Communicating with Other Health Professionals
At the end of the chapter, the reader will be able to:
1 Identify standards for the healthcare work environment.
2 Identify communication barriers in professional relationships, including disruptive behaviors.
3 Describe methods to handle conflict through interpersonal negotiation when it occurs.
4 Discuss methods for communicating effectively in organizational settings.
5 Apply group communication principles to work groups.
6 Discuss application of research studies to clinical practice.
To be effective as a nursing professional, it is not enough to be deeply committed to the client. Ultimately, the workplace’s corporate climate and work atmosphere will have an effect on the relationship that takes place between you and your client. Disruptive behavior (workplace bullying) creates conflicts on the job. The negative consequences of working in a dysfunctional atmosphere are adverse effects on client care and on the staff’s physical and psychological health. This chapter focuses on principles of communication and strategies you can use to help deal with other professionals, promote more collaborative relationships, and function more effectively as an interdisciplinary team member and leader. Specific bridges to communication with other health professionals are described, together with strategies to remove communication barriers.
Basic concepts
Standards for a healthy work environment
A culture of collegiality is essential for a work environment that is to provide high-quality client care. Yet, when the Joint Commission surveyed nurses, more than 90% reported witnessing disruptive behavior; more than half reported they themselves had been subjected to verbal abuse (Joint Commission, 2008). As described in Chapter 22, failures in collaboration and communication among health care providers are among the most common factors contributing to increased errors and adverse client outcomes. Other outcomes include nurse dissatisfaction, job turnover, lost productivity, absenteeism, task avoidance, poor morale, impact on nurse’s physical and mental health, and even legal action (Gerardi & Connell, 2007; Kerfoot, 2008; Olender-Russo, 2009; Rosenstein & O’Daniel, 2005; Spence-Laschinger, Leiter, Day, & Gilin, 2009).
The American Association of Critical Care Nurses (ACCN) in 2004 issued six standards characteristic of a healthy workplace (online, www.aacn.org):
• Nurses must be as efficient in communication skills as they are in clinical skills.
• Nurses must be relentless in pursuing and fostering true collaboration.
• Nurses must be valued and committed partners in making policy, directing and evaluating clinical care, and leading organizational operations.
• Staffing must ensure the effective match between patient needs and nurse competencies.
• Nurses must be recognized and recognize others for the value each brings to the work of the organization.
• Nurse leaders must fully embrace the imperative of a healthy work environment, authentically live it, and engage others in its achievement.
Professional Nursing organizations have identified eight elements of a healthy workplace environment:
• Collaborative culture with respectful communication and behavior
• Communication-rich culture that emphasizes trust and respect
Code of Behavior
The goal of collaboration is to communicate effectively with team members to provide best care. As part of creating a culture of teamwork where staff is valued, a standard across organizations should be zero tolerance for disruptive or bullying behaviors. To accomplish this, each organization needs one well-defined code of behavior applied consistently to all staff. The Joint Commission adopted standards originally scheduled to begin in 2009 that state each health care organization must create a code of conduct defining acceptable and unacceptable behaviors, as well as establishing an agency process for handling disruptive behaviors (Joint Commission line, www.jointcommission.org/SentinelEventAlert/Issue40, July 9, 2008).
Incidence
Incivility is common in large organizations, especially hospitals. Although less than 3% of physicians and less than 3% of nurses exhibit disruptive behaviors, this is enough to effect client outcomes (Rosenstein & O’Daniel, 2005). Seventeen percent of professionals surveyed knew of a disruptive behavior that resulted in a specific adverse client outcome; 86% of nurses reported witnessing disrespect or harassment from physicians; and 72% reported receiving disrespectful behavior from other nurses (O’Daniel & Rosenstein, 2008). A number of authors have found that nurse-to-nurse destructive, disruptive behaviors occur more frequently than such physician-nurse interactions (Woelfle, 2007).
Definitions
Conflict was defined in Chapter 14 as a hostile encounter. The nursing literature uses a variety of terms to refer to persistent uncivil behaviors such as workplace bullying; verbal abuse; horizontal/lateral violence; “eating your young”; in-fighting; mobbing, harassment, or scapegoating. In this situation, the nurse victim is less powerful and is thus unable to bring an end to this behavior. For discussion in this textbook, we use the term disruptive behavior and use the original definition from Leymann in Sweden: at least two negative acts per week, occurring over more than 6 months in duration (Johnson, 2009).
Disruptive behaviors are prolonged and may include overt behaviors: rudeness, verbal abuse, intimidation, putdowns; angry outbursts, yelling, blaming, or criticizing team members in front of others; sexual harassment; or even threatening physical confrontations. Other disruptive behaviors are more covert and passive: withholding information, withholding help, giving unreasonable assignment loads, refusal to perform an assigned task, impatience or reluctance to answer questions, not returning telephone calls or pages, and speaking in a condescending tone (O’Reilly for Joint Commission, 2008, online). These behaviors threaten the well-being of nurses and the safety of clients (Wachs, 2009).
Creating a culture of regard
Organizations have sometimes tolerated disruptive workplace behaviors (Olender-Russo, 2009). Australian nurses associated this with organizational restructuring or downsizing, or both (Hutchinson, Vickers, Jackson, & Wilkes, 2005). There are organizational pressures on nurses to increase their productivity and be more cost-effective. In Johnson’s survey, 95% of emergency department nurses reported that disruptive bullying was done to two or more staff nurses by a supervisor in their department, leading us to speculate that agencies accept this as a useful management strategy (Johnson & Rea, 2009).
We need to become aware of how to discourage disruptive behaviors as we work to develop a healthy, collaborative workplace atmosphere. A climate that promotes collaboration and positive communication among caregivers contributes to satisfaction with one’s work and better job retention. Most importantly, commitment to collaboration with other professionals helps sustain a high quality of client care (Joint Commission Resources, 2006). Building an organizational infrastructure that creates a climate that stresses our common mission and core values, and empowers nurses, starts with explicitly stated expectations of mutual respect. Administrators and nurse managers need to model behaviors that convey regard for staff and enforce policies of zero tolerance for disrespect.
Respect
Feeling respected or not respected is an integral part of how nurses rate the quality of their work environment (Bournes & Milton, 2009). Three key factors are a positive climate of professional practice, a supportive manager, and positive, respectful relationships with other staff.
Etiology
Nurses say they feel respected and appreciated if their opinions are listened to attentively and they receive feedback from authority figures as to the value of their work competence. When their opinions are discounted or ridiculed, they feel disrespected, angry, and frustrated (Parse, 2006). Feelings of powerlessness decrease self-esteem and increase anger. In an unhealthy atmosphere in which a staff member feels intimidated by authority and unable to change disruptive behaviors, they may direct their anger toward peers (Gerardi & Connell, 2007). Respect is a natural extension of the practice of nursing, as identified in the American Nurses Association’s Code of Ethics (2001). Typically, nurses describe behaviors indicating lack of respect to include demeaning verbal comments, nonverbal actions such as eye rolling, not paying attention to their opinions, interrupting, not responding to telephone or e-mail, and physical or sexual harassment.
Applications
Conflicts will inevitably arise in the work setting. Nurses have a responsibility to learn to work cooperatively. Refer to Box 23-1. Aside from the nurse-client conflicts described in Chapter 14, most workplace conflicts occur between the nurse and authority figures. In addition, conflict may arise from agency employee policies. Internal employee-management disputes detract from the agency’s health care mission and from its financial bottom line.
Many of the same strategies for conflict resolution discussed for conflicts between client and nurse can be applied to conflicts between the nurse and other health care workers. Review the principles of conflict management in Figure 14-1 in Chapter 14. As mentioned, conflict is not necessarily detrimental to productivity and job satisfaction. Successful resolution often has a positive effect on both outcomes.
Identify sources of conflict
Conflict often stems from miscommunication.You need to think through the possible causes of the conflict. Conflict also stems from overly defensive responses to a situation. So you need to identify your own feelings about it and respond appropriately, even if the response is a deliberate choice not to respond verbally. Interpersonal conflicts that are not dealt with leave residual feelings that reappear in future interactions.
Set goals
Your primary goal in dealing with workplace conflict is to find a high-quality, mutually acceptable solution: a win-win strategy. In many instances, a better collaborative relationship can be developed through the use of conflict management communication techniques (Bacal, n.d.; Boone, King, Gresham, Wahl, & Suh, 2008). To reframe a clinical situation as a cooperative process in which the health goals and not the status of the providers becomes the focus:
• Identify your goal. A clear idea of the outcome you wish to achieve is a necessary first step in the process. Remember the issue is the conflict, not your coworker.
• Obtain factual data. It is important to do your homework by obtaining all relevant information about the specific issues involved—and about the client’s behavioral responses to a health care issue—before engaging in negotiation.
• Intervene early. Be assertive. The best time to resolve problems is before they escalate to a conflict. Create a forum for two-way communication, preferably meeting periodically. Structured formats have been developed for you to use in conflict resolution, especially in team meetings. Nielsen and Mann (2008) mention the format of DESC:
• Avoid negative comments that can affect the self-esteem of the receiver. Even when the critical statements are valid (e.g., “You do …” or “You make me feel …”), they should be replaced with “I” statements that define the sender’s position. Otherwise, needless hostility is created and the meaning of the communication is lost.
• Consider the other’s viewpoint. Having some idea of what issues might be relevant from the other person’s perspective provides important information about the best interpersonal approach to use. In addition to dealing with your own feeling, you need an ability to deal with the feelings of the others. Be cooperative, acknowledging the team’s interdependence and mutual goals.
Avoiding barriers to resolution
Refer to Box 23-2 for tips on how to turn conflict into collaboration. Much of the individual behavior was discussed in Chapter 14, such as avoiding the use of negative or inflammatory, anger-provoking words. Also avoid phrases that imply coercion or that are patronizing. Examples include: “We must insist that …” or “You claim that …” Most individuals react to anger directed at them with a fight-or-flight response. Anyone can have a moment of rudeness, but monitor your own communications to avoid any pattern of abusive behaviors, including blaming or criticizing staff to others. Katrinli et al.’s study (2008) showed that when nurse supervisors become aware of how their behavior affects their nurses, they can increase the nurses’ performance, increase their job involvement, and increase organizational identification.
Physician-nurse conflict resolution
The history of nurse-physician communication is described by Seago (2008) as a “game” in which nurses made treatment recommendations without appearing to do so, and physicians asked for recommendations without appearing to do so, with both parties striving to avoid open disagreements. She notes that the literature indicates that communication between doctor and nurse is still often contentious. Remarkable increases in safety in airline and space programs were achieved by creating a climate in which junior team members were free to question decisions of more senior, powerful team members. It is recommended that health care adopt a similar philosophy. The American Medical Association (AMA, 2008) has specifically stated that codes of conduct define appropriate behavior as including a right to appropriately express a concern you have about client care and safety. While this is being set forth as a medical code of conduct for physicians, should it also apply to nurses?
Nurses influence physician-client communication. Nurses assess what physicians tell clients, encourage clients to seek clarification, encourage second opinions, and spend time defending the physician’s competence. Better collaboration and better communication are associated with safer care and better client care outcomes. In a meta-analysis of existing research, Seago (2008) found these factors to be associated with reduced drug errors, reduced client mortality, improved client satisfaction, and somewhat with shorter hospital stays. Methods to improve safe communication are discussed in Chapter 22.
There will be occasions when you have collaboration difficulties. One major factor related to job satisfaction and job retention is “disruptive” communication between other professionals, especially physician-nurse interactions. Case law defines disruptive physician behavior as conduct that disrupts the operation of the hospital, affects the ability of others to get their jobs done, and creates a hostile work environment.
Gender and Historic Communication: The relationship between the doctor and the nurse remains an evolving process. Changes in the physician-nurse communication process are occurring as nurses become more empowered, more assertive, and better educated. Most nurses occasionally encounter problems in the physician-nurse relationship. The differences in power, perspective, education, pay, status, class, and sometimes gender are contributing factors. Contemporary society is redefining traditional gender role behavior, negating some of the traditional “nurse as subservient female” stereotypical behaviors. Reflect on content presented on gender differences in communication to determine whether your current situation might be related to gender differences in communication styles rather than a more serious problem. Some doctors are reluctant to be challenged; some nurses are quick to feel slighted. Some physician-nurse relationships are marked with conflict, mistrust, and disrespect. Although these feelings are changing, it is slow, and some physicians still regard themselves as the only legitimate authority in health care, seeing the professional nurse as an accessory. An attitude that excludes the nurse as a professional partner in health care promotion benefits no one and is increasingly challenged as being costly to professionals and clients alike.
It is important to remain flexible yet not to yield on important, essential dimensions of the issue. Sometimes it is difficult to listen carefully to the other person’s position without automatically formulating your next point or response, but it is important to keep an open mind and to examine the issue from a number of perspectives before selecting alternative options. The communication process should not be prematurely concluded. You can apply the same principles of conflict resolution discussed in Chapter 14 when dealing with a physician-nurse conflict. Make a commitment to open dialogue. Listening should constitute at least half of a communication interaction. Foster a feeling of collegiality. Use strategies from that chapter to defuse anger. During your negotiation, discussion should begin with a statement of either the commonalities of purpose or the points of agreement about the issue (e.g., “I thoroughly agree Mr. Smith will do much better at home. However, we need to contact social services and make a home care referral before we actually discharge him; otherwise, he will be right back in the hospital again”). Points of disagreement should always follow rather than precede points of agreement. Empathy and a genuine desire to understand the issues from the other’s perspective enhance communication and the likelihood of a successful resolution.
Nurses have a responsibility to foster good physician-client communication. This is especially true when it becomes obvious to you from content, tone, or body language that antagonism is developing. Do you think it is ever appropriate for a nurse to criticize a physician’s actions to a client? A common underlying factor in at least 25% of all malpractice suits is an inadvertent or deliberate critical comment by another health care professional concerning a colleague’s actions. So think before you speak!
Solutions that take into consideration the needs and human dignity of all parties are more likely to be considered as viable alternatives. Backing another health professional into a psychological corner by using intimidation, coercion, or blame is simply counterproductive. More often than not, solutions developed through such tactics never get implemented. Usually there are a number of reasons for this, but the basic issues have to do with how the problem was originally defined and the control issues that were never actually dealt with in the problem-solving discussion. The final solution derived through fair negotiation is often better than the one arrived at alone.
Nurse-to-nurse conflict resolution
Although it is inevitable that you will encounter some communication problems with nurse colleagues, remember that, if managed appropriately, these conflicts can lead to innovative solutions and improved relationships.
Negotiating with Nursing Authority Figures: Negotiating can be even more threatening with a nursing supervisor or an instructor who has direct authority, because these people have some control over your future as a staff nurse or student. Supervision implies a shared responsibility in the overall professional goal of providing high-quality nursing care to clients. The wise supervisor is able to promote a nonthreatening environment in which all of the aspects of professionalism are allowed to emerge and prosper. In a supervisor-nurse relationship, conflict may arise when expectations for performance are unclear or when the nurse is unable to perform at the desired level. Communication of expectations often occurs after the fact, within the context of an employee performance evaluation. To effectively manage requires that performance expectations are known from the beginning. The supervisor needs to advise you about the need for improvement as part of an ongoing, constructive, interpersonal relationship. When the supervisor gives constructive criticism, it is in a nonthreatening and genuinely caring manner. In studying approaches to authority figures, you are encouraged to analyze your overall personal responses to authority, as in Exercise 23-1.
Managing Nursing Staff Problems: Improving how nurses deal with conflict is an investment in coworkers, our organization, and ultimately in improved client outcomes. Nonaction has been identified as the most common repressive management strategy (Bacal, n.d.). Nurse managers have learned that ignoring conflict among staff does not solve problems. Avoidance perpetuates the status quo or leads to an escalation. When managed appropriately, you reduce time wasted by staff in griping, defending, and so on, as illustrated in the following case.
Collaborating with peers
The nurse-client relationship occurs within the larger context of the professional relationship with other health disciplines. How the nurse relates to other members of the health team will affect the level and nature of the interactions that transpire between nurse and client. Interpersonal conflict between health team members periodically is concealed from awareness and projected onto client behaviors.
The client’s agitated behavior began to escalate again, and another interdisciplinary conference was called. Although the stated focus of the dialogue was on constructive ways to help Mr. Tomkins cope with disruptive anxiety, the underlying issues related to the strong feelings of the day nursing staff that their interventions were being undermined. Equally strong was the conviction of the evening staff that they were acting in the client’s best interest by letting him out of the seclusion room as soon as his behavior normalized. Until the underlying behaviors could be resolved satisfactorily at the staff level, the client continued to act out the staff’s anxiety, as well as his own.
Similar types of issues arise now and again when there is no input from different work shifts in developing a comprehensive nursing care plan. The shift staff may not agree with specific interventions, but instead of talking the discrepancy through in regularly scheduled staff conferences, they may act it out, unconsciously undoing the work of the other shifts.
Occasionally you may have to work with a peer with whom you develop a “personality conflict.” Stop and consider what led up to the current situation. Generally it is due to an accumulation of small annoyances that occurred over time. The best method to avoid such situations is to verbalize occurrences rather than ignoring them until they become a major problem. Avoid the “blame game” and discuss in a private, calm moment what you both can do to make things better.
Whenever there is covert conflict among nursing staff or between members of different health disciplines, it is the client who ultimately suffers the repercussions. The level of trust the client may have established in the professional relationship is compromised until the staff conflict can be resolved.
Delegation or supervision of unlicensed personnel
Delegation is defined as the transfer of responsibility for the performance of an activity from one individual to another while retaining accountability for the outcome. Whether delegating to a peer or unlicensed assistive personnel (UAP), the nurse is only transferring the responsibility for the performance of the activity, not the professional accountability for the overall care (American Nurses Association, 1994). In earlier times, delegating and trusting went hand in hand, because the nurse was transferring responsibility to a peer and had some assurance of the skills and knowledge of that peer. The present health care environment poses a much different reality in which some UAPs possess minimal experience, skills, or knowledge.
The challenges of maintaining professional integrity and concurrently surviving in today’s health care arena are felt by nurses in all settings. Effective and appropriate use of delegation can facilitate your ability to meet these challenges. But more often than not, novice nurses are inadequately prepared for the demands of delegating much of their nursing tasks to UAPs while retaining responsibility for interpreting patient outcomes.
Inherent in effective delegation is an adequate understanding of the skills and knowledge of UAPs, as well as of the Nurse Practice Act of the state in which you are practicing. Within each state’s Nurse Practice Act are specific guidelines describing what nursing actions can and cannot be delegated, and to what type of personnel these actions can be delegated. In addition to knowing nurse practice guidelines and the skills and knowledge level of UAPs, the nurse must educate and reinforce the UAPs’ knowledge base, assess the UAPs’ readiness for delegation, delegate appropriately, oversee the task, and evaluate and record the outcomes. The appropriate implementation of these principles (e.g., educating, assessing, overseeing, and evaluating) is a costly process both in time and energy. Practice Exercise 23-2 to facilitate your understanding of the principles. The following case example highlights one particular principle.
Advocacy
Nursing organizations have identified trends toward increased use of unlicensed workers in agencies wishing to reduce costs. Such organizations speak out about the burden this places on registered nurses. Becoming active in your state nurses’ association or professional specialty organization allows you to add your voice to this debate. Obtain a copy of your state’s Nurse Practice Act. Usually these can be downloaded from your state Board of Nursing’s Web site. This document will spell out what you, as a registered nurse, can delegate and to whom.
Even as a beginning staff nurse you will be expected to delegate some client care duties to others. You are responsible for the completeness, quality, and accuracy of this care. To avoid conflicts in delegating client care, clearly state your expectations. It is your responsibility to ensure that care was given correctly.
Strategies to remove barriers to communication with other professionals
Just as you treat clients with respect, you have an ethical responsibility to treat coworkers with respect. Nurses need to be appreciated, recognized, and respected as professionals for the work they do. Unsupportive and uncivil coworkers and workplace conflicts negatively influence retention of nursing staff. Communication can become distorted rather than open when you are concerned about offending a more powerful individual. Strategies for dealing with disrespectful or disruptive behaviors include establishing common communication expectations and skills (described in Chapter 22), teaching conflict resolution skills, and creating a culture of mutual respect within the health care system. Ideally, the system has ongoing education, leadership and team collaboration support, and policies to evaluate behavior violations.
Clarify communications
You can use skills taught in this textbook to improve both the clarity of message content and the emotional tone of interactions. Communication problems lead to a large percentage of disruptive behaviors, especially telephone communication. Message clarity is enhanced when standardized formats such as SBAR, discussed in Chapter 22, are used: The nurse identifies self by name, position, the client by name, diagnosis, the problem (include current problem, vital signs, new symptoms, etc.), and clearly states his or her request.
Use conflict resolution strategies and respond to putdowns and destructive criticisms
The strategies for handling angry clients, as described in Chapter 14, can be applied to your relations with anger from colleagues. This chapter details a number of conflict resolution steps (see Box 23-3). In addition, you need to develop a strategy to respond to unwarranted putdowns and destructive criticisms. Generally, they have but one intent: to decrease your status and enhance the status of the person delivering the putdown. The putdown or criticism may be handed out because the speaker is feeling inadequate or threatened. Often it has little to do with the actual behavior of the nurse to whom it is delivered. Other times the criticism may be valid, but the time and place of delivery are grossly inappropriate (e.g., in the middle of the nurses’ station or in the client’s presence). In either case, the automatic response of many nurses is to become defensive and embarrassed, and in some way actually begin to feel inadequate, thus allowing the speaker to project unwarranted feelings onto the nurse.
Recognizing a putdown or unwarranted criticism is the first step toward dealing effectively with it. If a comment from a coworker or authority figure generates defensiveness or embarrassment, it is likely that the comment represents more than just factual information about performance. If the comment made by the speaker contains legitimate information to help improve one’s skill and is delivered in a private and constructive manner, it represents a learning response and cannot be considered a putdown. Learning to differentiate between the two types of communication helps the nurse to “separate the wheat from the chaff.”
Whereas the first response allows the nurse to learn useful information to incorporate into practice, the second response serves to antagonize, and it is doubtful much learning takes place. What will happen is that the nurse will be more hesitant about approaching the supervisor again for clinical information. Again, it is the client who ultimately suffers.
Once a putdown is recognized as such, you need to respond verbally in an assertive manner as soon as possible after the incident has taken place. Waiting an appreciable length of time is likely to cause resentment and loss of self-respect. It may be more difficult later for the other person to remember the details of the incident. At the same time, if the nurse’s own anger, not the problem behavior, is likely to dominate the response, it is better to wait for the anger to cool a little and then to present the message in a more reasoned manner.
Process for responding to putdowns
In responding to putdowns, the nature of the relationship should be considered. Attitudes are important. Respect for the value of each individual as a person should be evidenced throughout the interaction. Try to determine how to respond to this person in a productive way so that you are on speaking terms but still get your point across. Even if you do not fully succeed in your initial tries, you probably will have learned something valuable in the process.
Address the objectionable or disrespectful behaviors first. Briefly state the behavior and its impact on you. It is important to deliver a succinct verbal message without getting lost in detail and without sounding apologetic or defensive. Do not try to give a prolonged explanation of your behavior at this point in the interaction and do not suggest possible motivations.
Emphasize the specifics of the putdown behavior. Once the putdown has been dealt with, you can discuss any criticism of your behavior on its own merits. Refer only to the behaviors identified and do not encourage the other person to amplify the putdown.
Prepare a few standard responses. Because putdowns often catch one by surprise, it is useful to have a standard set of opening replies ready. Examples of openers might include the following:
A reply that is specific to the putdown delivered is essential. The tone of voice needs to be even and firm. In the clinical example given previously, the nurse might have said to the head nurse: “My school is not an issue, and your criticism is unnecessary,” or “It seems to me that the assessment of the child’s ears, not my school, is the issue, and your superior tone is uncalled for.”
An important aspect of putdowns is that they get in the way of the nurse’s professional goal of providing high-quality nursing care to clients. The effect of the head nurse’s second response is for both nurses to assume the reddened eardrums are from crying and not to reevaluate the child’s eardrums. Feeling resentful and less sure of her clinical skills, the staff nurse is less likely to risk stirring up such feelings again. If fewer questions are asked, important information goes unshared. In the clinical example just cited, a possible ear infection might not be detected.
Criticize constructively
Giving constructive criticism and receiving criticism is difficult for most people (Box 23-4). When a supervisor gives constructive criticism, some type of response from the person receiving it is indicated. Initially, it is crucial that the conflict problem be clearly defined and acknowledged. To help handle constructive criticism, nurses can do the following:
• Schedule a time when you are calm.
• Request that supervisory meetings be in a place that allows privacy.
• Listen carefully to the criticism and then paraphrase it.
• Acknowledge that you take suggestions for improvement seriously.
• Discuss the facts of the situation but avoid becoming defensive.
• Develop a plan for dealing with similar situations; become proactive rather than reactive.
Use peer negotiation
As students, you will encounter situations in which the behavior of a colleague causes a variety of unexpressed differences or disagreement because the colleague’s interpretation of a situation or meaning of behavior is so different from yours. The conflict behaviors can occur as a result of age differences, differences in values, philosophical approaches to life, ways of handling problems, lifestyles, definitions of a problem, goals, or strategies to resolve a problem. These differences cause friction and turn relationships from collaborative to competitive.
Generally, conflict increases anxiety. When interaction with a certain peer or peer group stimulates anxious or angry feelings, the presence of conflict should be considered. Once it is determined that conflict is present, look for the basis of the conflict and label it as personal or professional. If it is personal in nature, it may not be appropriate to seek peer negotiation. It might be better to go back through the self-awareness exercises presented in previous chapters and locate the nature of the conflict through self-examination.
Sharing feelings about a conflict with others helps to reduce its intensity. It is confusing, for example, when nursing students first enter a nursing program or clinical rotation, but this confusion does not get discussed, and students commonly believe they should not feel confused or uncertain. As a nursing student, you face complex interpersonal situations. These situations may lead you to experience loneliness or self-doubt about your nursing skills compared with those of your peers. These feelings are universal at the beginning of any new experience. By sharing them with one or two peers, you usually find that others have had parallel experiences. In reviewing Exercise 23-3, think of a conflict or problem that has implications for your practice of nursing, one you would be willing to share with your peers.
Self-awareness is beneficial in assessing the meaning of a professional conflict. Now that you have had an opportunity to study different types of conflict, work on Exercise 23-4.
Develop a support system
Collegial relationships are an important determinant of success as professional men and women entering nursing practice. Studies show the importance of mutual support (Woelfle & McCaffrey, 2007).
Although there is no substitute for outcomes that demonstrate professional competence, interpersonal strategies can facilitate the process. Integrity, respect for others, dependability, a good sense of humor, and an openness to sharing with others are communication qualities people look for in developing a support system.
Forming a reliable support system at work to share information, ideas, and strategies with colleagues adds a collective strength to personal efforts and minimizes the possibility of misunderstanding. With problem or conflict situations, getting ideas from trusted colleagues beforehand enhances the probability of accomplishing outcomes more effectively. An Australian study of 157 registered nurses working in a private hospital found that support lowered job-related stress and increased job satisfaction. Support was given to nurses by supervisors and other nurses (Bartram, Joiner, & Stanton, 2004).
Professional organizations do not usually have the primary purpose of providing emotional support; however, small subgroups within professional organizations may be used for personal support. A professional support group composed of individuals with similar work experience can be comforting. Often, family and friends have a limited understanding of the emotional impact of your experiences.
Use group process
Creating opportunities for interdisciplinary groups to get together is a highly effective strategy for enhancing collaboration and communication. Ideas include collaborative rounds, team briefings, and committees to discuss problems. Some studies associate daily team rounds and joint decision making with shorter hospital stay and lower hospital charges.
Team briefing meetings
In addition to clarifying client information exchange and opening communication, some meetings could focus on opening up communication in a nonantagonistic fashion focusing on improving “people skills” such as conveying mutual respect and improving staff relations. Conflict situations among colleagues or among departments become negative when not dealt with. Recognition provides a potential opportunity for improvement. When effectively addressed, there is a tendency for the team to become stronger and to function more effectively.
Organizational work groups
Successful participation in work groups requires flexibility and good communication. This is especially true when the task is to implement some agency change. The Joint Commission also recommends violence audits and violence prevention inservice programs for all employees to address techniques for violence de-escalation (www.jointcommission.org/SentinelEventAlert/Issue45, June 3, 2010).
Work toward an organizational climate of mutual respect
As mentioned earlier, the Joint Commission is requiring all health care organizations to have written codes of behavior and to establish internal processes to handle disruptive behaviors. Organizational strategies are discussed in Chapter 22; other strategies within the organization could include understanding the organizational system.
Understand the organizational system
Whenever you work in an organization, you automatically become a part of a system that has norms for acceptable behavior. Each organizational system defines its own chain of command and rules about social processes in professional communication. Even though your idea may be excellent, failure to understand the chain of command or an unwillingness to form the positive alliances needed to accomplish your objective dilutes the impact. For example, if your instructor has been defined as your first line of contact, then it is not in your best interest to seek out staff personnel or other students without also checking with the instructor.
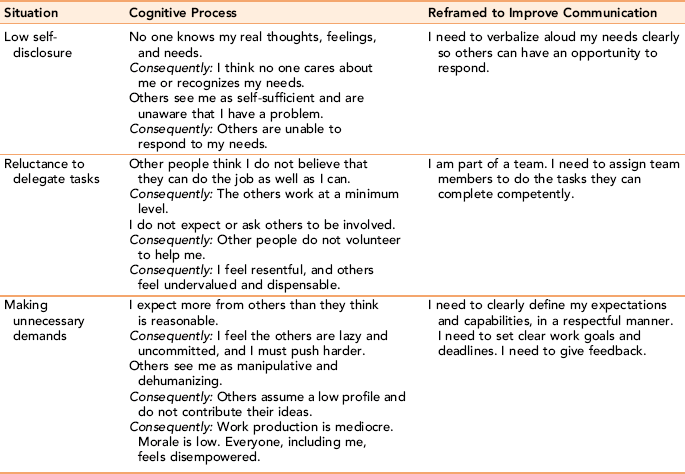
Although sidestepping the identified chain of command and going to a higher or more tangential resource in the hierarchy may appear less threatening initially, the benefits of such action may not resolve the difficulty. Furthermore, the trust needed for serious discussion becomes limited. Some of the reasons for avoiding positive interactions stem from an internal circular process of faulty thinking. Because communication is viewed as part of a process, the sender and receiver act on the information received, which may or may not represent the reality of the situation. Examples of the circular processes that block the development of cooperative and receptive influencing skills in organizational settings are presented in Table 23-1.
Document and use the complaint procedure to report incidences
In handling disruptive behavior occurrences, documentation is a key step. Some suggest beginning with a staff survey. Some agencies may hold “communication training sessions” after the offenses have been documented. Prevention strategies might include participation in assertiveness training inservices or the TeamSTEPPS program as cited in Chapter 22. Educational interventions that increase staff awareness are extremely effective, as are rehearsals similar to the exercises in this book (Bigony et al., 2009).
Summary
In this chapter, the same principles of communication used in the nurse-client relationship are broadened to examine the nature of communication among health professionals. Most nurses will experience conflicts with coworkers at some time during their careers. The same elements of thoughtful purpose, authenticity, empathy, active listening, and respect for the dignity of others that underscore successful nurse-client relationships are needed in relations with other health professionals. Building bridges to professional communication with colleagues involves concepts of collaboration, coordination, and networking. Modification of barriers to professional communication includes negotiation and conflict resolution. Learning is a lifelong process, not only for nursing care skills but for communication skills. These will develop as you continue to gain experience working as part of an interdisciplinary group.
References
American Association of Critical Care Nurses. Zero tolerance for abuse position statement, 2004. www.aacn.org/WD/Practice/Docs/Zero_Tolerance_for_Abuse.pdf
American Medical Association Disruptive behavior: model medical staff code of conduct, 2008. Available online:, www.ama-assn.org/ama/pub/about-ama/our-people, www.ama-assn.org/go/omss. [Accessed March 14, 2009].
American Nurses Association. Code of Ethics for nurses with interpretative statements. Washington, DC: Author, 2001.
American Nurses Association. Registered professional nurses and unlicensed assistive personnel. Washington, DC: Author, 1994.
Bacal, R. Dealing with angry employees. [online article], n.d. Available online: http://work911.com/articles/angrye.htm.
Bacal, R. Organizational conflict: the good, the bad & the ugly. [online article], n.d. Available online: http://work911.com/articles/orgconflict.htm.
Bartram, T., Joiner, T.A., Stanton, P., et al. Factors affecting the job stress and job satisfaction of Australian nurses: implications for recruitment and retention. Contemp Nurse. 2004;17(3):293–304.
Bigony, L., Lipke, T.G., Lundberg, A., et al. Lateral violence in the perioperative setting. AORN J. 2009;89(4):688–696.
Boone, B.N., King, M.L., Gresham, L.S., et al. Conflict management training and nurse-physician behaviors. J Nurses Staff Dev. 2008;24(4):168–175.
Bournes, D.A., Milton, C.L. Nurses’ experiences of feeling respected-not respected. Nurs Sci Q. 2009;22(1):47–56.
Gerardi, D., Connell, M.K. The emerging culture of health care: from horizontal violence to true collaboration. Nebr Nurse. 2007;40(3):16–18.
Hutchinson, M., Vickers, M., Jackson, D., et al. I’m gonna do what I want to do: organizational change as a legitimized vehicle for bullies. Health Care Manag Rev. 2005;30(4):331–336.
Johnson, S.L. International perspectives on workplace bullying among nurses: a review. Int Nurs Rev. 2009;56:34–40.
Johnson, S.L., Rea, R.E. Workplace bullying: concern for nurse leaders. J Nurs Admin. 2009;39(2):84–90.
Joint Commission for the Accreditation of Healthcare Organizations, Behaviors that undermine a culture of safety. Sentinel Event Alert, 2008;40(July 9):1–3. www.jointcommission.org/SentinelEventAlert/.
Joint Commission for the Accreditation of Healthcare Organizations, Preventing Violence in the health care setting. Sentinel Event Alert, 2010;45(June 3):1–3. www.jointcommission.org/SentinelEventAlert/.
Joint Commission Resources. Civility in the health care workplace, 2009;vol 6:1–8. Available online:, http://www.jcipatientsafety.org/15419/. [Accessed March 1,].
Katrinli, A., Atabay, G., Gunay, G., et al. Leader-member exchange: organizational identification and the mediating role of job involvement for nurses. J Adv Nurs. 2008;64(4):354–362.
Kerfoot, K. Moving toward zero: the leader’s mandate. Nurs Econ. 2008;26(5):331–332.
Nielsen, P., Mann, S. Team function in obstetrics to reduce errors and improve outcomes. Obstet Gynecol Clin. 2008;35(1):61–65.
O’Daniel, M., Rosenstein, A.H. Professional communication and team collaboration. In: Hughes R.G., ed. Patient safety and quality: an evidence-based handbook for nurses. Rockville, MD: Agency for Research and Quality, 2008. [[AHRQ Pub no. 08-0043]].
Olender-Russo, L. Creating a culture of regard: an antidote for workplace bullying. Creat Nurs. 2009;15(2):75–81.
O’Reilly, K.B. AMA meeting: disruptive behavior standard draws fire. Available online: www.ama-assn.org/amednews/2008/12/01/prse1201.htm.
Parse, R.R. Feeling respected: a Parse method study. Nurs Sci Q. 2006;19:51–56.
Rosenstein, A.H., O’Daniel, M. Disruptive behavior and clinical outcomes: perceptions of nurses and physicians. Am J Nurs. 2005;105(1):54–64.
Seago, J.A. Professional communication. In: Hughes R.G., ed. Patient safety and quality: an evidence-based handbook for nurses. Rockville, MD: Agency for Healthcare Research and Quality, 2008. [[AHRQ Publication no. 08-0043]].
Spence-Laschinger, H.K., Leiter, M., Day, A., et al. Workplace empowerment, incivility and burnout: impact on staff nurse recruitment and retention outcomes. J Nurs Manag. 2009;17:302–311.
Wachs, J. Workplace incivility, bullying, and mobbing. AAOHN. 2009;57(2):88.
Woelfle, C.Y., McCaffrey, R. Nurse on nurse. Nurs Forum. 2007;42(3):123–131.