Clinical Judgment
Applying Critical Thinking and Ethical Decision Making
At the end of the chapter, the reader will be able to:
1 Define terms related to thinking, ethical reasoning, and critical thinking.
2 Identify and discuss the three principles of ethics underlying bioethical reasoning.
3 Describe the 10 steps of critical thinking.
4 Identify criteria necessary for acquisition of a value.
5 Discuss the application of ethics in nurse-client relationships.
6 Analyze the critical thinking process used in clinical judgments with clients.
7 Apply the critical thinking process to decision making in clinical nursing situations.
8 Demonstrate ability to analyze, synthesize, and evaluate a complex simulated case situation to make a clinical judgment.
9 Discuss application of findings from a research study to clinical practice.
This chapter examines the principles of ethical decision making and the process for critical thinking. Both are essential foundational knowledge for you to make effective nursing clinical judgments. These competencies, together with expert communication skills, are an integral part of nursing practice (Fero, Witsberger, Wesmiller, Zullo, & Hoffman, 2009). Ethical discussions in this book focus on the current literature in bioethics as held in Western society. In addition to basic content knowledge, throughout this book are included ethical dilemmas to help you begin applying your knowledge.
Critical thinking is a learned skill that teaches you how to “think about your thinking.” In the past, expert nurses accumulated this skill with on-the-job experience, through trial and error. But this is an essential nursing skill that can be learned with practice while in school. The Applications section of this chapter specifically walks you through the reasoning process in applying the 10 steps of critical thinking.
Basic concepts
There are many ways of thinking (Figure 3-1). Students often attempt to use total recall by simply memorizing a bunch of facts (e.g., memorizing the cranial nerves by using a mnemonic such as “On Old Olympus’ Towering Tops…”). At other times, we rely on developing habits by repetition, such as practicing cardiopulmonary resuscitation (CPR) techniques. More structured methods of thinking, such as inquiry, have been developed in disciplines related to nursing. For example, you are probably familiar with the scientific method. As used in research, this is a logical, linear method of systematically gaining new information, often by setting up an experiment to test an idea. The nursing process uses a method of systematic steps: assessment before planning, planning before intervention, and evaluation.

Knowing about your individual thinking style is vital not only for your own learning but also because your values affect the quality of relationships you are able to establish with clients. This chapter focuses on the most important concepts to help you develop your clinical judgment abilities. Completing the exercises will help you develop your skills.
Ethical reasoning
In clinical situations, nurses often face ethical dilemmas. Most nurses report facing ethical dilemmas in their work on a weekly basis. Examples include issues involving client choice, quality of life, and end-of-life decisions. A nurse frequently has to act in value-laden situations. For example, you may have clients who request abortions or who want “do not resuscitate” (DNR; “no code”) orders. Your decisions affect the client’s rights and the client’s quality of life. A willingness to comply with ethical and professional standards is a hallmark of a professional.
Yet, members of many professions have difficulty applying ethical principles to clinical care situations. When various professionals answered questions about ethical dilemmas presented to them, physician responses were correctly ethically based 49.2% of the time, nurse responses 46.3%, and adult citizens 40% (Johnson, 2005). Is being ethically correct less than half the time acceptable? Student practice in applying ethical principles is important. Although it is true that most agencies have ethics committees that often are the primary party involved with the client or family in resolving difficult ethical dilemmas, on many other occasions, you, the nurse, will be called on to make ethical decisions.
As nurses, we need to have a clear understanding of the ethics of the nursing profession. Nursing organizations have formally published ethical codes, such as those from American Nurses Association (ANA) or the Federation of European Countries (Sasso, 2008). Academic programs now include application to clinical practice in the curriculum.
Ethical theories and decision-making models
Ethical theories provide the bedrock from which we derive the principles that guide our decision making. There is no one “right” answer to an ethical dilemma: The decision may vary depending on which theory the involved people subscribe to. The following section briefly describes the most common models currently used in bioethics. They are, for the most part, representative of a Western European and Judeo-Christian viewpoint. As we become a more culturally diverse society, other equally viable viewpoints may become acculturated. This discussion focuses on three decision-making models: utilitarian/goal-based, duty-based, and rights-based models.
The utilitarian/goal-based model says that the “rightness” or “wrongness” of an action is always a function of its consequences. Rightness is the extent to which performing or omitting an action will contribute to the overall good of the client. Good is defined as maximum welfare or happiness. The rights of clients and the duties of a nurse are determined by what will achieve maximum welfare. When a conflict in outcome occurs, the correct action is the one that will result in the greatest good for the majority. An example of a decision made according to the goal-based model is forced mandatory institutionalization of a client with tuberculosis who refuses to take medicine to protect other members of the community. The client’s hospitalization produces the greatest balance of good over harm for the majority. Thus, “goodness” of an action is determined solely by its outcome.
The deontologic or duty-based model is person centered. It incorporates Immanuel Kant’s deontologic philosophy, which holds that the “rightness” of an action is determined by other factors in addition to its outcome. Respect for every person’s inherent dignity is a consideration. For example, a straightforward implication would be that a physician (or nurse) may never lie to a client. Do you agree? Decisions based on this duty-based model have a religious-social foundation. Rightness is determined by moral worth, regardless of the circumstances or the individual involved. In making decisions or implementing actions, the nurse cannot violate the basic duties and rights of individuals. Decisions about what is in the best interests of the client require consensus among all parties involved. Examples are the medical code “do no harm” and the nursing duty to “help save lives.”
The human rights–based model is based on the belief that each client has basic rights. Our duties as health care providers arise from these basic rights. For example, a client has the right to refuse care. Conflict occurs when the provider’s duty is not in the best interests of the client. The client has the right to life and the nurse has the duty to save lives, but what if the quality of life is intolerable and there is no hope for a positive outcome? Such a case might occur when a neonatal nurse cares for an infant with anencephaly (born without brain tissue in the cerebrum) in whom even the least invasive treatment would be extremely painful and would never provide any quality of life.
Ethical dilemmas arise when an actual or potential conflict occurs regarding principles, duties, or rights. Of course, many ethical or moral concepts held by Western society have been codified into law. Laws may vary from state to state, but a moral principle should be universally applied. Moral principles are shared by most members of a group, such as physicians or nurses, and represent the professional values of the group. Conflict arises when a nurse’s professional values differ from the law in her state of residence. Conflict may also arise when you have not come to terms with situations in which your personal values differ from the profession’s values. One example is doctor-assisted suicide (euthanasia). Legally, at the turn of the twenty-first century, such an act was legal in Oregon but illegal in Michigan. Professionally, the ANA Code of Ethics guides you to do no harm. Personally, your belief about whether euthanasia is right or wrong may be at variance with either of the above.
Bioethical Principles
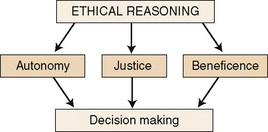
To practice nursing in an ethical manner, you must be able to recognize the existence of a moral problem. Once you recognize a situation that puts your client in jeopardy, you must be able to take action. Three essential, guiding ethical principles have been developed from the theories cited earlier. The three principles that can assist us in decision making are autonomy, beneficence (nonmaleficence), and justice (Figure 3-2).
Autonomy versus Medical Paternalism: Autonomy is the client’s right to self-determination. In the medical context, respect for a client’s autonomy is a fundamental ethical principle. It is the basis for the concept of informed consent, which means your client makes a rational, informed decision without coercion (Ebbesen & Pedersen, 2008). The medical profession went from having a paternalistic relationship with clients to letting them decide. In the past, nurses and physicians often made decisions for clients based on what they thought was best for the client. This paternalism sometimes discounted the wishes of clients and their families. The ethical concept of client autonomy has so strongly emerged as a client right in Western countries that aspects involved in an individual’s right to participate in medical decisions about his own care have become law.
This moral principle of autonomy means that each client has the right to decide about his or her health care. Clients who are empowered to make such decisions are more likely to comply with your treatment plan. Internal factors such as pain may interfere with a client’s ability to choose. External factors such as coercion by a care provider may also interfere. As a nurse, you and your employer must legally obtain the client’s permission for all treatment procedures. In the United States, under the Patient Self-Determination Act of 1991, all clients of agencies receiving Medicaid funds must receive written information about their rights to make decisions about their medical care. Nurses, as well as physicians, must provide clients with all the relevant and accurate information they need to make an “informed” decision whether they agree to treatments. The ANA states that it is the nurse’s responsibility to assist clients to make these decisions, as discussed in Chapter 2 (see Informed Consent section).
Many of the nursing theories incorporate concepts about autonomy and empowering the client to be responsible for self-care, so you may find this easy to accept as part of your nursing role. However, what happens if the client’s right to autonomy puts others at risk? Whose rights take precedence?
The concept of autonomy has also been applied to the way we practice nursing, but our professional autonomy has some limitations. For example, the American Medical Association’s Principles of Medical Ethics says a physician can choose whom to serve, except in an emergency; however, the picture is a little different in nursing practice. According to the ANA Committee on Ethics, nurses are ethically obligated to treat clients seeking their care. For example, you could not refuse to care for a client with AIDS who is assigned to you.
A nurse has autonomy in caring for a client, but this is somewhat limited because legally she must also follow physician orders and be subject to physician authority. Before the nurse or physician can override a client’s right to autonomy, he or she must be able to present a strong case for their point of view based on either or both of the following principles: beneficence and justice.
Beneficence and Nonmaleficence
Beneficence implies that a decision results in the greatest good or produces the least harm to the client. This is based on the Hippocratic Oath and its concept of “do no harm.” Avoiding actions that bring harm to another person is known as nonmaleficence. An example is the Christian belief of “do not kill,” which has been codified into law but has many exceptions (e.g., soldiers sent to war are expected to kill the enemy).
In health care, beneficence gives care providers the moral obligation to act at all times for the benefit of their clients. Again, nursing theorists have incorporated this into the nursing role, so you may find this easy to accept. Helping others may be why you chose to become a nurse. In nursing, you not only have the obligation to avoid harming your clients, but you also are expected to advocate for your clients’ best interests.
Beneficence is challenged in many clinical situations (e.g., requests for abortion or euthanasia). Currently, some of the most difficult ethical dilemmas involve situations where decisions may be made to withhold treatment. For example, decisions are made to justify such violations of beneficence in the guise of permitting merciful death. Is there a moral difference between actively causing death and withholding treatment, when the outcome for the client is the same death? There are clear legal differences. In most states, a health care worker who intentionally acts to cause a client’s death is legally liable.
Other challenges to beneficence occur when the involved parties hold different viewpoints about what is best for the client. Consider a case in which the family of an elderly, poststroke, comatose, ventilator-dependent client wants all forms of treatment continued, but the health care team doesn’t believe it will benefit the client. The initial step toward resolution may be holding a family conference and really listening to the viewpoints of family members, asking them whether the client ever expressed wishes verbally or in writing in the form of an advance directive. Maintaining a trusting, open, mutually respectful communication may help avoid an adversarial situation.
Justice
Justice is actually a legal term; however, in ethics, it refers to being fair or impartial. A related concept is equality (e.g., the just distribution of goods or resources, sometimes called social justice or distributive justice). Within the health care arena, this distributive justice concept might be applied to scarce treatment resources. As new and more expensive technologies that can prolong life become available, who has a right to them? Who should pay for them? If resources are scarce, how do we decide who gets them? Should a limited resource be spread out equally to everyone? Or should it be allocated based on who has the greatest need?
Unnecessary Treatment: Decisions made based on the principle of justice may also involve the concept of unnecessary treatment. Are all operations that are performed truly necessary? Why do some clients receive antibiotics for viral infections, when we know they do not kill viruses? Are unnecessary diagnostic tests ever ordered solely to document that a client does not have Condition X, just in case there is a malpractice lawsuit?
Social Worth: Another justice concept to consider in making decisions is that of social worth. Are all people equal? Are some more deserving than others? If a client Dan is 7 years old instead of 77 years old, and the expensive medicine would cure his condition, should these factors affect the decision to give him the medicine? If there is only one liver available for transplant today, and there are two equally viable potential recipients—Larry, age 54, whose alcoholism destroyed his own liver; or Kay, age 32, whose liver was destroyed by hepatitis she got while on a life-saving mission abroad—who should get the liver?
Veracity: Truthfulness is the bedrock of trust. And trust is an essential component of the professional nurse-client relationship. Not only is there a moral injunction against lying, but it is also destructive to any professional relationship. Generally, nurses would agree that a nurse should never lie to a client. However, there is controversy about withholding information from a client. We need clarity about truth telling. There will be times when we need to exercise some judgment about to whom to disclose information. We have an obligation to protect potentially vulnerable clients from information that would cause emotional distress. Although it is never acceptable to lie, nurses have evaded answering questions by saying, “You need to ask your physician about that.” Can you suggest another response?
Steps in ethical decision making
The process of moral reasoning and making ethical decisions has been broken down into steps. These steps are only a part of the larger model for critical thinking. Table 3-1 summarizes a model useful for nurses that was adapted from Lincourt’s model. This model covers the most essential parts of an ethical reasoning process. If you are the moral agent making this decision, you must be skillful enough to implement the actions in a morally correct way. Consider the following case.
TABLE 3-1
| Moral Component | Data | Evaluation |
| Claim | Clear statement of the claim or dilemma; issues and values are clearly identified | Are values of all parties represented? Who has a stake in the outcome? Are there any ethical conflicts between two or more values? |
| Evidence | Clarify the facts; list the grounds, statistics, and so on | Are they true? Relevant? Sufficient? |
| Warrant | Agency policy, professional standards of care, written protocols, legal precedents | Are they general? Are they appropriate? |
| Basis | Identify the moral basis for each individual’s claim; list backing, such as ethical principle of autonomy, beneficence, or justice | Is the backing recognizable? Impressively strong? |
| Rebuttal | List the benefit and the burdens; weigh them for each alternative in terms of possible consequences for each of the parties involved* | How strong and compelling is the rebuttal argument? Is the decision in accord with or in conflict with the law? |
*Benefits might include profit for one of the parties. Burden might include causing physical or emotional pain to one of the parties or imposing financial burden on them.
In deciding how to spend your limited time with these clients, do you base your decision entirely on how much good you can do for each client? Under distributive justice, what should happen when the needs of these four conflict? You could base your decision on the principle of beneficence and do the greatest good for the most clients, but this is a very subjective judgment. Would one of these clients benefit more from nursing care than the others?
In using ethical decision-making processes, nurses must be able to tolerate ambiguity and uncertainty. One of the most difficult aspects for the novice nurse to accept is that there often is no one “right” answer; rather, usually several options may be selected, depending on the person or situation.
Critical thinking
Critical thinking is an analytical process in which you purposefully use specific thinking skills to make complex clinical decisions. You are able to reflect on your own thinking process. We can paraphrase the American Philosophical Association definition, which considers critical thinking as a purposeful, self-regulating process of interpretation, analysis, evaluation, and inference for the purpose of making judgments (Worell & Profetto-McGrath, 2007).
Although no consensus has been reached on a critical thinking definition in the nursing arena, current definitions are similar (Ravert, 2008). Generally, we define critical thinking as the purposeful use of a cognitive framework to identify and analyze assumptions and evidence to recognize emergent client situations, make clear, objective clinical decisions, and intervene appropriately (Mangena & Chabeli, 2005; Wilgis & McConnell, 2008). It encompasses the steps of the nursing process, but possibly in a more circular loop than we usually envision the nursing process. Critical thinking allows the nurse to modify the care plan based on the client’s responses to her nursing interventions (Fero et al., 2009).
Critical thinking is more than just a cognitive process of following steps. It also has an affective component—the willingness to engage in self-reflective inquiry. As you learn to be a critical thinker, you improve and clarify your thinking process skills, so that you are more accurately able to solve problems based on available evidence. Although the cognitive skills can be taught, the affective willingness to use critical thinking process is an ingrained trait that may be difficult to change. Changing from a lecture method of nurse education to a learner-centered approach would have faculty “model” the critical thinking process for students.
Characteristics of a critical thinker
Critical thinkers are skilled at using inquiry methods. They approach problem solutions in a systematic, organized, and goal-directed way when making clinical decisions. They continually use past knowledge, communication skills, new information, and observations to make these clinical judgments. Table 3-2 summarizes the characteristics of a critical thinker.
TABLE 3-2
Characteristics of a Critical Thinker
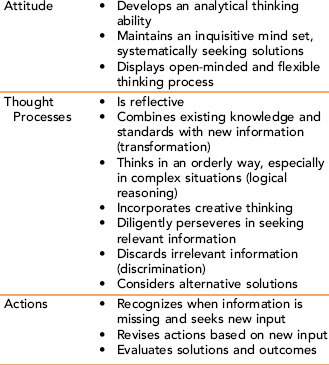
Based on information from Facione PA: Critical thinking: what is it and why it counts, Milbrae, CA, 2006, California Academic Press; Scheffer BK, Rubenfeld MG: A consensus statement on critical thinking in nursing, J Nurs Educ 39(8):352–359, 2000; and Worrell JA, Profetto-McGrath J: Critical thinking as an outcome of context-based learning among post RN students: a literature review, Nurse Educ Today 27:420–426, 2007.
Expert nurses recognize that priorities change continually, requiring constant assessment and alternative interventions. When the authors analyzed the decision-making process of expert nurses, they all used the critical thinking steps described in this chapter when they made their clinical judgments, even though they were not always able to verbally state the components of their thinking processes. Expert nurses organized each input of client information and quickly distinguished relevant from irrelevant information. They seemed to categorize each new fact into a problem format, obtaining supplementary data and arriving at a decision about diagnosis and intervention. Often, they commented about comparing this new information with prior knowledge, sometimes from academic sources but usually from information gained from preceptors. They constantly scan for new information, and constantly reassess their client’s situation. This is not linear. New input is always being added. This contrasts with novice nurses who tend to think in a linear way, collect lots of facts but not logically organize them, and fail to make as many connections with past knowledge. Novice nurses’ assessments are more generalized and less focused, and they tend to jump too quickly to a diagnosis without recognizing the need to obtain more facts.
Because nurses are responsible for a significant proportion of decisions that affect client care, and are key gatekeepers in preventing harm, employing agencies periodically retest staff nurses for competencies. This procedure was initially done just to retest or recertify technical skills, such as CPR. Now many agencies have added other competency testing, including evaluation of critical thinking/clinical judgment skills (Rush, 2008).
Barriers to thinking critically and reasoning ethically
Barriers that decrease a nurse’s ability to think critically, including attitudes such as “my way is better,” interfere with our ability to empower clients to make their own decisions. Our thinking habits can also impede communication with clients or families making complex bioethical choices. Examples include becoming accustomed to acknowledging “only one right answer” or selecting only one option. Behaviors that act as barriers include automatically responding defensively when challenged, resisting changes, and desiring to conform to expectations. Cognitive barriers, such as thinking in stereotypes, also interfere with our ability to treat a client as an individual.
Cognitive Dissonance
Cognitive dissonance refers to the mental discomfort you feel when there is a discrepancy between what you already believe and some new information that does not go along with your view. In this book, we use the term to refer to the holding of two or more conflicting values at the same time.
Personal Values versus Professional Values
We all have a personal value system developed over a lifetime that has been extensively shaped by our family, our religious beliefs, and our years of life experiences. Our values change as we mature in our ability to think critically, logically, and morally. Strongly held values become a part of self-concept. Our education as nurses helps us acquire a professional value system. In nursing school, as you advance through your clinical experiences, you begin to take on some of the values of the nursing profession (Box 3-1). You are acquiring these values as you learn the nursing role. The process of this role socialization is discussed in Chapter 7. For example, maintaining client confidentiality is a professional value, with both a legal and a moral requirement. We must take care that we do not allow our personal values to obstruct care for a client who holds differing values.
Values clarification and the nursing process
The nursing process offers many opportunities to incorporate values clarification into your care. During the assessment phase, you can obtain an assessment of the client’s values with regard to the health system. For example, you interview a client for the first time and learn that he has obstructive pulmonary disease and is having difficulty breathing, but he insists on smoking. Is it appropriate to intervene? In this example, you know that smoking is detrimental to a person’s health and you, as a nurse, find the value of health in conflict with the client’s value of smoking. It is important to understand your client’s values. When your values differ, you attempt to care for this client within his reality. He has the right to make decisions that are not always congruent with those of his health care providers (Bromley & Braslow, 2008).

The values people hold often are observed in their interest in, involvement with, and commitment to people, places, and things.
When identifying specific nursing diagnoses, it is important that your diagnoses are not biased. Examples of value conflicts might be spiritual distress related to a conflict between spiritual beliefs and prescribed health treatments, or ineffective family coping related to restricted visiting hours for a family in which full family participation is a cultural value. In the planning phase, it is important to identify and understand the client’s value system as the foundation for developing the most appropriate interventions. Plans of care that support rather than discount the client’s health care beliefs are more likely to be received favorably. Your interventions include values clarification as a guideline for care. You help clients examine alternatives. During the evaluation phase, examine how well the nursing and client goals were met while keeping within the guidelines of the client’s value system.
To summarize, in case of conflict (with own personal ethical convictions), nurses must put aside their own moral convictions to provide necessary assistance in a case of emergency when there is imminent risk to a patient’s life (Sasso, 2008). Ethical reasoning and critical thinking skills are essential competencies for making clinical judgments, in an increasingly complex health care system (Carter & Ruckholm, 2008). To apply critical thinking to a clinical decision, we need to base our intervention on the best evidence available. These skills can be learned by participating in simulated patient case situations. These skills will enable you to provide higher quality nursing care (Fero et al., 2009; Ravert, 2008).
Applications
Accrediting agencies for nursing curriculums require inclusion of critical thinking curriculum. Accepted teaching-learning methods for assessing critical thinking include case studies, questioning, reflective journalism, client simulations, portfolios, concept maps, and problem-based learning (Sorensen & Yankech, 2008; Wilgis & McConnell, 2008). As a nurse, you are faced with processing copious amounts of information to be considered before making a decision about your client’s situation. Often, you must consider more than one possibility but make your decision quickly. To provide safe care, you must be able to apply critical thinking skills to clinical situations (Fero et al., 2009; Rogal & Young, 2008).
Participation in clinical research
You or your clients may be called on at some time to participate in clinical research trials. The focus of this book is to examine ethical dilemmas faced in nursing practice, and this does not encompass the ethical aspect of conducting or participating in research studies. To examine what makes clinical research ethical, consult a nursing research book.
Solving ethical dilemmas in nursing
Nurses indicate a need for more information about dealing with the ethical dilemmas they encounter, yet most say they receive little education in doing so. Exercises 3-1 (autonomy), 3-2 (beneficence), and 3-3 (justice) give you this opportunity.
The ethical issues that nurses commonly face today can be placed in three general categories: moral uncertainty, moral or ethical dilemmas, and moral distress. Moral uncertainty occurs when a nurse is uncertain as to which moral rules (i.e., values, beliefs, or ethical principles) apply to a given situation. For example, should a terminally ill client who is in and out of a coma and chooses not to eat or drink anything be required to have IV therapy for hydration purposes? Does giving IV therapy constitute giving the client extraordinary measures to prolong life? Is it more comfortable or less comfortable for the dying client to maintain a high hydration level? When there is no clear definition of the problem, moral uncertainty develops, because the nurse is unable to identify the situation as a moral problem or to define specific moral rules that apply. Strategies that might be useful in dealing with moral uncertainty include using the values clarification process, developing a specific philosophy of nursing, and acquiring knowledge about ethical principles.
Ethical or moral dilemmas arise when two or more moral issues are in conflict. An ethical dilemma is a problem in which there are two or more conflicting but equally right answers. Organ harvesting of a severely brain-damaged infant is an example of an ethical dilemma. Removal of organs from one infant may save the lives of several other infants. However, even though the brain-damaged child is definitely going to die, is it right to remove organs before the child’s death? It is important for the nurse to understand that, in many ethical dilemmas, there is often no single “right” solution. Some decisions may be “more right” than others, but often what one nurse decides is best differs significantly from what another nurse would decide.
The third common kind of ethical problem seen in nursing today is moral distress. Moral distress results when the nurse knows what is “right” but is bound to do otherwise because of legal or institutional constraints. When such a situation arises (e.g., a terminally ill client who does not have a “do not resuscitate” medical order and for whom, therefore, resuscitation attempts must be made), the nurse may experience inner turmoil.
Nurses in the National Rural Bioethics Project reported that three of their most commonly encountered ethics problems had to do with resuscitation decisions for dying clients with unclear, confusing, or no code orders; patients and families who wanted more aggressive treatment; and colleagues who discussed clients inappropriately.
Because values underlie all ethical decision making, nurses must understand their own values thoroughly before making an ethical decision. Instead of responding in an emotional manner on the spur of the moment (as people often do when faced with an ethical dilemma), the nurse who uses the values clarification process can respond rationally. It is not an easy task to have sufficient knowledge of oneself, of the situation, and of legal and moral constraints to be able to implement ethical decision making quickly. Expert nurses still struggle. Taking time to examine situations can help you develop skill in dealing with ethical dilemmas in nursing, and the exercises in this book will give you a chance to practice. Each chapter in this book has also included at least one ethical dilemma, so you can discuss what you would do.
Finally, in thinking about your own ethical practice, reflect on how important it is for your client to be able to always count on you. Consider the following client journal entry (Milton, 2002):
Professional values acquisition
Professional values or ethics consist of the values held in common by the members of a profession. Professional values are formally stated in professional codes. One example is the ANA Code of Ethics for Nurses. Often, professional values are transmitted by tradition in nursing classes and clinical experiences. They are modeled by expert nurses and assimilated as part of the role socialization process during your years as a student and new graduate. Professional values acquisition should perhaps be the result of conscious choice by a nursing student. This is the first step in values acquisition. Can you apply it to your own life? It may also help you understand the value system of your clients. Refer to Box 3-2 for the seven criteria for aquisition of a value.
Values are a strong determinant in making selections between competing alternatives. Consider whether the nursing profession holds values regarding the following situation: What if you observed a nurse charting that a medicine was given to a client when you know it was not? What professional value should guide your response? Exercise 3-4 will give you an opportunity to practice explaining which of your choices are based on the profession’s values.
Applying critical thinking to the clinical decision-making process
This section discusses a procedure for developing critical thinking skills as applied to solving clinical problems. Different examples illustrate the reasoning process developed by several disciplines. Unfortunately, each discipline has its own vocabulary. Table 3-3 shows that we are talking about concepts with which you are already familiar. It also contrasts terms used in education, nursing, and philosophy to specify 10 steps to help you develop your critical thinking skills. For example, the nurse performs a “client assessment,” which in education is referred to as “collecting information” or in philosophy may be called “identifying claims.”
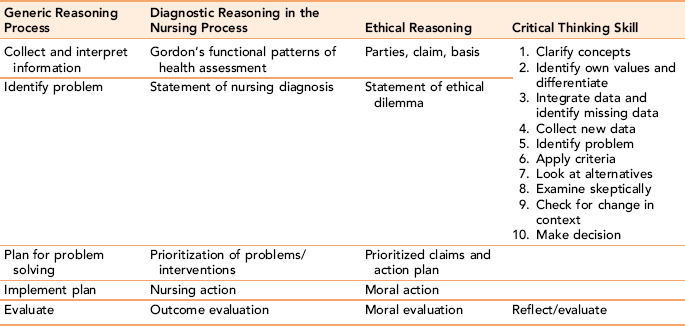
The process of critical thinking is systematic, organized, and goal directed. As critical thinkers, nurses are able to explore all aspects of a complex clinical situation (Worrell & Profetto-McGrath, 2007). This is a learned process. Among many teaching-learning techniques helping you develop critical thinking skills, most are included in this book: reflective journaling, concept maps, role-playing, guided small group discussion, and case study discussion. An extensive case application follows. During your learning phase, the critical thinking skills are divided into 10 specific steps. Each step includes a discussion of application to the clinical case example provided.
To help you understand how to apply critical thinking steps, read the following case and then see how each of the steps can be used in making clinical decisions. Components of this case are applied to illustrate the steps and stimulate discussion in the critical thinking process; many more points may be raised. From the outset, understand that, although these are listed as steps, they do not occur in a rigid, linear way in real life. The model is best thought of as a circular model. New data are constantly being sought and added to the process.
Step 1: Clarify concepts
The first step in making a clinical judgment is to identify whether a problem actually exists. Poor decision makers often skip this step. To figure out whether there is a problem, you need to think about what to observe and what basic information to gather. If it is an ethical dilemma, you not only need to identify the existence of the moral problem, but you need to also identify all the interested parties who have a stake in the decision. Figuring out exactly what the problem or issue is may not be as easy as it sounds.
Case Discussion
This case is designed to present both physiologic and ethical dilemmas. In clarifying the problem, address both domains.
• Physiological concerns: Based on the diagnosis, the initial treatment goal was to restore homeostasis. By Day 5, is it clear whether Mrs. Vlios’s condition is reversible?
• Ethical concerns: When is a decision made to initiate treatment or to abide by the advance directive and respect the client’s wishes regarding no treatment?
• What are the wishes of the family? What happens when there is no consensus?
• Assumptions: Is the diagnosis correct? Does the client have dementia? Or was her confusion a result of dehydration and a strange hospital environment?
Step 2: Identify your own values
Values clarification helps you identify and prioritize your values. It also serves as a base for helping clients identify the values they hold as important. Unless you are able to identify your client’s values and can appreciate the validity of those values, you run the risk for imposing your own values. It is not necessary for your values and your client’s values to coincide; this is an unrealistic expectation. However, whenever possible, the client’s values should be taken into consideration during every aspect of nursing care. Discussion of the case of Mrs. Vlios presented in this section may help you with the clarification process.
Having just completed the exercises given earlier should help your understanding of your own personal values and the professional values of nursing. Now apply this information to this case.
Case Discussion
Identify the values of each person involved:
• Family: Mrs. Vlios signed an advance directive. Sara wants it adhered to; Todos wants it ignored. Why? (Missing information: Are there religious beliefs? Is there unclear communication? Is there guilt about previous troubles in the relationship?)
• Personal values: What are yours?
• Professional values: The ANA says nurses are advocates for their clients; beneficence implies nonmaleficence (“do no harm”), but autonomy means the client has the right to refuse treatment. What is the agency’s policy? What are the legal considerations? Practice refining your professional values acquisition by completing the values exercises in this chapter.
In summary, you need to identify which values are involved in a situation or which moral principles can be cited to support each of the positions advocated by the involved individuals.
Step 3: Integrate data and identify missing data
Think about knowledge gained in prior courses and during clinical experiences. Try to make connections between different subject areas and clinical nursing practice.
• Identify what data are needed. Obtain all possible information and gather facts or evidence (evaluate whether data are true, relevant, and sufficient). Situations are often complicated. It is important to figure out what information is significant to this situation. Synthesize prior information you already have with similarities in the current situation. Conflicting data may indicate a need to search for more information.
• Compare existing information with past knowledge. Has this client complained of difficulty thinking before? Does she have a history of dementia?
• Look for gaps in the information. Actively work to recognize whether there is missing information. Was Mrs. Vlios previously taking medications to prevent depression? For a nurse, this is an important part of critical thinking.
• Collect information systematically. Use an organized framework to obtain information. Nurses often obtain a client’s history by asking questions about each body system. They could just as systematically ask about basic needs.
• Organize your information. Clustering information into relevant categories is helpful. For example, gathering all the facts about a client’s breathing may help focus your attention on whether the client is having a respiratory problem. In your assessment, you note rate and character of respirations, color of nails and lips, use of accessory muscles, and grunting noises. At the same time, you exclude information about bowel sounds or deep tendon reflexes as not being immediately relevant to his respiratory status. Categorizing information also helps you notice whether there are missing data. A second strategy that will help you organize information is to look for patterns. It has been indicated that experienced nurses intuitively note recurrent meaningful aspects of a clinical situation.
Case Discussion
Rely on prior didactic knowledge or clinical experience. Cluster the data. What was Mrs. Vlios’s status immediately before hospitalization? What was her status at the time of hospitalization? What information is missing? What additional data do you need?
• Physiology: Consider pathophysiologic knowledge about the effects of hypovolemia and electrolyte imbalances on the systems such as the brain, kidneys, and vascular system. What is her temperature? What are her laboratory values? What is her 24-hour intake and output? Is she still dehydrated?
• Psychological/cognitive: How does hospitalization affect older adults? How do restraints affect them?
• Social/economic: Was weight loss a result of dehydration? Why was she without food? Could it be due to economic factors or mental problems?
• Legal: What constitutes a binding advance directive in the state in which Mrs. Vlios lives? Is a living will valid in her state, or does the law require a health power of attorney? Are these documents on file at the hospital?
Step 4: Obtain new data
Critical thinking is not a linear process. Expert nurses often modify interventions based on the response to the event, or change in the client’s physical condition (Fero et al., 2008). Constantly consider whether you need more information. Establish an attitude of inquiry and obtain more information as needed. Ask questions; search for evidence; and check reference books, journals, the ethics sources on the Internet, or written professional or agency protocols.
Evaluate conflicting information. There may be time constraints. If a client has suspected “respiratory problems,” you may need to set priorities. Obtain data that are most useful or are easily available. It would be useful to know oxygenation levels, but you may not have time to order laboratory tests. But perhaps there is a device on the unit or in the room that can measure oxygen saturation.
Sometimes you may need to change your approach to improve your chances of obtaining information. For example, when the charge nurse caring for Mrs. Vlios used an authoritarian tone to try to get the sister and brother to provide more information about possible drug overdose, they did not respond. However, when the charge nurse changed his approach, exhibiting empathy, the daughter volunteered that on several occasions her mother had forgotten what pills she had taken.
Step 5: Identify the significant problem
• Analyze existing information: Examine all the information you have. Identify all the possible positions.
• Make inferences: What might be going on? What are the possible diagnoses? Develop a working diagnosis.
• Prioritize: Which client problem is most urgently in need of your intervention? What are the appropriate interventions?
Case Discussion
A significant physiologic concern is sepsis, regardless of whether it is an iatrogenic (hospital-acquired) infection or one resulting from immobility and debilitation. A significant ethical concern is the conflict among family members and client (as expressed through her living will). At what point do spiritual concerns take priority over a worsening physical concern?
Step 6: Examine skeptically
Thinking about a situation may involve weighing positive and negative factors, and differentiating facts that are credible from opinions that are biased or not grounded in true facts.
• Challenge your own assumptions.
• Consider whether any of your assumptions are unwarranted. Does the available evidence really support your assumption?
• Discriminate between facts and inferences. Your inferences need to be logical and plausible, based on the available facts.
In trying to evaluate a situation, consciously raising questions becomes an important part of thinking critically. At times there will be alternative explanations or different lines of reasoning that are equally valid. The challenge is to examine your own and others’ perspectives for important ideas, complicating factors, other plausible interpretations, and new insights. Some nurses believe that examining information skeptically is part of each step in the critical thinking process rather than a step by itself.
Case Discussion
Challenge assumptions about the cause of Mrs. Vlios’s condition. For example, did you eliminate the possibility that she had a head injury caused by a fall? Could she have liver failure as a result of acetaminophen overdosing? Have all the possibilities been explored? Challenge your assumptions about outcome: Are they influenced by expected probable versus possible outcomes for this client? If she, indeed, has irreversible dementia, what will the quality of her life be if she recovers from her physical problems?
Step 7: Apply criteria
In evaluating a situation, think about appropriate responses.
• Laws: There may be a law that can be applied to guide your actions and decisions. For example, by law, certain diseases must be reported to the state. If you suspect physical abuse, there is a state statute that requires professionals to report abuse to the Department of Social Services.
• Legal precedents: There may have been similar cases or situations that were dealt with in a court of law. Legal decisions do guide health care practices. In end-of-life decisions, when there is no legally binding health care power of attorney, the most frequent hierarchy is the spouse, then the adult children, then the parents.
• Protocols: There may be standard protocols for managing certain situations. Your agency may have standing orders for caring for Mrs. Vlios if she develops respiratory distress, such as administering oxygen per face mask at 5 L/min.
Case Discussion
Many criteria could be used to examine this case, including the Nurse Practice Act in the area of jurisdiction, the professional organization code of ethics or general ethical principles of beneficence and autonomy, the hospital’s written protocols and policies, state laws regarding living wills, and prior court decisions about living wills. Remember that advance directives are designed to take effect only when clients become unable to make their own wishes known.
Step 8: Generate options and look at alternatives
• Evaluate the major alternative points of view.
• Involve experienced peers as soon as you can to assist you in making your decision.
• Use clues from others to help you “put the picture together.”
• Can you identify all the arguments—pro and con—to explain this situation? Almost all situations will have strong counterarguments or competing hypotheses.
Case Discussion
The important concept is that neither the physician nor the nurse should handle this alone; rather, others should be involved (e.g., the hospital bioethics committee, the ombudsman client representative, the family’s spiritual counselor, and other medical experts such as a gerontologist, psychologist, and nursing clinical specialist).
Step 9: Consider whether factors change if the context changes
Consider whether your decision would be different if there were a change in circumstances. For example, a change in the age of the client, in the site of the situation, or in the client’s culture may affect your decision. A competent nurse prioritizes which aspects of the situation are most relevant and can modify her actions based on the client’s response (Fero et al., 2009).
Case Discussion
If you knew the outcome from the beginning, would your decisions be the same? What if you knew Mrs. Vlios had a terminal cancer? What if Mrs. Vlios had remained in her senior housing project and you were the home health nurse? What if Mrs. Vlios had remained alert during her hospitalization and refused IVs, hyperalimentation, nasogastric tubes, and so on? What if the family and Mrs. Vlios were in agreement about no treatment? Would you make more assertive interventions to save her life if she were 7 years old, or a 35-year-old mother of five young children?
Step 10: Make the final decision
After analyzing available information in this systematic way, you need to make a judgment or decision. An important part of your decision is your ability to communicate it coherently to others and to reflect on the outcome of your decision for your client.
The critical thinker needs to be able to accept that there may be multiple solutions that can be equally acceptable. In other situations, you may need to make a decision even when there is incomplete knowledge. Be able to cite your rationale or present your arguments to others for your decision choice and interventions.
After you implement your interventions, examine the client outcomes. Was your assessment correct? Did you obtain enough information? Did the benefits to the client and family outweigh the harm that may have occurred? In retrospect, do you know you made the correct decision? Did you anticipate possibilities and complications correctly? This kind of self-examination can foster self-correction. It is this process of reflecting on one’s own thinking that is the hallmark of a critical thinker.
Summarizing the critical thinking learning process
The most effective method of learning these steps in critical thinking results from repeatedly applying them to clinical situations. This can occur in your own clinical care. A new graduate nurse must, at a minimum, be able to identify essential clinical data, know when to initiate interventions, know why a particular intervention is relevant, and differentiate between problems that need immediate intervention versus problems that can wait for action. Repeated practice in applying critical thinking can help a new graduate fit into the expectations of employers.
Students have demonstrated that critical thinking can be learned in the classroom, as well as through clinical experience. Effective learning can occur when opportunities are structured that allow for repeated in-class applications to client case situations. This includes using real-life case interviews with experienced nurses, which allow you to analyze their decision-making process. The interview and analysis of an expert nurse’s critical thinking described in Exercise 3-5 explains how this is done using a 10-minute recording.
You may also help increase your critical thinking and clinical problem-solving skills by discussing the following additional case example. Remember that most clinical situations requiring decision making will not involve the types of ethical dilemmas discussed earlier in this chapter.
Summary
Critical thinking is the ability to think about your thinking. It is not a linear process. Analysis of the thinking processes of expert nurses reveals that they continually scan new data and simultaneously apply these steps in clinical decision making. They monitor the effectiveness of their interventions in achieving desired outcomes for their client. A nurse’s values and critical thinking abilities often have a profound effect on the quality of care given to a client, even affecting client mortality outcomes. Functioning as a competent nurse requires that you have knowledge of medical and nursing content, an accumulation of clinical experiences, and an ability to think critically. Almost daily, we confront ethical dilemmas and complicated clinical situations that require expertise as a decision maker. We can follow the 10 steps of the critical thinking process described in this chapter to help us respond to such situations. Developing skill as a critical thinker is a learned process, one requiring repeated opportunities for application to clinical situations. Reflecting on one’s own thinking about case example situations provided in this chapter can assist such learning.
References
Bromley, E., Braslow, J.Y. Teaching critical thinking in psychiatric training: a role for the social sciences. Am J Psychiatry. 2008;165(11):1396–1401.
Carter, L.M., Rukholm, E. A study of critical thinking, teacher-student interaction, and discipline-specific writing in an online educational setting for registered nurses. J Contin Educ Nurs. 2008;39(3):133–138.
Ebbesen, M., Pedersen, B.D. The principle of respect for autonomy—concordant with the experience of oncology physicians and molecular biologists in their daily work? BMC Med Ethics. 2008;9:5.
Facione, P.A. Critical thinking: what is it and why it counts. Milbrae, CA: California Academic Press, 2006.
Fero, L.J., Witsberger, C.M., Wesmiller, S.W., et al. Critical thinking ability of new graduate and experienced nurses. J Adv Nurs. 2009;65(1):139–148.
Johnson, P. US journalists fare well on test of ethics, study finds. USA Today. 2005:5D. [February 2].
Mangena, A., Chabeli, M.M. Strategies to overcome obstacles in the facilitation of critical thinking in nursing education. Nursing Education Today. 2005;25:291–298.
Milton, C. Ethical implications for acting faithfully in nurse-person relationships. Nurs Sci Q. 2002;15:21–24.
Ravert, P. Patient simulator sessions and critical thinking. J Nurs Educ. 2008;47(12):557–562.
Rogal, S.M., Young, J. Exploring critical thinking in critical care nursing education: a pilot study. J Contin Educ Nurs. 2008;39(1):28–33.
Rush, K.L., Dyches, C.E., Waldrop, S., et al. Critical thinking among RN-to-BSN distance students participating in human patient simulation. J Nurs Educ. 2008;47(11):501–507.
Sasso, L. Federazione Europea delle Profeessioni Infermieristiche Action Plan 2007, 2008.
Sasso, L., Stievano, A., Jurado, M.G., et al. Code of ethics and conduct for European nursing. Nurs Ethics. 2008;15(6):821–836.
Sorensen, H.A., Yankech, L.R. Precepting in the fast lane: improving critical thinking in new graduate nurses. J Contin Educ Nurs. 2008;39(5):208–216.
Stokowski, L.A. Ethical dilemmas for healthcare professionals: can we avoid influenza? Medscape Infectious Diseases. 2009:1–7.
Wilgis, M., McConnell, J. Concept mapping: an educational strategy to improve graduate nurses’ critical thinking skills during a hospital orientation program. J Contin Educ Nurs. 2008;39(3):119–126.
Worrell, J.A., Profetto-McGrath, J. Critical thinking as an outcome of context-based learning among post RN students: a literature review. Nurse Educ Today. 2007;27:420–426.