Self-Concept in the Nurse-Client Relationship
At the end of the chapter, the reader will be able to:
2 Describe the features of and functions of self-concept.
3 Identify theoretical models of the self and self-concept.
4 Discuss Erikson’s theory of psychosocial ego development.
5 Identify functional health patterns and nursing diagnosis related to self-concept pattern disturbances.
6 Apply the nursing process to the nursing diagnosis of body image disturbance.
7 Apply the nursing process to the nursing diagnosis of personal identity disturbance.
8 Apply the nursing process to the nursing diagnosis of self-esteem disturbance.
9 Apply the nursing process to the nursing diagnosis of spiritual distress.
This chapter explores self-concept as a key informant of behavior in human interaction and nurse-client relationships. The chapter describes theoretical frameworks for how self-concept develops. The Applications section discusses body image, personal identity, spirituality, and self-esteem as important clinical components of self-concept and applies the nursing process to self-concept disturbances. The key role of self-concept in nurse-client relationships is explored.
Basic concepts
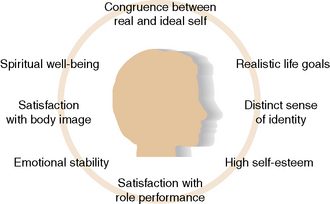
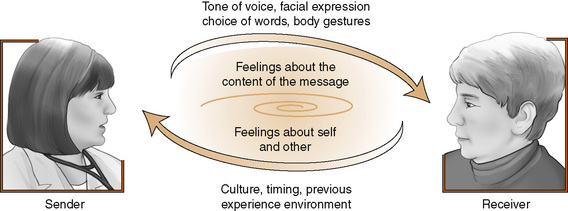
Self-concept is an integral component of nurse-client relationships. It is a difficult idea to conceptualize due to its many facets and abstract nature. Figure 4-1 identifies aspects that are relevant to an appreciation of the self-concept’s role in communication. The nursing diagnosis Association (NANDA International, 2009) recognizes self-concept pattern disturbances as approved nursing diagnoses. A healthy self-concept reflects attitudes, emotions and values that are realistically consistent with meaningful purposes in life and satisfying to the individual. A well-differentiated sense of personal identity permits the self-as-knower to experience a feeling of distinctness from others and a sense of sameness through time (Konig, 2009).
Definition
Self-concept refers to an acquired set of thoughts, feelings, attitudes, and beliefs that individuals have about the nature and organization of their personality. Cunha and Goncalves (2009) refer to the self as an open system, which is fluid and dynamic. Like fingerprints, no two self-concepts are exactly alike. Self-concepts help people experience who they are and what they are capable of becoming physically, emotionally, intellectually, socially, and spiritually in relationship or community with others. McCormick & Hardy (2008) state, “identity, the definition of one’s self, is the heart of one’s life” (p. 405). Consciousness of one’s personal identity allows a person to make authentic choices and maintain well-developed personal boundaries in relationships with others.
Self-concepts create and reflect our personal reality and worldview. The four aspects of self-concept—physical, cognitive, emotional, and spiritual—represent the holistic self, and are important determinants of behavior. Different aspects of self become more prominent, depending on the particular situation in which people find themselves (Prescott, 2006). From a patient-centered health care perspective, relevant self-concept patterns include body image (physical), personal identity (cognitive and perceptual awareness), self-esteem (emotional valuing), and spirituality (connectivity with a higher purpose or God).
Features and functions of self-concept
Self-concept is an active, rather than static source of information about the self. Hunter (2008) suggests, “As one ages, the ‘self’ develops and becomes a more and more unique entity formed by personal experiences and personally developed values and beliefs” (p. 318). Self-concept is not necessarily a unified concept. It consists of multiple self-images, some of which may not match with each other or be supportive of the whole. For example, a star athlete can be a marginal student. Which is the true self-image, or are both valid? One can think of self-concept basically as the response to the question, “Who am I?” (Exercise 4-1).
Self-concepts provide important bridges to meaning. They help individuals make personal sense of their past, as it relates to the present and as it might be in the future (Lee & Oyserman, 2009). Personal decisions congruent with self-concept affirm the sense of self-identity, whereas those that are not consistent with important self-concepts create doubt and uncertainty.
Possible Selves
Possible selves is a term used to explain the future-oriented component of self-concept. Future expectations are important variables in goal setting and motivation (Lee & Oyserman, 2009). For example, a nursing student might think, “I can see myself becoming a nurse practitioner.” Such thoughts help the novice nurse work harder to achieve professional goals. Blazer (2008) suggests self-perceptions of personal health and well-being may be as important as objective data for predicting health outcomes over time. Communication can provide important support for exploring positive possibilities for personal identity and for helping clients reframe or avoid the establishment of negative possible selves.
Negative concepts of possible selves can become a self-fulfilling prophecy (Markus & Nurius, 1986). For example, Martha receives a performance evaluation indicating a need for improved self-confidence. Viewing the criticism as a negative commentary on her “self,” she performs awkwardly and freezes when asked questions in the clinical area.
Self-Concept/Environment Relationships
The social environment plays an important role in shaping a person’s self-concept. Set factors such as poverty, dysfunctional parenting styles, loss of a parent, lack of educational opportunities, and level of parental literacy contribute to negative self-concepts. A stable home environment, sports, academic success, professional opportunities, praise for successful accomplishments, and supportive parents and mentors help to foster positive self-concepts. Reflective appraisals refer to the personalized messages received from others that help shape self-concepts and contribute to self-evaluations (Hybels & Weaver, 2008).
Understanding the interplay between person and environment in explaining self-concept has important implications for the nurse-client relationship. It is a reciprocal relationship in which the nurse’s perceptions of self and other limit or enhance communication, and support or diminish a client’s sense of self-esteem. Identity (self-concept) is carved out from personal experiences of life, and forms the basis for behavioral expression and interpersonal reactions to the environment. A well-defined, accurate self-concept allows nurses to effectively communicate in most situations.
Self-awareness for nurses is just as critical as it is for clients. Although cognitive awareness of the self-concept is never fully complete, the Johari Window (Luft & Ingham, 1955) provides a disclosure/feedback model to help people learn more about their self-concept. The model consists of four areas:
• Open self (arena): what is known to self and others
• Blind self: what is known by others, but not by self
• Hidden self (façade): what is known by self, but not by others
• Unknown self: what is unknown to self and also unknown to others
The larger the open self box is, the more one knows about oneself and the more flexibility there is to realistically interpret and constructively cope with challenging health situations. Increasing the open area through asking for and receiving feedback (decreasing blind self), and using self-disclosure (decreasing the hidden self) leads to more authentic self-awareness. Decreasing the level of unknown area through self-discovery, new observations by others, and mutual illumination of experiences increases the open area.
The basic goal of any constructive relationship is to help the participants enlarge self-knowledge and enhance their potential by integrating disowned, neglected, unrecognized, or unrealized parts of the self into the personality. Expected outcomes include enhanced self-esteem, greater productivity, and increased personal satisfaction.
Theoretical models of self concept
William James (1890) was among the first theorists to address the self-concept as an important idea in psychology. He makes a distinction between “the I and the me: the I is equated with the self-as-knower and the me is equated with the self-as-known” (Konig, 2009, p. 102). James believed that a person has as many different social selves as there are distinct groups of persons about whose opinion he or she cares.
George Mead approaches the self from a sociologic perspective, emphasizing the influence of culture, moral norms, and language in framing self-concepts through interpersonal interactions (symbolic interactionism). The self affects and is influenced by how people experience themselves in relation to others (Elliott, 2008).
Any threat to the self-system creates anxiety. Freud’s ego defense mechanisms help explain how a person unconsciously protect the self against full awareness of potential and actual threats (see Chapter 20).
The self is a central construct in humanistic and psychodynamic theories of personality. Carl Rogers (1951) defined the self as “an organized, fluid, but consistent conceptual pattern of perceptions of characteristics and relationships or the ‘I’ or the ‘me’ together with values attached to these concepts” (p. 498).
Harry Stack Sullivan (1953) believed that self-concepts begin in infancy. He referred to each person’s self-images as a self-system that people develop to help them in the following ways: (1) develop a consistent image of self, (2) protect themselves against feeling anxiety, and (3) maintain their interpersonal security. Sullivan asserted that the self develops out of social interactions with others, most notably the mother. During early childhood, people develop self-personifications of a good me (resulting from reward and approval experiences), a bad me (resulting from punishment and disapproval experiences), and a not me (resulting from anxiety-producing experiences that are dissociated by the person as not being a part of their self-concept). Therapeutic interpersonal interactions can correct and build a different sense of self.
Erikson’s theory of psychosocial development
Erik Erikson (1968, 1982) believed that personality develops and becomes more complex as a person recognizes and responds to evolving developmental challenges (psychosocial crises) that occur with regularity throughout the life cycle. If individuals receive encouragement and support, they are more likely to master each psychosocial challenge and move successfully into the next stage of ego development with a strong sense of self.
The first four stages of Erikson’s psychosocial model of development serve as building blocks for the central developmental task of establishing a healthy ego identity (identity vs. identity diffusion). Working through the remaining stages of ego development refines and expands the ego identity established in late adolescence.
Successful resolution of developmental tasks in adulthood includes finding a meaningful occupation, establishing committed relationships and starting a family, contributing to the welfare of family and others, and sharing one’s wisdom with the larger community. A well-lived life results in a sense of integrity about oneself and one’s life at life’s closing chapter. Failure to master previous developmental stages can leave a person feeling despair and regret. Mastering psychosocial tasks successfully throughout the life cycle helps people feel a sense of integrity and enthusiasm about the life they have led, with few regrets, even when confronting death. Failure to successfully complete tasks associated with a developmental stage results in a reduced capacity to effectively negotiate later stages and a weakened sense of self. Erikson believed that stage development is never final. People have the potential to successfully rework developmental stages at a later time.
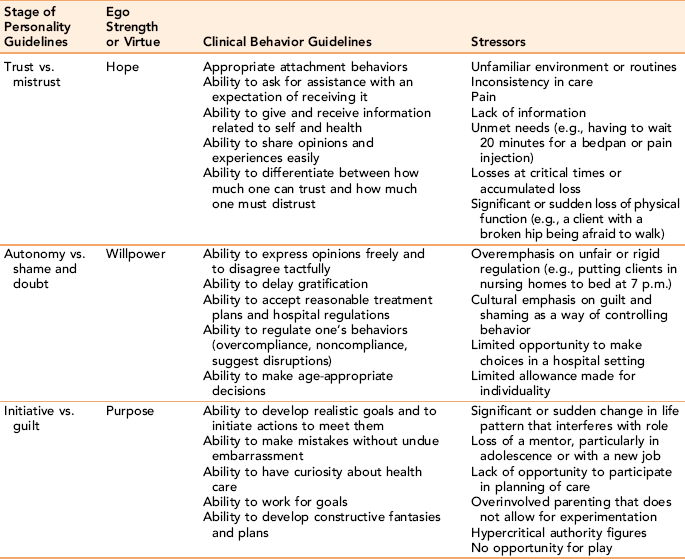
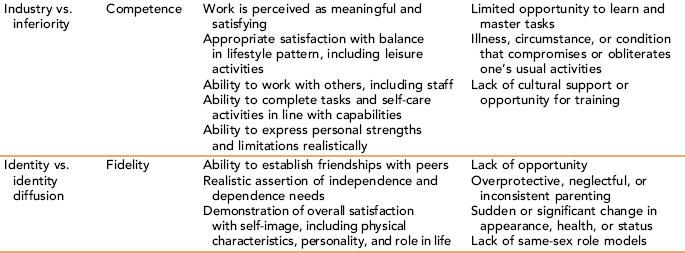
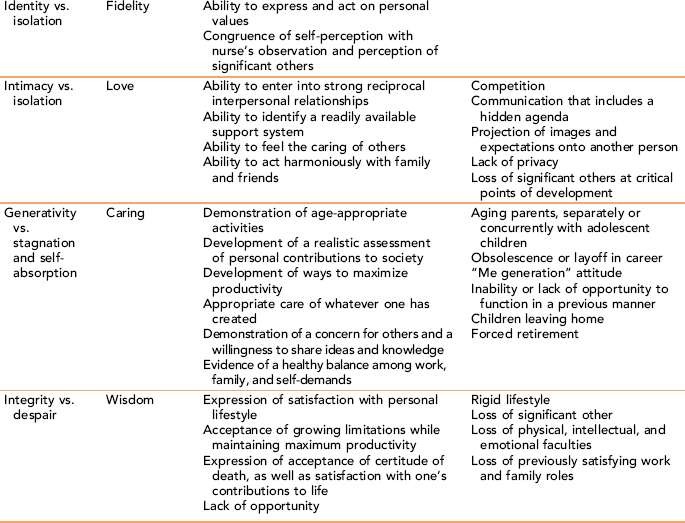
Erikson’s stages of ego development are outlined in Table 4-1. Nurses use Erikson’s model as an important part of client assessment. Analysis of behavior patterns using this framework can identify age-appropriateness or arrested ego identity development. Exercise 4-2 focuses on applying Erikson’s concepts to client situations.
Applications
Self-concept as a nursing diagnosis
The self-concept is an essential starting point for understanding the behavior of clients in nurse-client relationships. Serious injury or illness inevitably challenges self-concept. As a person’s perception of inner self-coherence is disturbed, the future becomes uncertain and unpredictable (Ellis-Hill & Horn, 2000). The following case example illustrates the extent of challenge.
Four aspects of self-concept are particularly relevant to consider in nurse-client relationships: body image, personal identity, self-esteem, and spirituality. These issues are addressed in Gordon’s (2007) functional health patterns under self-perception, self-concept patterns, and value-belief patterns. North American Nursing Diagnosis Association (NANDA International, 2009). Relevant to self-concept are nursing diagnoses related to body image, human dignity, personal identity, powerlessness, self-concept, and self-esteem. Disturbances in self-concept directly and indirectly influence role relationships, as discussed in Chapter 7.
Body image
Body image is the physical dimension of self-concept. Our body image changes throughout life, influenced by the process of aging, the appraisals of others, cultural and social factors, and physical changes resulting from illness or injury.
Physical appearance and body image are not necessarily the same. Body image refers to how people perceive their physical characteristics. For example, individuals with an eating disorder may see themselves as a “fat” person despite being dangerously underweight.
The value individuals place on body image reflects sociocultural norms and media presentations. Different cultures characterize similar physical characteristics as positive and others as negative. In the United States, a trim figure for women and a lean, muscular body for men are admired (Vartanian, 2009). In other cultures, obesity may be viewed as a sign of prosperity, fertility, or the ability to survive (Boston Women’s Health Book Collection, 1998).
Body image is closely intertwined with personal identity such that any change in body function or physical appearance can affect personal identity and challenge a person’s self-esteem. Hair loss with chemotherapy, moon face with high doses of prednisone, stroke limitations, removal of a breast or limb, burns, and loss of energy can all affect body image.
Physical appearance influences how people respond to a person (Rhode, 2009). Physically attractive people, appropriately dressed, and well groomed typically command more positive attention than those who are not. Individuals who deviate significantly from the norm in height, weight, or physical characteristics, and those who look considerably older or younger than their chronologic age often suffer discrimination (Williams, 2009). They speak of receiving subtle inequities, of being treated differentially, and as having intellectual and character shortcomings attributed to them solely on the basis of appearance.
Disturbances in body image can be long lasting. In a study of overweight adolescents, a primary theme that emerged was “a forever knowing of self as overweight” (Smith & Perkins, 2008).
Hidden body image disturbances
Although most people think of body image as describing visible differences in physical characteristics, subtle differences related to loss of body function apply. Medical conditions such as traumatic brain injury, infertility, impotence, loss of bladder or bowel function, and reliance on mechanical devices such as dialysis and pacemakers can create unseen body image disturbances. Loss of energy from cancer treatments can change a person’s self-image as a person with zest and vigor, to one who is frail and vulnerable.
Alteration in control and loss of sensation also represent body image disturbance. Clients in pain from fibromyalgia and those subject to seizures, alcoholism, cardiac arrhythmias, or diabetic fluctuations in blood sugar may exhibit few obvious physical changes, but they can experience similar feelings of insecurity and uncertainty about their body image.
Assessment Strategies: The meaning of body image is an important dimension to assess as it differs from person to person. Some, like Ray Charles or Christopher Reeves frame a negative body image as a positive feature of who they are. Others let a physical deviation become their only defining feature.
Assessment data supportive of a nursing diagnosis related to a self-concept disturbance in body image might include one or more of the following behaviors:
• Verbal expression of negative feelings about the body
• No mention of changes in body structure and function, or preoccupation with changed body structure or function
• Reluctance to look at or touch a changed body structure
• Social isolation and loss of interest in friends after a change in body structure, appearance, or function
• Physical changes usually require significant psychosocial and role performance adjustment (Drench, Noonan, Sharby, & Ventura, 2006); a comprehensive assessment should include the client’s strengths and limitations, expressed needs and goals, the nature and accessibility of the client’s support oonansystem, and the impact of body image change on lifestyle
Supportive Nursing Strategies: Modeling acceptance starts with the nurse. Nurses see clients with serious body image changes on a regular basis; for the client, it is a unique and potentially horrifying experience. Showing the client that a physical change does not frighten the nurse reduces the fear that people will turn away. Anticipatory guidance with visitors to prepare them for dramatic changes in their family member’s or friend’s appearance helps promote acceptance.
Providing relevant information and creating opportunities for the client to ask questions make it acceptable for the client to explore changes in self-concept related to body image is an important nursing strategy. Validation checks, asking whether the client has any questions, and suggesting realistic responses can facilitate communication about alterations in body image.
Nurses can introduce adaptive functioning by helping clients anticipate and respond with dignity to the reactions of others. Clients often worry about how their physical or emotional changes will be accepted by others. Asking questions about what the client expects, providing coaching, and helping clients identify social supports is helpful. Talking with others, for example, having a Reach for Recovery volunteer visit with a mastectomy client, is a simple intervention that helps increase the client’s adjustment and acceptance of body image disturbances.
Personal identity
Karademas et al. (2008) describe personal identity as an intrapersonal psychological process consisting of a person’s perceptions or images of personal abilities, characteristics, and potential growth potential. Personal identity is based on cognitive understandings of the self derived from perceptual and cognitive processing of personally relevant data about the self.
Each person’s self-concept is anchored in self-descriptions advanced by the culture. A clear cultural identity is positively related to self-concept clarity and self esteem (Usborne and Taylor, 2010). Understanding fundamental differences in cultural worldview orientation helps nurses frame interventions in ways that support ethno-cultural variations. For example, Western cultures tend to be individualistic, whereas Asian cultures see the individual as part of a collective group. Oyserman and Markus (1998) note:
From a North American perspective, a collective answer to the “who am I” question is that “I am a bounded, autonomous whole.” The solution to this question from a Japanese perspective is “I am a member or a participant of a group.” (p. 110)
Exercise 4-3 helps the nurse identify the contribution of life experiences that contribute to self-concept.
The Challenge of Health Status Changes: Illness, genetic factors, pain, or injury affecting cognitive abilities can compromise or crush the sense of personal identity. For example, in a study of stroke victims, findings showed a more negative sense of self, reduced social activity, and lower self-esteem, even after rehabilitation (Ellis-Hill & Horn, 2000). Individuals with brain injury or dementia can suffer a complete loss of self. Although sensory images enter the psyche, the normal cognitive processes people use to interpret their meaning can’t make sense of them. Without cognitive ability, people don’t know who they are. People with dementia lose their ability to set realistic goals, implement coherent patterns of behavior, or control basic elements of their lives. As the disease progresses, they can no longer recognize significant others or retain a sense of their personal identity.
Perception and cognition play an important role in a person’s recognition of personal identity and the ability to communicate who they are to other people. Any health change can challenge a person’s stable sense of personal identity. People get used to other persons treating them in certain ways because of status, work, or personality characteristics. Heijmans et al. (2004) suggest that, in addition to accepting an illness with its accompanying personal needs, people may need to adapt to an altered social identity and find new ways to initiate and maintain social relationships. This requires an emotional appraisal and adjustment, because things are not the same for the client or for those with whom the person interacts. Renegotiating relationships can be awkward, and clients often need the nurse’s help in how to respond.
Perception
Perception is referred to as the gatekeeper of personal identity because it is the initial cognitive process through which a person transforms external sensory data into selected images of reality. Perception allows a person to cluster sensory images into a meaningful pattern. It is a cognitive process, not an emotional one. Consider the image in Figure 4-2. Depending on where your eyes focus, one can draw different conclusions about the image. The same is true about life: Reality lies in the eye of the beholder. Perceptions differ because people develop mindsets that automatically alter sensory data in personal ways. Messages perceived as being consistent with a person’s self-concept are likely to be heard, whereas messages that are incompatible with self-images create emotional distress. Global perceptual distortions can occur as a result of delirium, psychosis, or psychoactive drug reactions.
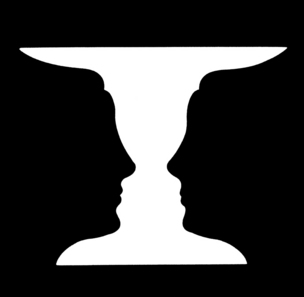
Figure 4-2 The figure-ground phenomenon. Are the figures presented in white against a black background or in black against a white background? Does it make a difference in your perception of the figures? (From the Westinghouse Learning Corporation: Self-instructional unit 12: perception, 1970. Reprinted with permission.)
Mental disorders such as depression and schizophrenia generate a distorted perceptual filter affecting perception and cognitive interpretations. Clients can distort the meaning of objective data, leading the person to engage in dysfunctional behaviors as a result. Validation of perceptual data is needed because the nurse and the client may not be processing the same reality. For example, others may perceive a person as being witty and interesting, whereas the individual internally views himself as dull and boring. Simple perceptual distortions can be challenged with compassionate questioning and sometimes, targeted humor.
Cognition
Cognition is a complex, creative, logical process that people use to make sense of perceptions. The cognitive aspects of self-concept are best characterized by the level, clarity, and logic of thinking. People with strong critical thinking skills tend to make good decisions. An example of a cognitive distortion is imagining the worst-case scenario when something minor goes wrong.
Assessment: Cognitive assessment is accomplished through client history, mental status examination, and assessment of functional capabilities. Clients or close significant others, or both, should be asked about the client’s medical and psychiatric history, medications, and any significant changes in observed changes in memory, cognitive reasoning, or expressive language. Inquiring about functional abilities to perform activities of daily living is valuable. Client data are compared with the performance of others with similar demographic background and life experiences. Significant deviations, as well as defined changes in the quality and quantity of cognitive performance, are areas for concern. It is crucial for example, to differentiate between cognitive dysfunction as the result of medication adverse effects, delirium, or depression and a true dementia (Arnold, 2005).
Serious injury or illness creates major challenges to personal identity. Particularly devastating to one’s self-concept is disease or injury affecting the brain because of their impact on processing information and communicating with others. They can erase memories, skills and the knowledge needed to conduct essential life tasks. Treating each client as a valued person, with relevant ideas, opinions, and feelings should underscore each specific treatment plan. With effort, it is usually possible to communicate even with cognitively compromised individuals in simple ways.
Planning and Intervention: Respect for the client perspective, active listening, and active involvement in collaborative planning strengthen a sense of personal identity through ownership and understanding of the treatment plan. Trying to understand the client as a valued person and the personalized meaning of the health disruption is an important common denominator in supporting the client’s personal identity.
Supportive Nursing Strategies: Interventions needed to strengthen personal identity in the face of major illness, injury, or death in clinical settings start with respecting individual preferences, values, and beliefs, and applying the simple axiom of treating each patient with the same respect as you would like to be treated in a similar situation. Box 4-1 presents guidelines to strengthen realistic perceptions and facilitate accurate cognitive processing of health care information.
Frequent perceptual checks and active listening are helpful interventions (see Chapter 10). When combined with well-thought-out inferences about the meaning of client behaviors, they enhance the quality of decision-making in the nurse-client relationship. Checking in with clients allows the nurse to use perceptual data in a conscious, deliberate way to facilitate the relationship process. Because the client feels heard and because communication focuses on matters of interest and concern to the client, mutuality occurs with greater frequency.
Successful outcomes related to a nursing diagnosis of personal identity disturbances include new adaptive coping skills, a richer appreciation of life and one’s purpose, a reordering of priorities, and enriched relationships with family and friends. A positive reframing of personal identity in the face of serious illness can contribute to better treatment adherence and a stronger sense of well-being.
Responding to Cognitive Distortions: It is not so much what happens to us as it is how we interpret and respond to our circumstances that create problems. Box 4-2 identifies common cognitive distortions. Simple perceptual distortions can be challenged with compassionate questioning, new information, and simple targeted humor. Cognitive behavioral therapy (CBT), originally developed by Aaron Beck, is the treatment of choice for clients with significant perceptual/cognitive distortions. With CBT approaches, people are initially taught to recognize their cognitive distortions, when thoughts interact with inner emotions to control behavior. This awareness is followed with strategies designed to reframe negative thinking patterns. Providing additional information, using Socratic questioning, modeling cues to behavior, and coaching clients to challenge cognitive distortions through the use of positive self-talk, mindfulness, values exploration, and a present orientation are common techniques.
Self-talk is a cognitive strategy people can use to lessen cognitive distortions. When the thought carries a negative value, it can affect the individual as though the thought represented the whole truth about the person. The thought “I stuttered in the interview” becomes emotionally translated into “I know I probably won’t get the job. I’m just no good.” One feature of one interview suddenly becomes a major defining statement of self. The pervading thoughts create a decrease in self-esteem.
Supportive Nursing Strategies: Changing internal self-talk resets the thinking process. With positive self-talk as a therapeutic strategy, the person chooses the feeling he or she will have about a situation or person. Providing additional information, modeling cues to behavior, using Socratic questioning to challenge the validity of cognitive distortions, and coaching clients to use positive self-talk is helpful. Exercise 4-4 gives practice in recognizing and responding to cognitive distortions.
Combining self-talk strategies with social support forms the basis for a prevention plan designed to correct cognitive distortions. A thinking schema that allows the client to step back and view the situation as an objective observer might before beginning to resolve it is helpful. Enlisting the help of others for support and advice leads to more effective problem solving.
Feedback and social support are powerful antidotes to cognitive distortions about responsibility. Although a plan to correct cognitive distortions is easier to articulate than to implement, these guidelines have proved useful in helping people to relinquish faulty thinking patterns and to take constructive action instead.
Self-esteem: emotional aspects of personal identity
Self-esteem refers to the affective or emotional aspects of self (Huitt, 2004). Representing an emotional appraisal of a person’s worth or value, self-esteem is defined as the emotional value a person places on his or her personal self-worth in relation to others and the environment. Self-esteem affects a person’s ability to weather stress without major changes in self-perception. With a positive attitude about self, an individual is more likely to view life as a glass that is half full rather than half empty. People who view themselves as worthwhile and as being valuable members of society have high self-esteem. People with low self-esteem do not value themselves and do not feel valued by others.
Self-esteem mirrors a person’s inner sense of self and adds an additional filter to perceptual and cognitive awareness of self. It also reflects cultural norms, genetic temperament, and supportive relationships. A key characteristic is the respect people have for themselves and their opinion of their conduct of life. Self-esteem can be related to either a specific dimension of self, “I am a good writer,” or it may have a more global meaning, “I am a good person who is worth knowing.”
People with high self-esteem have a strong emotional and intellectual conviction that they are worthy of respect and recognition, and believe that they have something unique and useful to offer to society. They respect and like who they are, and are generally satisfied with their looks, personality, skills, and ability to successfully negotiate their lives. They accept responsibility for their success and failures, and take calculated risks to achieve important personal goals. They are more likely to be motivated to make changes. Life’s inevitable problems are viewed as challenges that one can learn and grow from.
Self-esteem is not something that happens suddenly. People who learn to set realistic standards for themselves and strive to meet them are more likely to experience higher self-esteem. They are able to manage feelings and emotions in a positive way. They know and like themselves, based on an accurate perception of their strengths and limitations. In this way, the emotional components of self-concept are joined together with perceptual and cognitive components of personal identity.
By contrast, people with low self-esteem do not hold a high opinion of themselves and feel that they are worth less than others. They tend to be defensive in relationships and seek constant reassurance from others because of their own self-doubt. Instead of taking actions that could raise self-esteem, they worry and see challenges as problems rather than as opportunities.
Self-esteem tends to be relatively stable over time and across situations, but the experience of success or failure can cause fluctuations in self-esteem (Crocker, Brook, & Niiya, 2006). Sources of situational challenges to self-esteem include loss of a job; loss of an important relationship; negative change in appearance, role, or status; and verbal or physical abuse, neglect, chronic illness, codependency, and criticism by significant others. These situations leave people feeling unvalidated and undervalued as good persons. Illness, injury, and other health issues challenge a person’s self-esteem. Findings from a sizable number of research studies demonstrate an association between lower self-esteem in clients and changes in health status, functional abilities, and emotional dysfunction (Vartanian, 2009; Vickery, Sepehri, & Evans, 2008).
Situational self-esteem can be influenced by cognitive strategies to correct affective distortions in communication and maladaptive thinking patterns interfering with a person’s self-worth. Self-esteem can be enhanced through personal choices to engage fully with life, trying new things and learning new skills. Encouraging relationships with family, friends, teachers, and successful participation in social activities and clubs promote the process of achieving self-esteem. Exercise 4-5 introduces the role of social support in building self-esteem.
Assessment Strategies: Self-esteem is closely linked to our emotions, particularly those that directly involve self-concepts such as pride or shame (Brown & Marshall, 2001). Verbal and nonverbal behaviors that indicate powerlessness, frustration, inadequacy, anxiety, anger, or apathy suggest low self-esteem. Factors that contribute to affective margins of distortion in communications with clients are presented in Figure 4-3. Exercise 4-6 provides practice with clarifying feelings.
Nurses can help clients sort out and clarify the facts and emotions that get in the way of a person’s awareness of his or her intrinsic value. Note how the client describes achievements. Does the client devalue accomplishments, project blame for problems on others, minimize personal failures, or make self-deprecating remarks? Does the client express shame or guilt? Does the client seem hesitant to try new things or situations, or express concern about ability to cope with events? Observe defensive behaviors. Lack of culturally appropriate eye contact, poor hygiene, self-destructive behaviors, hypersensitivity to criticism, need for constant reassurance, and an inability to accept compliments are behaviors associated with low self-esteem. Table 4-2 identifies characteristic behaviors related to self-esteem.
TABLE 4-2
Behaviors Associated with High vs. Low Self-Esteem
| People with High Self-Esteem | People with Low Self-Esteem |
| Expect people to value them | Expect people to be critical of them |
| Are active self-agents | Are passive or obstructive self-agents |
| Have positive perceptions of their skills, appearance | Have negative perceptions of their skills, appearance, sexuality, and behaviors |
| Perform equally well when being observed as when not being observed | Perform less well when being observed |
| Are nondefensive and assertive in response to criticism | Are defensive and passive in response to criticism |
| Can accept compliments easily | Have difficulty accepting compliments |
| Evaluate their performance realistically | Have unrealistic expectations about their performance |
| Are relatively comfortable relating to authority figures | Are uncomfortable relating to authority figures |
| Express general satisfaction with life | Are dissatisfied with their lot in life |
| Have a strong social support system | Have a weak social support system |
| Have a primary internal locus of control | Rely on an external locus of control |
Therapeutic Strategies: Armed with an understanding of the underlying personalized feelings as a threat to self-esteem, (e.g., intense fear, anguish about an anticipated loss, and lack of power in an unfamiliar situation), nurses provide the opening for the client to tell his or her story. The nurse might identify a legitimate feeling by saying, “It must be frustrating to feel that your questions go unanswered,” and then saying, “How can I help you?” From a nonreactive position, the nurse can demonstrate caring about the client as a person by helping the client obtain needed information and seeking validation of legitimate client concerns.
When people have low self-esteem, they feel they have little worth and that no one really cares enough to bother with them. The nurse helps clients increase self-esteem by being psychologically present as a sounding board. Just the process of engaging with another human being who offers a different perspective can have the effect of enhancing self-esteem. The implicit message the nurse conveys with personal presence and interest, information, and a guided exploration of the problem is twofold. The first is confirmation of the client: “You are important, and I will stay with you through this uncomfortable period.” The second is the introduction of the possibility of hope: “There may be some alternatives you haven’t thought of that can help you cope with this problem in a meaningful way.” Once a person starts to take charge of his or her life, a higher level of well-being can result.
The nurse can use several strategies to help a client deepen self-esteem. Communication in the form of focused questions can assist clients in reflecting on their strengths and accomplishments. The nurse can give the client self-esteem–related feedback: “The thing that impresses me about you is…” or, “What I notice is that although your body is weaker, it seems as if your spirit is stronger. Is that your perception as well?” Such questions help the client focus on positive strengths. Exercise 4-7 strengthens the nurse’s skill in this area.
Self-efficacy
Self-efficacy is strongly associated with self-esteem, and the nursing diagnosis of powerlessness. People who believe that they can handle threatening situations value their competence and ability to succeed. They are less likely to harbor self-doubts or dwell on personal deficiencies when difficulties arise. Self-efficacy is a term originally developed by Albert Bandura (2007) in referring to a person’s perceptual belief that he or she has the capability to perform general or specific life tasks successfully. Self-efficacy influences motivation and outcome expectancies. People need to believe that they can succeed in performing a task or coping with a difficult situation to actively try to master the tasks involved. People with a strong sense of self-efficacy can approach difficult tasks as challenging and master them. Self-efficacy helps them sustain their efforts in the face of temporary setbacks and decreases anxiety. Those with a weak sense of self-efficacy view difficult tasks as threatening and will not persist if obstacles or setbacks occur.
People develop self-efficacy through personal experience with mastering tasks, seeing others similar to themselves perform tasks successfully, and through verbal support. Breaking difficult tasks down into achievable steps and completing them constructs a resilient sense of self-efficacy.
Self-help and mutual support groups can be helpful adjuncts to treatment for clients having trouble with self-efficacy in managing their illness or injury. Discovering that others have similar issues and have found ways to cope with them successfully encourages clients and reinforces a sense of self-efficacy and hope that they too can achieve functional success. The understanding, social support, and reciprocal learning found in these groups provide opportunities for valuable information sharing and role modeling (Humphreys, 2004).
Spiritual aspects of personal identity
Spiritual self-concepts, found in the innermost core of an individual, are concerned with a person’s relationship with God or a higher power, and the vital life forces that support wholeness. When a person’s body fails, or circumstances seem beyond one’s control, it is often the spirit that sustains a person’s sense of self-integrity and helps them maintain a more balanced equilibrium. Baldacchino and Draper (2001) note the presence of a spiritual force in a client’s strong will to live, positive outlook, and sense of peace.
Spirituality is a unified concept, closely linked to a person’s worldview, providing a foundation for a personal belief system about the nature of God or a Higher Power, moral-ethical conduct, and reality. Spirituality is a term often used synonymously with religion, but it is a much broader concept (Baldacchino & Draper, 2001). A key difference is that religion involves a formal acceptance of beliefs and values within an organized faith community, whereas spirituality describes self-chosen beliefs and values that give meaning to a person’s life. It may or may not be associated with a particular faith (Tanyi, 2006).

Spirituality is associated with meaning and purpose in life (Sessanna, Finnell, & Jezewski, 2007; Tanyi, 2006). A number of research studies link spirituality to health, quality of life, and well-being (Molzahn & Sheilds, 2008).
Spirituality helps us answer vital questions about what it is to be human, which human events have depth and value, and what are imaginative possibilities of being. Over the course of a lifetime, spiritual beliefs change, deepen, or are challenged by circumstances that are beyond a person’s control. Spiritual strength allows nurses and other health care professionals to willingly stand with others in darkness, and yet remain whole—to deal with the everyday challenges and stresses of nursing in a spirit of peace and hope. Spiritual aspects of self-concept can be expressed through:
• Membership in a specific religious faith community with a set of formal, organized beliefs
• Nature, meditation, or other personalized lifeways and practices linked with a higher purpose in life
• Cultural and family beliefs about forgiveness, justice, human rights, right and wrong learned in early childhood
• Crisis, or existential situations that stimulate a search for purpose, meaning, and values lying outside the self
Health crises can be a time of spiritual renewal, when one discovers new inner resources, strengths, and capacities never before tested. Or it can be a time of spiritual desolation, leaving the individual feeling powerless to control or change important life circumstances (Krebs, 2001).
Assessment
The Joint Commission (2004) mandates that health care agencies, including long-term hospice and home care services, must assess spiritual needs, provide for the spiritual care of clients and their families, and supply appropriate documentation of that care. Carson and Stoll (2008) refer to three areas of spiritual concern as a framework for nursing assessment: spiritual distress, spiritual needs, and spiritual well-being. Spiritual distress wears many faces: a lack of purpose and meaning in life, inability to forgive, loss of hope, and spirit of alienation. NANDA (2009) nursing diagnoses present specific nursing interventions for providing spiritual support: Risk for Spiritual Distress, Spiritual Distress, Readiness for Enhanced Hope, and Readiness for Enhanced Spiritual Well-being.
Assessment of spiritual needs should be approached with respect and sensitivity for the client’s beliefs and values. Assessment questions might include evaluation of the client’s
• Willingness to talk about personal spirituality or beliefs
• Belief in a personal God or Higher Power
• Relevance of specific religious practices to the individual
• Changes in religious practices or beliefs
• Areas of specific spiritual concern activated by the illness; for example, is there an afterlife?
• Extent to which illness, injury, or disability has had an effect on spiritual beliefs
A client’s spiritual needs may be quite obvious and firmly anchored in positive relationships with clergy and a personal God, or defined philosophical understanding of life and one’s place in it. Spiritual needs also can reveal evidence of conflict or anger toward a Higher Power, who is held responsible for a negative health situation. For example, the noted author C. S. Lewis (1976) calls his God “the cosmic sadist” as he experienced his personal grief following the death of his wife. Spiritual pain can be as severe as physical pain and often is closely accompanied by emotional pain. Asking about the effect an illness or health problem has had on spiritual beliefs yields useful information. Being able to talk freely about spiritual distress helps put it into perspective (McSherry, 2000).
Identifying a client’s current religious affiliations and practices is important, and inquiring about religious rituals important to the client is essential. Josephson and Peteet (2007) suggest that the client’s words can be an entry into a discussion of spirituality; for instance, if the client uses a phrase such as “By the grace of God, I passed the final examination,” you might ask something like, “It sounds like God plays a role in your life, is that true?” (p. 186).
Spiritual rituals and practices can be used to promote hope, support, and peace for a client experiencing spiritual pain. You can inquire about current spiritual practices and preferences by asking, “Are there any spiritual practices that are particularly important to you now?” When assessing the client’s current spiritual preferences, you should also consider past religious affiliations. It is not unusual for the religion listed on the client’s chart to be different from the religious practices the client currently follows. In addition, people who have never committed to a strong sense of religion previously will seek religious support in times of crisis (Baldacchino & Draper, 2001). Spiritual assessment information should be documented in the client’s record.
Spiritual well-being can be demonstrated through hopefulness in the face of adversity, compassion for self and others, and a sense of inner peace. Miller (2007) suggests, “Hope is central to life and specifically is an essential dimension for successfully dealing with illness and for preparing for death” (p. 12). Hope is critical in maintaining the “spirit” of a person in health care settings. How else can one explain the will to live or the complete serenity of some individuals in the face of life’s most adverse circumstances? Hope does not guarantee a positive outcome. It simply helps a person stay connected with life. Lack of hope is expressed in feelings of powerlessness, hopelessness, and frustration. Useful assessment questions might consist of: “What do you see as your primary sources of strength at the present time?” and, “In the past, what have been sources of strength for you in difficult times?” Miller (2007) identified several hope-inspiring strategies found in the literature, for example, helping clients and families to develop achievable aims, realize a sense of interpersonal connectedness, live in the present, and find meaning in their illness/situation. Sharing uplifting memories, affirmation of worth, and unconditional caring presence can stimulate a sense of hopefulness.
Exercise 4-8 helps in understanding spiritual responses to distress. Spirituality can be a powerful resource for families and it is important to incorporate questions about the family’s spirituality if they are involved with the client. Each family’s expression of spirituality and use of spiritual resources is unique. Tanyi (2006) suggests nurses can incorporate spiritual assessment with the family, using questions such as
What gives the family meaning in their daily routines?
What gives the family strength to deal with stress or crisis?
How does the family describe their relationship with God/Higher Power or the universe?
What spiritual rituals, practices, or resources do the family use for support?
Are their any conflicts between family members related to spiritual views, and if so, what might be the impact on the current health situation?
Strategies
The compassionate presence of the nurse in the nurse-client relationship is the most important tool the nurse has in helping the client explore spiritual and existential concerns (Carson & Koenig, 2008). Providing opportunities for clients to be self-reflective about their spirituality helps people sustain their beliefs, values, and spiritual sense of self in the face of tragedy. Gordon and Mitchell (2004) write, “Spiritual care is usually provided in a one-to-one relationship, is completely person centered and makes no assumptions about personal conviction or life orientation” (p. 646).
Providing privacy and quiet times for spiritual activities is important. The support of “nursing presence” and unstructured time for helping clients cope with spiritual issues, combined with referrals to chaplains, is an important component of nursing intervention. Nurses can help individuals and families contact spiritual advisors or clergy, or act as their advocate in ensuring appropriate spiritual rituals are followed related to dietary restrictions, Sabbath activities, meditating or praying, and at end of life. For example, in some forms of the Jewish religion, turning lights on or off or adjusting the position on an electric bed is not permitted on the Sabbath. There is no rule against these tasks being accomplished by the nurse.
Philosophical discussion may not be necessary. Spiritual connections can provide comfort for the dying and their families through prayer or hymns. Thomas (2009) describes the impact of familiar spiritual songs as he reflects on spiritual moments spent with his wife at the end of her life.
Prayer and Meditation
Praying with a client, even when the client is of a different faith, can be soothing for some patients. Nurses need to distinguish between their own spiritual orientation and needs, and that of their clients. It is not appropriate to impose a spiritual ritual on a client that would be at odds with his or her spiritual beliefs. There should be some evidence from the client’s conversation that praying or reading the Bible with a client would be an acceptable support.
According to some researchers (Daaleman, Usher, Williams, Rawlings, & Hanson, 2008; Sulmasy, 2006), spiritual support can be effectively provided through indirect means such as recognizing the human value and dignity of clients, and respecting their autonomy in shared decision making, as by supporting them through prayer.
Evaluation
Client outcomes associated with successful resolution of spiritual distress, and/or spiritual well being include connecting, or reconnecting with God or a higher power, decreased guilt, forgiveness of others, expressions of hope, and evidence that the client finds meaning in his or her current situation. Thomas (2009) describes his spiritual process of journeying to a different place with grief as follows:
Summary
Chapter 4 focuses on the self-concept as a key variable in the nurse-client relationship. Self-concept refers to an acquired constellation of thoughts, feelings, attitudes, and beliefs that individuals have about the nature and organization of their personality. Self-concepts are created through experiences with the environment and personal characteristics.
The four aspects of self-concept patterns most relevant to the practice of nursing and the nurse-client relationship are body image, personal identity, self-esteem, and spirituality. Disturbances in body image refer to issues related to changes in appearance and physical functions, both overt and hidden. Personal identity is constructed through cognitive processes of perception and cognition. Serious illnesses such as dementia and psychotic disorders threaten or crush a person’s sense of personal identity. Self-esteem is associated with the emotional aspect of self-concept, and reflects the value a person puts on the personal self-concept and its place in the world. Assessment of spiritual needs and corresponding spiritual care is a Joint Commission requirement for quality care.
Understanding the dimensions of self-concept and the critical role it plays in directing behavior is key to working effectively with clients and families. It is always a core variable to consider in nurse-client relationships. Nurses play an important role in providing support and guidance for clients related to self-concept.
References
Arnold, E. Sorting out the 3 D’s: Delirium, dementia, depression. Holist Nurs Pract. 2005;19(3):99–104.
Baldacchino, D., Draper, P. Spiritual coping strategies: a review of the literature. J Adv Nurs. 2001;34(6):833–841.
Bandura, A. Self-efficacy in health functioning. In: Ayers S., et al, eds. Cambridge handbook of psychology, health & medicine. ed 2. New York: Cambridge University Press; 2007:191–193.
Boston Women’s Health Book Collective. Our bodies, ourselves for the new century. New York: Touchstone Simon & Schuster, 1998.
Blazer, D. How do you feel about…? Health outcomes late in life and self-perceptions of health and well-being. The Gerontologist. 2008;48(4):415–422.
Brown, J., Marshall, M. Self-esteem and emotion: some thoughts about feelings. Pers Soc Psychol Bull. 2001;27(5):575–584.
Carson, V., Koenig, H. Spiritual dimensions of nursing practice, Revised ed. West Conshohoeken, PA: Templeton Press, 2008.
Carson, V., Stoll, R. Spirituality: Defining the indefinable and reviewing its place in nursing. In Carson V., Koenig H., eds.: Spiritual dimensions of nursing practice, Revised ed., West Conshohoeken, PA: Templeton Press, 2008.
Crocker, J., Brook, A.T., Niiya, Y. The pursuit of self-esteem: contingencies of self-worth and self-regulation. J Pers. 2006;74(6):1749–1771.
Cunha, C., Goncalves, M. Commentary: Accessing the experience of a dialogical self: Some needs and concerns. Culture & Psychology. 2009;15(3):120–133.
Daaleman, T.P., Usher, B.M., Williams, S.W., et al. An exploratory study of spiritual care at the end of life. Ann Fam Med. 2008;6(5):406–411.
Drench, M., Noonan, A., Sharby, N., et al. Psychosocial Aspects of Health Care. Prentice Hall, 2006.
Elliott, A. Concepts of the self. Malden, MA: Polity Press, 2008.
Ellis-Hill, C., Horn, S. Change in identity and self-concept: a new theoretical approach to recovery following a stroke. Clin Rehabil. 2000;14(3):279–287.
Erikson, E. Identity: youth and crisis. New York: Norton, 1968.
Erikson, E. The life cycle completed: a review. New York: Norton, 1982.
Gordon, M. Self-perception-self-concept pattern, Manual of nursing diagnoses, ed 11. Chestnut Hill, MA: Bartlett Jones, 2007.
Gordon, T., Mitchell, D. A competency model for the assessment and delivery of spiritual care. Palliat Med. 2004;18(7):646–651.
Heijmans, M., Rijken, M., Foets, M., et al. The stress of being chronically ill: from disease-specific to task-specific aspects. J Behav Med. 2004;27:255–271.
Huitt, W., Self-concept and self-esteem. Educational psychology interactive. Valdosta State University: Valdosta, GA, 2004. Available online:, http://www.edpsycinteractive.org/col/regsys/self.html. [Accessed November 26, 2009].
Humphreys, K. Circles of recovery: self-help organizations for addictions. Cambridge: Cambridge University Press, 2004.
Hunter, E. Beyond death: inheriting the past and giving to the future, transmitting the legacy of one’s self. Omega. 2008;56(40):313–329.
Hybels, S., Weaver, R. Communicating effectively, ed 9. New York: McGraw-Hill, 2008.
James, W.. The principles of psychology, New York, Henry Holt, 1890;vol 1.
Joint Commission on the Accreditation of Health Care Organizations Comprehensive accreditation manual for hospitals: the official handbook, Chicago, JCAHO, 2004. Available online:, www.jcaho.org. [Accessed April 15, 2009].
Josephson, A., Peteet, J. Talking with patients about spirituality and worldview: practical interviewing techniques and strategies. Psychiatr Clin North Am. 2007;30:181–197.
Karademas, E., Bakouli, A., Bastouonis, A., et al. Illness perceptions, illness-related problems, subjective health and the role of perceived primal threat: Preliminary findings. J Health Psychol. 2008;13(8):1021–1029.
Konig, J. Moving experience: dialogues between personal cultural positions. Culture & Psychology. 2009;15(1):97–119.
Krebs, K. The spiritual aspect of caring: an integral part of health and healing. Nurs Adm Q. 2001;25(3):55–60.
Lee, S.J., Oyserman, D. Possible selves theory. In: Anderman E., Anderman L., eds. Psychology of classroom learning: an encyclopedia. Detroit, MI: Macmillan Reference, 2009.
Lewis, C.S. A grief observed. New York: Bantam Books, 1976.
Luft, J., Ingham, H. The Johari window, a graphic model of interpersonal awareness. In: Proceedings of the western training laboratory in group development. Los Angeles: UCLA; 1955.
Markus, H., Nurius, P. Possible selves. Am Psychol. 1986;41:954–969.
McCormick, M., Hardy, K. Re-visioning family therapy: race, culture and gender in clinical practice, ed 2. New York: The Guilford Press, 2008.
McSherry, W. Making sense of spirituality in nursing practice. New York: Harcourt, 2000.
Miller, J. Hope: A construct central to nursing. Nurs Forum. 2007;42(1):12–19.
Molzahn, A., Sheilds, L. Why is it so hard to talk about spirituality? Can Nurse. 2008;10(4):25–29.
NANDA International. Nursing Diagnosis: Definitions and Classification 2009–2011. Ames, Iowa: J. Wiley and Sons, 2009.
Oyserman, D., Markus, H. Self as social representation. In: Flick U., ed. The psychology of the social. Cambridge, United Kingdom: Cambridge University Press; 1998:107–125.
Prescott, A. The concept of self in medicine and health care. New York: Nova Science Publishers, Inc, 2006.
Raholm, M.B. Uncovering the ethics of suffering using a narrative approach. Nurs Ethics. 2008;15(1):62–72.
Rhode, D. The injustice of appearance. Stanford Law Rev. 2009;61(5):1033–1102.
Rogers, C. Client centered therapy. New York: Houghton Mifflin, 1951.
Rowland, J.H., Desmond, K.A., Meyerowitz, B.E., et al. Role of breast reconstructive surgery in physical and emotional outcomes among breast cancer survivors. J Natl Cancer Inst. 2000;92(17):1422–1429.
Sessana, L., Finnell, D., Jezewski, M.A. Spirituality in nursing and health related literature: a concept analysis. J Holist Nurs. 2007;25(4):252–262.
Smith, M.J., Perkins, K. Attending to the voices of adolescents who are overweight to promote mental health. Arch Psychiatr Nurs. 2008;22(6):391–393.
Sullivan, H.S. The interpersonal theory of psychiatry. New York: W.W. Norton & Co., Inc, 1953.
Sulmasy, D.P. Spiritual issues in the care of dying patients. J Am Med Assoc. 2006;296(11):1385–1392.
Tanyi, R. Spirituality and family nursing: spiritual assessment and interventions for families. J Adv Nurs. 2006;53(3):287–294.
Thomas, J. My Saints Alive: A Journey of Life, Love, and Loss, 2010. [Unpublished manuscript, Charlottesville, VA, September].
Usborne, E., Taylor, D. The role of cultural identity clarity for self-concept, clarity, self-esteem, and subjective well-being. Pers Soc Psychological Bulletin. 2010;36(7):883–897.
Vartanian, L. When the body defines the self: Self-concept clarity, internalization, and body image. J Soc Clin Psychol. 2009;28(1):94–126.
Vickery, C., Sepehri, A., Evans, C. Self-esteem in an acute stroke rehabilitation sample: a control group comparison. Clin Rehabil. 2008;22:179–187.
Williams, N. Addressing negative attitudes to weight. Pract Nurse. 2009;37(3):33–34.