Communication for a Safe Environment
At the end of the chapter, the reader will be able to:
1 Identify client communication safety goals.
2 Identify how communication skills enhance client safety, as well as quality of care.
3 Describe why client safety is a complex system issue, as well as an individual function.
4 Describe how open communication and organizational error reporting contribute to a culture of safety.
5 Discuss how to advocate for safe, high-quality care as a team member.
6 Use simulations to demonstrate communication skills that affect client care; specifically apply standardized formats such as SBAR in a simulated conversation with a physician.
This chapter focuses on communication concepts designed to assist nurses and their health team colleagues in creating a safe environment for their clients. Although “safety” is recently getting increased attention, client safety is (and has always been) a priority in nursing care (Gore, Hunt, & Raines, 2008). Quality of care is dependent, in part, on communication (Joint Commission on Accreditation of Healthcare Organizations [JCAHO], 2008). Miscommunication is a dominant factor cited in error reports. The quality of communication and the quality of the client-provider relationship have long been used as indicators of quality of care (Agency for Healthcare Research and Quality [AHRQ,c]).
Basic concepts
In healthcare organizations, safety is generally defined as freedom from accidental injury. Since the days of Hippocrates, the concept of “do no harm” has been incorporated into healthcare ethical practice. The nursing profession has always had safe practice as a major goal. It is the basic tenet of the American Nurses Association’s Code of Ethics for Nurses. The National Patient Safety Foundation (NPSF; online, www.npsf.org/pdf/r/researchagenda.pdf) has a more specific definition: “avoidance, prevention, amelioration of adverse outcomes or injuries stemming from the process of healthcare itself.” In a more comprehensive definition, the American Association of Colleges of Nursing (AACN, 2006a) defines safety as the minimalization of risk for harm to patients and to providers through both system effectiveness and individual performance. Health care organizations and professional organizations generally try to ensure safe care by establishing safety rules and procedures. This chapter restricts discussion to innovations in communication procedures designed to improve client safety.
Recent overall safety issues
In the early part of this century, the quality and safety of health care in the United States was mediocre or worse (Bates, 2009). In a British study comparing mortality data from the United States with 14 other Western countries between 1997 and 2003, the United States had only a 4% decrease in deaths from amenable causes, whereas the average decrease for other countries was 17% (Nolte & McKee, 2008). Much has changed in our practice since the landmark 1999 Institute of Medicine (IOM) study that found that preventable health care errors were responsible for almost 98,000 deaths each year in the United States. This IOM report, “To Err Is Human: Building a Safer Health System,” made client safety a national American priority (Kohn, 1999).
Expense, resistance to change, and the lack of centralized data reporting slowed adoption of new practices. Worldwide, unsafe practice has compromised care for clients in many countries. Errors have a high financial cost in addition to the human cost, exceeding $29 billion dollars per year just in the United States (AHRQb). It is estimated that 70% of reported errors are preventable. “Preventable” means the error occurs through a medical intervention, not because of the client’s illness. Fatigue is repeatedly cited as a factor contributing to errors. Risk doubled when nurses worked more than 12 consecutive hours (Scott, Rodgers, Hwang, & Zhang, 2006). Medical and Nursing organizations, as well as health care delivery organizations, have taken initiatives designed to foster “best practice” safer client care by designing protocols for care that are evidence based. At the same time, new technology tools are making care safer (refer to Chapters 25 and 26). This chapter limits discussion to only those practices relevant to communication.
Nurses are often the “last line of defense” against error. It is an ethical imperative (Lachman, 2008). Nurses are in a position to prevent, intercept, or correct errors. Individual nurses have many opportunities to prevent error, particularly by communicating clearly to others even when the hierarchy seems to discourage questioning authorities (Donaldson, 2008). The quality of your communication affects safety factors such as medication errors, client injuries from falls, clinical outcomes related to client adherence to his treatment plan, and rehospitalization rates. The Applications section of this chapter focuses on nursing communication practices to promote safer care.
Poor communication compromises client safety
Multiple studies have pinpointed miscommunication as a major causative agent in sentinel events, that is, errors resulting in unnecessary death and serious injury (Leonard & Bonacum, 2008). Poor communication has been identified as the root cause of serious medical errors as much as 70% of the time in reported errors (Joint Commission, b,c). However, errors do not usually have one cause but result from a series of flaws in the care system. The problem is complex; therefore, solutions also will be complex.
Medication errors
According to the American Medical Association (AMA, eVoice, 2008), approximately 80% of medication errors are due to communication breakdown. Although some medication errors stem from lack of knowledge about the drug (its side effects, etc.), many other drug errors occur when a nurse fails to follow the rules for verification: right med, right client, right dose, and right time.
Miscommunication during “handoff” transfers of client
Miscommunication errors most often occur during a handoff procedure, when one staff member transfers responsibility for care to another staff member. More than half of incidences of reported serious miscommunications occurred during client handoff, when those assuming responsibility for the client (coming on duty) are given a verbal, face-to-face synopsis of the client’s current condition by those who had been caring for him and are now going off duty (Evans, Pereira, & Parker, 2008; Henkind & Sinnett, 2008).
Client outcomes
The literature suggests some progress in preventing sentinel events, but errors are still common, resulting in unnecessary harm to clients. In addition to errors, outcomes include increased costs, increased rates of hospitalization, longer recovery rates, and more medical complications. Beside risks to client safety, poor communication is also related to client dissatisfaction and risk for malpractice lawsuits. A survey of clients found that 34% experienced errors and 68% cited poor communication between nurses and physicians and others as a cause of errors (Kaiser Family Foundation, 2004). Annual current statistics about sentinel events are available on the Joint Commission Web site (TJC, c).
New initiatives for safer care
We are redeveloping our health care system to make client care safer. There is consensus that this requires improving communication. Best nurse-physician collaborative communication has empirically been associated with lower risk for negative client outcomes and greater satisfaction. Research studies support this concept (DeVoe, Wallace, Pandhi, Solotaroff, & Fryer, 2008; Elder, Brungs, Nagy, Kudel, & Render, 2008). The current renewed focus on improving patient safety will cause standardization of many health care practices. “Standardization is among the best methods to improve quality and reduce costs of care…even if the standard is something as simple as a checklist” (Mathews & Pronovost, 2008, p. 2914). Changes in communication to reduce errors and increase safety need to be institutionalized at the system level and implemented consistently at the staff level. Safe communication about client care matters needs to be clear, unambiguous, timely, accurate, complete, open, and understood by the recipient to reduce errors (Amato-Vealey, Barba, & Vealey, 2008).
Communication goals and standards to improve client safety
Overall, medical goals are complex and have shifting priorities. Safe client care is always a priority, however. Measuring safety is problematic because not everyone uses the same definitions of “unsafe,” nor do they use the same outcome measures. The number of surgeries done on the wrong site is a very specific outcome, even though most hospitals do not report to a national overseer in the United States, so data may not be readily accessible. When we focus on communication problems leading to adverse client outcomes, the data are much less specific. With the current increased focus on improving communication to promote a climate of client safety, we need communication that is open and client centered. Safety goals to improve communication about clients among his or her various providers are aimed at reducing client mortality, decreasing medical errors, and promoting effective health care teamwork. These goals need to be mutually established by the health team in a climate of respect to assure maximum clarity among providers.
Communication health care safety goals from governing organizations include:
1. IOM’s 8 Goals. A worldwide wake up occurred when IOM published their report, citing hospital errors as causing almost 100,000 deaths per year. Yet, 5 years later, Nolte and McKee’s (2008) analysis showed more than 101,000 preventable deaths per year in clients younger than 75 years. The IOM specifically included improving accurate, complete communication as one of their eight goals. IOM has suggested that hospitals need to create structured handoff protocols, that is, a standardized format for reporting client status when care provider A goes off duty, turning care responsibility over to care provider B. This standardized communication format is needed to facilitate better communication for patient safety.
2. AHRQ in the Department of Health and Human Services, with a Congressional mandate, has taken a leading role in the United States to improve client safety. AHRQ’s role is to prevent medical errors and promote client safety. They fund research and compile data to develop and publish “best practices” evidenced-based care protocols. Several other sites publish “best practice info” (online resources such as http://healthlinks.washington.edu/ebp).
3. The World Health Organization (WHO), a part of the United Nations, has actively sought to improve worldwide client safety. In 2005, WHO designated Joint Commission International as the WHO Collaborating Center for patient safety solutions. In 2007, WHO (Joint Commission International) published nine solutions; number 2 is “correctly identifying the patient,” and number 3 is “better communication during patient hand-over” (from one caregiver to another).
Communication goals for healthcare safety from professional organizations include:
1. Joint Commission Guidelines. This organization regulates hospitals. They attribute more than 60% of sentinel events in hospitals to miscommunication. Many of their current National Patient Safety Goals are aimed at structuring and improving communication. Goal 2 is to improve the effectiveness of communication among caregivers. Section 2E addresses communication guidelines needed to manage handoff communication. When a client is transferred or “handed off” to another care provider, unit, or agency, hospitals are encouraged to develop a standard communication protocol to improve the effectiveness of communication. This should result in increased client safety (AHRQ,c).
2. AACN. Recommendations for nursing curriculums related to safety and communication include application of research-based/evidence-based knowledge as the basis for practice; recognition that safety is a complex issue that involves all providers; establishing and maintaining…open communication and cooperation within the interdisciplinary team; and using standardized “hand off” communications (AACN, 2006a).
Changes toward bettering communications leading to safer care
General communication problems identified by the AMA are listed in Box 22-1. Foremost recommendations include:
Use “best practices” by increasing use of evidenced-based “best practice” versus “usual practice.” Agencies such as AHRQ (c) have begun to fund research to identify the most effective methods of promoting clear communication among health team members and agencies, as well as the most effective treatments. This information is used to develop and distribute protocols for best practice, including formats of standard communication techniques. We need more studies of interventions to promote best communication between nurse and physician with documented outcomes for clients.
Create a team culture of safety communication. Creating effective health teams means getting all team members to value teamwork more than individual autonomy. Team culture includes shared norms, values, beliefs, and staff expectations. In Canada, Sutter et al.’s 2009 study, as well as findings from the Canadian Health Services Research Foundation, identified effective team communication as a core competency. Team collaborative communication strategies involve shared responsibility for problem solving and decision making, as well as coordination of care. Teamwork failures including poor communication and failures in physician supervision have been implicated in two-thirds of harmful errors to clients (Singh, Thomas, Peterson, & Studdert, 2007). Creating a safe environment requires us to communicate openly, to be vigilant and accountable. Systems should create expectations of a work environment in which staff can speak up and express concerns, and alert team members to unsafe situations.
Problems or barriers for individual health care workers
Strategies for effective communication to promote client safety are listed in Box 22-2. They are discussed in the following subsections.
Usual practice versus empirically derived best practices
There is a major lack of research utilization for best practice. Though you are exposed to the use of research findings in your practice, many staff nurses lack the time and skills to actively seek new study results that would improve their daily practice. Physicians are still likely to use their own experience rather than documented recommended best practice methods. Research-based evidence is often absent or lacks high-quality consensus. Widespread adoption of best practices had not yet been accomplished in the decade after IOM’s 1999 report. Best practice recommended therapies were found to have been received by only 55% of adult clients and 47% of child clients (Mangione-Smith et al., 2007).
Communication differences among professions
Each profession has its unique vocabulary and method of communicating. Physician’s expectations may be “just the facts” briefly, whereas nurses have been educated to describe the broad picture. Medical communication is a goal-oriented, problem-solving behavior, which requires not only skill practicing but reflection on the process and outcome. Developing communication skills has now become a curriculum thread in nursing educational programs.
Hierarchical power differences exist between physicians and nurses. This difference in power intimidates some nurses communicating with physicians. Historic autonomy for physicians is being replaced by empowerment of teams for decision making. The concept of equity is integral to a functioning team. Historically, physicians and nurses are accustomed to working in a hierarchy where physicians make treatment decisions independently rather than though consultations with a team. This is sometimes termed medicine’s “culture of individualism.” Implementing measures specified by best practice evidence and sharing decision making about the client’s care require that physicians correspondingly relinquish some autonomy (Mathews & Pronovost, 2008). Effective teamwork, including open communication, openness to new concepts, and honest error reporting, are basic components in establishing a new safety culture. This requires some readjustment in the way both physicians and nurses think about their roles.
Reluctance to report errors
According to IOM, only a tiny fraction of unsafe care incidents are submitted to reporting databases or agencies (Kohn, 1999). Some estimate that more than 90% of errors go unreported (Elder et al., 2008). A redesign is needed if we really want to create a culture of safety. The health care industry is looking at models created by other industries such as aviation or nuclear power, which have excellent safety records. Aviation’s successful Crew Resource Management practice model has been used as a template for some in the health care industry. One needed step is to require the reporting of “near misses” so new safer protocols can be created. A centralized agency, such as the United Kingdom’s Patient Safety Agency, with a database on instances of errors and near misses would provide a database for analyses that would be of great use in designing safer delivery systems. In the United States, error reporting is hidden, underreported, and local, rather than being nationally available. Accurate incident reporting and greater transparency are crucial if future errors are to be prevented.
Another step in creating a culture of safety is to overcome current fear of punitive outcomes involved in error reporting. Providers are concerned about negative consequences of disclosing errors, such as malpractice litigation, reputation damage, job security, personal feelings such as loss of self-esteem, among others. Elder et al.’s (2008) study reported that nurses remain strongly conflicted about disclosing their errors to peers and physicians. In their survey, less than half of the intensive care unit nurses witnessing a near-miss error were likely to report it. Creating a new safety climate would require retraining nurses in error disclosure to help prevent future errors. Meanwhile providers struggle with the current systems for reporting errors.
Low level of client health literacy versus client education
Multiple studies show that health-care–related communication occurs at a level far exceeding the understanding abilities of the majority of average persons (Denham, 2008). According to the AMA, 50% of adults are at increased risk for serious adverse health consequences because of their low level of understanding of medical terminology and their tendency to hide this problem from their doctors and nurses. Inadequate heath literacy leads clients to misunderstand information about their treatment, causing errors.
Barriers in the current health care system
Problems with structural barriers in health care organizations that impede communications
The greatest barrier to safer care is fragmentation of care systems. Evidenced-based practices have to be reinforced and implemented at a system-wide level. Although most hospitals and agencies have some form of error reporting, they lack a system-wide department for processing safety information. One model to be emulated is that of Kaiser Permanente, which implemented a national patient safety plan in 2000.
Applications
Discussion in this section is limited to safety strategies that promote effective communication such as the mantra “Simplify, Clarify, Verify” (Fleischmann, 2008). A few general strategies are mentioned. (For a complete discussion, refer to OM [2001, 2004].) Consider how you will apply evidence-based practice information such as that in the sample.
New teaching strategies to help nurses learn to communicate for safer care
Quality and Safety Education competencies for all Nurses (QSEN) have been developed by national leaders in nursing education (for full discussion, refer to Cronenwett et al. [2007]). Among these competencies are communication skills. Some new teaching strategies help students.
Develop a safety priority attitude
The IOM has urged organizations to create an environment in which safety is a top priority. For example, equipment can be standardized and simplified, and display a readout about the reason an alarm is ringing. One of our primary roles as nurses is to advocate for client safety. Beyea (2008a) recommends that nurses, as individuals, take active efforts to improve our safety understanding, beginning by assessing our own safety learning needs in our particular area of practice (online, NPSF: EdNeedsAsessment, www.npsf.org/pdf/r/researchagenda.pdf). Errors occur when you assume someone else has addressed a situation (Beyea, 2008b). A prime goal is to improve communication about client condition among all the people providing care to that client.
Use practice simulations
Virtual client-nurse scenarios, whether using technologically enhanced dummies or active learning situations such as case studies provided in this textbook, allow practice without risk for potentially devastating outcomes with an actual client care situation. Nursing education programs are beginning to use “live models” to simulate clients. Actors are trained to portray clients with specific illnesses. Student nurses practice communicating with them to elicit histories, as well as practicing skills such as physical examinations. (For more ideas, read Gore et al. [2008] and Henneman [2009].)
Develop an evidence-based practice
Close the gap between best evidence and the way communication occurs in your current practice (Figure 22-1). Apply information from evidence-based best practice databanks for safe practice. The process for development of practice guidelines, protocols, situation checklists, and so on is not transparent or easy. Solutions include gathering more evidence on which to base our practice. When is the “evidence” sufficiently strong to warrant adoption of a standardized form of communication about care? At the nurse-client level, Beauregard, nurse-administrator at Beaumont Hospital in Royal Oak, Michigan, has commented that “the nurse-patient relationship is a pivotal component of any patient safety program…(and) the number one driver of patient safety is communication” (Runy, 2008). We are beginning to compile best practice protocols for acute and preventative care; many are available on AHRQ’s Web site (online, www.ahrq.gov) or in their Patient Safety and Quality: An Evidence-Based Handbook for Nurses (Hughes, 2008). Even though these are free and available to all, studies show that best care is delivered only half of the time (Mangione-Smith et al., 2007). In regard specifically to communication, so far there is relatively scant research to designate specific communication formats that will lead to safer care. Some of the clinical strategies that show promise are described in the following subsections.
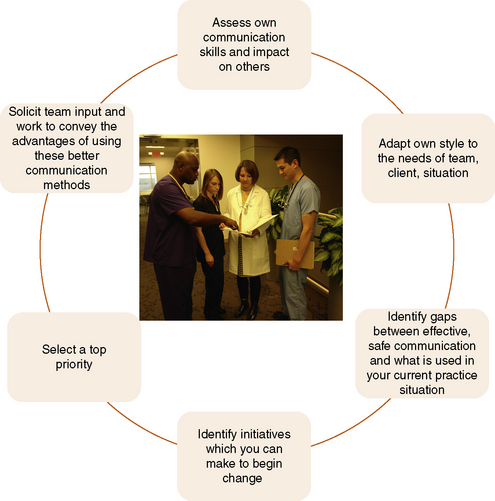
Figure 22-1 Communication competencies for creating safer care. (Adapted from Carey M, Buchan H, Sanson-Fisher R: The cycle of change: implementing best-evidence clinical practice, Int J Qual Healthc 21(1):37–43, 2009; Cronenwett L, Sherwood G, Barnsteiner J, et al.: Quality and safety education for nurses, Nurs Outlook 55(3):122–131, 2007.)
Use Data from Analyses of Error Data Reporting to Improve Nursing Practices
A metaanalysis of results from error reporting demonstration grants found that as error reporting improves, error detection rates increase and severity decreases (AHRQ, b,d).
Use Standardized Communication Tools
Safety communication improvement solutions include using standardized communications tools, participating in team training communicating seminars, adopting technology-oriented tools, and empowering clients to be partners in safer care. Communication that promotes client safety needs to include both communication of concise critical information and active listening. Physicians, nurses, medical technologists, pharmacists, and other givers of care work in what Shortell and Singer (2008) call “functional silos”; that is, they are educated separately and for the most part work separately, which has caused them to have differing methods of communication. Educational programs impart very different communication expectations for nurses than those taught to medical students. Nurses are taught to communicate in detailed narrative form, to describe the broad picture when discussing a client with his physician. Physicians are taught to speak concisely, to diagnose and summarize. Or as Leonard and Bonacum (2008) say, “Physicians want bullet points,” or just the headlines. Each group holds slightly different expectations about communication content and may have separate vocabularies. Nurses want their observations or assessments taken seriously. Solutions include team training and use of a standardized communication tool. Although currently there is no one universally accepted process, use of a shared format across disciplines can promote effective communication and client safety. The following are a sample of newer, more commonly used forms of team strategies designed to decrease or avoid errors of communication that lead to mistakes in health care.
Use of Checklists
Checklists serve as cognitive guides to accurate task completion. Checklists have been effectively used to improve client safety, especially in areas managing rapidly change, such as preoperative areas, emergency departments, and anesthesiology. Checklists have built-in redundancy. The floor nurse uses the preoperative checklist to verify that everything has been completed before sending the client to the surgical suite, but then this list is again checked when the client arrives but before the actual surgery. Such system redundancies are used to prevent errors. But they have limited and specific uses, and do not address underlying communication problems. No standardized protocol exists for checklist development, but use of expert panels with multiple pilot testing is recommended. One example found in most agency preoperative areas is a checklist where standard items are marked as having been done and available in the client’s record/chart. For example, laboratory results are documented regarding blood type, clotting time, and so forth. In one cardiac area study, one common cause of adverse events was missing equipment; therefore, a checklist might be used before surgery to verify the presence of specific needed equipment (Wong et al., 2007). Adoption of assertion checklists empowers any team member to speak up when they become aware of missing information.
Use of SBAR
In 2002, at Kaiser Permanente’s northern California regional risk management department’s perinatal patient safety project, physicians and nurses training together expressed disappointment with their communication. In response, Bonacum, Leonard, and other Kaiser administrators developed and encouraged staff to begin implementing a standardized briefing format (known by its acronym SBAR) for use by all staff communicating with each other—nurses, physicians, and all other team members. Adapted by Bonacum (2009) from principles used in communication on nuclear submarines, the SBAR tool provides structured language and fosters active listening. SBAR is designed to convey only the most critical information by eliminating excessive language. SBAR eliminates the authority gradient, flattening the traditional physician-to-nurse hierarchy. This makes it possible for staff to say what they think is going on. This improves communication and creates collaboration. This concise format is gaining wide adoption in the United States and Great Britain (Bonacum, 2009; Fleishmann, 2008; Leonard, 2009; Leonard & Bonacum, 2008). Refer to Box 22-3.
SBAR is used as a situational briefing, so the team is “on the same page” (Bonacum, 2009). SBAR simplifies verbal communication between nurses and physicians because content is presented in an expected format. In addition to communications between two individuals, it is used in small groups, such as the obstetrical delivery team and the surgical team. Success soon spread this format to use in surgery, for telephone contacts and in other acute care settings. Velji et al. (2008) have shown SBAR use to also be effective in improving safe communication in other types of agencies, such as rehabilitation facilities. Some, including Kaiser Staff, have even informally adopted it for their e-mail communications (Bonacum, 2009). Some hospitals use laminated SBAR guidelines at the telephones for nurses to use when calling physicians about changes in client status and requests for new orders (Leonard, 2009). Documenting the new order is the only part of SBAR that gets recorded. Refer to Table 22-1 for an example. Then practice your use of SBAR format in Exercise 22-1.
TABLE 22-1
SBAR Structured Communication Format
| S | Situation | Identify yourself; identify the client and the problem. In 10 seconds state what is going on. This may include client’s date of birth, hospital ID number, verification that consent forms are present, etc. |
| B | Background | State relevant context and brief history. Review the chart if possible before speaking or telephoning to the physician. Relate the client’s background, including client’s diagnosis, problem list, allergies, as well as relevant vital signs, medications that have been administered, laboratory results, etc. |
| A | Assessment | State your conclusion, what you think is wrong. List your opinion about the client’s current status. Examples would be client’s level of pain, medical complications, level of consciousness, problem with intake and output, or your estimate of blood loss, etc. |
| R | Recommendation or request | State your informed suggestion for the continued care of this client. Propose an action. What do you need? In what time frame does it need to be completed? Always should include an opportunity for questions. Some sources recommend that any new verbal orders now be repeated for feedback clarity. If no decision is forthcoming, reassert your request. |
Adapted from information during interviews with Leonard (2009), Bonacum (2009), and Fleishmann (2008).
“Evidence-based reports show that [client] adverse events have decreased through use of SBAR” (Denham, 2008, p. 39). Practicing use of standardized communication formats by student nurses has been found to improve their ability to effectively communicate with physicians about emergent changes in client condition (Krautscheid, 2008). Use of a common communication tool with non-nurse members of the health team should also reduce risk (see Figure 22-1). This format sets expectation about what will be communicated to another member of the health care team. Practice using this format in Exercises 22-2 and 22-3.
Team training: models of communication strategies for collaborative practice
Health provider collaborations
There is a close relationship between effective teamwork and client safety. Kramer and Schmalenberg developed a scale of five levels of collaboration based on their nursing research: collegial (equal in power but different); collaborative (mutual but not equal power); student-teacher (physicians have the power but are friendly and willing to inform nurses); neutral; and negative (physicians have total power and are disruptive to nurses, who then feel frustrated or hostile). The first three have good physician-nurse communication.
The majority of reported errors have been found to stem from poor teamwork and poor communication. An effective team has clear, accurate communication understood by all. All team members work together to promote a climate of client safety. To improve interdisciplinary health team collaboration, Boone and associates (2008) recommend that physicians and nurses jointly share communication training and team building sessions to develop an “us” rather than “them” work philosophy. When clashes occur, differences need to be settled. Specific conflict resolution techniques are discussed in Chapter 23.
Various models of team training
Team training is a tool to increase collaboration between physicians and nurses. Use of teams is a concept that has been around for years within medical and nursing professions. For example, medicine has used medical rounds to share information among physicians. Nursing has end-of-shift reports, when responsibility is handed over to the next group of nurses. Team training programs are available such as “TeamSTEPPS,” or Team Strategies and Tools to Enhance Performance and Patient Safety. This program emphasizes improving client outcomes by improving communication using evidence-based techniques.
Communication skills include briefing and debriefing, conveying respect, clarifying team leadership, cross-monitoring, situational monitoring feedback, assertion in a climate valuing everyone’s input, and use of standard communication formats such as SBAR and CUS. Creating a team culture means each member is committed to:
Nursing teamwork
The traditional client report from one nurse handing over care to another nurse needs to be accurate, specific, and clear, and allow time for questions to foster a culture of client safety. Using SBAR or any other standardized communication format for report would result in a safer environment for your clients (Amato-Vealey et al., 2008), as well as having staff work staggered shifts (Woods et al., 2008).
Regarding handoffs, AHRQ’s TeamSTEPPS program (2008) recommends that all team members use the “I PASS the BATON” acronym during any transition by staff in client care. Table 22-2 explains this communication strategy.
TABLE 22-2
| I | Introduction | Introduce yourself and your role |
| P | Patient | State patient’s name, identifiers, age, sex, location |
| A | Assessment | Present chief complaint, vital signs, symptoms, diagnosis |
| S | Situation | Current status, level of certainty, recent changes, response to treatment |
| S | Safety concerns | Critical laboratory reports, allergies, alerts (e.g., falls) |
| the | ||
| B | Background | Comorbidities, previous episodes, current medications, family history |
| A | Actions | State what actions were taken and why |
| T | Timing | Level of urgency, explicit timing and priorities |
| O | Ownership | State who is responsible |
| N | Next | State the plan: what will happen next, any anticipated changes |
Developed by the US Department of Defense. Department of Defense Patient Safety Program: Healthcare Communications Toolkit to Improve Transitions in Care. Falls Church, VA: TRICARE Management Activity; 2005.
Interdisciplinary rounds
Contemporary health care teams use “interdisciplinary rounds” to increase communication among the whole team—physicians, pharmacists, therapists, nurses, and dieticians (Woods et al., 2008). This strategy may increase communication and positively affect client outcome. For example, daily discharge multidisciplinary rounds have been correlated with decreased length of hospital stay.
Interdisciplinary “team” meetings can be used daily or weekly to explore common goals/concerns/options, smooth problems before they escalate into conflicts, or provide support. Lower on the scale are clinical teaching rounds, where a physician once weekly teaches nurses, which has the goal of encouraging physician communication with the nursing staff.
Establish open communication about errors
Most state Boards of Nursing require nurses to report unsafe practice by coworkers, but many nurses have mixed feelings about reporting a colleague, especially to a state agency (Elder et al., 2008). Physicians also have reservations about reporting problems (Zbar, Taylor, & Canady, 2009). One focus of team training can be creating an in-house agency system climate in which team members feel comfortable speaking out about their safety concerns. In this new nonpunitive reporting environment, staff are encouraged to report errors, mistakes, and near misses. In safety literature, compiling a database that includes near-miss situations that could have resulted in injury is important information in preventing future errors. They work in a climate in which they feel comfortable making such reports. A complete error reporting process should include feedback to the person reporting. Administrators should assume errors will occur and put in place a plan for “recovery” that has well-rehearsed procedures for responding to adverse events.
Briefings and debriefings
In team situations, such as in the operating room, the team may use another sort of standardized format. The leader (the surgeon, in this case) presents to the team a brief overview of what procedure is about to happen, asking anyone who sees a potential problem to speak up. In this manner, the leader “gives permission” for every team member to speak up. This can include the client also, as many clients will not speak unless specifically invited to do so. A debriefing is usually led by someone other than the leader. It occurs toward the end of a procedure and is a “recap” or summary as to what went well or what might be changed (Bonacum, 2009). This is similar to the feedback nurses ask clients to do after they have presented some educational health teaching, which verifies that the client understood the material.
Technology-oriented solutions create a climate of client safety to avoid errors
Prevention of misidentification of client is an obvious error prevention strategy. Before administering medication, the nurse needs to verify client allergies, use another nurse to verify accuracy for certain stock medications, and re-verify client’s identity. Joint Commission’s best practice recommendation is to check the client’s name band and then ask him to verbally confirm his name and give a second identifier such as his date of birth. Use of technology such as bar-coded name bands may offer protection against misidentification (AHRQ, d). Some name bands include the client’s picture, as well as name, date of birth, and bar code for verification of client identity.
Many agencies including the Veterans Administration (VA) Hospital System have used bar codes for years. When a new medication is ordered by a physician, it is transmitted to the pharmacy, where it is labeled with the same bar code as is on the client’s name band. The nurse administering that medication must first verify both codes by scanning with the battery-operated bar code reader, just as a

grocery store employee scans merchandise. In the VA, this resulted in a 24% decrease in medication administration errors (Wright & Katz, 2005). In a similar fashion, bar-coded labels on laboratory specimens prevent mixups.
Other technology used to improve safe care
Health information technologies are said to be a key tool for increasing safety, as well as decreasing health care costs, and increasing quality of care (Bates, 2009). These are discussed in Chapters 25 and 26 and include electronic health records, clinical decision supports, and computerized registries or national databanks that monitor treatment. Electronic transmission of prescriptions to pharmacies in the community could help decrease errors caused by misinterpretation of handwritten scripts, yet by 2008 only 6% of American physicians had adopted electronic prescribing. Radiofrequency identification is an emerging technology allowing you to locate a certain nurse, identify a patient, or even locate an individual medication. Radiofrequency identification may be able to be incorporated into the nurse’s handheld computer.
Improve care efficiency
Measures to improve efficiency may also increase the time you have for communication with clients. Some changes such as equipment at bedside may increase client safety by decreasing possible infections.
TCAB (Transforming Care At the Bedside)
Begun in 2003, Transforming Care At the Bedside [TCAB; pronounced tee-cab] is an Institute for Healthcare Improvement Initiative funded by the Robert Wood Johnson Foundation to improve client safety and the quality of hospital bedside care by empowering nurses at the bedside to make system changes (online, TCAB;www.rwj.org/pr/product.jsp?id=31512; Runy, 2008; Stefancyk, 2008a, 2008b, 2009).
This program has four core concepts to improve care:
1. Create a climate of safe, reliable patient care. Uses practices such as brainstorming and retreats for staff nurses, to develop better practice and better communication ideas. One example is nurses initiate presentation of the client’s status to physicians at morning rounds, using a standard format. Another strategy is to empower staff nurses to make decisions.
2. Establish unit-based vital teams. Interdisciplinary, supportive care teams foster a sense of increased professionalism for bedside nurses. This together with better nurse-physician communication should positively affect client outcomes.
3. Develop client-centered care. This ensures continuity of care and respects family and client choices.
4. Provide value-added care. This eliminates inefficiencies, for example, by placing high-use supplies in drawers in each client’s room
Evaluation in more 60 project hospitals showed that units using this method cut their mortality rate by 25% and reduced nosocomial infections significantly. Nurse-physician collaboration and communication was improved, with both physicians and nurses voicing increased satisfaction. Nurses said that overall they felt empowered (Stefancyk, 2008b).
Client outcomes of team training programs
Multiple studies tend to demonstrate increased satisfaction, primarily from nurses, when team communication strategies are implemented. To date, little evidence exists about effects on client outcomes, although some literature indicates anesthesia team training has reduced errors. More research into the effects of communication interventions is needed. But what is really needed is an overhaul in the conception of what an interdisciplinary “team” is.
Advantages
Ideally, the health care team would provide the client with more resources, allow for greater flexibility, promote a “learning from each other” climate, and promote collective creativity to problem solving. Use of standardized communication tools would foster collaborative practice by creating shared communication expectations.
Obstacles to effective teamwork include lack of time, culture of autonomy, heavy workloads, and different terminologies and communication styles held by each discipline. Building in redundancy cuts errors but takes extra time, which can be irritating.
Client-provider collaborations
Communicating with clients about the need for them to participate in their care planning is a goal set in 2009 by Joint Commission (online, www.jcipatientsafety.org/). Goal 13 states, “Encourage patients’ active involvement in their own care as a patient safety strategy,” which includes having clients and families report their safety concerns. Clients and their families should be specifically invited to be an integral part of the care process. Another strategy is to provide more opportunities for communication.
Emphasize to each client that he is a valued member of the health team who is expected to actively participate in his care. Safe care is a top goal shared by client and care provider. Empowering your client to be a collaborator in his or her own care should enhance error prevention. Emphasizing this provider-client partnership is the second step in a communication model described by Fleischmann and Rabatin (2008). In building the relationship, to establish rapport, participants follow the acronym PEARLS: P = partnership; E = empathy; A = apology, such as “sorry you had to wait”; R = respect; L = legitimize or validate your client’s feelings and concerns with comments such as “many people have similar concerns”; S = support. One outcome measured before and then 6 months after staff participated in a communications continuing education program was an increase in client satisfaction with care, up 16% in the emergency departments, up 17% in inpatient units, and up 28% in outpatient settings (Fleischmann, 2008). AHRQ advises clients to speak up if they have a question or concern, to ask about test results rather than to assume that “no news is good news.”
Daily client briefings
Physicians have long used hospital rounds to briefly speak with each of their patients. Some supervising nurses have begun this practice.
Use of written materials
In one hospital system, written pamphlets are given to each client on admission instructing them to become a partner in their care. A nurse comes into the client’s room at a certain time each day, sits, and makes eye contact. Together, nurse and client make a list of today’s goals, which are written on a whiteboard in the client’s room (Runy, 2008). As part of safety and communication, awareness of language barriers can be signaled to everyone entering the room by posting a logo on the chart, and room or bed. Use of interpreters and information materials written in the client’s primary language may also reduce risk (AHRQ, 2004).
Assessment of client’s level of health literacy
The IOM has stressed that it is important to make verbal and written information as simple as possible (Denham, 2008). As a nurse, you need to assess the health literacy level of each client. Provide privacy to avoid embarrassment. Obtain feedback to determine client’s understanding of teaching: Simplify, Clarify, Verify! In evaluating for literacy levels, some clues to low literacy or limited understanding are excuses such as “forgot my glasses,” humor, or use of a family member to read written materials.
Summary
There is a renewed effort to maximize client safety by minimizing errors made by all health care workers. Because miscommunication has been documented to be a most significant factor in occurrence of errors, this chapter focused on communication solutions. It described some individual and system solutions.
References
Agency for Healthcare Research and Quality [AHRQ, a]. National healthcare quality report. www.ahrq.gov/qual/nhqr05.htm. [Author].
Agency for Healthcare Research and Quality [AHRQ, b]. Medical errors: the scope of the problem: an epidemic of errors. www.ahrq.gov/qual/errback.htm. [Author].
Agency for Healthcare Research and Quality[AHRQ, c], Patient safety initiative: building foundations, reducing risk. Patient Safety Goals, 2009. Available online:, www.ahrq.gov/qual/pscongrpt/psinisum.htm. [Accessed February 28, 2009].
Agency for Healthcare Research and Quality[AHRQ, d]. Mistaken identity. http://cme.medscap.com/viewarticle/586256_2. [Author].
Agency for Healthcare Research and Quality [AHRQ, e] Literacy and health outcomes: summary, evidence report/technology assessment number 87, 2004. Available online:, http://www.ahrq.gov/clinic/epcsums/litsum.htm. [Accessed March 1, 2009].
Agency for Healthcare Research and Quality, [Publication No. 06-0020-3]. TeamSTEPPS [trademark], pocket guide, Rockville, MD, Author, 2008. Available online:, http://teamsteps.ahrq.gov/index.htm.
Amato-Vealey, E.J., Barba, M.P., Vealey, R.J., et al. Hand-off communication: a requisite for perioperative patient safety. AORN J. 2008;88(5):763–770.
American Association of Colleges of Nursing, Hallmarks of quality and patient safety: recommended baccalaureate competencies and curricular guidelines to ensure high-quality and safe patient care. J Prof Nurs, 2006;22(6):329–330. Available online:, www.aacn.org. or, http://qsen.org/competencydomains/safety. [Accessed June 1, 2009].
American Association of Colleges of Nursing Safety, 2006. Available online:, http://www.qsen.org. or, www.pedsnurses.org/dmdocuments/BaccaliareateEssentials.pdf. [Accessed June 6, 2009].
American Medical Association eVoice Best practice information, 2008. October 2, Available online, http://co106w.col106.mail.live.com/. [Accessed May 2, 2009].
American Medical Association. Safe communications universal precautions. Patient safety tip card, AMA Bookstore. Chicago: Author, 2008.
Bates, D.W. The effects of Health Information Technology on inpatient care [editorial]. Arch Intern Med. 2009;169(2):105–107.
Beyea, S.C. Learning more about the science of patient safety. AORN J. 2008;87(3):633–635.
Beyea, S.C. Placing patient safety first. AORN J. 2008;87(4):829–831.
Bonacum, D., CSP, CPHQ, CPHRM, Vice President, Safety Management, Kaiser Foundation Health Plan, Inc. [Kaiser Permanente]: Personal interview, 2009. [February 25,].
Boone, B.N., King, M.L., Gresham, L.S., et al. Conflict management training and nurse-physician collaborative behaviors. J Nurs Staff Dev. 2008;24(4):168–175.
Cronenwett, L., Sherwood, G., Barnsteiner, J., et al. Quality and safety education for nurses. Nurs Outlook. 2007;55(3):122–131.
Denham, C.R. SBAR for patients. J Patient Saf. 2008;4(1):38–48.
DeVoe, J.E., Wallace, L.S., Pandhi, N., et al. Comprehending care in a medical home: a usual source of care and patient perceptions about health communication. J Am Board Fam Med. 2008;21(5):441–445.
Donaldson, M.S. An overview of ‘To err in Human’ reemphasizing the message of patient safety. In: Hughes R.G., ed. Patient safety and quality: an evidence-based handbook for nurses. Rockville, MD: Agency for Healthcare Research and Quality, 2008. [[AHRQ pub no. 08-0043]].
Elder, N.C., Brungs, S.M., Nagy, M., et al. Nurses’ perceptions of error communication and reporting in the intensive care unit. J Patient Saf. 2008;4:162–168.
Evans, A.M., Pereira, D.A., Parker, J.M., et al. Discourses of anxiety in nursing practice: a psychoanalytic case study of the change-of-shift handover ritual. Nurs Inq. 2008;15(1):40–48.
Fleischman, A., J., Rabatin. Provider-Patient Communication. In: conference materials supplied by Mayo Health Care System Medical Continuing Education Department. Rochester: MN; 2008. [obtained May 27].
Fleischmann, J.A., MD, Medical Vice President of Franciscan Skemp, Mayo HealthCare System, LaCrosse, WS: Personal interview, 2008. [May 29,].
Gore, T., Hunt, C.W., Raines, K.H., et al, Mock hospital unit simulation: a teaching strategy to promote safe patient care. Clin Simulation Nurs, 2008;4(3):e57–e64. Available online:, www.elsevier.com/locate/ecsn. [Accessed February 13, 2009].
Henkind, S.J., Sinnett, J.C. Patient care, square-rigger sailing, and safety. JAMA. 2008;300(14):1691–1693.
Henneman, E.A., Roche, J.P., Fisher, D.L., et al. Error identification and recovery by student nurses using human patient simulation: opportunity to improve patient safety. Appl Nurs Res. 2009;23(1):11–21.
Hughes, R.G., eds. Patient safety and quality: an evidence-based handbook for nurses, vols 1–3. Rockville, MD: Agency for Healthcare Research and Quality, 2008. [April [AHRQ Publication No. 08-0043]].
Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Washington, DC: National Academy Press, 2001.
Institute of Medicine. Insuring America’s health: principles and recommendations. Washington, DC: National Academy Press, 2004.
Joint Commission on Accreditation of Healthcare Organizations[JCAHO,a], Behaviors that undermine culture of safety. Sentinel Event Alert 2008;40. Available online:, http://www.jointcommission.org/SentinelEvents/SentinelEventAlert/sea_40.htm. [Accessed July 9, 2008].
Joint Commission on Accreditation of Healthcare Organizations [JCAHO,b] Root causes of sentinel events. Author, 2006, www.jointcommission.org/SentinelEvants/Statistics/.
Joint Commission on Accreditation of Healthcare Organizations [JCAHO,c]. Sentinel event statistics. www.jointcommissioninternational.org/24839/.
Joint Commission International. WHO Solutions. www.jointcommissioninternational.org/24839/.
Kaiser Family Foundation/AHRQ/Harvard School Family Foundation/AHRQ/Harvard School, conducted. National survey on consumers’ experiences with patient safety and quality information, 2004. Available online:, http://www.kff.org/kaiserpolls/pomr111704pkg.cfm. [Accessed February 20, 2009].
Kohn L.T., Corrigan J.M., Donaldson M.S., eds. To err is human: building a safer health system. Institute of Medicine, Committee on Quality in America, National Academy Press: Washington, DC, 1999. Available online:, http://www.guideline.gov/.
Kramer, M., Schmalenberg, C. Securing ‘good’ nurse-physician relationships. Nurs Manag. 2003;34:34–38.
Krautscheid, L.C., Improving communication among healthcare providers: preparing student nurses for practice. Int J Nurs Educ Sch, 2008;5(1). article 40. Available online:, http://www.bepress.com/ijnes/vol5/iss1/art40/. [Accessed October 21, 2008].
Lachman, V.D. Patient safety: the ethical imperitive. Dermotology Nursing. 2008;20(2):134–136.
Leonard, M. SBAR, 2009. [personal communication [e-mail] February 20].
Leonard, M., Bonacum, D., SBAR application and critical success factors of implementation. Kaiser Permanente Health Care System presentation, May 2008, by Dr. Rabatin Jeff, Consultant, Pulmonary and Critical Care Medicine, Mayo Healthcare System, Rochester, MN, 2008.
Leonard, M., Graham, S., Bonacum, D., et al. The human factor: the critical importance of effective teamwork and communication in providing safe care. Qual Saf Health Care. 2004;13(Suppl 1):i85–i90.
Mangione-Smith, R., DeCristofara, A.H., Setodji, C.M., et al. The quality of ambulatory care delivered to children in the United States. N Engl J Med. 2007;357(15):1515–1523.
Mathews, S.C., Pronovost, P.J. Physician autonomy and informed decision making. JAMA. 2008;300(24):2913–2915.
Nolte, E., McKee, C.M. Measuring the health of nations: updating an earlier analysis. Health Aff. 2008;27(1):58–71.
Runy, L.A., The nurse and patient safety. H&HN, 2008;82(11):43–48. Available online:, www.cinahl.com/cgi-bin/refsvc?jid=1774%accno=2010112696. [Accessed January 6, 2009].
Scott, L.D., Rodgers, A.E., Hwang, W.T., et al. Effects of critical care nurses’ work hours on vigilance and patients’ safety. Am J Crit Care. 2006;15:30–37.
Shortell, S.M., Singer, S.J. Improving patient safety by taking systems seriously. JAMA. 2008;299(4):445–447.
Singh, H., Thomas, E., Peterson, L., et al. Medical errors involving trainees. Arch Intern Med. 2007;167(19):2030–2036.
Stefancyk, A.L. Transforming care at the bedside: transforming care at Mass General. Am J Nurs. 2008;108(9):71–72.
Stefancyk, A.L. Transforming care at the bedside: nurses participate in presenting patients in morning rounds. Am J Nurs. 2008;108(11):70–72.
Stefancyk, A.L. Transforming care at the bedside: high-use supplies at the bedside. Am J Nurs. 2009;109(2):33–35.
Sutter, E., Arndt, J., Arthur, N., et al. Role understanding and effective communication as core competencies for collaborative practice. J Interprof Care. 2009;23(1):41–51.
Velji, K., Baker, G.R., Fancott, C., et al. Effectiveness of an adapted SBAR communication tool for a rehabilitation setting. Healthc Q. 2008;11(3 Spec No.):72–79.
Wong, D.R., Torchiana, D.F., Vander Salm, T.J., et al. Impact of cardiac intraoperative precursor events on adverse outcomes. Surgery. 2007;141(6):715–722.
Woods, D.M., Holl, J.L., Angst, D., et al, Improving clinical communication and patient safety: clinician-recommended solutions. J Healthc Qual, 2008;30(5):4354. Available online:, www.ahrq.gov/downloads/pub/advances2/vol3/Advances_woods_78.pdf. [Accessed November 27, 2008].
Wright, A.A., Katz, I.T. Bar coding and patient safety. N Engl J Med. 2005;353(4):329–331.
Zbar, R.I., Taylor, L.D., Canady, J.W., et al. The disruptive physician: righteous Maverick or dangerous Pariah? Plast Reconstr Surg. 2009;123(1):409–415.