Health Teaching in the Nurse-Client Relationship
At the end of the chapter, the reader will be able to:
1 Define health teaching and client education.
2 Identify the domains of learning.
3 Discuss theoretical frameworks used in client-centered health teaching.
4 Apply the nursing process in health teaching.
5 Discuss health teaching applications in different settings.
This chapter focuses on specialized communication strategies for health teaching and client education. The chapter explores theories of teaching and learning as the basis for effective health teaching and client education. It describes instructional principles and strategies that nurses can use with clients and families to help them make sound judgments about their health, learn technical skills needed to self-manage chronic illness, and work effectively with community resources to maximize health and well-being.
Basic concepts
Taylor, Lillis, and Lemone (2005) define teaching as “a planned method or series of methods used to help someone learn” (p. 477). Health teaching is a specialized form of teaching, defined as a focused, creative, interpersonal nursing intervention in which the nurse provides information, emotional support, and health-related skills training. Although health teaching has many definitions, most do not address the complexity of the teaching process in health care (Wellard, Turner, & Bethune, 1998). For example, the “learner” in a health care setting can be a client, the client’s family, a caregiver, or a community. Whereas other teaching situations instruct learners having a similar level of education and knowledge, health-teaching formats must be designed to meet the diverse learning needs of individuals from different socioeconomic, educational, and experiential backgrounds. A highly educated client, a noncompliant client, and a low-literacy client with the same medical condition have similar content requirements for health teaching but may demonstrate very different learning needs.
Masters (2008) describes client (patient) education as a set of planned educational activities, resulting in changes in health-related behaviors and attitudes, as well as knowledge. Health teaching is a highly participatory process involving multilevel interventions, linked by a common goal of maximizing client health and well-being. Specific teaching strategies, the type of involvement of others, and the level of content will necessarily reflect each client’s unique learning needs.
Contemporary contexts of health teaching
The context of health teaching shapes how knowledge is constructed and delivered. Although health teaching has always been an integral part of the nurse-client relationship, it is even more prominent in a managed-care health care delivery system with mandated limitations on time and resources (Greiner & Valiga, 1998). Nurses carry larger caseloads and generally have less time to spend with their clients. They must help clients achieve favorable health outcomes with fewer visits. This requires a stronger emphasis on helping clients to develop critical thinking skills, and encouragement of greater client responsibility for the self-care management of complex health problems. The realities of a managed health care environment requires a practical approach to health teaching with additional opportunities for critical questions specifically related to the situation.
An evolving paradigm shift in health care delivery from a medical hospital-based model of health care to a community-based, public health emphasis creates new learning conditions and challenges. Today’s health care requirements mandate a broader content base for health teaching that includes primary prevention and quality-of-life issues (Ragland, 1997). Structured learning situations have yielded to a dynamic context-based format for health teaching, with a greater emphasis on the coaching components of health care teaching. Short, clear instructions, coupled with reflective prompts to elicit client feedback, create critical thinking opportunities.
Opportunities for health teaching occur can anywhere, for example, in the community, schools, parish nursing, the home, the hospital, and in clinics. Health teaching can be formal or informal. Ideally, it is a continuous process beginning in the community and extending across health care settings and systems. Even emergency departments provide opportunities for “teachable moments” for clients (Szpiro, Harrison, Van Den Kerkhof, & Lougheed, 2008).
Health teaching can take place under less-than-ideal circumstances. For many clients, the hospital or medical office is an anxiety-producing environment in which only part of what is said gets heard. Time constraints can limit the amount of material that can be covered in an individual session. Follow-up instructions or contacts, and written backup materials are useful adjuncts to onsite teaching. Physical and/or mental symptoms, difficulty with concentration or memory, and hearing and vision loss can further compromise the ability of a client to receive or process information. Health teaching can occur during home visits as the nurse observes clients having specific difficulties with aspects of health care. Referred to as guided care, this type of on the spot health teaching is targeted to specific health issues as they appear (Doherty, 2009).
Health teaching formats range from informal one-to-one relationships, formal structured group sessions, and family conferences. The media provides health teaching guidelines related to primary prevention (e.g., safe sex and drug abuse prevention commercials) to targeted community groups.
Technology is rewriting virtually every form of education. Advances have expanded the depth and breadth of health information available to the health consumer and are an important resource for nurses. Telehealth formats work by telecasting health information through video or interactive computers. This type of health teaching is becoming increasingly important in rural areas, where distance precludes onsite nursing health teaching and support.
The Internet provides instant health information, with a wide range of learning resources to accommodate different levels of knowledge and learning styles. People can also learn from the experience of others with similar health conditions through chat rooms and blogs.
Information on the Internet is searchable, up to date, inexpensive to obtain, and accessible at any time of day. For example, the American Diabetes Association and the American Cancer Society have online tools to help clients understand their disease and related treatment options. Although the Internet is a powerful learning tool, it has limitations as an accurate information resource. Not all information is relevant or credible. Helping clients to interpret content as it applies to their health situation and to differentiate appropriate information from misinformation is a vital component of health teaching using this instructional modality.
Professional, legal, and ethical mandates
Health teaching is not an option. It is a legal and ethical responsibility. The Joint Commission has established educational standards requiring health care agencies to provide systematic health education and training for clients that is:
• Specific to the client’s needs
• Sufficient for clients to make informed decisions and to take responsibility for self-management activities related to their needs
• Provided to clients in an understandable manner, and designed to accommodate various learning styles
• Reflected in documented evidence of the client’s understanding and response to the medical information
Professional nursing standards, developed by the American Nurses Association (ANA), reinforce the importance of health teaching as an essential nursing intervention (ANA, 2004). State Nurse Practice Acts mandate health teaching as an independent professional nursing function. Medicare requirements portray health teaching as a skilled nursing intervention for reimbursement purposes. The ANA Credentialing Center’s Magnet Recognition Program (2005) devotes an entire section to the role of the nurse related to client education. Educating clients about their health conditions and treatment options is a legal and ethical responsibility of the nurse related to informed consent.
Domains of learning
Health teaching is a dynamic process that involves making relevant connections to meaning within three domains initially described by Benjamin Bloom as cognitive (understanding content), affective (changing attitudes and promoting acceptance), and psychomotor (hands-on skill development). The domains are interrelated. When people learn about and practice a skill, they also develop “cognitive knowledge” about the factors that contribute to its success. As they become more proficient in performing a skill, people accept and value the skill and knowledge. Bloom’s taxonomy describes a hierarchy of learning objectives ranging from the least to the most complex that are applicable to learning in each domain.
The cognitive domain is the focus when the client has a knowledge deficit. For example, objectives in the cognitive domain for a client with a recent diagnosis of diabetes would include understanding the disease; the role of diet, exercise, and insulin in diabetic control; and trouble signs that would require immediate attention. Learning outcomes would consist of having a basic understanding of the disease process and treatment protocols, and being able to apply new information to meet personal health needs. A certain level of cognitive knowledge is an essential pre-requisite for learning in the affective and psychomotor domains.
The information clients and families need related to informed consent falls into the cognitive domain. Cognitive learning formats allow for clarification of information and correction of misinformation that may have been received from other providers, family, friends, or the Internet.
Appealing to the cognitive domain, the nurse would provide concrete explicit information verbally, in writing, and/or with related pictures to explain the desired outcome and steps needed to achieve it. . Avoid the use of general abstract terms. “You must lose 7 pounds” is better that “you must lose weight” (Redman, 2007, p. 14).
Bloom’s levels of knowledge acquisition (in ascending order) were revised in the 21st century to represent verbs rather than nouns. The hierarchy of synthesis and evaluation was reversed. The revised Bloom’s taxonomy for the cognitive domain now consists of:
• Knowledge  Remembering: recognizing, recalling information and facts
Remembering: recognizing, recalling information and facts
• Comprehension Understanding: interpreting, explaining, or constructing meaning
• Application Applying: carrying out or executing a procedure; using information in a new way
• Analysis Analyzing: considering constituent parts and how they relate to each other, and the whole
• Evaluation Evaluating: making judgments, critiquing, prioritizing, selecting, verifying
• Synthesis Creating: putting material together in a coherent whole, reorganizing material into a new pattern, creating something new (Anderson & Krathwohl, 2001)
The affective domain is concerned with emotional attitudes related to acceptance, compliance, valuing, and taking personal responsibility. Affective learning is essential when the client has issues that interfere with compliance or has reservations about treatment or self-efficacy. Health teaching targeted at the affective domain is more complex because of its association with values and beliefs. It usually takes longer than learning in the cognitive domain (Leahy & Kizilay, 1998).
The psychomotor domain refers to learning a skill through hands-on practice. Performance learning promotes greater understanding than reading or hearing about a skill and is more likely to be remembered. Many skills required for effective self-care management require hands-on training, and supervised practice of a skill is one of the best ways for the nurse to evaluate the client’s mastery of essential skills required for self-care management. Usually psychomotor learning involves demonstration of the skill by the nurse, followed by the client’s return demonstration. Desired outcomes relate to proficiency in performing the motor skill, developing personal confidence, and the ability to adjust the performance of the skill when challenged with new situations.
Another factor to consider is how people learn best. Box 16-1 presents characteristics of different learning styles.
Theoretical frameworks
Client-centered health teaching
Carl Rogers’ (1983) ideas provide a theoretical foundation for the use of teaching methodologies in client-centered health teaching. Rogers emphasizes the primacy of the teacher-learner relationship as the means through which learning occurs. He describes learner-centered teaching as an interactive process. Applied to health care, a learner-centered approach involves engaging clients as active partners in the learning process and helping them take responsibility for their own learning, to whatever extent is possible. Rogers insists that the teacher must start where the learner is, structuring the learning process to support the learner’s natural desire to learn, and being mindful of learner characteristics that enable or impede the process.
The same conditions of unconditional positive regard related to empathy, authenticity, and respect that are required for a successful therapeutic relationship apply to health teaching. Through a teaching relationship, clients begin to challenge old, unworkable ideas and habits; transform unproductive understandings and actions; and act on new perspectives (Hansen & Fisher, 1998).
Client-centered strategies place the learner in charge of his or her learning and build on personal strengths to achieve learning objectives. A highly participative learning environment, in which the nurse provides the teaching while the learner assumes primary responsibility for the learning process, encourages empowerment (Post-White, 1998). Empowerment strategies include providing sufficient information, specific instructions, and emotional support—but no more than is required—to allow each client to take charge of his or her health care to whatever extent is possible. The following case example illustrates the impact of a client-centered teaching encounter on a client.
Providing health information in unambiguous, concrete, objective terms using the client’s terminology allows the client to integrate the health teaching in his or her unique way.
Andragogy and pedagogy
Andragogy refers to the “art and science of helping adults learn” (Knowles, Holton & Swanson, 1998). According to Knowles, who applied the term andragogy to adult learning, adult learners are self-directed and goal oriented. The adult’s orientation to learning is practical and action oriented. Adult learners want to see the practicality of what they are learning. They favor a problem-focused approach to learning, and learn best when directly engaged in learning the skills and knowledge to help them master immediate life problems. The adult client learner expects the nurse to inquire about previous life experience and to incorporate this knowledge into the teaching plan. Figure 16-1 identifies Knowles’ model of adult learning.
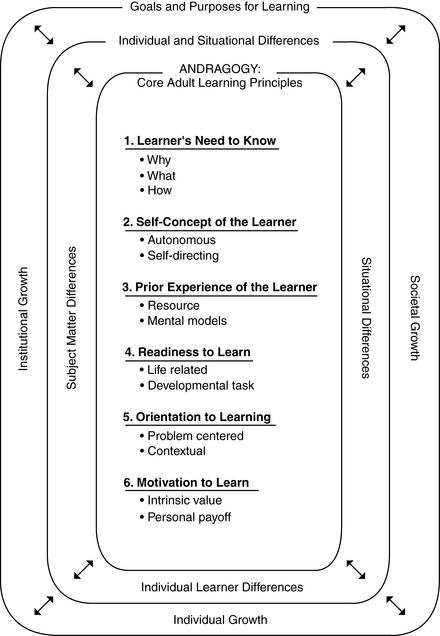
Figure 16-1 Andragogy model: a core set of adult learning principles. (From Knowles M, Holton E, Swanson R: The adult learner: the definitive classic on adult education and training (p. 182), Terre Haute, IL, 1998, Butterworth-Heinemann.)
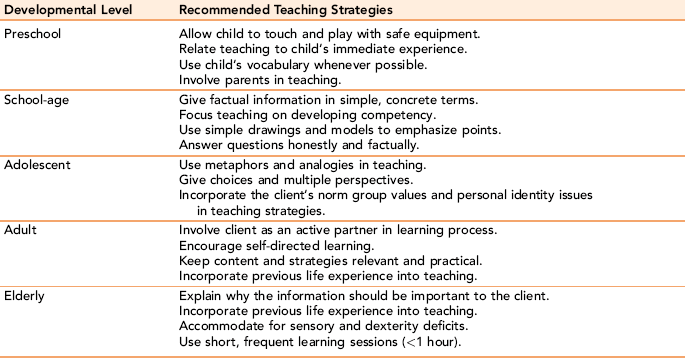
Pedagogy refers to the processes used to help children learn. A key difference between pedagogy and andragogy is the need to provide the child learner with additional direct guidance and structure in learning content. Children come to the learning experience with far less life experience that can be tapped as resources for learning. Recommended teaching strategies for learners at different developmental levels are presented in Table 16-1.
Behavioral models
Behavioral approaches are based on the theoretical framework of B. F. Skinner (1971). He believed that behavior is learned, and that it is possible to change behavior by altering the predictable consequence or response to the behavior. Behavioral approaches use a structured learning format in which learning occurs by linking a desired behavior with reinforcement for performing the behavior. Behavior modification is used to teach people skills, to get children to assume a responsibility, and to curb or break an undesired behavior or habit.
Reinforcement, which refers to the consequences of performing targeted behaviors, is a central concept. Behaviorists believe that reinforcement strengthens learner responses. Behaviors that are rewarded (positive reinforcement) tend to be repeated. Ignored behaviors tend to diminish or disappear (extinction). When undesired behaviors are penalized, by having a reward removed or by a negative consequence, they tend to decrease. Different types of reinforcement with examples are found in Table 16-2. Research demonstrates that positive reinforcement produces the best results. As a person begins to routinely do desired behaviors, material or tangible rewards are gradually replaced with social reinforcement such as praise.
TABLE 16-2
| Concept | Purpose | Example |
| Positive reinforcer | Increases probability of behavior through reward | Stars on a board, smiling, verbal praise, candy, tokens to “purchase” items |
| Negative reinforcer | Increases probability of behavior by removing aversive consequence | Restoring privileges when client performs desired behavior |
| Punishment | Decreases behavior by presenting a negative consequence or removing a positive one | Time-outs, denial of privileges |
| Ignoring | Decreases behavior by not reinforcing it | Not paying attention to whining, tantrums, or provocative behaviors |
Reinforcement schedules refer to the timing of rewards. Schedules are identified as being continuous with rewards given for each success or interval schedules in which the reward is not given for each performance; instead, the reinforcement is given after a certain number of successful attempts (fixed interval) or after a random number of responses (variable ratio).
Selecting rewards (reinforcers) that have meaning to the learner is critical because what is reinforcing to one person may not be so for another. Referred to as the Premack principle, the choice of reinforcer should always be something of value to the individual learner. Initially, reinforcement is given immediately after each successful performance. Once a behavioral outcome is achieved, new content is introduced and rewards are distributed less frequently. Variable ratio reinforcement schedules are the most effective for maintaining behaviors.
Behavioral Strategies
Modeling is a behavioral strategy that describes learning by observing another person performing a behavior. Nurses model behaviors both unconsciously and consciously in their normal conduct of nursing activities and teaching situations. Bathing an infant, feeding an older person, and talking to a scared child in front of significant caregivers provide opportunities for informal teaching through modeling behaviors.
Shaping refers to the reinforcement of successive approximations of the target behavior. The long-term goal is broken down into smaller steps. The person is reinforced for any behavior that gets him or her closer to accomplishing the desired behavior. Rewarding specific behaviors that move the person in the direction of the desired behavior (successive approximations) motivates the person to engage in the desired behavior. Steps build one upon the other, moving learners from the familiar to the unfamiliar as they progress toward meeting treatment goals.
Chaining refers to linking single behaviors together in a series of steps leading to the targeted desired behavior, for example, having a client with diabetes draw up insulin in the syringe. Once this task is mastered, the client can be instructed to inject an orange, followed by learning body sites for injection, and finally to inject the medication into identified sites. Prompts are faded as the single action tasks are mastered.
Implementing a Behavioral Approach
A behavioral approach starts with a careful description and quantification of a concrete behavior requiring change. Describe each action as a single behavioral unit (e.g., failing to take a medication, cheating on a diet, or not participating in unit activities). It is important to start small so the client will experience success. Counting the number of times the client engages in a behavior as a baseline before implementing the behavioral approach allows the nurse and the client to monitor progress.
The next step in the process is to define the problem in behavioral terms and to validate the problem statement with the client (e.g., “The client does not take his medication as prescribed,” or “The client does not attend any unit activities.”). A behavioral approach requires the cooperation of the client and a mutual understanding of the problem on the part of the nurse and the client. Active listening skills can alert the nurse to any concerns or barriers to implementation.
Next, the nurse and client reframe the problem as a solution statement (e.g., “The client will attend all scheduled unit activities.”). If the problem and solution are complex, you can break them down into simpler definitions, beginning with the simplest and most likely behavior to stimulate client interest. Identify the tasks in sequential order; define specific consequences, positive and negative, for behavioral responses; and solicit the client’s cooperation.
Once these data are complete, the next step is to establish a learning contract with the client that serves as a formal commitment to the learning process. Contracts spell out the responsibilities of each party and the consequences if positive behaviors are completed or, in the case of undesired behaviors, negative consequences if behaviors persist. The contract should include:
Initially, each instance of expected behavior should be rewarded. If the client is noncompliant or needs to pay more attention to a particular aspect of behavior, the nurse can say, “This (name the behavior or skill) needs a little more work.” One advantage of a behavioral approach is that it never considers the client as bad or unworthy.
Exercise 16-1 provides practice with a behavioral learning approach.
Applications
Applying the nursing process in health teaching
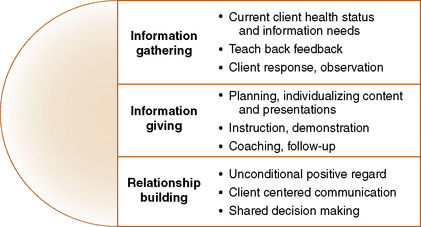
Patient education consists of clinical teaching, which is provided in all clinical settings and health education, which focuses on wellness, health promotion and disease prevention (Dreeben, 2010). As people assume greater responsibility for managing their own health, client and health education become increasingly important as a vital nursing function, Nurses assume different roles in health teaching. Depending on the situation and specific client needs, the nurse can act as a guide, an information provider, or as a resource and emotional support. As a guide, you can coach clients on actions they can take to improve their health and offer suggestions on the modifications needed as their condition changes. As information provider, you can help clients become more aware of why, what, and how they can learn to take better care of themselves. As resource support, you can help the client connect with appropriate community and health supports. By providing emotional support and appropriate descriptive, evaluative feedback, you can encourage positive learning efforts and help clients minimize the impact of negative events or temporary setbacks. Helping clients to anticipate actual and potential effects of a medication or treatment reduces anxiety and the incidence of errors. Health teaching responsibilities can be categorized into three broad categories: information gathering, information giving, and relationship building, as presented in Figure 16-2. Before beginning the education process, you should learn about all aspects of care for the client’s condition (Bonaldi-Moore, 2009).
Assessment
Health teaching formats follow the nursing process, beginning with an assessment of client learning needs, strengths, and limitations. Bastable (2008) notes, “Learners are usually the most important source of needs assessment data about themselves” (p. 98).
Clients enter a learning situation with a story model of their illness or disability that helps them make sense of what is happening to them. Understanding the story forms the basis for intervention. Physical symptoms have an emotional, relational, and social context that have important diagnostic value for health teaching focus. They can have an effect on relationships, work, and engagement in activities, which can be of considerable concern to the client and/or others involved with the client.
Broad, open-ended questions help nurses understand the learning needs of individual clients and families in a practical way, for example, “Tell me what this illness has been like for you so far,” or “Tell me what your doctor has told you about your treatment.” Asking questions demonstrates a genuine interest in what is important to clients and families, and helps tailor teaching responses to each client’s unique needs. Box 16-2 provides other questions nurses can use to assess client learning needs.
Probing the learner’s beliefs about his or her illness and proposed treatment is important because beliefs and values influence learning. For example, the client who believes that any drugs taken into the body are harmful will have a hard time learning about the insulin injection he needs to take every day. The same would be true of a client with depression, who views taking antidepressant medication as a “crutch,” and not as a necessary treatment of a mental disorder. Finding out what the client feels is his or her primary health concern is important. This may differ from the reason that the client is seeking treatment.
Assessment of client learning needs should include the client’s knowledge level, motivation, and ability to learn (see Chapter 15). A sometimes overlooked component in a learning assessment involves potential environmental barriers, such as limited health insurance, transportation difficulties, lack of follow-up facilities, and cultural dietary considerations and poverty. People may not have the money for medication, or a visit to the pediatrician for an ear infection may have a co-pay that the mother cannot afford. Health illiteracy can be a product of poverty, as well as culture (Lowenstein, Foord-May, & Romano, 2009). Failure to consider these factors can impact the effectiveness of health teaching and produce dangerous outcomes.
When processing assessment data as the basis for planning teaching interventions, it is appropriate to ask yourself the following questions:
• What specific information does the client need to enhance self-management and/or compliance with treatment?
• What attitudes does the client hold that potentially could enable or hinder the learning process?
• What specific skills does this client need for self-management?
Learner variables important in the teaching/learning process generally fall into two categories: readiness to learn and ability to learn. Incorporation of cultural values and the nurse’s self-awareness of bias are other important features of effective client education at individual, family, community, and society levels.
Learning readiness
Teaching cannot begin until the client is ready. The teachable moment takes place when the learner feels that there is a need to know the information and has the capacity to learn it. Two of the most important variables affecting learning new behaviors involve readiness and ability to learn. Learning readiness refers to a person’s mind-set and openness to engaging in a learning or counseling process for the purpose of adopting new behaviors.
Factors that affect readiness to learn
Readiness to learn is not the same as the cognitive ability to learn. Nurses need to remember that learning is never smooth or linear in its development. Rather than challenge the client’s learning pattern, the nurse needs to understand it and incorporate it into new opportunities for learning (Blackie, Gregg, & Freeth, 1998). This is the art of health teaching. For example, a statement “I notice that we don’t seem to be making much headway with the dietary changes required by your high cholesterol. I wonder if there are some issues that we have not addressed that may be getting in the way” is empathetic, and directly focused on what needs to happen next..” Psychosocial and physical factors that can affect the learner’s ability to learn include previous knowledge and experience about the illness, as well as its personal and cultural meaning.
Level of Anxiety
High anxiety can compromise the teaching/learning process by interfering with the client’s ability to focus attention and comprehend the material. Accurately assessing and managing a client’s level of anxiety before health teaching is essential, as is choosing a time when the client is most likely to be receptive (Stephenson, 2006). Developing a relationship with the client helps establish credibility and trust, and decreases anxiety. Active listening and eliciting the expectations of clients help the nurse get a more complete picture of a situation and can illuminate less obvious apprehension.
Factors that affect ability to learn
Many factors affect a client’s capacity to learn new information and ways of behaving. Some clients are ready to learn but are unable to do so with traditional learning formats (Hemmings, 1998). Assessing the client’s ability to learn and adapting the learning format to the learner’s unique characteristics makes a difference. If the client cannot understand what is being taught, learning does not take place.
Physical Barriers
A client’s physical condition or emotional state can temporarily preclude teaching. A client in pain can focus on little else. A client emerging from the shock of a difficult diagnosis may require teaching in small segments or postponement of serious teaching sessions until time to absorb the diagnosis has elapsed. Certain physical and mental conditions limit attention or compromise cognitive processing abilities. The client with significant thought disorders may need very concrete instructions and frequent prompts to perform adequately. Nausea, weakness, or speech or motor impairments may make it difficult for the client to maintain motivation. Medications or the period of disorientation after a diagnostic test or surgical procedure can influence the level of the client’s ability to participate in learning. Careful assessment will usually reveal when the client’s physical or emotional condition is a barrier to learning.
Comorbid health problems that could interfere with the goals or process of teaching are important pieces of data that influence what can and should be taught. For example, an exercise program might be useful for an overweight person, but if the client also has a cardiac condition or other problem that would limit activity, this information has a direct impact on the goals and strategies of the intervention.
Other physical or emotional issues favor learning. Mezirow (1990) notes that crisis and life transitions provide a format for the most significant adult learning because the anxiety associated with the crisis situation (if it is not extreme) can create the need to learn, and attention is likely to be more intense. Crisis learning is particularly effective with homeless and immigrant clients, who may not voluntarily seek health care or want to engage in health teaching at any other time. Health teaching for these clients should be immediate, practical, designed to resolve the crisis situation, and carefully organized to maximize client attention.
Assessment is an interactive process in which clients should be encouraged to ask questions. By introducing the idea that most people have questions, clients feel freer to question data or to ask for more explanation. At the end of an assessment interview, you can summarize important points and ask for validation. This helps to ensure a common understanding of the issues and identify any misinformation. It also reinforces the idea of a reciprocal relationship as the basis for health teaching.
Family Support and Teaching Needs
Health teaching can involve family members in either a supportive role or as a primary recipient. Comprehensive health teaching is required for those actively involved as a primary caregiver, for example, with children, or clients with significant mobility, sensory deficits, or cognitive deficits. Content presentations to these family members would be the same as those given to the client.
When family members take supportive roles, for example, with teenagers, clients in crisis, and frail elder or critically ill clients with intact cognitive abilities, health teaching should focus on what they need to know to support the client. Family caregivers need to be in a position to support the client’s efforts to implement new behaviors. Information and anticipatory guidance about what to expect when the client goes home and early warning signs of complications or potential problems should be given to family support members, as well as to clients. Knowing when to seek professional assistance and resource support is critical information.
Family support is an important dimension of health maintenance for frail elders, and individuals who depend on others for direction and oversight of treatment for a chronic condition. Any change in the level of support from primary caregivers can affect a client’s willingness or ability to learn. When these supports are no longer available through death or incapacity, the client may lack not only motivation but the skills to cope with complex health problems.
Emotional issues of loss and change complicate the learning needs of this client. Edward could function and maintain his health when he could rely on his wife for support. To enhance Edward’s learning readiness, the nurse might initially have to assess for depression and then help him find alternative ways to meet his dependency needs, for example, by expanding his social support system.
Planning
Health teaching is not a static process or one-time event. Stephenson (2006) notes that nurses need to consider the following questions:
What does the client understand so far?
What is the most important to learn about now?
What is the amount of information desired, prioritization preferred, and method of learning? (p. 243)
Planning requires more than knowledge of current client status. Each learning situation has a past and a present reality. Past experience and beliefs about illness, medications, certain treatments, cultural values, and the reactions of others produce assumptions that influence motivation and the acceptance of health teaching. Sample nursing diagnoses amenable to health teaching are presented in Box 16-3.
Nurses need to know what previous information the client has received and to whom the client looks for health information. Focusing on accurate information without destroying the credibility of well-meaning and influential informal health informants in the client’s life is part of the art of health teaching. Nothing is gained by injuring the reputation of the person who gave the client the information. Instead, you could say, “There have been some new findings that I think you might be interested in. Current thinking suggests that (give example) works well in situations like this.” With this statement, the nurse can introduce a different way of thinking without challenging the person identified in the client’s mind as expert.
Although too much information puts the learner into informational overload so that critical content is not learned, not enough direction can also prove harmful.
Organized planning is pivotal to the purpose and methodology of health teaching. Timely comprehensive health information presented in an orderly fashion is a critical component of successful coping and treatment compliance. For example, a person with a recent myocardial infarction will need to learn about:
• The medications, diet, and exercise regimens needed to improve cardiac function
• Lifestyle changes to reduce stress and improve cardiac function
In addition to giving complete information, the nurse can ask, “Do you have any questions for me?” and suggest that if things come up that the client has questions about later, the client should ask for further clarification.
Often hours or days after the teaching takes place clients will have questions or concerns about the information they received. Planning should include additional opportunities for discussion after the client has had time to absorb the initial information. You can encourage the client to jot down questions that may develop as they occur.
Developing Learning Goals
Setting mutual goals with clients with periodic reviews helps to motivate clients and serves as a benchmark for evaluating change. It is important to establish goals with your client rather than for your client. Clear learning goals that the client is interested in meeting, and has the necessary ability and resources to achieve increase the chances that the information will be understood and applied (London, 2001). Prioritizing goals and objectives that are important to client health and well-being helps nurses and clients focus on the most relevant specifics.
Identify outcome goals with a general statement about what the client needs to achieve as a result of the teaching. (e.g., “After health teaching, the client will maintain dietary control of her diabetes.”). An interim goal might be, “After health teaching, the client will develop an appropriate diet plan for 1 week.”). Setting realistic goals prevents disappointment. Box 16-4 summarizes guidelines to use in the development of effective health teaching goals and objectives. Exercise 16-2 provides experience with developing relevant behavioral outcome goals.
Developing Measurable Objectives
Objectives are powerful guides to organizing content and suggesting appropriate planning activities. Each objective should describe an immediate action step that the client should take to accomplish relevant treatment outcomes. Teaching objectives should be modest and achievable in the time frame allotted. They should be logically organized and build on one another for maximum effectiveness. To determine whether an objective is achievable, consider the client’s level of experience, educational level, resources, and motivation. Then define each learning objective needed to achieve the health goal in specific measurable behavioral terms.
Objectives should support the overall health outcome and directly relate to the nursing diagnosis. For example, the nursing diagnosis for a client with newly diagnosed diabetes might read, “knowledge deficit related to diabetic diet.” Examples of appropriate progressive learning objectives required for mastering diabetic control might occur as follows:
• First teaching session: The client will identify the purpose of a diabetic diet and appropriate foods.
• Second teaching session: The client will identify appropriate foods and serving sizes allowed on a diabetic diet.
• Third teaching session: The client will demonstrate actions for urine/blood testing for glucose at home.
• Fourth teaching session: The client will identify foods to avoid on the diabetic diet and the rationale for compliance.
• Fifth teaching session: The client will describe symptoms and actions to take for hyperglycemia and hypoglycemia.
Timing
Health teaching is not an add-on; it is an essential nursing intervention. Factors involved in timing are presented in Box 16-5. Teaching interventions should never be eliminated because the nurse lacks time, but they can be streamlined. Even in the most limited situation, schedule a block of time for health teaching. You will need to consider how much time is required to learn a particular skill or body of knowledge, and build this into the learning situation. Complicated and/or essential skill development needs blocks of time and repeated practice with feedback.
Pick times for teaching when energy levels are high, the client is not distracted by other things, it is not visiting time, and the client is not in pain. Careful observation of the client will help determine the most appropriate times for learning.
People have saturation points as to how much they can learn in one time period. Because even under the best of circumstances, people can absorb only so many details and fine points, limit information to two or three points at a time. Keep the teaching session short, interesting, and to the point. Ideally, teaching sessions should last no longer than about 20 minutes, including time for questions. Otherwise, the client may tire or lose interest. Scheduling shorter sessions with time in between to process information helps prevent sensory overload and reinforces teaching points.
In addition to scheduled teaching sessions, nurses have many opportunities for informal teaching that occur during the course of providing care. Simple, spontaneous health teaching takes minutes, yet it can be highly effective. The following case example, taken from Heartsounds (Lear, 1980), illustrates this point.
This teaching intervention probably took less than 5 minutes, yet its effect was long-lasting and healing. There are countless opportunities for informal health teaching in clinical practice if the nurse consciously looks for them.
Implementation
Each teaching session should demonstrate a thorough knowledge of the topic, a keen understanding of the client’s learning needs, and a genuine interest in the client. The client must be actively involved in the process. Effective teaching involves not only a healthy exchange of information, but plenty of opportunities to ask questions and to receive feedback.

Health Teaching Format
No one teaching strategy can meet the needs of all clients (Rycroft-Malone et al., 2000), but people learn best when there is a logical flow and building of information from simple to complex. Begin by presenting a simple overview of what will be taught and why the information is important to learn. Include only essential information in your overview; for example, give a brief explanation of the health care problem, risk factors, treatment, and self-care skills the client will need to manage at home (Lee et al., 1998). Incorporate or ask about previous related experience. Introductory content that builds on the person’s experiences, abilities, interests, motivation, and skills is more likely to engage the learner’s attention.
Deliver key points and allow regular opportunities for client feedback and questions. If the material is complex, it can be broken down into smaller learning segments. For example, diabetic teaching could include the following segments:
• Introduction, including what the client does know
• Basic pathophysiology of diabetes (keep description simple and short)
• Demonstration of insulin injection with return demonstration
• Recognizing signs and symptoms of hyperglycemia and hypoglycemia
A strong closing statement summarizing major points reinforces the learning process. Exercise 16-3 provides practice with developing a mini teaching plan.
Using Clear Language
Use clear precise language. Choice of words should be familiar to the client. Whenever possible, avoid the use of nonessential adjectives. Place words with more than one meaning in context as many words have more than one connotation. Consider the word cold. It can refer to temperature, an illness, an emotional tone, or a missed opportunity. Using too general or vague language leaves the learner wondering what the nurse actually meant. For example, “Call the doctor if you have any problems” has more than one meaning. “Problems” can refer to side effects of the medication, a return of symptoms, problems with family acceptance, changed relationships, and even alterations in self-concept. In this case, clear descriptors should cover the following:
• Identification of specific behaviors warranting attention
• What needs to happen if problems arise and under what specific circumstances
• Who needs to be contacted (with contact information) if something goes wrong
A clear statement that the nurse might use is, “If you should develop a headache or feel dizzy in the next 24 hours, call the emergency room doctor right away.”
Note that comprehension involves more than simply hearing or decoding written words. It includes understanding language nuances and being able to put underlying themes together in ways that make sense of the message as a unified whole. Verbally checking in with clients to confirm a common understanding of words and concepts is critical to knowledge transfer in health teaching. Doak, Doak, Gordon, and Lorig (2001) suggest asking the client, “What does this material tell you about____________ [subject]? What does it tell you to do?” (p. 188).
Visual Aids
Visual aids can be used to reinforce a message by providing concrete images. Simple images and few words work better than complex visual aids (Huntsman & Binger, 1981). For example, the nurse might show a new mother pictures of common infant rashes. A chart or model showing the heart might help another client understand the anatomy and physiology of a heart disorder. Perdue, Degazon, and Lunny (1999) suggest that DVD tapes are useful in teaching clients with limited reading skills. They have the advantage of allowing clients to watch them again at their convenience. Related discussions help to correct misinterpretations and emphasize pertinent points.

Preparing Written Handouts
Written backup materials to which clients can refer when needed reinforce learning. Attention to the client’s reading level and health care literacy helps ensure that the pamphlets can be read. Most reading materials should be geared to a sixth-grade reading level. Even people with adequate health literacy comprehend information better when the language is simple and clear. Incorporating relevant line drawings or pictures can be useful with clients who have language issues. Large-print pamphlets and audiotapes are helpful learning aids for those with sight problems.
Guidelines for preparing effective written materials include the following:
• Present the most important information first.
• Illustrations and diagrams should be designed to enhance clarity and appeal.
• Make sure that the content is current, accurate, objective, and consistent with information provided by other health providers.
• Use appropriate language at a literacy level that the reader can understand.
• Use a 12-point font and avoid using all capital letters for reading ease.
• Define technical terms in lay language and avoid medical jargon.
• Check for spelling errors and stay away from complicated sentences.
• Include resources with contact information that the client can refer to for further information or for help with problems.
Using Advance Organizers
Advance organizers, sometimes called a mnemonic, consist of cue words, phrases, or letters related to more complex data. They are designed to help people remember and recall difficult concepts. For example, the letters in the word diabetes can help a client remember key concepts about diabetes:
Each letter stands for a concept or action needed to control diabetes. Taken together, the client has a useful tool for remembering all related concepts.
Nursing students can use mnemonics to help them remember key points. Word associations promote remembering in much the same way that linking new information to previously learned information does. For example, the four F’s (fat, forty, female, family history) can help students remember risk factors for gallbladder disorder. Developing mnemonics can be fun and creative.
Accommodating Special Learning Needs
The level of information and amount of time for health teaching should reflect differences and changes in client circumstances. Clients experiencing a recent diagnosis will need more detailed basic information than clients having an unanswered question or requiring follow-up information. If a client’s condition worsens, becomes stable, or improves, you will need to modify teaching goals, content, and strategies to reflect relevant changes.
Accommodating for Cultural Diversity: Clients with English as a second language or a strong ethnic background usually require learning accommodations. Health teaching and educational programs that take into consideration the cultural health practices of individuals and families are likely to be more successful. Whenever possible, include cultural values or beliefs about health in teaching content and delivery. Use culturally relevant terminology.
Use fewer, rather than more words to explain a concept and allow extra time to practice psychomotor skills with feedback. When teaching a client with English as a second language, keep in mind that words from one language do not necessarily translate with the same meaning into another. Words for certain concepts either do not exist or the phrases used for expressing and describing them can differ. Sometimes there is a tendency for people to speak louder when instructing someone from a different culture. This is not necessary. People with health literacy issues because of language are neither deaf nor unable to grasp information, if their special needs are taken into account. Speak slowly in a normal conversational tone. Lorig (2001) suggests that in preparing teaching materials for translation, the following are important:
• Use nouns rather than pronouns, and simple unambiguous language
• Use short simple sentences of less than 16 words each
• Avoid the use of metaphors and informal slang
• Avoid verb forms that have more than one meaning, or include would or could (p. 181).
If the client still is unable to understand important concepts with accommodations, enlisting the services of a trained medical interpreter becomes an essential intervention.
Learners handicapped by memory deficits, lack of insight, poor judgment, and limited problem-solving abilities also require special accommodations. Special needs learners respond best when the content is presented in a consistent, concrete, and patient manner, with clear and frequent cues to action. Clients with limited literacy skills may benefit from using audiotapes in addition to or instead of written materials.
Giving Feedback
Feedback is an essential component of successful health teaching programs. To appreciate its significance, consider the effect on your performance if you never received feedback from your instructor. Feedback about how the client is accomplishing teaching goals should be descriptive, and include areas of accomplishment and need for growth. Effective feedback is honest and based on concrete data. When providing feedback, keep it simple and focus only on behaviors that can be changed. Behavioral statements on a continuum (e.g., “You seem skilled with drawing up the medication, but you may need a little more practice with selecting sites.”) are more effective than absolute statements (e.g., “You still are not doing this correctly.”).
Feedback given as soon as possible after an observation is more likely to be accepted by the client. Indirect feedback—provided through nodding, smiling, and sharing information about the process and experiences of others—reinforces learning. Exercise 16-4 provides practice with giving feedback in health teaching.

Teaching self-management and caregiving skills
The subject of health teaching would be incomplete without a discussion of strategies focused on the development of self-management and caregiving skills needed by an increasing number of people coping with chronic illness and disability in the community. Although a lot of self-management strategies are disease or disability specific, common to most chronic conditions are issues of fatigue, pain, sleep management, lifestyle adjustments, limitations in social/role activities, self-efficacy, and identity issues.
Using a Problem-Solving Teaching Approach
Teaching about medications is a critical example of self-management education related to client safety where you can use a problem-solving approach. Begin by providing the client with both generic and commercial names of medications. Many medications look alike, so correctly labeling them and having clients/family caregivers visually identify the medication is helpful. Medication reconciliation is extremely important for elderly clients who usually are taking multiple medications, with the potential for getting them mixed up. Make sure that the client has the finances to obtain medication on a regular basis. If equipment is used, for example, syringes for insulin, make sure the client can read the calibrations and is injecting in appropriate areas.
You will need to clearly identify the purpose of the medication, expected therapeutic response, and side effects of the medications the client is receiving. Discuss what happens if the client misses a dose or decides to stop the medication. For example, doubling up on the next dose or stopping a medication abruptly may create significant issues for clients. Missing birth control pills even for a short period may result in an unwanted pregnancy. If blood tests are required to determine the efficacy or toxicity of the prescribed drug, the rationale and timing should be explained. Talk about symptoms that could require immediate medical attention and what to do in case of emergency. As with other forms of health teaching, summarize key points at the conclusion of the teaching session. Family members need to be given enough information to support client adherence to the treatment protocol. Box 16-6 provides medication teaching tips developed by the Institute for Safe Medication Practices.
The Center for the Advancement of Health (2002) has identified problem solving, decision making, utilization of resources, development of client/provider partnerships, and taking action as essential self-management skills. Key caregiving skills identified in the literature are those involving “monitoring, interpreting, making decisions, taking actions, making adjustments, accessing resources, providing hands-on care, working together with the ill person, and navigating the health care system” (Schumacher & Marren, 2004, p. 460).
Not all of these skills can be taught simultaneously. Development of self-management and caregiving skills requires a contextual, problem-based teaching approach. In addition to medical management of chronic conditions, people need coaching and support to integrate health-related changes into life roles, and management of the emotions created by having a chronic condition (Lorig & Holman, 2003). Repetition is important, as is careful inquiry with open-ended questions about any issues that might compromise compliance.
Clients and families should be advised of what to expect from treatment and medications, as well as risks, benefits, prognosis, and options for treatment. This information allows them to make better health care decisions. They should understand why an action is important, what they can expect from following a treatment protocol, and how aspects of treatment can help them.
Clients and families need to know the danger signals to watch for that would require a prompt call for assistance. They should be coached on the types of circumstances requiring a call to their health care provider.

Teach-Back Method
Allowing extra time for the client to talk about and do return demonstrations of tasks reinforces learning (Bohny, 1997). Teach back or show back is a teaching strategy used to evaluate and verify a client’s understanding of health teaching and/or ability to execute self-management skills. It involves asking the learner to repeat back relevant information and treatment instructions in his or her own words (Lorenzen, Melby, & Earles, 2008). Asking the learner to describe actions that would need to be taken if a protocol or procedure cannot be followed exactly or if the actions a client takes fails to produce the desired effect can be included. The method provides the nurse with valuable data about areas of skill learning that may need additional attention. Using it as you go along reinforces each piece of information and eliminates the problem of delivering a comprehensive teaching plan only to discover that the client lost your train of thought after the first few sentences.
Coaching Clients
Coaching is an effective teaching strategy used to teach self-management and problem-solving skills to clients and families experiencing unfamiliar tasks and procedures (Lewis & Zahlis, 1997). For example, coaching can help clients distinguish between which symptoms require immediate medical attention and which ones can be handled with self-management strategies.
Coaching clients as they negotiate a complex health care system can prove invaluable. For example, the nurse might assist the client or family in opening a communication with a health agency and choosing the appropriate questions to ask. Or, it may be as simple as coaching people to seek information from several sources rather than calling only one and waiting for a response (Lorig & Holman, 2003).
Coaching emphasizes the client’s autonomy in developing appropriate solutions, as the client is always in charge of the pace and direction of the learning. Through a coaching dialogue, you can encourage a client to critically think about the elements of a situation, consider multiple options, and evaluate the appropriateness of choosing one option over another. Assessment for coaching purposes starts with an exploration of how the client is experiencing the fundamental patterns of a situation. This assessment assists clients to challenge obstructive perceptions, connect past experience with current knowledge about the context of a situation, look for cues in a situation, and consider the consequences of taking different actions.
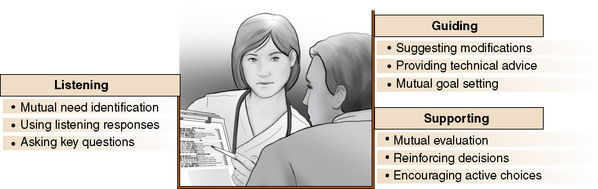
In the coaching role, nurses can present different perspectives that the client may not have considered. Coaching can include role-playing and value clarification. The process can inform the client about timing of actions, potential outcomes, areas that need special attention, and contextual issues that might not otherwise emerge in a teaching situation. In addition to giving appropriate information, coaching involves taking the client step by step through a procedure or activities in which the client takes the lead in choice of actions. The secret of successful coaching is to provide enough information to help the client take the next step without taking over. Coaching involves a number of skills presented Figure 16-3. Exercise 16-5 provides practice with coaching as a teaching strategy.
Providing Transitional Cues
Directions for self-management of illness or disability may seem simple and obvious to you, but clients or families may have difficulty with material simply because they do not know how the information fits together in their particular circumstances. Instead of using generic explanations of skills and medication management, use language and concepts specific to the client’s situation. For example, connecting the purpose of taking a medication with the actual actions you want the client to take helps fix the process in a person’s mind and makes it easier to remember related instructions. Ask clients how they will implement an essential medical management strategy such as using an inhaler or adhering to a therapeutic diet. This discussion requires clients to seriously consider how an application directly affects them and any changes in lifestyle behaviors needed to accommodate for it.
Health teaching applications in different settings
Group presentations offer the advantage of being able to teach a number of people at one time. The format allows people to learn from each other, as well as from the teacher. Health teaching topics that lend themselves to a group format include care of the newborn, diabetes, oncology, and prenatal and postnatal care (Redman, 2007).
Formal group teaching should be structured in a space large enough to accommodate all participants. The learner should be able to hear and see the instructor and visual aids without strain. Technical equipment should be available and in working order. Should the equipment not work, it is better to eliminate the planned teaching aid completely than to spend a portion of the teaching session trying to fix it.
Preparation and practice can ensure that your presentation is clear, concise, and well spoken. In a group presentation, you will need to establish rapport with your audience. Make eye contact immediately and continue to do so throughout the presentation. Extension of eye contact to all participants communicates acceptance and inclusion. A quote at the beginning capturing the meaning of the presentation or a humorous opening grabs the audience’s attention. Strengthen content statements with careful use of specific examples. Citing a specific problem and the ways another person dealt with it gives general statements credibility. Repeating key points and summarizing them again at the conclusion of the session helps reinforce learning.
If you plan to use PowerPoint, use a font that is large enough to see from a distance (32 point is recommended) and include no more than four or five items per slide. Use the slides wisely to identify key points, not as the primary content for the presentation. Face the audience, not the slides. Practice your presentation to ensure that you keep within the time frame and allot time for short discussion points. The key points can help you stay on track and move through the agenda. It is up to you as the presenter to set the pace. No matter how interesting the presentation and dialogue that it stimulates, running out of time can be frustrating for the audience and presenter.
Anticipate questions and be on the alert for blank looks. No matter how good a teacher you are, you will from time to time experience the blank look. When this occurs, it is appropriate to ask, “Does anyone have any questions about what I just said?” Give reinforcement for participation verbally, “I’m so glad you brought that up,” or “That’s a really interesting question (or comment).” Smiling and nodding your head are nonverbal reinforcers. If a participant has a question that you cannot answer, do not bluff it. Instead, say, “That is a good question. I don’t have an answer at this moment, but I will get back to you with it.” Sometimes another person will have the required information and will share it.
Handouts and other materials provide additional reinforcement. Make sure that the information is accurate, complete, easy to understand, logical, and very important, that you have enough for all participants. Exercise 16-6 provides an opportunity to practice health teaching in a group setting.
Health Teaching in the Home
Preparing for discharge has specialized teaching/learning needs that nurses need to consider in caring for clients and families (see also Chapter 24). Relevant areas of learning needs to assess are identified in Box 16-7.
In home care, the nurse is a guest in the client’s home. Part of the teaching assessment includes appraisal of the home environment, family supports, and resources, as well as client needs. Although teaching aids and structured teaching strategies available in the hospital setting may not be available, in many ways the home offers a teaching laboratory unparalleled in the hospital. The nurse can actually “see” improvisations in equipment and technique that are possible in the home environment. Family members may have ideas that the nurse would not have thought of, and the nurse can see the obstacles the family face.
Always call before going to the client’s home. This is common courtesy; it also protects the nurse’s time if the client is going to be out. Teaching in home care settings is rewarding. Often, the nurse is the client’s only visitor. Family members often display a curiosity and willingness to be a part of the learning group, particularly if the nurse actively uses knowledge of the home environment to make suggestions about needed modifications.
When in the home, it is important to model appropriate behaviors (e.g., washing hands in the bathroom sink before touching the client). Simple strategies, like not washing one’s hands in the kitchen sink where food is prepared, encourage the client to do likewise.
Teaching in home care settings has to be short-term and comprehensive, because most insurance companies will provide third-party reimbursement only for intermittent, episodic care. Nurses need to plan teaching sessions realistically so that they can be delivered in the shortest time possible. Content must reflect specific information the client and family need to provide immediate effective care for the client, nothing more and nothing less. Sometimes it is tempting to include more than what is essential to know. Because there are so many regulations regarding the length and scope of skilled nursing interventions imposed by third-party reimbursement guidelines, the nurse needs to pay careful attention to health teaching content and formats. At the same time, reviewing medications with clients and families at every visit is useful.
Helping clients access supportive services can be extremely helpful to families who would not otherwise do so even with the appropriate written information. Having knowledge of community resources is essential. This knowledge allows you to help clients and families select from a number of existing resources and create new ones through novel uses of family and community support systems. Expert nurses know that clients often can be a source of information about resources they may not know about. An understanding of Medicare, Medicaid, and other insurance matters (e.g., regulations, required documentation, and reimbursement schedules) is factored into the management of health care teaching in home health care.
Evaluation
Regardless of the setting in which health teaching takes place, the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) requires written documentation of client health teaching. Notes about the initial assessment should be detailed, comprehensive, and objective. Teaching content and delivery should be related to assessment data, including client preferences, previous knowledge, and values. Included in the documentation are the teaching actions, the client response, and any clinical issues or barriers to compliance. If family members are involved, this information should be acknowledged. Accurate documentation serves a critical purpose in health teaching, helps ensure continuity, and prevents duplication of teaching efforts. The client’s record informs other health care providers of what has been taught and what areas need to be addressed in future teaching sessions. See the following example for documentation of home health teaching:
4/8/Blood glucose check normal. Vital signs stable. Client on insulin for 10 years; has difficulty prefilling syringes. Lives with son who works. Nursing diagnosis: knowledge deficit related to prefilling syringes and ineffective coping in self-medication related to poor eyesight. Nurse prefilled syringes, wrote out med schedule, and discussed in detail with client. Client receptive to medication instruction, but may have difficulty with insulin prefill secondary to poor vision. Instructed client on medications, signs and symptoms to report to MD, diet and safety measures. Client able to repeat instructions. Spoke with son regarding medication supervision.
Summary
This chapter describes the nurse’s role in health teaching. Theoretical frameworks, client-centered teaching, critical thinking, and behavioral approaches guide the nurse in implementing health teaching. Teaching is designed to access one or more of the three domains of learning: cognitive, affective, and psychomotor. Assessment for purposes of constructing a teaching plan centers on three areas: What does the client already know? What is important for the client to know? What is the client ready to know?
Essential content in all teaching plans includes information about the health care problem, risk factors, and self-care skills needed to manage at home. No one teaching strategy can meet the needs of all individual clients. The learning needs of the client will help define relevant teaching strategies. Several teaching strategies, such as coaching, use of mnemonics, and visual aids, are described. Repetition of key concepts and frequent feedback make the difference between simple instruction and teaching that informs. Documentation of the learning process is essential. The client’s record becomes a vehicle of communication, informing other health care workers what has been taught and what areas need to be addressed in future teaching sessions.
References
American Nurses Association. Scope and standards of practice. Washington, DC: Author, 2004.
American Nurses Credentialing Center. The magnet recognition program. Recognizing excellence in nursing service. Application manual. Silver Spring, MD: Author, 2005.
Anderson L.W., Krathwohl D.R., Bloom B., eds. A taxonomy for learning, teaching and assessing: a revision of Bloom’s Taxonomy of educational objectives: Complete edition. New York: Longman, 2001.
Bastable, S.B. Nurse as educator: principles of teaching and learning for nursing practice, ed 3. Sudbury, MA: Jones and Bartlett Publishers, 2008.
Blackie, C., Gregg, R., Freeth, D. Promoting health in young people. Nurs Stand. 1998;12(36):39–46.
Bohny, B. A time for self-care: role of the home healthcare nurse. Home Healthc Nurse. 1997;15(4):281–286.
Bonaldi-Moore, L. The nurse’s role in educating postmastectomy breast cancer patients. Plastic Surgical Nursing. 2009;29(4):212–219.
Center for the Advancement of Health. Essential elements of self-management interventions. Washington, DC: Author, 2002.
Doherty, D. Guided care nurses help chronically ill patients. Patient Educ Manag. 2009;16(12):139–141.
Doak, C., Doak, L., Gordon, L., Lorig, K. Selecting, preparing and using materials. In Lorig K., ed.: Patient education: a practical approach, ed 3, Thousand Oaks, CA: Sage Publications, 2001.
Dreeben, O. Patient Education in Rehabilitation. Sudbury MA: Jones and Bartlett Publishers, 2010.
Greiner, P., Valiga, T. Creative educational strategies for health promotion. Holist Nurs Pract. 1998;12(2):73–83.
Hansen, M., Fisher, J.C. Patient teaching: patient-centered teaching from theory to practice. Am J Nurs. 1998;98(1):56–60.
Hemmings, D. Health promotion for people with learning disabilities in the community. Nurs Times. 1998;94(24):58–59.
Huntsman, A., Binger, J. Communicating effectively. Wakefield, MA: Nursing Resources, 1981.
Joint Commission. What did the doctor say? Improving health literacy to promote patient safety. In: Health Care at the Crossroads Reports. Oakbrook Terrace, IL: Joint Commission Resources, Inc; 2007.
Knowles, M., Holton, E., Swanson, R. The adult learner: the definitive classic on adult education and training, 1998. [Terre Haute, IL].
Leahy, J., Kizilay, P. Fundamentals of nursing practice: a nursing process approach. Philadelphia: WB Saunders, 1998.
Lear, M.W. Heartsounds. New York: Pocket Books, Simon & Schuster, 1980.
Lee, N., Wasson, D., Anderson, M., et al. A survey of patient education post discharge. J Nurs Care Qual. 1998;13(1):63–70.
Lewis, F., Zahlis, E. The nurse as coach: a conceptual framework for clinical practice. Oncol Nurs Forum. 1997;24(10):1695–1702.
London, F. Take the frustration out of patient education. Home Healthc Nurse. 2001;19(3):158–160.
Lorenzen, B., Melby, C., Earles, B. Using principles of health literacy to enhance the informed consent process. AORN J. 2008;88(1):23–29.
Lorig, K. Patient education: a practical approach, ed 3. Thousand Oaks, CA: Sage Publications, 2001.
Lorig, K., Holman, H. Self-management education: history, definition, outcomes and mechanisms. Ann Behav Med. 2003;26(1):1–7.
Lowenstein, A., Foord-May, L., Romano, J. Teaching strategies for health education and health promotion. Sudbury, MA: Jones and Bartlett, 2009.
Manning, S. The nurses I’ll never forget. Nursing. 1992;22(8):47.
Masters, K. Role development in professional nursing. Sudbury MA: Jones and Bartlett Publishers, Inc, 2008.
Mezirow, J. Fostering critical reflection in adulthood: a guide to transformative and emancipatory learning. San Francisco, CA: Jossey-Bass, 1990.
Perdue, B., Degazon, C., Lunny, M. Diagnoses and interventions with low literacy. Nurs Diagn. 1999;10(1):36–39.
Post-White, J. Wind behind the sails: empowering our patients and ourselves. Oncol Nurs Forum. 1998;25(6):1011–1017.
Ragland, G. Instant teaching treasures for patient education. St Louis: Mosby, 1997.
Redman, B.K. The practice of patient education: a case study approach, ed 10. St. Louis: Mosby, 2007.
Rogers, C. Freedom to learn for the ’80s. Columbus, OH: Merrill, 1983.
Rycroft-Malone, J., Latter, S., Yerrell, P., et al. Nursing and medication education. Nurs Stand. 2000;14(50):35–39.
Skinner, B.F. Beyond freedom and dignity. New York: Knopf, 1971.
Schumacher, K., Marren, J. Home care nursing for older adults: state of the science. Nurs Clin North Am. 2004;39:443–471.
Stephenson, P. Before the teaching begins: managing patient anxiety prior to providing education. Clin J Oncol Nurs. 2006;10(2):241–245.
Szpiro, K., Harrison, M., Van Den Kerkhof, Loutheed, M.D. Patient education in the emergency department. Adv Emerg Nurs J. 2008;30(1):34–49.
Taylor, C., Lillis, C., Lemone, P. Fundamentals of nursing: the art and science of nursing care, ed 5. Philadelphia: Lippincott Williams & Wilkins, 2005.
Wellard, S., Turner, D., Bethune, E. Nurses as patient-teachers: exploring current expressions of the role. Contemp Nurse. 1998;7(1):12–14.