Communicating with Clients in Stressful Situations
At the end of the chapter, the reader will be able to:
1 Define stress and associate concepts.
2 Describe biological and psychosocial models of stress.
3 Identify concepts related to coping with stress.
4 Discuss stress assessment strategies.
5 Describe stress reduction strategies nurses can use in stressful situations.
This chapter provides a framework for understanding basic concepts of stress, and supporting client and family coping with stress through the nurse-client relationship. Included in the chapter are physiologic and psychological models of stress reactions, and descriptions of behaviors associated with stress reactions. The chapter addresses nursing interventions and communication strategies nurses can use to help people cope more effectively with stress.
Basic concepts
Stress represents a natural physiologic, psychological, and spiritual response to the presence of a stressor. Stress feelings set into motion an immediate emergency physiologic response to real or perceived threats. Normally, the stress response turns off when the immediate danger has passed.
A stressor is defined as a demand, situation, internal stimulus, or circumstance that threatens a person’s personal security or self-integrity. Stressors can be catastrophic (war, hurricane, earthquake), related to a major life change (marriage, divorce, death, moving to a new area), or experienced as a minor hassle (traffic jam, child misbehavior, computer crashes).
Stressors can be potential, actual or imagined, and negative or positive. Illness, significant loss (e.g., job or relationship, home), a move to a different city, and loss of income can create negative stress. A job promotion, impending wedding and birth of a child are positive events that can be stressors. Box 20-1 lists personal sources of stress.
Stressors likely to stimulate an intense stress response are those in which a person has limited control over the situation, the situation is ambiguous, or the current situation resembles unresolved stressful events in the past. Concurrent and cumulative stressors increase the stress response level. The intensity and duration of stress varies according to the circumstances, level of social support, and the emotional state of the person. People have different tolerance levels for stress. Some people are highly sensitive to any stressor, others are more laid-back and have selective responses to stressful circumstances. Stress reduces the efficiency of cognitive functions and reduces access to previous knowledge. Caplan (1981) emphasizes the importance of community education, and socio-cultural support as a way to compensate for perceptual deficits and minimize the impact of negative stress.
Characteristics of stress
Hans Selye used the term eustress to describe a short-term, mild level of stress. It acts as a positive stress response with protective and adaptive functions, and is perceived as being within the person’s ability to manage. Distress is defined as a negative stress that causes a higher level of anxiety, and is perceived as exceeding the person’s coping abilities. It is experienced as being unpleasant and diminishes performance.
Current research suggests that men and women respond to stress differently. Men respond with patterns of “fight or flight,” whereas women use a “tend and befriend” approach. Women use nurturing activities to reduce stress and promote safety for self and others. They seek social support from others, particularly from other women (Taylor, Klein, Lewis, Gruenewald et al. 2000). Children express stress through behavior, according to their stage of development, and family patterns. Acting out behaviors can mask a child’s distress.
Levels of stress
Mild stress can be beneficial. It helps people stay focused and alert. Mild stress serves as a motivator to develop skills to meet challenges and accomplish goals. Awareness of personal strengths and mastery of coping strategies learned in mastering a stressful situation helps people cope better in other life circumstances (Aldwin & Levenson, 2004).
Moderate stress occurs when people experience frustration or conflict over an inability to change a desired outcome through their own efforts. When people are stressed, they are more susceptible to illness (Dolbier, Smith & Steinhardt (2007). Chronic stress is implicated in the development and exacerbation of cardiac conditions, migraine, and digestive disorders. Stress create comorbidities between physical disease and mental disorder (Askew & Keyes, 2005).
High stress levels interfere with a person’s ability to function because anxiety reduces a person’s objectivity. People have trouble envisioning possibilities, weighing options, making choices, and taking action. They can exhibit anger, anxiety, and depressive symptoms. Severe or chronic stress weakens the immune system, thereby contributing to the development of stress-related illnesses (Martin, Lae, & Reece, 2007). Untreated, severe mental stress reactions associated with traumatic events can develop into post-traumatic syndrome, a clinical disorder. Stress and coping is said to account for up to 50% of the variation in psychological symptoms (Sinha & Watson, 2007).
Biological and psychosocial models of stress
Walter Cannon (1932) was the first to describe a scientific physiologic basis for an acute stress response. Cannon believed that when people feel physically well, emotionally centered, and personally secure, they are in a state of dynamic equilibrium or homeostasis. Stress disturbs homeostasis. Physiologically, the sympathetic-adrenal medulla system in the brain sets into motion an immediate hormonal cascade designed to mobilize the body’s energy resources to cope with acute stress.
Cannon proposed that people attempt to adapt to stress with either a “fight or flight” response. The fight response refers to a person’s inclination to take action against a threat if the threat appears to be resolvable, and the flight component, to flee, if it is unlikely that the threat can be overcome.
General adaptation syndrome
Stress hormone levels generally revert to normal once the cause of the stress is resolved. Hans Selye (1950) expanded on Cannon’s work in describing responses to longer term stress exposure. He described a three-stage progressive pattern of nonspecific physiologic responses, which he branded as alarm, resistance, and exhaustion. The alarm stage is similar to Cannon’s acute stress response, characterized by increased activity in the hypothalamic-pituitary-adrenal (HPA) axis. Corticosteroids are released, which mobilizes the body’s energy resources. If the stressor is not resolved in the initial alarm stage, a second adaptive phase referred to as “resistance” occurs as the body tries to accommodate for the stressor. In the resistance stage, the alarm symptoms subside as the immune system helps the body to adapt as best it can. Although the acute stress symptoms seem to disappear, the body functions less efficiently, and the resistance stage drains productive energy. If the body fails to adapt, or is still unable to resist the continued stress, it leads to “exhaustion.” In the exhaustion stage, people are at high risk for stress-related illness or mental disorder.
The same physiologic response occurs regardless of whether a stressor is psychological or physical. Activation of the HPA axis occurs with the stress of critical illness, surgery, trauma, and emotional disorders (Johnson & Renn, 2006). The longer the physiologic responses remain elevated, the greater its negative effect on the organism.
Allostasis
A recent theory of stress response challenges the idea that physiologic systems respond to stressors as an attempt to achieve a fixed level of homeostasis (Sterling & Eyer, 1988). Allostasis describes how the organism achieves homeostasis through adaptation, referred to as “stability through change” (McEwen, 2000, p. 1219). The interaction between stressors and physical responses is ongoing such that individuals become more or less susceptible to the negative consequences of stress over time.
The brain serves as a “primary mediator” between the “current stressor exposure, internal regulation of bodily processes, and health outcomes” (Ganzel, Morris, & Wethington, 2010, p. 134). The brain determines what experiences are threatening or nonthreatening, and the physiologic response requirements of each situation. It tries to find a new homeostasis that better fits the requirements of the environmental stressor, using a range of adaptive functioning (allostatic accommodation). The inclusion of genetic risk factors, early life events, and lifestyle behaviors in the model offers a way to understand the interaction between stressful events and physiologic adaptation processes (McEwen & Wingfield, 2003). Figure 20-1 identifies relationships in the allostasis model.
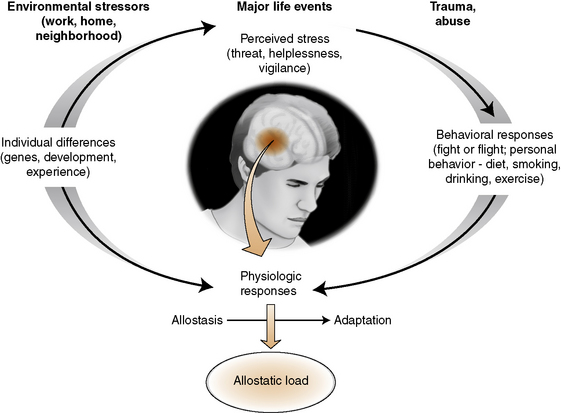
Stress hormones protect the body against short-term acute stress (allostasis). Stress mediators, such as social support, are capable of producing protective effects. When small or moderate levels of stressor exposure are encountered, and social support is available, the outcome is increased health and functioning. If a stressor continues, presents repeated challenges, or stress responses are ineffective, there is “wear and tear” on the body, which can have a damaging effect. McEwen (2007) terms this phenomena allostatic load. The allostatic load can be negligible or severe and protracted enough to result in significant illness or death.
Stimulus stress model
In 1967, Thomas Holmes and Richard Rahe developed a stress model that considered stressful life events such as marriage, divorce, death, losing a job, and so on as stimuli that threaten or disrupt homeostasis. The Holmes and Rahe scale gave each individual life event a weighted numerical score reflecting its stress impact on a person. Stressors requiring a significant change in the lifestyle of the individual have greater impact, as do cumulative stresses occurring within a short time. The quantity and severity of stressors influence a person’s potential for developing later physical illness.
Transactional model of stress
Lazarus and Folkman’s (1984) transactional model of stress is one of the most widely used to explain stress responses. It is based on the premise of a stressful experience is the result of a transaction between a situation or circumstance in the environment (stressor) and the individual experiencing the stressor. The transaction is the dynamic that accounts for a stressor’s impact on a person. A person’s perception of stressful events and interpretation of its meaning, and not the objective stress value of a stressor, determines the stress response.
Stress responses to cumulative daily stressors are a primary focus of the transactional model (Neale, Arentz, & Jones-Ellis, 2007). The model asserts that stress is as likely to occur with daily “hassles” as it is with major life events. The transactional model considers appraisal of stressors and coping strategies as a primary emphasis.
Primary and Secondary Appraisal: A person’s interpretation of a stressful event is the result of two levels of cognitive appraisal. A primary appraisal initially evaluates the magnitude of the stressor, followed by a secondary appraisal evaluating an individual’s perceived ability to cope with it (Figure 20-2). Both are required to determine whether a stressor will be appraised as harm, threat, or challenge (Folkman, 2008).
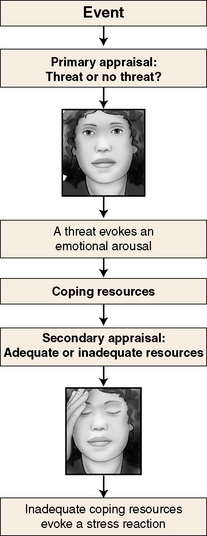
Primary appraisal focuses on the stressor or stressful event itself—its content and strength as a personal threat. A person determines whether an event is stressful and draws one of three conclusions: It is not stressful, it is a relatively benign stressor, or it poses a significant threat to self-integrity. Stressors perceived as a major threat to self elicit a stronger stress response, for example, losing an important relationship or being diagnosed with a serious illness. Primary stress appraisals can include threat of harm or losses that are anticipated but have not yet occurred.
When a primary cognitive appraisal determines a stressor to be a significant threat, the person automatically switches to a secondary appraisal related to coping skills. Secondary appraisal involves a person’s perception of personal coping skills and the availability of resources in the environment to aid in reducing stressor impact.
Coping with stress
Knowledge of coping is essential to understanding how stress affects people (Skinner, Edge, Altman, & Sherwood, 2003). Coping strategies can reduce or increase the effects of stressors and the development of distress. In their classic work, Pearlin and Schooler (1978) define coping as “any response to external life strains that serves to prevent, avoid, or control emotional distress” (p. 2). They identify three purposes of coping strategies:
• To change the stressful situation
• To change the meaning of the stressor
• To help the person relax enough to take the stress in stride
People learn coping strategies from parents, peers, and the circumstances life presents to them. Those with a variety of life opportunities and supportive people in their lives have an advantage over people who lack either opportunity or support system. People who have been overprotected or have been exposed to danger without support or mentoring generally lack experience with coping skills. Exercise 20-1 helps identify adaptive and maladaptive coping strategies in your life.
Types of coping strategies
Lazarus and Folkman (1984) identify two types of coping. Problem-focused coping strategies use approach behaviors, for example, confronting a problem directly, seeking social support, and constructive problem solving. Negotiation, directly confronting challenging issues, and taking action are deliberately used to change a stressful situation. Recognition of personal and outside resources can foster options, and people who have options generally are better able to cope with stress. Balancing coping resources include health, energy, problem-solving skills, the amount and availability of social supports and other material resources to cope effectively with the stressor. Individuals who are generally capable, have financial resources, and are by nature optimistic typically handle stress more easily.
Emotion-focused coping refers to avoidance behaviors that serve to distance the person from stress. They can be helpful alone or in combination with problem-solving strategies when people are faced with overwhelming irreversible situations.
Research suggests that constructive emotion-focused coping, featuring change in attitude, acceptance, and emotional respite from overthinking about a stressful situation, is associated with positive outcomes (Mohr, Goodkin, Gatto, & Van der Wende, 1997). Emotion-focused coping can be a positive realistic choice when a situation cannot be changed, and the person deliberately chooses to “let go” of negative feelings associated with it. Most people use both types of coping strategies, with the choice of strategy being somewhat dependent on the nature of the stressor.
Helping clients and families develop a different perspective can be just as important as the more traditional problem-solving strategies used to cope with stress (Michalenko, 1998).
Defensive Coping Strategies: People need time to absorb the meaning of a serious stressor. As a short-term coping strategy, defense mechanisms can be temporarily adaptive in minimizing the threat of a potentially overwhelming stressor (Richards & Steele, 2007). As a primary stress reducer, and over time, defense mechanisms are ineffective because they serve as a disincentive to action. Ego defense mechanisms represent a largely unconscious pattern of coping that people use to protect the self from full awareness of challenging conflict situations. They are designed to protect the ego from anxiety and loss of self-esteem by denying, avoiding, or attributing responsibility for a challenging conflict to an external source. Persistent use of ego defense mechanisms as a primary coping strategy generally is considered pathologic, although a few have positive value. Recent authors (Reich, Zautra and Hall, 2010; Vaillant and Mukamal, 2001) contend that healthy defense mechanisms; humor, anticipation, affiliation (asking for help) and sublimation can be adaptive and are associated with resilience. For example, sublimation is used to channel extreme anger impulses into acceptable behaviors, for example, by becoming a butcher or boxer. Table 20-1 provides definitions and examples of common defense mechanisms.
TABLE 20-1
| Ego Defense Mechanism | Clinical Example |
| Regression: returning to an earlier, more primitive form of behavior in the face of a threat to self-esteem | Julie was completely toilet trained by 2 years. When her younger brother was born, she began wetting her pants and wanting a pacifier at night. |
| Repression: unconscious forgetting of parts or all of an experience | Elizabeth has just lost her job. Her friends would not know from her behavior that she has any anxiety about it. She continues to spend money as if she were still getting a paycheck. |
| Denial: unconscious refusal to allow painful facts, feelings, or perceptions into awareness | Bill Marshall has had a massive heart attack. His physician advises him to exercise with caution. Bill continues to jog 6 miles a day. |
| Rationalization: offering a plausible explanation for unacceptable behavior | Annmarie tells her friends she is not an alcoholic even though she has blackouts, because she drinks only on weekends and when she is not working. |
| Projection: attributing unacceptable feelings, facts, behaviors, or attitudes to others; usually expressed as blame | Ruby just received a critical performance evaluation from her supervisor. She tells her friends that her supervisor does not like her and feels competitive with her. |
| Displacement: redirecting feelings onto an object or person considered less of a threat than the original object or person | Mrs. Jones took Mary to the doctor for bronchitis. She is not satisfied with the doctor’s explanation and feels he was condescending, but says nothing. When she gets to the nurse’s desk to make the appointment, she yells at her for not having the prescription ready and taking too much time to set the next appointment. |
| Intellectualization: unconscious focusing on only the intellectual and not the emotional aspects of a situation or circumstance | Johnnie has been badly hurt in a car accident. There is reason to believe he will not survive surgery. His father, waiting for his son to return to the intensive care unit, asks the nurse many questions about the equipment, and philosophizes about the meaning of life and death. |
| Reaction formation: unconscious assuming of traits opposite of undesirable behaviors | John has a strong family history of alcoholism on both sides. He abstains from liquor and is known in the community as an advocate of prohibition. |
| Sublimation: redirecting socially unacceptable unconscious thoughts and feelings into socially approved outlets | Bob has a lot of aggressive tendencies. He decided to become a butcher and thoroughly enjoys his work. |
| Undoing: verbal expression or actions representing one feeling, followed by expression of the direct opposite | Barbara criticizes her subordinate, Carol, before a large group of people. Later, she sees Carol on the street and tells her how important she is to the organization. |
It is important to remember most ego defense mechanisms are unconscious. Because a defensive reframing of a conflict in a person’s mind is usually not under the conscious control of the client, it is difficult to help them consider alternative coping strategies without support. Challenging defense mechanisms directly usually is not successful. The Prochaska model and motivational interviewing (see Chapter 15) offer guidelines for gently casting doubt, providing new information and introducing problem-solving strategies to assist clients in positively reframing secondary appraisals.
Social support
Social support is a key factor in alleviating stress and promoting the self-efficacy people need for successful coping and mastery of stress (Caplan, 1981). Social support is defined as the emotional comfort, advice, and instrumental assistance that a person receives from other people in their social network (Taylor, Welch, Kim, & Sherman, 2007). Social support has three distinct functions: validation, emotional support, and correction of distorted thinking. Social support can refer to both the “perceived availability of help, or support actually received (Schwarzer & Knoll, 2007, p. 244). A person’s social networks are drawn from family, friends, church, work, social groups, or school. Being able to contact family and friends when you need an emergency babysitter or an extra hand in a stressful situation immediately lessens stress.
Social support allows for honest sharing of feelings and concerns in an emotionally supportive relationship. Not only does sharing with others reduce stress by “externalizing” negative emotions, but family and friends can provide a sounding board, practical assistance, and tangible encouragement. Seeking help can empower both seeker and provider of emotional support. Sharing a laugh, eating a meal with others, and being in good company helps people feel more relaxed, which, in turn, reduces stress levels.
Social support does not have the same meaning for all cultures in terms of self-disclosure. Taylor et al. (2007) report that Asian American clients may be more comfortable with an implicit form of social support that does not require extensive sharing of thoughts. Examples of implicit social support include showing kindness, caring, acceptance, and positive regard for a client.
Applications
Stress can worsen almost any illness. Factors that influence the impact of stress are identified in Box 20-2. Addressing relevant issues and teaching clients related coping strategies as early as possible enhances recovery potential. Clients and family members usually welcome an opportunity to tell their story and talk about concerns beyond the concrete needs of a stressful situation.
Understanding how a stressful event relates to other life issues, including stressors from the past, and current financial or family concerns puts the current stressor in context. Ask open-ended questions about changes in daily routines, new roles and responsibilities, and the client/family’s understanding of diagnosis and treatment options.
Pay attention to cultural values. What is a small stressor in one culture can be huge in another, and normal coping strategies can be quite different. When clients present with stress-related symptoms, an initial assessment should include:
• Identification of stress factors the person is experiencing, including which one(s) is causing the most stress
• Perception of stressor as being harmful, threatening, or challenging
• Value or meaning attached to the stressor
• Identification of usual coping strategies and methods used to cope with current stressors
• Assessment of linked or underlying issues such as developmental stage, culture, family understandings, and level of support
Identifying sources of stress in health care
Disruptions in health status create stress, anxiety, and vulnerability. Health-related stressors for clients and families include fear of death, uncertainty about clinical outcome, changes in roles, disruption of family life, and financial concerns created by the hospitalization (Leske, 1998).
Hospitalization intensifies stress. Hospital-related stress can negatively impact client outcomes, level of satisfaction with care, and compliance with treatment. Examples include physical discomfort, strange noises and lights, unfamiliar people asking personal questions, and strange equipment. Clients and their families experience anxiety with transfer to the intensive care unit, and again when they are preparing to a step-down or regular unit, and still again when they are transitioning to home (Chaboyer, James, & Kendall, 2005). Providing immediate practical and emotional support during each of these transitions can reduce unnecessary stress. Box 20-3 provides an assessment/intervention tool that you can use to organize assessment data and plan interventions.
A client-centered approach involves differentiating the type of stress a client is experiencing. For example, stress perceived as a threat provokes anxiety, whereas stress associated with loss presents as depression and grief. The strategies that nurses would use to help clients reduce their stress would differ based on the source of the stress. When stress presents as anxiety, the nurse might suggest problem-solving techniques. However, if the stress is related to a significant loss, the nurse would want to focus on the loss and work with the client from a grief perspective.
Behavioral Observations: Distress often presents through behavior rather than being communicated with words. Emotional distress in collectivistic cultures, for example, Hispanic and Asian, are commonly expressed through somatic symptoms (Lehrer, Woolfolk, & Sime, 2007). Physical and mental symptoms of stress include:
• Significant changes in eating or sleeping habits
• Headaches, gastric problems, muscular tension, aches and pains, tightness in the throat
• Restlessness and irritability
• Inability to cope with normal everyday concerns and obligations
Anger, hostility, shame, embarrassment, dread, and social withdrawal are behaviors associated with anxiety. Stress anxiety can present as emotional numbness, feelings of going crazy, a déjà vu experience, or night terrors. Other symptoms can include inability to recall information, blocked speech, and fear of losing control (Arnold, 1997).
Putting your observations into words helps clients link emotional states to specific stress reactions using words rather than behavior. For example, you might say, “This (name stressor) must be very upsetting,” or “It seems like you are pretty anxious about…” If individual clients feel uncomfortable about talking about stress initially, let them know that you will be there when they do feel like talking. When people can put their needs and behaviors in words, they experience less anxiety. They need additional information and frequent support delivered in a calm, competent manner.
Anger and Hostility: Anger and hostility are the most common stress emotions associated with feeling helpless or psychologically threatened. Blame is a frequent form of hostility. Family members angrily blame each other for an injury, blame the physician for operating (or not operating) on a loved one, and criticize the nurse for not responding quickly enough.
Anger projected on the nurse can temporarily threaten a nurse’s involvement. Recognizing hostility as a cry for help in coping with escalating stress makes it easier to respond empathetically. Most outbursts have little to do with you, personally, other than that you are available, you are the one most involved with the care of the loved one, and you are least likely to retaliate.
Reflecting on how hostility relates to underlying anxiety helps nurses remain empathetic. Often, people become hostile when they don’t understand what is happening or have little control over a treatment outcome. What a hostile anxious client or family needs most at that moment, despite their behavior, is understanding, comfort, and human caring. Listen, ask, and respond empathetically to contributory themes and feelings.
Allow verbal venting within reason. Set limits if necessary, but do so with a calm attitude and manner. Carefully listening to a client’s concerns goes a long way toward neutralizing anger and hostility. The client feels heard, even if the issues cannot be fully resolved to the client’s satisfaction. In the course of the conversation, both nurse and client can sort out how the client perceptually experiences a stressor as a basis for focusing on productive solutions. Exploring anger and anxiety as a normal response to stress allows a conversational space to contradict false information. If client and/or family expectations are unrealistic, or can’t be met in the current situation, alternative explanations and suggestions can be introduced. Exercise 20-2 is designed to address the relationship between anger and anxiety.
Assessment of coping skills
Assessment of a client’s coping behaviors and social support network is critical to understanding stress from a holistic perspective. Ask about coping strategies a client has used in the past and what the person is currently using to resolve stress. Relevant issues include those about the cultural meanings of stressors and typical family coping strategies. Sample questions might include:
• What kinds of things increase your stress?
• What leisure activities do you engage in?
• What do you do to relieve your stress?
• What are your usual methods of coping when you do not feel stress?
Nurses should ask these questions using an informal conversational format. Clients will feel more comfortable if their nurse presents an open, nonthreatening stance and a calm attitude. Appearing patient, being willing to listen, and being attentive without being intrusive is reassuring to anxious clients. The client’s reactions will serve as a guide as to how much and how quickly the information can be gathered.
Assessment of immediate social support
Asking questions about how the client and family is coping with the current situation provides useful contextual data. Stress-related family assessments can include the following questions:
• Does the family perceive the stressors in the same way as the client?
• Have important issues been discussed fully?
• To what extent are family values challenged by the current situation?
• How might the family and client work together to improve their stress management skills?
• Are family members and the client communicating with each other?
Because family members can be a major support for clients experiencing stress, nurses can inquire about their willingness to be involved with a different set of questions.
• What are the family’s and client’s expectations of care?
• In what ways, if any, are the expectations different?
• What does the family or client need from you as the nurse? From each other?
• Is there a family spokesperson?
• What are the client’s cultural, religious, and family values concerning the meaning of the stressor?
Identifying sources of strength and hope
In times of stress, people, particularly women, will reach out to others for solace, support, and direction (Taylor et al., 2000; Taylor, 2006). Some people turn to their God or Higher Power, others to family and friends. People without a social network should be linked with community resources, the point being that interpersonal connection is an essential buffer against stress. Community resources include support groups, social services, and other public health agencies that provide practical support, as well as social contacts. The more knowledgeable the nurse is about community resources, the better the client and family are served. Exercise 20-3 is designed to help you become better acquainted with resources in your community.
Stress challenges and/or strengthens people’s spirituality. Health disruptions bring mortality and morbidity into sharper relief as personal issues. This is because before having a significant illness or a life-changing health-related crisis, people don’t think about their personal death or the fact that a life can be changed completely. They haven’t seen firsthand the effects of death or potentially lethal complications of disorders.
Belief in a personal God provides interested clients with an incomparable personal resource that helps them cope with shattered dreams and incomprehensible life crises. Some people rely on faith to facilitate their acceptance of a reality that cannot be changed. Stress can challenge a person’s spiritual connections and it is not uncommon for people to experience a spiritual void in stressful times. Assessing and providing spiritual comfort to clients is an important consideration in caring for clients experiencing stress.
Assessing impact on family relationships
Nurses play an important role in helping client families reduce their own stress levels in health care situations. They can help families process complex information and address specific concerns. Topics can include what will happen next, how to explain the illness, or what the client or family could have done differently to change the situation. For example, the nurse might say to the wife of a recent paraplegic, “Seeing your husband like this must be a terrible shock. I suspect you might be wondering how you are going to cope with his care at home.” This type of statement normalizes feelings and introduces subjects that are difficult but necessary to talk about. Table 20-2 identifies interventions to decrease family stress.
TABLE 20-2
Nursing Interventions to Decrease Family Anxiety
| Recommendation | Specific Actions |
| Identify a family spokesperson and support persons involved in decision making | Choose a person the family/client trusts; Establish mechanisms for contact |
| Identify a primary nursing contact for the family | If possible, choose the nurse most in contact with the client, Meet with the family within 24 hrs of admission to explain roles of each healthcare team member, Provide contact number to family spokesperson. |
| Discuss family access to the client | Arrange for visitation based on unit protocols, client condition/needs, family preferences, Educate the family about visiting hours, how to reach the hospitalist, when rounds occur, Involve family in client care whenever possible and desired. |
| Call the family about any changes in client condition or treatment | Inform family of changes as they occur, Provide frequent status reports, Allow time for questions. |
| Provide complete data in easily understandable terms | Ask questions about what the client/family understands about the client’s condition, how they are coping, what they fear, Check for misunderstandings, incomplete information, Provide information based on family needs, Respect cultural and personal desire for level of information disclosure. |
| Actively involve the client/family in all clinical decisions; | Hold formal care conferences for important care decisions, Take into account and respect client preferences, spiritual and cultural attitudes, Allow time for questions, Strive for consensus in decisions |
| Connect family with support services | Provide information about support groups, hospital based social, spiritual, medicare, hospice, home care, and other care services as needed. |
| Ensure collaborative rapport and support among health care team members. | Maintain clear communication among health care team members. Avoid conflicting messages to the family. Provide opportunities for staff to decompress and discuss difficult situations and feelings. |
Data from: Davidson J, Powers K, Hedayat K, Tieszen M, Kon A. et. Al. Clinical practice guidelines for support of the family in the patient-centered intensive care unit: American College of Critical Care Medicine Task Force 2005-2005. Critical Care Medicine. 35(2): 605-622, 2007; Leske J: Interventions to decrease family anxiety, Crit Care Nurs 22(6):61–65, 2002.
Considering stress issues for children
Health disruptions create special problems for children because they lack the words and life experience to sort out the meaning of illness, either their own or that of a significant family member (Compas et al., 2001). Children express their stress through behavior. Signs of distress such as academic decline, gastric distress, and headaches can alert the nurse to unvoiced stress. In the hospital, children withdraw, demonstrate clinging behaviors, or have frequent meltdowns. Uncertainty creates stress for both parents and children (Stewart & Mishel, 2000).
Parents may need help with communicating information about serious illness to children, with thinking through their children’s reactions, and with advice on ways to break bad news or set realistic limits with an ill child. Nurses should base their responses on detailed knowledge of the child’s cognitive and psychosocial development, as well as concrete data. Children need to have their questions answered simply and honestly. Hearing information from someone they trust is important in modifying the uncertainty of a serious illness. Small children can be encouraged to express their stress feelings through drawings and manipulating puppets.
Considering stress issues for older adults
Stress issues for older adults occur during a phase of life when health and loss of important personal supports are no longer the assets they were during other phases of adulthood. Changes in lifestyle and financial status after retirement are sources of stress, particularly for people who have not thought about necessary changes in the life cycle associated with retirement or loss of a spouse. Worries about finances, fears of not being able to live independently, or of being moved to an assisted living or nursing home are common. Older adults living alone can feel vulnerable about their safety or ability to reach help should they experience a sudden physical change. The loss of significant people, isolation and loneliness can complicate treatment issues.
In addition to the normal stress reducers and coping strategies discussed in this and other chapters, nurses can help older clients develop tangible ways to promote physical and emotional safety, and to maximize their health situation. Sometimes all it takes is simple suggestions and well-timed questions about recreational activities or hobbies that the older adult has not considered.
Stress management strategies for the older adult from a health promotion perspective include maintaining an active social life and a healthy lifestyle that keeps mind and body active. Sharing concerns and developing leisure or volunteer interests help older adults develop a harmonious lifestyle that acts to release and reduce stress. Most communities have low-impact exercise activities, continuing education, and social outlets for older adults. Elderly caregivers of clients with dementia can benefit from some of the suggestions in Chapter 19 to reduce stress and balance their health and well-being with that of a family member with dementia.
Stress reduction strategies
Information is an essential need for both clients and families, and an important stress reducer. Each family member’s health and well-being is affected by the communication and actions of the health care team during a hospitalization (Davidson, 2009). Relevant information can range from providing basic data about visiting hours, the timing of tests and procedures, plans for discharge, to complex facts about the client’s condition or treatment. Information sharing should begin with orienting clients and families to the health care situation or unit, and providing enough information to familiarize but not overwhelm them as to what they might expect from health care. Take time to briefly explain the following:
• What will happen during tests or surgery
• Who is likely to interview the client, and why
• How the client can best cooperate or assist in his or her treatment process
In stressful situations, the perceptual field narrows so most people hear only a fraction of what has been said. Information and directions given in the first 48 hours of an admission should be repeated, usually more than once, because this is the time of highest stress. A calm approach and repetition of instructions can help clients in stressful situations relax enough to hear important instructions. Providing written instructions that can be discussed at the time and then left with the client or family enhances understanding. Allow time to answer questions and provide the client’s family with the health provider’s contact numbers to call if other issues arise.
Processing strong feelings
Clients experiencing stress should be given the opportunity to express their feelings, thoughts, and worries. Crying, anger, and magical thinking are normal reactions to situations that one cannot control. Although aggression toward self or others cannot be tolerated, the client should be allowed to express anger and should be given the lead in how he or she wants to address stressors, if there is no immediate jeopardy to treatment.
Listen carefully and ask gentle, probing questions. Helpful statements can include, “This must be very difficult for you to absorb. Can you tell me what you are experiencing right now?” This listening response allows the client to put concerns into words. If the client tells the nurse, “I think I’m losing my mind,” the nurse might respond, “Many people feel that way. It feels that way, but what is happening is that you are feeling disoriented because this situation is sudden and overwhelming. It’s a normal response. Can you identify what worries you the most?” Notice in both probes, the nurse normalizes the client’s “strange” feelings. Acknowledging the legitimacy of feelings as a normal response to an abnormal situation reinforces the client’s self-integrity and helps the client put boundaries on his or her anxiety.
Allowing clients to be in charge of areas and issues that are not at odds with a treatment protocol, and helping clients discover the real causes of their frustration can reduce stress through direct action. Encourage clients to take one day at a time in their expectations and recovery activities. Concrete assistance with negotiating appropriate referral resources is helpful.

Anticipatory guidance
Anticipatory guidance is a term used to describe the process of sharing information about a circumstance, concern, or situation before it occurs. Fear of the unknown intensifies the impact of a stressor. Knowing what lies ahead can often prevent the development of a crisis (Hoff & Hallisey, 2009).Your response to client/family anxiety should be tentative and reflect your level of knowledge about the unique concerns of the client, as well as the condition and situation. In framing a response, you might reflect on the following:
• What type of information would be most helpful to this particular client at this particular time, given what the client has told me?
• How would I feel if I was in this person’s position, and what would I want to know that might bring me comfort in this situation?
It is difficult to directly answer stress-related questions about uncertainties, such as “If I take the chemotherapy, will I be cured, or am I going to die anyway?” The reality is that there may be no single answer. It helps to ask the client what prompted the question, and to have a good idea of the client’s level of knowledge before answering. Honest communication is essential, but sensitivity to the client’s experience is critical.
Providing anticipatory guidance can put needless worry to rest. For example, you could use a simple statement such as “You’ve never had this procedure before. Let me explain how it works” (Keller & Baker, 2000).
When providing anticipatory guidance, do not offer more than what the situation dictates. Encourage the client to expand on suggestions rather than presenting a full plan. The growth in client ability to set priorities, to develop a plan that has meaning to them, and to establish milestones in the evaluation process stimulates self-confidence and decreases stress. Exercise 20-4 provides practice in helping clients handle stressful situations.
Anticipatory guidance can be helpful in preparing family members for their first visit with a client with a visible disfigurement, a marked physical or psychological deterioration, or the presence of life support machines. If you sense family awkwardness in how to approach a vulnerable or comatose client, you could say to a family member: “You might want to identify yourself and tell your father you are here with him.”
Priority Setting: Clients need support and encouragement when coping with stress, but they don’t always know where to start. Priority setting helps reduce hesitation and offers a stepwise framework for stress resolution. In addition to helping clients determine which task elements are critical and which can be addressed later, nurses can help clients break down tasks into smaller manageable segments. The most important tasks should be scheduled during times when the client or family has the most energy and freedom from interruption.
Nurses need to help clients identify the concrete tasks needed to achieve treatment goals, including the people involved, the necessary contacts, the amount of time each task will take, and specific hours or days for each task. Some tasks are more important than others in stressful situations, and not everything can be handled at once. A helpful suggestion might be, “Let’s see what you need to do right now and what can wait until tomorrow.” Tasks that someone else can do and those that are not essential to the achievement of goals should be delegated or ignored for the moment.
Supporting client efforts
Without command over the controllable parts of life, people feel helpless and stressed. Coping mechanisms such as negotiation, specific actions, seeking advice, and rearranging priorities can significantly diminish stress through direct action. Once stressors are named, nurses can use health teaching formats and coaching that help clients to:
Promoting a healthy lifestyle
Encouraging a healthy lifestyle is an essential but sometimes overlooked component of stress reduction strategies. Good health habits improve stress resistance. Eating a healthy diet, and avoiding emotional eating and the wrong foods give people a sense of control and well-being. Too much caffeine and alcohol can exacerbate stress. Laughter dissolves it.
Adequate quality sleep is restorative. Healthy nighttime habits, such as establishing a scheduled bedtime and having a small snack before bedtime, encourages sleep. Regular exercise helps the body release tension, as well as contributes to fitness. Exercise can be accomplished in a social setting, for example, hiking or biking. Certain exercise programs such as yoga or tai chi incorporate meditation, deep breathing, and muscle stretching, all of which are known to reduce stress.
Organizing time and doing activities that energize rather than stress, balancing work with leisure activities, restructuring priorities, and eliminating unnecessary obligations reduce stress.
Helping families handle stress
Families can suffer potentially overwhelming stress when their family member is critically ill or injured. Contemporary health care environments with advanced technology, shorter stays, and multiple caregivers are complex and anxiety producing. Sources of stress for families can include “fear of death, uncertain outcome, emotional turmoil, financial concerns, role changes, disruption of routines, and unfamiliar hospital environments” (Leske, 2002, p. 61). Families look to nurses for support and direction. Consistent regular communication is key to family satisfaction and effective shared decisions. Direct family contact offers firsthand insight into client preferences, health care needs and resources especially when the client is unable to provide this information (Davidson, 2009).
It is helpful to put yourself in the family’s position and to put into words how you might feel in a similar situation. Statements such as “Most people would feel anxious in this situation,” or “It would be hard for anyone to have all the answers in a situation like this” help put stressors and stress responses into perspective.
Families have a strong need to remain physically close to the client in critical care situations and there is a strong correlation between proximity to the client and satisfaction with care (Davidson, 2009). When this need translates into constant attendance, family members can become physically and emotionally exhausted (Leske, 2000). A preventive strategy is to suggest that the family members take short breaks. Family members may need “permission” to go to a movie or eat in a restaurant outside the hospital. Usually, they will do so only with an assurance that they will be called should there be any change in the client’s condition.
Being able to “do something” for the client helps family members defuse their anxiety. Family members want to provide support and comfort. Letting family members participate in the client’s care to whatever extent is possible for the client and comfortable for the family can be a meaningful experience for both. On the other hand, it is important to ask family members about how they would like to participate, rather than making assumptions.
Stress management therapies
Mind/body therapies are coping strategies designed to lessen the intensity of the stressor on a person once the stress response has occurred. Examples include meditation, relaxation techniques, yoga, and cognitive restructuring. Altering physiologic reactions such as blood pressure, heart rate, muscle tension, and respiratory rate helps people experience greater calm and peace of mind (Luskin et al., 1998). Regular practice of these techniques can improve physical and emotional well-being.
Meditation: Meditation is a stress-reduction strategy dating back to early Christian times. People use meditation to develop a sense of inner peace and tranquility, and to center themselves. Meditation allows people to decrease stress by focusing their attention on something other than the stress, and clears the mind of disturbing thoughts. This action helps to reduce the concentration of stress hormones attached to stressful thinking. A guide to meditation is provided in Box 20-4.
Mindfulness is a stress management tool that can be used at any point. It can be as simple as focusing on deep breathing. Focusing completely on your breathing, music, or what is happening in the current moment forces you to at least momentarily let go of stressful thoughts. It is an easy way of quieting the mind and decreasing the intensity of stressful feelings.
Biofeedback: Biofeedback plays an important role in management of clients with chronic stress responses affecting individual body systems (e.g., essential hypertension, migraine headaches, Raynaud’s disease, and ulcerative colitis). People are trained to voluntarily take control over a variety of physiologic activities such as their brain activity, blood pressure, heart rate, pain, migraine or tension headaches, and other bodily functions as a means to improve their health. Biofeedback provides awareness of minute-by-minute changes in biologic activity. The goal is to lower physiologic arousal and promote relaxation (Grazzi & Andrasik, 2010). Equipment used with biofeedback includes the electroencephalogram, skin temperature devices; blood pressure measures; galvanic skin resistance measurements; and the electromyogram, which measures muscle tension.
Progressive Relaxation: Progressive relaxation is a technique that focuses the client’s attention on conscious control of voluntary skeletal muscles. Originally developed by Edmund Jacobson (1938), a physiologist physician, the technique consists of alternately tensing and relaxing muscle groups. Each muscle group is worked with individually with the client sitting in a relaxed position in a chair with arm supports or lying down. Davis, Eshelman and McKay (2008) provide an excellent step-by-step description of the basic procedure for progressive relaxation.
A variant of progressive relaxation is deep breathing. This can be accomplished anywhere and at any time a person experiences stress.
• Deeply inhale to the count of 10, and hold your breath.
• Exhale slowly, again to the count of 10.
• Concentrate as you do this exercise only on your breathing.
The person breathes 10 times in a row with each inhalation/exhalation counted as 1 breath. Focusing the mind on the continuous rhythm of inhaling and exhaling turns the mind away from thinking about specific stressors. To experience the progressive relaxation technique, see Exercise 20-5.
Yoga and Tai Chi: Yoga is a mind/body exercise practice rooted in ancient India. The practice of yoga emphasizes correct alignment, controlled postures or poses, and regulated breathing to help people relax and reduce stress. Controlling breathing helps to quiet the mind. Some forms of yoga place an emphasis on meditation and developing self-awareness.
Tai chi is a system initially developed in China. It consists of posture or movements practiced in a slow, graceful manner. It involves stretching, rhythmic movements coordinated with controlled breathing. The concentration required for both yoga and tai chi require a person to forget distressing thoughts at least for the moment.
Guided Imagery: Guided imagery is a technique often used in combination with relaxation strategies for cancer pain and stress (Kwekkeboom, 2008). Imagery techniques use the client’s imagination to stimulate healing mental images designed to promote stress relief. The process involves asking the client to imagine a scene, previously experienced as safe, peaceful, or beautiful. Supportive prompts to engage all of senses deepen the imagery experience. The healing scene can be used each time that the client begins to experience stress.
Addressing occupational stress in nurses
Nurses face a greater risk for burnout than people in other lines of work. They work in high-stress service environments, helping people cope with serious life and death situations every day. Freudenberger (1980) defines burnout as “a state of fatigue or frustration brought about by devotion to a cause, way of life, or relationship that failed to produce an expected reward” (p. 13). It develops in individuals involved with “people work,” and is characterized by emotional exhaustion, depersonalization, and a sense of diminished professional accomplishment (Maslach, 2001). Although burnout shares some characteristics with depression and anxiety, it is a different syndrome, clearly linked to a work environment, and personal expectations of self and others within that setting.
The development of burnout begins insidiously, particularly in nurses who strive for perfection. Unchecked, it is a progressive syndrome associated with emotional exhaustion and loss of meaning. Freudenberger (1980) refers to burnout as the “overachievement syndrome.” People who are high achievers, committed, and passionate about their work are more at risk to develop burnout symptoms.
The need to be perfect does not allow for error, or the reserve needed to correct for unexpected events (Porter-O’Grady, 1998). A story about Babe Ruth offers an appropriate metaphor. Coaching a young, aspiring ball player, he asked the boy how he planned to pitch the ball. The boy answered, “I’m going to throw it with all my might and get it right where it needs to go. I’m going to give it 110 percent.” Ruth had different advice: “Throw the ball with 80 percent of your might. You will need the reserve to correct for any mistakes.” Nurses need the same reserve to correct for the inevitable curve balls inherent in clinical practice—and life in general. Contemporary thinking about burnout considers it as originating from combined factors in the work environment and within the person. Six areas of organizational contributors to burnout include workload, control, reward, community, fairness, and values (Freeney & Tiernan, 2009; Maslach & Leiter, 1997). Sources of work-related burnout for nurses include working too many hours or at an accelerated pace with no respite, feeling unappreciated, giving too much to needy clients, trying to meet multiple demands of administrators, lack of community with coworkers, and feeling resentment, in place of the meaning that work once held.
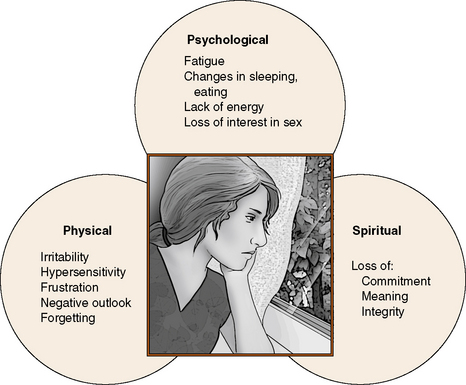
Symptoms of Burnout: A person experiencing burnout is always tired and preoccupied with work (Vernarec, 2001). People who are burned out feel disillusioned and lack zest for their work. Other signs include loss of motivation and ideals, boredom or dissatisfaction at work, irritability and cynicism, resentment of expectations, and avoidance of meaningful encounters with clients and families. Headaches, gastric disturbances, skipping meals or eating compulsively on the run, feeling irritated by the intrusion of others, and a lack of balance between a nurse’s work and personal life can signal the onset of burnout. In a study of co-workers’ perceptions of colleagues suffering from burnout, signs observed included a struggle to achieve unobtainable goals, wanting to manage alone, and becoming isolated from others (Ericson-Lidman & Strandberg, 2007). Figure 20-3 identifies common symptoms of burnout.
Burnout Prevention Strategies: The ABCs of burnout prevention (Arnold, 2008) are presented in Table 20-3. Reflecting on the sources of stress in your life puts boundaries on it. Think about your goals, and what is important to you. Rather than simply complaining, seek role models or trusted coworkers who can offer you the support and sensitivity you need to become aware of what is going on in your life. A useful exercise is to imagine yourself a year from now and ask yourself how important the issue would be a year from now.
TABLE 20-3
| Suggested Strategy | |
| Awareness | Use self-reflection and conversations with others to sort out priorities and identify parts of life out of balance. Recognize and allow feelings. |
| Balance | Maintain a healthy lifestyle. Balance care of others with self-care/self-renewal needs. |
| Choice | Differentiate between things you can change and those you cannot. Deliberately make choices that are purpose driven and meaningful. |
| Detachment | Detach from excessive ego involvement and personal ambition. Share responsibility and credit for care. Use meditation to center self. |
| Altruistic Egoism | Take scheduled time for self, learn to say no, practice meditation, and develop outside interests that enrich the spirit. |
| Faith | Burnout is a malaise of the spirit. Trust in a higher power or purpose to center yourself when you do not know what will happen next. |
| Goals | Identify and develop realistic goals in line with personal strengths. Seek feedback and support. |
| Hope | Hope is nurtured through conversations with others that lighten the burden, and a belief in one’s possibilities and personal worth in the greater scheme of things. |
| Integrity | Recognize that each of us is the only person who can determine the design and application of meaning in our lives. |
Data from: Arnold E: Spirituality in educational and work environments (pp. 386–399). In Carson V, Harold Koenig, editors: Spiritual dimensions of nursing practice, revised edition, Conshohocken, PA, 2008, Templeton Foundation Press.
Identifying realistic goals that are achievable and in line with your personal values is an excellent burnout prevention strategy. Goals should be aligned with purpose and values. Focusing on one thing at a time and finishing one project before starting another has several benefits. Achieving small related goals promotes self-efficacy and offers hope that more complex goals are achievable.
Maintaining a healthy balance among work, family, leisure, and lifelong learning activities enhances personal judgments, satisfaction, and productivity in all three spheres. Actively schedule a time for each of these activities and stick to it.
Remember that you always have choices. People experiencing burnout lose sight of this fact. Life is a series of choices and negotiations. The choices we make create the fabric of our lives. Refusing to delegate work because someone else cannot do it as well, or not going out to dinner with friends because you have too much work to do are choices—bad options that lead to burnout.
Detachment from ego and/or taking responsibility for outcomes is a critical component of burnout prevention. It means that you don’t allow emotional involvement in a task or relationship to undermine your quality of life, values, or needs. Someone once asked Mother Teresa how she was able to remain so energetic and hopeful in the midst of suffering she encountered in Calcutta. She replied that it was because she did the best she could and didn’t worry about the outcome because she couldn’t control it.
It is important to pay as much attention to your own personal needs as you do to the needs of others. Although this seems obvious, nurses sometimes consider attention to their own needs as being selfish. However, one cannot give from an empty cupboard. Replenishing the self actually improves what one can give to others.
Faith is defined as an intangible connection with a larger purpose or higher power to guide and support a person during both good and bad times. Faith helps people develop an optimistic worldview and experience less distress.
Nurses experiencing burnout often feel helpless and hopeless about changing their situation, other than to leave it. Hope is a powerful antidote for burnout. Exercise 20-6 provides an opportunity to think about your personal burnout potential and ways to achieve better balance in your life.
Burnout challenges personal integrity in the sense that important values are ignored or devalued. When you begin to forget who you are and try to become what everyone else expects of you, you are in trouble. Reclaim yourself. Taking responsibility for yourself and doing what is important to you helps to reverse burnout. Take the risk to be all that you are, as well as all that you can be, without worrying about what others think. Seek professional supports such as training, staff retreats, staff support networks, and job rotation to stimulate new ideas and insights. Professional support groups are effective as a means of providing encouragement to nurses in acute settings (Parish, Bradley, & Franks, 1997).
Summary
This chapter focuses on the stress response in health care, and supporting client and family coping with stress through nurse-client relationships. Stress can negatively impact client outcomes, level of satisfaction with care, and compliance with treatment. A fundamental goal in the nurse-client relationship is to empower clients and families with the knowledge, support, and resources they need to cope effectively with stress.
Stress is a part of everyone’s life. Mild stress can be beneficial, but greater stress levels can be unhealthy. Concurrent and cumulative stresses increase the response level. Theoretical models address stress as a physiologic response, as a stimulus, and as a transaction between person and environment. Factors that influence the development of a stress reaction include the nature of the stressor, personal interpretation of its meaning, number of previous and concurrent stressors, previous experiences with similar stressors, and availability of support systems and personal coping abilities.
People use problem- and emotion-focused coping strategies to minimize stress. Social support is key to effectively coping with stress. Assessment should focus on stress factors the person is experiencing, the context in which they occur, and identification of coping strategies. Supportive interventions include giving information, opportunities to express their feelings, thoughts, and worries, and anticipatory guidance.
Nurses are at the forefront of health care delivery to clients and families experiencing complex health and life issues. They too can experience stress and need support to do their job effectively. Burnout prevention requires recognition and resolution of organizational and personal factors contributing to job-related stress in professional nurses.
References
Aldwin, C.M., Levenson, M.R. Posttraumatic growth: a developmental perspective. Psychol Inq. 2004;15(1):19–22.
Arnold, E. Spirituality in educational and work environments. In Carson V., Koenig H., eds.: Spiritual dimensions of nursing practice, revised edition, Conshohocken, PA: Templeton Foundation Press, 2008.
Arnold, E. The stress connection: women and coronary heart disease. Crit Care Nurs Clin North Am. 1997;9(4):565–575.
Askew, R., Keyes, C. Stress and somatization: a sociocultural perspective. In: Oxinton K.V., ed. Psychology of stress. Hauppage, NY: Nova Biomedical Publishers; 2005:129–144.
Benson, H. The relaxation response. New York: Morrow, 1975.
Cannon, W.B. The wisdom of the body. New York: Norton Pub, 1932.
Caplan, G. Mastery of stress: psychosocial aspects. Am J Psychiatry. 1981;13(8):41.
Chaboyer, W., James, H., Kendall, M., et al. Transitional care after the intensive care unit. Crit Care Nurse. 2005;25(3):16–27.
Compas, B., Connor-Smith, J.K., Saltzman, H., et al. Coping with stress during childhood and adolescence: problems, progress, and potential in theory and research. Psychol Bull. 2001;127(1):87–127.
Davidson, J. Family-centered care: meeting the needs of patients’ families and helping families to critical illness. Crit Care Nurse. 2009;29(3):28–34.
Davidson, J., Powers, K., Hedayat, K., Tieszen, M., Kon, A., et al. Clinical practice guidelines for support of the family in the patient-centered intensive care unit: American College of Critical Care Medicine Task Force 2005–2005. Crit Care Med. 2007;35(2):605–622.
Davis, M., Eshelman, E., McKay, M., et al. The relaxation and stress reduction workbook. Oakland CA: New Harbinger Publications, Inc, 2008.
Dolbier, C., Smith, S., Steinhardt, M.A., et al. Relationships of protective factors to stress and symptoms of illness. Am J Health Behav. 2007;31(4):423–433.
Erikson-Lidman, E., Strandberg, G. Burnout: co-workers’ perceptions of signs preceding workmates’ burnout. J Adv Nurs. 2007;60(2):199–208.
Folkman, S. The case for positive emotions in the stress process. Anxiety Stress Coping. 2008;21(1):3–14.
Freeney, Y., Tiernan, J. Exploration of the facilitators of and barriers to work engagement in nursing. Int J Nurs Stud. 2009;46:1557–1565.
Freudenberger, H. Burn-out: the high cost of high achievement. Garden City, NY: Doubleday, 1980.
Ganzel, B., Morris, P., Wethington, E., et al. Allostasis and the human brain: integrating models of stress from the social and life sciences. Psychol Rev. 2010;117(1):134–174.
Grazzi, L., Andrasik, F. Non-pharmacological approaches in migraine prophylaxis: behavioral medicine. Neurol Sci. 2010;31(Suppl 1):S133–S135.
Hoff, L.A., Hallisey, B., Hoff, M., et al. People in crisis: clinical diversity perspectives, ed 6. New York, NY: Routledge, 2009.
Holmes, T., Rahe, R. The social readjustment rating scale. J Psychosom Res. 1967;11:213–218.
Jacobson, E. Progressive relaxation. Chicago: University of Chicago Press, 1938.
Johnson, K., Renn, C. The hypothalamic-pituitary-adrenal axis in critical illness. AACN Clin Issues. 2006;17(1):30–40.
Keller, V., Baker, L. Communicate with care. RN. 2000;63(1):32–33.
Kwekkeboom, K. Patients’ perceptions of the effectiveness of guided imagery and progressive muscle relaxation. Complement Ther Clin Pract. 2008;14(3):185–194.
Lazarus, R., Folkman, S. Stress, appraisal and coping. New York: Springer, 1984.
Lehrer, P., Woolfolk, R., Sime, W., et al. Principles and practice of stress management. New York: Guilford Press, 2007.
Leske, J. Family stresses, strengths, and outcomes after critical injury. Crit Care Nurs Clin North Am. 2000;12(2):237–244.
Leske, J. Interventions to decrease family anxiety. Crit Care Nurs. 2002;22(6):61–65.
Leske, J. Treatment for family members in crisis after critical injury. AACN Clin Issues. 1998;9(1):129–139.
Luskin, F., Newell, K., Griffith, M., et al. A review of mind-body therapies in the treatment of cardiovascular disease. Altern Ther Health Med. 1998;4(3):46–61.
Martin, P., Lae, L., Reece, J., et al. Stress as a trigger for headaches: relationship between exposure and sensitivity. Anxiety Stress Coping. 2007;20(4):393–407.
Maslach, C. What have we learned about burnout and health? Psychol Health. 2001;16:607–611.
Maslach, C., Leiter, M.P. The truth about burnout: how organizations cause personal stress and what to do about it. San Francisco: Jossey-Bass, 1997.
McEwen, B. Allostasis, allostatic load, and the aging nervous system: role of excitatory amino acids and excitotoxicity. Neurochem Res. 2000;9(10):1219–1231.
McEwen, B. Physiology and neurobiology of stress and adaptation: central role of the brain. Physiol Rev. 2007;87(3):873–904.
McEwen, B.S., Wingfield, J.C. The concept of allostasis in biology and biomedicine. Hormones Behav. 2003;43:2–15.
Michalenko, C. The odyssey of Marian the brave: a biopsychosocial fairy tale. Clin Nurse Spec. 1998;12(1):22–26.
Mohr, D.C., Goodkin, D.E., Gatto, N., et al. Depression, coping and level of neurological impairment in multiple sclerosis. Mult Scler. 1997;3:254–258.
Neale, D.J., Arentz, A., Jones-Ellis, J., et al. The negative event scale: measuring frequency and intensity of adult hassles. Anxiety Stress Coping. 2007;20(2):163–176.
Parish, C., Bradley, L., Franks, V., et al. Managing the stress of caring in ITU: a reflective practice group. Br J Nurs. 1997;6(20):1192–1196.
Pearlin, L.I., Schooler, C. The structure of coping. J Health Soc Behav. 1978;19:2–21.
Porter-O’Grady, T. A glimpse over the horizon: choosing our future. Orthop Nurse. 1998;17(Supp 2):53–60.
Reich, J., Zautra, A., Hall, J., et al. Handbook of adult resilience. New York, NY: The Guilford Press, 2010.
Richards, M., Steele, R. Children’s self-reported coping strategies: the role of defensiveness and repressive adaptation. Anxiety Stress Coping. 2007;20(2):209–222.
Schwarzer, R., Knoll, N. Functional roles of social support within the stress and coping process: a theoretical and empirical overview. Int J Psychol. 2007;42(4):243–252.
Selye, H. Stress and the general adaptation syndrome. Br Med J. 1950;4667:1383–1392.
Sinha, B., Watson, D. Stress, coping and psychological illness: a cross-cultural study. Int J Stress Manag. 2007;14(4):386–397.
Skinner, E., Edge, K., Altman, J., et al. Searching for the structure of coping: a review and critique of category systems for classifying ways of coping. Psychol Bull. 2003;129(2):216–269.
Sterling, P., Eyer, J. Allostasis: a new paradigm to explain arousal pathology. In: Fisher S., Reason J., eds. Handbook of life stress, cognition and health. New York: Wiley; 1988:629–649.
Stewart, J.L., Mishel, M.H. Uncertainty in childhood illness: a synthesis of the parent and child literature. Sch Inq Nurs Pract. 2000;14(4):299–319. [discussion 321–326].
Taylor, S.E. Tend and befriend: biobehavioral bases of affiliation under stress. Curr Dir Psychol Sci. 2006;15:273–277.
Taylor, S.E., Welch, W.T., Kim, H.S., et al. Cultural differences in the impact of social support on psychological and biological stress responses. Psychol Sci. 2007;18:831–837.
Taylor, S., Klein, L., Lewis, B., et al. Biobehavioral responses to stress in females: tend and befriend, not fight or flight. Psychol Rev. 2000;107(3):411–429.
Valiant, G., Mukamal, K. Successful aging. Am J Psychiatry. 2001;158:839–847.
Vernarec, E. How to cope with job stress. RN. 2001;64(3):44–46.