing contamination with food material. Similarly, unless wounds are full-thickness or closure is necessary to prevent food contamination of deeper defects, suturing of intra-oral injuries is not generally indicated.
Management of horses with facial trauma
A horse with major facial trauma should be assessed immediately for the presence of life-threatening respiratory obstruction, epistaxis, and any indication of other major dysfunction, such as neurological or ocular disturbance. Maintenance of a patent airway must be a priority and if required, insertion of an emergency tracheotomy tube should be carried out without delay. Most nasal hemorrhage (from nasal cavity and/or sinuses) associated with facial injury ceases without need for particular action. Secondary infection of the paranasal sinuses is common following facial fracture and appropriate antibiotics should be administered. Sinus lavage may also be of benefit with an open fracture of the sinus walls, or where there has been significant intrasinus hemorrhage. In horses with major facial wounds, the extent of osseous or dental injury and the presence of radiodense foreign bodies should be assessed using multiple radiographic projections or, if available, computed tomographic (CT) imaging, before any attempt is made to repair the overlying soft tissues.
Management of specific intra-oral injuries
Lips and cheeks
One of the most commonly encountered injuries to the lips is traumatic injury to the commisures of the lips arising from the use of a bit. Damage to the soft tissues may occur directly from inappropriate pressure on the bit or as a result of soft tissue being trapped between the bit and the rostral cheek teeth. The appearance of these injuries is determined by severity and chronicity, ranging from a fresh wound to ulceration and eventually to scar tissue formation. To facilitate healing it is sensible to remove the inciting cause, which can mean a period of time without using a bit. This is often impractical and minimizing ongoing soft tissue trauma must then be the primary goal. The use of a wide rounded bit such as a rubber snaffle and removal of sharp cheek tooth edges, can assist in the prevention of lip and cheek damage. Rounding the profile of the rostral aspect of the 06s (first maxillary and mandibular cheek teeth), known as ‘bit-seating’, may also be employed. Any such profiling should be performed with awareness of the possibility of exposing the rostral (6th) pulp and thus causing pulpitis if reductions are excessive. If large, displaced or sharp wolf teeth are present and felt to be contributing to the problem, their extraction may also be indicated.
Abrasions or lacerations of the cheeks within the oral cavity can arise from direct trauma to the soft tissues by sharp or prominent buccal enamel points/edges or displaced or fractured teeth. Injuries may be detected, when acute, as mucosal lacerations or fresh abrasions (Fig. 9.1) or when chronic (characterized by ulceration with thickened mucosal edges or scar tissue; Fig. 9.2). The removal of the inciting cause usually resolves the problem.


Trauma to the external lip or muzzle is usually the result of the horse biting or playing with a fixed object in its environment. These injuries are typically full thickness, and although wound breakdown often ensues, an attempt at sutured repair is usually indicated to maximize the chance of a good cosmetic and functional outcome. Following lavage of the wound and debridement of any obviously devitalized tissue, a multi-layer repair of the defect is usually undertaken (Fig. 9.3) beginning with apposition of the oral mucosa with simple interrupted or continuous absorbable sutures. External closure of the skin wound using non-absorbable suture material or staples then follows. However, with more extensive defects, separate closure of the muscular layer should also be performed with absorbable sutures to afford the best chance of healing by primary intention. It may be beneficial to minimize excessive movement at the suture line by separating the adjacent musculature at the edges of the wound, thus reducing the chance of dehiscence. Should the sutured wound subsequently partly or fully dehisce, it may be left to heal by second intention. If cosmetic or functional outcome is poor, secondary repair of the wound can be undertaken at a later date.
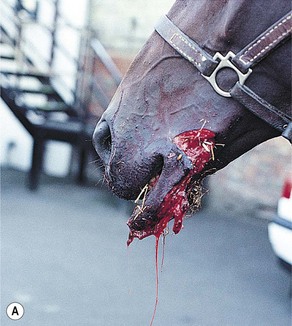
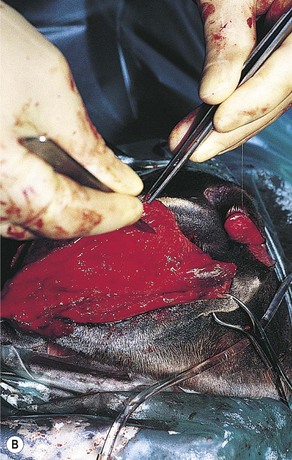
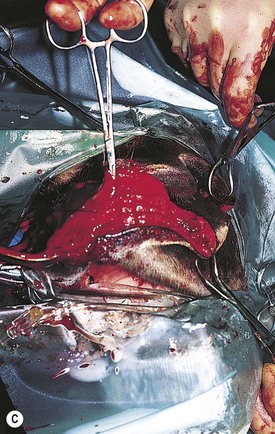

Fig. 9.3 (A) An extensive laceration of the lower lip which also has a full-thickness defect through the left cheek into the mouth. (B) Separating the skin from the underlying musculature. (C) Repair of facial musculature using a continuous suture of 4 metric polydioxanone. (D) Although the lesion was repaired in layers, partial wound dehiscence resulted in an orofacial fistula. This was successfully repaired by a second operation.
Tongue
There are two main types of direct injury to the tongue that are encountered in practice. Lacerations of the lateral margins of the tongue (Fig. 9.4) may be caused by the horse inadvertently biting itself, trauma from displaced or fractured teeth or from a foreign body. Injuries to the tongue arising from inappropriate restraint may also be encountered. In the latter case, aggressive use of a leading bit (typically a chifney) can result in laceration of the dorsal or lateral margins of the rostral portion of the tongue. These injuries can range from small superficial cuts to near-total transaction of the tongue (Fig. 9.6). Occasionally, a horse is examined that has previously sustained a severe laceration of the tongue that has healed, leaving a large defect in its dorsum or lateral border (Fig. 9.5). Grasping the tongue as a means of restraint can also result in injury should the handler fail to release the tongue if the horse pulls back; excessive traction can cause laceration of the lingual frenulum. It is not usually necessary to repair these injuries.
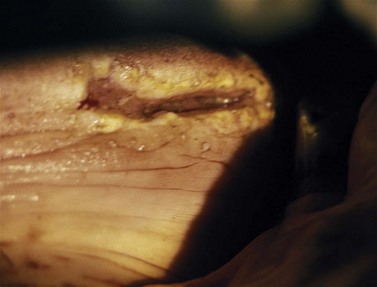

Fig. 9.6 This severely lacerated tongue has been severed almost completely. The injury was repaired using simple interrupted sutures of 4 metric polydioxanone alternated with vertical mattress sutures of the same material. The wound healed by primary intention, and the horse regained normal use of its tongue.

Horses that have sustained a laceration of the tongue due to dental or foreign body trauma at the back of the mouth typically present with acute signs of oral discomfort and excessive salivation. A thorough examination of the oral cavity, using a full-mouth speculum, is necessary to assess these injuries. Due to their hidden location, some caudal lacerations of the tongue may be more readily detectable by digital examination, rather than by direct visualization. However, oral endoscopy, if available, is the preferred technique to image the caudal tongue and a dental mirror may also reveal some such lesions. Care should be taken to palpate the dorsal and both lateral margins of the base of the tongue, particularly at the level of the occlusal surface of the mandibular cheek teeth. Once the inciting cause is removed, these injuries tend to heal without further intervention, although anti-inflammatory and/or antibiotic therapy may be beneficial in some cases. On occasion, focal abscess formation or more generalized infection of the tongue may occur following foreign body penetration (often with food material, wire fragments, or wood splinters). Such cases may present with signs of oral discomfort and excessive salivation; however, early diagnosis is often more difficult than for the lacerations discussed above. In these cases, the tongue is often grossly normal to visualisation without use of endoscopy, but palpation of the affected site may reveal an area of firmness within the softer body of the tongue, which elicits a pain response on digital pressure and which may be associated with focal malodour. Depending on the severity of clinical signs, aggressive treatment with broad-spectrum antibiotics or surgical drainage of a lingual abscess may be necessary.
In the case of a severe, bit-induced laceration of the tongue (Fig. 9.6), assessment of the wound (and tongue viability) is often best performed under general anesthesia. A gauze bandage tied around the tongue caudal to the wound can be used as an effective tourniquet. Gentle traction to the bandage also allows good exposure of the more caudal parts of the tongue. Glossectomy may be necessary if the tongue tip is considered unviable (Fig. 9.7), and removal of tissue up to the level of rostral attachment of the frenulum is unlikely to affect function. Intravenous administration of sodium fluorescein has been recommended as an aid to assess tongue viability. Oversewing the body of the tongue with simple interrupted or a continuous suture of polyglactin 910 or polydioxanone should be attempted after removal of the necrotic tip. Severe lacerations are repaired using simple interrupted and vertical mattress sutures applied alternately (Fig. 9.8). The latter should incorporate a significant bulk of lingual musculature to take up some of the tension and to ensure more satisfactory healing. All dead space should be obliterated if possible.


Multiple-layer closure of thicker areas of the tongue may be required. It should be remembered that the tongue is very mobile, and the risk of wound dehiscence is significant unless care is taken to align the tongue correctly and to repair the injury accurately. If the injury is not dealt with immediately, some necrosis and a high level of wound contamination may occur. In such circumstances, all devitalized tissue must be debrided carefully to minimize the risk of wound dehiscence. When placing vertical mattress tension sutures care must be taken to avoid damage to the lingual blood supply. Although this blood supply is good, vascular compromise may result in necrosis of the more rostral aspects of the tongue, particularly when the tip is involved. The dorsum of the tongue has a much stronger mucosa than its ventral aspect, and suture retention is better in this site. Tension sutures should, therefore, be placed in this area.
Oropharynx
Lesions at the base of the tongue and in the oropharynx are difficult to evaluate visually, by palption or imaging, and are also difficult to surgically repair due to their inaccessibility. Diagnosis is best achieved by oral endoscopy. Fortunately, these inaccessible wounds usually heal well without the need for surgical repair. Daily lavage of the oral cavity with a saline solution may be of value in reducing wound contamination with food material. This site is also prone to damage by ingested foreign bodies, which are usually twigs or pieces of wood. In most circumstances, affected horses show a sudden onset of oral discomfort, dysphagia, inappetance, excessive salivation, and occasionally, epistaxis. Foreign bodies within the oropharynx (Fig. 9.9) can often be detected by nasopharyngeal endoscopy as they frequently protrude through the intrapharyngeal ostium. Foreign bodies can usually be retrieved manually with the horse under heavy sedation or general anesthesia. Repair of any mucosal injury is usually unnecessary.

Ulceration of a caudal pharyngeal soft tissue pillar is a not uncommon sequel of dental ‘floating’. The soft tissues at this site are in very close proximity to the occlusal surface of the caudal mandibular cheek teeth (Fig. 9.10). Trauma may occur if excessive caudal movement of the rasp blade occurs during manual rasping of the last mandibular cheek tooth (311, 411), or if soft tissue becomes trapped between the tooth and rasp blade or motorized burr. Ulceration can vary in severity, and although clinical signs are generally self-limiting, affected horses may demonstrate oral dysphagia until healing occurs, which can be days or even weeks later. Systemic antibiotic and anti-inflammatory therapy is indicated with more severe injuries.

Mandibular interdental space (‘bar’ or ‘physiological diastema)
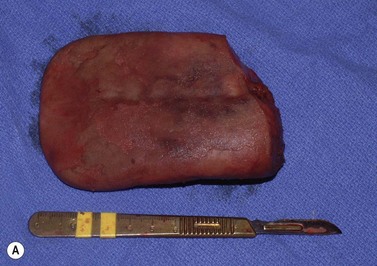
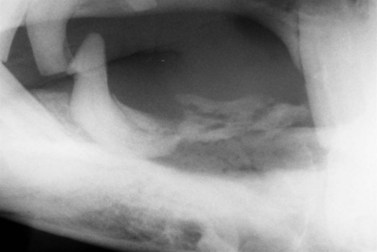
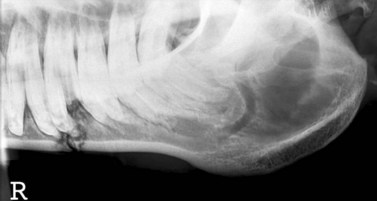
Injuries to the dorsal (intraoral) aspect of the mandibular interdental space (mandibular ‘bar’) are invariably caused by damage from a bit. Aggressive use of a bit, or indirect, blunt, bit-related trauma, such as when a loose horse treads on trailing reins, may result in damage to one or both mandibular bars. In the most severe cases, the injury may cause a mandibular fracture (see Fig. 13.47 in Chapter 13). However, more often with recent injuries there is ulceration/laceration of the overlying gingiva that is painful to pressure, and the horse resents further bitting. If the damage is superficial, these injuries will heal unaided, providing time is allowed without bit contact. In a small proportion of cases, the dorsal cortex of the bone underlying the damaged mucosa may become devitalized and subsequent sequestrum formation (Figs 9.11 & 9.12) can result in a chronically discharging and painful focus. Radiographic examination (oblique lateral projections) and/or ultrasonographic examination may be necessary to confirm the presence of a sequestrum. If a sequestrum is identified, surgical removal is necessary if healing is to be expected, and this can be performed satisfactorily with the horse sedated and using regional (subgingival) analgesia. A longitudinal incision of the gingiva overlying the affected area permits the introduction of a bone curette which is used to elevate the sequestrum. Primary closure of such surgical sites is unnecessary and ridden work using a bit may resume once the mucosa has healed completely.

Hard and soft palates
Injuries to the hard palate are rare but may accompany severe head trauma (Fig. 9.13). In some circumstances, there may be an underlying fracture of the palatine processes of the premaxillary and/or the maxillary bones. In general, these injuries can be left as open wounds, to heal by second intention. However, if the hard palate injury has caused an oronasal fistula, such lesions should always be repaired surgically. A suspected oronasal fistula may be confirmed by a combination of thorough clinical and endoscopic examinations, and by radiography after oral administration of barium sulfate. While such a fistula may heal by second intention, surgical repair should be attempted if the site is accessible. It may be possible to repair the defect by debriding the wound and curetting any area of oronasal mucosal continuity and simply suturing the palatal mucosa with interrupted, polydioxanone sutures (Fig. 9.14). If the injury cannot be repaired adequately in this manner, it may be possible to close the defect by creating a mucoperiosteal flap, or by making tension-relieving incisions in adjacent portions of the palate and then suturing the defect. Care should be taken to avoid damaging the palatine blood supply. Post-repair feeding should be carried out by nasogastric intubation for the first 4 or 5 days to reduce the risk of suture dehiscence. If the rostral portion of the skull is grossly unstable following a maxillary or premaxillary injury, the fractures may require surgical repair. However, it is surprising how frequently horses with such major injuries respond successfully to conservative management.

Fig. 9.13 This horse sustained severe trauma to the maxilla which resulted in a fracture of the premaxillary bone and laceration of the hard palate. There was direct continuity between the oral and nasal cavities.

Fig. 9.14 This is the surgical repair of the injury illustrated in Fig. 9.13. The fracture has been reduced with cerclage wire after radical debridement of the site. The palate has been sutured partially using simple interrupted and vertical mattress sutures of 4 metric polydioxanone. The horse made an uneventful recovery, and the cerclage wire was subsequently removed.
Iatrogenic injuries to the hard palate are uncommon but usually arise from dental intervention. The greater palatine artery courses close to the palatal margin of the maxillary cheek teeth. Inadvertent laceration may occur during ‘wolf’ tooth removal or intra-oral extraction of a cheek tooth, and profuse hemorrhage ensues. This hemorrhage is dramatic but rarely life-threatening and is usually effectively controlled by pressure. If the defect is large enough it may be possible to insert and suture in place some gauze bandage packing. The affected horse should be kept in a quiet environment until bleeding subsides. If the horse is sedated, it is useful to keep its head very elevated on a headstand. Lacerations of the hard palate mucosa may also arise iatrogenically from the use of dental extraction forceps during oral extraction procedures, but such injuries typically heal by second intention without intervention.
Injuries to the soft palate are uncommon but may result iatrogenically from surgical procedures involving the soft palate or adjacent structures, such as surgical correction of epiglottal entrapment. When attempting to axially divide the displaced mucosa using a curved bistoury, the soft palate may become inadvertently damaged. However, there are new safer knives available to avoid such risks. Injuries may also arise from the use of motorized dental instrumentation, particularly during procedures to reduce overgrowths of the caudal mandibular or maxillary cheek teeth. In the case of large overgrowths (such as with supernumerary maxillary cheek teeth), the soft palate may ‘billow’ around the tooth during swallowing, and damage may ensue unless particular care is taken and equipment incorporating a soft-tissue guard or clutch is used. The soft palate may also be lacerated by extraction forceps during oral extraction of a caudal maxillary (especially a caudal supernumerary) cheek tooth.
Full-thickness injuries to the soft palate inevitably result in the development of an oronasal fistula because of contamination with food and saliva. Whilst some of these defects heal by second intention, surgical repair should be attempted as soon as possible after the injury has been identified. Access for surgical repair is very limited, especially in smaller horses and ponies. A general anesthetic should be administered and an oral speculum used to permit access to the mouth. Good lighting (e.g., a head light) should be provided, and the area should be endoscopically examined to assess the extent of the injury. Long-handled retractors should be used to depress the base of the tongue and retract the cheeks in order to evaluate the injury and assist in its subsequent repair. Long-handled needle holders, forceps and scissors are also of great help when attempting repair of such an injury. Separating the oropharyngeal mucosa from its overlying musculature will facilitate soft palate closure in two layers, enhancing the likelihood of achieving first intention healing. The musculature and nasopharyngeal mucosa are closed as one, and the oropharyngeal mucosa as the other. Simple-continuous sutures using polydioxanone for each layer are preferred.
Even though such defects may be closed effectively, and initially appear to be healing well, dehiscence is common some days or weeks later. This is because of the high mobility of the palate for very prolonged periods during mastication and deglutition, and the presence of food and saliva within the oral cavity and oropharynx. It is not unusual for second and even third attempts at repair of full-thickness palatal defects to fail. However, small fistulae may heal spontaneously. As described above, feeding such cases by nasogastric intubation for some days postoperatively is important to reduce the risk of dehiscence of the suture line. Similarly, this method of feeding helps in the conservative management of such a fistula and should be combined with muzzling of the patient, in an attempt to reduce contamination of the airway by food and bedding material.
Salivary tissue
Injuries to the salivary glands usually occur as a result of direct trauma. The parotid gland is the most vulnerable because of its large size and superficial location behind the angle of the jaw. Such injuries can be repaired by wound debridement, cleansing, and closure of the skin. Salivary cutaneous fistulae are rare after this sort of injury.
Injuries to the parotid duct at more rostral sites are more common and usually associated with direct trauma to the ventral border of the mandible, which the duct crosses beneath before entering the oral cavity. In some cases, there may be little evidence of an injury to the duct, and there may be no need for specific treatment as such wounds may readily heal spontaneously. However, in a proportion of cases, there is direct continuity between a ruptured salivary duct and a skin wound that may result in the development of a salivary facial fistula (Fig. 9.15). Such injuries often have the dramatic consequence of creating a profuse discharge of saliva during eating and mastication. Although saliva tends to have an inhibitory effect on healing, most of these wounds eventually close within 1–2 weeks, without need for specific treatment. It is the authors’ practice to manage all parotid duct fistulae conservatively in the certain knowledge that in the vast majority of cases the fistula heals uneventfully.

Fig. 9.15 This horse developed a salivary fistula, which caused saliva to flow out under pressure during eating (arrow) following damage to the parotid duct during surgical treatment of a chronic mandibular infection.
In those unusual cases in which the fistula does not close, surgical repair may be effective. The duct should be dissected from the edge of the fistula and closed with simple interrupted sutures of 2-metric polyglactin 910. Insertion of a catheter into the parotid duct may facilitate accurate suturing. Injury to the parotid duct may occur inadvertently during facial or dental surgery. However, an understanding of the local anatomy should preclude such an occurrence. Transection of the parotid duct may be performed electively when carrying out a buccotomy technique for removal of mandibular or maxillary cheek teeth. In such cases, an end-to-end anastomosis can be carried out using simple interrupted sutures of 2 metric polyglactin 910. A parotid duct fistula may follow surgical removal of sialoliths, which are occasionally encountered in older horses. Secondary closure of such wounds may be effective or, alternatively, they may be left to heal by second intention.
Injuries to the mandibular or sublingual salivary glands or ducts are very rare. The authors have encountered one horse with a ranula associated with the sublingual salivary duct that was managed successfully by oral marsupialization.
Temporomandibular articulation
Despite its superficial location, traumatic injuries to the temporomandibular joint are rare. On occasion, an open wound is encountered with direct communication to the joint; these cases are typically presented for treatment some time after initial injury, usually due to non-healing of the wound. Thorough assessment of the injury using skyline radiographic projections3 (Fig. 9.16; or preferably by computed tomography if available) and ultrasonography is essential when planning treatment. Debridement of the wound and lavage of the joint are performed under general anesthesia and aided by arthroscopy, followed by post-surgical wound management and antibiotic therapy. This usually results in successful resolution of the articular sepsis; however, some masticatory dysfunction may be a long-term sequel. Mandibular condylectomy and meniscectomy with a successful outcome have also been described and are an option for cases with severe or longstanding injury.4 Further details of temporomandibular disease are presented in Chapter 23.

Management of mandibular and maxillary fractures
Rostral mandibular fractures
Fractures of the rostral mandible are the most common type of jaw fracture sustained by horses.5,6 Such injuries typically arise from play behavior with or biting of stable furniture such as bucket handles, rack chains, window bars, and mangers and are most common in young horses. Although they are invariably contaminated and often dramatic in appearance, appropriate management usually results in good functional and cosmetic repair.7 Aside from some protrusion of the lower lip and scant hemorrhage, there is often little outward sign of injury. Oral pain tends not to be a feature, and affected horses are often found eating with little sign of discomfort; indeed most fractures are already heavily contaminated with food material when first examined (Fig. 9.17). The injury typically comprises partial avulsion of one or more incisor teeth with a variable amount of associated bone. Fractures typically range from simple loss or loosening of a single (usually corner) incisor tooth and its labial alveolar bone plate, to more extensive or complex fractures involving a single fragment accommodating several incisor teeth or several fragments. The fractured portion of the mandible is usually displaced ventrally, with a gingival or mucosal wound on the floor of the mouth communicating with the open fracture (Fig. 9.18). Bilateral fractures are less common (Fig. 9.19).



Near-complete avulsion of a single tooth with only gingival or minimal bone attachment may be dealt with by removal of the avulsed tooth by sharp dissection of the remaining gingiva, but most other types of injury warrant an attempt at reduction. Unless obviously devitalized, teeth should be left in situ, as removal can take place at a later date, if necessary. As these fractures often occur in young (1–2-year-old) horses, the avulsed teeth are usually deciduous incisors and thus the loss of any severely avulsed teeth is of minimal, long-term consequence. In contrast, the fracture often involves the dental sacs of developing permanent incisor teeth, and every effort should be made to retain these, given that their loss or disruption causes eventual maleruption of the permanent dentition.
Radiography may be unnecessary for the assessment of some simple rostral mandibular fractures because the choice of repair technique is determined by the clinical presentation of the fracture rather than by its radiological appearance. Radiography is much more important for horses with bilateral or comminuted rostral mandibular fractures which usually require a more complicated repair. Surgical reduction may be performed in the standing sedated patient, aided by bilateral regional analgesia of the mandibular nerves within the mental foramina, or under general anesthesia. Following lavage and gentle curettage of the fracture, satisfactory reduction is usually possible with relative ease. The objective of fracture repair is to re-establish anatomical alignment (to optimize cosmetic and functional outcome) and to stabilize the fracture fragments. Whilst some rostral mandibular fractures heal without surgical intervention, healing in such cases is often delayed and almost invariably results in long-term disfigurement of the incisor arcade.
Fracture reduction in the young horse can usually be achieved through placement of single or multiple intra-oral tension wires attaching the avulsed portion to the caudal interdental space of the contralateral aspect of the mandible. Wires can be inserted via appropriate holes in the mandible drilled with a 2.7- or 3.2-mm Steinmann pin held in a hand chuck (Fig. 9.20) or by using an air drill (Fig. 9.21). Cannulation of the holes with a 14-gauge needle facilitates placement of the wire between teeth. A 14-gauge needle may be pushed through the softer mandibular bones of young foals without prior drilling of holes. At the completion of the procedure, the wire should pass through the fracture fragment, across the floor of the mouth, through the contralateral mandibular diastema then around the labial aspect of the rostral mandible (Fig. 9.22). The exact positioning of the anchoring holes will vary depending on fracture configuration and individual anatomical features. Wires are pressed digitally into the floor of the mouth to remove as much ‘slack’ as possible and to ensure they impinge as little as possible on the tongue. The ends are then brought together on the labial aspect of the mandible at a site distant to the fracture. Once the wire has been tightened and cut, it is necessary to protect the adjacent soft tissues from the sharp ends of the knot. A small amount of silicon polymer dental impression material, or acrylic bone cement can be affixed to the wire knot; alternatively, the tips of the wires can be sheathed with plastisol covers, which prevent labial abrasion.



Suturing large mucosal lacerations may prevent continued gross contamination of the fracture site but is not necessary in most cases. Postoperative lavage (with a saline solution or even tap water b.i.d or t.i.d) is recommended to prevent food accumulation in any large oral defects for the few days it takes for satisfactory granulation of the wound to occur. However, despite the contaminated nature of many of these fractures, the incidence of significant postoperative infections is very low. It is not usually necessary to make any significant dietary alterations following repair for a simple rostral mandibular fracture. However, hay should be pulled apart and fed loose from the ground or chopped so the horse does not have to prehend with the repaired teeth. Typically horses show little sign of having sustained an injury and bitted ridden work can resume unless signs of pain are observed. If a bit is to be used it should always be inserted very carefully. Wires should ideally remain in place for 6–8 weeks. Removal of the wire is usually simple in the standing sedated animal (Fig. 9.23). The visible oral portion of the wire is first cut with wire cutters, then the knot on the labial aspect of the jaw is grasped and pulled firmly, drawing the entire implant from the jaw.

With good surgical reduction, complications are rare. The major long term adverse consequence of a fracture of the rostral mandible is malalignment of the incisor arcades. Disruption or loss of permanent incisor tooth germs can result in a failure of some teeth to erupt, or to erupt in inappropriate positions. Occasionally, a permanent incisor tooth is noted erupting in the floor of the mouth, beside the original fracture line, although this sequel is usually of cosmetic importance only. Other sequelae include scarring of the gingiva and incisor diastema formation.
Fractures of the interdental space (diastema)
Fractures through the interdental space may be unilateral or bilateral. Unilateral fractures usually arise from direct trauma, but pathological fractures secondary to longstanding osteomyelitis/apical dental infection are not unknown. Bilateral mandibular fractures are common in foals, and unilateral fractures more typically occur in older horses. Treatment of traumatic, unilateral, hemimandibular fractures is usually unnecessary as the unaffected hemimandible acts as a splint to ensure relative stability of the fragments and therefore good fracture healing. Clearly, complete bilateral fractures result in major instability of the rostral portion of the mandible. Such fractures are usually transverse or short oblique in configuration, and have minimal comminution (Fig. 9.24). Fractures of the maxillary interdental space are by comparison much less common but may involve comminution and some degree of nasal obstruction. In addition to premaxillary fractures, there may be concurrent fracture of the nasal septum, nasal process, facial bones or hard palate. A full radiographic series, including dorsoventral, lateral and oblique views, is indicated to delineate the fracture(s), and to identify involvement of adjacent teeth and osseous fragments. Computed tomography, if available, provides comprehensive characterization of the fracture configuration.

Repair of fractures of the interdental space is performed under general anesthesia. Intravenous anesthesia or nasotracheal intubation increases working space for the surgeon in the oral cavity, permitting the surgeon access both sides of the mandible. If surgical repair of a maxillary fracture is to be attempted, a standard orotracheal intubation is usually performed.
Methods of fixation of fractures of the interdental space include tension-band wiring, oral acrylic splints, U-bars, external fixators, and bone plating. Minimally displaced, unilateral fractures often have sufficient interdigitation at the fracture site to limit movement and pain and usually respond well to conservative therapy, which is the authors` preferred option in most cases. However, non-displaced fractures of the interdental space may be repaired using tension-band wiring. The tension surface of the mandible lies along the dorsal border (oral surface) allowing tension-band wiring to be successful when minimal displacement is present. Minimally displaced fractures through the maxillary interdental space are rare and almost always bilateral. They have been successfully managed using a conservative approach, but such fractures also can be stabilized with tension band wires (Fig. 9.25) or an external fixation device.

Repair of bilateral interdental space mandibular fractures involves placing the anesthetized horse in dorsal recumbency; the oral cavity, left and right external cheek surfaces are then prepared for surgery. Holes are drilled between mandibular incisors as described previously. To repair rostral mandibular fractures, stab incisions are made bilaterally through the gingiva immediately caudal to the 06 (2nd premolar teeth). For more caudally situated mandibular fractures, horizontal stab incisions are made externally in the cheeks at a site between the 07s and 08s (second and third mandibular premolar teeth). Hemorrhage is minimized by using blunt dissection to separate underlying soft tissues. The buccal mucosa is incised, and a 3.2-mm drill bit is positioned between the 07 and 08 teeth just ventral to the gingival margin. Soft tissues are protected during drilling by use of a drill guide. Wire is threaded through the holes between the premolar teeth and directed rostrally to be interwoven through openings previously made between the incisors. Differing patterns for wire placement may be used incorporating one or two wires. The wire spanning the interdental space is twisted together to achieve compression at the fracture site. The stab incisions through the cheeks are left to heal by second intention or closed with a single suture. The wires are removed 6–8 weeks after fixation.
Intra-oral acrylic splints can also provide stable fixation of interdental space fractures and are technically easy to use.7 Following induction of general anesthesia and preparation of the oral cavity and cheeks, the fracture is reduced. Polymethylmethacrylate or cold-curing acrylic is mixed and molded to fit the oral surface of the mandible or premaxilla, extending from the incisors to the 06, taking care to avoid the frenulum of the tongue. A thickness of 6–8 mm is sufficient for most splints; the acrylic may be thickened at sites of wire incorporation to reduce fatigue and thus breakage of the splint. The splint is removed after curing and rough edges are smoothed with files. Multiple, 1.2-mm-diameter wire loops are placed through holes drilled into both sides of the mandible or premaxillae between the incisors and in the interdental space, rostral and caudal to the fracture line. The splint is drilled to match the holes in the mandible or maxillae and the wires are twisted together and bent down into the gingiva. Wire loops may also be placed around the 06s (second premolar teeth) to provide caudal anchorage. Holes for these wires are placed as described above for tension-band wiring. Alternatively, the methylmethacrylate splint can be formed over preplaced tension band wires between the incisors and premolars. This technique allows the fracture to be reduced completely before application of the splint.
Intra-oral acrylic splints require minimal surgical invasion of the mandible, avoid the risk of damage to dental buds or apices and provide fixation on the tension side of the fracture. Acrylic splinting can be used successfully in foals with inadequate incisor eruption for placement of wires. In foals, a wire loop can be passed around the mandible in the diastema as an additional anchorage point for the splint. Care should be taken to pass the wire close to the bone to avoid compression and necrosis of the soft tissues, although any gingival damage resolves rapidly after wire removal. The oral cavity should be flushed daily and the splint removed 6–8 weeks after surgery, in the standing, sedated patient.
Although intra-oral placement of U-bars with fixation around the teeth using wire has been described7 to treat bilateral fractures of the interdental space, there are simpler methods of repairing such unstable fractures. There have been reports of using intra-oral orthopedic plates screwed to the teeth which seem to have been effective. Both techniques have the obvious drawback of involving a relatively large intra-oral device.
A simpler approach involves the use of long AO cortical screws drilled into either the mandible or premaxilla to fix lateral acrylic bars (Fig. 9.26). This simple technique has proven valuable to repair unstable fractures of the interdental space (R. J. Payne, unpublished data). A 3.2-mm drill is used to create holes through stab incisions in the gingiva or cheeks (as described above) at several appropriate sites rostral and caudal to the fracture on both sides of the head. Pre-drilled flexible tubing is threaded onto the long cortical screws before their incomplete implantation in the jaw. The screws are left protruding clear of the jaw to accommodate the tubing, which is then filled with acrylic material. This material rapidly cures to create a very stable fixation of the fracture on either side of the jaw. This method avoids the presence of implants within the oral cavity and is as effective as proprietary external fixation devices or the use of trans-mandibular Steinmann pins, which have also been used to stabilize such fractures by attaching them to laterally applied acrylic bars (Fig. 9.27).


The implants occasionally break but can usually be replaced without requiring a second general anesthetic. The device is usually removed in the sedated patient at approximately 6–8 weeks postoperatively. The screw holes usually heal faster than those created by transmandibular Steinmann pins.
Fractures of the caudal mandible
Fractures involving the horizontal ramus in the region of the molar teeth are typically unilateral with minimal displacement or comminution (Fig. 9.28). They typically arise from external trauma, such as a kick injury or fall, but iatrogenic fractures arising from dental repulsion procedures are also encountered. Aside from painful mastication, clinical signs may be non-specific. Thickening of the horizontal ramus may be noted, both externally and upon intra-oral examination; this may be subtle and tends to be generalized rather than the focal thickening seen with dental apical infection. Close examination of the oral cavity may also reveal some mucosal bruising in the region of the fracture line and on occasion there is concurrent (usually transverse) fracture of an adjacent cheek tooth.
While fractures of the mandibular body (horizontal ramus) are seen occasionally in our hospital, those of the vertical ramus are very uncommon, in contrast to other authors’ findings.8 The extent of the fracture and the possible involvement of teeth, temporomandibular joints, or even the hyoid apparatus should be assessed using multiple radiographic projections or computed tomography, if available. Such imaging is important to assess possible comminution, and allow a more informed decision regarding the choice of a surgical versus a more conservative approach to treatment of the injury. Reported fractures of the vertical ramus include transverse and oblique configurations, but perhaps the most commonly encountered involve the angle of the mandible. Caudal mandibular fractures can be treated using a conservative approach, or by compression plating or external fixation.
Most fractures of the caudal region of the body or ramus of the mandible, but especially those resulting in minimal instability, malocclusion, and pain, are candidates for conservative management. The overlying, deep and tightly attached pterygoid and masseter muscles confer significant stability to these fractures, acting much in the manner of a splint. Anti-inflammatory medication increases patient comfort, and feeding mashes of complete pelleted feeds provides nutrition in an easily consumed form. Antimicrobial therapy is indicated when the fracture is open to the oral cavity, and oral lavage may be of benefit in such cases. Some horses are inappetant immediately following such injuries and ensuring adequate hydration is imperative in these cases. However, in those animals without major intra-oral fragmentation, it is often surprising how little discomfort they exhibit compared to human patients with similar injuries.
Radiological evaluation of the fracture should be performed periodically. Possible indications for internal fixation of the fracture are lack of healing or osteomyelitis at the fracture site; however, the best guide to progress is the clinical status of the patient. Most fractures of the horizontal ramus involve the alveoli of the adjacent cheek teeth, and the resulting inflammatory response and possible contamination of the site through external or oral wounds may cause pulpitis and loss of vitality of one or more teeth. Radiological assessment may demonstrate clear evidence of such dental infection; however, it is important to defer any possible dental extraction procedures until such time as the mandibular fracture has stabilized. Exodontia is rarely a surgical imperative and being traumatic in nature demands a stable mandible if further injury to the patient is to be avoided.
Fracture of the caudal angle of the mandible with degloving of the overlying soft tissues has been described.8 The injury results from placement of the head between stationary objects and then pulling back; similar injuries can occur following other forms of direct trauma, and may also cause facial nerve damage. Communication of such fractures with the oral cavity or adjacent alveoli is uncommon. Surgical removal of small fracture fragments can be performed with minimal functional or cosmetic disturbance. However, it is usually better practice to let these remain in situ in the hope that they may be incorporated into the fracture healing process, which is usually the case. It is only occasionally necessary to carry out sequestrectomy several weeks post-injury. Although most heal without complication, internal fixation may be indicated for larger fragments, where a ventrolateral approach to the mandible is used. It is critical that the facial artery, facial vein, parotid salivary duct and mental nerve are identified and preserved during surgical dissection. Elevation of the masseter muscle from the mandible is necessary and accomplished by transection of the attachments of the muscle at the ventral border of the mandible and reflecting the muscle dorsally. The orthopedic plate used depends entirely on fracture configuration and size of the patient. The plate should be placed on the ventrolateral aspect of the mandible, if possible. The plate is contoured and attached to the bone; a minimum of three screws on either side of the fracture is recommended. Dental apices should be avoided when applying screws more rostrally in young horses.
A similar approach may be adopted for fractures of the vertical ramus. Although most are treated conservatively, surgical repair may be considered if a fracture is grossly unstable, or if there is marked malocclusion preventing prehension or mastication, pain with unwillingness to eat, or if the fracture is bilateral. Internal or external fixation can be used to stabilize such fractures. However, with the exception of those causing major dysfunction of the temporomandibular joint, the splinting effect of the heavy muscles of mastication is usually effective in preventing major fragment displacement until fracture healing. Although bone plating provides a very stable construct, extensive surgical dissection is required at a site containing many large blood vessels, parotid tissue and the facial nerve. Fractures open to the oral cavity can be expected to become infected, necessitating removal of plates after fracture healing. External fixators can also be used in the treatment of caudal fractures of the mandibular body.
The prognosis for healing of caudal mandibular fractures is guarded to good. Complications are usually associated with communication with the oral cavity and involvement of the teeth. When surgical repair is undertaken, aggressive debridement of the fracture line with thorough lavage, and closure of oral mucous membranes (if possible) are the best means of preventing osteomyelitis and sequestration. Implant-associated infection necessitates removal of plates or pins, debridement of soft tissues, lavage, and antibiotic medication. Resolution of infection after implant removal often proceeds without further complication. Failure of fracture healing is a significant complication. This will depend on the degree of stability and, most importantly, on the presence of infection. Use of a more stable means of fixation and addressing any infection ensure the best prognosis for complete healing. Adjunctive therapy, including autogenous cancellous bone grafting and antimicrobial impregnated beads, may be indicated.
1 Szpaderska AM, Zuckerman JD, DiPietro LA. Differential injury responses in oral mucosal and cutaneous wounds. J Dent Res. 2003;82(8):621–626.
2 Schrementi ME, Ferreira AM, Zender C, DiPietro LA. Site-specific production of TGF-β in oral mucosal and cutaneous wounds. Wound Repair Regen. 2008;16(1):80–86.
3 Ramzan PH, Marr CM, Meehan J, Thompson A. Novel oblique radiographic projection of the temporomandibular articulation of horses. Vet Rec. 2008;162(22):714–716.
4 Nagy AD, Simhofer H. Mandibular condylectomy and meniscectomy for the treatment of septic temporomandibular joint arthritis in a horse. Vet Surg. 2006;35(7):663–668.
5 Sullins KE, Turner AS. Management of fractures of the equine mandible and premaxilla (incisive bone). Compendium Continuing Education for the Practicing Veterinarian. 1982;4(11):480–489.
6 DeBowes RM. Fractures of the mandible and maxilla. In: Nixon AJ, ed. Equine fracture repair. Philadelphia: WB Saunders; 1996:323–332.
7 Henninger RW, Beard WL, Schneider RK, et al. Fractures of the rostral portion of the mandible and maxilla in horses: 89 cases (1979–1997). Journal of the American Veterinary Medical Association. 1999;214:1648–1652.
8 Knox PM, Crabill MR, Honnas CM. Mandibular and maxillary fracture osteosynthesis. In: Baker GJ, Easley J. Equine dentistry. Philadelphia: Elsevier, 2005.