Health Promotion and Client Learning Needs
At the end of the chapter, the reader will be able to:
1 Define health promotion and disease prevention and related concepts.
2 Identify national agendas for health promotion and disease prevention.
3 Describe relevant theory frameworks for health promotion strategies.
4 Apply health promotion and disease prevention strategies for individuals.
5 Apply health promotion strategies at the community level.
6 Discuss the role of learner variables in client education.
This chapter focuses on health promotion and disease prevention concepts used in health care. Included in the chapter are theory-based frameworks for health promotion as the starting point for improving the health of our nation and reducing health disparities. The chapter describes communication strategies designed to support clients, families, and targeted populations in achieving a better health quality of life, through education and lifestyle changes. The chapter addresses health literacy, readiness, and ability to learn as important components of health promotion/disease prevention efforts. A framework for developing and implementing community-based health promotion programs completes the chapter.
Basic concepts
Health and health promotion
The concept of health and its importance as an essential underpinning in nursing practice are explored from the perspective of the social determinants influencing health and well-being in this chapter. Quality of life is viewed as a constituent of health.
Contemporary thinking recognizes that many determinants of health and well-being are embedded in the economics, culture, and social community in which people live and work. Health communication is conceptualized as being more than simple information transfer. Clients are held accountable for their health care decisions and expected to actively participate in shared decision making with their health care providers. Client education is viewed as part of a larger context of health promotion and disease prevention strategies (Hoving, Visser, Mullen & Borne, 2010).
Health in 2010 is described as “being free from disease, being able to function normally, experiencing well-being, and having a healthy lifestyle” (Fagerlind et al., 2010, p. 104). Health is identified as a fundamental human right intimately tied to a nation’s social and economic development (Jakarta Declaration; World Health Organization [WHO], 1997). Engaging in activities to promote a healthy lifestyle is viewed as a personal responsibility. Clients are expected to actively change lifestyle behaviors and make treatment choices to enhance personal health and well-being. Contemporary thinking is that the dialogue between providers and clients about health should be an equal exchange of information. The emotional impact of the health disruption, environmental factors, and client preferences are parts of clinical assessment. A focus on teaching self-management skills, with clients taking primary responsibility for implementation, directs content in client-centered care (Hoving et al., 2010).
Health promotion is an interactive education and support process. It enables and empowers people to reach their highest health potential by taking control of and improving the circumstances pertaining to their health and well-being (Green, 2008). Health promotion and disease prevention activities are essential elements of U.S. health, as “treatment alone is unlikely to have marked effects on health inequities or health status” (Frankish et al., 2006, p. 271).
Health promotion is more than disease prevention. The concept of health promotion embraces resources and actions to improve quality of life and well-being. For health promotion activities to fully succeed, they need to address environmental circumstances that can be detrimental to a healthy living style, and include advocacy for change through health policy initiatives and social action. Reliable access to resources and leadership training are part of an essential infrastructure needed to support health promotion approaches in the community.
Organized health promotion strategies can target individuals, families, high-risk groups, or communities. Health promotion interventions focus on helping people develop the self-management skills they need to achieve maximum functional health and personal well-being. Examples range from coaching new mothers (individual) to parenting groups (group or community). Health promotion activities related to exercise, nutrition, job stress, and a balanced lifestyle are increasingly incorporated as essential components into occupational settings.
Health Promotion as a Population Concept: Health promotion as a population concept recognizes the community as its principal voice in assuming control of and improving health and well-being. Strategies involve organized actions and educational programs to support and inform individuals, families, and communities about better ways to improve and maintain a healthy lifestyle.
In 1986, the WHO’s Ottawa Charter for Health Promotion documented essential prerequisites and resources needed for health promotion as “peace, shelter, education, food, income, a stable ecosystem, sustainable resources, social justice, and equity” (WHO, 1986). Desired outcomes of health promotion activities are optimum health and well-being. The Jakarta Declaration on Health Promotion (1997) reaffirmed its relevance and called for the following actions:
Disease prevention
Health promotion and disease prevention are related concepts. Disease prevention is concerned with identifying modifiable risk and protective factors associated with diseases and disorders. Zubialde, Mold, and Eubank (2009) assert, “The goal of prevention is managing risk of future disease, disability, or premature death” (p. 194). Interventions are designed to help individuals at risk for chronic disease avoid the occurrence of a disease, disorder, or injury, to slow the progression of detectable disease and/or reduce its consequences (WHO, 1998).
The emphasis is always on averting health problems before they occur or decreasing their impact once the health problem occurs. Disease prevention activities involve proactive decision making at all levels of prevention (Edelman & Mandel, 1998). The three tiers of prevention—primary, secondary, and tertiary prevention—represent a continuum of health care delivery focus.
• Primary prevention strategies emphasize reduction of risk factors, including genetic susceptibility as a methodology for preventing the initial appearance of a disease or disorder. Strategies emphasize establishing and maintaining lifestyles favorable to health and well-being. Examples include prenatal clinics, parenting classes, and stress management programs. Nutrition, exercise, and environmental safety are other examples, easily incorporated into ordinary health teaching conversations.
• Secondary prevention involves interventions designed to promote early diagnosis of symptoms through health screening, or timely treatment after the onset of the disease, thus minimizing their effects on a person’s life. Examples include mammograms, diabetes, respiratory, and blood pressure screenings. Screening for mental health problems during the course of primary care visits can detect undiagnosed depression, anxiety, and substance abuse. Early diagnosis has a direct impact on the course and treatment of acute and chronic illness (WHO, 2008).
• Tertiary prevention describes rehabilitation strategies designed to minimize the handicapping effects of a disease or injury once it occurs. Examples include teaching a cancer victim to manage chemotherapy symptoms, helping a stroke victim with bladder retraining to avoid infection, and teaching a client to cope effectively with the necessary adjustments a serious physical, social, or emotional illness imposes.
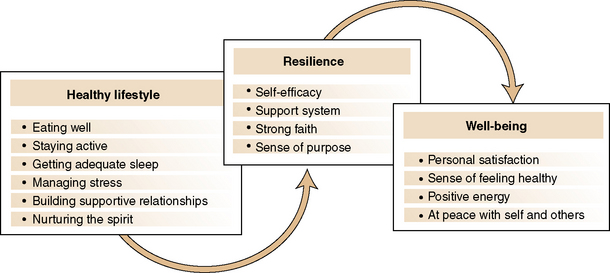
Well-being: Health promotion activities incorporate the WHO concept of an inseparable construct of health and well-being (Figure 15-1). Wellness or well-being is defined as a person’s subjective experience of satisfaction about his or her life related to six personal dimensions: intellectual, physical, emotional, social, occupational, and spiritual (Edlin & Golanty, 2009). People experience well-being as being at peace with themselves and others. People can experience well-being even with a serious health problem or terminal diagnosis (Saylor, 2004).
Lifestyle: Milio (1976) defines lifestyle as “patterns of choices made from the alternatives that are available to people according to their socioeconomic circumstances and the ease with which they are able to choose certain ones over others” (quoted in Cody, 2006, p. 186). The significance of this statement is that not everyone has the same options for having a healthy lifestyle.
Lifestyle factors are implicated as root factors in up to half of deaths in the United States (Edlin & Golanty, 2009). Deaths and chronic disease that compromise quality of life because of lifestyle factors can be prevented with changes in health habits. Chronic diseases and degenerative health conditions can be prevented or put off with changes in lifestyle. At the same time, it is important that lifestyle reflects socioeconomic and environmental circumstances such as diet, social isolation, lack of access, language barriers, and poverty. Action plans to help people take charge of their health and make a commitment to positive lifestyle changes must take into account the close relationship between individual factors and environmental supports in health promotion.
Ideally, building healthy lifestyles begins in childhood. As Frederick Douglass (Brainy Quotes, 2010) noted years ago, “It is easier to build strong children than to repair broken men.” Pender, Murdaugh, and Parsons (2006) identified six principles for achieving a healthy lifestyle: eating well, staying active, getting adequate sleep, managing stress, building supportive relationships, and nurturing one’s spirit. Comprehensive health promotion activities focused on individuals and their families, set within community, and larger ecosystem initiatives produce the best benefit, particularly when paired with social and resource support.
Resilience: Resilience is defined as “strength in the midst of change and stressful life events; the power of springing back or recovering readily from adversity” (Chapman, Lesch, & Aitken, 2005, p. 4). Resilience is a concept that helps explain why some people seem to weather adversity more easily than others and are able to grow from the experience. People can do this more easily when their stress is balanced with mechanisms to help them process it, and they acquire the skills they need to move forward with their lives (Schieveld, 2009). Psychosocial resilience is associated with self-efficacy, developing an organized way of coping with stressors, and the cultivation of a meaningful support system. A strong faith and sense of purpose also are factors (Freedman, 2008).
National health promotion and disease prevention agendas
The Committee on Assuring the Health of the Public in the 21st Century (2003) has cited three major trends influencing health care in the United States:
1. Demographic changes with the “population growing larger, older, and more racially and ethnically diverse, with a higher incidence of chronic disease”
2. Technical and scientific advances, which “create new channels for information and communication, as well as novel ways of preventing and treating disease”
3. “Globalization and health, to include the geopolitical and economic challenge of globalization, including international terrorism” (pp. 34–41)
Healthy people: national health promotion and disease prevention agendas
Each decade, the U.S. Department of Health and Human Services (HHS) publishes an updated health promotion and disease prevention agenda for the nation with specific national goals and objectives. Healthy People 2010 (HHS, 2000) presents the health promotion and disease prevention agenda for the nation. The third document of its kind, Healthy People 2010 puts forth 28 focus areas with corresponding national health objectives designed to identify and reduce the most preventable threats to health. Federal agencies intimately involved with health care developed the document with input from more than 350 national membership organizations and 250 state health, mental health, substance abuse, and environmental agencies.
The overarching goals for Healthy People 2010 are to “achieve increased quality and years of healthy life and the elimination of health disparities” (U.S. Department of Health and Human Services, HHS, 2002). Healthy People 2010 provides strong support for the nation’s move from a predominantly medical model of health care to a public health model. It incorporates the most relevant scientific expertise on health care as the basis for evaluating leading health indicators against outcome benchmarks for preventive health care. Each leading health indicator listed in Box 15-1 has associated objectives.
Healthy People 2020 is conceptualized as continuing earlier Healthy People initiatives related to addressing environmental factors contributing to the health status of individuals and populations, with a stronger focus on action plans and strategies. The vision for Healthy People 2020 is to have “a society in which all people live long, healthy lives” (U.S. Department of Health and Human Services, HHS, 2010). Proposed overarching goals to achieve this vision include the following:
• Eliminate preventable disease, disability, injury, and premature death.
• Achieve health equity, eliminate disparities, and improve the health of all groups.
• Create social and physical environments that promote good health for all.
• Promote healthy development and healthy behaviors across every stage of life.
Action models, proposed to achieve these goals, will provide clear priorities for what needs to be done, with focused strategies for addressing each goal. Objectives are projected to be organized in three categories—interventions, determinants, and outcomes—rather than in specific focus areas. More information about recommendations for the framework and format for Healthy People 2020 is available online (www.healthypeople.gov/HP2020).
Centers for disease control and prevention
Surveillance of health events is an important component of population-focused health promotion and disease prevention because it alerts health care providers to potential and actual health problems, and provides morbidity and mortality rates for evaluation purposes. The Centers for Disease Control and Prevention (CDC) is “the nation’s premiere health promotion, prevention and preparedness agency and a global leader in public health” (CDC, 2006). It is the operational part of the HHS, which is directly responsible for protecting the health and safety of the nation’s citizens and is committed to achieving improvement in people’s health. As such, it is an important resource for health promotion activities.
The CDC collects data about the incidence and prevalence of diseases and chronic illnesses, and ranks illnesses that kill Americans. It tracks the development of new health problems and illnesses appearing in the United States and is recognized globally for its dedication to promoting people’s health and well-being. This agency provides funding to states to implement health programs for Americans, and funding to developing countries related to prevention and treatment of AIDS. The CDC applies research findings to improve people’s daily lives. State and municipal health departments receive support from the CDC to detect and reduce health threats from bioterrorism. The CDC has four health promotion impact goals:
• Healthy people in every stage of life: All people, and especially those at greater risk for health disparities, will achieve their optimal life span with the best quality of life in every stage of life.
• Healthy people in healthy places: The places where people live, work, learn, and play will protect and promote their health and safety, especially those at greater risk for health disparities.
• People prepared for emerging health threats: People in all communities will be protected from infectious, occupational, environmental, and terrorist threats.
• Healthy people in a healthy world: People around the world will live safer, healthier, and longer lives through health promotion, health security, and health diplomacy (CDC, n.d.).
In 2001, the Institute of Medicine (IOM) published a landmark report, Crossing the Quality Chasm: A New Health System for the 21st Century, which identified six areas of focus for improvement of health care. The areas identified for health care improvement (Table 15-1) have relevance for preventive interventions. A second report in 2006 outlined recommendations to improve the quality of health care for mental and substance-use conditions (IOM, 2006).
TABLE 15-1
Institute of Medicine’s Six Aims for Improvement of Health Care
| Aim | Descriptor |
| Safe | Avoiding injuries to patients from the care that is intended to help them |
| Effective | Providing services based on scientific knowledge to all who could benefit and refraining from providing services for those not likely to benefit |
| Patient centered | Providing care that is respectful of and responsive to individual patient preferences, needs, and values, and ensuring that patient values guide all clinical decisions |
| Timely | Reducing waits and sometimes harmful delays for both those who receive and those who give care |
| Efficient | Avoiding waste, including waste of equipment, supplies, ideas, and energy |
| Equitable | Providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status |
Source: Institute of Medicine: Crossing the quality chasm: a new health system for the 21st century (p. 3), Washington, DC, 2001, Author.
Theory frameworks for health promotion
Theory frameworks for health promotion focus on how people make choices and decisions about their health. Redman (2004) suggests that the health belief model, the transtheoretical model, and social learning theory are particularly relevant in health education for self-management of chronic diseases. This section presents three theoretical frameworks, each of which takes into consideration a person’s beliefs about his or her ability to determine and influence health status and well-being.
Pender’s health promotion model
Pender’s (2006) revised health promotion model expands on an earlier health belief model developed by Rosenstock and his associates in the 1950s. The health belief model proposed that a person’s willingness to engage in health promotion behaviors is best understood through examining a person’s beliefs about the seriousness of a health condition and his or her capacity to influence its outcome.
Nola Pender’s revised health promotion model continues to include perceived benefits, barriers, and ability to take action related to health and well-being as important components of people’s health decision making. Added to these prior considerations is an emphasis on personal factors, including interpersonal influences and situational pressures, that can sway a person’s commitment to plan of action and health-promoting behaviors (Figure 15-2). Taken together, these dynamics act as internal or external “cues to action” influencing a person’s decision to seek health care or to engage in health-promoting activities. Examples include required school immunizations; interpersonal reminders, such as a family member’s experience with the health care system; the mass media; and ethnic approval. Using the health promotion model allows nurses to understand each person’s combination of personal and behavioral variables as a consideration in choosing the best approach to engage a client in advancing health and well-being.
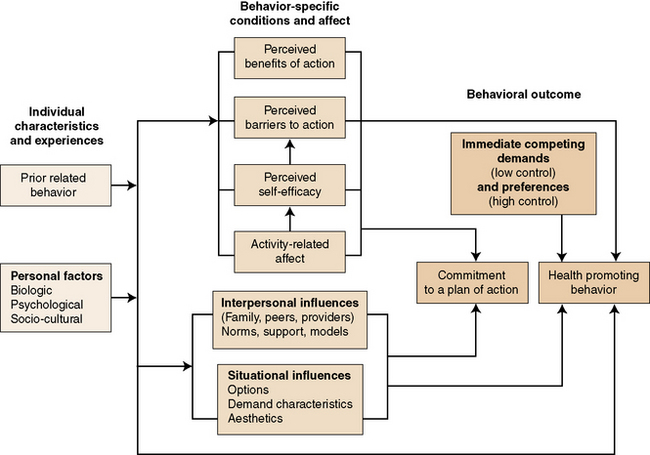
Figure 15-2 Health promotion model. (From Pender N: Health promotion in nursing practice (p. 50), Upper Saddle River, NJ, 2006, Prentice Hall.)
Exercise 15-1 provides practice with applying Pender’s health promotion model to common health problems.
Transtheoretical model of change
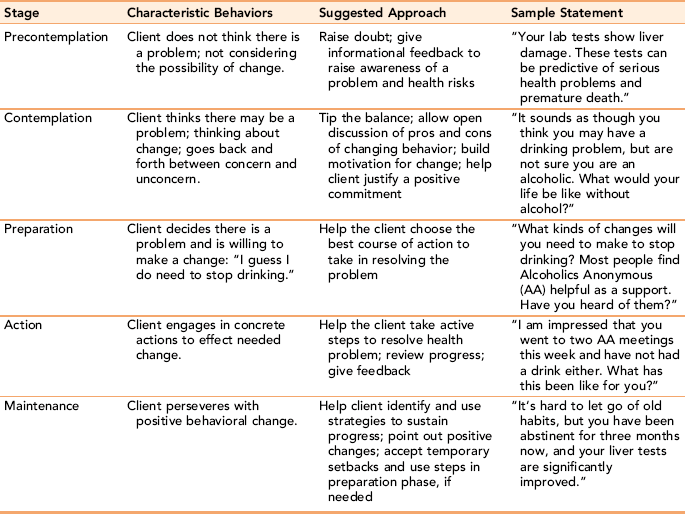
Prochaska’s model provides a simple way to help identify the motivational readiness of people to engage in specific health-promoting behaviors (Daley, Fish, Frid, & Mitchell, 2009; Prochaska, DiClemente, & Norcross, 1992). The transtheoretical model of change recognizes the difficulty most people have with changing longstanding unhealthy lifestyle habits. Their model describes motivation to change as a state of readiness, which fluctuates and can be influenced by external encouragement (DiClemente, Schlundt, & Gemmell 2004). The model identifies five stages through which people make a decision to make an intentional behavioral change and carry through with implementation.
The transtheoretical model proposes that the client’s intrinsic motivation is key to behavioral change and establishing preventive health behavior practices. Even people who are highly resistant to change can be motivated to change unhealthy behaviors. Assessment of the client’s motivation, or lack thereof, is coupled with targeted interventions to match an individual’s level of motivation or “readiness” to change the behavior. When motivational strategies match an individual’s readiness, the likelihood that the client will follow a recommended course of action toward behavior change increases. The strategies challenge, support, and accept the client’s readiness to change as the starting point for intervention.
The transtheoretical model is not a linear model. Clients can cycle through one or more of the stages several times before a permanent change takes place. Longstanding habits are hard to break. Setbacks and relapse with return to old behaviors can be expected, with an assumption that people will learn from the experience. Table 15-2 presents Prochaska’s Model of Change with suggested approaches for each stage and corresponding sample statements.
TABLE 15-2
Prochaska’s Stages of Change with Suggested Approaches and Sample Statements Applied to Alcoholism
Exercise 15-2 provides an opportunity to work with the transtheoretical model in understanding learning readiness.
Motivational interviewing
Motivational interviewing (MI) is “theoretically congruent” with the transtheoretical model of behavior change (Goodwin, Bar, Reed & Ashford, 2009, p. 204). Originally conceptualized for use in the treatment of alcoholism, the MI framework is used with a growing range of chronic health conditions that are caused by or exacerbated by unhealthy lifestyle behaviors, for example, diabetes and obesity (Carels et al., 2007; Kirk, Mutrie, Macintyre, & Fisher, 2004).
MI is an evidenced-based treatment approach to helping clients address resistance or ambivalence about health-related lifestyle changes. Motivational learning represents an interactive process in which the clinician strives to learn about the client’s goals, values, and concerns as they relate to consideration of targeted health behavior changes. Developed by Miller and Rollnick (2002), MI is part of a cooperative partnership between client and clinician characterized by “an active collaborative conversation and joint decision making process” (Rollnick, Miller, & Butler, 2008, p. 6). Strategies include listening carefully to the client’s description of the problem and the client’s ideas about how the problem might be resolved. This step is followed by mutually exploring the pros and cons of each proposed solution. It is important for the nurse to express empathy for the challenges faced by the client and to affirm the client’s opinions and progress (Levensky, Forcehimes, O’Donohue, & Bietz, 2007).
A motivational framework to change unhealthy behaviors is based on a person’s values, beliefs, and preferences and fits well with the current emphasis on client-centered health care (Miller, 2004; Sandelowski, DeVellis, & Campbell, 2008). The client and clinician form a collaborative relationship in which they are equal partners, each contributing a knowledge and expertise to the situation. The clinician provides guidance, knowledge, and support. The final decision is always the client’s responsibility. A critical component of MI is an acceptance of the client’s right to make the final decision and the need for the clinician to honor each client’s right to do so.
Social learning theory
Bandura’s (1997) contribution to the study of health promotion is his concept of self-efficacy. He believed that self-efficacy, described as a personal belief in one’s ability to execute the actions required to achieve a goal, is a powerful mediator of behavior and behavioral change. Having self-confidence in one’s ability to determine and implement actions has a direct influence on motivation and readiness to learn.
Self-efficacy and motivation are reciprocal processes; increased self-efficacy strengthens motivation, which, in turn, strengthens the client’s capacity to complete the learning task. A person’s perception of his her capability is a strong motivator even if it is not completely validated by the reality of the person’s abilities. This is a critical concept because both clients and family caregivers may have reservations about their competence to carry out treatments in the home or make changes in lifestyle. Providing support at critical junctions can improve motivation and beliefs in one’s ability to master essential tasks. Mastery is considered to be the strongest foundation of self-efficacy (Srof & Velsor-Friedrich, 2006).
Bandura considers learning to be a social process. He identified three sets of motivating factors that promote the learning necessary to achieve a predetermined goal: physical motivators, social incentives, and cognitive motivators. Physical motivators can be internal, such as memory of previous discomfort or a symptom that the client cannot ignore. Social incentives such as praise and encouragement increase self-esteem and give the client reason to continue learning.
Bandura refers to a third set of motivators as cognitive motivators, describing them as internal thought processes associated with change.
Below, the nurse combines the concept of a physical motivator with a social incentive related to something the client values (his grandson). The intervention is designed to help Francis recognize how changes in his health behavior can not only improve his health and well-being but give him a social outlet that could be important to him.
Nurse: I’m worried that you are continuing to smoke, because it does affect your breathing. There is nothing you can do about the damage to your lungs that is already there, but if you stop smoking it can help preserve the healthy tissue you still have (physical motivator) and you won’t have as much trouble breathing. I bet your grandson would appreciate it if you could breathe better and be able to play with him (social incentive). As Francis notices that he is coughing less when he gives up smoking, this new perceptual knowledge can act as an internal cognitive motivator to remain abstinent.
Applications
Applying health promotion and disease prevention strategies
The American Association of Colleges of Nursing (2008) identifies health promotion and disease prevention at individual and population levels as an essential component of professional nursing practice. It can be integrated informally into everyday nursing care, and formally in client education and screening programs. Nurses can play an important role in health promotion and disease prevention regardless of whether they work in primary or hospital care settings.
Nurses have unique opportunities to include primary and secondary prevention strategies with clients during routine health maintenance examinations and routine treatment. In the 21st century, health promotion strategies should be a part of everyday nursing care (Beckford-Ball, 2006). All nurses can participate in health screenings and client education. Examples of individualized health promotion strategies include encouraging regular medical checkups, providing client education, and offering health screenings to promote health and prevent disease (Maltby & Robinson, 1998).
Health promotion instruction can focus on condition-specific topics, or they can emphasize general education about healthy lifestyles. Condition-specific activities might include anticipatory guidance, and coaching for new mothers and caregivers of clients with chronic illness. Secondary prevention strategies focus on lifestyle/rehabilitative planning and interventions for clients with chronic conditions such as cardiac disorders or diabetes.
General education strategies related to positive lifestyle habits would emphasize diet, physical activity, regular sleep patterns, and stress reduction. Exercise 15-3 provides an opportunity to develop your own personal health portfolio.
A wide variety of topics lend themselves to health promotion focus. A sampling includes the following:
• Alcohol, nicotine, and other drug abuse prevention
• Prevention and early detection of common chronic diseases such as diabetes, cancer, heart disease, osteoporosis, co-occurring disorders
• Behaviors needed for a healthy lifestyle
• Family issues related to communication and parenting
• Job stress and burnout prevention for informal caregivers and at work sites
Promoting health for individuals
MI emphasizes a person’s capacity to take charge of their health and to master the lifestyle factors that interfere with optimal health and well-being. The communication process starts with establishing a collaborative relationship with a client and family before beginning to assess their readiness for change. You can use the stages of change identified in Table 15-2 to determine where you should start. Focusing on the family’s beliefs and values about health behaviors allows nurses to ease into a dialogue in which clients explore the pros and cons of different behaviors. Open-ended questions that place health issues within the context of everyday life provide broader information about issues that otherwise might not be identified. For example, asking a client about exercise may yield a one-sentence answer. Asking the same client to describe his activity and exercise during a typical day, and what makes it easier or harder for him to exercise provides better data. Potential concerns about strategies that may not be consistent with values, preferences, or goals are more readily identified. Client-centered and family perspectives on disease and treatment are not necessarily the same as those of their health care providers.
Assessment of social and environmental supports is important. Because perception of self-efficacy and competence influences a person’s willingness to participate in health-promoting behaviors, the assistance and support that others can provide to enable client success is critical. With this information, nurses are able to tailor their interventions to the client’s capacity to change. Although initially an MI approach may take a little longer, it is likely to be more effective because the client chooses actions with personal meaning and will be more committed to it.
Nurturing the development of self-efficacy helps people to feel more confident. Opportunities for shared decision making and learning self-management skills empower clients to take an active role in treatment and health promotion activities (Hoving et al., 2010). Nurses empower clients and families through provision of accurate, timely information, coaching supports, and targeted links to health screening and community services. Educational and referral supports enable clients and families to learn the skills they need to effectively manage chronic conditions and to live a healthy lifestyle. Helping people use technology to find information and resources is another form of encouraging clients to take charge of their health and well-being.
Gance-Cleveland (2007) suggests setting an agenda with clients as a way of determining what is most important to clients and what they are willing to change. Effective health promotion activities perceived as being relevant are more likely to produce positive results. Tailoring instruction and coaching to the needs, abilities, and characteristics of the client and/or target population is important.
Timing is important for full effectiveness. For example, providing pregnant mothers with a tour of the obstetrics (OB) unit and providing information before admission is more effective than providing it after admission.
Working with Disparities: Although disparities refer to differences in health across ethnic groups, gender, education, or income, the term usually is associated with inequalities in access, service use, and health outcomes. Although major advances in health care have occurred since the beginning of the 21st century these developments have not benefited target health populations equally (Kline & Huff, 2008, p. 180),
People with the greatest health burdens often have the least access to information, communication technologies, health care, and supporting social services. For example, people living in extreme poverty may not have access to preventive care, adequate nutrition, or the opportunity to live in a healthy environment, because of finances. They may not even think about it because they are at the survival level. Noting environmental deficits in the client’s environment that are beyond individual control can help you tailor meaningful health promotion supports.
Health promotion and disease prevention strategies help people to recognize health problems and support them in choosing the most effective ways to self-manage their symptoms in the community. In many instances, clients presenting with physical complaints in primary care have an underlying mental disorder or substance abuse problem. Making it a practice to assess for mental problems and co-occurring disorders during intake with a few well-placed questions can help detect mental health issues or negative substance use.
Nurses use one-to-one counseling and community-based group education formats to meet educational health care objectives related to health promotion and maintenance of health, prevention of illness, restoration of health, coping with impaired functioning, and rehabilitation.
Health promotion strategies at the community level
At the community level, nurses help locate populations at risk for health problems. They can use casefinding strategies to recognize individuals and families with identified risk factors and to connect them with needed supports, resources, and services. Uncovering unhealthy physical and social environments or living circumstances can start within the formal health system during intake, or informally through liaisons with the justice system and schools.
Nurses can help design and provide health education, social marketing, and screening services to targeted populations with unrecognized health risk factors. They can instruct targeted populations about the nature of an illness, disability, or unhealthy environment, and the use of their medications. Nurses can identify what community supports are available, and/or how services can be obtained and how to access them. Examples include drug prevention and teenage pregnancy prevention programs, plus one-on-one coaching with step-by-step instructions on how to access critical supports.
Community-based health promotion strategies
Although health promotion strategies at the individual level are associated with improved health and well-being, health promotion is also a community concept. It is difficult to change attitudes and lifestyles to promote health when a client’s social environment does not support these changes. Reducing generic environmental risks to maintaining health and well-being requires a community approach to health promotion.
Community is defined as “any group of citizens that have either a geographic, population-based, or self-defined relationship and whose health may be improved by a health promotion approach” (Frankish et al., 2006, p. 174). Equity and empowerment related to health care are the expected outcome of health promotion activities at the community level. Equity corresponds to the WHO directive that all people should have an equal opportunity to enjoy good health and well-being.
Empowerment at the community level recognizes the need for citizen participation in improving and promoting health. Community empowerment “seeks to enhance a community’s ability to identify, mobilize, and address the issues that it faces to improve the overall health of the community (Yoo, Weed, & Lempa, 2004, p. 256).
Unless the community as a whole can collectively challenge and eradicate inequities in health care access and treatment provision, health promotion activities will fall short of their targeted goals (Messias, De Jong, & McLoughlin, 2005). Health promotion activities use a proactive approach to capture the attention of people who otherwise might not be predisposed to taking charge of their health and/or may not know that they are at risk.
Grass roots health promotion activities provided for “at-risk” populations are a community resource designed to influence personal lifestyle choices, coping skills, and health behaviors. They are designed to engage those people who are most involved with a common environmental concern related to health as active participants. Key health issues in economically disadvantaged communities often are those with social roots such as violence or abuse, substance abuse, teen pregnancies, and AIDS (Blumenthal, 2009). Socioenvironmental factors that affect health include income, education, health insurance, cultural health practices, social support, and accessibility of health services.
Successful health promotion programs require individuals, groups, and organizations to act as active agents in shaping health practices and policies that have meaning to the target population. Community-based health promotion activities must be grounded in a community analysis of health issues of concern, as identified by the community itself. They must begin with an engagement and buy-in of the community in which the activity is to take place. WHO notes that health promotion activities should be “carried out by and with people, not on, or to people” (Jakarta Declaration; WHO 1997). Active participation of individuals, communities, and systems means a stronger and more authentic commitment to the establishment of realistic regulatory, organizational, and sociopolitical supports needed to achieve targeted health outcomes (Kline & Huff, 2008).
Using the precede-proceed model in community education
Community education is an important component of health promotion and disease prevention. The precede-proceed community-based health education model that Green and Kreuter (2005) developed is based on two fundamental assumptions: (1) health and health risks are multidetermined, and (2) health teaching must be multidimensional and participatory to be effective.
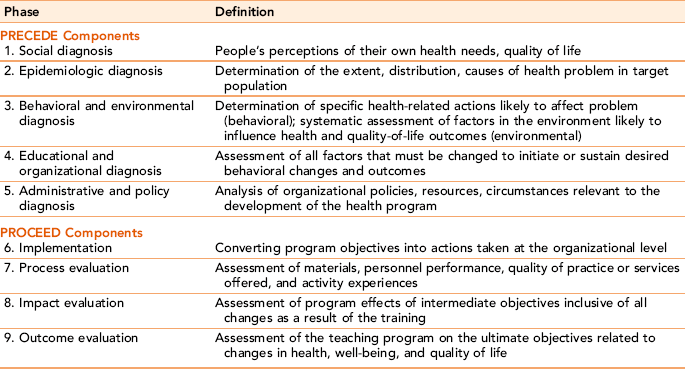
The PRECEDE component of the health education model refers to the assessment and planning components of program planning. The acronym PRECEDE stands for Predisposing, Reinforcing, Enabling Causes in Educational Diagnosis and Evaluation factors associated with the targeted problem area. Examples of these diagnostic behavioral factors are presented in Table 15-3. Careful assessment of these factors provides direction for the type of program and content most likely to engage the interest of diverse learners in community-based settings. The PRECEDE assessment takes place as a part of the planning process before the educational program is offered. Nurses also determine population needs and establish evaluation methods before implementation. Evaluation is a continuous process that begins when the program is implemented, and is exercised throughout the educational experience.
TABLE 15-3
PRECEDE-PROCEED Model: Examples of PRECEDE Diagnostic Behavioral Factors
| Factors | Examples |
| Predisposing factors | Previous experience, knowledge, beliefs, and values that can affect the teaching process (e.g., culture and prior learning) |
| Enabling factors | Environmental factors that facilitate or present obstacles to change (e.g., transportation, scheduling, and availability of follow-up) |
| Reinforcing factors | Perceived positive or negative effects of adopting the new learned behaviors, including social support (e.g., family support, risk for recurrence, and avoidance of a health risk) |
The PROCEED component (Policy, Regulatory, Organizational Constructs in Educational and Environmental Development) was added to the model by Green in the late 1980s. He realized that any viable educational model needed political, managerial, and administrative supports for full implementation of a community-based approach to health promotion and disease prevention. The utility of including the PROCEED component is that it explicitly considers critical environmental and cost variables such as budget, personnel, and critical organizational relationships as part of the planning process. Having the resources in place and assessing their sustainability is important in health promotion planning, though it is not always thought through in the planning phase. Bernard (2006) also observes that, because health promotion and disease prevention activities do not generate the same level of revenue, they may not be as sustainable when resources become tight. Nurses can play an important role in advocating for public policies supporting sustainable access to appropriate health resources. The full PRECEDE-PROCEED model is presented in Table 15-4. Exercise 15-4 provides an opportunity to think about community health problems that could be addressed with the PRECEDE-PROCEED model in planning appropriate health promotion interventions.
Learner variables in education for health promotion
Pender’s health promotion model serves as a guide for planning successful education with individuals and targeted high-risk groups. A person’s capacity to absorb and use health promotion information depends to a large degree on what the person believes about his or her health, and the extent to which personal actions will influence their health. Nurses can use the health belief model to focus on behaviors that have the greatest potential to meet specific health needs. Examples of health promotion education topics can relate to sexual health; developing a healthy lifestyle through eating well, physical activity, and stress reduction; organizational wellness; parenting skills; and anger management.
Guidelines proposed by the U.S. Preventive Services Task Force for health-promoting education and counseling are presented in Box 15-2. As with all types of education and counseling, learners need to be actively engaged in goal setting and developing action plans that have meaning to them. Choosing the right strategies requires special attention to the learner’s readiness, capabilities, and skills (see Chapter 16).
Ochieng (2006) contends that socioeconomic factors, level of education, age, and social networks are important contributors to understanding client preferences and working with clients to enable them to make the changes needed for a healthy lifestyle.
Clients requiring the same education program may demonstrate a wide range of learning, cognitive, experiential, and communication diversity, which may require adaption to maximize learning. Clients also will differ in their intellectual curiosity, learning preferences, motivation for learning, learning styles, and rate of learning.
Teaching and counseling initiatives related to health promotion need to be safe, timely, effective, client centered, equitable, and efficient. Health promotion programs should be designed to empower clients through an emphasis on the active role of the client as a stakeholder and inclusion in all aspects of the health promotion process.
Education and counseling for health promotion can include information on risk factors or behaviors impacting on health and ways to address negative social, economic, and environmental determinants of health. A health promotion format considers a person’s personal values and beliefs about his or her ability to achieve health behavior changes (self-efficacy) as part of client assessment.
Evaluation of health promotion activities is essential. In addition to evaluating immediate program effects, longitudinal evaluation of the impact of health promotion activities on morbidity, mortality, and quality of life is desirable. Keep in mind that what constitutes quality of life is a subjective reality for each client and may differ from person to person (Fagerlind et al., 2010).
Empowerment strategies
There seems to be little question of a “direct relationship between an individual’s level of health and the amount of perceived control the individual has in life situations” (Sheinfeld-Gorin & Arnold, 2006, p. 135). Empowering people to take the initiative with their own health and well-being is the cornerstone of health promotion and disease prevention strategies.
Information to empower clients in learning about healthy lifestyles, treatment, and potential side effects is readily available through the Internet (Coward, 2006). For many illnesses and health problems, clients and families can find specific information, regardless of the stage of their illness. Online support groups, chat rooms, and sharing of patient and family stories provide additional social support and practical learning tips for people who live in areas that are not geographically convenient to person-to-person contact. In the community, support groups are available for a wide variety of diagnoses. If the client or family does not use the Internet, flyers, fact sheets, and direct dialogue with opportunity for questions and follow-up can be helpful.
Active involvement of the learner enhances learning. Most people learn best when they engage more than one sense in the learning process and have an opportunity to practice essential skills. A highly participatory learning format, one that encourages different ways of thinking and opportunities to try out new behaviors, is far more effective than giving simple instructions to a client or family, or demonstration without teach back feedback (Willison, Mitmaker, & Andrews, 2005).
Strategies should demonstrate a sensitive appraisal and choice of targeted strategies, matched to the relevant needs of the individual, family, or group. When time is short, you will need to focus on the health teaching that addresses the most pressing of health needs. Many of the teaching learning strategies presented in Chapter 16 can be used or modified for health promotion health teaching. Exercise 15-5 provides an opportunity to use Maslow’s theory in structuring health promotion activities.
Community Empowerment
Social and political action to enhance health services can augment educational efforts using a PRECEDE-PROCEED framework at the community level. Community empowerment strategies are used to help identify and address environmental and social issues needed to improve the overall health of the community.
Empowerment at the community level is sometimes referred to as “capacity building.” Community-focused empowerment strategies build on the personal strengths, community resources, and problem-solving capabilities already existing in individuals and communities that can be used to address potential and actual health problems (Leddy, 2005). Capacity building requires the inclusion of informal and formal community leaders as valued stakeholders. Networking, partnering, and creating joint ventures with indigenous and local religious infrastructures is a powerful consensus building strategy needed for effective health promotional education planning and implementation. Box 15-3 outlines a process for engaging the community in health promotion activities.
Health Literacy
Parker, Ratzan, and Lurie (2003) define health literacy as “the degree to which people have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions” (p. 194). Approximately 21% of U.S. adults would be classified as functionally illiterate, which means they read at or below a ninth grade level and would have trouble comprehending written instructions on medication bottles, negotiating the health care system, and fully understanding consent forms (Davis et al., 1998). Health literacy can be further compromised with visual or auditory impairment, or diminished mental alertness, acute illness, limited education, and cultural differences. Health literacy is more than the capacity to read. It also includes medical knowledge, system navigational skills and initiative (Dewalt & Pignone, 2005).
Low health literacy is associated with medication nonadherence, increased incidence of side effects, and inadequate understanding of the impact of a medication on health outcomes (Ownby, 2006). People with inadequate health literacy tend to have worse health status, and functional physical and mental health. They also are less likely to seek preventive health care (Baker et al., 2002; Cutilli, 2007).
Low health literacy is not the same as having below average intelligence. People with inadequate health literacy may be highly intelligent, but functionally unable to fully grasp medical terminology. People with English as a second language can exhibit a much lower level of functional health literacy that is directly attributable to language limitations. Others demonstrate a lower level of functional literacy related to limited education or learning disabilities.
A persistent stigma about low literacy and learning disabilities exists even though it is unfounded. For this reason, many people try to hide the fact that they cannot read or do not know the meaning of complex words. They feel ashamed, so they fake their inability to understand by appearing to agree with the nurse educator, by saying they will read the instructions later, or by not asking questions. Functional illiteracy influences the type of questions a client might ask of a health professional and the adequacy of their descriptions about their illness or disability. Some of the problems clients with low literacy skills have in accessing health information include the following:
• Taking instructions literally
• Having a limited ability to generalize information to new situations
• Decoding one word at a time rather than reading a passage as a whole
• Skipping over uncommon or hard words
• Thinking in individual rather than categorical terms (Doak, Doak, & Root, 1996)
Educationally disadvantaged or functionally illiterate people are interested in learning, but nurses should adapt teaching situations to accommodate literacy learning differences. Marks (2009) suggests having written materials modified to six- to eighth-grade reading levels, and providing lists of key instructions for use after visits.
Using symbols and images with which the client is familiar helps overcome the barriers of low literacy. Taking the time to understand the client’s use of words and phrases provides the nurse with concrete words and ideas that can be used as building blocks in helping the client understand difficult health-related concepts. Otherwise, the client may misunderstand what the nurse is saying.
Safeer and Keenan (2005) suggest that clients can understand medical information better when a small amount of information is presented slowly, in easily understood everyday words. . Box 15-4 identifies guidelines for teaching low-literacy clients. Nurses should keep instructions as simple as possible, presenting ideas in an uncomplicated, step-by-step format. Advance organizers help low-literacy clients remember important concepts (see Chapter 16). Familiar words supplemented by common related pictures provide an extrasensory input for the client and improve retention. Drawings, diagrams, and photographs provide additional cues, allowing the client to understand meanings he or she would be unable to grasp through words alone.
Use common concrete words rather than abstract or medical terminology and examples, for example, “Call the doctor on Monday if you still have pain or swelling in your knee.” In addition to using simple words and literal interpretations, the nurse should use the same words to describe the same thing. For example, if you use “insulin” in one instance and “medicine” or “drug” later to describe the same medication, the client may become confused. The same instructions, written exactly as they were spoken, act as a reminder once the person leaves the actual teaching situation.
Sequence the content logically beginning with a core concept. Remember that the client with low health literacy may not be able to read or interpret the label instructions on the bottle. You can use the following question sequence to teach a client about taking a new medication.
Apply simple concrete common words such as “You should take your medicine with your meals,” or “Call your doctor if you have stomach pain.” Teach a little at a time. Select small, related pieces of data and structure them into informational chunks so that the client can remember the information through association, even if one fact is forgotten.
Whenever possible, link new information and tasks with what the client already knows. This strategy builds on previous knowledge and reinforces self-efficacy in mastering new concepts. Keeping sentences short and precise, and using active verbs helps clients understand what is being taught. When technical words are necessary for clients to communicate about their condition with other health professionals, clients may need direct instruction or coaching about appropriate words to use. Table 15-5 presents core constructs of health literacy.
TABLE 15-5
Core Constructs of Health Literacy
| I. Basic Literacy or Comprehension | Reading information, appointment cards |
| Interpreting medical tests, dosages, and instructions, side effects, contraindications | |
| Understanding brochures, medication labels, informed consent, insurance documents | |
| II. Interactive and Participatory Literacy (able to engage in two way Interactions) | Provision of appropriate and usable information Comprehension and ability to carry out information Mutual decision making Remembering and carrying out information |
| III. Critical literacy | Ability to weigh critical scientific facts Capacity to assess competing treatment options |
Adapted from Marks R: Ethics and patient education: Health literacy and cultural dilemmas, Health Promot Pract 10(3):328–332, 2009.
Developmental Level
Developmental level affects both teaching strategies and subject content. You will find that clients are at all levels of the learning spectrum with regard to their social, emotional, and cognitive development. Developmental learning capacity is not always age related. It is easily influenced by culture and stress. Social and emotional development does not always parallel cognitive maturity. Mirroring the client’s communication style and framing messages that reflect developmental characteristics helps improve comprehension and understanding. Parents can provide useful information about their child’s immediate life experiences and commonly used words to incorporate in health teaching.
Culture
Culture adds to the complexity of health promotion strategies in health care. Values, norms, and beliefs are an integral part of a person and heavily influence collective community lifestyles (See Chapter 11). Culture helps explain assumptions about health and illness, the causes of and treatments for different types of illnesses, and traditionally accepted health actions or practices to prevent or treat illness. Incorporating health-related cultural beliefs in health teaching promotes better acceptance.
In many cultures, the family assumes a primary role in the care of the client even when the client is physically and emotionally capable of self-care. All parties needing information, especially those expected to support the learning process of the client, should be included from the outset in all aspects of health teaching for health promotion. “Empowering ethnocultural communities through informal care may be the most culturally appropriate approach for improving the health status of ethnocultural populations” (Chiu, Balneaves, & Barroetavena 2006, p. 3)
Client motivation and participation increase with the use of indigenous teachers and cultural recognition of learning needs. If health literacy is related to language, qualified interpreters should be used for translation and preparation of written materials.
The culturally sensitive nurse develops knowledge of the preferred communication style of different cultural groups and uses this knowledge in choosing teaching strategies. For example, Native Americans like stories. Their tradition of telling stories orally is a primary means of teaching that the nurse can use as a teaching methodology for health promotion purposes.
Self-Awareness
Nurses have an ethical and legal responsibility in health teaching to maintain the appropriate expertise and interpersonal sensitivity to client needs required for effective learning. It is easy enough to remain engaged and to provide interesting teaching formats for the self-directed, highly motivated learner. It takes much more energy and imagination to impart hope to clients and to stimulate their emotions and interest when they see little reason to participate in learning about lifestyle changes and self-care management. Although the nurse is responsible for the quality of health teaching, only the client can assure the outcome. At all times, the nurse respects the client’s autonomy. Some clients want symptom relief, whereas others want more in-depth teaching. Nurses have an ethical responsibility to provide appropriate health teaching and the right to hope that if the information is not used now, perhaps later it will be.
Summary
This chapter focuses on health promotion as the basis for health education that can be applied at all practice levels. The WHO describes health promotion as a process of enabling people to increase control over and improve their health. Optimal health and well-being are considered the desired outcomes of health promotion activities. A health promotion/disease prevention focus views the client as an informed consumer and a valued partner in health care. Theory models relevant to health promotion include Pender’s health promotion model, Prochaska’s transtheoretical model, Miller’s MI, and Bandura’s social learning theory.
Learner variables important to the success of health promotion activities can be categorized as readiness to learn and ability to learn. Physical factors, level of anxiety, level of social support, active involvement of the learner, and inclusion of family members are identified as elements of readiness to learn. Lack of appropriate supports, physical barriers, health literacy, culture, and developmental status are factors that may influence the client’s ability to learn.
Nurses participate routinely in community health promotion and disease prevention activities. They have an ethical and legal responsibility in health teaching to maintain the appropriate expertise and interpersonal sensitivity to client needs required for effective learning.
References
American Association of Colleges of Nursing. The essentials of baccalaureate education for professional nursing practice. Washington DC, 2008. [Author].
Bandura, A. Self-efficacy: the exercise of control. New York: WH Freeman, 1997.
Baker, D.W., Gazmararian, J.A., Williams, M.V., et al. Functional health literacy and the risk of hospital admission among medicare managed care enrollees. Am J Public Health. 2002;92(8):1278–1283.
Beckford-Ball, J. The essence of care benchmark for patient health promotion. Nurs Times. 2006;102(14):23–24.
Bernard, M. Health promotion/disease prevention: tempering the giant geriatric tsunami. Geriatrics. 2006;61(2):5–7.
Blumenthal, D.S., Clinical community health: revisiting “the community as patient. Educ Health, 2009;22(2):1–8. available online, http://www.educationforhealth.net.
Brainy Quotes. Frederick Douglas. available online http://www.brainyquote.com/quotes/quotes/f/frederickd201574.html. [Accessed, August 2, 2010].
Carels, R., Darby, L., Cacciapaglia, H., et al. Using motivational interviewing as a supplement to obesity treatment: a stepped-care approach. Health Psychol. 2007;26(3):369–374.
Centers for Disease Control. CDC: our story. available online http://www.cdc.gov/about/ourstory.htm, 2006.
Chapman, L., Lesch, N., Aitken, S. WELCOA Special report: Resilience, Omaha NE, Wellness Councils of America, 2005. www.welcoa.org/freeresources/pdf/resilience_case_study.pdf. [Accessed August 2, 2010].
Chiu, L., Balneaves, L., Barroetavena, M., et al. Use of complementary and alternative medicine by Chinese individuals living with cancer in British Columbia. J Compl Integr Med. 2006;3(1):1–21.
Cody, W. Philosophical and theoretical perspectives for advanced practice nursing, ed 4, Sudbury MA: Jones and Bartlett Publishers; 2006:183–190.
Collier, S. Mrs. Hixon was more than “the C.V.A. in 251. Nursing. 1992;22(5):62–64.
Committee on Assuring the Health of the Public in the 21st Century (Institute of Medicine). The future of the public’s health in the 21st century. Washington, DC: National Academies Press, 2003.
Coward, D. Supporting health promotion in adults with cancer. Fam Community Health. 2006;29(Suppl 1):S52–S60.
Cutilli, C. Health literacy in geriatric patients: an integrative review of the literature. Orthop Nurs. 2007;26(1):43–48.
Daley, L., Fish, A., Frid, D., Mitchell, L. Stage specific education/counseling intervention in women with elevated blood pressure. Prog Cardiovasc Nurs. 2009;24(2):45–52.
Davis, T., Michielutte, R., Askov, E., et al. Practical assessment of adult literacy in health care. Health Educ Behav. 1998;22(5):613–624.
Dewalt, D.K., Pignone, M. The role of literacy in health and health care. Am Fam Physician. 2005;72(3):387–388.
DiClemente, C., Schlundt, B., Gemmell, B. Readiness and stages of change in addiction treatment. Am J Addict. 2004;13(2):103–119.
Doak, C.C., Doak, L.G., Root, J.H. Teaching patients with low literacy skills. Philadelphia: JB Lippincott, 1985.
Doak, C.C., Doak, L.G., Root, J.H. Teaching patients with low literacy skills, ed 2. Philadelphia: JB Lippincott, 1996.
Edelman, C., Mandel, C. Health promotion throughout the lifespan, ed 4. St Louis: Mosby Year Book, 1998.
Edlin, G., Golanty, E. Health and wellness, ed 10. Sudbury, MA: Jones & Bartlett Publishers, 2009.
Fagerlind, H., Ring, L., Brulde, B., Feltelius, N., Lindblad, A. Patients’ understanding of the concepts of health and quality of life. Patient Educ Couns. 2010;78:104–110.
Frankish, C.J., Moulton, G., Rootman, I., et al. Setting a foundation: underlying values and structures of health promotion in primary health care settings. Prim Health Care Res Dev. 2006;7:172–182.
Freedman, R. Coping, resilience, and outcome. Am J Psychiatry. 2008;165(12):1505–1506.
Gance-Cleveland, B. Motivational interviewing: improving patient education. J Pediatr Health Care. 2007;21:81–88.
Goodwin, A., Bar, B., Reid, G., Ashford, S. Knowledge of motivational interviewing. J Holist Nurs. 2009;27(3):203–209.
Green, J. Health education—the case for rehabilitation. Crit Public Health. 2008;18(4):447–456.
Green, L., Kreuter, M. Health program planning: an educational and ecological approach, ed 4. New York: McGraw Hill, 2005.
Hoving, C., Visser, A., Mullen, P.D., van den Borne, B. A history of patient education by health professionals in Europe and North America. Patient Educ Couns. 2010;78(3):275–281.
Institute of Medicine (IOM). Crossing the quality chasm: A new health system for the 21st century. Washington DC: National Academy Press; 2001.
Institute of Medicine (IOM). Improving the quality of health care for mental and substance-use conditions: The quality chasm series. Washington DC: National Academy Press; 2006.
Kirk, A., Mutrie, N., Macintyre, P., Fisher, M. Promoting and maintaining physical activity in people with type 2 diabetes. Am J Prevent Med. 2004;27:289–296.
Kline, M., Huff, R. Health promotion in multicultural populations: a handbook for practitioners and students, ed 2. Thousand Oaks, CA: Sage Publications, 2008.
Leddy, S. Integrative health promotion: conceptual bases for nursing practice. Sudbury, MA: Jones and Bartlett Publishers, 2005.
Levensky, E., Forcehimes, A., O’Donohue, W., Beitz, K. Motivational interviewing: an evidence-based approach to counseling helps patients follow treatment recommendations. Am J Nurs. 2007;107(10):50–58.
Maltby, H., Robinson, S. The role of baccalaureate nursing students in the matrix of health promotion. J Community Health Nurs. 1998;15(3):135–142.
Markle-Reid, M., Weir, R., Browne, G., et al. Health promotion for frail older home care clients. J Adv Nurs. 2006;54(3):381–395.
Marks, R. Ethics and patient education: health literacy and cultural dilemmas. Health Promot Pract. 2009;10(3):328–332.
Messias, D., De Jong, M., McLoughlin, K. Being involved and making a difference: empowerment and well-being among women living in poverty. J Holist Nurs. 2005;23(1):70–88.
Miller, W. Values and motivational interviewing: a symposium. Minuet. 2004;11(3):19–20.
Miller, W., Rollnick, S. Motivational interviewing: preparing people for change, ed 2. New York: Guilford Press, 2002.
Milio, N. A framework for prevention: changing health-damaging to health-generating life patterns. Am J Public Health. 1976;66:435–439.
Ochieng, B. Factors affecting choice of a healthy lifestyle: implications for nurses. Br J Community Nurs. 2006;11(2):78–81.
Ownby, L. Medication adherence and cognition: medical, personal and economic factors influence level of adherence in older adults. Geriatrics. 2006;61(2):30–35.
Parker, R., Ratzan, S., Lurie, N. Health illiteracy: a policy challenge for advancing high-quality health care. Health Aff. 2003;22(4):147–153.
Pender, N., Murdaugh, C., Parsons, M. Health promotion in nursing practice, ed 4. Upper Saddle River, NJ: Prentice Hall, 2006.
Prochaska, J., DiClemente, C., Norcross, J. In search of how people change: applications to addictive behaviors. Am Psychol. 1992;47(9):1102–1114.
Redman, B. Patient self management of chronic disease: the health care provider’s challenge. Sudbury, MA: Jones and Bartlett Publishers, 2004.
Rollnick, S., Miller, W., Butler, C. Motivational interviewing in health care: helping patients change behavior. New York: Guilford Press, 2008.
Safeer, R.S., Keenan, J. Health literacy: the gap between physicians and patients. Am Fam Physician. 2005;72:463–468.
Sandelowski, M., DeVellis, B., Campbell, M. Variations in meanings of the personal core value “health”. Patient Educ Couns. 2008;73(2):347–353.
Saylor, C. The circle of health: a health definition model. J Holist Nurs. 2004;22(2):98–115.
Schieveld, J. On grief and despair versus resilience and personal growth in critical illness. Intens Care Med. 2009;35:779–780.
Sheinfeld-Gorin, S., Arnold, J. Health promotion in practice. San Francisco, CA: Josey Bass, 2006.
Srof, B., Velsor-Friedrich, B. Health promotion in adolescents: a review of Pender’s health promotion model. Nurs Sci Q. 2006;19(4):366–373.
U.S. Department of Health and Human Services (HHS). Healthy people 2010. Washington, DC: U.S. Government Printing Office, 2000.
U.S. Department of Health and Human Services (HHS). Healthy people 2020. available at www.healthypeople.gov/HP2020. [Accessed April 18, 2010].
U.S. Preventive Services Task Force. Guide to Clinical Preventive Services, 2nd ed. Baltimore: Williams and Wilkins, 1996.
Willison, K., Mitmaker, L., Andrews, G. Integrating complementary and alternative medicine with primary health care through public health to improve chronic disease management. J Complement Integr Med. 2005;2(1):1–24.
World Health Organization, Geneva, Switzerland. Health promotion glossary, 1998. [Author].
World Health Organization. Jakarta declaration on leading health promotion into the 21st century. 1997, available online < www.who.int/hpr/NPH/docs/jakarta_declaration_en.pdf. [> Accessed, October 3, 2009].
World Health Organization (WHO), Ottawa, Ontario, Canada. Ottawa Charter for Health Promotion: First International Conference on Health Promotion, 1986. November 21available online, http://www.who.int/healthpromotion/conferences/previous/ottawa/en/. [Accessed September 21, 2009].
World Health Organization (WHO) and World Organization of Family Doctors (WONCA) (2008). Integrating mental health into primary care: a global perspective. Geneva, Switzerland: WHO Press, 2008.
Yoo, S., Weed, N., Lempa, M., et al. Collaborative community empowerment: an illustration of a six-step process. Health Promotion Pract. 2004;5(3):256–265.
Zubialde, J., Mold, J., Eubank, D. Outcomes that matter in chronic illness: a taxonomy informed by self-determination and adult-learning theory. Fam Syst Health. 2009;27(30):193–200.