The Head
THE SKULL
The skull is a complex of bones formed in both membrane and cartilage. Those that surround the brain make up the cranium. These include the dermal bone roof, the calvaria, fused with the cartilage-bone walls and floor. The skull bones that surround the entrances into the digestive and respiratory systems make up the bones of the face. Articulated with the cranial bones are the mandibles of the jaw, the ear ossicles, and the hyoid apparatus.
Various skull elements fuse with one another during development or have been lost phylogenetically, with the result that each species has distinctive features that may not be present in others. The dog’s skull varies more in shape among the different breeds than does the skull of other species of domestic animals.
Dorsal and Lateral Surfaces of the Skull (Figs. 5-1 through 5-4)
The paired frontal and parietal bones form the dorsum of the cranium or calvaria. The parietal bone joins the frontal bone rostrally and its fellow medially. Caudally, the parietal bone meets the occipital bone, which forms the caudal surface of the skull. The unpaired interparietal bone fuses with the occipital bone prenatally and appears as a process extending rostrally. The ventral border of the parietal bone joins the squamous temporal and basisphenoid bones. Rostral to the parietal bone is the frontal bone, which forms the dorsomedial part of the orbit.
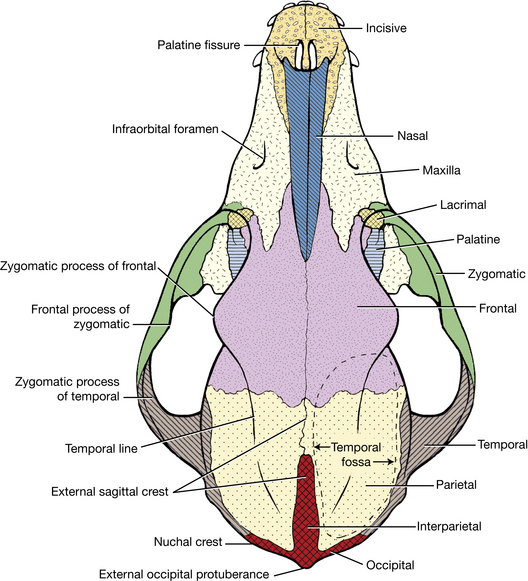
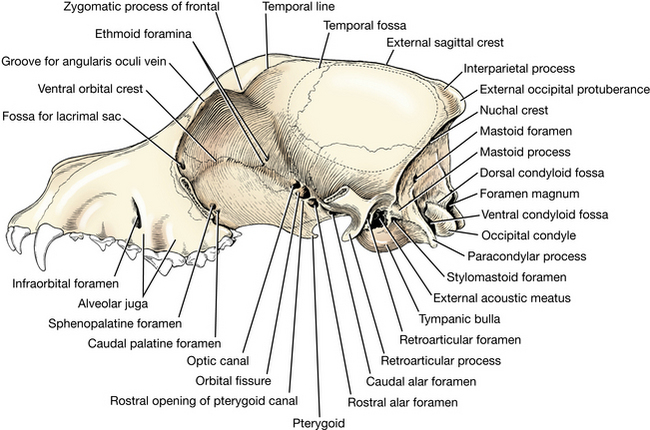
The external sagittal crest is a median ridge formed by the parietal and interparietal bones. It varies in height and may be absent. In most brachycephalic breeds, the sagittal crest is replaced by a pair of sagittal temporal lines. Each extends from the external occipital protuberance to the zygomatic process of the frontal bone. The nuchal crest is a transverse ridge that marks the transition between the dorsal and caudal surfaces of the skull. The external occipital protuberance is median in position at the caudal end of the sagittal crest.
On each side of the dorsum of the skull is the temporal fossa. The fossa is convex. It is bounded medially by the sagittal crest or the temporal line, caudally by the nuchal crest, and ventrally by the zygomatic process of the temporal bone. The temporal fossa is continuous rostrally with the orbit. The temporal muscle arises from this temporal fossa on the frontal, parietal, and squamous temporal bones.
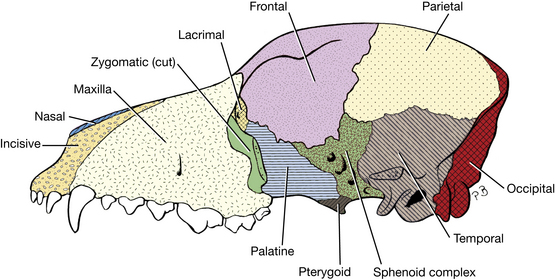
Lateral portions of the frontal and parietal bones form the lateral surface (Fig. 5-3) of the cranium. The caudoventral part of the lateral surface of the skull is composed largely of the temporal bone. This compound bone comprises squamous, tympanic, and petrous parts.
The squamous part forms the ventral portion of the temporal fossa and bears a zygomatic process, which forms the caudal part of the zygomatic arch. It articulates dorsally with the parietal bone, rostrally with the basisphenoid wing, and caudally with the occipital bone.
Rostral to the squamous temporal bone, the ventrolateral surface of the cranium is formed by the wings of the basisphenoid and presphenoid. The wing of the basisphenoid articulates caudally with the squamous part of the temporal bone, dorsally with the parietal and frontal bones, and rostrally with the wing of the presphenoid.
Facial Bones
The facial part of the dorsal surface of the skull is formed by parts of the frontal, nasal, maxillary, and incisive bones. All are paired. The nasal bone meets its fellow on the midline, the frontal bone caudally, and the maxilla and incisive bone laterally. The maxilla contains the upper cheek teeth and upper canine. The incisive bone bears the three upper incisor teeth and has a long nasal process that articulates with the maxilla and nasal bone. The nasal aperture is bounded by the incisive and nasal bones. It is nearly circular in brachycephalic breeds and is oval in the dolichocephalic breeds.
The orbit is the cavity in which the eye is situated. A portion of it is bony. The orbital margin is formed by the frontal, lacrimal, and zygomatic bones. The lateral margin of the orbit is formed by the orbital ligament, which extends from the frontal process of the zygomatic bone to the zygomatic process of the frontal bone. The medial wall of the orbit is formed by the orbital surfaces of the frontal, lacrimal, presphenoid, and palatine bones.
The zygomatic arch is formed by the zygomatic process of the maxilla, the zygomatic bone, and the zygomatic process of the temporal bone. The arch serves as an origin for the masseter muscle, which closes the jaws.
The pterygopalatine fossa is located ventral to the orbit. The maxilla, palatine bone, and zygomatic bone bound the rostral part. The caudal part is bounded by the palatine and pterygoid bones and the wings of the sphenoid bones. The pterygoid muscles arise from this fossa.
The three openings in the caudal part of the orbit are, from rostral to caudal, the optic canal, the orbital fissure, and the rostral alar foramen. The optic canal passes through the presphenoid, and the alar canal passes through the basisphenoid. The orbital fissure is formed in the articulation between the basisphenoid and presphenoid bones. The optic nerve passes through the optic canal. Passing through the orbital fissure are the oculomotor, trochlear, abducent, and ophthalmic nerves and some vessels. Emerging from the rostral alar foramen are the maxillary artery and the maxillary nerve.
In the rostral part of the pterygopalatine fossa are several foramina. The caudal palatine foramen and sphenopalatine foramen are closely related openings of about equal size located on the rostromedial wall of the fossa. The sphenopalatine foramen is dorsal to the caudal palatine. The major palatine artery, vein, and nerve enter the palatine canal through the caudal palatine foramen and together course to the hard palate. The sphenopalatine artery and vein and the caudal nasal nerve enter the nasal cavity via the sphenopalatine foramen. Rostrolateral to these is the maxillary foramen, the caudal opening of the infraorbital canal. The infraorbital artery, vein, and nerve course rostrally through this canal. A small part of the rostromedial wall of the pterygopalatine fossa, just caudal to the maxillary foramen, often presents an open defect that is normally occupied by a thin plate of bone, which serves as the origin of the ventral oblique eye muscle. Caudal to the maxillary foramen are a number of small openings, most of them for the small nerves and vessels that pass through their respective alveolar canals to the roots of the two molar teeth and the caudal root of the last premolar. Above the maxillary foramen in the lacrimal bone is the shallow fossa for the lacrimal sac. The fossa is continued rostrally by the nasolacrimal canal for the nasolacrimal duct.
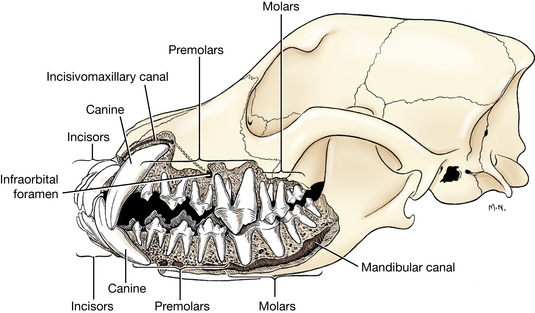
The facial part of the lateral surface of the skull rostral to the orbit includes the lateral surface of the maxilla and the incisive bone. Dorsal to the third premolar tooth is the infraorbital foramen, the rostral opening of the infraorbital canal. The roots of the cheek teeth produce lateral elevations, the alveolar juga.
Ventral Surface of the Skull (Figs. 5-5 to 5-7)
The ventral aspect of the cranium consists of the basioccipital bone, tympanic and petrosal parts of the temporal bone, the basisphenoid bone, and the presphenoid bone. The basioccipital bone forms the caudal third of the cranial base. It articulates laterally with the tympanic and petrous parts of the temporal bone and rostrally with the body of the basisphenoid. Caudally, the occipital condyle articulates with the atlas. The paracondylar process, a ventral projection of the occipital bone, articulates with the caudolateral part of the tympanic bulla. The digastricus muscle arises from the paracondylar process.
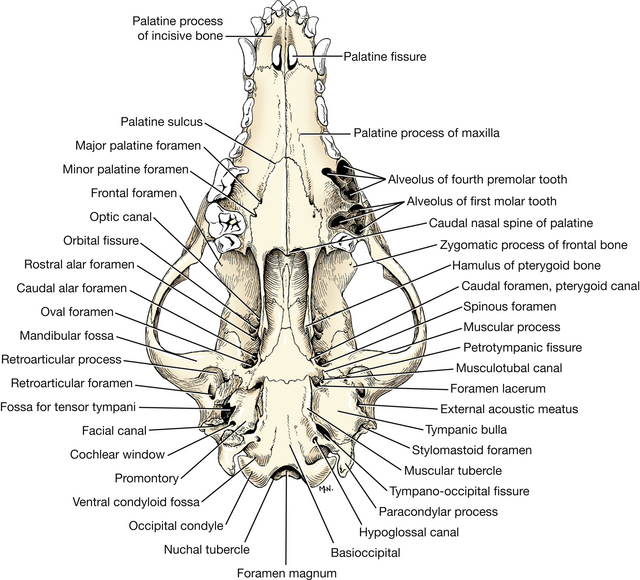
The tympanic part of the temporal bone has a bulbous enlargement, the tympanic bulla, which encloses the middle ear cavity and its ossicles (Fig. 5-8). On the lateral side of the bulla is the external acoustic meatus. In life, the tympanic membrane closes this opening and the annular cartilage of the external ear attaches around its periphery.
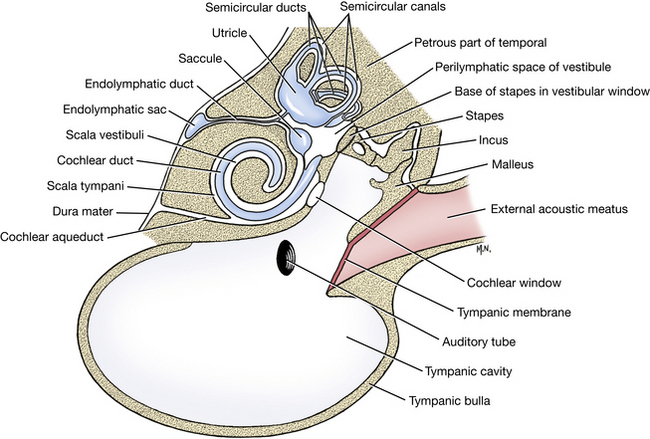
The petrosal part of the temporal bone contains the membranous and bony labyrinths of the inner ear (Fig. 5-8). The major portion of this bone is visible inside the cranial cavity. The tympanic bulla has been removed on one side. This exposes a barrel-shaped eminence, the promontory, on the ventral surface of the petrosal part of the temporal bone. The promontory contains the cochlear window, which is closed in life by a membrane. The vestibular window lies dorsal to the promontory and contains the footplate of the stapes (Fig. 5-8). The stapes articulates with the incus, which in turn articulates with the malleus. The malleus is attached to the medial side of the tympanic membrane. The mastoid process is the only part of the petrosal portion of the temporal bone to reach the exterior. It is small and lies caudal to the external acoustic meatus lateral and dorsal to the root of the prominent paracondylar process. The mastoid parts of the cleidocephalicus, sternocephalicus, and splenious muscles terminate on the mastoid process.
The basisphenoid articulates caudally with the basioccipital and rostrally with the presphenoid and pterygoid bones. The oval foramen, round foramen, and alar canal pass through the basisphenoid bone. The presphenoid articulates caudally with the basisphenoid and pterygoid, laterally with the perpendicular part of the palatine, and rostrally with the vomer. Only a small median portion of the presphenoid is exposed on the ventral surface of the cranium. The optic canals pass through the orbital wing of the presphenoid.
The rostral alar foramen, caudoventral to the orbital fissure, is the rostral opening of the alar canal. The caudal opening of this short canal is the caudal alar foramen. The round foramen opens from the cranial cavity into the alar canal. The maxillary nerve from the trigeminal nerve enters the alar canal from the cranial cavity through this round foramen. The nerve courses rostrally and leaves the alar canal by the rostral alar foramen. In addition, the maxillary artery traverses the full length of the alar canal.
The oval foramen, a direct opening into the cranial cavity, is caudolateral to the caudal alar foramen. The mandibular nerve from the trigeminal nerve leaves the cranial cavity through this opening.
The foramen lacerum lies at the rostromedial edge of the tympanic bulla. A loop of the internal carotid artery protrudes through this opening. This loop is between the part of the internal carotid that is coursing rostrally in the carotid canal and the part that returns through the foramen lacerum and enters the cavernous sinus on the floor of the cranial cavity.
The musculotubal canal lies lateral to the foramen lacerum and caudal to the oval foramen. It is the bony enclosure of a cartilaginous tubular connection, the auditory tube, which runs from the middle ear to the nasopharynx.
The tympano-occipital fissure is an oblong opening between the basilar part of the occipital bone and the tympanic part of the temporal bone. The petro-occipital canal and the carotid canal leave the depths of the fissure at about the same place. The carotid canal transmits the internal carotid artery. The petro-occipital canal transmits the ventral petrosal venous sinus. Neither canal can be adequately demonstrated on an articulated skull. The glossopharyngeal, vagus, and accessory nerves course peripherally from the jugular foramen through the tympano-occipital fissure. Also passing through this fissure are the internal carotid artery, venous radicles of the vertebral and internal jugular veins, and sympathetic postganglionic axons from the cranial cervical ganglion.
The hypoglossal canal, for the passage of the hypoglossal nerve, lies caudomedial to the tympano-occipital fissure in the occipital bone.
The mandibular fossa of the zygomatic process of the temporal bone articulates with the condyle of the mandible to form the temporomandibular joint. The retroarticular process forms the caudal wall of the medial aspect of the mandibular fossa. The retroarticular foramen caudal to this process conducts the emissary vein from the temporal venous sinus.
Between the tympanic bulla and the mastoid process of the temporal bone is the stylomastoid foramen. This is the opening of the facial canal that conducts the facial nerve peripherally through the petrosal part of the temporal bone.
Facial Bones
The ventral surface of the facial part of the skull is characterized by the teeth and hard palate. There is a superior (maxillary) and an inferior (mandibular) dental arch. Each tooth lies in an alveolus or socket. Interalveolar septae separate the alveoli of adjacent teeth. An alveolus is subdivided by interradicular septae for those teeth with more than one root. In the superior dental arch single alveoli are present in the incisive bones for the incisor teeth and in the maxilla for the canine and first premolar teeth. There are two alveoli in the maxilla for the second premolar and two for the third. The fourth premolar and the two molars each have three alveoli in the maxilla. The hard palate is composed of the horizontal parts of the palatine, maxillary, and the incisive bones. An opening, the palatine fissure, is located on each side of the midline between the canine teeth.
The palatine bones form the caudal third of the hard palate. The major palatine foramen is medial to the fourth cheek tooth. Caudal to this is the minor palatine foramen. The major palatine artery, vein, and nerve and their branches emerge through these foramina. The choanae are the openings of the right and left nasal cavities into the nasopharynx. They are located at the caudal end of the hard palate, where the vomer articulates with the palatine bones.
Caudal Surface of the Skull (Figs. 5-3, 5-9)
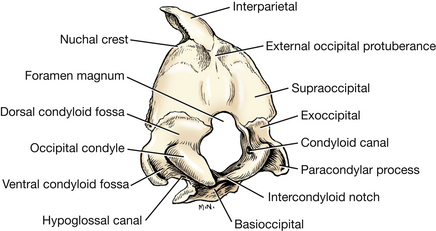
During development the occipital bone is formed by paired exoccipitals (which bear the condyles), a supraoccipital, and a basioccipital. The lateral borders form a nuchal crest where the occipital meets the parietal and squamous temporal bones. Mid-dorsally, an external occipital protuberance is formed where the interparietal bone is fused to the occipital at the caudal end of the sagittal crest. The foramen magnum is the large opening from the cranial cavity through which the medulla of the brain stem is continued as the spinal cord. The mastoid foramen is located in the occipitotemporal suture, dorsolateral to the occipital condyle. It transmits the caudal meningeal artery and vein. The rest of the caudal surface of the skull is roughened for muscular attachment.
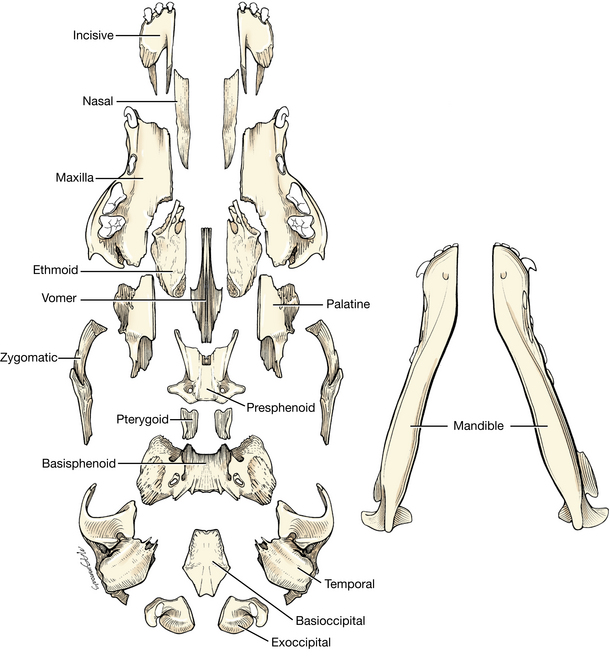
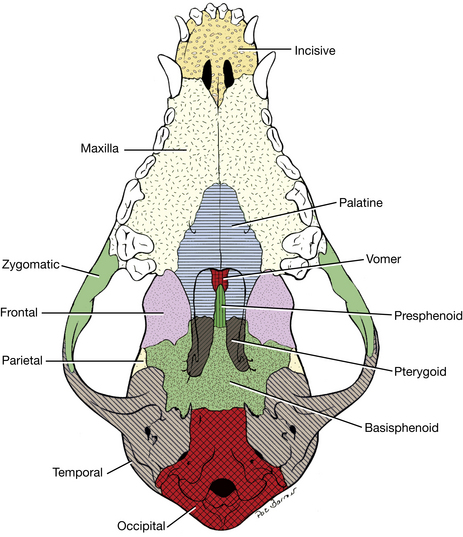
If a disarticulated skull is available for study, try to locate each of the bones in the whole skull (Figs. 5-6, 5-10). Being able to visualize one bone in relation to another aids in radiographic interpretation of normal features. Several of the skull bones overlap each other to a considerable degree, so that it is not always possible to see the boundaries of an individual bone in situ. The presphenoid bone, through whose orbital wings the optic nerves pass, is a good example. Identify the optic canal of an intact skull and note the outline of the presphenoid sutures with adjacent bones. Orient an individual presphenoid bone in a similar position. Do the same for the more caudally located basisphenoid bone with its temporal wings and for the basioccipital bone, which is part of the occipital ring. These three bones form the basicranial axis of the skull upon which the brain rests (Fig. 5-7). Study the components of the disarticulated ethmoid bone, which would be located at the rostral end of the basicranial axis. The bone is described with the nasal cavity on p. 223.
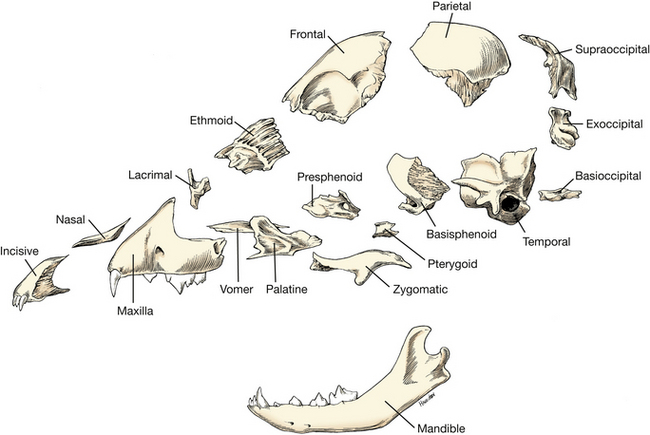
With the aid of diagrams of the disarticulated skull (Figs. 5-6, 5-10), try to locate the other bones on the intact skull.
Mandible
The two mandibles (Figs. 5-11, 5-12) compose the lower jaw. Each mandible bears the inferior teeth and articulates with the mandibular fossa of the zygomatic process of the temporal bone. The two mandibles join rostrally at the intermandibular articulation. Each mandible can be divided into a body, or horizontal part, and a ramus, or perpendicular part. The alveolar border of the mandible contains alveoli for the roots of the teeth. The incisors, canine, first premolar, and third molar have one root each. The last three premolars and first two molars have two roots each.
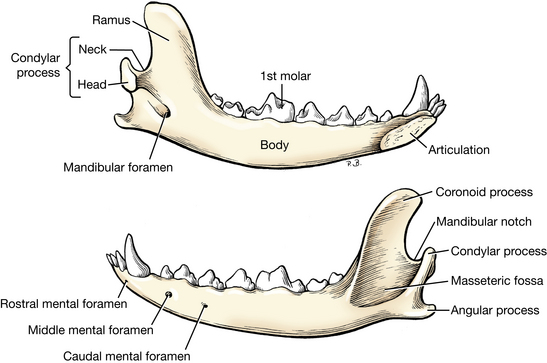
On the lateral surface of the ramus of the mandible is the triangular masseteric fossa for the insertion of the masseter muscle. The dorsal half of the ramus is the coronoid process. Its medial surface has a shallow depression for insertion of the temporal muscle. Ventral to this is the mandibular foramen. This foramen is the caudal opening of the mandibular canal, which is located in the ramus and body of the mandible. It transmits the inferior alveolar artery and vein and the inferior alveolar nerve. It opens rostrally at the three mental foramina, where mental nerves supply sensory innervation to the adjacent lower lip and chin. The pterygoid muscles insert on the medial surface of the mandible and on the angular process, ventral to the insertion of the temporal muscle.
The condylar process helps form the temporomandibular joint. Between the condylar process and the coronoid process is a U-shaped depression, known as the mandibular notch. Motor branches of the mandibular nerve pass across this notch to innervate the masseter muscle.
The angular process is a hooked eminence ventral to the condylar process. It serves for the attachment of the pterygoids medially and the masseter laterally.
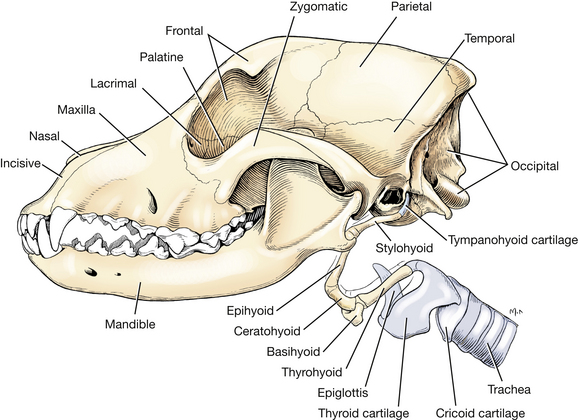
Hyoid Bones
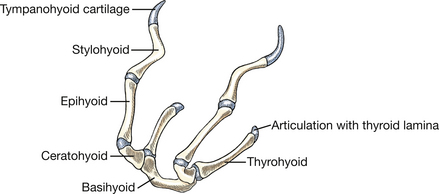
The hyoid apparatus (Figs. 5-3, 5-13, 5-26) is composed of the hyoid bones, which stabilize the tongue and the larynx by suspending them from the skull. This apparatus extends from the mastoid process of the skull to the thyroid cartilage of the larynx. It consists of the short tympanohyoid cartilage and the following articulated bones: the stylohyoid, epihyoid, ceratohyoid, basihyoid, and thyrohyoid. All of the bones are paired except for the basihyoid, which unites the elements of the two sides in the root of the tongue. Examine these on the wet specimens provided, as well as on your own specimen.
Teeth
The teeth are arranged in superior (upper) and inferior (lower) arches that face each other. The inferior arch is narrower than the superior (Figs. 5-3, 5-5, 5-11).
The upper teeth are contained in the incisive and maxillary bones. Those whose roots are embedded in the incisive bone are known as the incisor teeth. Caudal to these and separated from them by a space is the canine tooth. Behind this are the cheek teeth, which are divided into premolars and molars. The inferior incisors, canine tooth, and inferior cheek teeth are all in the mandible. They are generally similar to the upper teeth. There is one more molar tooth in each mandible than in the corresponding maxilla. Some of the teeth—the incisors, the fourth premolar, and the molars—usually meet those of the opposite arch when the jaws are closed. The upper fourth premolar and first molar shear along the first lower molar. The first three premolars fail to meet during normal closure, and the opening between the teeth is called the premolar carrying space. In dogs with long muzzles, there may be a considerable interval between teeth, supernumerary teeth may be present, and some premolars do not occlude. In short-muzzle breeds the teeth are usually crowded, have shallow roots, and are all in wear. In addition, most of the teeth are set obliquely and some may be missing.
The dental formula for the permanent teeth of the dog is as follows:

The temporary or deciduous dentition (“milk teeth”) can be expressed by the following formula:

The deciduous teeth are erupted between 4 and 8 weeks.
The first incisor tooth (central) is next to the median plane and is followed by the second incisor (intermediate) and the third incisor (corner). In the permanent dentition the premolar and molar teeth are numbered from rostral to caudal; thus the tooth nearest the canine is number one. The fourth premolar is the largest cheek tooth of the maxilla; the largest cheek tooth of the mandible is the first molar. These are known as the sectorial or shearing teeth.
The first premolar and all of the molar teeth in the dog have no deciduous predecessor. The teeth of the permanent set are much larger than those of the deciduous set. The last permanent tooth erupts at 6 or 7 months.
Each tooth possesses a crown and a root (or roots), which is embedded in an alveolus of the jaw. The junction of root and crown is the neck of the tooth.
The roots of the teeth are fairly constant. The incisors and canines of both jaws have one each. In the upper jaw the first premolar has one root; the second and third have two each; the fourth premolar and the first and second molars have three each. The lower cheek teeth have two roots each, except the first premolar and third molar, which have one. The superior shearing tooth, which is the fourth premolar, has two rostral roots in a transverse plane and a large caudal root. Notice that the lateral roots of the fourth premolar lie ventrolateral to the infraorbital canal and that the medial root of the rostral pair lies ventromedial to the infraorbital foramen.
The outer surface of the teeth is the vestibular surface, and the inner surface is the lingual surface for mandibular teeth or the palatine surface for maxillary teeth. The sides of a tooth that lie in contact with or face an adjacent tooth are the contact surfaces. On the first incisor, the mesial contact surface is next to the median plane, whereas on all other teeth the mesial contact surface is directed toward the first incisor; the distal surface is the opposite surface. The surface of the tooth that faces the opposite dental arch is known as the occlusal or masticating surface.
Cavities of the Skull
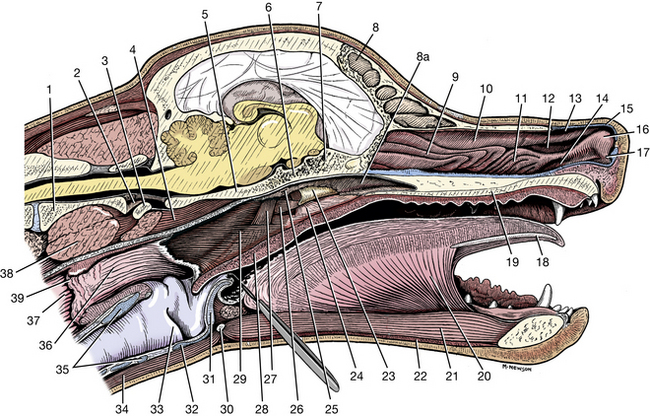
The cranial cavity (Figs. 5-14, 5-15) contains the brain and its coverings and vessels. The roof of the cranium, the calvaria, is formed by the parietal and frontal bones. The rostral two thirds of the base of the cranium is formed by the sphenoid bones. The caudal third is formed by the occipital and temporal bones. The caudal wall is the occipital bone, and the rostral wall is the cribriform plate of the ethmoid bone. The lateral walls are formed by the temporal, parietal, frontal, and sphenoid bones. The interior of the cranial cavity contains impressions formed by the gyri and sulci of the brain. Arteries leave grooves on the cerebral surface of the bones, whereas many of the veins lie in the diploë between the outer and inner tables of the bones. The base of the cranial cavity is divided into rostral, middle, and caudal cranial fossae.
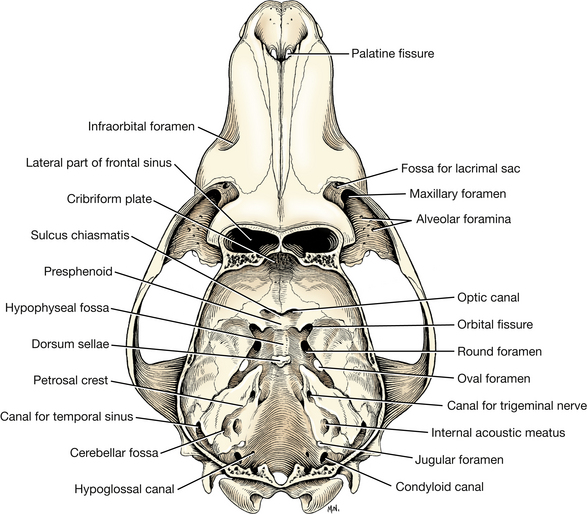
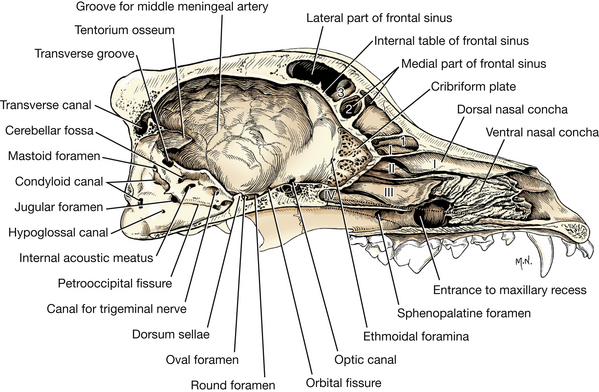
Fig. 5-15 Sagittal section of skull, medial view. Roman numerals I, II, III, IV indicate endoturbinates in the nasal cavity; arabic numerals 1, 2, 3 are ectoturbinates located in the frontal sinus.
The rostral cranial fossa is located rostral to the optic canals. The floor of this fossa is formed by the presphenoid bone and the cribriform plate of the ethmoid. It is bounded laterally by the frontal bone. The olfactory bulbs and the rostral parts of the frontal lobes of the brain lie in this fossa. The numerous foramina in the cribriform plate transmit blood vessels and olfactory nerves from the olfactory epithelium of the caudal nasal cavity to the olfactory bulbs of the brain. The much perforated cribriform plate of the ethmoid bone separates the cranium from the nasal cavity. (It can be the route of invasive organisms via the nasal cavity.) It is concave on its caudal surface and can be seen in a skull through the foramen magnum. On its rostral side it has many ethmoturbinate scrolls that project into and fill the caudal part of the nasal cavity and floor of the frontal sinus. In life, these thin ossified scrolls are covered by olfactory mucosa. The optic canal is a short passage in each orbital wing of the presphenoid bone through which the optic nerve courses.
The middle cranial fossa extends caudally from the optic canals to the petrosal crests and the dorsum sellae. It is situated on a more ventral level than the rostral cranial fossa. Several paired foramina are found on the floor of this fossa. Caudal to the optic canal is the orbital fissure. The oculomotor, trochlear, and abducent nerves and the ophthalmic nerve from the trigeminal nerve leave the cranial cavity through this opening. Caudal and lateral to the orbital fissure is the round foramen that transmits the maxillary nerve from the trigeminal nerve to the alar canal. Caudolateral to the round foramen is the oval foramen that transmits the mandibular nerve from the trigeminal nerve and the middle meningeal artery, which enters the cranial cavity from the maxillary artery.
The sella turcica, on the dorsal surface of the basisphenoid, contains the hypophysis. It is composed of a shallow hypophyseal fossa, which is limited rostrally by the presphenoid bone and bounded caudally by a raised quadrilateral process, the dorsum sellae. The caudal part of the middle cranial fossa is the widest part of the cranial cavity. The parietal and temporal lobes of the cerebrum are located here.
The caudal cranial fossa extends from the petrosal crests and dorsum sellae to the foramen magnum. The floor of this fossa is formed by the basioccipital bone and petrosal parts of the temporal bones. It contains the cerebellum, the pons, and the medulla.
Study the foramina and canals on the floor and sides of the braincase (Figs. 5-14, 5-15). The opening of the carotid canal is located under the rostral tip of the petrosal part of the temporal bone.
The canal for the trigeminal nerve is in the rostral end of the petrosal part of the temporal bone. The trigeminal ganglion is located in the canal. Caudal to this is the internal acoustic meatus, through which the facial and vestibulocochlear nerves pass. Dorsocaudal to the internal acoustic meatus is the cerebellar fossa, which contains a small lateral portion of the cerebellum.
The jugular foramen is located between the petrosal part of the temporal and the occipital bones. It opens to the outside through the tympano-occipital fissure and transmits the glossopharyngeal, vagus, and accessory cranial nerves as well as the sigmoid venous sinus. Caudomedial to the jugular foramen is the hypoglossal canal for the hypoglossal nerve. Dorsal to this foramen is the condyloid canal, which transmits a venous sinus.
Projecting rostroventrally from the caudal wall of the cranial cavity is the tentorium osseum. This is composed of processes from the parietal and occipital bones. The dural membrane, the tentorium cerebelli, attaches to the petrosal crests and the tentorium osseum, separating the cerebrum from the cerebellum. A relatively median foramen for the dorsal sagittal sinus is located on the rostral surface of the occipital bone dorsal to the tentorium osseum. It opens into the paired transverse canals. This foramen transmits the dorsal sagittal venous sinus to the transverse sinus in the transverse canal. The transverse sinus continues ventrolaterally through the transverse groove of the occipital bone. Then, as the temporal sinus, it passes through the temporal bone lateral to the petrous portion. At the retroarticular foramen, the temporal sinus communicates with the maxillary vein via the emissary vein.
Nasal Cavity
The nasal cavity is the facial part of the respiratory passages. Its bony part begins at the nasal aperture and is composed of two symmetrical halves separated by a median nasal septum. The caudal openings of the two halves of the nasal cavity are the choanae. The choanae are at the caudal end of the nasal septum, where the nasal cavity opens into the single nasopharynx. On a skull split on the median plane, study the bony scrolls or conchae, which lie in the nasal fossa. Compare them with the mucosa-covered conchae of a hemisected embalmed head.
The conchae (Figs. 5-15, 5-16, 5-17, 5-19, 5-24) project into each half of the nasal cavity and, with their mucosa, act as baffles to warm and cleanse inspired air. Their caudal portions also contain olfactory neurons, whose axons course to the olfactory bulbs of the brain through the cribriform plate.
The dorsal nasal concha originates as the most dorsal scroll on the cribriform plate and extends rostrally as a shelf attached along the medial surface of the nasal bone.
The ventral nasal concha consists of several elongated scrolls that attach to a crest on the medial surface of the maxilla. It lies in the middle of the nasal cavity but does not come into contact with the median nasal septum.
The ethmoidal labyrinth is composed of many delicate scrolls that attach to the cribriform plate caudally and occupy the fundus of the nasal cavity. Dorsally, the scrolls extend as ectoturbinates into the rostral portion of the frontal sinus. Ventrally, as endoturbinates, the scrolls attach to the vomer, which separates the entire ethmoidal labyrinth from the nasopharynx. The endoturbinates usually extend into the presphenoid bone.
The ethmoid bone complex is located between the cranium and the facial part of the skull. It consists of the ethmoidal labyrinth, the cribriform plate caudally, a median bony perpendicular plate of the nasal septum, and the orbital laminae laterally. The ethmoid bone complex is surrounded by the frontal bone dorsally, the maxilla laterally, and the vomer and the palatine ventrally. The ethmoidal labyrinth, consisting of ectoturbinates and endoturbinates attached to the cribriform plate, has an orbital lamina on each side that forms the medial wall of the maxillary recess (Fig. 5-19).
The nasal septum separates the right and left nasal cavities. It is composed of cartilage and bone. The cartilaginous part, the septal cartilage, forms the rostral two thirds of this median partition. It articulates with other cartilages at the nares, which prevent collapse of the nostrils. Ventrally, the septal cartilage fits into a groove formed by the vomer; dorsally, it articulates with the nasal bones where they meet at the midline. The osseous part of the nasal septum is formed by the perpendicular plate of the ethmoid bone, the septal processes of the frontal and nasal bones, and the sagittal portion of the vomer.
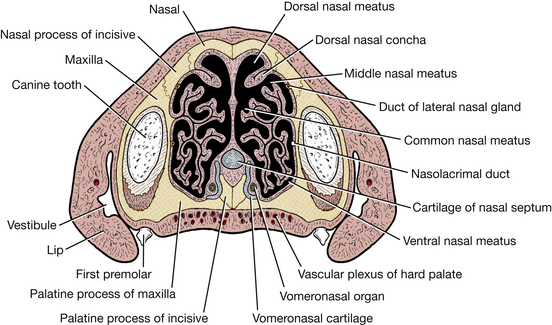
In each half of the nasal cavity, the shelflike dorsal nasal concha and the scrolls of the ventral nasal concha divide the cavity into four primary passages known as meatuses (Fig. 5-16, 5-17). The dorsal nasal meatus lies between the nasal bone and the dorsal nasal concha. The small middle nasal meatus lies between the dorsal nasal concha and the ventral nasal concha, whereas the ventral nasal meatus is dorsal to the hard palate. Because the conchae do not reach the nasal septum, a vertical space, the common nasal meatus, is formed on each side of the nasal septum. This space extends from the nasal aperture to the choanae in a longitudinal direction and from the nasal bone to the hard palate in a vertical direction.
Paranasal Sinuses
There are three frontal sinuses (Figs. 5-14, 5-15) located between the outer and inner tables of the frontal bone. They are designated lateral, rostral, and medial. The lateral frontal sinus is much larger than the others and is the only one of clinical relevance. Its size and shape vary with the type of skull. It occupies the zygomatic process and extends caudally, bounded laterally by the temporal line and medially by the median septum. It may be partially divided by bony septa extending into it. Ethmoidal ectoturbinates project into the rostral floor of the sinus. The rostral frontal sinus is small and lies between the median plane and the orbit. The ethmoid labyrinth bulges into this sinus. The medial frontal sinus lies between the median septum and the walls of the other two sinuses. It is very small and may be absent. All three sinuses communicate with the nasal cavity.
The maxillary recess (Fig. 5-15, 5-19) communicates with the nasal cavity. Its opening lies in a transverse plane through the rostral roots of the superior fourth premolar tooth.
The recess continues caudally to a plane through the last molar tooth. The walls of the maxillary recess are formed laterally and ventrally by the maxilla and medially by the orbital lamina of the ethmoid bone. The lateral nasal gland occupies the rostral portion of this recess. Its duct opens rostrally into the dorsal vestibule, and its secretion prevents desiccation caused by nasal panting.
Tympanic Cavity
The tympanic cavity is the cavity of the middle ear. It houses the auditory ossicles and communicates with the nasopharynx via the auditory tube. It is bounded ventrally by the tympanic bulla and dorsally by the petrosal part of the temporal bone. Laterally, the external acoustic meatus is closed by the tympanic membrane (Figs. 5-5, 5-8, 5-18).
Joints of the Head
The atlanto-occipital joint was described with the vertebrae. The temporomandibular joint is between the condylar process of the mandible and the mandibular fossa of the zygomatic process of the squamous part of the temporal bone. The articulation is elongated transversely. There is a thin cartilaginous articular disc that separates the articular surfaces of each bone and divides the joint capsule into two compartments. Lateral and caudal ligaments strengthen the joint capsule.
The intermandibular articulation is a synchondrosis with an interdigitating surface that persists throughout life in most dogs.
LIVE DOG
Palpate the features of the skull of the dog’s head. The widest part of the head is the palpable zygomatic arch. Palpate the zygomatic process of the frontal bone (its widest point) and the orbital ligament between it and the frontal process of the zygomatic bone. This ligament forms the lateral border of the rostral part of the orbit. Follow the frontal bone caudally to the temporal line and sagittal crest. Feel the external occipital protuberance and follow the nuchal crest ventrally on each side to the mastoid process of the temporal bone. Flex and extend the atlanto-occipital joint. Follow the frontal bones rostrally to the nose and maxillary bones. Feel the infraorbital foramen on the side of the maxilla at the level of the rostral roots of the fourth premolar. Reflect the lip and study the crowns and necks of the teeth of each dental arch. Find the shearing teeth and note how they come into contact with each other.
Palpate the coronoid process of the mandible medial to the zygomatic arch and the angular process ventrally. Feel the body of the mandible and move the temporomandibular joint by opening the mouth. Palpate the mental foramina, which lie rostrally on the lateral side of the body of the mandible. Palpate the hyoid bones.
STRUCTURES OF THE HEAD
To facilitate the dissection of the head, it should be removed and divided on the median plane. Using a hand saw, make a complete transection of the neck at the level of the fourth cervical vertebra.
Section the head and attached portion of the neck on the median plane using a band saw. Wash the cut surface to remove bone dust and hair.
Skin both halves, leaving the muscles in place. Leave a narrow rim of skin around the margin of the eyelids and at the edge of the lips. Preserve the nose and the philtrum, which is the median groove separating the right and left parts of the superior lip. Skin only the base of the ear.
The right side of the head will be used for the dissection of vessels and nerves, whereas the left side will be used for muscles. At the end of each dissection period, wrap the head in cheesecloth moistened with 1% phenol water or 2% phenoxyethanol before covering your specimen. A plastic bag is useful to prevent desiccation.
Muscles of the Face
The muscles of the face function to open, close, or move the lips, eyelids, nose, and ear. They are all innervated by the facial (seventh cranial) nerve, with the exception of an elevator of the upper eyelid.
Cheek, Lips, and Nose
The superior (upper) and inferior (lower) lips (labia oris) form the lateral wall of the vestibule, which is bounded medially by the teeth and gums. Caudal to the lips the cheek (buccae) forms the lateral wall of the vestibule. The nose is the region rostral to the orbits that bounds the rostral portion of the respiratory passageway.
The platysma (Fig. 5-20) is a cutaneous muscle that passes from the dorsal median raphe of the neck to the angle of the mouth, where it radiates into the orbicularis oris in the lips. It is the most superficial muscle, covering the ventrolateral surface of the face. Transect this muscle and reflect it.
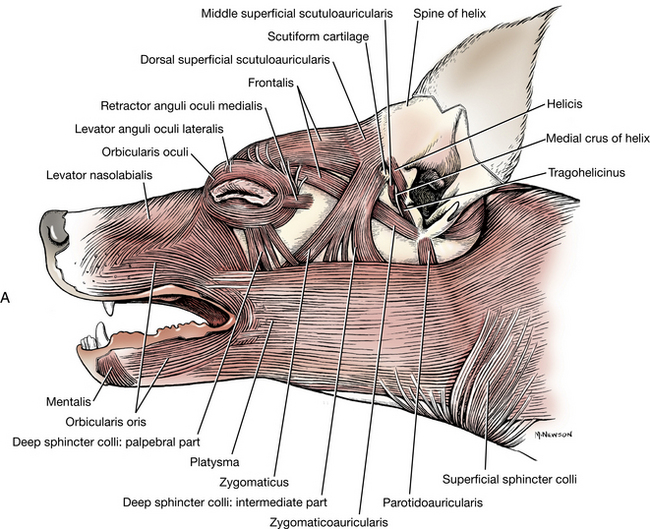
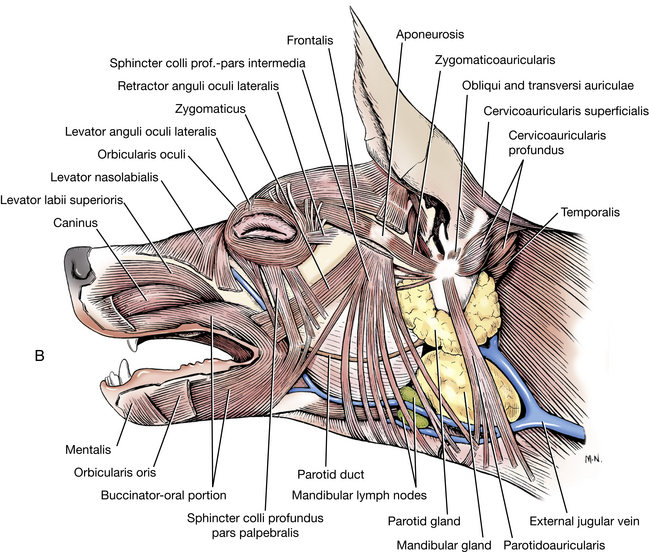
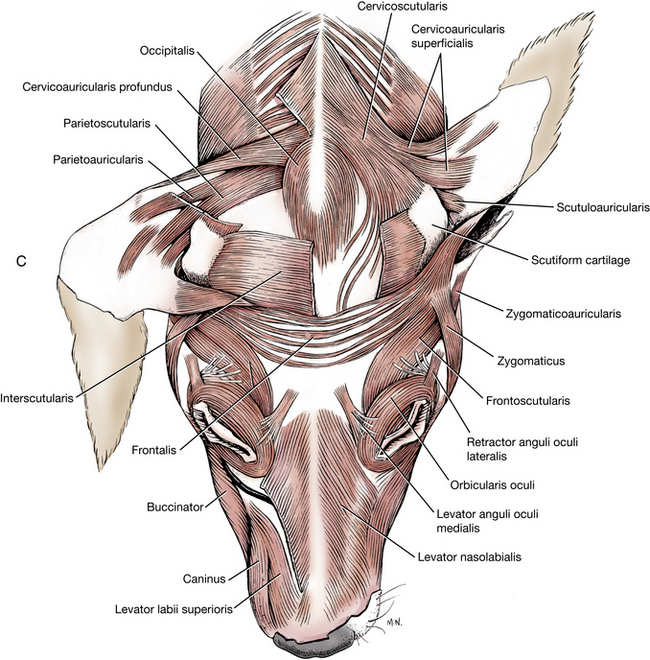
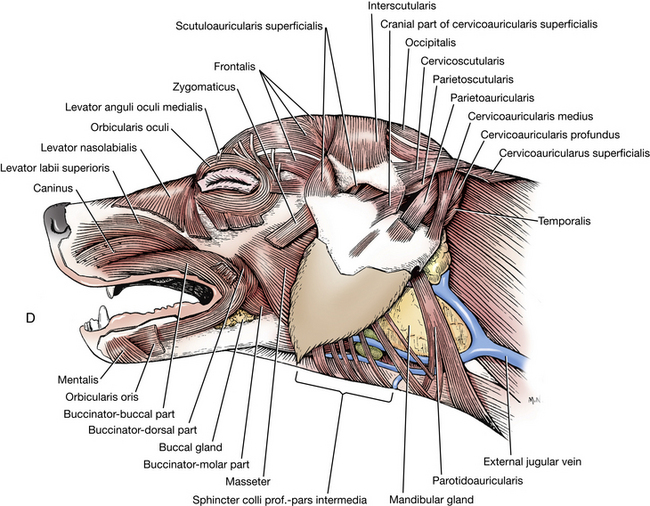
Fig. 5-20 A, Superficial muscles of head, left lateral view. B, Superficial muscles of the head, lateral aspect. (Platysma and sphincter colli superficialis removed.) (Adapted from Evans HE: Miller’s anatomy of the dog, ed 3, Philadelphia, 1993, Saunders.)
C, Deep muscles of the head and ear, dorsal aspect. (Adapted from Evans HE: Miller’s anatomy of the dog, ed 3, Philadelphia, 1993, Saunders.) D, Deep muscles of the head and ear, lateral aspect. (Adapted from Evans HE: Miller’s anatomy of the dog, ed 3, Philadelphia, 1993, Saunders.)The orbicularis oris lies near the free borders of the lips and extends from one lip to the other around the angle of the mouth. The fibers of each side end at the median plane in the incisor region of both jaws.
The buccinator muscle is a thin, wide muscle that forms the foundation of the cheek. It attaches to the alveolar margins of the mandible and maxilla and the adjacent buccal mucosa. It may be found between the rostral border of the masseter muscle and the orbicularis oris. Place your finger within the cheek and press outward. This will help define the buccinator. A portion of the buccinator lies deep to the orbicularis oris muscle and is difficult to separate from it. It functions to return food from the vestibule to the occlusal surface of the teeth.
The levator nasolabialis is a flat muscle lying beneath the skin on the lateral surface of the maxillary bone. It arises from the maxillary bone, courses rostroventrally, and attaches to the edge of the superior lip and on the naris, the external opening of each half of the nasal cavity. It dilates the nostril and raises the superior lip.
Eyelids
Before dissecting the eyelids, palpebrae, observe their external features. The superior and inferior palpebrae (upper and lower eyelids) border the palpebral fissure. They join at either end of the fissure to form the medial and lateral palpebral commissures. Each commissure is attached by ligaments to adjacent bone. The medial palpebral ligament (Fig. 5-21) is well developed and attaches the medial commissure to the frontal bone near the nasomaxillary suture. The lateral palpebral ligament is poorly developed and attaches to the zygomatic bone at the orbital ligament.
The upper eyelid bears cilia (eyelashes) on its free border. The lower eyelid lacks cilia. The cutaneous or external surface of the eyelid is covered by hair. The posterior or inner surface is covered by a mucous membrane, the palpebral conjunctiva (Fig. 5-36). Follow the palpebral conjunctiva posteriorly to its reflection from the eyelids onto the globe of the eye, which is the bulbar conjunctiva. The angle formed by this reflection is called the fornix. The potential cavity thus formed, the conjunctival sac, is bounded posteriorly by the bulbar conjunctiva (where it covers the sclera) and anteriorly by the palpebral conjunctiva.
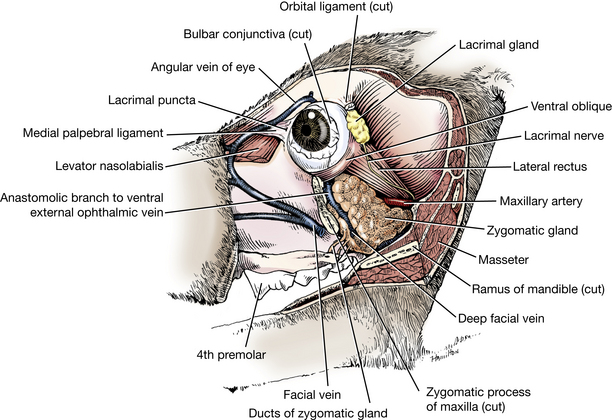
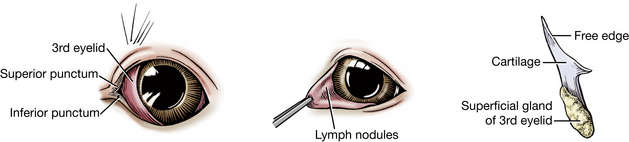
At the medial commissure, observe the triangular prominence of finely haired skin, the lacrimal caruncle. The lacrimal punctum (Figs. 5-21, 5-35) of each lid is the beginning of the dorsal and ventral lacrimal ducts. Each is a small opening on the conjunctival margin of the lid a few millimeters from the medial commissure. The puncta may be difficult to see without the aid of magnification. They are easier to see in a live dog. The lacrimal gland (Figs. 5-21, 5-23, 5-49, 5-53), located ventral to the zygomatic process of the frontal bone, secretes through many duct openings into the dorsolateral part of the conjunctival sac. After this serous fluid has passed across the cornea, it is collected by the puncta and passes in succession through the lacrimal duct of each lid, the lacrimal sac, and the nasolacrimal duct to the ventral nasal meatus of the rostral part of each half of the nasal cavity. There, evaporation of the lacrimal secretion takes place. A significant contribution to tear secretion comes from the gland of the third eyelid, conjunctival goblet cells, and tarsal glands of the eyelids. The lacrimal gland and the rostral opening of the nasolacrimal duct will be seen later.
The plica semilunaris, or third eyelid (Fig. 5-35), is a concave fold of palpebral conjunctiva and cartilage that protrudes from the medial angle of the eye. The cartilage is T shaped, with an expanded portion in the medial canthus and a stem that extends ventrally into the orbit. It is surrounded by a body of fat and glandular tissue, the superficial gland of the third eyelid. This will be dissected shortly. Its serous secretion enters the conjunctival sac under the third eyelid at the medial commissure. Lift the third eyelid from the bulbar conjunctiva and examine its bulbar (lateral) surface. Note the slightly raised lymphoid tissue.
There are several muscles associated with the eyelids. The orbicularis oculi (Fig. 5-20) lies partly in the eyelids and is attached medially to the medial palpebral ligament. Laterally, the fibers of the muscle blend with those of the retractor anguli oculi lateralis, which covers the lateral palpebral ligament. The action of the muscle is to close the palpebral fissure. The levator palpebrae superioris arises deep within the orbit and will be dissected with the muscles of the eyeball. It elevates the superior lid.
The External Ear
The rostral auricular muscles (Fig. 5-20) include those muscles that lie on the forehead caudal to the orbit and converge toward the auricular cartilage. Transect the muscles at their origins and turn them toward the auricular cartilage. Notice that the mid-dorsal part arises from its fellow of the opposite side.
The scutiform cartilage is a small, boot-shaped, cartilaginous plate located in the muscles rostral and medial to the external ear. It is an isolated cartilage interposed in the auricular muscles.
The caudal auricular muscles are the largest group. Most of these muscles arise from the median raphe of the neck and attach directly to the auricular cartilage. Transect the caudal auricular muscles and turn the external ear ventrally to expose the temporal muscle.
The other superficial muscles of the face, all innervated by the facial nerve, will not be dissected. They are collectively referred to as the mimetic muscles or muscles of facial expression.
Oral Cavity
The oral cavity, or mouth, is divided into the vestibule and the oral cavity proper. The vestibule is the cavity lying outside the teeth and gums and inside the lips and cheeks. The ducts of the parotid and zygomatic salivary glands open into the dorsocaudal part of the vestibule. The parotid duct opens through the cheek on a small papilla located opposite the caudal end of the upper fourth premolar or shearing tooth. The ducts of the zygomatic gland (Figs. 5-21, 5-23) open into the vestibule lateral to the last upper molar tooth.
The oral cavity proper is bounded dorsally by the hard palate and a small part of the adjacent soft palate, laterally and rostrally by the dental arches, and ventrally by the tongue and adjacent mucosa. Its caudal boundary ventrally is the body of the tongue at the palatoglossal arch. Pull the tongue away from one mandible and note the fold of tissue that extends from the body of the tongue to the beginning of the soft palate; this is the palatoglossal arch (Fig. 5-22). The oral cavity communicates freely with the vestibule by numerous interdental spaces and is continued caudally by the oropharynx.
Tongue
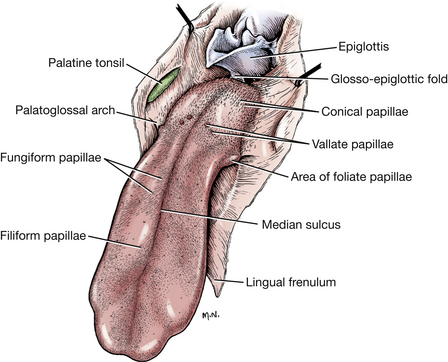
Examine the tongue (Fig. 5-22). It is a muscular organ composed of the interwoven bundles of intrinsic and extrinsic muscles. These will be dissected later. It is divided into a root, which composes its caudal third; a body, which is the long, slender, rostral part of the tongue; and a free extremity, the apex. The mucosa covering the dorsum of the tongue is modified to form various types of papillae. A dissecting microscope facilitates examination of these structures. Five types of papillae are recognized by their shape. The filiform papillae are found predominantly on the body and apex of the tongue. They are arranged in rows like shingles, with their multiple pointed tips directed caudally. At the root of the tongue, the filiform papillae are replaced by conical papillae, which have only one pointed tip. The fungiform papillae have a smooth, rounded surface and are fewer in number. They are located among the filiform papillae. A few may be scattered caudally among the conical papillae. The foliate papillae are found on the lateral margins of the root of the tongue, rostral to the palatoglossal arch. They are leaflike but appear as a row of parallel grooves in the fixed specimen. The vallate papillae are located at the junction of the body and root of the tongue. There are four to six in the dog, and they are arranged in the form of a V with the apex directed caudally. They are larger than the others, have a circular surface, and are surrounded by a sulcus. There are taste buds on vallate, foliate, and fungiform papillae.
The tongue is attached rostrally to the floor of the oral cavity by a ventral median fold of mucosa, the lingual frenulum (Figs. 5-22, 5-23). Examine the medial cut surface of the apex of the tongue. On the midline, just under the mucosa, is the lyssa (Fig. 5-24). This fusiform fibrous spicule extends from the apex to the level of the attachment of the frenulum. Expose the lyssa.
Salivary Glands
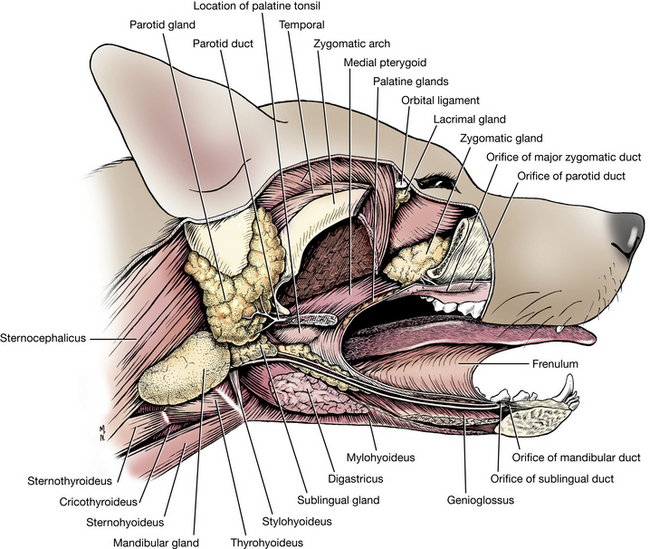
Turn the tongue medially and observe the slightly raised elevation of mucosa that is lateral to the rostral part of the frenulum and protrudes from the floor of the oral cavity. This is the sublingual caruncle. Extending caudally from the caruncle is the sublingual fold. (This is easier to see in the live animal.) The mandibular duct and major sublingual duct (Figs. 5-23, 5-46) are found in this fold. They course rostrally to open on or beside the sublingual caruncle, separately or through a common opening. Carefully incise the mucosa over these ducts from the caruncle to the root of the tongue at the palatoglossal arch. Bluntly reflect the mucosa to expose the ducts and associated salivary tissue. The major sublingual duct is connected caudally with the monostomatic sublingual gland. This is closely associated with the mandibular salivary gland. There are also sublingual gland lobules (the polystomatic sublingual gland) deep to the mucosa of the sublingual fold. These have independent microscopic ducts opening into the oral cavity. Follow the mandibular and major sublingual ducts to the root of the tongue. Their origin will be seen when these glands are dissected from the lateral side of the head.
Expose the mandibular salivary gland (Figs. 2-12, 5-23, 5-46) on the lateral side of the head just caudal to the angle of the mandible, where it lies between the maxillary and linguofacial veins. It is covered by a thick capsule that also includes the caudal part of the monostomatic sublingual gland (Figs. 5-23, 5-46). Incise the capsule that surrounds these two glands and free the caudal portion by elevating it from the capsule.
Locate the division between the rostrally located sublingual gland, which is roughly triangular, and the larger ovoid mandibular gland. The ducts of both glands leave the rostromedial surface and enter the space between the masseter and the digastricus muscles. These ducts course rostrally beside the frenulum to open in the oral cavity at the sublingual caruncle. Lobules of the sublingual gland continue into the oral cavity with these ducts, where they can be seen beneath the oral mucosa.
The parotid salivary gland (Figs. 2-12, 5-23) lies between the mandibular gland and the ear. It is closely applied to the base of the auricular cartilage of the ear. A small parotid lymph node may be found along the rostral border of this gland. The parotid duct (Figs. 5-23, 5-41) is formed by two or three converging radicles, which unite and leave the rostral border of the gland. It grooves the lateral surface of the masseter muscle as it passes to the cheek. It opens into the vestibule on a small papilla at the level of the caudal margin of the fourth upper premolar. Evert the upper lip near the commissure and find the small opening into the vestibule. The zygomatic salivary gland is medial to the zygomatic bone between the eyeball and the pterygoid muscle where it will be dissected with the eye. The ducts of the zygomatic salivary gland open into the vestibule near the last molar, caudal to the parotid duct.
Palate
Examine the roof of the oral cavity. The hard palate is crossed by approximately eight transverse ridges (Fig. 5-24). A small eminence, the incisive papilla, is located just caudal to the central incisor teeth. The fissure on either side of this papilla is the oral opening of the incisive duct. The incisive duct passes through the palatine fissure and opens into the ventral nasal meatus. Extending caudally from the incisive duct, close to its entrance into the nasal cavity, is the vomeronasal organ (Fig. 5-16). This tubular structure about 2 cm long lies at the base of the nasal septum dorsal to the hard palate and is an olfactory receptor of sexual stimuli. It can sometimes be seen on the sagittal section of the head if the cut was made slightly to one side of the midline.
Pharynx
The pharynx (Figs. 5-24, 5-25) is a passage that is common, in part, to both the respiratory and digestive systems. It is located between the oral cavity and esophagus and is divided into oral, nasal, and laryngeal parts. The oropharynx extends from the level of the palatoglossal arches to the caudal border of the soft palate and the base of the epiglottis at the caudal end of the root of the tongue. The dorsal and ventral boundaries of the oropharynx are the soft palate and the root of the tongue. The lateral wall of the oropharynx contains the palatine tonsil in the tonsillar fossa.
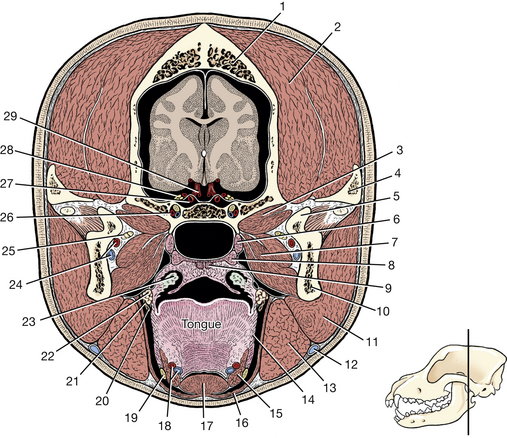
Fig. 5-25 Transection of head through palatine tonsil.
4. Zygomatic process of temporal bone
23. Palatine tonsil in tonsillar fossa
24. Inferior alveolar a. and v.
25. Mylohyoid, inferior alveolar, and lingual nn.
26. Maxillary a., v., and n. in alar canal
27. Internal carotid a. in cavernous sinus
28. Cranial nerves III, IV, and VI and ophthalmic division of V
The palatine tonsil (Figs. 5-22, 5-23, 5-25) is elongated and is located caudal to the palatoglossal arch. The medial wall of the fossa, which partially covers the tonsil, is the semilunar fold. The tonsil is attached laterally throughout its entire length. Reflect the tonsil from the fossa.
The nasal cavity extends from the nares to the choanae. It is divided into right and left halves by the nasal septum. Each half is divided into four meatuses. These were described with the bones of the nasal cavity and should be reviewed now. On the floor of the rostrolateral end of the ventral meatus, find the opening of the nasolacrimal duct on the ventral aspect of the alar fold (Fig. 5-24). It may be necessary to remove the rostral end of the cartilaginous septum to see the opening. This duct comes from the lacrimal sac at the medial commissure of the eye.
The nasopharynx extends from the choanae to the junction of the palatopharyngeal arches at the caudal border of the soft palate. A palatopharyngeal arch extends caudally on each side from the caudal border of the soft palate to the dorsolateral wall of the nasopharynx. It is a fold of mucosa that covers the palatopharyngeus muscle. On the lateral wall of the nasopharynx, dorsal to the middle of the soft palate, is an oblique, slitlike opening, the pharyngeal opening of the auditory tube.
The laryngopharynx (Fig. 5-24) is dorsal to the larynx. It extends from the palatopharyngeal arches to the beginning of the esophagus. The esophagus begins at an annular constriction at the level of the cricoid cartilage, the pharyngoesophageal limen.
Pharyngeal Muscles
The pharyngeal muscles (Figs. 5-24, 5-32) aid directly in swallowing. The cricopharyngeus arises from the lateral surface of the cricoid cartilage. Its fibers are inserted on the median dorsal raphe of the laryngopharynx. Caudally, its fibers blend with the esophagus.
The thyropharyngeus arises from the lateral side of the thyroid lamina and is inserted on the median dorsal raphe of the pharynx. This muscle is rostral to the cricopharyngeus and caudal to the hyopharyngeus.
The hyopharyngeus is in two parts as it arises from the lateral surface of the thyrohyoid bone and the ceratohyoid bone. This origin was previously transected. The fibers of both parts form a muscle plate that passes dorsally over the larynx and pharynx to be inserted on the median dorsal raphe of the pharynx with its fellow from the opposite side. These pharyngeal muscles are all innervated by pharyngeal branches of the glossopharyngeal and vagus nerves. The remaining pharyngeal muscles and muscles of the palate listed here need not be dissected (Figs. 5-24, 5-32).
The palatopharyngeus passes from the soft palate into the lateral and dorsal wall of the pharynx. Its border is in the palatopharyngeal arch. The pterygopharyngeus arises from the pterygoid bone, passes caudally, and is inserted in the dorsal wall of the pharynx. These muscles constrict and shorten the pharynx.
The stylopharyngeus arises from the stylohyoid bone and passes caudolaterally deep to the hyopharyngeus and thyropharyngeus muscles to be inserted in the dorsolateral wall of the pharynx. It acts to dilate the pharynx.
The levator veli palatini arises from the tympanic part of the temporal bone and passes ventrally to enter the soft palate caudal to the pterygoid bone. It raises the caudal end of the soft palate (Fig. 5-24).
The tensor veli palatini arises mainly from the cartilaginous wall of the auditory tube and is inserted on the pterygoid bone and medially on the soft palate.
Larynx
Cartilages of the Larynx (Figs. 5-26 to 5-29)
Study the cartilages of the larynx on the hemisected head and on specimens from which the muscles have been removed. Visualize their topography in your bisected specimen and palpate them through the laryngeal mucosa. The laryngeal cartilages that will be dissected include the paired arytenoid and the unpaired epiglottic, thyroid, and cricoid cartilages.
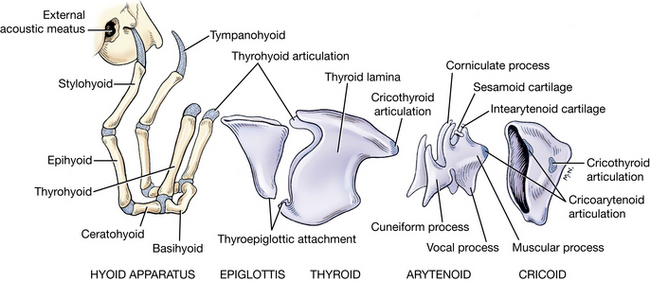
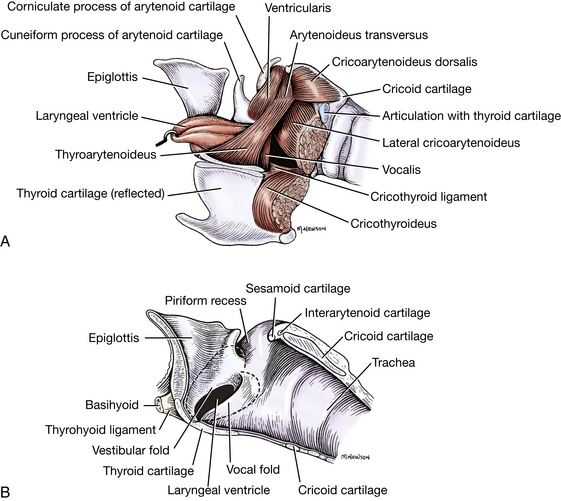
Fig. 5-27 A, Laryngeal muscles, left lateral view. The left side of the thyroid cartilage is reflected. B, Median section of the larynx. (The dotted line indicates the extent of the lateral ventricle and the laryngeal ventricle.) (Adapted from Evans HE: Miller’s anatomy of the dog, ed 3, Philadelphia, 1993, Saunders.)
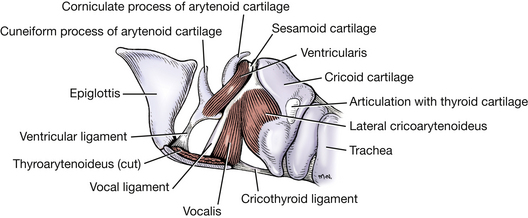
Fig. 5-28 Laryngeal muscles, left lateral view. The left half of the thyroid cartilage has been removed along with the thyroarytenoideus, arytenoideus transversus, and cricoarytenoideus dorsalis.
The epiglottic cartilage lies at the entrance to the larynx. Its lingual surface is attached to the basihyoid bone and faces the oropharynx. The apex lies just dorsal to the edge of the soft palate. The lateral margin is attached by mucosa to the cuneiform process of the arytenoid to form the aryepiglottic fold. Caudally, the epiglottis attaches to the body of the thyroid cartilage.
The thyroid cartilage forms a deep trough, which is open dorsally. The rostral cornu articulates with the thyrohyoid bone; the caudal cornu articulates with the caudal aspect of the cricoid cartilage. Ventrally, the caudal border is notched by a median caudal thyroid incisure. The cricothyroid ligament attaches the caudal border to the ventral arch of the cricoid cartilage.
The cricoid cartilage forms a complete ring that lies partially within the trough of the thyroid cartilage. It has a wide dorsal plate, or lamina, and a narrow ventral arch. Near the caudal border at the junction of the lamina and the arch, there is a lateral facet for articulation with the caudal cornu of the thyroid cartilage. On the cranial border of the lamina, there is a prominent pair of lateral facets for articulation with the arytenoid cartilages.
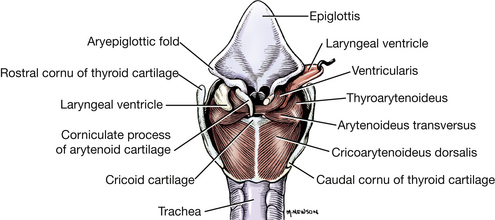
The arytenoid cartilage is paired, irregular in shape, and located in a sagittal plane. Each articulates medially with a facet on the rostral border of the cricoid lamina and has a lateral muscular process and a ventrally directed vocal process. The vocal fold is attached between the vocal process of the arytenoid and the midventral part of the thyroid cartilage. The arytenoid cartilage bears a corniculate process dorsally. Rostral to this process, the cuneiform process is attached to the arytenoid. The vestibular fold extends from the thyroid cartilage ventrally to the ventral portion of the cuneiform process and forms the rostral boundary of the laryngeal ventricle. The laryngeal ventricle is a diverticulum of the laryngeal mucosa bounded laterally by the thyroid cartilage and medially by the arytenoid cartilage. It opens into the larynx between the vestibular fold rostrally and vocal fold caudally. Observe these folds and the laryngeal ventricle on the medial side of your specimen (Figs. 5-27 through 5-29).
The glottis consists of the vocal folds, the vocal processes of the arytenoid cartilages, and the rima glottidis, which is the narrow passageway through the glottis. At this level the size and shape of the air passageway can be altered by muscular activity.
Muscles of the Larynx
The cricothyroid muscle (Fig. 5-27) lies ventral to the insertion of the sternothyroideus muscle and passes from the cricoid cartilage to the thyroid lamina. It tenses the vocal fold indirectly by drawing the ventral parts of the cricoid and thyroid cartilages together. It is innervated by the cranial laryngeal nerve, a branch of the vagus. Observe this on the lateral side.
On the medial side of the specimen reflect the mucosa of the laryngopharynx from the dorsal aspect of the larynx. Separate the thyroid lamina from the cricoid and arytenoid cartilages to expose the muscles.
The cricoarytenoideus dorsalis (Figs. 5-27, 5-29) arises from the dorsolateral surface of the cricoid cartilage and inserts on the muscular process on the lateral surface of the arytenoid cartilage. It rotates the arytenoid so that the vocal process moves laterally, opening the glottis. It is the only laryngeal muscle that functions primarily to open the glottis. Transect the muscle and examine the articular surface of the cricoarytenoid joint. On the intact specimen of laryngeal cartilages, grasp the muscular process of the arytenoid with forceps and pull it caudomedially as it would be pulled by the functioning cricoarytenoideus dorsalis muscle. Observe the abduction of the vocal process and fold that widens the glottal opening.
The cricoarytenoideus lateralis arises from the lateral surface of the cricoid cartilage and inserts on the arytenoid cartilage between the cricoarytenoideus dorsalis and the vocalis. It acts to close the glottis by pulling the muscular process ventrally and thus moving the vocal process medially. Expose this muscle by reflecting the cricoid medially away from the thyroid lamina.
The thyroarytenoideus is the parent muscle that gives rise to the vocalis muscle medially and ventricularis muscle rostrally. It arises along the internal midline of the thyroid cartilage and inserts on the arytenoid cartilage. Its function is to relax the vocal fold and to constrict the glottis.
The vocalis is a medial division of the thyroarytenoid muscle. It arises on the internal midline of the thyroid cartilage and inserts on the vocal process of the arytenoid cartilage. Cut the laryngeal mucosa of the vocal fold and observe the medial side of this muscle. Attached along its rostral border is the vocal ligament (Fig. 5-28).
The cricoarytenoideus dorsalis and lateralis and the thyroarytenoideus muscles are innervated by the caudal laryngeal nerve from the recurrent laryngeal nerve. The ventricularis and arytenoideus transversus will not be dissected. Notice the relationship of laryngeal ventricle to the laryngeal muscles. From its laryngeal opening, it runs rostrally between the thyroid lamina and thyroarytenoideus laterally and the vestibular fold, the cuneiform process, and the ventricularis medially.
The External Ear
The external ear (Fig. 5-30) consists of the auricle and the external acoustic meatus (ear canal). The external acoustic meatus is mostly cartilaginous but has a short osseous part on the lateral aspect of the tympanic bulla. The cartilaginous part of the meatus makes a right-angle turn in the deeper part of its course and extends to the tympanic membrane.
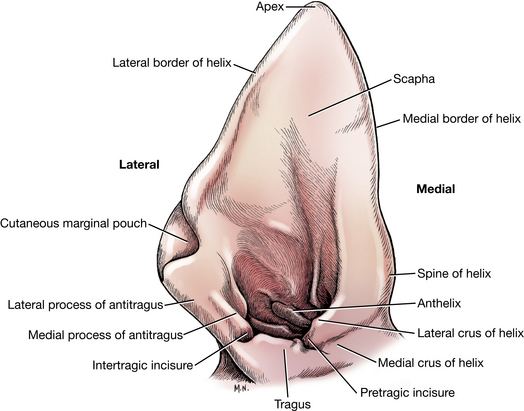
Except for one small annular cartilage adjacent to the skull, the external ear consists of a single auricular cartilage that is rolled into a tube ventromedially. The tubular part becomes the external acoustic meatus. Remove the skin from the base of the auricular cartilage. The auricular cartilage is funnel shaped. Its external, convex surface faces caudally; its internal, concave surface faces rostrally. It has a slightly folded medial and lateral margin called the helix. The auricular cartilage is thin and pliable except proximally, where it thickens and rolls into a tube. On its internal, concave wall at the level of the beginning of the external acoustic meatus, there is a transverse ridge, the anthelix. Opposite the anthelix the rostral boundary of the initial part of the ear canal is formed by a thick, quadrangular plate of the auricular cartilage, the tragus. Projecting caudally from the tragus and completing the lateral boundary of the external ear canal is a thin, elongate piece of cartilage, the antitragus. The intertragic incisure separates these two parts of the auricular cartilage.
The lateral portion of the helix is indented proximally by an incisure. At this point the skin forms a pouch, the marginal cutaneous sac.
The medial helix is nearly straight. An abrupt angle in this border at its proximal end forms the spine of the helix. Between the spine of the helix and the tragus the medial border of the ear canal is formed by two curved portions of the cartilage, the medial and lateral crura of the helix. They both end laterally in a free border separated from the tragus by the pretragic incisure.
Incise the lateral wall of the ear canal by two parallel incisions starting at the intertragic and pretragic incisures. Reflect the isolated piece of the lateral wall to observe the course of the external acoustic meatus to the tympanic membrane.
Interposed between the auricular cartilage and the bony external acoustic meatus of the temporal bone is the annular cartilage. This is a band of cartilage that overlaps the bony projection of the meatus.
Muscles of Mastication and Related Muscles
On the left half of the head, cut all of the attachments of the temporal and masseter muscles to the zygomatic arch. Cut through the arch rostrally and caudally and remove all of the arch rostral to the temporomandibular joint.
The temporalis muscle (Figs. 5-23, 5-25, 5-31) arises from the temporal fossa and inserts on the coronoid process of the mandible. Remove the muscle from its wide origin by scraping it off the bone with a blunt instrument, such as a scalpel handle, and reflect it. Be vigorous; there is a large amount of muscle to remove. The temporal and masseter muscles fuse between the zygomatic arch and the coronoid process.
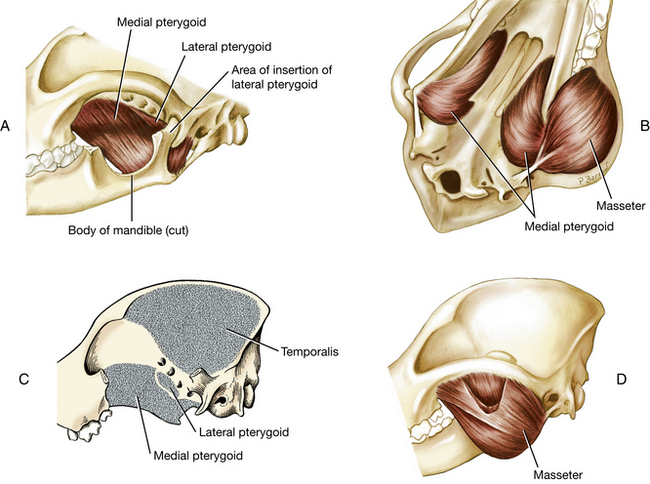
Fig. 5-31 Muscles of mastication. A, Pterygoideus medialis and lateralis. B, Masseter and pterygoideus medialis. C, Areas of origin of temporalis, pterygoideus medialis, and lateralis. D, Masseter cut to show the deep portion.
The masseter muscle (Figs. 2-12, 5-20, D, 5-23, 5-25, 5-31) arises from the zygomatic arch, where its deep portion is intermingled with the fibers of the temporal muscle. It inserts in the masseteric fossa, the ventrolateral surface of the ramus of the mandible, and the angular process. The muscle is covered by a strong, glistening aponeurosis and contains many tendinous intermuscular strands.
Transect the temporal muscle as close to its insertion as possible. With bone cutters, remove the coronoid process and the remaining attached muscles. Observe the dorsal surface of the pterygoid muscles, which are now exposed in the ventral orbit.
Between the eyeball and the pterygoid muscles is the zygomatic salivary gland (Figs. 5-21, 5-23, 5-46). It is hidden laterally by the zygomatic bone. The gland opens into the vestibule by one main and several minor ducts lateral to the last superior molar tooth.
The medial and lateral pterygoid muscles (Figs. 5-23, 5-25, 5-31, 5-46, 5-53) arise from the pterygopalatine fossa and insert on the medial surface and caudal margin of the ramus of the mandible and angular process, ventral to the insertion of the temporal muscle. The muscles need not be distinguished from each other. The bulk of the muscle mass is the medial pterygoid. On the medial side of your specimen, cut the mucosa of the oropharynx from the rostral end of the palatine tonsil to the midline at the junction of the soft and hard palates. Reflect the cut edges to expose the ventral surface of the medial pterygoid muscle. On a dog skull, remove the mandible and place your thumb in the pterygopalatine fossa to appreciate the position of this muscle. The eyeball and its periorbital sheath would rest on your thumb.
The temporal, masseter, and pterygoid muscles (Fig. 5-31) function to close the jaws. They are innervated by the mandibular nerve, a branch of the trigeminal nerve (cranial nerve V).
Reflect the mandibular and parotid salivary glands to expose the digastricus muscle.
The digastricus (Figs. 2-12, 5-23, 5-25) arises from the paracondylar process of the occipital bone and is inserted on the body of the mandible. A tendinous intersection crosses its belly and divides it into rostral and caudal parts. Transect it and expose its attachments. It acts to open the jaws. The rostral portion is innervated by the mandibular nerve (a branch of the trigeminal, cranial nerve V), whereas the caudal belly receives the facial nerve (cranial nerve VII) innervation.
Lingual Muscles
The muscles of the tongue (Figs. 5-24, 5-25, 5-32) may be divided into extrinsic and intrinsic groups. Three paired extrinsic muscles enter the tongue. The styloglossus and hyoglossus muscles are best exposed on the lateral side, the genioglossus on the medial side.
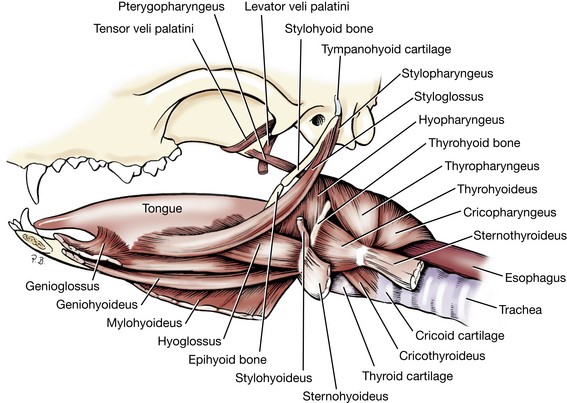
The styloglossus arises from the stylohyoid bone, passes rostroventrally lateral to the palatine tonsil, and inserts in the middle of the tongue. It retracts and elevates the tongue.
The hyoglossus arises from the thyrohyoid and the basihyoid and passes into the root of the tongue. It lies medial to the styloglossus and retracts and depresses the tongue.
The genioglossus arises from the intermandibular articulation and adjacent surface of the body of the mandible. It joins its fellow at the median plane and is bounded medially by the geniohyoideus and laterally by the hyoglossus. Its caudal fibers protrude the tongue, and its rostral ones retract the apex. It lies partly in the frenulum. These muscles are all innervated by the hypoglossal nerve (cranial nerve XII).
Hyoid Muscles
The hyoid muscles (Fig. 5-32) are associated with the hyoid apparatus, which suspends the larynx and anchors the tongue. They function in swallowing, lolling, lapping, and retching. All muscles of this group have names with the suffix hyoideus. The prefixes of the hyoid muscles designate the bone or part from which they arise. Dissect the following hyoid muscles from the lateral side.
The sternohyoideus, from its origin on the sternum and first costal cartilage, is fused to the deeper sternothyroideus for the first third of its length. It then separates from this muscle and runs an independent course, adjacent to the ventral midline, to insert on the basihyoid bone. Its origin was previously dissected.
The thyrohyoideus is a short muscle that lies dorsal to the sternohyoideus. It extends from the thyroid cartilage of the larynx to the thyrohyoid bone.
The sternohyoideus and thyrohyoideus muscles are innervated by ventral branches of cervical spinal nerves and the hypoglossal nerve (cranial nerve XII).
The mylohyoideus spans the intermandibular space. It arises as a thin sheet of transverse fibers from the medial surface of the body of the mandible. It is inserted on its fellow muscle at the midventral raphe. Caudally, it inserts on the basihyoid. It forms a sling that aids in the support of the tongue. It is innervated by the mandibular nerve of the trigeminal.
The geniohyoideus lies deep to the mylohyoideus. It is a muscular strap that arises on and adjacent to the intermandibular articulation. It parallels its fellow along the median plane and attaches to the basihyoid. Contraction of the geniohyoideus draws the hyoid apparatus and larynx rostrally. It is innervated by the hypoglossal nerve.
The Eye and Related Structures
The orbit is a conical cavity containing the eyeball and ocular adnexa. These were exposed when the muscles of mastication were dissected. The orbital margin is formed by the frontal, lacrimal, maxillary, and zygomatic bones and the orbital ligament laterally. The medial wall of the orbit is formed by parts of the frontal, presphenoid, and lacrimal bones. The ventral wall includes the zygomatic salivary gland and the pterygoid muscles. The dorsal and lateral walls are formed primarily by temporal muscle.
The periorbita (Fig. 5-53) is a cone-shaped sheath of connective tissue and smooth muscle that encloses the eyeball and its muscles, vessels, and nerves. Where the periorbita contacts the bone medially, it is the periosteum of the orbit. Its apex is caudal where it attaches to the bony margin of the optic canal and the orbital fissure. Here it is continuous with the dura intracranially. Rostrally, it widens to blend with the periosteum of the face. Orbital fat may be observed on both sides of the periorbita.
Reflect the orbital ligament and the periorbita from the dorsolateral surface of the eyeball. The lacrimal gland (Figs. 5-21, 5-23, 5-49, 5-53) is a small, flat lobular structure lying on the medial side of the orbital ligament within the periorbita. Small ducts that cannot be seen without a microscope empty their secretion into the conjunctival sac at the dorsal fornix.
Incise the periorbita longitudinally on its lateral side and reflect it to expose the eyeball muscles and the levator of the upper eyelid (Figs. 5-33, 5-54).
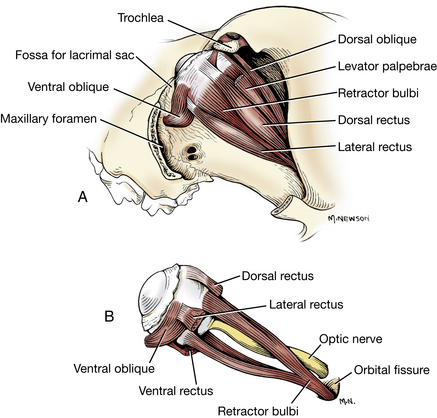
Fig. 5-33 A, Extrinsic muscles of left eyeball, dorsolateral view. B, Retractor bulbi muscle exposed, lateral view.
The levator palpebrae superioris (Fig. 5-33, 5-54) is narrow and superficial. It begins at the apex of the orbit, extends over the dorsal rectus, and widens to insert as a flat tendon in the upper eyelid. It is innervated by the oculomotor nerve (cranial nerve III).
There are seven extrinsic muscles of the eyeball (Figs. 5-33, 5-34, 5-49, 5-54): two obliquus muscles, four rectus muscles, and the retractor bulbi. All of these extrinsic muscles insert on the fibrous coat of the eyeball, the sclera, near the equator of the eyeball. The rectus muscles insert closer to the corneoscleral junction than the retractor muscles.

The four rectus muscles are the dorsal rectus, medial rectus, ventral rectus, and lateral rectus. As they course rostrally from their small area of origin around the optic canal and orbital fissure, they diverge and attach to the sclera on an imaginary line encircling the eyeball at its equator. In the spaces between the rectus muscles, parts of the retractor bulbi can be seen. The retractor bulbi muscle consists of four fascicles that surround the optic nerve, a dorsal pair and a ventral pair. The retractor bulbi and lateral rectus are innervated by the abducent nerve (cranial nerve VI). The other three recti are innervated by the oculomotor nerve.
The dorsal oblique ascends on the dorsomedial side of the extraocular muscles dorsal to the medial rectus. Roll the dorsal aspect of the eyeball laterally to expose these muscles. The dorsal oblique is a narrow muscle that forms a long tendon rostrally that passes through a groove in the trochlea. The trochlea is a cartilaginous plaque attached at the level of the medial angle of the eye to the wall of the orbit. This must be detached to roll the eyeball laterally. The tendon of the dorsal oblique muscle turns and courses laterally after passing around the trochlea and attaches to the sclera under the tendon of insertion of the dorsal rectus muscle. This insertion is difficult to distinguish and need not be dissected (Fig. 5-33, 5-54). The dorsal oblique is innervated by the trochlear nerve (cranial nerve IV).
The ventral oblique arises from the rostral border of the palatine bone at the level of the maxillary foramen, passes ventral to the ventral rectus, and is inserted on the sclera at the insertion of the lateral rectus. This is the only extraocular muscle that does not arise from the apex of the orbit. It is innervated by the oculomotor nerve (cranial nerve III).
To understand the action of these individual muscles, consider the eyeball as having three imaginary axes that cross in the center of the globe (Fig. 5-34). The dorsal and ventral rectus muscles would rotate the eyeball around a horizontal axis through the equator from medial to lateral. The medial and lateral rectus muscles would rotate it around a vertical axis through the equator from dorsal to ventral. The oblique muscles would rotate the eyeball around a longitudinal axis passing from anterior to posterior through the center of the eyeball.
Enlarge the opening of the palpebral fissure by cutting through the lateral commissure and the underlying conjunctiva to the eyeball. This will facilitate exposure of the third eyelid in the medial angle. Elevate the third eyelid and observe the lymph nodules on its bulbar conjunctival surface and the superficial gland of the third eyelid (Fig. 5-35).
Bulbus Oculi
In the following dissection, leave the bulbus oculi, or eyeball, in the orbit. Many of these structures are best observed in a fresh eye under a dissecting microscope. Freeze-dried preparations of the opened eyeball are instructive for seeing the zonular fibers that suspend the lens. Directional terms used with reference to the eyeball are anterior and posterior and superior and inferior. The wall is composed of three layers: an external fibrous coat, a vascular coat, and an internal coat that includes the retina (Figs. 5-36 through 5-38).
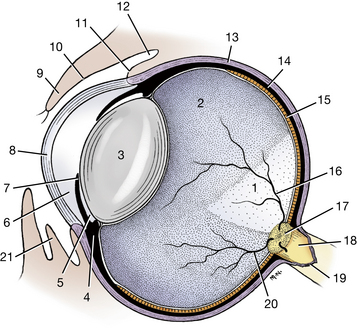
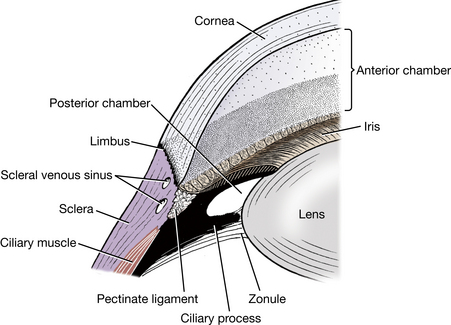
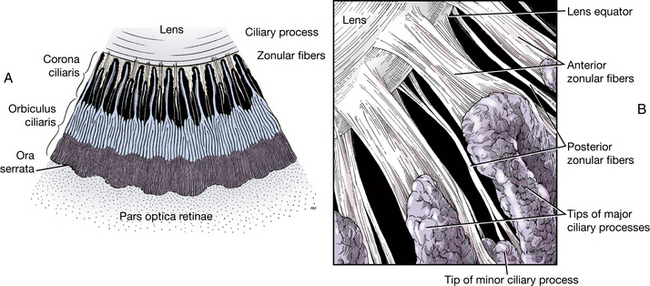
Fig. 5-38 A, Inner surface of a ciliary body segment. B, Zonular fibers passing along ciliary processes before attaching to lens, anterior view.
1. The external fibrous coat is composed of the cornea, which forms the anterior one fourth, and the sclera, which forms the posterior three fourths. The cornea is transparent and circular. It meets the dense, opaque sclera peripherally at the corneoscleral junction, or limbus, of the cornea. The sclera is dull gray-white. Anteriorly, it is covered by bulbar conjunctiva. Posterior to this, the extrinsic ocular muscles insert in its wall, and it is penetrated by blood vessels and nerves, including the large optic nerve posteriorly. Transect and reflect the attachments of the lateral rectus and retractor bulbi muscles on the eyeball and observe the optic nerve on the posterior surface of the globe.
2. The middle vascular coat (the uvea) is deep to the sclera and consists of three continuous parts from posterior to anterior: the choroid, ciliary body, and iris. The iris, which has circular and radial smooth muscle, can be seen through the cornea as a pigmented diaphragm with a central opening, the pupil. While the eyeball is in the orbit, use a sharp scalpel or razor blade to make a sagittal cut through the eyeball from anterior to posterior pole and remove the lateral half of the eyeball.
The choroid is the posterior portion of the vascular coat and is firmly attached to the sclera. It is pigmented and lines the internal surface of the sclera as far anterior as the ciliary body posterior to the lens. The junction of the choroid and the ciliary body, called the ora serrata (Fig. 5-38, A), is seen as an undulating line in the overlying retina. The fundus is the posterior or deep portion of the eyeball that is seen with the ophthalmoscope. The light-colored, reflective area in the dorsal part of the fundus is the tapetum lucidum (Fig. 5-36) of the choroid. This is a specialized layer of cells in the choroid behind the retina that reflects light rays.
The vascular coat forms a thick circular mound at the level of the limbus. This is the ciliary body (Fig. 5-36). The ciliary body, located between the iris and choroid, contains numerous muscle bundles that function in the regulation of the shape of the lens. The internal surface of the ciliary body is marked by longitudinal folds, the ciliary processes (Figs. 5-37, 5-38, A and B). Observe these on the lateral portion of the eyeball that was removed. These processes surround but do not attach to the lens at its equator. They consist of several hundred pigmented folds alternating in length, which are small at their posterior border near the ora serrata but enlarge anteriorly as they approach the lens.
The zonule is the suspensory apparatus of the lens (Figs. 5-37, 5-38). It is composed of numerous fine strands, zonular fibers, which pass from the region of the ora serrata along the ciliary processes to the equator of the lens. The lens is suspended from the ciliary processes by the zonular fibers. Contraction of the ciliary muscles pulls the ciliary body and processes toward the lens and therefore relaxes the tension on the zonular fibers attached to the lens. This allows the elastic lens to become more spherical and accommodate for near vision. (In other words, contraction of the ciliary muscle is required for near vision.)
The lens in an embalmed specimen is firm and opaque. In life, it is transparent and elastic. It is bounded posteriorly by the transparent jelly-like vitreous body, which fills the vitreous chamber posterior to the lens. Anteriorly, the lens is bounded by the iris and the aqueous humor. The aqueous humor fills the space between the cornea and the lens. This space is divided by the iris into two chambers. The anterior chamber is the space between the cornea and the iris. The posterior chamber is a narrow cavity between the iris and the lens. Aqueous humor is continually produced by the ciliary epithelium covering the ciliary processes. It circulates through the zonular fibers into the posterior chamber before passing through the pupil into the anterior chamber. From the anterior chamber the aqueous humor is drained through a trabecular meshwork at the iridocorneal angle (Fig. 5-37), where it passes into the venous system via the venous scleral sinus. The iridocorneal angle is traversed by a meshwork of fibers with intervening spaces. This meshwork of the angle is referred to as the pectinate ligament (Fig. 5-37). The integrity of this angle is critical in the drainage of aqueous humor from the eyeball. Failure in the drainage results in increased intraocular pressure, which is known as glaucoma. Remove the lens. Note the zonular fibers as they stretch and break.
3. The internal coat of the eye, the “nervous coat,” consists of the retina and its associated blood vessels and the nerves surrounding the vitreous body. That portion of the retina containing the light-sensitive rods and cones, the bipolar cells, and the ganglion cells is the pars optica retinae. It covers the internal surface of the choroid from the point where the optic nerve enters to the level of the ciliary body. From this boundary, called the ora serrata (Fig. 5-38), there is a thin non–light-receptive portion of the retina that passes anteriorly over the posterior surface of the ciliary body as the pars ciliaris retinae and continues on the posterior surface of the iris as the pars iridica retinae. The ciliary portion of the retina is two layers thick and forms the blood-aqueous barrier, through which aqueous fluid is secreted into the posterior chamber. The iridial portion of the retina is also a double cell layer consisting of pigment cells, which give the iris its color, and myoepithelial cells, which form the dilator pupillae.
In the embalmed specimen the nervous layer of the pars optica retinae has a gray-white appearance, and it readily peels away from the single layer of pigmented epithelial cells on its posterior surface, which remains attached to the choroid. This pigmented layer of the retina and the pigment of the choroid give the interior of the eyeball a brown to black appearance except where the specialized layer of the choroid, the tapetum lucidum, is located. This tapetal area exhibits a variety of brilliant colors from silver to blue to green or orange. In this area there is no pigment in the pigment epithelial cells of the retina covering the tapetum lucidum. The brown-black portion of the interior of the eyeball is sometimes referred to as the nontapetal area or nontapetal nigrum.
Notice the entrance of the optic nerve into the posterior aspect of the eyeball. This is the optic disk. With careful observation of the disk, you may see the retinal vessels that enter with it to supply the internal surface of the retina. The posterior portion of the eyeball that includes the area of the optic disk, tapetum lucidum, and adjacent nontapetal nigrum is referred to as the fundus of the eyeball. The optic disk may be found in the interior region of the tapetum lucidum or at or below its inferior border. This varies with the breed of dog.
Superficial Veins of the Head
The external jugular vein (Figs. 5-39 through 5-41) is formed by the confluence of the linguofacial and maxillary veins caudal to the mandibular salivary gland, which lies between these two veins.
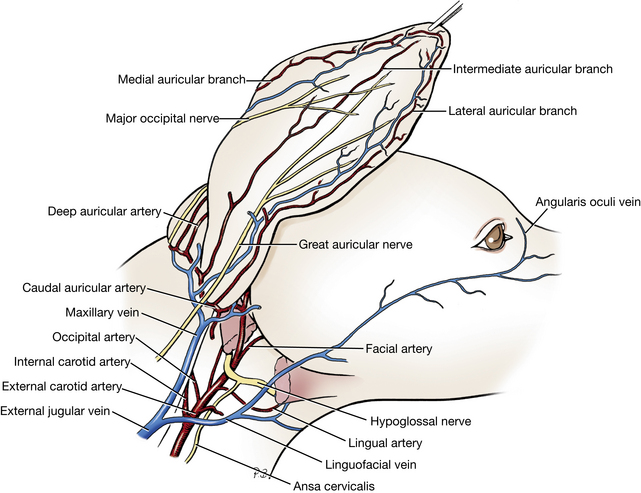
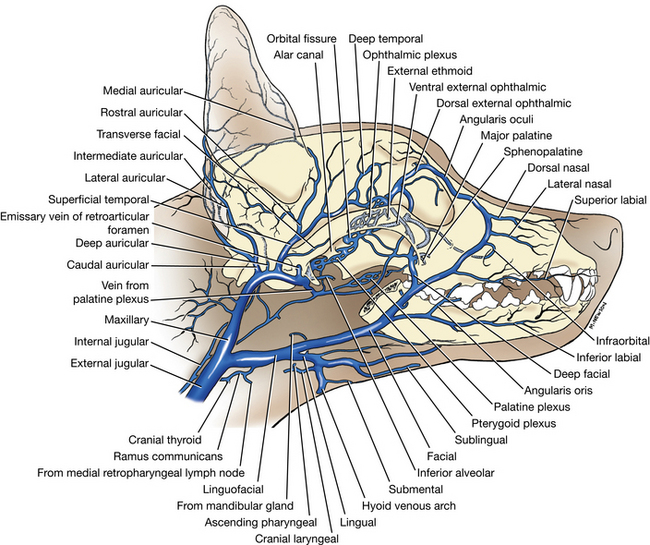
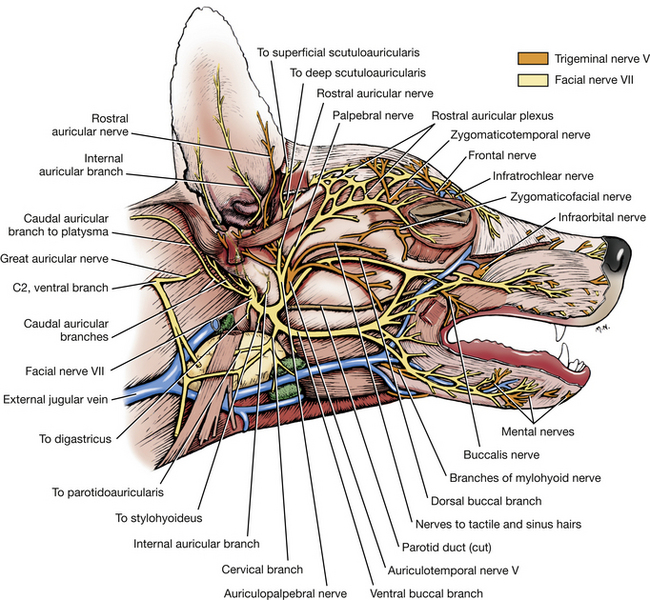
The lingual vein (Fig. 5-40) is the first large tributary that enters the linguofacial vein ventrally. Its radicles drain blood from the tongue, the larynx, and part of the pharynx. These radicles will not be dissected.
The facial vein is the other tributary of the linguofacial. The radicles that form the facial vein lie on the dorsal surface of the muzzle. One of these, the dorsal nasal, runs caudally from the nares, whereas another, the angularis oculi, passes rostrally from the medial aspect of the orbit, where it is continuous with the ophthalmic plexus within the periorbita (Fig. 5-40). Blood may drain from the face in either direction through the angularis oculi. There is also a large communication between the ophthalmic plexus and the facial vein, via the deep facial vein, which is ventral to the zygomatic bone. Identify these veins. The remaining branches will not be dissected, for to do so would sacrifice nerves and arteries. These branches drain the lateral muzzle and the upper and lower lips. The facial vein generally follows the rostral and ventral borders of the masseter muscle before it meets the lingual vein. Note the two or three small mandibular lymph nodes along the linguofacial vein just rostroventral to the mandibular salivary gland.
The maxillary vein drains the ear, orbit, palate, nasal cavity, cheek, and mandible as well as the cranial cavity.
Facial Nerve
The facial, or seventh cranial, nerve (Figs. 5-41, 5-48) innervates all of the superficial muscles of the head and face as well as the caudal belly of the digastricus and the platysma of the neck. The nerve enters the petrosal part of the temporal bone through the internal acoustic meatus, courses through the facial canal of that bone, and leaves the skull at the stylomastoid foramen just caudal to the external acoustic meatus, where it divides into several branches.
Reflect the parotid gland. Dissect deep between the parotid and sublingual glands to expose the facial nerve arising from the stylomastoid foramen caudal to the horizontal portion of the ear canal. The maxillary vein may be transected as it crosses the lateral surface of the nerve at this site. Dissect the following branches of the facial nerve.
The auriculopalpebral nerve arises as the facial nerve curves rostrally ventral to the external acoustic meatus. Dissect deep to the rostral edge of the parotid gland to locate the nerve. Rostral auricular branches course through the parotid gland and are distributed to the rostral auricular muscles. The auriculopalpebral nerve crosses the zygomatic arch, supplies branches to the rostral auricular plexus, and continues to the orbit to supply palpebral branches to the orbicularis oculi. Beyond this, a branch passes medial to the orbit and continues rostrally on the nose to supply the muscles of the nose and upper lip.
Two buccal branches of the facial nerve course across the masseter muscle to innervate the muscles of the cheek, the upper and lower lip, and the lateral surface of the nose. The dorsal buccal branch lies above the parotid duct. The ventral buccal branch is below the parotid duct, near the ventral border of the masseter. Identify these two branches and the parotid duct.
A branch of the mandibular nerve from the trigeminal or fifth cranial nerve, known as the auriculotemporal nerve, is apparent in the dissection field of the auriculopalpebral branch of the facial nerve. The auriculotemporal nerve emerges between the caudal border of the masseter muscle and the base of the external acoustic meatus below the zygomatic arch. It may be found deep to the origin of the auriculopalpebral nerve. The auriculotemporal nerve supplies sensory branches to the skin of the external ear and the temporal, zygomatic, and masseteric regions.
Cervical Structures
The thyroid gland (Figs. 3-15, 5-42, 5-52) is dark colored and usually consists of two separate lobes lying lateral to the first five tracheal rings. Occasionally, a connecting isthmus is present.
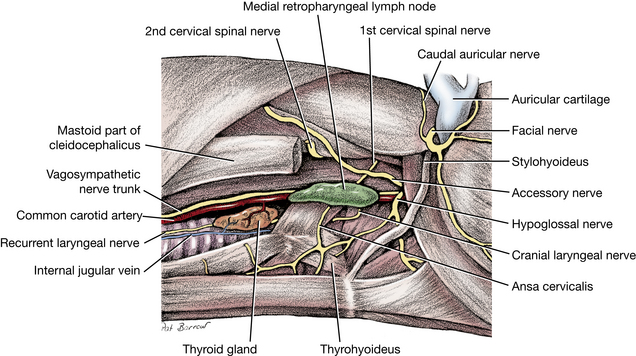
There are two parathyroid glands associated with each thyroid lobe. They are small, light-colored, spherical bodies. The external parathyroid most commonly lies in the fascia at the cranial pole of the thyroid lobe. It may be entirely separate from the thyroid tissue or embedded in the cranial pole of the thyroid external to its capsule. The internal parathyroid lies deep to the thyroid capsule on the medial aspect of the lobe. Occasionally, it is embedded in the parenchyma of the thyroid and is difficult to locate. The location of these glands is subject to variation.
The cervical portion of the esophagus extends from the laryngopharynx to the thoracic portion of the esophagus at the thoracic inlet. It begins opposite the middle of the axis dorsally and opposite the caudal border of the cricoid cartilage ventrally. A plicated ridge of mucosa, the pharyngoesophageal limen, marks the boundary between the laryngopharynx and the esophagus (Fig. 5-24). The esophagus inclines to the left, so that at the thoracic inlet it usually lies to the left of the trachea (Fig. 3-15).
The trachea extends from a transverse plane through the middle of the axis to a plane between the fourth and fifth thoracic vertebrae. It is composed of approximately 35 C-shaped tracheal cartilages. They are open dorsally, and the space is bridged by the tracheal muscle.
Common Carotid Artery
On the right side, expose the common carotid artery in the carotid sheath and observe the following branches.
1. The caudal thyroid artery (Figs. 3-14, 3-16) has a variable origin from the major arterial branches in the thoracic inlet. It passes cranially on the trachea supplying the trachea, esophagus, and thyroid gland.
2. The cranial thyroid artery (Figs. 5-43, 5-45) arises from the ventral surface of the common carotid at the level of the larynx. It supplies the thyroid and parathyroid glands, the pharyngeal muscles, the laryngeal muscles and mucosa, the cervical parts of the trachea and esophagus, and the adjacent portions of the sternocephalicus and the mastoid part of the cleidocephalicus. Clean the origin of this vessel.
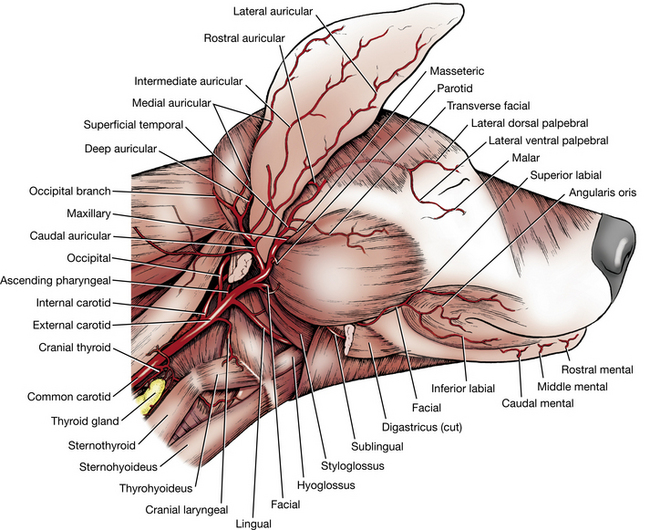
The large medial retropharyngeal lymph node (Fig. 5-42) is dorsal to the common carotid artery at the larynx and ventral to the wing of the atlas. Afferent vessels arise from the tongue, the nasal cavity, the pharynx, the salivary glands, the external ear, the larynx, and the esophagus. The tracheal trunk of each side arises from this lymph node.
Identify the internal and external carotid arteries, which are the terminal branches of the common carotid artery.
3. The internal carotid artery (Figs. 5-43, 5-45) is closely associated with the occipital artery, the first branch of the external carotid. A bulbous enlargement at the origin of the internal carotid artery is the carotid sinus, a baroreceptor. (The carotid body, a chemoreceptor, lies at the bifurcation of the carotid arteries.) Beyond this the internal carotid artery ascends across the lateral surface of the pharynx medial to the occipital artery. No branches leave the internal carotid in its extracranial course. It enters the carotid canal deep in the tympano-occipital fissure. The internal carotid passes rostrally through this canal and emerges at the foramen lacerum, where it loops back on itself to reenter the canal. It passes on to the floor of the cranial cavity and turns rostrally within the cavernous sinus. At the level of the attachment of the pituitary, it leaves the sinus dorsally and branches to form the cerebral arterial circle that supplies the brain. Its branches to the brain will be dissected later.
4. The external carotid artery (Figs. 5-43 through 5-45) passes cranially, medial to the digastricus. At the caudal border of the mandible, rostroventral to the annular cartilage of the ear, the vessel terminates by dividing into the superficial temporal and maxillary arteries. The maxillary is the direct continuation of the external carotid. Dissect the following branches of the external carotid. Transect the digastricus muscle and remove the caudal portion.
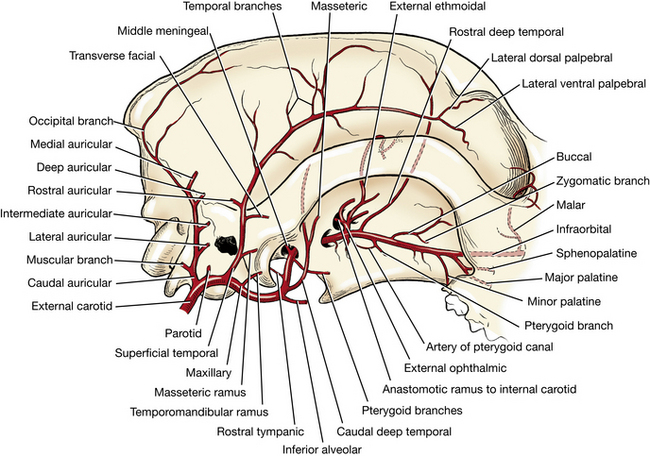
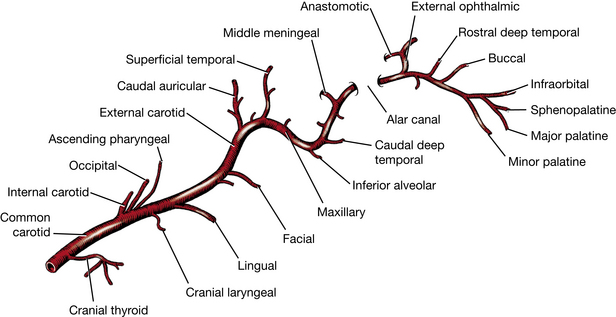
a. The occipital artery (Fig. 5-52) leaves the external carotid adjacent to the internal carotid and passes dorsally to supply the muscles on the caudal aspect of the skull and the meninges. Do not trace this artery.
b. The cranial laryngeal artery (Fig. 5-52) is a ventral branch that supplies the adjacent sternomastoideus and pharyngeal muscles. It enters the larynx between the thyrohyoid bone and the thyroid cartilage to supply the mucosa and laryngeal muscles.
c. The lingual artery (Figs. 5-39, 5-52) leaves the ventral surface of the external carotid and passes rostrally to supply the tonsil and tongue. On its course to the tongue it is accompanied by the hypoglossal nerve.
d. The facial artery (Fig. 5-39) leaves the external carotid beyond the lingual, medial to the digastricus. A branch, the sublingual artery, continues medial to the digastric muscle and is accompanied by the mylohyoid nerve. It runs rostrally into the tongue. The facial artery courses rostrolaterally between the digastric and masseter muscles to reach the cheek lateral to the mandible, where it supplies the lips and nose.
e. The caudal auricular artery usually arises from the external carotid at the base of the ear and courses dorsally under the caudal auricular muscles. Reflect the caudal limb of the parotid gland to expose the caudal auricular and its branches, which need not be dissected. Lateral, intermediate, and medial auricular branches course distally on the convex caudal surface of the ear. Occasionally, this artery arises closer to the origin of the external carotid.
f. The superficial temporal artery arises rostral to the base of the auricular cartilage at the caudodorsal border of the mandible and courses dorsally. It supplies the parotid gland, the masseter and temporal muscles, the rostral auricular muscles, and the eyelids.
g. The maxillary artery (Figs. 5-44, 5-45) is the larger terminal branch of the external carotid artery. It is deeply placed and is closely associated with a number of cranial nerves. From its origin with the superficial temporal, it passes rostromedially ventral to the temporomandibular joint medial to the retroarticular process in its course to the alar canal.
Remove the auricular muscles and reflect the ear caudally. Repeat the dissection that was done on the left side to expose the orbital structures. Cut through the origin of the temporal muscle along its margin. With a blunt instrument, remove it from the temporal fossa. Cut the attachments of the temporal and masseter muscles to both sides of the zygomatic arch. Sever the orbital ligament at the arch. With bone cutters or Stryker saw, detach each end of the zygomatic arch and remove all of it. Transect the temporal muscle as close to its insertion on the coronoid process as possible. Cut off the coronoid process below the level of the ventral border of the zygomatic arch with bone cutters. Remove all the temporal muscle to expose the periorbital tissues and the pterygoid muscles. Vessels and nerves entering the temporal muscle must be severed. Loosen the temporomandibular joint by forcing the articular end of the mandible medially. Rotate the mandible so that the stump of the coronoid process is forced laterally.
In the oral cavity, reflect the mucosa from the level of the root of the tongue to the frenulum along the sublingual fold.
Mandibular Nerve
The branches of the mandibular nerve from the trigeminal or fifth cranial nerve have been exposed by this dissection (Figs. 5-41, 5-46). The mandibular nerve leaves the cranial cavity through the oval foramen (Fig. 5-47). Branches arise on the surface of the pterygoid muscles ventral and lateral to the apex of the periorbita. These include the pterygoid, deep temporal, and masseteric nerves that contain somatic motor neurons that innervate the muscles of mastication. Most of these branches have been severed by the dissection. The buccal nerve crosses the pterygoid muscles and enters the cheek lateral to the zygomatic salivary gland. Remove the zygomatic gland to get better exposure. This nerve is sensory to the mucosa and skin of the cheek.
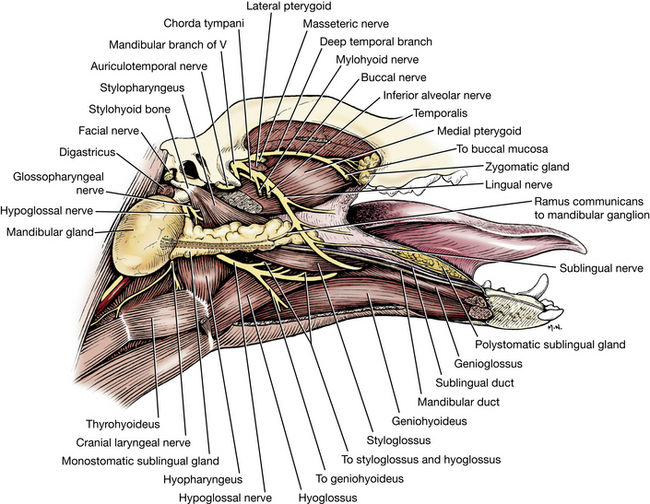
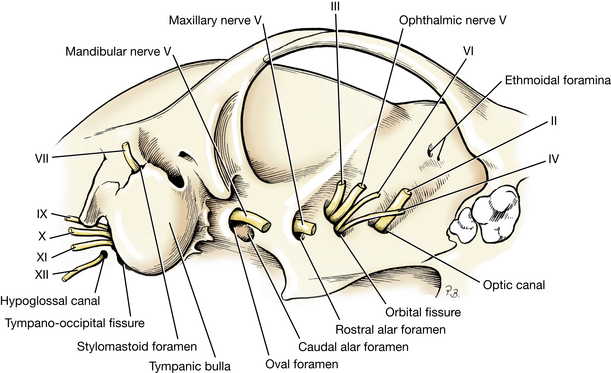
Rotate the stump of the coronoid process laterally to observe the lingual, inferior alveolar, and mylohyoid nerves, which cross the dorsal surface of the medial pterygoid muscle (Fig. 5-46).
The lingual nerve (sensory) is the largest and most rostral of the three. It can be observed coursing across the pterygoid muscles and passing between the styloglossus and mylohyoideus. On the medial side of the specimen, pull the tongue medially and observe the nerve between these muscles and the place where it crosses the lateral side of the mandibular and sublingual ducts and enters the tongue. It is sensory to the rostral two thirds of the tongue. Taste (SVA) is via the chorda tympani, a branch of cranial nerve VII.
The inferior alveolar nerve (sensory) enters the mandibular foramen on the medial side of the ramus of the mandible. It courses through the mandibular canal, supplying sensory nerves to the teeth. The mental nerves that emerge through the mental foramina and supply the lower lip are branches from this nerve.
The mylohyoid nerve (motor and sensory) is a caudal branch of the inferior alveolar. It reaches the ventral border of the mandible, supplies a branch to the rostral belly of the digastricus muscle, and continues into the mylohyoid muscle. Observe this nerve emerging on the medial side of the angle of the mandible lateral to the mylohyoideus. It is motor to the mylohyoideus and sensory to the skin between the mandibles.
The auriculotemporal nerve (sensory) leaves the mandibular nerve at the oval foramen, passes caudal to the retroarticular process of the temporal bone, and emerges between the base of the auricular cartilage and the masseter muscle, where it was previously seen.
Maxillary Artery
Complete the disarticulation of the temporomandibular joint and remove the lateral pterygoid muscle. Reflect the ramus of the mandible laterally and identify the following branches of the maxillary artery (Figs. 5-44, 5-45, 5-49). The first three arise before the maxillary artery enters the alar canal.
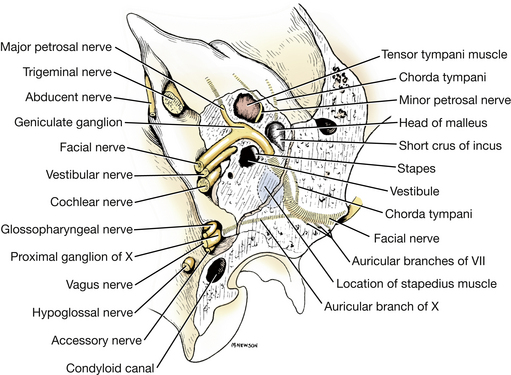
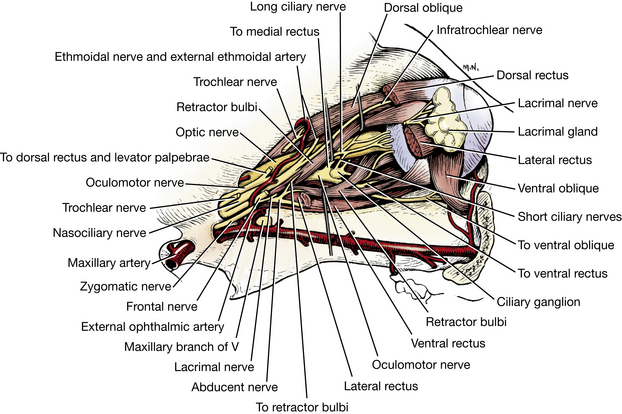
1. The inferior alveolar artery enters the mandibular foramen with the inferior alveolar nerve and courses through the mandibular canal. It supplies branches to the roots of the teeth in the lower jaw. Mental branches supply the skin (Fig. 5-43).
2. The caudal deep temporal artery arises near the inferior alveolar artery and enters the temporal muscle. Only the origin of this artery may be seen.
3. The middle meningeal artery (Fig. 5-50) passes through the oval foramen and courses dorsally in a groove on the inside of the calvaria. It will be followed in a later dissection to the dura over the cerebral hemispheres. Do not dissect its origin.
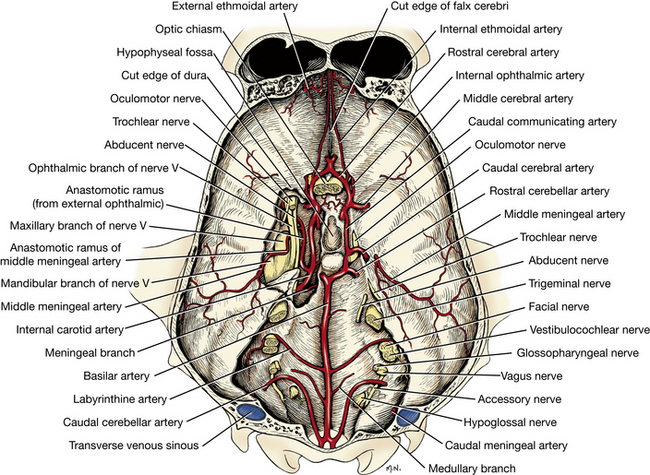
4. The external ophthalmic artery arises from the maxillary on its emergence from the alar canal and penetrates the apex of the periorbita adjacent to the orbital fissure. The external ophthalmic artery gives rise to the vessels that supply the structures within the periorbita. Incise the periorbita longitudinally along its dorsolateral border and reflect it.
The branches of the external ophthalmic artery need not be dissected. One anastomotic branch passes caudally through the orbital fissure to join the internal carotid and middle meningeal arteries within the cranial cavity. Another anastomotic branch joins the internal ophthalmic artery emerging from the optic canal on the optic nerve. From this anastomosis posterior ciliary arteries are supplied to the eyeball. Branches of the external ophthalmic artery supply the extrinsic muscles of the eyeball and the lacrimal gland. The external ethmoidal artery passes dorsal to the extraocular muscles and enters an ethmoidal foramen. Within the cranial cavity it joins with the internal ethmoidal artery and passes through the cribriform plate to the ethmoid labyrinth and the nasal septum.
5. Among the terminal branches of the maxillary artery are the minor and major palatine and sphenopalatine arteries. The latter two usually arise from the descending palatine artery as it courses rostroventrally over the medial pterygoid muscle. Only the origins of these vessels need be observed. Their origins can be seen at the rostral border of the medial pterygoid muscle deep to the zygomatic salivary gland, which should be removed.
The minor palatine artery passes ventrally, caudal to the hard palate, and is distributed to the adjacent soft and hard palates. Clean the mucosa from the palate just medial to the last molar and see the branches of this vessel.
The major palatine artery enters the caudal palatine foramen and passes through the major palatine canal to supply the hard palate.
The sphenopalatine artery passes through the sphenopalatine foramen to the interior of the nasal cavity.
6. The maxillary artery terminates as the infraorbital artery, which supplies the malar artery to the eyelids and dental branches to the caudal cheek teeth. The infraorbital artery enters the maxillary foramen and passes through the infraorbital canal. Within the canal, dental branches arise. These supply the premolars, the canine teeth, and the incisor teeth. The infraorbital artery emerges from the infraorbital foramen and terminates as the lateral and rostral dorsal nasal arteries, which supply the nose and the upper lip.
Cranial Nerves
There are 12 pairs of cranial nerves (Figs. 5-46 to 5-54). Each pair is both numbered with a roman numeral and named. The numbers indicate the rostrocaudal order in which they arise from the brain; their names are descriptive. Some of these have already been dissected; others will be dissected now.
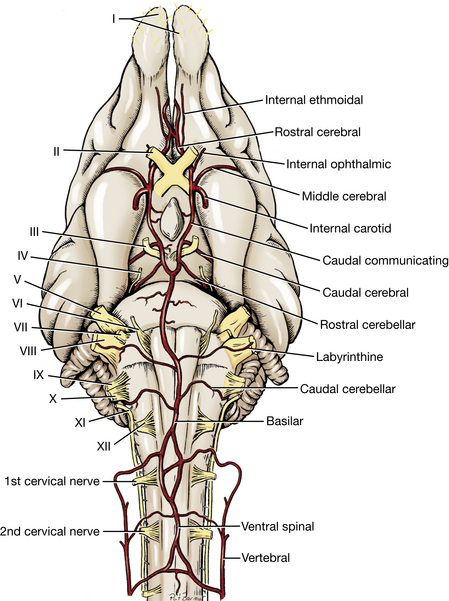
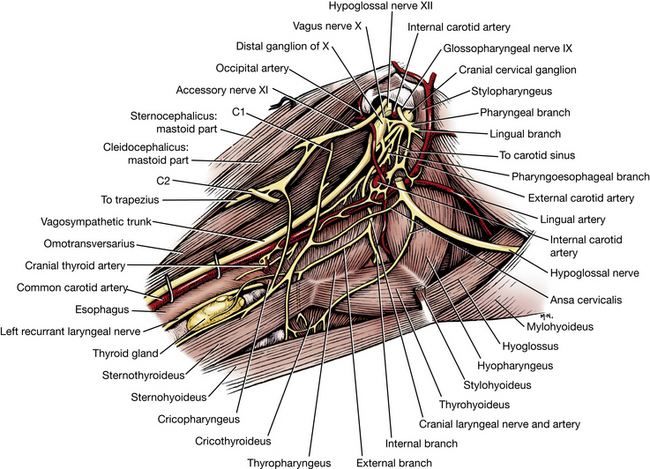
Fig. 5-52 Nerves emerging from tympano-occipital fissure, right lateral view. The digastricus muscle and the medial retropharyngeal lymph node were removed.
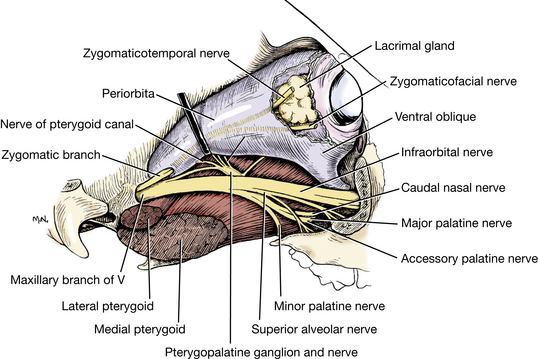
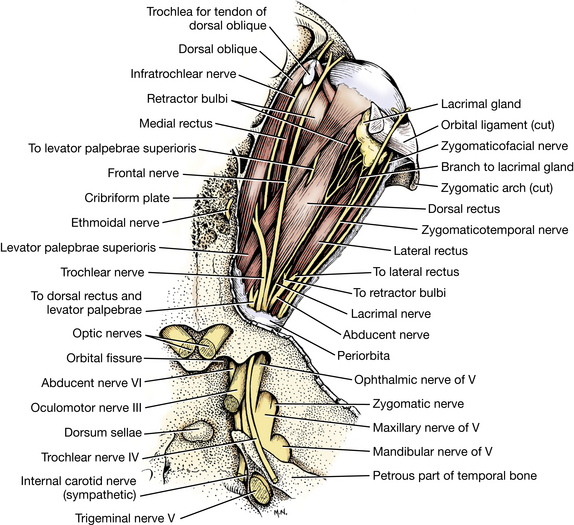
I The olfactory, or first cranial, nerve consists of numerous axons that arise in the olfactory epithelium of the caudal nasal mucosa and pass through the cribriform foramina to the olfactory bulbs. These include axons from the vomeronasal organ that course along the nasal septum. No dissection is necessary.
II The optic, or second cranial, nerve is surrounded by the retractor bulbi muscle within the periorbita. Observe the nerve in the periorbita and as it enters the optic canal. It is surrounded by an extension of meninges from the cranial cavity to the eyeball.
III The oculomotor, or third cranial, nerve passes through the orbital fissure and enters the periorbita with the optic nerve. Expose the proximal half of the optic nerve. Lift it gently and observe the oculomotor nerve on its lateroventral aspect. Do not dissect its individual branches. The oculomotor nerve innervates the dorsal, medial, and ventral rectus; the ventral oblique; and the levator palpebrae superioris. The ciliary ganglion is an irregular enlargement at the termination of the oculomotor nerve on the ventral surface of the middle of the optic nerve. This ganglion contains parasympathetic cell bodies of postganglionic axons that innervate the sphincter pupillae of the iris. It functions to regulate the size of the pupil in response to the amount of light entering the eye and in accommodation.
IV The trochlear, or fourth cranial, nerve enters the periorbita through the orbital fissure. It innervates the dorsal oblique; it need not be dissected.
V The trigeminal, or fifth cranial, nerve divides into three nerves as it emerges from the trigeminal canal in the petrosal part of the temporal bone: the ophthalmic, the maxillary, and the mandibular. The mandibular nerve has been dissected.
The ophthalmic nerve (sensory) passes through the orbital fissure and supplies sensory nerves that enter the periorbita. These need not be dissected. The frontal and infratrochlear nerves pass rostrally between the dorsal oblique and dorsal rectus muscles to innervate the medial aspect of the superior and inferior eyelids. Long ciliary nerves follow the optic nerve and innervate the eyeball. The ethmoidal nerve passes through an ethmoidal foramen and the cribriform plate to innervate the nasal mucosa and skin of the nose.
The maxillary nerve (sensory) enters the alar canal through the round foramen. It emerges from the rostral alar foramen and crosses the pterygopalatine fossa dorsal to the pterygoid muscles and ventral to the periorbita, accompanied by the maxillary artery.
a. The zygomatic nerve (sensory) here enters the periorbita and divides into two branches that pass rostrally on the inner surface of the lateral part of the periorbita to innervate the lacrimal gland and the lateral portion of the superior and inferior eyelids.
b. The pterygopalatine ganglion is dorsal to the maxillary nerve on the surface of the medial pterygoid muscle. It contains cell bodies of postganglionic parasympathetic axons that supply the lacrimal, nasal, and palatine glands. The postganglionic axons course with the branches of the maxillary nerve to their terminations. Reflect the periorbita dorsally and the maxillary nerve ventrally to see this small, flat ganglion on the pterygoid muscle.
c. The pterygopalatine nerve arises beyond the level of the pterygopalatine ganglion from the ventral surface of the maxillary nerve and divides into three nerves: the minor and major palatine nerves of the palate and the caudal nasal nerve of the nasal mucosa. Dissect their origin only.
d. The infraorbital nerve (sensory) is the continuation of the maxillary nerve in the pterygopalatine fossa. It enters the infraorbital canal through the maxillary foramen. Along its course through the infraorbital canal, it gives off superior alveolar branches, which supply the roots of the teeth of the superior arcade via the alveolar canals. As the infraorbital nerve emerges from the infraorbital foramen, it divides into a number of fasciculi, which are distributed to the skin and adjacent structures of the superior lip and nose. Dissect these branches as they emerge from the infraorbital foramen.
VI The abducent, or sixth cranial, nerve passes through the orbital fissure and enters the periorbita. It innervates the retractor bulbi and the lateral rectus. Observe this small nerve entering the dorsal border of the lateral rectus near its origin.
VII The facial, or seventh cranial, nerve enters the internal acoustic meatus of the petrosal part of the temporal bone. It courses through the facial canal and emerges through the stylomastoid foramen, where its motor branches to the facial muscles have been dissected.
VIII The vestibulocochlear, or eighth cranial, nerve enters the internal acoustic meatus and terminates in the membranous labyrinth of the inner ear. It is the nerve involved in balance and hearing. It will be dissected with the brain.
Observation of the ninth, tenth, and eleventh cranial nerves and the sympathetic trunk ganglion at the base of the skull is facilitated by removal of the origin of the digastricus muscle for a lateral view. Likewise, removal of the insertion of the longus capitis muscle provides a medial view. These neural structures are found just medial and ventral to the tympanic bulla near the tympano-occipital fissure.
Locate the sympathetic trunk where it is joined with the vagus. Follow it cranially to a level ventral and medial to the tympanic bulla, where the two nerves separate. The sympathetic trunk is ventral to the vagus. The distal ganglion of the vagus (sensory) is located dorsal to this separation and caudal to the cranial cervical ganglion. Trace the sympathetic trunk cranial to the separation and note an enlargement, the cranial cervical ganglion (visceral motor). This is the most cranial group of cell bodies of sympathetic postganglionic axons. These axons are distributed to the smooth muscles and glands of the head via blood vessels and other nerves. On the lateral side, observe the internal carotid artery coursing dorsocranially over the lateral surface of the cranial cervical ganglion. Notice the dense plexus that these nerves form in the immediate vicinity of the ganglion.
IX The glossopharyngeal, or ninth cranial, nerve passes through the jugular foramen and the tympano-occipital fissure. Beyond the fissure the glossopharyngeal crosses the lateral surface of the cranial cervical ganglion and divides into pharyngeal and lingual branches that are sensory to the pharyngeal mucosa and motor to the stylopharyngeus and other pharyngeal muscles. In addition, some branches course to the carotid sinus and others contribute to the pharyngeal plexus along with branches of the vagus nerve. Observe the nerve where it crosses the ganglion.
X The vagus, or tenth cranial, nerve passes through the jugular foramen and the tympano-occipital fissure. It courses along the common carotid artery in the neck with the sympathetic trunk and through the thorax on the esophagus to terminal branches in the thorax and abdomen (which have already been dissected).
There are two ganglia associated with this nerve. The proximal ganglion (Fig. 5-48) of the vagus lies in the jugular foramen and cannot be seen. The distal ganglion of the vagus is found outside the tympano-occipital fissure, ventral and medial to the tympanic bulla and caudal to the cranial cervical ganglion (Fig. 5-52). These are sensory ganglia. Find the distal ganglion with the vagus nerve caudal to the cranial cervical ganglion on the sympathetic trunk. The distal ganglion contains the cell bodies of the visceral afferent neurons that are distributed to most of the viscera of the body. Caudal to the distal ganglion, the vagus joins the sympathetic trunk, with which it remains associated throughout its cervical course to the thoracic inlet. The following branches are distributed to cranial cervical structures.
Branches from the vagus and glossopharyngeal nerves and the cranial cervical ganglion form a pharyngeal plexus, which innervates the caudal pharyngeal muscles and the cranial esophagus. The cranial laryngeal nerve leaves the vagus nerve at the distal ganglion and passes ventrally to the larynx, where it supplies the cricothyroid muscle and the laryngeal mucosa. Identify this nerve. The origin of the recurrent laryngeal nerve was seen in the thoracic inlet. It innervates the cervical esophagus and trachea in its course up the neck and terminates as the caudal laryngeal nerve, which enters the larynx under the caudal edge of the cricopharyngeus muscle. It innervates all the muscles of the larynx except the cricothyroideus.
XI The accessory, or eleventh cranial, nerve passes through the jugular foramen and the tympano-occipital fissure along with the ninth and tenth cranial nerves. It passes caudally and by a ventral branch innervates the mastoid part of the sternocephalicus and cleidocephalicus muscles. The dorsal branch supplies the cervical part of the cleidocephalicus and the trapezius.
XII The hypoglossal, or twelfth cranial, nerve passes through the hypoglossal canal. It passes ventrorostrally, lateral to the vagosympathetic trunk and the carotid arteries. It lies medial to the mandibular salivary gland, digastricus, and mandible. The hypoglossal nerve is closely associated with the lingual artery. Deep to the mylohyoideus, it innervates the extrinsic and intrinsic muscles of the tongue. The ansa cervicalis (Figs. 5-42, 5-52) leaves the hypoglossal nerve to join the first cervical spinal nerve, before rejoining the hypoglossal nerve in the region of the hyoid muscles.
LIVE DOG
Examine the lips and cheeks and the vestibule they border. Examine the teeth of both arcades. Evert the caudal part of the superior lip and find the opening of the parotid duct at the level of the fourth superior premolar. Try to feel the parotid duct through the platysma as the duct crosses the middle of the masseter muscle. Palpate the ventral portion of the external acoustic meatus. This is covered by the parotid salivary gland, but the gland is difficult to feel. Palpate the firm ovoid mandibular salivary gland ventral to the parotid. The monostomatic sublingual gland is at the rostral end of the mandible but cannot be identified by palpation. Open the mouth and examine the oral cavity. Observe the frenulum of the tongue and the sublingual caruncle where the mandibular and sublingual salivary ducts open. Examine the surface of the body and apex of the tongue. Recognize and feel the filiform papillae. Observe the prominent lingual vein on the ventral surface. In the anesthetized dog, this vein can be used for intravenous injections. Pull the tongue to one side to see the palatoglossal arch where the oral cavity is continued by the oropharynx. Pull the tongue forward and see the root of the tongue in the floor of the oropharynx, the epiglottis caudal to it, the palatine tonsils partly covered by the semilunar folds on each side of the oropharynx, and the soft palate dorsally.
Observe the philtrum on the nose. Feel the cartilaginous parts of the nose rostral to the incisive and nasal bones. Palpate the infraorbital foramen where the infraorbital nerve can be anesthetized with a local nerve block. Touch the lateral angle of the eyelids and observe the reflex closure of the palpebral fissure: sensory V and motor VII.
Examine the eyelids and observe the caruncle at the medial commissure. Evert the eyelids slightly and look for the lacrimal puncta along their borders near the medial commissure. Consider lacrimal flow from its origin at the lacrimal gland, across the cornea and along the conjunctival sacs, and through its collecting system to the ventral meatus, where it is usually evaporated. Observe the margin of the third eyelid. Gently press the eyeball caudally into the periorbita in the orbit by pushing on it through the superior eyelid. Observe the passive protrusion of the third eyelid across the cornea. Recognize the palpebral and bulbar conjunctivae, the sclera, limbus, cornea, iris, pupil, and anterior chamber. Move the head side to side to stimulate the vestibular part of the vestibulocochlear nerve (VIII) and watch the involuntary quick horizontal movements of the eyeballs. The quick adduction toward the nose is a function of the medial rectus and its oculomotor (III) nerve innervation. The quick abduction away from the nose is a function of the lateral rectus and its abducent (VI) nerve innervation. Palpate along zygomatic arch and try to feel the palpebral branch of the auriculopalpebral (VII) nerve where it crosses the arch to innervate the orbicularis oculi.
Palpate the temporal and masseter muscles above and below the zygomatic arch, respectively. Palpate caudal and ventral to the masseter to feel the digastricus.
Palpate the scutiform cartilage in the auricular muscles medial to the external ear. Examine the external ear. Follow the helix and identify the cutaneous pouch laterally. At the opening into the external acoustic meatus, identify the crura of the helix medially, the pretragic incisure, the tragus rostrally, the intertragic incisure, and the antitragus laterally. Recognize the anthelix on the caudal wall of the external acoustic meatus opposite the tragus.
Palpate the trachea from the thoracic inlet to the larynx. Feel the cricoid and thyroid cartilages of the larynx. Palpate the basihyoid bone and try to feel the other hyoid bones. Normally, the thyroid gland and medial retropharyngeal lymph node cannot be palpated. Palpate the small flat subcutaneous mandibular lymph nodes at the angle of the mandible.