CHAPTER 47 Upper arm
SKIN AND SOFT TISSUE
SKIN
Cutaneous vascular supply
The blood supply to the skin of the upper arm can be divided into three regions with separate supply: the deltoid region, supplied by musculocutaneous perforators, and the medial and lateral regions, supplied by fasciocutaneous perforators (Cormack & Lamberty 1994; Salmon 1994) (Fig. 47.1, Fig. 47.2).
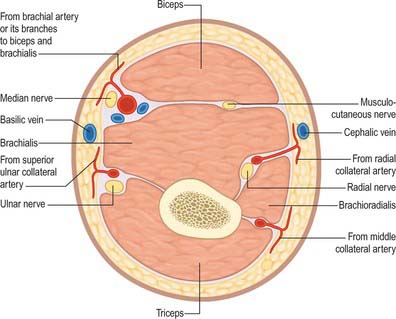
Fig. 47.1 Transverse section through the upper arm to show the location of fasciocutaneous perforators lying on the superficial aspect of the deep fascia.
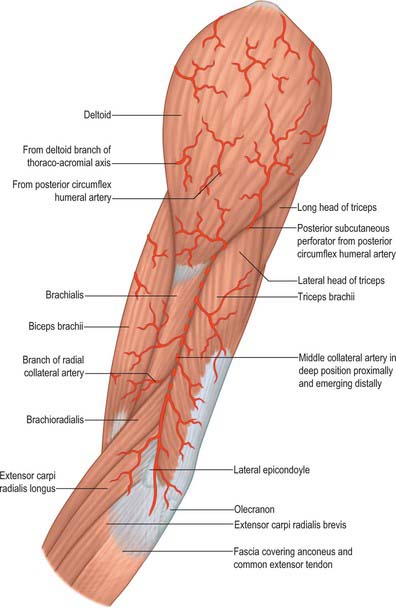
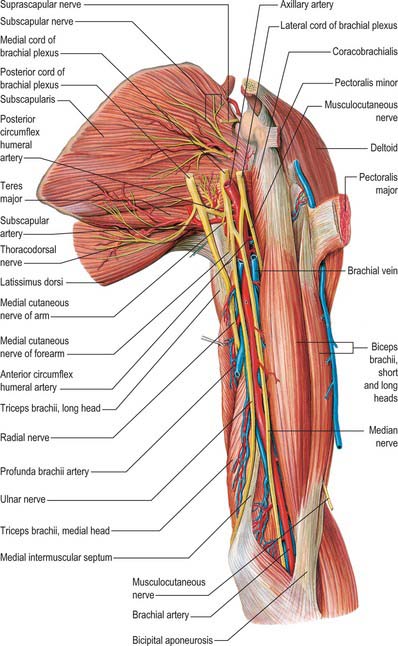
Fig. 47.2 Muscles of the left upper arm, viewed from the lateral aspect showing fasciocutaneous and musculocutaneous perforating vessels.
The deltoid region is supplied by the posterior circumflex humeral artery (p. 817) via musculocutaneous perforators. After the posterior circumflex humeral artery passes through the quadrangular space (p. 814) it gives off a descending branch, which runs down to the deltoid insertion and the overlying skin, and an ascending branch which passes superiorly towards the acromion, pierces the edge of deltoid and the deep fascia to fan out and supply the overlying skin.
The medial side of the upper arm is supplied by five or six fasciocutaneous perforators which arise from the brachial artery, the superior ulnar collateral artery and, if present, the single artery to biceps. These perforators pass along the medial intermuscular septum to spread out in the deep fascia and anastomose with perforating vessels superiorly and inferiorly and from the lateral side. There are virtually no musculocutaneous perforators through biceps or triceps.
The lateral side of the upper arm below deltoid is supplied by perforating vessels from the middle collateral and radial collateral arteries (the terminating bifurcation of the profunda brachii). The middle collateral artery sends perforators to the skin via the lateral intermuscular septum between brachioradialis and triceps, while the radial collateral artery gives off cutaneous perforators via the intermuscular septum between brachialis and brachioradialis. These cutaneous vessels anastomose with those from the medial side.
Cutaneous innervation
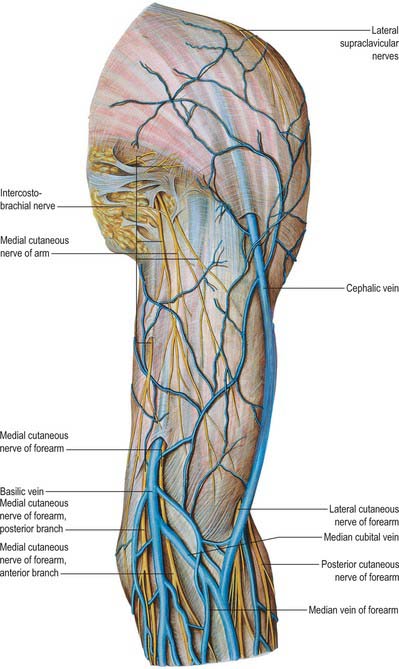
The skin of the shoulder region is supplied by the supraclavicular nerves from the cervical plexus. The floor of the axilla and upper medial surface of the arm is supplied by the lateral branch of the second intercostal nerve (the intercostobrachial nerve). The lower aspect of the medial side of the upper arm is supplied by the medial cutaneous nerve of the arm. The lateral aspect of the upper arm is supplied by the upper lateral cutaneous nerve (a branch of the axillary nerve) and the lower lateral cutaneous nerve (a branch of the radial nerve). The posterior aspect is supplied by the posterior cutaneous nerve of the arm, a branch of the radial nerve (Fig. 45.15, Fig. 45.14).
SOFT TISSUE
Brachial fascia
Brachial fascia, the deep fascia of the upper arm, is continuous with the fascia covering deltoid and pectoralis major: it forms a thin, loose sheath for muscles of the upper arm, and sends septa between them. It is thin over biceps, but thicker over triceps and the humeral epicondyles, and is strengthened by fibrous aponeuroses from pectoralis major and latissimus dorsi medially and from deltoid laterally. Strong medial and lateral intermuscular septa extend from it on each side.
The lateral intermuscular septum extends distally from the lateral lip of the intertubercular sulcus of the humerus along the lateral supracondylar ridge to the lateral epicondyle, and blends with the tendon of deltoid. It gives attachment to triceps behind, and brachialis, brachioradialis and extensor carpi radialis longus in front. It is perforated in the middle third by the radial nerve and the radial collateral branch of the profunda brachii artery. The thicker medial intermuscular septum extends from the medial lip of the intertubercular sulcus, distal to teres major, along the medial supracondylar ridge to the medial epicondyle, and blends with the tendon of coracobrachialis. It gives attachment to triceps behind, and brachialis in front. It is perforated by the ulnar nerve, superior ulnar collateral artery, and the posterior branch of the inferior ulnar collateral artery. At the elbow, the brachial fascia is attached to the epicondyles of the humerus and the olecranon of the ulna, and is continuous with the antebrachial fascia. Medially, just below the middle of the upper arm, it is traversed by the basilic vein and lymphatic vessels and, at various levels, branches of the brachial cutaneous nerves.
Together, the lateral and medial intermuscular septa of the upper arm divide the upper arm into anterior and posterior compartments.
MUSCLES
The muscles of the upper arm are coracobrachialis, which acts only on the shoulder joint; biceps and triceps, which cross both shoulder and elbow joints; and brachialis, which acts only at the elbow joint (Fig. 47.2, Fig. 47.3).
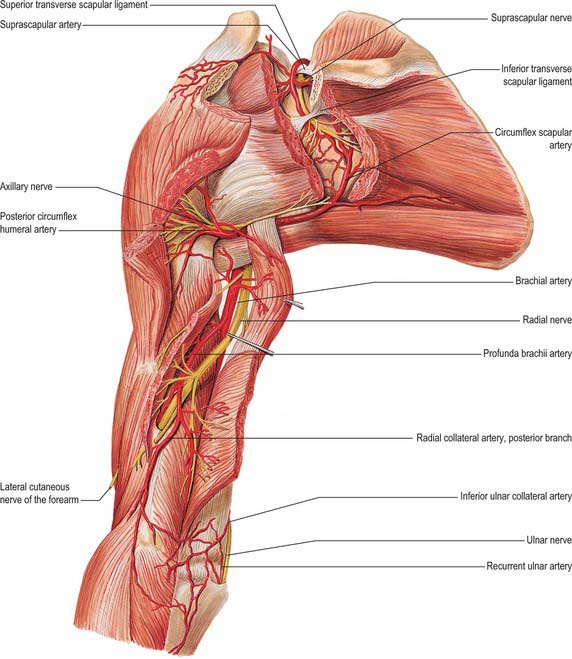
Fig. 47.3 Muscles, vessels and nerves of the left upper arm, viewed from the posterior aspect.
(From Sobotta 2006.)
ANTERIOR COMPARTMENT
Coracobrachialis
Coracobrachialis arises from the apex of the coracoid process, together with the tendon of the short head of biceps, and also by muscular fibres from the proximal 10 cm of this tendon; it ends on an impression, 3–5 cm in length, midway along the medial border of the humeral shaft between the attachments of triceps and brachialis (Fig. 46.20, Fig. 47.4). Accessory slips may be attached to the lesser tubercle, medial epicondyle or medial intermuscular septum.
Coracobrachialis forms an inconspicuous rounded ridge on the upper medial side of the arm; pulsation of the brachial artery can be felt and often seen in the depression behind it. The muscle is perforated by the musculocutaneous nerve. Anteriorly it is related to pectoralis major above and, at its humeral insertion, to the brachial vessels and median nerve, which cross it. The tendons of subscapularis, latissimus dorsi, and teres major, the medial head of triceps, the humerus and the anterior circumflex humeral vessels all lie posterior. The axillary artery (third part) and proximal parts of the median and musculocutaneous nerves lie medial. Biceps and brachialis lie lateral.
One or more branches from the axillary artery pass deep to the lateral root of the median nerve, and the musculocutaneous nerve, to reach the deep surface of the muscle. Branches from the anterior circumflex humeral artery also supply the deep surface of the muscle. The accompanying artery of the musculocutaneous nerve sends a recurrent branch to the coracoid attachment and gives off a series of branches to the muscle during its intramuscular course. Accessory branches from the thoracoacromial artery provide additional supply to the superficial part of coracobrachialis.
Biceps brachii
Biceps brachii derives its name from its two proximally attached parts or ‘heads’ (Fig. 46.20). The short head arises by a thick flattened tendon from the coracoid apex, together with coracobrachialis. The long head starts within the capsule of the shoulder joint as a long narrow tendon, running from the supraglenoid tubercle of the scapula at the apex of the glenoidal cavity, where it is continuous with the glenoidal labrum (p. 805). The tendon of the long head, enclosed in a double tubular sheath (an extension of the synovial membrane of the joint capsule), arches over the humeral head, emerges from the joint behind the transverse humeral ligament, and descends in the intertubercular sulcus, where it is retained by the transverse humeral ligament and a fibrous expansion from the tendon of pectoralis major. The two tendons lead into elongated bellies that, although closely applied, can be separated to within 7 cm or so of the elbow joint. At this joint they end in a flattened tendon, which is attached to the rough posterior area of the radial tuberosity; a bursa separates the tendon from the smooth anterior area of the tuberosity. As it approaches the radius, the tendon spirals, its anterior surface becoming lateral before being applied to the tuberosity. The tendon has a broad medial expansion, the bicipital aponeurosis, which descends medially across the brachial artery to fuse with deep fascia over the origins of the flexor muscles of the forearm (Fig. 47.5). The tendon can be split without difficulty as far as the tuberosity, whence it can be confirmed that its anterior and posterior layers receive fibres from the short and long heads, respectively.
In 10% of cases, a third head arises from the superomedial part of brachialis and is attached to the bicipital aponeurosis and medial side of the tendon of insertion. It usually lies behind the brachial artery, but it may consist of two slips, which descend in front of and behind the artery. Less often, other slips may spring from the lateral aspect of the humerus or intertubercular sulcus.
Biceps is overlapped proximally by pectoralis major and deltoid; distally it is covered only by fasciae and skin, and it forms a conspicuous elevation on the front of the arm. Its long head passes through the shoulder joint; its short head is anterior to the joint. Distally it lies anterior to brachialis, the musculocutaneous nerve and supinator. Its medial border touches coracobrachialis, and overlaps the brachial vessels and median nerve; its lateral border is related to deltoid and brachioradialis.
Biceps brachii is typically supplied by up to eight vessels originating from the brachial artery in the middle third of the arm. These vessels pass laterally, posterior to the median nerve and divide into ascending and descending branches just before reaching the deep surface of the muscle. Smaller branches arise from the anterior circumflex humeral artery and the deltoid branch of the acromial division of the thoracoacromial axis.
There is great variation in the arterial supply to the muscle. The main arterial supply may originate from the superior or inferior ulnar collateral artery, subscapular artery, axillary artery, ulnar or radial arteries in cases of proximal bifurcation of the brachial artery, or the profunda brachii artery.
Biceps brachii is innervated by the musculocutaneous nerve, C5 and 6, with separate branches passing to each belly.
Biceps brachii is a powerful supinator, especially in rapid or resisted movements. It flexes the elbow, most effectively with the forearm supinated, and acts to a slight extent as a flexor of the shoulder joint. It is attached, via the bicipital aponeurosis, to the posterior border of the ulna, the distal end of which is drawn medially in supination. The long head helps to check upward translation of the humeral head during contraction of deltoid. When the elbow is flexed against resistance, the tendon of insertion and bicipital aponeurosis become conspicuous.
Lowering the hand under the influence of gravity by extension at the elbow calls for controlled lengthening of biceps. This is an example of a habitual movement in which muscle tension increases despite increasing length. As the hand descends and the elbow extends, the vertical through the centre of gravity of the forearm is carried further from the fulcrum of movement; the turning moment exerted by the load therefore increases and must be matched by an increase in the moment exerted by the muscle.
Brachialis
Brachialis arises from the lower half of the front of the humerus, starting on either side of the insertion of deltoid, and extending distally to within 2.5 cm of the cubital articular surface (Fig. 46.20, Fig. 47.4). It also arises from the intermuscular septa, more from the medial than the lateral, since it is separated distally from the lateral intermuscular septum by brachioradialis and extensor carpi radialis longus. Its fibres converge to a thick, broad tendon which is attached to the ulnar tuberosity and to a rough impression on the anterior aspect of the coronoid process.
Brachialis may be divided into two or more parts. It may be fused with brachioradialis, pronator teres or biceps. In some cases it sends a tendinous slip to the radius or bicipital aponeurosis.
Anterior are biceps, the brachial vessels, musculocutaneous and median nerves. Posterior are the humerus and capsule of the elbow joint. Medial are pronator teres, and the medial intermuscular septum, which separates it from triceps and the ulnar nerve. Lateral are the radial nerve, radial recurrent and radial collateral arteries, brachioradialis and extensor carpi radialis longus.
The blood supply to brachialis typically consists of two main arteries (superior and inferior) supplemented by a system of accessory arteries. The superior main artery originates from the brachial artery distal to the site of origin of the superior ulnar collateral artery and travels laterally to enter the anterior surface of the upper third of the muscle. The inferior main artery originates either from the superior ulnar collateral artery or directly from the brachial artery and enters the mid-portion of the muscle. The accessory arteries are small, variable in number, origin and course. They can arise from the brachial artery, the superior and inferior ulnar collateral arteries, or the profunda brachii artery.
Brachialis is innervated by the musculocutaneous nerve (C5 and 6), and radial nerve (C7) to a small lateral part of the muscle.
POSTERIOR COMPARTMENT
Triceps
Triceps fills most of the extensor compartment of the upper arm (Fig. 46.22, Figs 47.2-47.4). It arises by three heads (long, lateral and medial), from which it takes its name.
The long head arises by a flattened tendon from the infraglenoid tubercle of the scapula, blending above with the glenohumeral capsule. Its muscular fibres descend medial to the lateral head and superficial to the medial head, and join them to form a common tendon.
The lateral head arises by a flattened tendon from a narrow, linear, oblique ridge on the posterior surface of the humeral shaft, and from the lateral intermuscular septum. The origin on the humerus ascends with varying obliquity from its lateral border above the radial groove and behind the deltoid tuberosity to the surgical neck medial to the insertion of teres minor. These fibres also converge to the common tendon.
The medial head, which is overlapped posteriorly by the lateral and long heads, has a particularly extensive origin, from the entire posterior surface of the humeral shaft, below the radial groove from the insertion of teres major to within 2.5 cm of the trochlea, from the medial border of the humerus; the medial intermuscular septum and the lower part of the lateral intermuscular septum. Some muscular fibres reach the olecranon directly, the rest converge to the common tendon.
The tendon of triceps begins near the middle of the muscle. It has two laminae, one superficial in the lower half of the muscle, the other in its substance. After receiving the muscle fibres, the two layers unite above the elbow and are attached, for the most part, to the upper surface of the olecranon. On the lateral side a band of fibres continues down over anconeus to blend with antebrachial fascia.
The long head descends between teres minor and major, dividing the wedge-shaped interval between them and the humerus into triangular and quadrangular parts (Fig. 46.22). The triangular space contains the circumflex scapular vessels; it is bounded above by teres minor, below by teres major, laterally by the long head of triceps. The quadrangular space transmits the posterior circumflex humeral vessels and the axillary nerve; it is bounded above by subscapularis, teres minor and the articular capsule, below by teres major, medially by the long head of triceps, and laterally by the humerus.
The lateral head of triceps forms an elevation, parallel and medial to the posterior border of the deltoid; it stands out prominently when the elbow is actively extended. The mass which lies medial to it, and disappears under the deltoid, is the long head.
The blood supply to triceps is mainly from the profunda brachii artery and the superior ulnar collateral artery, with an accessory supply from the posterior circumflex humeral artery. The medial head of triceps is supplied on its anterior surface by two or three branches from the superior ulnar collateral artery. The posterior surface is supplied by a large proximal branch from the profunda which passes medially in front of the radial nerve. The long head of triceps is supplied on its anterior surface by two arteries, one arising from the axillary artery in front of the tendon of latissimus dorsi and the other arising from either the brachial artery or the superior ulnar collateral. The posterior surface receives a recurrent branch from the posterior circumflex humeral artery immediately after traversing the quadrangular space. The lateral surface receives a number of small branches from the profunda brachii in its distal portion. The lateral head of the triceps is primarily supplied by branches of the profunda brachii, with an additional supply from a branch of the posterior circumflex humeral artery.
Triceps is the major extensor of the forearm at the elbow joint. The medial head is active in all forms of extension. The lateral and long heads are minimally active except in extension against resistance, as in thrusting or pushing or supporting body weight on the hands with the elbows semiflexed. When the flexed arm is extended at the shoulder joint, the long head may assist in drawing back and adducting the humerus to the thorax. The long head supports the lower part of the capsule of the shoulder joint, especially when the arm is raised. Articularis cubiti probably draws up the posterior part of the capsule of the elbow joint during extension of the forearm. In forceful supination of the semiflexed forearm, involving contraction of both supinator and biceps brachii, the triceps contracts synergistically to maintain the semiflexed position.
VASCULAR SUPPLY AND LYMPHATIC DRAINAGE
ARTERIES
Brachial artery
The brachial artery, a continuation of the axillary, begins at the distal (inferior) border of the tendon of teres major and ends about a centimetre distal to the elbow joint (at the level of the neck of the radius) by dividing into radial and ulnar arteries (Fig. 47.5, Fig. 47.6). At first it is medial to the humerus, but gradually spirals anterior to it until it lies midway between the humeral epicondyles. Its pulsation can be felt throughout.
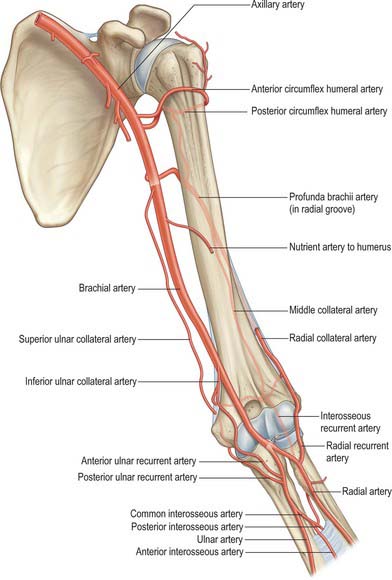
Fig. 47.6 The arterial anastomoses around the left elbow joint viewed from the anterior aspect.
(From Drake, Vogl and Mitchell 2005.)
Relations
The brachial artery is wholly superficial, covered anteriorly only by skin and superficial and deep fasciae. The bicipital aponeurosis crosses it anteriorly at the elbow, separating it from the median cubital vein; the median nerve crosses it lateromedially near the distal attachment of coracobrachialis. Posterior are the long head of triceps, separated by the radial nerve and profunda brachii artery, and then successively by the medial head of triceps, the attachment of coracobrachialis and brachialis. Proximally the median nerve and coracobrachialis lie laterally while distally the biceps and the muscles overlap the artery. Proximally the medial cutaneous nerve of the forearm and ulnar nerve lie medially, while distally the median nerve and basilic vein lie medially. With the artery are two venae comitantes, connected by transverse and oblique branches.
At the elbow the brachial artery sinks deeply into the triangular intermuscular cubital fossa (p. 831).
Variants
The brachial artery, with the median nerve, may diverge from the medial border of the biceps, descending towards the medial humeral epicondyle, usually behind a supracondylar process from which a fibrous arch crosses the artery, and which then runs behind or through pronator teres to the elbow. Occasionally the artery divides proximally into two trunks which reunite. Frequently it divides more proximally than usual into radial, ulnar and common interosseous arteries. Most often the radial branches arise proximally, leaving a common trunk for the ulnar and common interosseous; sometimes the ulnar arises proximally, the radial and common interosseous forming the other division; the common interosseous may also arise proximally. Sometimes slender vasa aberrantia connect the brachial to the axillary artery or to one of the forearm arteries, usually the radial. The brachial artery may be crossed by muscular or tendinous slips from coracobrachialis, biceps, brachialis or pronator teres. Rarely the median nerve crosses behind, and not in front of, the brachial artery near the insertion of coracobrachialis.
Branches
These are profunda brachii, nutrient, superior, middle and inferior ulnar collateral, deltoid, muscular, radial and ulnar arteries.
The profunda brachii (Fig. 47.2, Fig. 47.3, Fig. 47.5, Fig. 47.6) is a large branch from the posteromedial aspect of the brachial artery, distal to teres major. It follows the radial nerve closely, at first posteriorly between the long and medial heads of triceps, then in the spiral groove covered by the lateral head of triceps. It supplies muscular branches, the nutrient artery of the humerus, and finally divides into terminal radial and middle collateral branches (Fig. 47.6). The radial collateral branch pierces the lateral intermuscular septum to reach the anterior aspect of the epicondyle of the humerus in the groove between brachioradialis and brachialis, and takes part in the anastomosis around the elbow. The middle collateral branch runs posterior to the septum and epicondyle.
The profunda brachii can originate from a common origin with the posterior circumflex humeral artery, from the axillary artery proximal to the tendon of latissimus dorsi or from the distal portion of the axillary artery.
Middle collateral (posterior descending) branch
The middle collateral artery is the larger terminal vessel. It arises posterior to the humerus and descends down the posterior surface of the lateral intermuscular septum to the elbow (Fig. 47.4, Fig. 47.6). Proximally, the artery lies between brachialis (anteriorly) and the lateral head of triceps (posteriorly) while distally it lies between brachioradialis (anteriorly) and the lateral head of triceps (posteriorly). It may pierce the deep fascia and become cutaneous or remain deep to the fascia until anastomosing with the interosseous recurrent artery behind the lateral epicondyle; it gives off about five small fasciocutaneous perforators and often has a small branch that accompanies the nerve to anconeus.
This artery and its fasciocutaneous perforators provide the anatomical basis to allow a skin flap (the lateral arm flap) to be surgically raised (either pedicled or by free tissue transfer) for reconstructing areas of tissue missing elsewhere in the body.
Radial collateral (anterior descending) branch
The radial collateral artery is the continuation of the profunda (Fig. 47.6). It accompanies the radial nerve through the lateral intermuscular septum, descending between brachialis and brachioradialis anterior to the lateral epicondyle, anastomosing with the radial recurrent artery. It supplies brachialis, brachioradialis, the radial nerve and a few fasciocutaneous perforators.
The nutrient artery of the humerus arises near the mid-level of the upper arm, and enters the nutrient canal near the attachment of coracobrachialis, posterior to the deltoid tuberosity; it is directed distally.
Superior ulnar collateral artery
The superior ulnar collateral artery arises a little distal to the mid-level of the upper arm, usually from the brachial artery, but often as a branch from the profunda brachii (Figs 47.4-47.6). It accompanies the ulnar nerve, piercing the medial intermuscular septum to descend in the posterior compartment and supply the medial head of triceps. It passes between the medial epicondyle and olecranon, ending deep to flexor carpi ulnaris by anastomosing with the posterior ulnar recurrent and inferior collateral arteries. A branch sometimes passes anterior to the medial epicondyle and anastomoses with the anterior ulnar recurrent artery.
Middle ulnar collateral artery
If present, the middle ulnar collateral artery arises from the brachial artery between the superior and inferior ulnar collaterals. It passes anterior to the medial epicondyle and anastomoses with the anterior ulnar recurrent artery. It supplies triceps and sends small fasciocutaneous perforators to the skin.
Inferior ulnar collateral (supratrochlear) artery
The inferior ulnar collateral artery begins approximately 5 cm proximal to the elbow, passes medially between the median nerve and brachialis and, piercing the medial intermuscular septum, curls round the humerus between the triceps and bone (Fig. 47.5, Fig. 47.6). It forms, by its junction with the middle collateral branch of the profunda brachii artery, an arch proximal to the olecranon fossa. As it lies on brachialis it gives off branches which descend anterior to the medial epicondyle to anastomose with the anterior ulnar recurrent artery. Behind the epicondyle a branch anastomoses with the superior ulnar collateral and posterior ulnar recurrent arteries.
VEINS
Brachial veins
The brachial veins flank the brachial artery, as venae comitantes with tributaries similar to the arterial branches; near the lower margin of subscapularis they join the axillary vein. The medial branch, however, often joins the basilic before it becomes the axillary.
These deep veins have numerous anastomoses with each other and with the superficial veins.
Superficial veins
The cephalic vein ascends in front of the elbow superficial to a groove between the brachioradialis and biceps, crosses superficial to the lateral cutaneous nerve of the forearm, ascends lateral to biceps and between pectoralis major and deltoid, where it adjoins the deltoid branch of the thoracoacromial artery (Fig. 45.5, Fig. 47.7). Entering the infraclavicular fossa to pass behind the clavicular head of pectoralis major, it pierces the clavipectoral fascia, crosses the axillary artery and joins the axillary vein just below clavicular level. It may connect with the external jugular by a branch anterior to the clavicle. Sometimes the median cubital vein is large, transferring most blood from the cephalic to the basilic vein; the proximal cephalic vein is then absent or much diminished.
INNERVATION
Median nerve
The median nerve (Fig. 45.7, Fig. 47.5, Fig. 47.8) enters the arm lateral to the brachial artery. Near the insertion of coracobrachialis it crosses in front of (rarely behind) the artery, descending medial to it to the cubital fossa where it is posterior to the bicipital aponeurosis and anterior to brachialis, separated by the latter from the elbow joint.
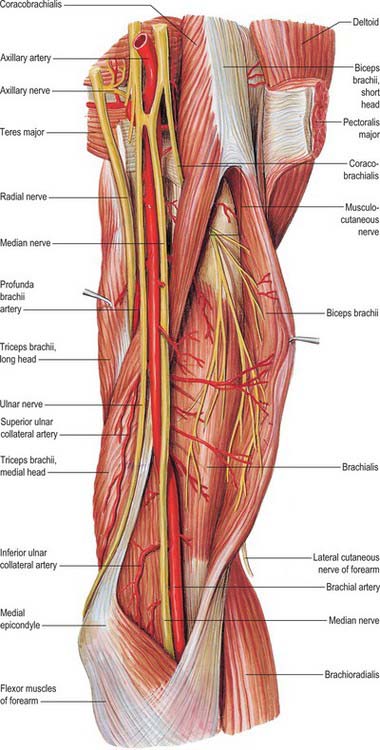
Fig. 47.8 Anterior aspect of the left upper arm dissected to show the musculocutaneous nerve.
(From Sobotta 2006.)
It gives off vascular branches to the brachial artery and usually a branch to pronator teres, a variable distance proximal to the elbow joint.
Musculocutaneous nerve
The musculocutaneous nerve is the nerve of the anterior compartment of the arm (Fig. 47.5, Fig. 47.8). It gives a branch to the shoulder joint and then passes through coracobrachialis, which it supplies, emerging to pass between biceps and brachialis. It sends branches to both these muscles. In the cubital fossa it lies at the lateral margin of the biceps tendon where it continues as the lateral cutaneous nerve of the forearm.
The musculocutaneous nerve has frequent variations. It may run behind coracobrachialis or adhere for some distance to the median nerve and pass behind biceps. Some fibres of the median nerve may run in the musculocutaneous nerve, leaving it to join their proper trunk; less frequently the reverse occurs, and the median nerve sends a branch to the musculocutaneous. Occasionally it supplies pronator teres and may replace radial branches to the dorsal surface of the thumb.
Ulnar nerve
The ulnar nerve gives no branches in the arm (Fig. 47.5, Fig. 47.8). It runs distally through the axilla medial to the axillary artery and between it and the vein, continuing distally medial to the brachial artery as far as the midarm. Here it pierces the medial intermuscular septum, inclining medially as it descends anterior to the medial head of triceps to the interval between the medial epicondyle and the olecranon, with the superior ulnar collateral artery.
Radial nerve
The radial nerve descends behind the third part of the axillary artery and the upper part of the brachial artery, anterior to subscapularis and the tendons of latissimus dorsi and teres major (Figs 47.2-47.4, Fig. 47.8). With the profunda brachii artery it inclines dorsally, passing through the triangular space (see p. 814) below the lower border of teres major, between the long head of triceps and the humerus. Here it supplies the long head of triceps, and gives rise to the posterior cutaneous nerve of the arm which supplies the skin along the posterior surface of the upper arm. It then spirals obliquely across the back of the humerus, lying posterior to the uppermost fibres of the medial head of triceps which separate the nerve from the bone in the first part of the spiral groove. Here it gives off a muscular branch to the lateral head of triceps and a branch which passes through the medial head of triceps to anconeus. On reaching the lateral side of the humerus it pierces the lateral intermuscular septum to enter the anterior compartment; it then descends deep in a furrow between brachialis and proximally brachioradialis, then more distally extensor carpi radialis longus. Anterior to the lateral epicondyle it divides into superficial and deep terminal rami.
The branches of the radial nerve in the upper arm are: muscular, cutaneous, articular and superficial terminal and posterior interosseous.
Muscular branches
Muscular branches supply triceps, anconeus, brachioradialis, extensor carpi radialis longus and brachialis in medial, posterior and lateral groups. Medial muscular branches arise from the radial nerve on the medial side of the arm. They supply the medial and long heads of triceps; the branch to the medial head is a long, slender filament which, lying close to the ulnar nerve as far as the distal third of the arm, is often termed the ulnar collateral nerve. A large posterior muscular branch arises from the nerve as it lies in the humeral groove. It divides to supply the medial and lateral heads of triceps and anconeus, that for the latter being a long nerve which descends in the medial head of triceps and partially supplies it; it is accompanied by the middle collateral branch of the profunda brachii artery and passes behind the elbow joint to end in anconeus. Lateral muscular branches arise in front of the lateral intermuscular septum; they supply the lateral part of brachialis, brachioradialis and extensor carpi radialis longus.
Cutaneous branches
Cutaneous branches are the posterior and lower lateral cutaneous nerves of the arm and the posterior cutaneous nerve of the forearm.
Lower lateral cutaneous nerve of the arm
The lower lateral cutaneous nerve of the arm perforates the lateral head of triceps distal to the deltoid tuberosity, passes to the front of the elbow close to the cephalic vein and supplies the skin of the lateral part of the lower half of the arm.
Posterior cutaneous nerve of the arm
The small posterior cutaneous nerve of the arm arises in the axilla and passes medially to supply the skin on the dorsal surface of the arm nearly as far as the olecranon. It crosses posterior to and communicates with the intercostobrachial nerve.
Posterior cutaneous nerve of the forearm
The posterior cutaneous nerve of the forearm arises with the lower lateral cutaneous nerve of the arm. Perforating the lateral head of triceps, it descends first lateral in the arm, then along the dorsum of the forearm to the wrist, supplying the skin in its course and joining, near its end, with dorsal branches of the lateral cutaneous nerve of the forearm.
Lesions of the radial nerve in the upper arm
Lesions of the radial nerve at its origin from the posterior cord in the axilla may be caused by pressure from a long crutch (crutch palsy). Triceps is only involved when lesions occur at this level and is usually spared in the more common lesions of the radial nerve in the arm as it lies alongside the spiral groove, where the nerve is commonly affected by fractures of the humerus. Compression of the nerve against the humerus occurs if the arm is rested on a sharp edge such as the back of a chair (‘Saturday night palsy’). Both these injuries cause weakness of brachioradialis with wasting and loss of the reflex. There is both wrist and finger drop due to weakness of wrist and finger extensors, as well as weakness of extensor pollicis longus and abductor pollicis longus. There may be sensory impairment or paraesthesiae in the distribution of the superficial radial nerve. However, nerve overlap means that only a small area of anaesthesia usually occurs on the dorsum of the hand between the first and second metacarpal bones.
Medial cutaneous nerve of arm
The medial cutaneous nerve of arm supplies the skin of the medial aspect of the arm (Fig. 47.7). It is the smallest branch of the brachial plexus, and arises from the medial cord and contains fibres from the eighth cervical and first thoracic ventral rami. It traverses the axilla, crossing anterior or posterior to the axillary vein, to which it is then medial, and communicating with the intercostobrachial nerve; it descends medial to the brachial artery and basilic vein (Fig. 47.7) to a point midway in the upper arm, where it pierces the deep fascia to supply a medial area in the distal third of the arm, extending on to its anterior and posterior aspects. Rami reach the skin anterior to the medial epicondyle, and over the olecranon. It connects with the posterior branch of the medial cutaneous nerve of the forearm. Sometimes the medial cutaneous nerve of the arm and the intercostobrachial nerve are connected in a plexiform manner in the axilla. The intercostobrachial nerve may be large and reinforced by part of the lateral cutaneous branch of the third intercostal nerve. It then replaces the medial cutaneous nerve of the arm and receives a connection representing the latter from the brachial plexus (occasionally this connection is absent).
Medial cutaneous nerve of forearm
The medial cutaneous nerve of forearm comes from the medial cord (Fig. 47.7). It is derived from the eighth cervical and first thoracic ventral rami. At first it is between the axillary artery and vein and gives off a ramus which pierces the deep fascia to supply the skin over the biceps, almost to the elbow. The nerve descends medial to the brachial artery, pierces the deep fascia with the basilic vein midway in the arm and divides into anterior and posterior branches. The larger, anterior branch usually passes in front of, occasionally behind, the median cubital vein, descending anteromedial in the forearm to supply the skin as far as the wrist and connecting with the palmar cutaneous branch of the ulnar nerve. The posterior branch descends obliquely medial to the basilic vein, anterior to the medial epicondyle, and curves round to the back of the forearm, descending on its medial border to the wrist, supplying the skin. It connects with the medial cutaneous nerve of the arm, the posterior cutaneous nerve of the forearm, and the dorsal branch of the ulnar.
Cormack GC, Lamberty BGH. The Arterial Anatomy of Skin Flaps. Edinburgh: Churchill Livingstone, 1994.
Salmon M. Anatomic studies. In: Taylor GI, Razaboni RM. Book 1: Arteries of the Muscles of the Extremities and the Trunk. Book 2: Arterial Anastomotic Pathways of the Extremities. New York: Quality Medical Publishing, 1994.