The Skeletal and Muscular Systems
Superficial Structures of the Thorax
Extrinsic Muscles of the Thoracic Limb and Related Structures
Intrinsic Muscles of the Thoracic Limb
Lateral Muscles of the Scapula and Shoulder
Medial Muscles of the Scapula and Shoulder
BONES OF THE VERTEBRAL COLUMN AND THORAX
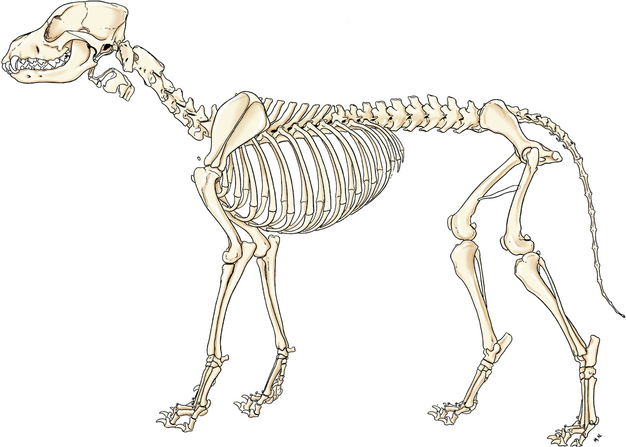
Before dissection of muscles is explained, the bones of that region (Fig. 2-1) are described. A thorough understanding of the relationships of muscles and bones facilitates learning the muscular attachments and functions.
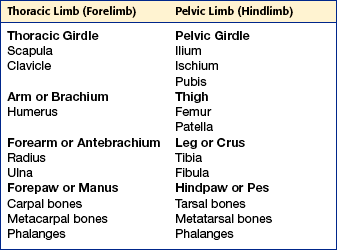
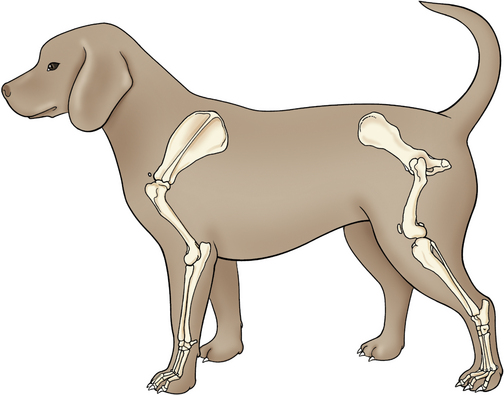
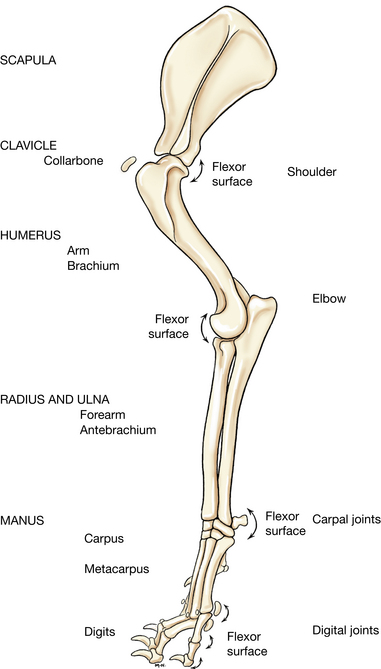
The appendicular skeleton includes the bones of the thoracic girdle and forelimbs and the pelvic girdle and hind limbs (Table 2-1, Fig. 2-2).
The axial skeleton consists of the bones of the skull; hyoid apparatus; cartilages of the larynx; and bones of the vertebral column, ribs, and sternum.
BONES OF THE THORACIC LIMB
The thoracic girdle consists of paired scapulae and clavicles (Fig. 2-10). The scapula is large, whereas the clavicle is reduced. The dog’s clavicle (Fig. 2-10) is a small oval plate located cranial to the shoulder within the clavicular tendon in the brachiocephalicus muscle (Fig. 2-12). The clavicle is one of the first bones to show a center of ossification in the fetal dog, but in the adult it is partly or completely cartilaginous. It is frequently visible in dorsoventral radiographs of the trunk, medial to the shoulder joint.
Scapula
The scapula (Figs. 2-3 and 2-4), a flat, roughly triangular bone, possesses two surfaces, three borders, and three angles. The ventral angle is the distal or articular end that forms the glenoid cavity, and the constricted part that unites with the expanded blade is referred to as the neck.
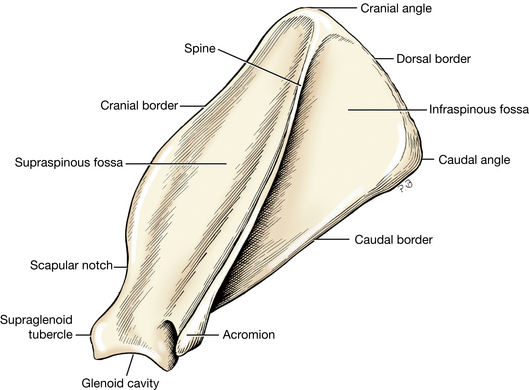
The lateral surface (Fig. 2-3) of the scapula is divided into two nearly equal fossae by a shelf of bone, the spine of the scapula. The spine is the most prominent feature of the bone. It begins at the dorsal border as a thick, low ridge and becomes thinner and wider toward the neck. In all breeds the free border is slightly thickened, and in some it is everted caudally. The distal end is a truncated process, the acromion, where part of the deltoideus muscle arises. On a continuation of the spine proximally, the omotransversarius attaches. The remaining part of the spine provides a place for insertion of the trapezius and for origin of that part of the deltoideus that does not arise from the acromion.
The supraspinous fossa is the entire lateral surface cranial to the spine of the scapula. The supraspinatus arises from all but the distal part of this fossa.
The infraspinous fossa, caudal to the spine, is triangular, with the apex at the neck. The infraspinatus arises from the infraspinous fossa.
The medial or costal surface has two areas. A small proximal and cranial rectangular area, the serrated face, serves as insertion for the serratus ventralis muscle. The large remaining part of the costal surface is the subscapular fossa, which is nearly flat and usually presents three straight muscular lines that converge distally. The subscapularis arises from the whole subscapular fossa.
The cranial border of the scapula is thin. Near the ventral angle the border is concave as it enters into the formation of the neck. The notch thus formed is the scapular notch. The dorsal end of the cranial border thickens and, without definite demarcation at the cranial angle, is continuous with the dorsal border.
The dorsal border extends from the cranial to the caudal angles. In life it is capped by a narrow band of cartilage, but in the dried specimen the cartilage is destroyed by ordinary preparation methods. The rhomboideus attaches to this border.
Just proximal to the ventral angle, the thick caudal border bears the infraglenoid tubercle, from which arise the teres minor and the long head of the triceps. The middle third of the caudal border of the scapula is broad and smooth; part of the subscapularis and the long head of the triceps arise from it. Somewhat less than a third of the dorsal segment of the caudal border is thick and gives rise to the teres major.
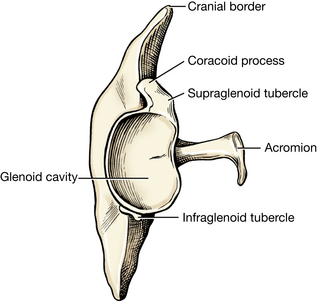
The ventral angle forms the expanded distal end of the scapula. The adjacent constricted part, the neck, is the segment of the scapula distal to the spine and proximal to the expanded part of the bone that forms the glenoid cavity. Clinically, the ventral angle is by far the most important part of the scapula, because it enters into the formation of the shoulder joint. The glenoid cavity articulates with the head of the humerus. Observe the shallowness of the cavity.
The supraglenoid tubercle is an eminence at the cranial part of the glenoid cavity. The tubercle shows a slight medial inclination on which a small tubercle, the coracoid process, can be distinguished. The coracobrachialis arises from the coracoid process, whereas the biceps brachii arises from the supraglenoid tubercle.
LIVE DOG
Palpate the borders of the scapula, spine, acromion, and supraglenoid tubercle.
Humerus
The humerus (Fig. 2-5) is located in the arm, or brachium. This bone enters into the formation of both the shoulder joint and the elbow joint. The shoulder joint is formed by the articulation of the scapula and humerus; the elbow joint is formed by the articulation of the radius and ulna with each other and with the humerus. The proximal extremity of the humerus includes the head, neck, and the greater and lesser tubercles. The distal extremity, the condyle, includes the trochlea, capitulum, and the radial and olecranon fossae, which communicate proximal to the trochlea through the supratrochlear foramen. The medial and lateral epicondyles are situated on the sides of the condyle. The body of the humerus lies between the two extremities.
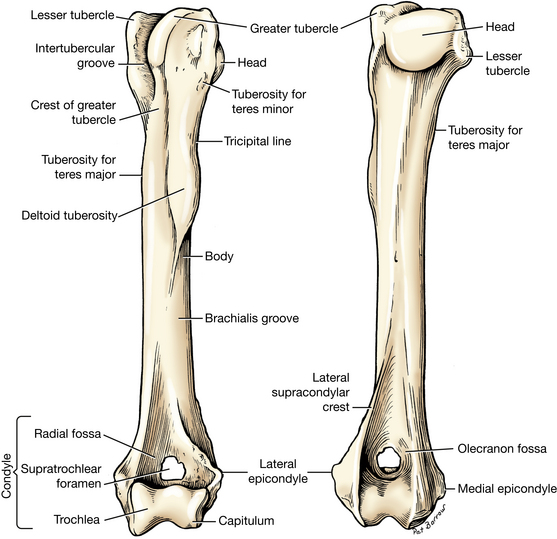
The head of the humerus is the part that articulates with the scapula. It presents more than twice the area of the glenoid cavity of the scapula and is elongated sagittally. Although the shoulder joint is a typical ball-and-socket joint, it normally undergoes only flexion and extension. The intertubercular groove begins at the cranial end of the articular area. It lodges the tendon of origin of the biceps brachii and is deflected toward the median plane by the greater tubercle, which forms the craniolateral part of the proximal extremity. The greater tubercle is convex at its summit and, in most breeds, higher than the head. It is continued distally in the body of the humerus by the crest of the greater tubercle. The greater tubercle receives the insertions of the supraspinatus and the infraspinatus and part of the deep pectoral. Between the head of the humerus and the greater tubercle are several foramina for the transmission of vessels. The infraspinatus is inserted on the smooth facet on the lateral side of the greater tubercle. The lesser tubercle lies on the medial side of the proximal extremity of the humerus, caudal to the intertubercular groove. It is not as high or as large as the greater tubercle. The subscapularis attaches to its proximal border. The neck of the humerus is not distinct except caudally. It is the line along which the head and parts of the tubercles have fused with the body.
The cranial surface of the humerus is distinct in the middle third of the body, where it furnishes attachment for the brachiocephalicus and part of the pectorals. Distally it fades but may be considered to continue to the medial lip of the trochlea. On the proximal third of the cranial border are two ridges. They continue to the cranial and caudal parts of the greater tubercle. The ridge that extends proximally in a craniomedial direction is the crest of the greater tubercle and is also the cranial border of the bone. This forms part of the area of insertion of the pectorals and the cleidobrachialis.
The ridge extending to the caudal part of the greater tubercle is on the lateral surface of the humerus. Distally it is thickened to form the deltoid tuberosity. The deltoideus inserts here. From this tuberosity to the caudal part of the greater tubercle, the ridge forms the prominent tricipital line. The lateral head of the triceps arises from this line. The teres minor inserts on the tuberosity of the teres minor adjacent to the proximal extremity of the tricipital line. The smooth brachialis groove is on the lateral surface of the body. The brachialis, which originates in the proximal part of the groove, spirals around the bone in the groove so that distally it lies on the craniolateral surface. Distal to this groove is the thick lateral supracondylar crest. The extensor carpi radialis and part of the anconeus attach here. The crest extends distally to the lateral epicondyle.
The caudal surface is smooth and rounded transversely and ends in the deep olecranon fossa.
The crest of the lesser tubercle crosses the proximal end of the medial surface and ends distally at the teres major tuberosity. The teres major and latissimus dorsi are inserted on this tuberosity. Caudal and proximal to this, the medial head of the triceps arises and the coracobrachialis is inserted. Approximately the middle third of the medial surface is free of muscular attachment and is smooth.
The distal end of the humerus, including its articular areas and the adjacent fossae, is the humeral condyle. The articular surface is divided unevenly by a low ridge. The large area medial to the ridge is the trochlea, which articulates with both the radius and the ulna and extends proximally into the adjacent fossae. The articulation with the trochlear notch of the ulna is one of the most stable hinge joints (ginglymus) in the body. The small articular area lateral to the ridge is the capitulum, which articulates only with the head of the radius.
The lateral epicondyle is smaller than the medial one and occupies the enlarged distolateral end of the humerus proximal to the capitulum. It gives origin to the common digital extensor, lateral digital extensor, ulnaris lateralis, and supinator. The lateral collateral ligament of the elbow also attaches here. The lateral supracondylar crest extends proximally from this epicondyle and is the origin for the extensor carpi radialis.
The medial epicondyle is the enlarged distomedial end of the humerus proximal to the trochlea. Its caudal projection deepens the olecranon fossa. The anconeus arises from this projection. The elevated portion of the medial epicondyle serves as origin for flexor carpi radialis, flexor carpi ulnaris, pronator teres, and the superficial and deep digital flexor muscles. The medial collateral ligament of the elbow also attaches here.
The olecranon fossa is a deep excavation of the caudal part of the humeral condyle. It receives the anconeal process of the ulna during extension of the elbow. On the cranial surface of the humeral condyle is the radial fossa, which communicates with the olecranon fossa by an opening, the supratrochlear foramen. No soft structures pass through this foramen.
Radius
The radius and ulna are the bones of the antebrachium, or forearm. It is important to know that they cross each other obliquely so that the proximal end of the ulna is medial and the distal end is lateral to the radius. The radius (Fig. 2-6), the shorter of the two bones of the forearm, articulates proximally with the humerus and distally with the carpus. It also articulates with the ulna, proximally by its caudal surface and distally near its lateral border.
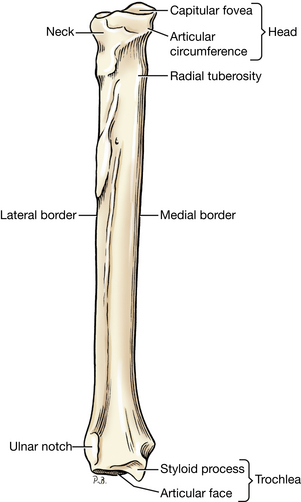
The proximal extremity consists of head, neck, and tuberosity. The head of the radius, like the whole bone, is widest medial to lateral. It forms proximally an oval, depressed articular surface, the fovea capitis, which articulates with the capitulum of the humerus. The smooth caudal border of the head is the articular circumference for articulation with the radial notch of the ulna. The small radial tuberosity lies distal to the neck on the medial border of the bone. The biceps brachii and brachialis insert in part on this tubercle.
The body of the radius is compressed so that it possesses cranial and caudal surfaces and medial and lateral borders. It is slightly convex cranially. At the carpal end, the body blends without sharp demarcation with the enlarged distal extremity. The caudal surface of the radius is roughened and slightly concave. It has a ligamentous attachment to the ulna. Distally it broadens and becomes the expanded caudal surface of the distal extremity. The cranial surface of the radius, convex transversely, is relatively smooth throughout.
The distal extremity of the radius is the trochlea. Its carpal articular surface is concave. On the lateral surface of the distal extremity is the ulnar notch, a slightly concave area with a facet for articulation with the ulna. The medial surface of the distal extremity ends in a rounded projection, the styloid process. The medial collateral ligament of the carpus attaches proximal to the styloid process. The cranial surface of the distal extremity presents three distinct grooves. The most medial groove, which is small, short, and oblique, contains the tendon of the abductor digiti I longus. The middle and longest groove, extending proximally on the shaft of the radius, is for the extensor carpi radialis. The most lateral of the grooves on this surface is wide and of variable distinctness. It contains the tendon of the common digital extensor.
Ulna
The ulna (Fig. 2-7) is located in the caudal part of the forearm. It exceeds the radius in length and is irregular in shape and generally tapers from its proximal to its distal end. Proximally the ulna is medial to the radius and articulates with the trochlea of the humerus by the trochlear notch and with the articular circumference of the radius by the radial notch. This forms the elbow. Distally the ulna is lateral and articulates with the radius medially and with the ulnar and accessory carpal bones distally.
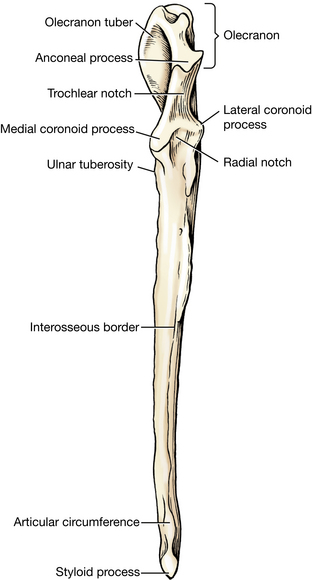
The proximal extremity is the olecranon, which includes the olecranon tuber and the anconeal process. It serves as a lever arm for the extensor muscles of the elbow. It is four sided, laterally compressed, and medially inclined. Its proximal end, the olecranon tuber, is grooved cranially and enlarged and rounded caudally. The triceps brachii, anconeus, and tensor fasciae antebrachii attach to the caudal part of the olecranon. The ulnar portions of the flexor carpi ulnaris and deep digital flexor arise from its medial surface.
The trochlear notch is a smooth, vertical, half-moon–shaped concavity facing cranially. The whole trochlear notch articulates with the trochlea of the humerus. At its proximal end a sharp-edged, slightly hooked anconeal process fits into the olecranon fossa of the humerus when the elbow joint is extended. At the distal end of the notch are the medial and lateral coronoid processes, which articulate with the humerus and radius. The medial coronoid process is larger. Between these processes is the radial notch for articulation with the articular circumference of the radius.
The body of the ulna is three sided in its middle third; proximal to this the bone is compressed laterally, whereas the distal third gradually loses its borders, becomes irregular, and is continued by the pointed distal extremity. The ulnar tuberosity is a small, elongated eminence on the medial surface of the bone at its proximal end, just distal to the medial coronoid process. The biceps brachii and the brachialis insert on this eminence. The interosseous border is distinct, rough, and irregular, especially at the junction of the proximal and middle thirds of the bone, where a large, expansive, but low eminence is found. This eminence indicates the place of articulation with the radius by means of a heavy ligament. Frequently, a vascular groove medial to the crest marks the position of the caudal interosseous artery. This groove is most conspicuous in the middle third of the ulna. The body shows a distinct caudal concavity.
The distal extremity of the ulna is the head with its prominent styloid process. A part of this process articulates with the ulnar and accessory carpal bones. The head articulates medially with the radius.
Carpal Bones
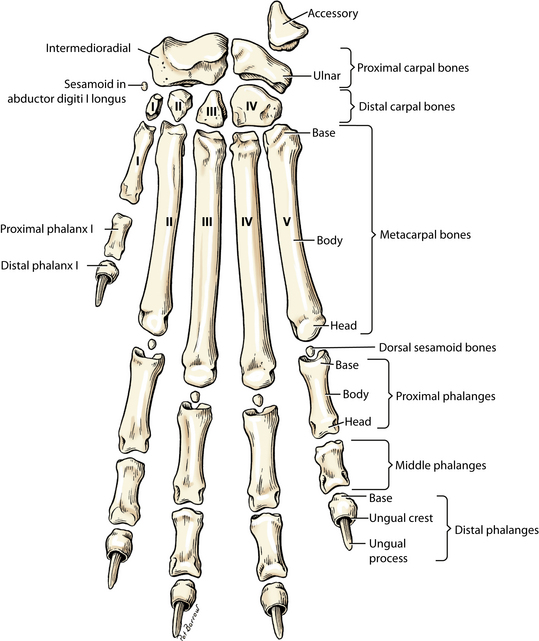
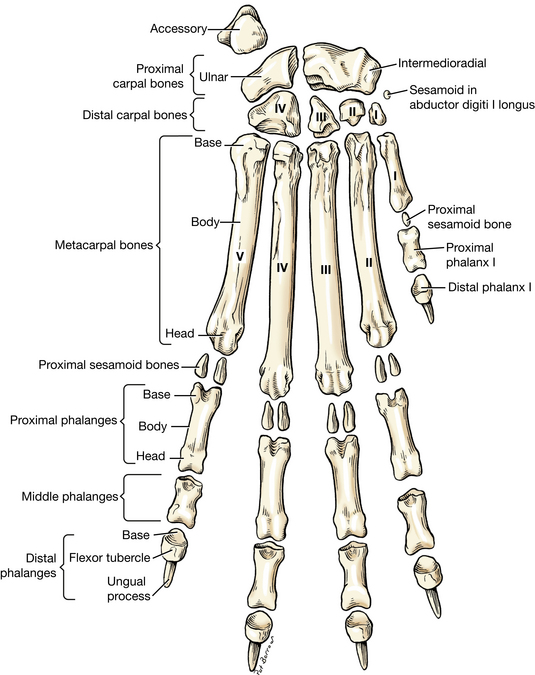
The term carpus (Figs. 2-8 to 2-10) is used to designate that part of the extremity between the antebrachium and metacarpus that includes all the soft structures as well as the bones. The carpus includes seven small, short irregular bones arranged into two rows. These are most conveniently studied on radiographs. The proximal row contains three bones. The largest of these, the intermedioradial carpal (often referred to as the radial carpal), is on the medial side and articulates proximally with the radius. The ulnar carpal is the lateral member of the proximal row. Its palmar portion projects distally palmar and lateral to the fourth carpal bone. The accessory carpal, the palmar member, is a short rod of bone that articulates with the styloid process of the ulna and the ulnar carpal bone and serves as a lever arm for some of the flexor muscles of the carpus. The distal row consists of four bones numbered from the medial to the lateral side. From the smallest on the medial side, these are the first, second, third, and fourth carpal bones. The fourth carpal bone is the largest and articulates with the base of the fourth and fifth metacarpals.
Metacarpal Bones
The metacarpus (Figs. 2-8 and 2-9) contains five bones. The metacarpal bones are long bones in miniature, possessing a slender body, or shaft, and large extremities. The proximal extremity is the base, and the distal one is the head. The metacarpals, like the carpals and digits, are numbered from medial to lateral. Proximally all articulate principally with the corresponding carpal bones, except the fifth, which articulates with the fourth carpal. Distally all articulate with the corresponding proximal phalanges. Note the sagittal ridge on the head for articulation with the sagittal groove in the base of the corresponding proximal phalanx. The interosseous muscles largely fill the intermetacarpal spaces palmar to the metacarpal bones.
The first metacarpal bone is atypical. It is a vestigial structure, but unlike the first metatarsal bone in the hindpaw, it is constantly present.
Phalanges
In the forepaw there are three phalanges for each of the four main digits (Figs. 2-8 and 2-9); the first digit, or pollex, a dewclaw, has two phalanges. Each proximal and middle phalanx has a proximal base, a body, and a distal head.
On the distal phalanx, a thin shelf of bone, the ungual crest, overlaps the claw and forms a band of bone around the proximal portion of the claw. The ungual process is a curved conical extension of the distal phalanx into the claw. The rounded dorsal part of the base is the extensor process on which the common digital extensor tendon is inserted. A small process on the palmar surface is the flexor tubercle for insertion of the deep digital flexor tendon.
Two proximal sesamoid bones are located in the interosseous tendons on the palmar surface of each metacarpophalangeal joint (digits II–V). Four small dorsal sesamoid bones (none for the first digit) are embedded in the common digital extensor tendons as they pass over the metacarpophalangeal joints (Figs. 2-8 and 2-9).
LIVE DOG
Flex and extend the shoulder joint. Palpate the greater tubercle of the humerus. Follow its cranial part to the crest of the greater tubercle and cranial border of the humerus. Palpate the groove medial to the greater tubercle and its crest. Palpate the deltoid tuberosity on the lateral surface of the body and the epicondyles on the condyle of the humerus. Note the width of the condyle at the elbow and the more prominent medial epicondyle.
Because of the size of the medial epicondyle, most elbow joint separations (luxations) caused by injury result in the humerus being displaced medial to the ulna. Note that replacement would require flexion of the elbow to allow the anconeal process of the ulna to pass over the crest of the lateral epicondyle.
Flex and extend the elbow. Palpate the olecranon tubercle proximally, the head of the radius laterally, and the medial coronoid process of the ulna medially deep to the muscles. Note that the combined bones at the elbow are not as wide as the humeral condyle. Flex and extend the antebrachiocarpal joint and palpate the styloid process of the radius medially and ulna laterally.
Flex and extend the carpus. Note that the major motion is at the antebrachiocarpal joint. Palpate the accessory carpal. Palpate the metacarpals and phalanges and flex and extend the metacarpophalangeal and interphalangeal joints. Note that the flexor surface of the metacarpophalangeal joint is the palmar surface despite being the wider angle while bearing weight. Note the relationship of the metacarpal pad to the metacarpophalangeal joints and the digital pads to the distal interphalangeal joints.
MUSCLES OF THE THORACIC LIMB
Superficial Structures of the Thorax
General study of the ventral surface of the trunk should be made before the dissection of the thoracic region is begun. Find the umbilicus. This is represented by a scar that may be either flat or slightly raised and is located on the midventral line, one third to one fourth of the distance from the xiphoid cartilage to the scrotum or vulva. In most dogs it is hidden by hair. The umbilicus is irregularly oval and may be from a few millimeters to a centimeter in length. The umbilicus serves as a landmark in abdominal surgery. Notice that the hair over a large area around the umbilicus slants toward it, thus forming a vortex.
Pick up a fold of skin, or common integument, which consists of an outer thin epithelium, the epidermis, and an underlying thicker layer of connective tissue, the dermis. Skin thickness varies on different parts of the body, depending on the extent of the dermis. Notice that the skin is thickest in the neck region, thinner over the sternum, and thinnest on the ventral surface of the abdomen; also notice that the skin of the dorsum of the neck and thorax is loosely attached.
The mammae vary in number from 8 to 12, but 10 is average. They are situated in two rows, usually opposite each other. The number is usually reduced in the smaller breeds.
When 10 glands are present, the cranial four are the thoracic mammae, the following four are the abdominal mammae, and the caudal two are the inguinal mammae. When the abdominal and inguinal mammae are maximally developed, the glandular tissue in each row appears to form a continuous mass. The mammae lie in areolar connective tissue and are not fused to the body wall. The cranial pair of thoracic mammae are smaller than the other pair. Each mamma has a papilla, or nipple, that is partly hairless and contains about 12 openings, but these vary and are difficult to see if the animal is not lactating.
The costal cartilages of the tenth, eleventh, and twelfth ribs unite with each other to form the costal arch. Palpate this arch and the caudal border and free end of the last or thirteenth rib. This rib does not attach to the costal arch and is therefore called a “floating rib.”
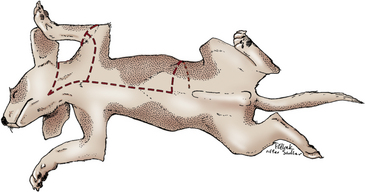
Make a midventral incision through the skin only from the cranial end of the neck to the umbilicus (Fig. 2-11). From the umbilicus extend a transverse incision to the mid-dorsal line on the left side. From a point on the midventral incision directly opposite the arm, extend a transverse incision to the left elbow. Make a complete circular incision through the skin around the elbow. Extend a third transverse incision from the cranial end of the midventral incision to the mid-dorsal line on the left side. This should pass just caudal to the ear. Carefully reflect the skin of the thorax and neck to the mid-dorsal line. The skin will be intimately fused with the thin underlying cutaneous muscle over the neck, thorax, and abdomen. The muscle should be left on the specimen as far as is possible.
The subcutaneous tissue that now confronts the dissector is composed of areolar tissue and fascia. Areolar tissue appears as a thin layer of loose, irregularly arranged connective tissue that often contains fat. Fascia is a denser, more regularly arranged thin layer of connective tissue. It is more fibrous, and it envelops the body beneath the skin and encloses individual muscles or groups of muscles. The superficial fascia is deep to the areolar tissue, forming the deep portion of the subcutaneous tissue that covers the entire body. It blends with the deep fascia, which is more firmly attached to the muscle that it encloses. These are not always easily distinguished from each other. The areolar tissue is often distended with embalming fluid. (Clinical subcutaneous injections are made into this tissue.) When the fatty areolar tissue and fascia with vessels and nerves are removed from a muscle, the muscle is said to be “cleaned.”
All muscles have attachments. In most instances the more proximal attachment, the part that moves the least, is considered the origin. The insertion is the more distal attachment, or the part that moves the most. The origin is usually a direct attachment of the muscle cells to the bone. The insertion often is by a tendon or aponeurosis extending from the muscle cells to the bone. A tendon consists of dense, regularly arranged fibrous connective tissue organized into a small, well-defined bundle. An aponeurosis has the same consistency as a tendon, but the fibrous tissue is arranged as a thin sheet of tissue. A ligament is dense fibrous connective tissue between bones, although the term is also used for a variety of thin fibrous connections between organs or between an organ and the body wall.
Read before you dissect! In many instances, during the study of muscles, a description of a specific muscle will be given before the instructions for dissection. At no time should muscles be removed or even transected without instructions. In each instance clean the exposed surface of the muscle being described, isolate its borders, and verify its origin and insertion. If the muscle is to be “transected,” free it from underlying structures first. As each muscle is defined, visualize its attachments and position on the skeleton and understand its function.
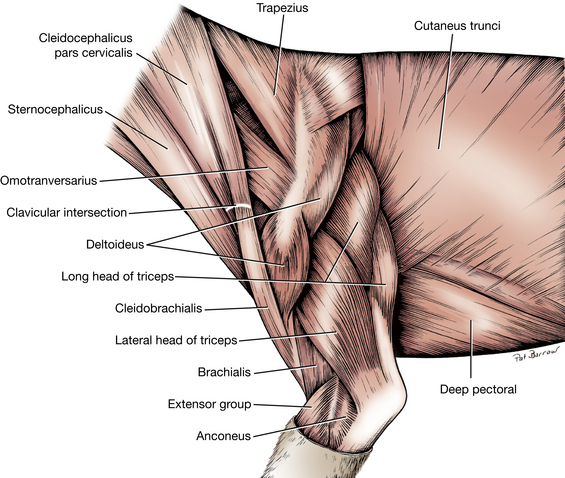
The cutaneus trunci (Figs. 2-15 and 2-17) is a thin sheet of muscle that covers most of the dorsal, lateral, and ventral walls of the thorax and abdomen. It has no direct bony attachments. It is more closely applied to the skin than to underlying structures and is often reflected with the skin before being observed. Like all cutaneous muscles, it is developed in the superficial fascia of the thorax and abdomen. Caudal to the shoulder the fibers sweep obliquely toward the axilla; farther caudally they are principally longitudinal and arise from the superficial fascia over the pelvic region.
The attachments of the cutaneus trunci are the superficial fascia of the trunk and the skin. The muscle sends a fasciculus to the medial side of the forelimb; caudal and ventral to this the fibers fray out over the deep pectoral muscle. The cutaneus trunci twitches the skin. It is innervated by the lateral thoracic nerve. In the male dog there is a distinct development of this muscle adjacent to the ventral midline caudal to the xiphoid. This is the preputial muscle, which passes caudally and radiates into the prepuce, forming an arch with the muscle of the opposite side. It functions to support the cranial end of the prepuce during the nonerect state and to pull the prepuce back over the glans penis after erection and protrusion.
Sever the axillary and ventral attachments of the cutaneus trunci and reflect it dorsally. Caution: Beneath the thin cutaneus trunci is the thicker latissimus dorsi muscle, which should be left in place on the lateral side of the trunk.
LIVE DOG
Grasp the skin in several areas and note the variation in thickness. Note where it is especially loose and suitable for subcutaneous injections of fluids. Pinch the skin over the side of the thorax and observe the skin wrinkling that occurs because of reflex activity of the cutaneus trunci muscle. Palpate the costal arch to locate the last floating rib. Feel for the umbilicus.
Extrinsic Muscles of the Thoracic Limb and Related Structures
The extrinsic muscles of the thoracic limb are those that attach the limb to the axial skeleton; the intrinsic muscles extend between the bones that compose the limb itself. Extrinsic muscles of the thoracic limb are as follows:
In the ventral thoracic region are the superficial and deep pectoral muscles, which extend between the sternum and the humerus. Thoroughly clean these muscles. In thin specimens this will require little dissecting. In pregnant or lactating bitches, it will require reflecting the two thoracic mammae caudally, and in fat specimens the forelimb will probably have to be manipulated so that the borders of the muscles are clearly discernible before cleaning. Always clean the extremities of a muscle as well as the middle part. Actually see and feel the attachments. Visualize the muscle’s position and action on the skeleton and attempt to palpate it on a live dog.
1. The two superficial pectoral muscles (Figs. 2-12 through 2-14, 2-18) lie under the skin between the cranial part of the sternum and the humerus. Their caudal border is thin; their cranial border is thick and rounded and forms the caudal border of a triangle at the base of the neck. The smaller descending pectoral is superficial to the transverse pectoral, which it obliquely crosses from its origin on the first sternebra to its insertion on the crest of the greater tubercle of the humerus. The transverse pectoral arises from the first two or three sternebrae and inserts over a longer distance on the crest of the greater tubercle of the humerus. It is related on its deep surface to the deep pectoral muscle (ascending pectoral). At their insertions these muscles lie between the brachiocephalicus in front and the biceps brachii and humerus behind. Clean both of these superficial pectoral muscles. Transect them 1 cm from the sternum, and reflect them toward the humerus. As muscle attachments are being cleaned, examine the skeletal parts involved.
ORIGIN: The first two sternebrae and usually a part of the third; the fibrous raphe between adjacent muscles.
INSERTION: The whole crest of the greater tubercle of the humerus.
ACTION: To adduct the limb when it is not bearing weight or to prevent the limb from being abducted when bearing weight.
INNERVATION: Cranial pectoral nerves (C7, C8).
2. The deep pectoral muscle (Figs. 2-12, 2-14, 2-15, 2-16, 2-18) extends from the sternum to the humerus and is larger and longer than the superficial pectoral muscles. It lies largely under the skin, the thoracic mammae, and the ventral portion of the cutaneus trunci. The papilla of the caudal thoracic mamma usually lies at the caudal border of the muscle. Only the cranial part is covered by the superficial pectoral muscles. An abdominal slip of this muscle is often present on the caudolateral border. Transect the deep pectoral muscle 2 cm from, and parallel to, the sternum, and clean the distal part to its insertion.
ORIGIN: The ventral part of the sternum and the fibrous raphe between fellow muscles; the deep abdominal fascia in the region of the xiphoid cartilage (the caudal end of the sternum).
INSERTION: The major portion partly muscular, partly tendinous on the lesser tubercle of the humerus; an aponeurosis to the greater tubercle and its crest; the caudal part to the medial brachial fascia.
ACTION: When the limb is advanced and fixed: to pull the trunk cranially and to extend the shoulder joint. When the limb is not supporting weight: to draw the limb caudally and flex the shoulder joint. To adduct the limb.
INNERVATION: Caudal pectoral nerves (C8, T1).
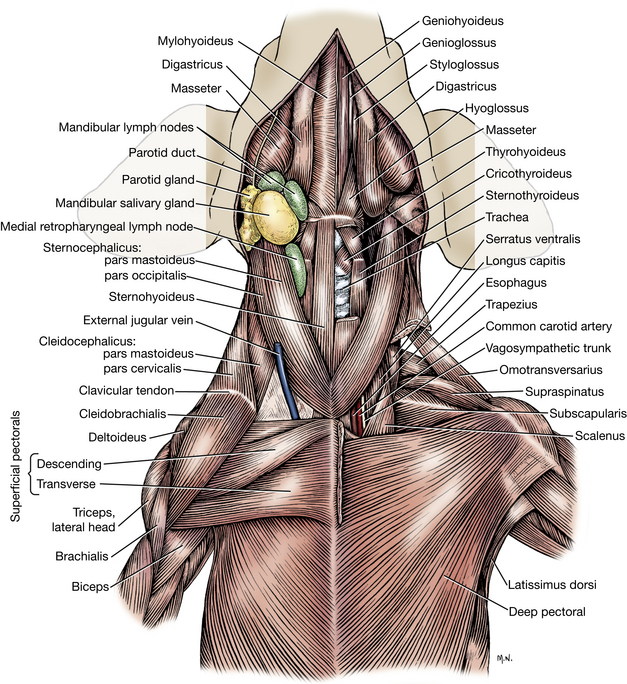
The superficial fascia of the neck is continued on the head as the superficial fascia of the various regions of the head. Caudally it becomes continuous with the superficial brachial and pectoral fasciae. Some of the fascia is also continued into the axillary space. Notice that the external jugular vein is completely wrapped by it. Save this vein for future orientation. The cutaneous muscles of the neck are completely enveloped by the fascia. Only the platysma will be dissected.
The platysma (Fig. 5-20, A) is the best developed of the cutaneous muscles of the neck and head. Its fibers sweep cranioventrally over the dorsal part of the neck and over the lateral surface of the face. The muscle may have been reflected with the skin. Its insertion will be seen when the head is dissected.
3. The brachiocephalicus (Figs. 2-12 through 2-15, 2-18, 3-1) of the dog is a compound muscle developmentally, although it appears as one muscle that extends from the arm to the head and neck. One end attaches on the distal third of the humerus, where it lies between the biceps brachii medially and the brachialis laterally. Proximally on the humerus it partly covers the pectoral muscles at their insertions and lies craniomedial to the deltoid muscle. It crosses the cranial surface of the shoulder, divides into two parts, and obliquely traverses the neck. At the shoulder a faint line crosses the muscle. This is the edge of a fibrous plate, the clavicular intersection, on the deep surface of which the vestigial clavicle (collar bone) is connected. A band of connective tissue can be felt extending from this vestigial clavicle to the manubrium of the sternum and to the scapula. Although the clavicle has lost its functional significance in the dog, it is still considered the origin of the components of the brachiocephalicus muscle. Thus the muscle distal to the clavicular intersection that attaches to the humerus is the cleidobrachialis. The muscle that extends from the clavicular tendon to the neck and head is the cleidocephalicus. The cleidocephalicus has two parts: a thin pars cervicalis, which attaches to the dorsal midline of the neck (formerly called the cleidocervicalis), and beneath it a thicker pars mastoidea, which attaches to the mastoid process of the skull (formerly called the cleidomastoideus). The cervical part of the cleidocephalicus is bounded caudally by the trapezius and cranially by the occipital part of the sternocephalicus.
Transect the cervical part of the cleidocephalicus to expose the extent of the mastoid part below. Note that the mastoid part runs toward the head deep to the sternocephalicus. Transect the mastoid part of the muscle and search for the clavicle by inserting a finger on the medial side of the clavicular intersection.
ATTACHMENTS: All attachments are movable, but the clavicle or clavicular intersection is considered the origin for purposes of naming the muscles. The cleidobrachialis attaches to the distal end of the cranial border of the humerus. There is also a significant fascial tie into the axilla. The cervical part of the cleidocephalicus attaches to the cranial half of the mid-dorsal fibrous raphe and sometimes to the nuchal crest of the occipital bone. The mastoid part of the cleidocephalicus attaches to the mastoid process of the temporal bone with the sternomastoideus muscle.
ACTION: To advance the limb; to extend the shoulder joint and draw the neck and head to the side.
INNERVATION: Accessory nerve and ventral branches of cervical spinal nerves.
4. The sternocephalicus (Figs. 2-12, 2-15, 2-16) arises on the sternum and inserts on the head. At the cranial end of the sternum the muscle is thick, rounded, and closely united with its fellow of the opposite side. Even after the main parts of the paired muscle diverge, there may be considerable crossing of fibers between the two on the ventral surface of the neck. The dorsal border of the sternocephalicus is adjacent to the ventral border of the cleidocephalicus. The external jugular vein crosses its lateral surface obliquely. Notice that the cranial part of the muscle divides into two parts and that the thicker ventral portion is closely related to the mastoid part of the cleidocephalicus. The ventral or mastoid part of the sternocephalicus (formerly the sternomastoideus) is similar to the mastoid part of the cleidocephalicus in shape and insertion. It represents the chief continuation of the sternocephalicus to the head. The thin but wide dorsal portion of the sternocephalicus is the occipital part (formerly the sterno-occipitalis).
ORIGIN: The first sternebra or manubrium.
INSERTION: The mastoid part of the temporal bone and the nuchal crest of the occipital bone.
ACTION: To draw the head and neck to the side.
INNERVATION: Accessory nerve and ventral branches of cervical spinal nerves.Transect the left sternocephalicus close to the manubrium and reflect it. The sternohyoid and sternothyroid muscles are both covered by the deep fascia of the neck and lie dorsal to the sternocephalicus at their origin.
The sternohyoideus (Figs. 2-12 and 5-32) lies on the trachea, covered by the sternocephalicus caudally. A midventral groove indicates the separation of right and left muscles.
ORIGIN: The first sternebra and the first costal cartilage.
INSERTION: The basihyoid bone.
ACTION: To pull the tongue and larynx caudally.
INNERVATION: Ventral branches of cervical spinal nerves.
The sternothyroideus (Figs. 2-12 and 5-32) is covered at its origin by the sternohyoideus. The sternothyroideus inserts on the lateral surface of the thyroid cartilage. The left muscle is bounded dorsally by the esophagus and medially by the trachea. Notice that a tendinous intersection runs across the muscle 3 or 4 cm cranial to its origin. It is at this level that the sternohyoideus separates from the sternothyroideus.
ORIGIN: The first costal cartilage.
INSERTION: The caudolateral surface of the thyroid cartilage.
ACTION: Same as the sternohyoideus—to draw the larynx and tongue caudally.
INNERVATION: Ventral branches of cervical spinal nerves.
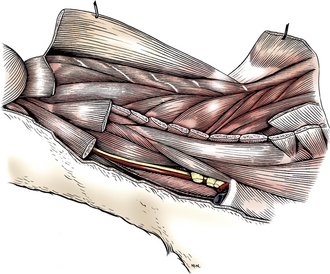
5. The omotransversarius (Figs. 2-12, Figs. 2-13, Figs. 2-15, Figs. 2-17, 3-1) is in a deeper plane than the cleidocephalicus. It is straplike and extends from the distal end of the spine of the scapula to the atlas. It is related to the deep cervical fascia medially. Its caudal part is subcutaneous, but cranially it is covered by the cervical part of the cleidocephalicus. Transect the omotransversarius through its middle and reflect each half toward its attachment. This will expose the superficial cervical lymph nodes located cranial to the scapula (Fig. 3-26).
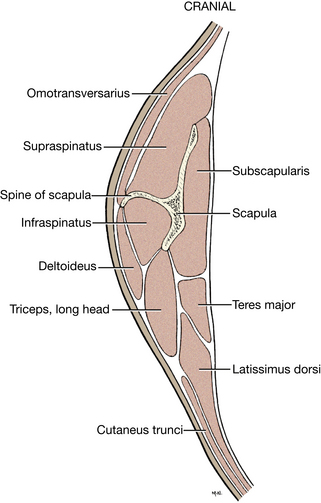
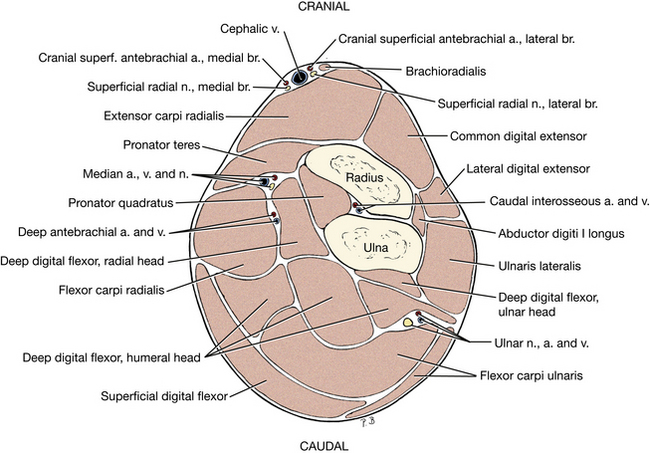
Fig. Figs. 2-17 Transverse section through middle of left scapula.
ATTACHMENTS: The distal end of the spine of the scapula; cranially, the transverse wing of the atlas.
ACTION: To advance the limb or flex the neck laterally.
The deep fascia of the neck is a strong wrapping that extends under the sternocephalicus, omotransversarius, and cleidocephalicus muscles. It covers the sternohyoideus and sternothyroideus ventrally and surrounds the trachea, thyroid gland, larynx, and esophagus. The deep fascia that covers the common carotid artery, vagosympathetic nerve trunk, internal jugular vein, and tracheal lymphatic trunk is the carotid sheath. Locate these structures in the carotid sheath between the omotransversarius dorsally and the sternothyroideus ventrally. The deep fascia of the neck continues dorsally and laterally to invest the deep cervical muscles.
The supraspinous ligament (Fig. 2-84) connects the dorsal aspects of all vertebral spines except the cervical vertebrae (do not dissect at this time). The nuchal ligament, composed predominantly of yellow elastic fibrous tissue, extends from the spine of the first thoracic vertebra to the spine of the axis. The median raphe of the neck is a longitudinal fibrous septum between right and left epaxial muscles dorsal to the nuchal ligament. It serves as the attachment for many of the cervical muscles. Observe these during the dissection of the following muscles.
6. The trapezius (Figs. 2-13, Figs. 2-15) is thin and triangular. It is divided into cervical and thoracic parts, separated by an aponeurosis. The muscle as a whole extends from the median raphe of the neck and the supraspinous ligament to the spine of the scapula. The cervical part is overlapped by the cervical part of the cleidocephalicus whereas the thoracic part overlaps the latissimus dorsi. Transect the trapezius by making an arching cut through the muscle, beginning at the middle of the cranial border. Extend it over the dorsal border of the scapula and continue through the aponeurotic area to the middle of the caudal border. Reflect the muscle to its attachments.
ORIGIN: The median raphe of the neck and the supraspinous ligament from the level of the third cervical vertebra to the level of the ninth thoracic vertebra.
INSERTION: The spine of the scapula.
ACTION: To elevate and abduct the forelimb.
7. The rhomboideus (Figs. 2-13, Figs. 2-14, Figs. 2-16, Fig. 2-76) lies beneath the trapezius and holds the dorsal border of the scapula close to the body. It has capital, cervical, and thoracic parts. The narrow rhomboideus capitis attaches the cranial dorsal border of the scapula to the nuchal crest of the occipital bone. The rhomboideus cervicis runs from the median raphe of the neck to the dorsal border of the scapula. The rhomboideus thoracis is short and thick, connecting the spines of thoracic vertebrae to the dorsal border of the scapula. Its caudal border is deep to the latissimus dorsi. The cervical and thoracic parts of the rhomboideus are contiguous on the dorsal border of the scapula. Transect the entire muscle a few centimeters from the scapula.
ORIGIN: The nuchal crest of the occipital bone; the median fibrous raphe of the neck; the spinous processes of the first seven thoracic vertebrae.
INSERTION: The dorsal border and adjacent surfaces of the scapula.
ACTION: To elevate the forelimb and draw the scapula against the trunk.
INNERVATION : Ventral branches of cervical and thoracic spinal nerves.
8. The latissimus dorsi (Figs. 2-14, Figs. 2-16 through 2-18) is large and roughly triangular. It lies caudal to the scapula, where it covers most of the dorsal and some of the lateral thoracic wall. Clean its ventrocaudal border. Directly caudal to the forelimb, transect the latissimus dorsi at a right angle to its fibers.
ORIGIN: The thoracolumbar fascia from the spinous processes of the lumbar and the last seven or eight thoracic vertebrae; a muscular attachment to the last two or three ribs.
INSERTION: The teres major tuberosity of the humerus and the teres major tendon.
ACTION: To draw the free limb caudally as in digging; to flex the shoulder joint.
INNERVATION: Thoracodorsal nerve (C7, C8, T1).
The thoracolumbar fascia is deep fascia of the trunk. It arises from the supraspinous ligament and spines of the thoracic and lumbar vertebrae; covers the muscles of the vertebrae, ribs, and abdomen; and fuses with the opposite fascia on the ventral midline along a median fibrous raphe, the linea alba. The thoracolumbar fascia serves as an attachment for numerous muscles. It will be dissected with the abdominal muscles.
9. The serratus ventralis cervicis and serratus ventralis thoracis (Figs. 2-14, Figs. 2-16, 2-76) form a continuous large fan-shaped muscle that passes from the cervical vertebrae and ribs to the dorsomedial aspect of the scapula and acts as a sling to support the body between the limbs. Visualize the attachments in a standing dog to appreciate how the trunk is suspended between the limbs. Abduct the forelimb. This will require severing the axillary artery and vein, the nerves contributing to the brachial plexus, and the axillary fascia. As the forelimb is progressively abducted, the attachment of the serratus ventralis will detach from the serrated face of the scapula. Because the forelimb is removed at this stage of the dissection, the detachment of the serratus ventralis may be completed. It is the only extrinsic muscle of the forelimb that has not been transected.
ORIGIN: The transverse processes of the last five cervical vertebrae and the first seven or eight ribs ventral to their middle.
INSERTION: The dorsomedial third of the scapula (serrated face).
ACTION: To support the trunk and depress the scapula.
INNERVATION: Ventral branches of cervical spinal nerves and the long thoracic nerve (C7).
LIVE DOG
Stand over a dog and palpate on both sides the superficial pectoral muscles from in front of the thoracic limbs and the deep pectoral muscles from behind. Place your fingers on the sternum and grasp the deep pectoral between your fingers medially and your thumb laterally. Extend the neck and palpate the brachiocephalicus, which will be stretched taut by this maneuver. With the neck extended, palpate the sternocephalicus, sternohyoideus, and sternothyroideus muscles at their attachment to the first sternebra. Palpate the trachea and appreciate the muscles that must be separated to expose the trachea to open it (a tracheostomy).
Palpate the spines of the thoracic vertebrae. The cervical spines caudal to the axis are not palpable. Try to separate the dorsal border of the scapula from the thoracic vertebral spines. The trapezius and rhomboideus prevent this. Palpate the sides of the thorax covered by the latissimus dorsi and feel its ventral border.
Visualize the attachments of the serratus ventralis muscles and how they keep the limb attached to the trunk when the dog is supporting weight. Occasionally, their termination on the scapula is torn by injury. This results in an abnormal elevation of the limb when the dog bears weight, and the dorsal border of the scapula will protrude dorsally beside or above the level of the thoracic spines.
Lateral Muscles of the Scapula and Shoulder
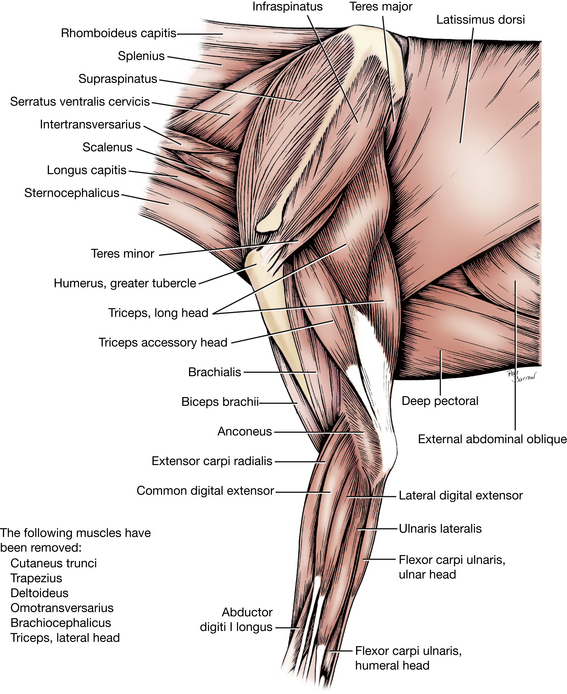
1. The deltoideus (Figs. 2-13, Figs. 2-15, Figs. 2-17) is composed of two portions that fuse and act in common across the shoulder. The scapular part arises as a wide aponeurosis from the length of the scapular spine and covers the infraspinatus. The latter muscle can be seen through this aponeurosis and should not be confused with the deltoideus. Observe the acromial part of the deltoideus, which arises from the acromion and has a fusiform shape. Both portions of the muscle fuse before they insert on the deltoid tuberosity of the humerus. Transect the combined muscle 2 cm distal to the acromion and reflect the stumps. Free the scapular part from the infraspinatus and work under the aponeurosis of origin to verify its attachment to the spine of the scapula.
ORIGIN: The spine and acromial process of the scapula.
INSERTION: The deltoid tuberosity.
2. The infraspinatus (Figs. 2-13, Figs. 2-16, Figs. 2-17) is fusiform and lies principally in the infraspinous fossa. Transect the infraspinatus halfway between its extremities. Free and reflect the distal half from the scapula by scraping the fibers away from the spine and fossa with the handle of the scalpel. Reflect the distal half to its insertion on the side of the greater tubercle. This will expose a subtendinous synovial bursa between the tendon of insertion and the greater tubercle of the humerus. A bursa is a closed connective tissue sac containing synovial fluid, which reduces friction.
ORIGIN: The infraspinous fossa.
INSERTION: A small, circumscribed area on the lateral side of the greater tubercle of the humerus.
To extend and laterally stabilize or flex the shoulder joint, depending on the degree of extension or position of the joint when the muscle contracts. To abduct the shoulder joint and to rotate the shoulder laterally. To prevent medial rotation when weight bearing and provide lateral stability to the shoulder joint.
INNERVATION: Suprascapular nerve.
3. The teres minor (Figs. 2-13, Figs. 2-16), a small, wedge-shaped muscle, is now exposed caudal to the shoulder joint. It is covered superficially by the deltoideus.
ORIGIN: The infraglenoid tubercle and distal third of the caudal border of the scapula.
INSERTION: The teres minor tuberosity of the humerus.
ACTION: To flex the shoulder joint, rotate the shoulder laterally, and prevent medial rotation when bearing weight.
4. The supraspinatus (Figs. 2-12, Figs. 2-13, Figs. 2-14, Figs. 2-16, Figs. 2-17, Figs. 2-19, Figs. 2-27), which is wider and larger than the infraspinatus, is largely covered by the cervical part of the trapezius and the omotransversarius. It lies in the supraspinous fossa and extends over the cranial border of the scapula so that a part of the muscle is closely united with the subscapularis medially. Clean and observe the insertion on the greater tubercle of the humerus.
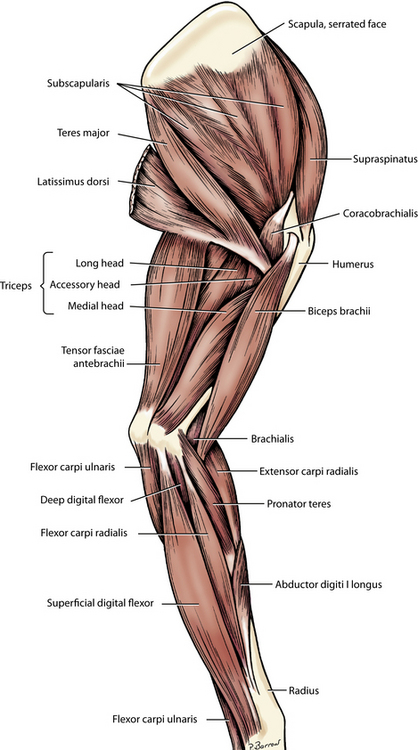
Fig. Figs. 2-19 Muscles of left thoracic limb, medial view.
ORIGIN: The supraspinous fossa.
INSERTION: The greater tubercle of the humerus, by a thick tendon.
ACTION: To extend and laterally stabilize the shoulder joint.
Medial Muscles of the Scapula and Shoulder
1. The subscapularis (Figs. 2-12, Figs. 2-13, Figs. 2-14, Figs. 2-17, Figs. 2-19) occupies the entire subscapular fossa, the boundaries of which it overlaps slightly. The supraspinatus is closely associated with it cranially, whereas the teres major has a similar relation caudally. Clean the insertion but do not transect the muscle.
ORIGIN: The subscapular fossa.
INSERTION: The lesser tubercle of the humerus.
ACTION: To adduct, extend, and medially stabilize the shoulder joint. To rotate the shoulder medially and prevent lateral rotation when bearing weight.
INNERVATION: Subscapular nerve. Considerable support is provided to the shoulder joint by the subscapularis muscle medially, the teres minor and infraspinatus muscles laterally, and the supraspinatus cranially. Luxation will not occur without injury to the joint capsule and its glenohumeral ligaments (Fig. 2-29).
2. The teres major (Figs. 2-13, Figs. 2-14, Figs. 2-16, Figs. 2-17, Figs. 2-19, Figs. 2-27), directly caudal to the subscapularis, belies its descriptive name because it is not round but has three surfaces. Its proximal end arises from the subscapularis and the proximal caudal border of the scapula. Fibers extend distally to attach to the tendon of insertion of the latissimus dorsi. Work between the distal half of the muscle and the subscapularis. Observe the close relationship between the teres major and the latissimus dorsi as they approach their insertion on the proximal medial surface of the body of the humerus. Transect the teres major and reflect the combined insertion to expose the belly of the coracobrachialis muscle.
ORIGIN: The caudal angle and adjacent caudal border of the scapula; the caudal surface of the subscapularis.
INSERTION: The teres major tuberosity of the humerus.
ACTION: Flex the shoulder, rotate the shoulder medially, and prevent lateral rotation when weight bearing.
3. The coracobrachialis (Figs. 2-14, Figs. 2-19) crosses the medial surface of the shoulder obliquely. It is a small spindle-shaped muscle that arises from the coracoid process of the scapula by a relatively long tendon that courses caudodistally across the lesser tubercle. There it crosses the tendon of insertion of the subscapularis. Its tendon is provided with a synovial sheath as it crosses the lesser tubercle of the humerus. The muscle belly is distal to the lesser tubercle and medial to the origin of the medial head of the triceps. The conjoined tendon of the teres major and latissimus dorsi crosses the insertion of the coracobrachialis. Notice that the coracobrachialis tendon courses cranial to the center of the shoulder. This accounts for its action as an extensor muscle of the shoulder. Free the coracobrachialis and isolate the tendon of origin by cutting into its tendon sheath.
ORIGIN: The coracoid process of the scapula.
INSERTION: The crest of the lesser tubercle of the humerus proximal to the teres major tuberosity.
ACTION: To adduct, extend, and stabilize the shoulder joint.
LIVE DOG
Locate the spine of the scapula and palpate the supraspinatus cranial to it and the infraspinatus and the scapular part of the deltoideus caudal to it. Find the acromion and palpate the acromial part of the deltoideus and the deltoid tuberosity. Palpate the greater tubercle and the acromion and estimate the middle position on a line between these structures. A needle inserted at this point through the deltoideus, cranial to the infraspinatus, will enter the shoulder (humeral) joint. Rotate the arm medially and laterally. The restriction to lateral rotation is by the teres major and subscapularis, whereas the restriction to medial rotation is by the teres minor and infraspinatus. Injury that tears the termination of the latter muscles allows excessive medial rotation. In the weight-bearing phase of walking, this causes the elbow to abduct. Occasionally, injury to the infraspinatus results in shortening of the muscle by contracture when it heals. This results in a constant excessive lateral rotation of the shoulder, and the dog stands with the elbow adducted. This persists during the swing phase (protraction), when there is also a compensatory abduction of the paw. On manipulation there is increased restriction to medial rotation. This can be corrected by cutting the tendon of the contracted infraspinatus. An overall function of the infraspinatus, supraspinatus, subscapularis, and coracobrachialis is to act as collateral ligaments to stabilize the shoulder joint medially and laterally during normal gait.
Caudal Muscles of the Arm (Brachium)
This group is a large, muscular mass that almost completely fills the space between the caudal border of the scapula and the olecranon. It consists of three muscles: the triceps brachii, the tensor fasciae antebrachii, and the anconeus. By far the largest of these muscles is the triceps. All of the caudal muscles of the arm are extensors of the elbow.
1. The tensor fasciae antebrachii (Figs. 2-14, 2-18, Figs. 2-19) is a thin strap that extends from the latissimus dorsi to the medial fascia of the forearm and the olecranon. It lies on the long head of the triceps.
ORIGIN: The fascia covering the lateral side of the latissimus dorsi.
2. The triceps brachii in the dog consists of four heads instead of the usual three, with a common tendon to the olecranon tuber. Only the long head arises from the scapula. The other three arise from the proximal end of the humerus.
The long head (Figs. 2-13 to Figs. 2-19, Figs. 2-27) completely bridges the humerus. It arises from the caudal border of the scapula and inserts on the olecranon tuber. It appears to have two bellies. Caudal to the shoulder, palpate a groove between the long and lateral heads of the triceps. Separate these two heads along this groove. Expose the tendon of the long head and notice the subtendinous bursa between it and the groove of the olecranon. Notice how the tendons of the other heads blend with that of the long head.
ORIGIN: The caudal border of the scapula.
INSERTION: The olecranon tuber.
ACTION: To extend the elbow and flex the shoulder.
The lateral head (Figs. 2-12, Figs. 2-13, Figs. 2-15, 2-18, 2-20, Figs. 2-27) of the triceps lies distal to the long head, caudal to the acromial part of the deltoideus, and lateral to the accessory head, which it covers. Transect the aponeurotic origin of the lateral head and reflect it to expose the underlying accessory and medial heads. This also exposes the brachialis muscle.
ORIGIN: The tricipital line of the humerus.
INSERTION: The olecranon tuber.
The accessory head (Figs. 2-13, Figs. 2-14, Figs. 2-16, 2-18, Figs. 2-19, Figs. 2-27) lies between the lateral and medial heads.
ORIGIN: The neck of the humerus.
INSERTION: The olecranon tuber.
The medial head (Figs. 2-14, 2-18, Figs. 2-19, 2-23, Figs. 2-27) lies caudally on the humerus lateral and caudal to the biceps brachii. Separate the muscle from the long head caudally and from the accessory head laterally. The long tendon of the accessory head is closely bound to its lateral surface.
ORIGIN: The crest of the lesser tubercle near the teres major tuberosity.
3. The anconeus (Figs. 2-13 through Figs. 2-16, 2-23) is a small muscle located almost completely in the olecranon fossa. Reflect the insertion of the lateral head of the triceps to uncover the lateral surface of this muscle. Notice that the most distal fibers lie in a transverse plane. On the lateral side, cut the origin of the anconeus from the lateral supracondylar crest and epicondyle. Reflect it to expose the elbow joint capsule. Open the joint capsule to expose the elbow at the level of the anconeal process of the ulna.
ORIGIN: The lateral supracondylar crest and the lateral and medial epicondyles of the humerus.
INSERTION: The lateral surface of the proximal end of the ulna (the olecranon).
LIVE DOG
Palpate the triceps brachii caudal to the arm and its termination on the olecranon. Appreciate the function of this muscle in extension of the elbow to support the weight of the animal in standing and during locomotion. Avulsion of its tendon or denervation of this muscle will cause the limb to collapse when weight is placed on it. Lightly striking the triceps tendon at the olecranon tuber will elicit reflex contraction and cause extension of the elbow in some dogs.
Cranial Muscles of the Arm
1. The biceps brachii (Figs. 2-12, Figs. 2-13, Figs. 2-14, Figs. 2-16, 2-18 through 2-20, Figs. 2-27, 2-30) has only one head. It is a long, fusiform muscle that lies on the medial and cranial surfaces of the humerus. It completely bridges this bone as it arises on the supraglenoid tuberosity of the scapula and inserts on the proximal ends of the radius and ulna. It is covered superficially by the pectoral muscles. Clean the muscle and transect it through its middle. Reflect the proximal half to its origin. This will require severing the transverse humeral retinaculum, a band of fibrous tissue that joins the greater and lesser tubercles and holds the tendon of origin in the intertubercular groove. An extension of the shoulder joint capsule (the intertubercular bursa) acts as a synovial sheath for this tendon. Reflect the distal half of the biceps to the proximal end of the radius and ulna, where it meets the brachialis tendon and bifurcates. The tendons of insertion lie on the elbow joint capsule, covering its medial collateral ligament. Delay cleaning these tendons until after the pronator teres muscle has been dissected.
ORIGIN: The supraglenoid tubercle.
INSERTION: The ulnar and radial tuberosities.
ACTION: To flex the elbow and extend the shoulder.
INNERVATION: Musculocutaneous nerve.
2. The brachialis (Figs. 2-12 through Figs. 2-16, 2-18 through 2-20, 2-30) should be studied from the lateral side. It is a long, thin muscle that lies in the brachialis groove of the humerus. From the proximal third of this groove, the brachialis curves laterally and cranially as it courses distally, crosses the elbow, and inserts by a terminal tendon on the medial side of the proximal end of the ulna. A large part of its lateral surface is covered by the lateral head of the triceps. Distally, it runs medial to the origin of the extensor carpi radialis. Its insertion will be dissected later with the biceps insertion. These are deep to the pronator teres.
ORIGIN: The proximal third of the lateral surface of the humerus.
LIVE DOG
Palpate the crest of the greater tubercle and, medial to it, feel the tendon of the biceps brachii in the intertubercular groove covered by the termination of the pectoral muscles. This part of the tendon is covered by a synovial sheath that is continuous with the shoulder joint capsule. Swelling of the tendon sheath will be felt when there is increased synovial fluid from lesions of the tendon, its sheath, or the shoulder joint. Distally in the arm, feel the terminal portions of the biceps brachii medially and the brachialis laterally on the cranial aspect of the elbow. Both muscles can be palpated here. Lightly striking these muscles at this site with a blunt object will elicit reflex contraction and elbow flexion in some dogs.
Before the rest of the skin is removed from the thoracic limb, examine the foot pads. The small pad that protrudes palmar to the carpus is the carpal pad. The largest in the paw, the metacarpal pad, is on the palmar side of the metacarpophalangeal joints and is triangular. The digital pads are ovoid and flattened. Each is located palmar to the distal interphalangeal joint.
Make a midcaudal incision through the skin from the olecranon through the carpal and metacarpal pads to the interdigital space between digits III and IV. Reflect the skin, dissect it free from the fascia, and remove it from the forelimb. The pads are closely attached to the underlying structures but may be dissected free and removed. Be careful not to cut too deeply and sever the underlying small tendons. Work distally on each of the four main digits and completely remove the skin and digital pads.
The areolar part of the subcutaneous tissue distal to the elbow is scanty. The principal veins and cutaneous nerves lie in large part on the superficial fascia of the antebrachium. For descriptive purposes, the superficial and deep fascia distal to the elbow may be divided into antebrachial, carpal, metacarpal, and digital parts.
The deep antebrachial fascia forms a single dense sleeve for the muscles of the forearm on the caudal surface. Make an incision through the deep antebrachial fascia from the olecranon to the accessory carpal bone. Carefully reflect the fascia cranially on the forearm. At first, the fascia is easily reflected because it lies on the epimysium of the muscles beneath. Cranially, it sends delicate septal leaves between muscles, and on reaching the radius, it firmly unites with its periosteum.
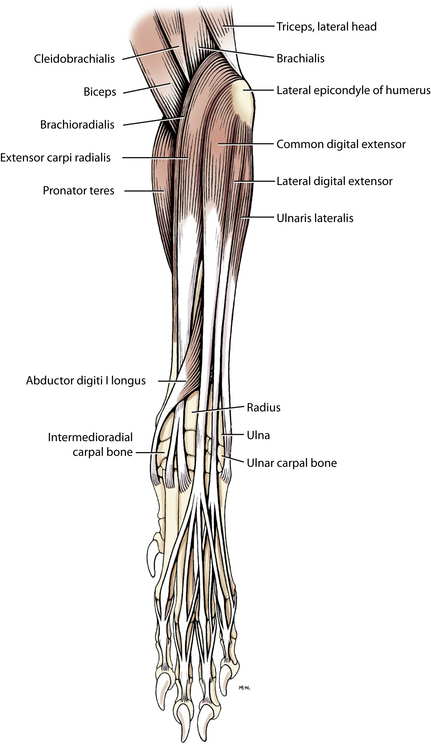
Cranial and Lateral Muscles of the Forearm (Antebrachium)
The cranial and lateral antebrachial muscles are, from cranial to caudal, the extensor carpi radialis, supinator, common digital extensor, lateral digital extensor, ulnaris lateralis, and abductor pollicis longus. Most of these muscles arise from the lateral epicondyle of the humerus. A slender, inconstant muscle, the brachioradialis (Figs. 2-20, 2-21), arises from the lateral supracondylar crest of the humerus, adjacent to the extensor carpi radialis, and passes distally and medially to insert on the distal fourth of the radius. If present, the muscle is frequently removed with the skin.
1. The extensor carpi radialis (Figs. 2-13 through Figs. 2-16, Figs. 2-19 through 2-22, Figs. 2-27) is the largest of the craniolateral antebrachial muscles. It lies on the cranial surface of the radius throughout most of its course and is easily palpated in the live dog. The tendon looks single but is distinctly double throughout its distal third. These closely associated tendons run first under the tendon of the abductor digiti I longus, then in the middle groove of the radius farther distally, and finally over the carpus. They are held in place on the dorsal surface of the carpus by the extensor retinaculum (Fig. 2-22). This is a transversely oriented condensation of carpal fascia that aids in holding in grooves all the tendons that cross the dorsum of the carpus. Between bundles of tendons the extensor retinaculum dips down to blend with the fibrous dorsal part of the joint capsule. Define by dissection the proximal and distal margins of the extensor retinaculum, but do not sever it along the tendons.
ORIGIN: The lateral supracondylar crest.
INSERTION: The small tuberosities on the dorsal surfaces of the base of metacarpals II and III.
2. The common digital extensor (Figs. 2-13, Figs. 2-14, Figs. 2-16, 2-20 through 2-22, Figs. 2-27) is shaped like, and lies caudal to, the extensor carpi radialis on the lateral side of the forearm. The four individual tendons that leave the muscle are closely combined where they cross the cranial surface of the abductor digiti I longus and then the carpus; here they are held in the lateral groove of the radius by the extensor retinaculum. Distal to the ligament the four tendons diverge, and each goes to the distal phalanx of the four main digits. Dissect the tendon of the common extensor that goes to the third or fourth digit. Free the tendon as it crosses each of the joints. It often contains a sesamoid bone at the metacarpophalangeal joint. Insertion is on the extensor process of the distal phalanx.
ORIGIN: The lateral epicondyle of the humerus.
INSERTION: The extensor processes of the distal phalanges of digits II, III, IV, and V.
ACTION: To extend the joints of the four principal digits and the carpus.
Notice that the distal interphalangeal joint is in a marked degree of overextension. This is brought about by the elastic dorsal ligament, which lies on each side of the common digital extensor tendon. The ligament attaches proximally to the sides of the base of the middle phalanx. Distally, it attaches to the dorsal surface of the ungual crest of the distal phalanx (Fig. 2-26). Its elasticity hyperextends the distal interphalangeal joint and thus retracts the claw.
3. The lateral digital extensor (Figs. 2-13, Figs. 2-14, Figs. 2-16, 2-20 through 2-22) is about half the size of the common digital extensor. It lies between the common digital extensor and the ulnaris lateralis. Its tendon begins at the middle of the forearm, passes under the extensor retinaculum in a groove between the radius and ulna, and immediately splits into three branches. The main part of each tendon attaches to the extensor process of the distal phalanx of digits III, IV, and V in common with the common digital extensor tendon.
ORIGIN: The lateral epicondyle of the humerus.
INSERTION: The proximal ends of all the phalanges of digits III, IV, and V, but mainly the extensor processes of the distal phalanges of these digits.
ACTION: To extend the carpus and joints of digits III, IV, and V.
4. The ulnaris lateralis [extensor carpi ulnaris] (Figs. 2-13, Figs. 2-16, 2-20 through 2-24) is larger than the lateral digital extensor and lies caudal to it. It is bounded deeply by the ulna and the large flexor group of muscles, which lie caudal and medial to it. It is the only flexor to arise on the lateral epicondyle. Expose the muscle and notice the two tendons of insertion.
ORIGIN: The lateral epicondyle of the humerus.
INSERTION: The lateral aspect of the proximal end of metacarpal V and the accessory carpal bone.
ACTION: To abduct the manus and flex the carpal joint and support the carpus when extended to support weight.
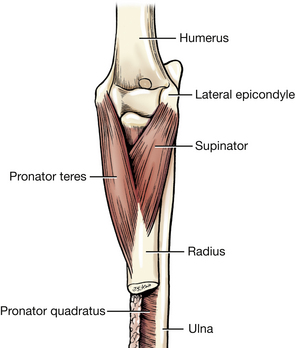
5. The supinator (Figs. 2-13, Figs. 2-14, 2-25) is short, broad, and flat and obliquely placed across the lateral side of the flexor surface of the elbow joint. It is covered superficially by the extensor carpi radialis and common digital extensors, which should be transected in the middle of their muscle bellies and reflected. The supinator lies principally on the proximal fourth of the radius. There is a sesamoid bone in this muscle where it crosses the head of the radius.
ORIGIN: The lateral epicondyle of the humerus.
INSERTION: The cranial surface of the proximal fourth of the radius.
ACTION: To rotate the forearm laterally so that the palmar side of the paw faces medially (supination); to flex the elbow.
6. The abductor digiti I longus (Figs. 2-13, Figs. 2-14, Figs. 2-16, 2-20 through 2-22) lies primarily in the groove between the radius and ulna and is triangular. Displace the digital extensors so that the bulk of the muscle is uncovered. Clean the muscle and transect its tendon as it obliquely crosses the extensor carpi radialis. There is a sesamoid bone in its tendon where it crosses the medial surface of the carpus. This muscle is also called the extensor carpi obliquus in domestic animals.
ORIGIN: The lateral border and cranial surface of the body of the ulna; the interosseous membrane.
INSERTION: The proximal end of metacarpal I.
ACTION: To abduct the first digit or pollex and extend the carpal joints.
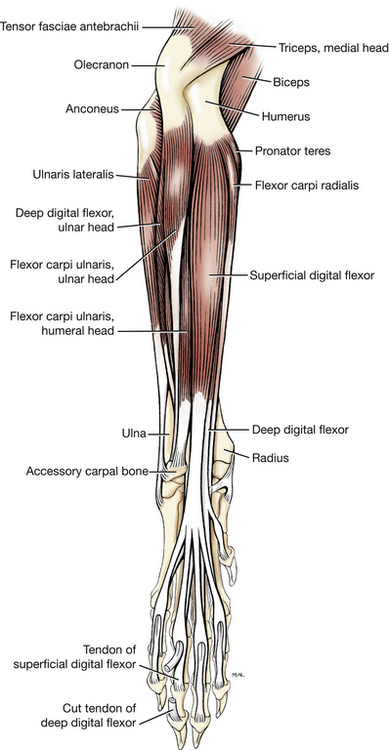
Caudal and Medial Muscles of the Forearm
The deep antebrachial fascia has been removed from this group of muscles. It will be necessary to clean the tendons of insertion when dissecting the individual muscles. The muscles in this group include, from the radius caudally, the pronator teres, the flexor carpi radialis, the deep digital flexor, the superficial digital flexor, and the flexor carpi ulnaris.
1. The pronator teres (Figs. 2-13, Figs. 2-14, Figs. 2-19 through 2-21, 2-23 through 2-25) extends obliquely across the medial surface of the elbow. It is round in transverse section at its origin and flat at its insertion. It lies between the extensor carpi radialis cranially and the flexor carpi radialis caudally. Displace adjacent muscles to see its origin and insertion.
ORIGIN: The medial epicondyle of the humerus.
INSERTION: The medial border of the radius between the proximal and middle thirds.
ACTION: To rotate the forearm medially so that the palmar side of the paw faces the ground (pronation); to flex the elbow.
Clean the tendons of insertion of the biceps and brachialis muscles, which are now exposed. The tendon of insertion of the biceps splits into two parts (Fig. 2-30). The larger of the two inserts on the ulnar tuberosity and the smaller inserts on the radial tuberosity. The terminal tendon of the brachialis inserts between these two tendons of the biceps, primarily on the ulnar tuberosity.
2. The flexor carpi radialis (Figs. 2-14, Figs. 2-19, 2-21 through 2-24) lies between the pronator teres cranially and the superficial digital flexor caudally. It covers the deep digital flexor, part of which can be seen. The flexor carpi radialis has a thick, fusiform belly, which, partly imbedded in the deep flexor, extends only to the middle of the radius. There it gives rise to a flat tendon that is augmented by fibers leaving the medial border of the radius. Clean the tendon to the point where it passes through the carpal canal deep to a thick layer of fibrous tissue on the palmar side of the carpus, the flexor retinaculum (Fig. 2-22). Do not cut through this fibrous tissue now. A synovial sheath extends from the distal end of the radius almost to the insertion of the muscle on the palmar surface of the second and third metacarpal bones. This will be exposed later.
ORIGIN: The medial epicondyle of the humerus and the medial border of the radius.
INSERTION: The palmar side of the base of metacarpals II and III.
3. The superficial digital flexor (Figs. 2-13, Figs. 2-14, Figs. 2-19, 2-21 through 2-24, 2-26, Figs. 2-27) lies beneath the skin and antebrachial fascia on the caudomedial side of the forearm. It covers the deep digital flexor and is fleshy almost to the carpus. Its tendon is at first single, then crosses the palmar (flexor) surface of the carpus medial to the accessory carpal bone in the carpal canal, where it is covered by the superficial part of the flexor retinaculum, and finally divides into four tendons of nearly equal size. These insert on the palmar surfaces of the base of the middle phalanges of the four principal digits. At the metacarpophalangeal joint, each forms a collar, the flexor manica, around the deep flexor tendon that passes through it. Clean each of the individual tendons as far as the metacarpophalangeal joints. Transect the muscle at the middle of the antebrachium. Transect the superficial part of the flexor retinaculum and turn the distal part of the superficial digital flexor toward the digits. Because all parts of the superficial digital flexor tendon are similar, only that to the third digit will be dissected. The superficial and deep digital flexor tendons are held firmly in place at the metacarpophalangeal joint by the palmar annular ligament, which crosses the flexor manica (Fig. 2-26). If any of the structures mentioned next are not clearly seen on the third digit, they should be verified on one or more of the other main digits. Observe that the tendon of the superficial digital flexor, which forms a flexor manica (Fig. 2-26), sheathes the deep digital flexor for a distance of more than 1 cm at the metacarpophalangeal joint. The superficial digital flexor tendon lies on the palmar side of the deep flexor tendon at the proximal end of its encircling sheath but on the dorsal side at the distal end. The superficial flexor tendon with its sheath and the deep flexor tendon are in a common synovial membrane, the digital synovial sheath.
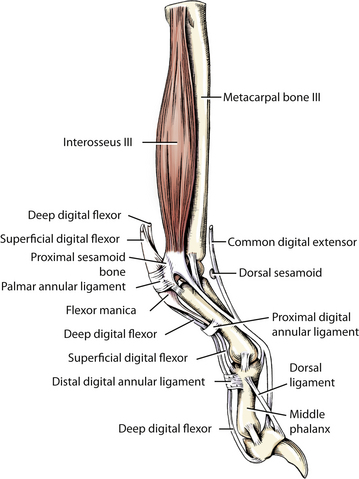
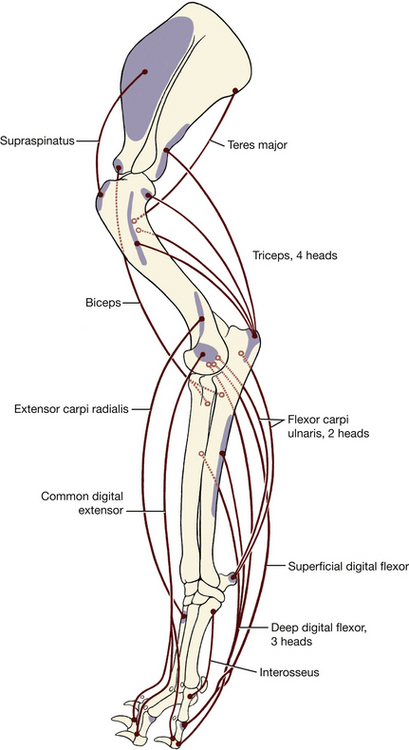
Fig. Figs. 2-27 Major extensors and flexors of left forelimb.
ORIGIN: The medial epicondyle of the humerus.
INSERTION: The palmar surface of the base (proximal end) of the middle phalanges of digits II, III, IV, and V.
ACTION: To flex the carpal, metacarpophalangeal, and proximal interphalangeal joints of digits II, III, IV, and V.
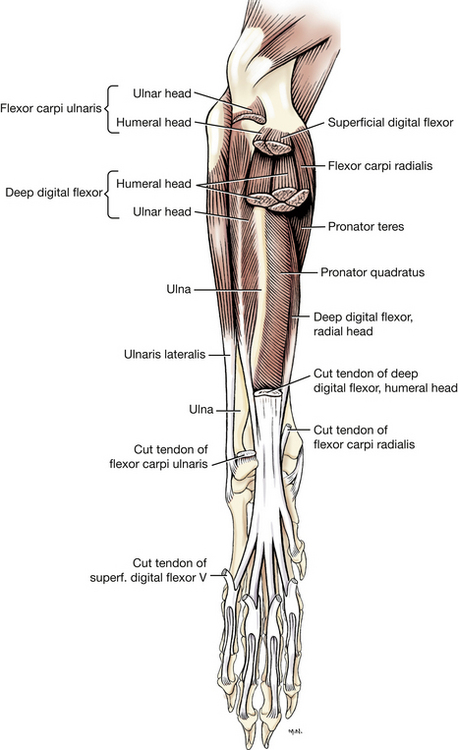
4. The flexor carpi ulnaris (Figs. 2-13, Figs. 2-14, Figs. 2-16, Figs. 2-19, 2-21, 2-23, 2-24, Figs. 2-27) consists of two parts that are distinct throughout their length. The ulnar head arises from the caudal border of the proximal end of the ulna. It is thin and wide proximally but narrow distally. It lies between the ulnaris lateralis and superficial digital flexor. The humeral head is large and fleshy and lies cranial to the ulnar head, except distally, where its tendon lies caudal to it. Dissect the insertion of this muscle on the accessory carpal bone and clean its origin. A subfascial bursa is present over the tendon of insertion of the humeral head, and an intertendinous bursa is found between the two tendons of insertion at the carpus.
ORIGIN: Ulnar head—the caudal border and medial surface of the olecranon; humeral head—the medial epicondyle of the humerus.
INSERTION: The accessory carpal bone.
5. The deep digital flexor (Figs. 2-13, Figs. 2-14, Figs. 2-19, 2-21 through 2-24, 2-26, Figs. 2-27) has three heads of origin of dissimilar size, which arise from the humerus, radius, and ulna. Their bellies, along with the pronator quadratus, lie on the caudal surfaces of the radius and ulna. Transect both muscle bellies of the flexor carpi ulnaris in the middle of the antebrachium. Reflect the stumps to expose and identify the three heads of the deep digital flexor muscle. Notice that the humeral head of this muscle is much larger than the other two heads and has several bellies. The ulnar head is small and arises from the caudal border of the ulna. The radial head is the smallest and comes from the medial border of the radius. The tendons of all three heads fuse at the carpus to form a single tendon. This tendon is held in place in the carpal canal by the thick, deep part of the fibrous flexor retinaculum.
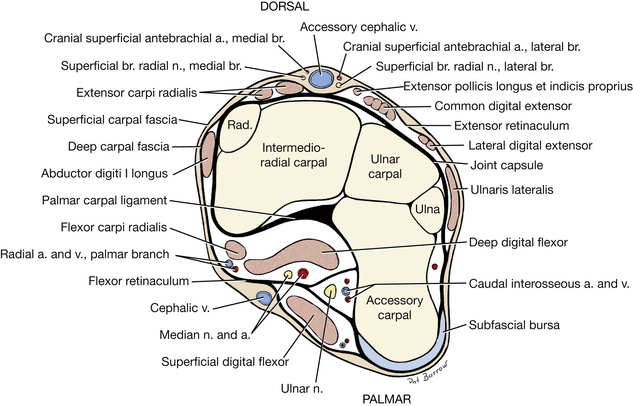
The carpal canal is formed by the accessory carpal bone laterally, the palmar carpal ligament and the carpal bones dorsally, and the flexor retinaculum on the palmar surface. Cut this retinaculum medially and reflect it laterally to the accessory carpal bone to expose the deep digital flexor tendon.
Distal to the carpus the deep digital flexor tendon divides into five branches. Each branch goes to the palmar surface of the base of the distal phalanx of its respective digit. There is a synovial bursa under the humeral head at the elbow and a carpal synovial sheath in the carpal canal. Dissect all of this digital flexor and the other digital muscles for digit III or IV. Observe all structures shown in Fig. 2-26. Digital synovial sheaths extend from above the metacarpophalangeal joints to the insertion of the tendons on the distal phalanges of all the digits. The digital synovial sheaths, except that of the first digit, are common to both the superficial and the deep flexor tendons. Dissect the deep digital flexor tendon to its insertion on the distal phalanx of the third digit. It has already been exposed with the superficial digital flexor tendon at the metacarpophalangeal joint. Note the annular digital ligaments that support the deep digital flexor tendon proximal and distal to the palmar surface of the proximal interphalangeal joint.
ORIGIN: Humeral head—the medial epicondyle of the humerus; ulnar head—the proximal three fourths of the caudal border of the ulna; radial head—the middle third of the medial border of the radius.
INSERTION: The flexor tubercle on the palmar surface of the distal phalanx of each digit.
ACTION: To flex the carpal and metacarpophalangeal joints and the proximal and distal interphalangeal joints of the digits.
INNERVATION: Median and ulnar nerves.
6. The pronator quadratus (Figs. 2-14, 2-21, 2-24, 2-25) fills in the space between the radius and ulna. Spread the flexor muscles and observe the pronator. The fibers of this muscle run transversely between the ulna and radius.
Muscles of the Forepaw (Manus)
There are several special muscles of the digits. Only the interossei will be dissected. The four interosseous muscles are fleshy and similar in size and shape (Figs. 2-26, Figs. 2-27). They lie deep to the deep digital flexor tendons and cover the palmar surfaces of the four main metacarpal bones. Transect the deep digital flexor tendon at the proximal end of the carpus and reflect it distally. Dissect the interosseous muscle of the third digit. Each muscle arises from the base of its respective metacarpal bone and the carpal joint capsule. After a short course, each divides into two tendons, which attach to the base of the proximal phalanx. Imbedded in each tendon is a sesamoid bone that lies on the palmar surface of the metacarpophalangeal joint. There are thus two proximal sesamoids imbedded in the tendon of insertion at metacarpophalangeal joints II, III, IV, and V. A lesser tendon continues obliquely across the proximal end on each side of the proximal phalanx and joins the common extensor tendon on the dorsal surface. The interosseous muscle is a flexor of the metacarpophalangeal (fetlock) joint and maintains the joint angle when the dog bears weight on the paw. Complete exposure of the tendon of insertion of an interosseous muscle can be accomplished by separating the third and fourth digits to the level of the carpometacarpal joint. Abduct the fourth and fifth digits to observe the full length of the interosseous muscle on the third digit. Transect the muscle at the middle of the metacarpal bone and reflect the distal portion to expose the sesamoid bones in the tendon at the metacarpophalangeal joint.
LIVE DOG
Palpate the lateral epicondyle of the humerus. Feel for the groove between the lateral supracondylar crest and the olecranon, where a needle can be inserted through the anconeus muscle into the elbow joint. Follow the extensor muscles distally in the forearm. Follow the tendons of the extensor carpi radialis and common digital extensor across the carpus. Flex the carpus and palpate the antebrachiocarpal joint on either side of these tendons where a needle puncture can be made.
Palpate the medial humeral epicondyle and the origins of the flexor muscles on it. At the carpus, palpate the terminations of the flexor carpi ulnaris and ulnaris lateralis on the accessory carpal. Palpate the tendon of the superficial digital flexor at the carpal canal. Flex the carpus and feel the tendon loosen. Extend it and feel the tendon become taut. Flex and extend the metacarpophalangeal and interphalangeal joints and appreciate the action of the digital extensors and flexors on these joints. Laceration of the digital flexors will cause overextension of the interphalangeal joints affected.
JOINTS OF THE THORACIC LIMB
The humeral or shoulder joint (Fig. 2-28) is a ball-and-socket joint between the glenoid cavity of the scapula and the head of the humerus. It is capable of movements in any direction, but the chief movements it undergoes are flexion and extension. Transect the subscapularis medially and the teres minor laterally to gain access to the humeral joint capsule. The humeral joint capsule is a loose sleeve of synovial membrane and thin fibrous tissue that unites the scapula and humerus. Poorly developed thickenings of the fibrous part of the joint capsule on each side are called the medial and lateral glenohumeral ligaments (Figs. 2-28, 2-29). There is a collagenous thickening across the tendon of origin of the biceps at the intertubercular groove; this is the transverse humeral retinaculum (Fig. 2-28). The joint capsule surrounds the tendon of origin of the biceps brachii in the intertubercular groove, forming its tendon sheath.
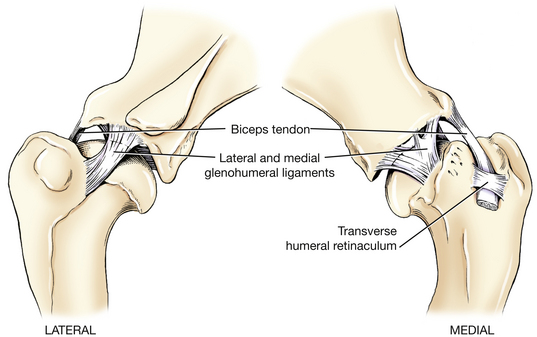
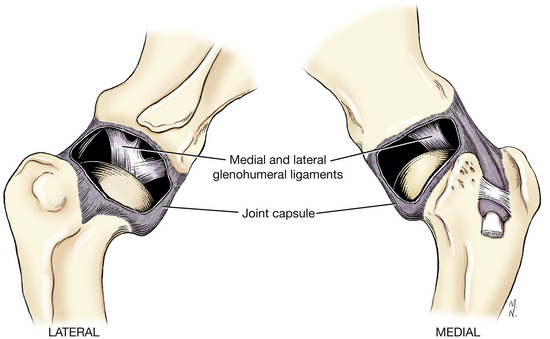
The elbow joint (Figs. 2-30, 2-31) is a hinge joint formed by the condyle of the humerus, the head of the radius, and the trochlear notch of the ulna. In addition, there is the proximal radioulnar articulation, although it is not weight bearing. The elbow joint capsule attaches to the articular margins; it extends distally a short distance between the radius and ulna. All compartments communicate with each other. The lateral and medial collateral ligaments are pronounced thickenings in the fibrous layer of the capsule. The biceps and brachialis tendons cover the distal portion of the medial collateral ligament. Transect and reflect these tendon insertions to expose the medial collateral ligament. Transect the medial collateral ligament to expose the medial coronoid process of the ulna that it covers. This is a site of osteochondrosis lesions. On the lateral side, transect and reflect the origin of the lateral digital extensor to expose the lateral collateral ligament (Fig. 2-31). These taut ligaments prevent adduction or abduction of the elbow and restrict movement to the sagittal plane. Some rotational movement occurs at the radioulnar joint.
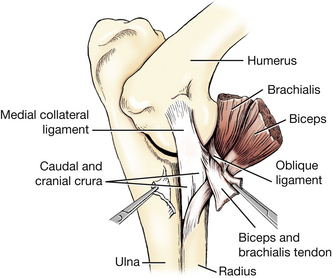
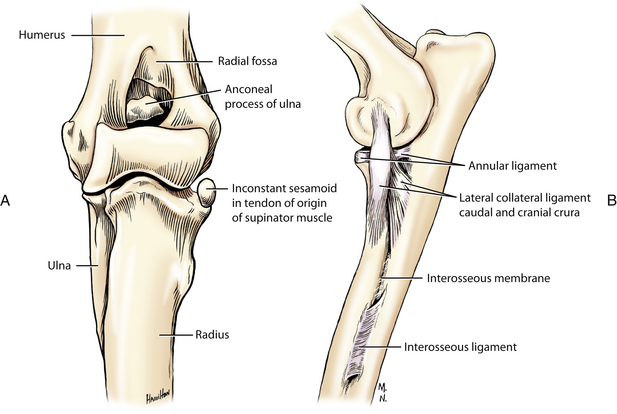
The interosseous ligament is a condensation of collagenous tissue that unites the radius and ulna proximally (Fig. 2-31).
The carpal joint is a composite of three articular levels: (1) proximally an antebrachiocarpal joint between the radius and ulna articulating with the intermedioradial and ulnar carpal bones; (2) a middle carpal joint between the two rows of carpal bones; and (3) a carpometacarpal joint between the distal row of carpal bones and the metacarpals. The carpal joint capsule extends as a sleeve from the distal ends of the radius and ulna to the metacarpus. It attaches to the carpal bones in its course across the joint and forms separate compartments. The antebrachiocarpal joint compartment does not communicate with the middle carpal joint compartment. The middle carpal and carpometacarpal joint compartments communicate between the distal row of carpal bones.
The joint capsule of the carpus differs from that of typical hinge joints in that both the dorsal and palmar surfaces are heavily reinforced by the fibrous layer of the joint capsule. On the dorsal surface of the joint, the fibrous layer of the capsule contains grooves in which the extensor tendons lie. This layer is loose between the radius and ulna proximally and the proximal row of carpals distally because most of the movement of the carpus takes place there. Cut through the joint capsule of this antebrachiocarpal joint to observe its components and the degree of movement of the joint. On the palmar side the palmar carpal ligament is a thick fibrous layer that firmly attaches to the bones of the carpus. This is important in preventing collapse of the carpus when the limb bears weight. This layer of fibrocartilage forms the deep (dorsal) boundary of the carpal canal (Fig. 2-22). Numerous ligaments within the joint capsule connect the various bones of the carpus. These will not be dissected.
The metacarpophalangeal, proximal interphalangeal, and distal interphalangeal joints are the three articulations of each main digit. Medial and lateral collateral ligaments support these joints.
Each metacarpophalangeal joint includes two proximal sesamoids in the tendons of the interossei, which articulate with the flexor surface of the metacarpal head.
BONES OF THE PELVIC LIMB
The pelvic girdle, or pelvis, of the dog consists of two hip bones, which are united at the symphysis pelvis midventrally and join the sacrum dorsally. Each hip bone, or os coxae, is formed by the fusion of three primary bones and the addition of a fourth in early life (Fig. 2-32). The largest and most cranial of these is the ilium, which articulates with the sacrum. The ischium is the most caudal, whereas the pubis is located ventromedial to the ilium and cranial to the large obturator foramen. The acetabulum, a socket, is formed where the three bones meet. It receives the head of the femur in the formation of the hip joint. The small acetabular bone, which helps form the acetabulum, is incorporated with the ilium, ischium, and pubis when they fuse (about the third month).
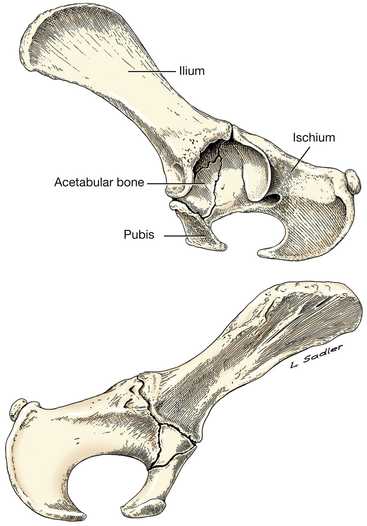
The pelvic canal is short ventrally but long dorsally. Its lateral wall is composed of the ilium, ischium, and pubis. Dorsolateral to the skeletal part of the wall, the pelvic canal is bounded by soft tissues. The pelvic inlet is limited laterally and ventrally by the arcuate line of the ilium. Its dorsal boundary is the promontory of the sacrum. The pelvic outlet is bounded ventrally by the ischiatic arch (the ischiatic arch is formed by the concave caudal border of the two ischii); mid-dorsally by the first caudal vertebra; and laterally by the superficial gluteal muscle, muscles of the pelvic diaphragm, and the sacrotuberous ligament.
Os Coxae
1. The ilium (Figs. 2-32, 2-33 through 2-35), a flat bone presenting two surfaces and three borders, forms the cranial one half to three fifths of the os coxae. It can be divided into a wide cranial part, which is concave laterally and known as the wing, and a narrow, laterally compressed caudal part, the body.
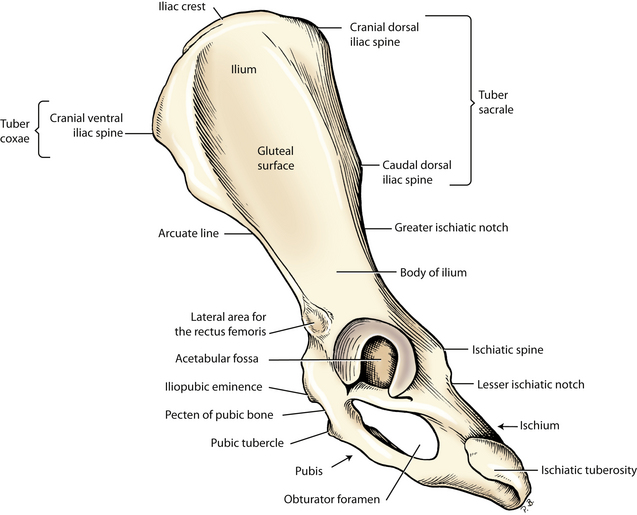
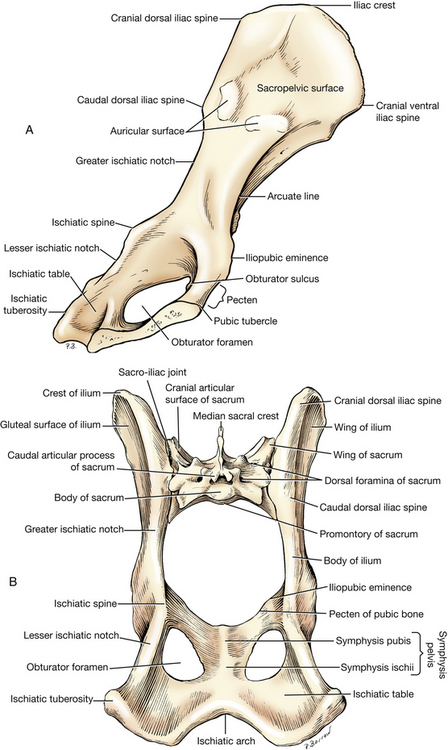
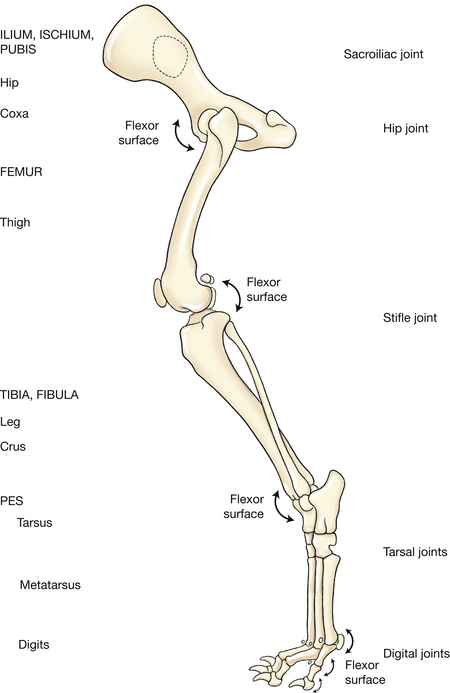
The cranial border is arciform and usually roughened and is more commonly known as the iliac crest. It is thin but gradually increases in thickness dorsally. The angle of junction of the iliac crest with the ventral border is known as the cranial ventral iliac spine, which provides a place of origin for both bellies of the sartorius and a part of the tensor fasciae latae. The tuber coxae is composed of the cranial ventral iliac spine and the adjacent part of the ventral border of the wing of the ilium. The rest of the ventral border is concave. It ends in the lateral area for the rectus femoris (Fig. 2-33) just cranial to the acetabulum.
The dorsal border of the ilium is broad and massive. The junction of the dorsal border with the iliac crest forms an obtuse angle that is a rounded prominence, the cranial dorsal iliac spine. Caudal to the cranial dorsal iliac spine is the wide but blunt caudal dorsal iliac spine. The two spines and intervening bone make up the tuber sacrale, which occupies nearly half the length of the dorsal border of the ilium. The caudal half of the dorsal border is gently concave. It forms the greater ischiatic notch and also helps form the ischiatic spine, which is dorsal to the acetabulum.
The external or gluteal surface (Fig. 2-33) of the wing of the ilium is nearly flat caudally and concave cranially, where it is limited by the iliac crest. The dorsal part of this concave area is bounded by a heavy ridge, the tuber sacrale. The gluteal surface is rough ventrocranially. The middle gluteal and a portion of the deep gluteal attach here.
The internal or sacropelvic surface (Fig. 2-34) of the wing of the ilium presents a smooth, nearly flat area that provides attachment for the iliocostalis, longissimus, and the quadratus lumborum muscles. The auricular surface is rough and articulates with a similar surface of the sacrum, forming the sacroiliac joint. The arcuate line is located along the ventromedial edge of the sacropelvic surface of the body of the ilium and runs from the auricular surface to the iliopubic eminence of the pubis. The tendon of the psoas minor attaches along the medial aspect of this line.
2. The ischium (Figs. 2-32 through 2-35) consists of tuberosity, body, table, and ramus. It forms the caudal part of the os coxae and enters into the formation of the acetabulum, obturator foramen, and symphysis pelvis. Its caudal border consists of the ischiatic tuberosity laterally and one half of the ischiatic arch medially. The ischiatic tuberosity is the thick caudolateral margin of the bone. The lateral angle of the tuber is enlarged and hooked; it furnishes attachment for the sacrotuberous ligament. The medial angle is rounded. The ventral surface is the place of origin for the biceps femoris, semitendinosus, and semimembranosus. The crus of the penis and the muscle that surrounds it also attach to the ischiatic tuberosity medially.
The body of the ischium is the part lateral to the obturator foramen. The ischiatic spine is a rounded crest dorsal to the acetabulum, where the body of the ischium meets the ilium. The coccygeus attaches here. Caudal to this spine the border of the ischium is depressed and marked by a series of low ridges produced by the tendon of the internal obturator. This area is known as the lesser ischiatic notch (Figs. 2-33, 2-34). The gemelli arise from the lateral surface adjacent to the lesser ischiatic notch.
The ramus of the ischium is the thin and wide medial part of the ischium. It is bounded laterally by the obturator foramen and blends caudally with the body of the ischium. The ramus meets its fellow at the symphysis and is fused with the pubis cranially. The ischiatic table is the flat portion where the ramus meets the body (Fig. 2-34). It faces dorsally and is the site of origin of the internal obturator muscle. The quadratus femoris and the external obturator arise from its ventral surface. The ischiatic arch is formed by the medial portion of the caudal border of each ischium.
3. The pubis (Figs. 2-32 through 2-35) extends from the ilium and ischium laterally to the symphysis medially and consists of a body and two rami. The body is located cranial to the obturator foramen. The cranial ramus extends from the body to the ilium and enters into the formation of the acetabulum. The caudal ramus fuses with the ischial ramus at the middle of the pelvic symphysis. The ventral surface of the pubis and adjacent ischial ramus serve as origin for the gracilis, the adductor, and the external obturator. The dorsal surface gives rise to a small part of the internal obturator and the levator ani. The obturator sulcus, a groove for the obturator nerve, is located at the cranial end of the obturator foramen and passes dorsally over the pelvic surface of the body of the bone. The iliopubic eminence projects from the cranial border of the cranial ramus of the pubic bone. The pectineus attaches to it. The pubic tubercle projects cranially from the pubis on the midline. The roughened cranial border of the pubis between the iliopubic eminence and the pubic tubercle is the pecten, to which the abdominal muscles attach by means of a prepubic tendon to be dissected later. The prepubic tendon is composed primarily of the tendons of the paired rectus abdominis and pectineus muscles.
The acetabulum (Figs. 2-32, 2-33) is a cavity that receives the head of the femur. Its articular surface is semilunar and is composed of parts of the ilium, ischium, and, in young animals, the acetabular bone (Fig. 2-32). In the adult the acetabular bone is fused imperceptibly with the pubis, ischium, and ilium. The circumference of the articular surface is broken at the caudomedial part by the acetabular notch. The acetabular fossa is formed by the ischium and the acetabular bone. The ligament of the head of the femur attaches in this fossa. The fossa and the notch are the nonarticular parts of the acetabulum. The two sides of the notch are connected by the transverse acetabular ligament.
The obturator foramen is closed in life by the obturator membrane and the external and internal obturator muscles that the membrane separates.
Femur
The femur (Figs. 2-35, 2-36), or thigh bone, is the largest bone in the body. The flexor angle of the hip is about 110 degrees. The flexor angle at the stifle is from 130 to 135 degrees.
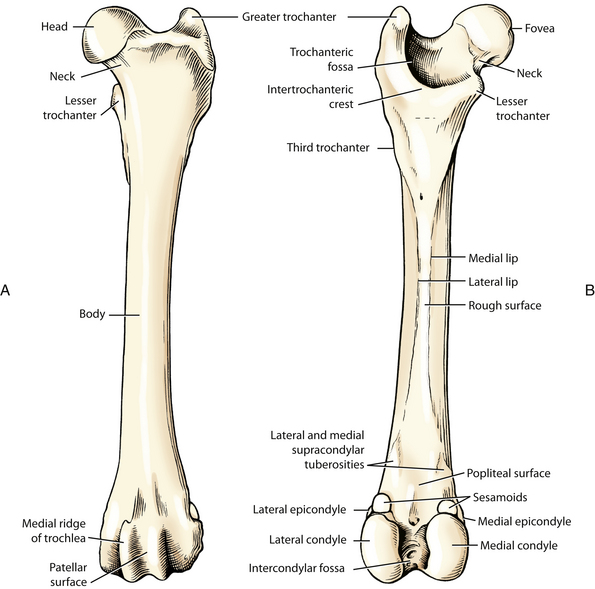
The femur is a typical long bone with a cylindrical body and two expanded extremities. The proximal extremity presents on its medial side a smooth, nearly hemispherical head, most of which is articular except for a small shallow fossa beginning near the middle of the head and usually extending to its caudomedial margin. This fossa is the fovea capitis femoris, to which the ligament of the head of the femur attaches. The head is attached to the medial part of the proximal extremity by the neck of the femur. The neck is distinct but short and provides attachment for the joint capsule. The greater trochanter, the largest eminence of the proximal extremity, is located directly lateral to the head. To it attach the middle gluteal and deep gluteal. The trochanteric fossa is a deep cavity medial to the greater trochanter. The gemelli and the external and internal obturators insert in this fossa. The lesser trochanter, a pyramidal projection at the proximal end of the medial side of the body of the femur, serves for the insertion of the iliopsoas. A ridge of bone extends from the summit of the greater trochanter to the lesser trochanter. This, the intertrochanteric crest, represents the caudolateral boundary of the trochanteric fossa. The quadratus femoris inserts on the crest at the level of the lesser trochanter. The third trochanter is poorly developed. It appears at the base of the greater trochanter as a small, rough area on which the superficial gluteal inserts. The third and lesser trochanters are located in about the same transverse plane. The vastus parts of the quadriceps femoris attach to the smooth proximal cranial part of the femur.
The body of the femur is slightly convex cranially. Viewed cranially, the body presents a smooth, rounded surface. The caudal surface is rough and is limited by medial and lateral lips. The lips, closest together in the middle of the body, diverge as they approach each extremity. The proximal part of the medial lip ends in the lesser trochanter, the distal part at the medial supracondylar tuberosity. The proximal part of the lateral lip ends in the third trochanter, the distal part at the lateral supracondylar tuberosity. The adductor inserts on most of the caudal rough surface, whereas a tendon extends from the pectineus to the distal part of the medial lip, where the semimembranosus also attaches.
The distal extremity of the femur presents several articular surfaces. The trochlea, with ridges, is the smooth groove on the craniodistal part of the bone for articulation with the patella. The medial trochlear ridge is usually thicker than the lateral. The patella is a sesamoid in the tendon of insertion of the large quadriceps femoris that extends the stifle. It aids in the protection of the tendon and the joint, but its chief purpose is redirection of the tendon of insertion of the quadriceps. The trochlea of the femur is continuous with the condyles, which articulate, both directly and through fibrocartilaginous menisci, with the tibia. The medial and lateral condyles are separated from each other by the intercondylar fossa, a deep, wide space. The two condyles are similar in shape and surface area. Each is convex transversely and longitudinally. At the depth of the intercondylar fossa the cruciate ligaments attach. On the caudodorsal aspect of each femoral condyle is a facet on which a sesamoid bone (fabella) rests. The medial and lateral fabellae are in the tendons of origin of the medial and lateral heads of the gastrocnemius muscle. Proximal to these sesamoid facets are the medial and lateral supracondylar tuberosities from which the gastrocnemii arise. The superficial digital flexor also arises from the lateral tuberosity. The popliteal surface is a large, flat, triangular area on the caudal surface of the distal extremity proximal to the condyles and intercondylar fossa. The medial and lateral epicondyles are rough areas on each side, proximal to the condyles. They serve for the attachment of the collateral ligaments of the stifle. The lateral epicondyle also gives rise to the popliteus. The small extensor fossa is located on the lateral epicondyle at the junction of the lateral condyle and the lateral lip of the trochlea; from it arises the long digital extensor. The semimembranosus is inserted just proximal to the medial epicondyle.
Tibia
The tibia (Fig. 2-37), the shin or leg bone, has a proximal articular surface that flares out transversely and is also broad craniocaudally. It is wider than the distal end of the femur, with which it articulates, and is formed largely by two relatively flat condyles. The medial condyle is separated from the lateral condyle by the intercondylar eminence. Both condyles include the articular areas on their proximal surfaces and the adjacent nonarticular parts of the proximal extremity. The lateral condyle is particularly prominent. It possesses a facet on its lateral side for articulation with the head of the fibula and provides origin for part of the peroneus longus and cranial tibial muscles. A sesamoid bone in the tendon of origin of the popliteus (seen in radiographs) articulates with the caudolateral condyle of the tibia. The semimembranosus is inserted on the medial condyle. Two biconcave fibrocartilages, the menisci, fill part of the space between the apposed condyles of the femur and tibia, making the joint congruent. The intercondylar eminence consists of two small, elongated tubercles, which form its highest part, and a shallow intercondylar area. The cranial intercondylar area is a depression cranial to the eminence and in large part between the condyles. It affords attachment to the cranial parts of the menisci and the cranial cruciate ligament. The caudal intercondylar area occupies a place similar to that of the cranial area but caudal to the eminence. It provides attachment for the caudal part of the medial meniscus. The popliteal notch is caudal to the caudal intercondylar area and is located between the two condyles. The popliteal vessels pass through the notch. The tibial tuberosity is the large quadrangular process on the proximocranial surface of the tibia. The quadriceps femoris, the biceps femoris, and the sartorius attach to this tuberosity by means of the patella and patellar ligament. The tibial tuberosity is continued distally by the cranial border of the tibia. It inclines laterally on the body. The following muscles attach wholly or in part to the cranial border of the tibia: biceps femoris, semitendinosus, gracilis, and sartorius. The extensor groove is a small, smooth groove located at the junction of the lateral condyle and the tibial tuberosity. The long digital extensor passes through it.
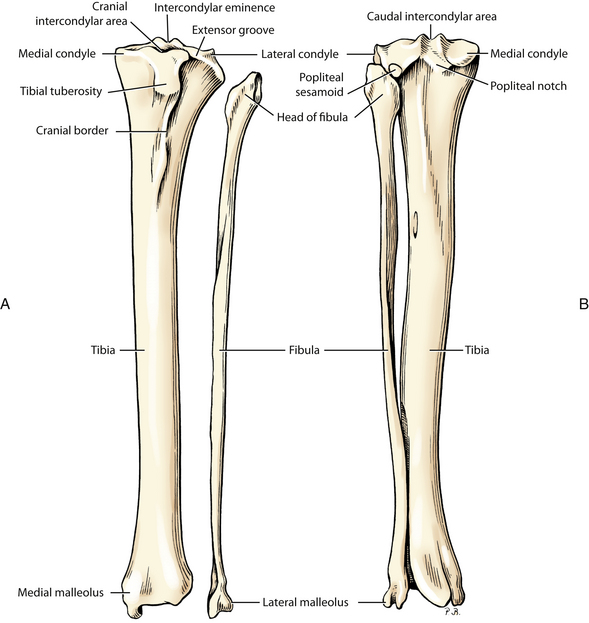
Fig. 2-37 A, Left tibia and fibula, cranial view. B, Articulated left tibia and fibula, caudal view.
The body is triangular proximally, nearly cylindrical in the middle, and four sided distally. The semitendinosus and gracilis are inserted on the proximal medial surface. The proximal third of the caudal surface serves for the insertion of the popliteus medially and for the origins of the deep digital flexor laterally.
The distal extremity of the tibia is quadrilateral in transverse section. The tibial cochlea, the articular surface, consists of two grooves that receive the ridges of the proximal trochlea of the talus. The medial part of the distal extremity of the tibia is the medial malleolus. The lateral surface of the distal extremity articulates with the fibula by a small facet. No muscles arise from the distal half of the tibia.
Fibula
The fibula (Figs. 2-35, 2-37) has proximal and distal extremities and an intermediate body. The proximal extremity, or head, articulates with the lateral condyle of the tibia. The distal extremity, the lateral malleolus, has two grooves that contain the tendons of the fibularis longus, fibularis brevis, and the lateral digital extensor. These grooves redirect the force of contraction. On the medial surface of the tibia is a distinct facet for articulation with the distolateral surface of the tibia and with the talus.
Tarsal Bones
The tarsus (Figs. 2-35, 2-38), between the metatarsals and the leg, is composed of seven tarsal bones and the related soft tissues. It is also called the hock. The bones are arranged in three irregular rows. The proximal row is composed of a long, laterally located calcaneus and a shorter, medially located talus. The talus has a trochlea on its proximal end with two ridges separated by a groove for articulation with the tibial cochlea. This is the tarsocrural joint where flexion and extension occur between the leg and hindpaw. The talus articulates with the calcaneus laterally and the central tarsal bone distally. The calcaneus articulates with the talus and the fourth tarsal bone.
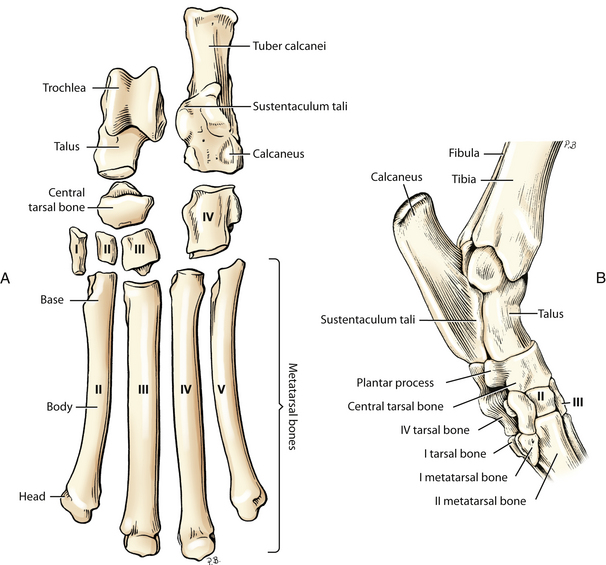
Fig. 2-38 A, Left tarsal and metatarsal bones disarticulated, dorsal view. B, Left tarsus, articulated, medial aspect. (Adapted from Evans: Miller’s anatomy of the dog, ed 3, Philadelphia, Saunders, 1993.)
The tuber calcanei is a traction process of the calcaneus that projects proximally and caudally. The extensor muscles of the hock insert on this process via the common calcanean tendon. On the medial side of the calcaneus is a bony process, the sustentaculum tali. The tendon of the lateral digital flexor glides over the plantar surface of this process.
The distal row consists of four bones. Three small bones, the first, second, and third tarsal bones, are located side by side and are separated from the proximal row by the central tarsal bone. The large fourth tarsal bone, which completes the distal row laterally, articulates with the calcaneus proximally. The fourth tarsal is as long as the combined lengths of the third and central tarsal bones against which it lies. The fourth tarsal bone is grooved on the distal half of its lateral surface for the passage of the tendon of the fibularis longus.
Metatarsal Bones
The metatarsal bones (Fig. 2-38) resemble the metacarpal bones except for the first, which may be divided, rudimentary, or absent.
Phalanges
The phalanges (Fig. 2-39) and sesamoids form the skeleton of the digit. Those of the hindpaw, or pes, are similar to those of the forepaw, or manus.
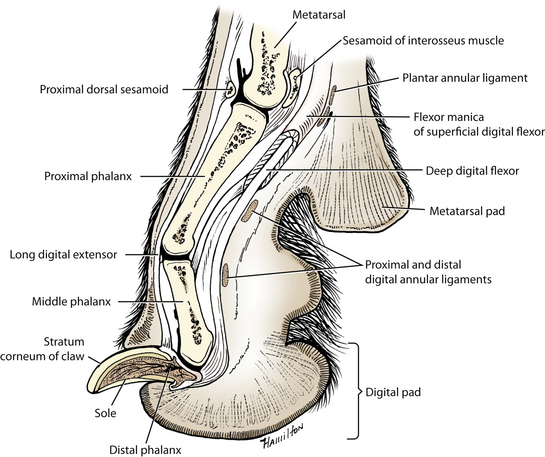
The first digit, or hallux, is frequently absent. When present, it is called a dewclaw and may vary from a fully developed digit, articulating with a normal first metatarsal bone, to a vestigial structure composed only of a terminal phalanx.
LIVE DOG
Palpate the iliac crests beside the sacrum at the cranial aspect of the pelvis, the entire length of the tuber ischii caudolaterally, and the ischiatic arch between these tuberosities. Note their symmetry. Pelvic fractures and sacroiliac luxation are common and result in palpable asymmetry.
Palpate the greater trochanter of the femur lateral to the hip. Place your thumb in the groove between the greater trochanter and the ischial tuberosity. Rotate the thigh laterally and note the displacement of your thumb by the greater trochanter. This will not occur when there is a hip luxation.
At the distal end of the femur, palpate the trochlea and the edges of the patella that articulate with it. Palpate the condyles of the femur and tibia. Flex, extend, and rotate the stifle to appreciate the level of this articulation. The tibial tuberosity and cranial border are palpable on the proximal tibia. Feel the body of the tibia where it is subcutaneous on the medial side. Palpate the narrow distal tibia and fibula. Flex and extend the tarsocrural joint, and on the dorsal aspect feel the ridges of the trochlea of the talus and the intermediate ridge of the cochlea of the tibia that participate in this joint. Palpate the tuber calcanei and note how a proximal pull on this lever will extend the joint. A fracture of this will cause the joint to overflex, and the dog will walk partly plantigrade.
MUSCLES OF THE PELVIC LIMB
Remove the skin from the caudal part of the left half of the trunk, the pelvis, and the thigh. Continue the midventral incision from the umbilicus to the root of the tail. In making this incision, closely circle the external genital parts and the anus. Extend an incision distally on the medial surface of the left thigh to the tarsus. Encircle the tarsus with a skin incision. First, reflect the skin from the medial surface of the thigh and crus and then, starting at the tarsus, reflect the whole flap of skin from the lateral surface of the leg, stifle, thigh, pelvis, and abdomen to the mid-dorsal line. The cutaneus trunci may be removed with the skin because it is more intimately attached to the skin than to the underlying structures.
There are superficial and deep fasciae of the pelvic limb. They cannot always be separated, and, in general, the deep one is more dense.
The superficial fascia of the trunk (Fig. 2-40) continues dorsally on the pelvis as the superficial gluteal fascia. In obese specimens much fat is present between this fascia and the deep fascia. The cutaneus trunci arises as an aponeurosis from the superficial gluteal fascia. It may be examined in the skin just reflected and in the previous dissection. Its fibers run cranioventrally to the caudal part of the axilla. Its most ventral border lies in the fold of the flank; dorsally, it is separated from its fellow by a narrow band of fascia over the lumbar area and pelvis. The superficial gluteal fascia passes to the tail as the superficial caudal fascia and continues distally on the limb as the superficial lamina of the fascia lata. Remove the fat-laden areolar tissue and the superficial fascia covering the caudal part of the trunk and pelvis. Do not cut into the glistening deep fascia underneath.
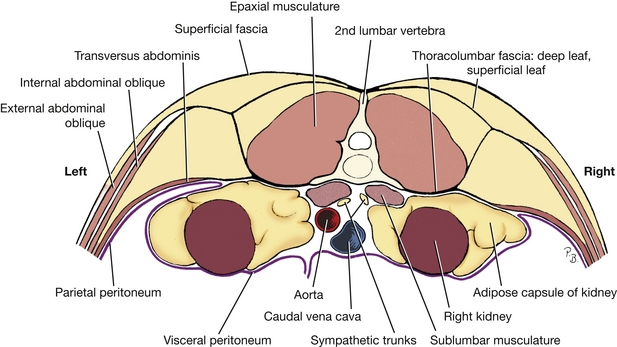
A thick deep fascia covers the dorsal muscles of the lumbar area, pelvis, and tail. The thoracolumbar fascia, which is the deep fascia of the trunk (Figs. 2-40, 2-41) is well developed in the lumbar region and is continued caudally at the iliac crest by the deep gluteal fascia. This distinct glistening fascia covers the muscles of the pelvis and serves in part as origin for the middle and superficial gluteals. The deep gluteal fascia is continued caudally on the tail by the deep caudal fascia. The latter follows the irregularities of the caudal muscles and closely binds these to the vertebrae of the tail. Distally, the deep gluteal fascia blends with the fascia of the thigh, where it becomes the medial and lateral femoral fasciae. The medial fascia is thin, whereas the lateral femoral fascia, the fascia lata, is thick and serves as an aponeurotic insertion for thigh muscles. The femoral fascia is continued on the leg as the crural fascia. Clean but do not cut any of the deep fascia until instructed to do so.
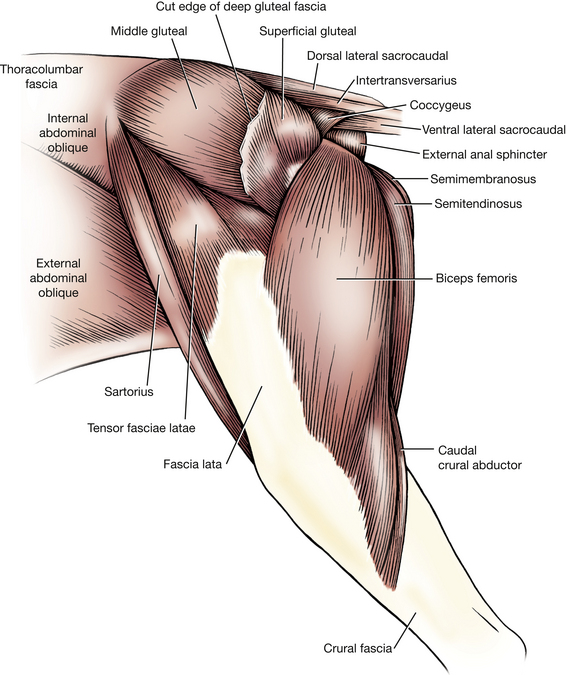
Caudal Muscles of the Thigh
This group consists of three primary muscles: biceps femoris, laterally; semitendinosus, caudally; and semimembranosus, medially. (A slender caudal crural abductor muscle is closely associated with the mediocaudal surface of the biceps [Figs. 2-41, 2-43].)
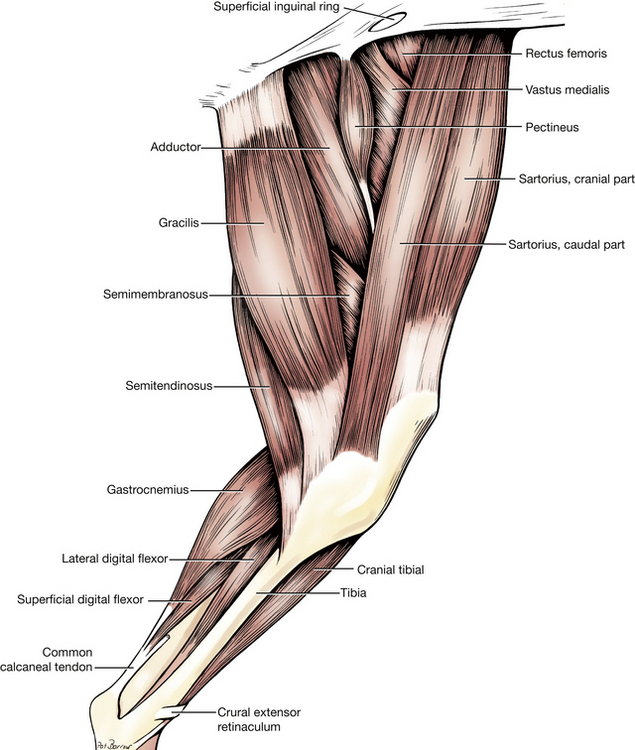
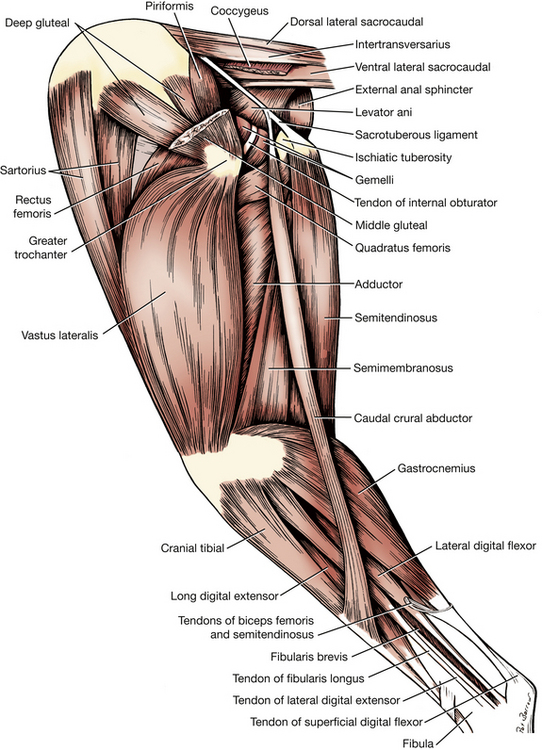
1. The biceps femoris (Figs. 2-41, 2-44, 2-45, 2-47, 2-52, 2-54 through 2-57) is the longest and widest of the muscles of the thigh. The bulk of its fibers run craniodistally, although caudally there are fibers that run directly distally. Identify the lateral aspect of the tuber ischii and the sacrotuberous ligament that extends from it to the sacrum. The biceps femoris arises from these structures. Cranially, it inserts by means of the fascia lata and crural fascia. Carefully clean the caudal border and the adjacent surface of the muscle. The lymph node lying in the fat at its caudal border directly caudal to the stifle is the popliteal lymph node. Do not cut the cranially lying fascia lata, which serves as part of its insertion. Caudally, a strand of heavy fascia runs to the tuber calcanei and helps to form the common calcanean tendon. Transect the biceps femoris. The sciatic nerve is interposed between the biceps femoris and the adductor. Observe the insertions of the biceps femoris.
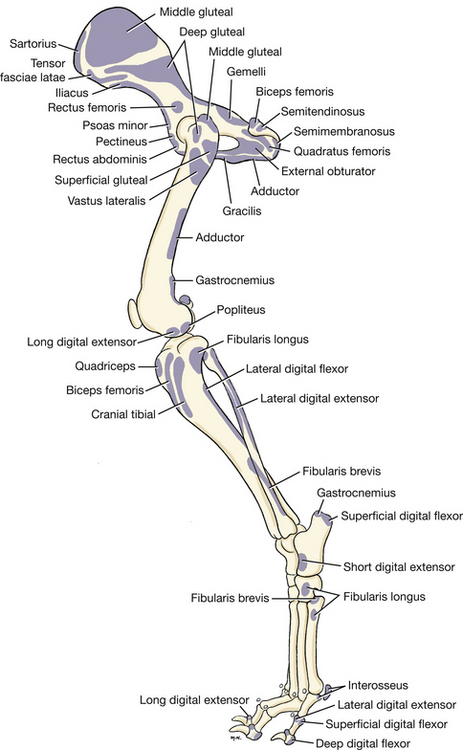
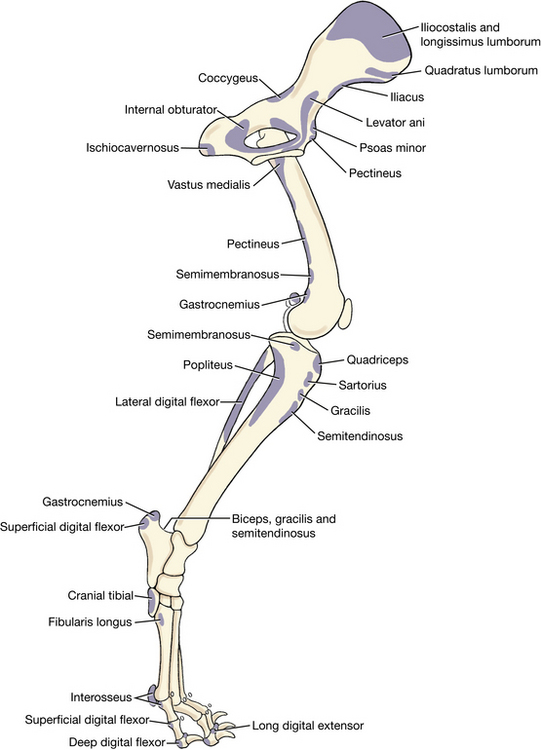
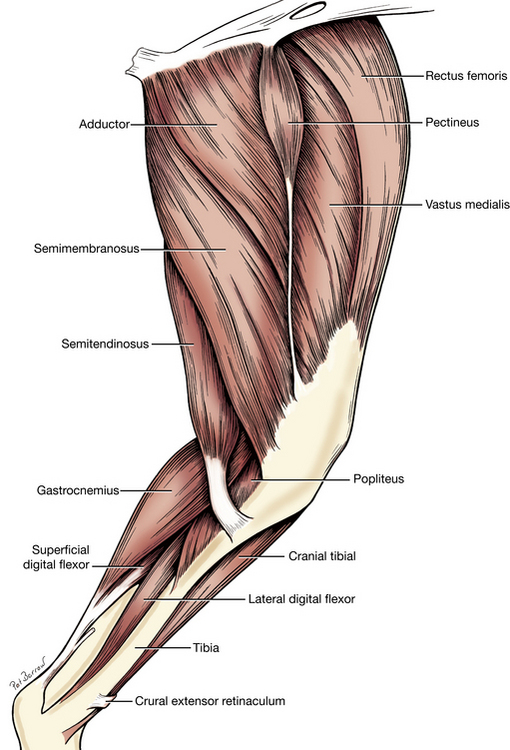
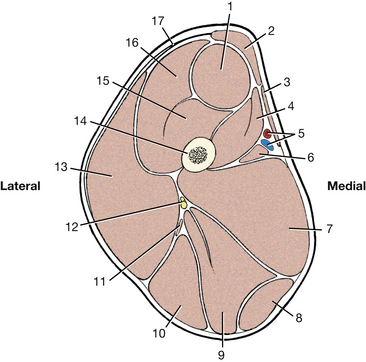
ORIGIN: The sacrotuberous ligament and the ischiatic tuberosity.
INSERTION: By means of the fascia lata and crural fascia to the patella, patellar ligament, and cranial border of the tibia; by means of the crural fascia to the subcutaneous part of the tibial body; the tuber calcanei.
ACTION: To extend the hip, stifle, and hock. The caudal part of the muscle flexes the stifle.
2. The semitendinosus (Figs. 2-41 through 2-47, 2-52, 2-54, 2-55, 2-57), near its origin, lies between the biceps femoris and semimembranosus. Near its insertion it lies on the medial head of the gastrocnemius and is covered by the gracilis. It is nearly as wide as it is thick and extends principally from the ischiatic tuberosity to the tibial body. By means of the crural fascia, it also attaches to the tuber calcanei. Completely free this muscle from surrounding structures but do not transect it.
ORIGIN: The ischiatic tuberosity.
INSERTION: The disto-cranial border of the tibia. The medial surface of the body of the tibia and the tuber calcanei by means of the crural fascia.
ACTION: To extend the hip, flex the stifle, and extend the hock.
3. The semimembranosus (Figs. 2-41 through 2-47, 2-50, 2-52, 2-57) is greater in transverse sectional area than the semitendinosus but is not as long. It is wedged between the semitendinosus and biceps femoris laterally and the gracilis and adductor medially. It has two bellies of nearly equal size. This short but thick muscle extends from the ischiatic tuberosity to the medial side of the distal end of the femur and the proximal end of the tibia. The insertions may be seen more adequately after the sartorius and gracilis muscles have been dissected.
ORIGIN: The ischiatic tuberosity.
INSERTION: The distal medial lip of the caudal rough surface of the femur and the medial condyle of the tibia.
ACTION: To extend the hip. The part that attaches to the femur extends the stifle; the part that attaches to the tibia flexes or extends the stifle, depending on the position of the limb.
Medial Muscles of the Thigh
1. The sartorius (Figs. 2-41 through 2-45, 2-47, 2-52) consists of two straplike parts that lie on the cranial and craniomedial surfaces of the thigh. These parts extend from the ilium to the tibia. The cranial part forms the cranial contour of the thigh and may be nearly 1 cm thick there. The caudal part is on the medial side of the thigh and is thinner, wider, and longer than the cranial part. Both muscle parts lie predominantly on the medial side of the large quadriceps femoris. Transect both parts and reflect the distal parts to their insertions on the patella and cranial border of the tibia.
ORIGIN: Cranial part—the crest of the ilium and the thoracolumbar fascia; caudal part—the cranial ventral iliac spine and the adjacent ventral border of the ilium.
INSERTION: Cranial part—the patella, in common with the rectus femoris of the quadriceps; caudal part—the cranial border of the tibia, in common with the gracilis.
ACTION: To flex the hip. The cranial part extends the stifle; the caudal part flexes the stifle.
2. The gracilis (Figs. 2-42, 2-44, 2-45, 2-47, 2-52, 2-54, 2-55) arises from the symphysial tendon, a thick, flat tendon attached ventrally to the symphysis pelvis. The aponeurosis of the gracilis covers the adductor. Transect the gracilis through its aponeurotic origin. Reflect it distally and observe its insertion as well as that of the semitendinosus on the cranial border of the tibia.
ORIGIN: The pelvic symphysis by means of the symphysial tendon.
INSERTION: The cranial border of the tibia and, with the semitendinosus, the tuber calcanei.
ACTION: To adduct the limb, flex the stifle, and extend the hip and hock.
The femoral triangle (Fig. 2-79) is the shallow triangular space through which the femoral vessels run to and from the pelvic limb. It is located on the proximal medial surface of the thigh with its base at the abdominal wall. The triangle lies between the caudal belly of the sartorius cranially and the pectineus and adductor caudally. The iliopsoas and rectus femoris form the proximal lateral part of the triangle. The vastus medialis forms the distal lateral part. This triangle contains, among other structures, the femoral artery and vein. Remove the medial femoral fascia and adipose tissue that covers and fills in around the femoral artery and vein. Notice that the vein lies caudal to the artery. The pulse is usually taken from the femoral artery here.
3. The pectineus (Figs. 2-42, 2-44 through 2-47, 2-49, 2-50) is a small, spindle-shaped muscle that belongs to the deep medial muscles of the thigh. It lies between the adductor caudally and the vastus medialis cranially. It has an origin on the prepubic tendon and iliopubic eminence. There is a small cartilage imbedded in the iliopubic origin. By blunt dissection with the handle of the scalpel, isolate the tendon of insertion on the caudomedial surface of the distal end of the femur. Transect the pectineus in the middle of its belly.
ORIGIN: From the iliopubic eminence and the pubic tubercle via the prepubic tendon.
INSERTION: The distal end of the medial lip of the caudal rough face of the femur.
4. The adductor (Figs. 2-42 through 2-44, 2-46, 2-47, 2-49, 2-50, A) consists of two muscles (adductor magnus et brevis and adductor longus) that are often not clearly divisible. It is a large pyramidal muscle compressed between the semimembranosus and pectineus that extends from the pelvic symphysis to the caudal aspect of the femur. It is partly covered by the biceps femoris laterally and gracilis medially. Transect the adductor at its origin along the symphysis. Do not transect the external obturator, which lies even deeper.
ORIGIN: The entire pelvic symphysis by means of the symphysial tendon, the adjacent part of the ischiatic arch, and ventral surface of the pubis and ischium.
INSERTION: The entire lateral lip of the caudal rough face of the femur.
Lateral Muscles of the Pelvis
1. The tensor fasciae latae (Figs. 2-41, 2-44) is a triangular muscle that attaches proximally to the tuber coxae. It lies between the sartorius cranially, the middle gluteal caudodorsally, and the quadriceps distomedially. Part of its caudodorsal surface is attached to the middle gluteal near its origin. The muscle can be divided into two portions. The cranial, more superficial portion is inserted on the lateral femoral fascia, which radiates over the quadriceps and blends with the fascial insertion of the biceps femoris. The deeper caudal portion is inserted on a layer of lateral femoral fascia that runs deep to the biceps toward the stifle on the lateral surface of the vastus lateralis. Transect the tensor fasciae latae across its middle and reflect the two halves toward their attachments.
ORIGIN: The tuber coxae and adjacent part of the ilium; the aponeurosis of the middle gluteal muscle.
INSERTION: The lateral femoral fascia.
ACTION: To tense the lateral femoral fascia, flex the hip, and extend the stifle.
INNERVATION: Cranial gluteal nerve.
2. The superficial gluteal (Figs. 2-41, 2-44, 2-50) is small and lies caudal to the middle gluteal. Its fibers run distally, from the deep gluteal fascia that covers the middle gluteal and from the sacrum and the first caudal vertebra to the level of the greater trochanter of the femur, where they converge before forming an aponeurosis that runs under the biceps to the third trochanter. Clean the superficial gluteal and transect it 1 cm from the beginning of its aponeurosis of insertion. Do not transect the caudally lying sacrotuberous ligament (Figs. 2-43, 2-58). This is a collagenous band that runs from the sacrum to the lateral angle of the ischiatic tuberosity. Notice that the superficial gluteal arises from the proximal half of this ligament. Sever the deep gluteal fascia 1 cm cranial to its junction with the muscle fibers of the superficial gluteal.
ORIGIN: The lateral border of the sacrum and the first caudal vertebra, partly by means of the sacrotuberous ligament; the cranial dorsal iliac spine by means of the deep gluteal fascia.
INSERTION: The third trochanter.
ACTION: To extend the hip and abduct the limb.
INNERVATION: Caudal gluteal nerve.
3. The middle gluteal (Figs. 2-41, 2-43, 2-44, 2-50, 2-57) is a large, ovoid muscle that lies between the tensor fasciae latae and the superficial gluteal. Clean the surface of the muscle by reflecting the deep gluteal fascia dorsocranial to the iliac crest. This reveals that the fibers of the muscle for the most part parallel its long axis. Carefully separate the cranioventral part of the middle gluteal from the underlying deep gluteal. The entire caudodorsal border of the middle gluteal is covered by the superficial gluteal. The deep caudal portion of the middle gluteal is readily separated from the main muscle mass and is called the piriformis muscle (Fig. 2-43). Starting at the middle of the cranioventral border of the middle gluteal, transect the entire muscle and reflect the distal half toward its insertion on the apex of the greater trochanter of the femur.
ORIGIN: The crest and gluteal surface of the ilium.
INSERTION: The greater trochanter.
ACTION: To extend and abduct the hip and to rotate the pelvic limb medially.
INNERVATION: Cranial gluteal nerve.
4. The deep gluteal (Figs. 2-43, 2-44, 2-48, 2-50) is fan shaped and completely covered by the middle gluteal. Its fibers converge to insert on the cranial face of the greater trochanter.
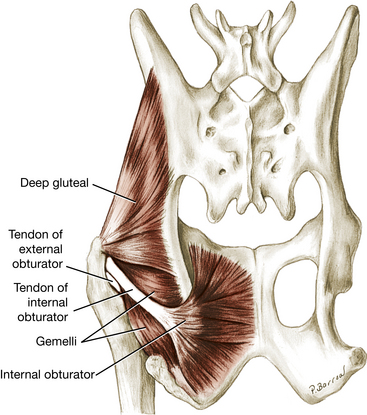
ORIGIN: The body of the ilium; the ischiatic spine.
INSERTION: The cranial aspect of the greater trochanter.
ACTION: To extend and abduct the hip and to rotate the pelvic limb medially.
INNERVATION: Cranial gluteal nerve.
The articularis coxae (Fig. 2-50, B) is a small, spindle-shaped muscle lying on the craniolateral aspect of the hip joint capsule. It is covered by the deep gluteal muscle. It arises from the lateral surface of the ilium along with the rectus femoris and inserts on the neck of the femur. (No dissection is necessary.)
Caudal Hip Muscles
The four muscles of this group are important because of their proximity to the hip. They lie caudal to the hip and extend from the inner and outer surfaces of the ischium to the femur. All rotate the limb laterally. This action opposes the medial rotation by the gluteals so that the thigh moves in a sagittal plane at the hip.
1. The internal obturator (Figs. 2-43, 2-45, 2-48, 2-50) is fan shaped on the dorsal surface of the ischium and pubis. Its muscle fibers converge toward the lesser ischiatic notch. The body of the muscle may be exposed at its origin on the dorsal surface of the ischium by removing the loose fat and the fascia caudomedial to the sacrotuberous ligament. The most caudal fibers of the internal obturator run craniolaterally toward the lesser ischiatic notch, where the tendon of the muscle begins. The tendon of the internal obturator passes over the lesser ischiatic notch ventral to the sacrotuberous ligament. Transect the sacrotuberous ligament and reflect the adjacent soft tissues to expose the tendon of insertion of the internal obturator muscle running to the trochanteric fossa. Transect the tendon of the internal obturator as it crosses the gemelli and reflect it to observe the bursa that lies between the tendon and the lesser ischiatic notch.
ORIGIN: The symphysis pelvis and the dorsal surface of the ischium and pubis.
INSERTION: The trochanteric fossa of the femur.
ACTION: To rotate the pelvic limb laterally at the hip.
2. The gemelli (Figs. 2-43, 2-44, 2-48, 2-50), two muscles fused together, lie under the tendon of the internal obturator. They are interposed between the quadratus femoris and external obturator distally and the deep gluteal proximally. The gemelli are deeply grooved by the tendon of the internal obturator so that their edges overlap this tendon.
ORIGIN: The lateral surface of the ischium, caudal to the acetabulum and ventral to the lesser ischiatic notch.
INSERTION: The trochanteric fossa.
ACTION: To rotate the pelvic limb laterally at the hip.
3. The quadratus femoris (Figs. 2-43, 2-44, 2-49, 2-50) is short and thick. It lies deep to the biceps femoris, where it is interposed between the adductor medially, the biceps femoris laterally, and the external obturator and gemelli dorsally. Its fibers are at right angles to the long axis of the thigh. It should be examined from both the medial and lateral sides. The dorsal border of the quadratus femoris lies closely applied to the ventral border of the gemelli.
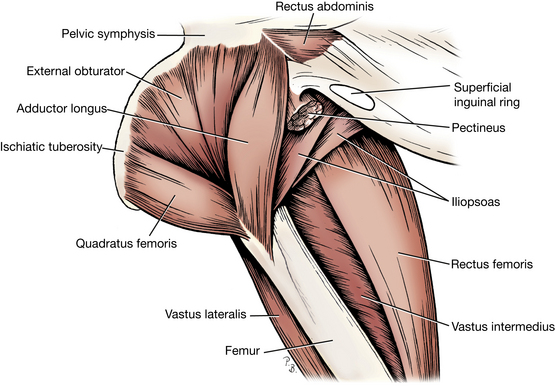
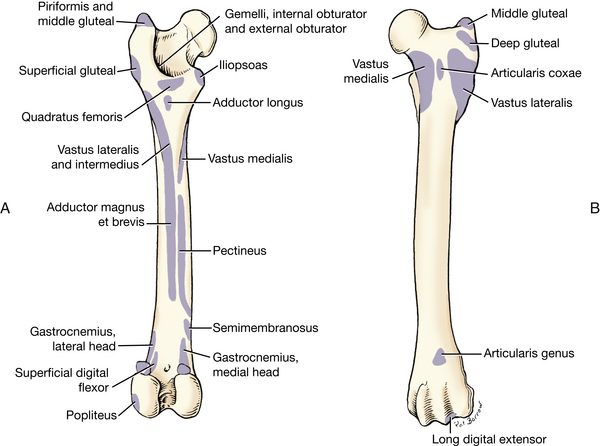
ORIGIN: The ventral surface of the caudal part of the ischium.
INSERTION: Intertrochanteric crest.
ACTION: To extend the hip and rotate the pelvic limb laterally.
4. The external obturator (Figs. 2-44, 2-48 through 2-50) is fan shaped and arises on the ventral surface of the pubis and ischium. It covers the obturator foramen. Its caudal border is covered by the quadratus femoris, whereas its cranial border is hidden by the adductor. Follow the external obturator to its insertion.
ORIGIN: The ventral surface of the pubis and ischium.
INSERTION: The trochanteric fossa.
Cranial Muscles of the Thigh
1. The quadriceps femoris (Figs. 2-42 through 2-47, 2-49, 2-50, 2-52, 2-57) is divided into four heads of origin, which are fused distally. It arises from the femur and the ilium and is inserted on the tibial tuberosity. The patella lies in the tendon of insertion. This muscle is the most powerful extensor of the stifle and is necessary for the animal to support its weight.
The patella, a sesamoid bone, is intercalated in the large tendon of insertion of the quadriceps. It articulates with the trochlea of the femur.
The patellar ligament extends from the patella to the tibial tuberosity. It is the distal end of the tendon of insertion of the quadriceps.
The rectus femoris (Figs. 2-42 through 2-44, 2-46, 2-47, 2-49) is the most cranial component of the quadriceps femoris and the only one to arise from the ilium. Proximally, it is circular in transverse section and passes between the vastus medialis and the vastus lateralis. Uncover the rectus femoris near its origin. Transect and reflect the proximal part. The rectus arises from the ilium cranial to the acetabulum and inserts on the tibial tuberosity. It is a flexor of the hip as well as an extensor of the stifle.
The vastus lateralis (Figs. 2-43, 2-44, 2-47, 2-49, 2-50) lies lateral and caudal to the rectus femoris, to which it is fused distally. The vastus lateralis is partly separated from the vastus intermedius by a scantily developed intermuscular septum. Notice that the vastus lateralis arises from the proximal part of the lateral lip of the caudal rough surface of the femur. It is inserted with the rectus femoris on the tibial tuberosity.
The vastus intermedius (Figs. 2-47, 2-49, 2-50) lies directly on the smooth cranial surface of the femur and is quite intimately fused with the other two vasti. It arises with the vastus lateralis, which covers it, from the lateral side of the proximal end of the femur. It inserts on the tibial tuberosity with the other members of the group.
The vastus medialis (Figs. 2-42, 2-45 through 2-47, 2-50) arises from the medial side of the proximal end of the cranial surface of the femur and the proximal end of the medial lip of the caudal rough surface. It is inserted with the other heads of the quadriceps on the tibial tuberosity.
ORIGIN: Rectus femoris—ilium; vasti muscles—proximal femur.
ACTION: To extend the stifle and flex the hip (rectus).
2. The iliopsoas (Figs. 2-44, 2-45, 2-49 through 2-51, 2-57), a sublumbar muscle, is now visible at its insertion on the lesser trochanter of the femur. This end of the muscle lies between the pectineus medially and the rectus femoris laterally. The iliopsoas represents a fusion of the psoas major and iliacus muscles. The psoas major is long and arises from transverse processes and bodies of lumbar vertebrae. It passes caudally and ventrally under the cranioventral aspect of the ilium, where it joins the iliacus. The iliacus (Fig. 2-51) is short and arises from the smooth ventral surface of the ilium between the arcuate line and the lateral border of the ilium. The two muscle masses continue caudoventrally as the iliopsoas to their conjoined insertion on the lesser trochanter. The action of the iliopsoas is to flex the hip and the lumbar vertebral column. It is the major flexor of the hip. Do not dissect it at this time but study the illustration of the deep dissection of sublumbar muscles.
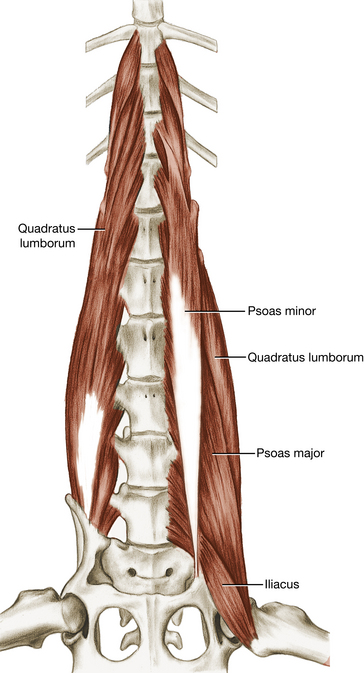
ORIGIN: Psoas major—lumbar vertebrae; iliacus—cranioventral ilium.
INNERVATION: Ventral branches of lumbar spinal nerves; femoral nerve.
Muscles of the Leg (Crus)
The muscles of the leg, or crus, the region between the stifle and hock, are divided into craniolateral and caudal groups. Note that the leg is not the pelvic limb. Remove the skin that remains on the distal part of the pelvic limb to the level of the proximal interphalangeal joints.
The superficial crural, tarsal, metatarsal, and digital fasciae are similar to the superficial fasciae of the corresponding regions of the forelimb. Cutaneous vessels and nerves course in the superficial fascia. One such vessel is the cranial branch of the lateral saphenous vein, which is used for venipuncture.
The medial and lateral femoral fasciae blend over the stifle and are continued distally in the leg as the deep crural fascia. The deep crural fascia covers the muscles of the leg and the free-lying surfaces of the crural skeleton. Septa from this fascia extend between the muscles to attach to the bone. Laterally, the fibers of the caudal branch of the biceps femoris radiate into it. Medially, the semitendinosus and gracilis are continuous with this fascia. These connections are located caudally where the crural fascia contributes to the common calcanean tendon.
Just proximal to the flexor surface of the tarsus, the deep crural fascia is thickened to form an oblique band of about 0.5 cm, the crural extensor retinaculum. As it stretches obliquely from the distal third of the fibula to the medial malleolus of the tibia, it binds down the tendons of the long digital extensor and the cranial tibial muscles.
The deep crural fascia decreases in thickness as it passes over the tarsus and becomes the deep tarsal fascia. A fibrous loop that attaches to the calcaneus wraps around the tendon of the long digital extensor. This is the tarsal extensor retinaculum. The deep fascia extends into the metatarsal and digital pads and closely joins these pads with the overlying skeletal and ligamentous parts. Make an incision through the cranial crural fascia and reflect it to the common calcanean tendon and the tibia.
Craniolateral Muscles of the Leg
1. The cranial tibial (Figs. 2-42 through 2-46, 2-52 through 2-57) is the most cranial muscle of this group. Its medial margin is in contact with the tibia. It arises from the cranial border and the adjacent proximal articular margin of the tibia. Its tendon inserts on the plantar surface of the base of the first and second metatarsals. The tendon of the cranial tibial runs under the crural extensor retinaculum and is provided with a synovial sheath over most of the flexor surface of the tarsus.
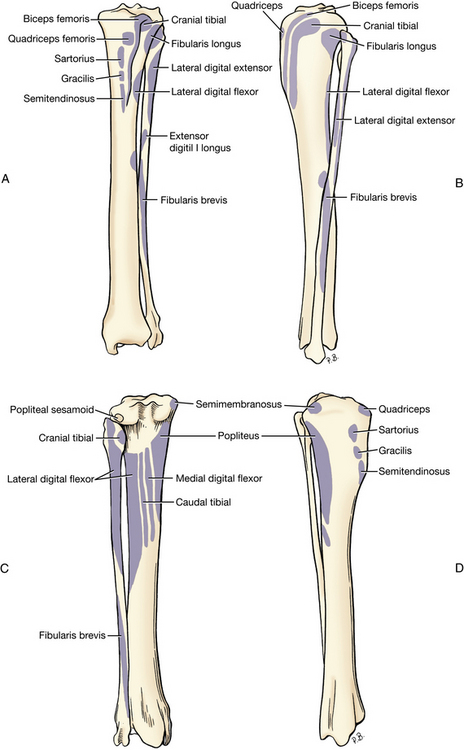
Fig. 2-52 A, Left tibia and fibula with muscle attachments, cranial view. B, Left tibia and fibula with muscle attachments, lateral view. C, Left tibia and fibula with muscle attachments, caudal view. D, Left tibia and fibula with muscle attachments, medial view.
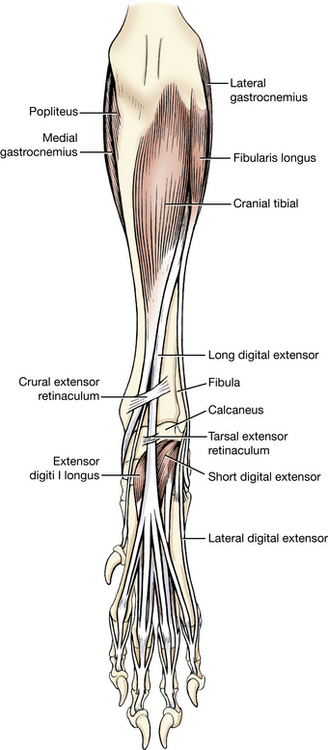
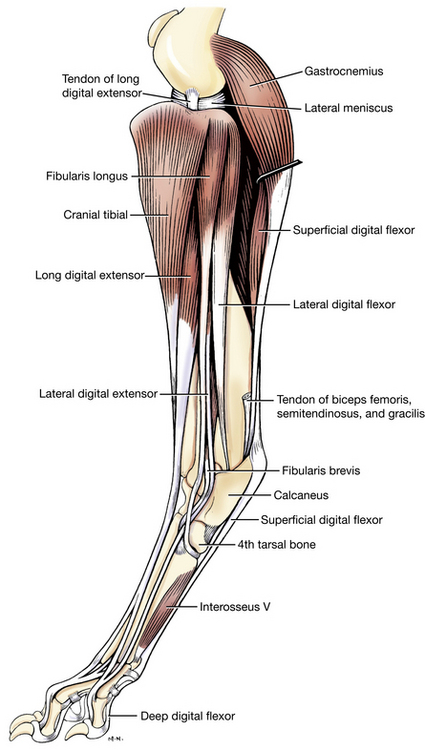
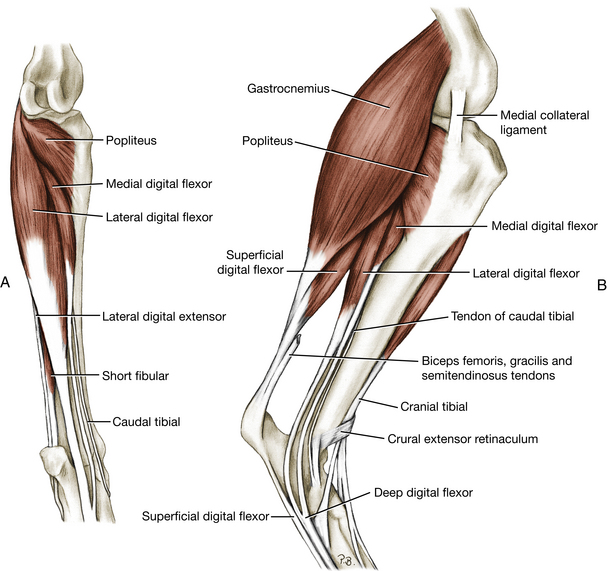
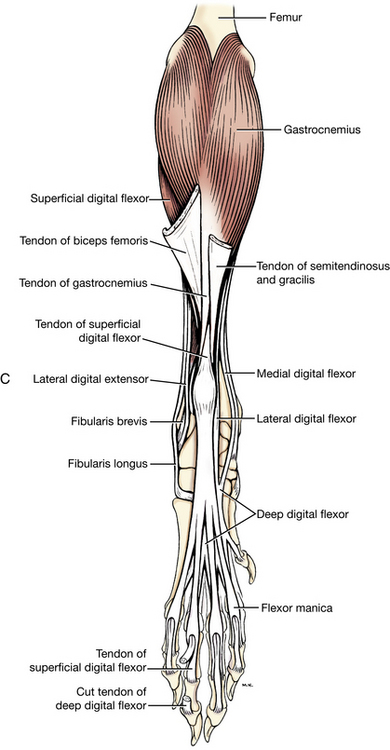
Fig. 2-55 A, Deep muscles of left crus, caudal view. B, Muscles of left crus, medial aspect.
C, Muscles of left pelvic limb, caudal view.
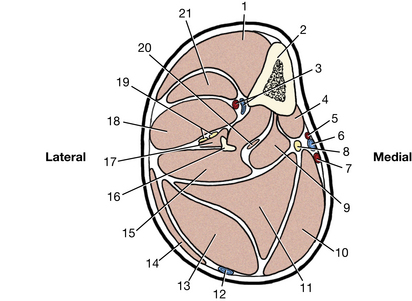
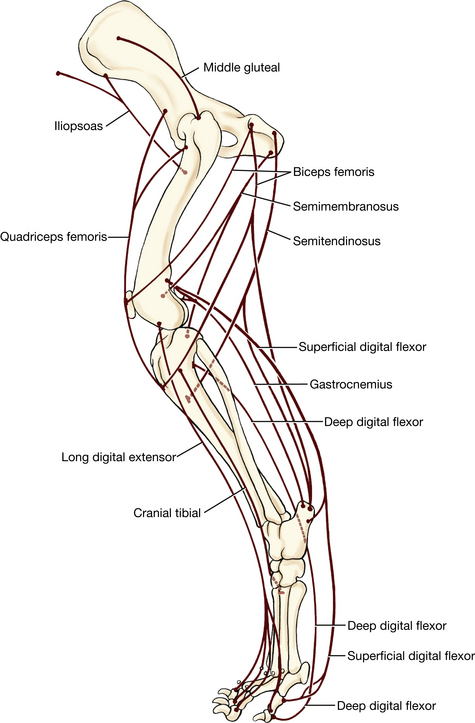
ORIGIN: The extensor groove and the adjacent articular margin of the tibia; the lateral edge of the cranial tibial border.
INSERTION: The plantar surface of the base of metatarsals I and II.
ACTION: To flex the tarsocrural joint and to rotate the paw laterally so that the plantar surface faces medially.
2. The long digital extensor (Figs. 2-43 through 2-45, 2-50, 2-53, 2-54, 2-56, 2-57) is a spindle-shaped muscle that is partly covered by the cranial tibial medially and the fibularis longus laterally. Expose the muscle and its tendon of origin from the extensor fossa of the femur. The tendon runs over the articular margin of the tibia in the extensor groove and is lubricated by an extension of the stifle joint capsule. In the distal crus it runs under the crural extensor retinaculum (Fig. 2-53). Observe the four tendons of insertion. As the tendons pass over the tarsus, they are surrounded by a synovial sheath and are held in place by the tarsal extensor retinaculum (Fig. 2-53). In the metatarsus the four tendons diverge toward their respective digits, where they insert on the extensor process of the distal phalanx.
ORIGIN: The extensor fossa of the femur.
INSERTION: The extensor processes of the distal phalanges of digits II, III, IV, and V.
ACTION: To extend the digits and flex the tarsus.
3. The fibularis longus (Figs. 2-43, 2-44, 2-52 through 2-56) lies just caudal to the long digital extensor, where a triangular portion of its short belly lies directly under the crural fascia. It is a short, thick, wedge-shaped muscle that lies in large part cranial to the fibula. It arises from the lateral collateral ligament of the stifle and the adjacent parts of the tibia and fibula. Its stout tendon courses distally on the lateral side of the fibula caudal to the crural extensor retinaculum. It has a long synovial sheath that begins at a plane through the crural extensor retinaculum and extends to its insertion on the fourth tarsal and the plantar surfaces of the base of all metatarsals. Open the synovial sheath at its proximal end. Preserving all ligaments and tendons that lie superficial to the tendon, trace it to its insertion on the fourth tarsal. Do not dissect the tendon beyond this attachment. Notice that it lies in a sulcus of the lateral malleolus of the fibula and that at the distal end of the tarsus it makes nearly a right angle as it turns medially around a groove in the fourth tarsal bone and courses to the plantar side.
ORIGIN: The lateral condyle of the tibia, the proximal end of the fibula, and the lateral epicondyle of the femur by means of the lateral collateral ligament of the stifle.
INSERTION: The fourth tarsal bone; the plantar aspect of the base of the metatarsals.
ACTION: To flex the tarsus and rotate the paw medially so that the plantar surface faces laterally.
The lateral digital extensor and the fibularis brevis (Figs. 2-43, 2-44, 2-52 through 2-55) are located beneath the peroneus longus on the lateral aspect of the leg and need not be dissected.
Caudal Muscles of the Leg
1. The gastrocnemius muscle (Figs. 2-42 through 2-46, 2-50, 2-53 through 2-57) consists of two heads that enclose the superficial digital flexor between them. These muscles form the caudal bulge of the leg (calf) and contribute the major component of the common calcanean tendon.
The two heads of the gastrocnemius arise from the medial and lateral supracondylar tuberosities of the femur. In each tendon of origin there is a sesamoid bone that articulates with the caudodorsal aspect of the femoral condyle.
Identify the lateral and medial heads of the gastrocnemius and follow them to their union as a common tendon that inserts on the proximal dorsal surface of the tuber calcanei. The superficial digital flexor muscle, which is hidden proximally between the two heads of the gastrocnemius, emerges distally as a superficial tendon that passes over the medial surface of the gastrocnemial tendon, caps the tuber calcanei, and continues over the plantar surface of the paw. With a probe, separate the gastrocnemius from the superficial digital flexor by entering between their tendons. Proximally, bluntly separate the superficial digital flexor from the heads of the gastrocnemius.
The superficial digital flexor has a common origin with the lateral head of the gastrocnemius—the lateral supracondylar tuberosity of the femur—and is closely adherent to that head. Transect each head of the gastrocnemius and reflect them proximally to see their origin and the associated sesamoid bones.
ORIGIN: The medial and lateral supracondylar tuberosities of the femur.
INSERTION: The proximal dorsal surface of the tuber calcanei.
ACTION: To extend the tarsus and flex the stifle.
2. The superficial digital flexor ( Figs. 2-42 through 2-46, 2-50, 2-54 through 2-57) is a spindle-shaped muscle that arises from the lateral supracondylar tuberosity of the femur with the lateral head of the gastrocnemius. Its deep surface is in apposition to the deep digital flexor and the popliteus, whereas its other surfaces are largely covered by the gastrocnemius. Proximal to the calcaneal process, its tendon passes from deep to superficial by crossing the medial surface of the gastrocnemius tendon. Farther distally the tendon widens, caps the tuber calcanei, attaches on each side, and continues distally. Make a sagittal incision through the superficial digital flexor tendon from the place where it gains the caudal side of the gastrocnemius to the tuber calcanei. Continue the incision distal to the tuber calcanei for an equal distance. Observe the large calcaneal bursa of the superficial digital flexor that lies under its tendon as it crosses the tuber calcanei. Notice the distinct medial and lateral attachments of the tendon on the tuber calcanei. Opposite the distal plantar surface of the tarsus, the tendon bifurcates; each of these branches in turn bifurcates, thus forming four tendons of nearly equal size. Each tendon is disposed in its digit as the corresponding tendon in the forepaw. They need not be dissected.
ORIGIN: The lateral supracondylar tuberosity of the femur.
INSERTION: The tuber calcanei and the bases of the middle phalanges of digits II, III, IV, and V.
ACTION: To flex the first two digital joints of the four principal digits; flex the stifle; extend the tarsus.
3. The deep digital flexor (Figs. 2-42 through 2-46, 2-52, 2-54 through 2-57) and the popliteus are the principal muscles yet to be dissected on the caudal surface of the leg. The separation between them runs distomedially. Transect the superficial digital flexor proximal to its tendon to expose these muscles. The two muscles that compose the deep digital flexor are now exposed.
The lateral digital flexor (formerly the flexor hallucis longus) (Figs. 2-44, 2-46, 2-52, 2-54, 2-56) arises from the caudolateral border of the proximal two thirds of the tibia, most of the proximal half of the fibula, and the adjacent interosseous membrane. Its tendon begins as a wide expanse on the caudal side of the muscle but condenses distally. Medial to the tuber calcanei, it is surrounded by the tarsal synovial sheath and bound in the groove over the sustentaculum tali of the calcaneus by the flexor retinaculum. At the level of the distal row of tarsal bones, observe the tendon of the lateral digital flexor joining that of the medial digital flexor to form a common tendon. The courses, relations, and attachments of the tendons distal to the tarsus are similar to those of the deep flexor tendon of the forelimb. Their dissection is not necessary.
The medial digital flexor (Figs. 2-52, 2-55, 2-56) is smaller and lies between the lateral digital flexor and the popliteus. From the proximal end of the tibia, it runs distomedially. Its tendon lies on the caudomedial side of the tibia. At the distal row of tarsal bones, it unites with the tendon of the lateral digital flexor.
ORIGIN: The caudal aspect of the proximal two thirds of the tibia, the proximal half of the fibula, and the adjacent interosseous membrane.
INSERTION: The flexor tubercle on the plantar surface of the base of each of the distal phalanges.
ACTION: To flex the digits and extend the tarsus.
4. The popliteus (Figs. 2-44 through 2-46, 2-50, 2-52, 2-53, 2-56) is covered by the gastrocnemius and the superficial digital flexor and lies on the stifle joint capsule and caudal surface of the proximal tibia. It arises from the lateral epicondyle of the femur by a long tendon that should be isolated just cranial to the lateral collateral ligament of the stifle. It courses caudally, medial to the lateral collateral ligament. At the junction of the tendon with the muscle, there is a sesamoid that articulates with the caudal aspect of the lateral condyle of the tibia. The muscle portion starts at the lateral tibial condyle and extends to the proximal third of the tibia on the medial side of the leg. Transect the popliteus at the tendomuscular junction and reflect it proximally to observe the sesamoid. The popliteus inserts on the proximal third of the tibia.
ORIGIN: The lateral epicondyle of the femur.
INSERTION: The proximal third of the caudal surface of the tibia.
LIVE DOG
Palpate the middle gluteal on the lateral side of the wing of the ilium. Follow it to its termination on the greater trochanter. Palpate the quadriceps femoris cranially in the thigh and feel the straplike sartorius along its cranial edge. Follow the quadriceps distally to its patella and the patellar ligament with its termination on the tibial tuberosity. Proximally, in the thigh feel the tensor fasciae latae between the sartorius and the quadriceps. Palpate the muscle mass in the caudal thigh. This includes, from lateral to medial, the biceps femoris, semitendinosus, semimembranosus, and gracilis. Feel the spindle-shaped pectineus proximally in the medial thigh on the caudal border of the femoral triangle. Abduct the limb and feel this muscle tighten. Palpate the pulse in the femoral artery just cranial to this muscle. The pulse rate and quality are usually determined here.
Grasp the tail and press down on the floor of the pelvis just cranial to the ischial arch. The muscle here is the internal obturator. The depression here between the tail and anus medially, superficial gluteal laterally, and internal obturator ventrally is the ischiorectal fossa, where perineal hernias occur.
Caudal to the stifle, feel for the popliteal lymph node between the distal ends of the biceps femoris and semitendinosus. In the leg, feel the craniolateral muscles that are the flexors of the tarsus and extensors of the digits. Proximally, their muscle bellies fill the concave surface of the body of the tibia. Caudally, feel the two gastrocnemius muscles proximally. Trace them from their origin on the distal femur to where their tendons join and form part of the common calcanean tendon. Follow this common tendon to the tuber calcanei. Feel the division between the gastrocnemius tendon and the tendon of the superficial digital flexor. Follow the latter on the plantar side of the tuber calcanei. Palpate the digital flexors distally in the caudal leg area and plantar aspect of the tarsus.
JOINTS OF THE PELVIC LIMB
The ischium and pubis of the right and left sides are joined on the median plane at the symphysis pelvis.
The sacroiliac joint (Figs. 2-58, 2-59) is an articulation of stability rather than mobility. The right and left wings of the ilia articulate with the broad right and left wings of the sacrum. In the adult most of the apposed articular surfaces are united by fibrocartilage that surrounds a small area of articulating hyaline cartilage with synovial fluid. Around the periphery of the articular areas, bands of strong collagenous tissue, the dorsal and ventral sacroiliac ligaments, reinforce the fibrocartilage. Do not dissect this joint.
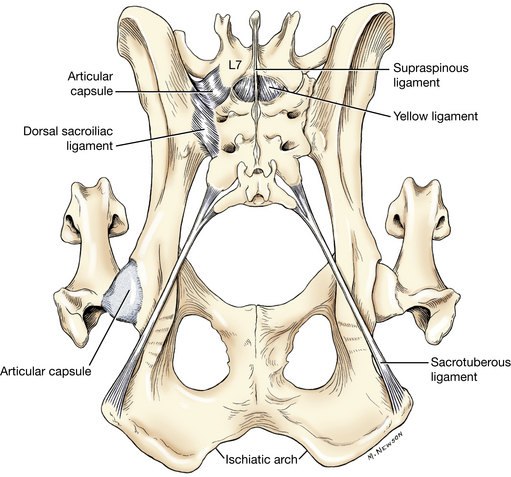
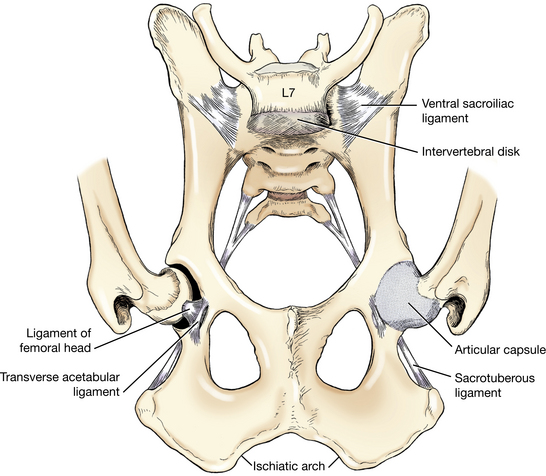
The sacrotuberous ligament (Figs. 2-58, 2-59) runs from the transverse processes of the last sacral and first caudal vertebrae to the lateral angle of the ischiatic tuberosity. It serves as an origin for several muscles that have been dissected.
The hip joint (Figs. 2-58, 2-59) is a ball-and-socket joint whose main movements are flexion and extension. This joint can move in any direction, but the opposed action of the medial and lateral rotator muscles limits the movement to primarily flexion and extension. The joint capsule passes from the neck of the femur to a line peripheral to the acetabular lip. Transect the deep gluteal and iliopsoas muscles at their insertions. Cut the hip joint capsule to expose the joint and associated ligaments. Consider the various muscles that may be encountered by surgical approaches to the hip from different directions.
The ligament of the femoral head (Fig. 2-59) is a thick band of collagenous tissue that extends from the acetabular fossa to the fovea capitis. At its acetabular attachment it may blend slightly with the transverse acetabular ligament. A synovial membrane covers it. Transect this ligament.
The transverse acetabular ligament (Fig. 2-59) is a small band that extends from one side of the acetabular notch to the opposite side. It is located at the ventrocaudal aspect of the acetabulum and continues as the acetabular lip, which deepens the acetabulum by forming a fibrocartilaginous border around it.
The joint capsule of the stifle (Figs. 2-60 through 2-64) forms three sacs. Two of these are between the femoral and tibial condyles (femorotibial joint sacs), and the third is beneath the patella (femoropatellar joint sac). All three sacs communicate with one another. The femorotibial joint sacs extend caudally and dorsally to incorporate the articulation of the gastrocnemial sesamoids. The lateral femorotibial sac continues distally through the extensor groove as the tendon sheath for the tendon of origin of the long digital extensor (Figs. 2-60, C, 2-61). It also surrounds the tendon of origin of the popliteus. Between each femoral condyle and the corresponding tibial condyle, there is a meniscus, or semilunar fibrocartilage, that develops in the joint capsule. The articular surface of the meniscus is continuous with the synovial layer of the joint sac. These are C-shaped disks with thick peripheral margins and thin, concave central areas that compensate for the incongruence that exists between the femur and tibia.
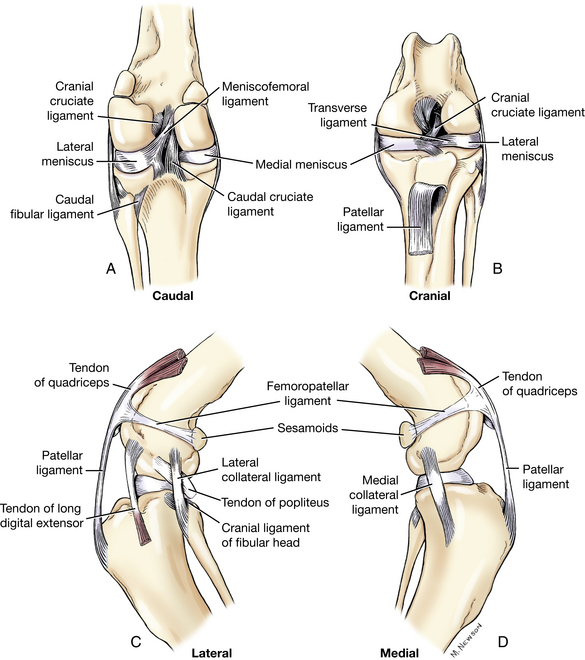
Fig. 2-60 A, Ligaments of left stifle joint, caudal view. B, Ligaments of left stifle joint, cranial view. C, Ligaments of left stifle joint, lateral view. D, Ligaments of left stifle joint, medial view.
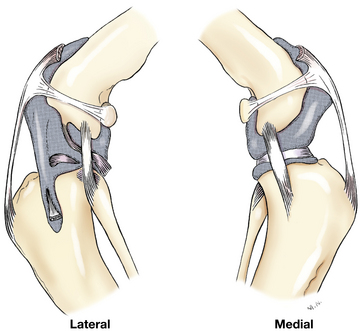
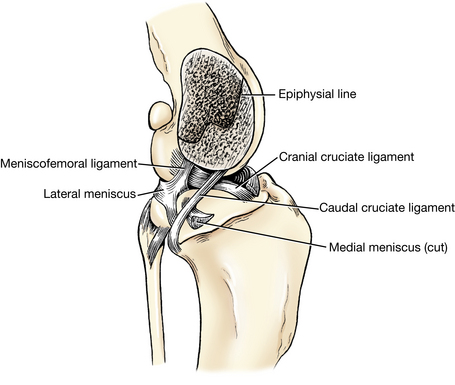
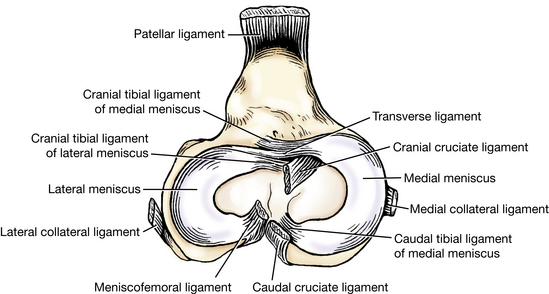
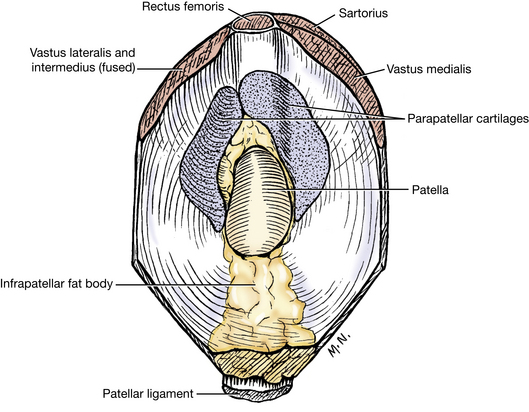
Clean the remaining fascia and related muscle attachments away from the stifle. Note the medial and lateral femoropatellar ligaments, which are thin fascial bands extending between the patella and the gastrocnemial sesamoid on each side (Figs. 2-60, 2-61). Transect the patellar ligament and reflect it proximally. Note the large quantity of fat between the patellar ligament and the joint capsule. Medial and lateral parapatellar fibrocartilages extend from the patella (Fig. 2-64). Note the proximal extent of the femoropatellar joint sac. Remove the fat around the joint, open the joint capsule, and remove as much joint capsule as necessary to observe the following ligaments.
Each meniscus attaches to the cranial and caudal intercondylar areas of the tibia (Fig. 2-63) via the cranial and caudal meniscotibial ligaments. A transverse ligament connects the cranial ends of the menisci. The caudal part of the lateral meniscus is attached to the intercondylar fossa of the femur by a meniscofemoral ligament (Figs. 2-60, 2-62, 2-63). The medial meniscus is attached to the medial collateral ligament and moves only slightly when the stifle is flexed. The lateral meniscus is separated from the lateral collateral ligament by the tendon of origin of the popliteus. When the stifle joint is flexed, the tibia rotates medially and the lateral meniscus moves caudally on the tibial condyle.
The femorotibial ligaments are the collateral and cruciate ligaments. The medial collateral ligament extends from the medial epicondyle of the femur to the medial side of the tibia distal to the medial condyle. It fuses with the lateral aspect of the medial meniscus.
The lateral collateral ligament extends from the lateral epicondyle of the femur over the tendon of origin of the popliteus to the head of the fibula and adjacent lateral condyle of the tibia. Clean these ligaments to observe their attachments. With the stifle extended, these ligaments prevent abduction, adduction, and rotation of the stifle. When the stifle joint is flexed, the lateral ligament is loosened.
The cruciate ligaments pass between the intercondylar areas of the tibia and femur and limit craniocaudal motion of these bones. The ligaments cross each other near their attachments in the intercondylar fossa of the femur.
The cranial cruciate ligament attaches within the intercondylar fossa of the femur to the caudomedial part of the lateral condyle. It extends distocranially to attach to the cranial intercondylar area of the tibia. This attachment is just behind the cranial attachment of the medial meniscus. The cranial cruciate ligament keeps the tibia from sliding cranially beneath the femur when the limb bears weight. It also limits medial rotation of the tibia when the stifle is flexed.
The caudal cruciate ligament attaches proximally within the intercondylar fossa of the femur to the medial condyle of the femur. Distally, it attaches to the medial edge of the popliteal notch of the tibia behind the caudal attachment of the medial meniscus. This ligament prevents caudal movement of the tibia beneath the femur when the limb bears weight. Observe the attachments of these ligaments. They are named in accordance with the position of their tibial attachments.
Flex the stifle and, while holding the femur firmly in one hand, try to move the tibia cranially with the other. In the normal dog there is no movement. Transect the tibial attachment of the cranial cruciate ligament and repeat the procedure. The excessive cranial excursion of the tibia that results is diagnostic for a ruptured cranial cruciate ligament.
Transect the collateral ligaments to observe the effect on the joint. Note the menisci and their attachments.
The two tibiofibular joints are a proximal joint between the head of the fibula and the lateral condyle of the tibia and a distal joint between the lateral malleolus of the fibula and the lateral surface of the distal end of the tibia. Throughout the length of the interosseous space between the tibia and fibula is a sheet of fibrous tissue uniting the two bones, the interosseous membrane of the crus.
The tarsal joint is a composite of several articulations and joint sacs. The tarsocrural joint sac is the largest and incorporates the articulations of the distal tibia and fibula with that of the talus and calcaneus. Greatest movement in the tarsus occurs between the cochlea of the tibia and the trochlea of the talus. Puncture to obtain synovia is made into this joint sac. Other joint sacs include the proximal and distal intertarsal sacs and the tarsometatarsal sac. Medial and lateral collateral ligaments cross the tarsus from the tibia and fibula to the metatarsal bones. Numerous ligaments join the individual tarsal bones to each other. These will not be dissected.
LIVE DOG
Place the thumb of one hand behind the greater trochanter. With the other hand, grasp the femur and flex and extend and rotate the hip. Try to lift the femoral head out of the acetabulum. This will be prevented by the ligament of the femoral head and joint capsule. To enter the hip joint with a needle, first palpate the cranial surface of the greater trochanter. Insert the needle here and pass it through the gluteal muscles in a medial and slightly ventral direction.
Stand behind the dog and palpate each stifle. Feel the patellar ligament and notice the normal slight depression caudal to it on the medial side. When the joint is swollen, this is less evident. Remember that there is fat between the patellar ligament and the stifle joint capsule.
With the dog recumbent, extend the stifle and palpate the patella. Move it laterally and medially. You should not be able to luxate the normal patella. Palpate the ridges of the trochlea. Follow them distally to the femoral condyles. Palpate the tibial condyles and the collateral ligaments of the stifle. With the stifle extended, rotate the tibia medially and laterally to test the integrity of the collateral ligaments. Flex the stifle, repeat this rotation, and note the normal increase in rotation, especially medially. This medial rotation is limited by the cranial cruciate ligament. Keep the stifle flexed and hold the femur with one hand while attempting to move the tibia cranially and caudally with the other hand to determine the integrity of the cruciate ligaments. To enter the stifle joint with a needle, pass the needle caudally on either side of the patellar ligament through the fat pad.
Palpate the tarsus. Flex and extend the tarsocrural joint and feel the ridges of the trochlea of the talus on the dorsal aspect. Inflammation of this joint will cause this joint sac to enlarge. To enter the tarsocrural joint with a needle, extend the joint and palpate the lateral ridge of the trochlea of the talus. Pass the needle through the fascia into the joint on either side of this ridge.
BONES OF THE VERTEBRAL COLUMN AND THORAX
The vertebral column (Fig. 2-1) consists of approximately 50 irregular bones. The vertebrae are arranged in five groups: cervical, thoracic, lumbar, sacral, and caudal. The first letter or abbreviation of the word designating each group followed by the number of vertebrae in each group expresses a vertebral formula. That of the dog is C7T13L7S3Cd20. The number of caudal vertebrae may vary. The three sacral vertebrae fuse to form what is considered a single bone, the sacrum.
A typical vertebra consists of a body; a vertebral arch consisting of right and left pedicles and laminae; and transverse, spinous, and articular processes (Figs. 2-68, 2-69).
The body of a vertebra is constricted centrally. The cranial extremity is convex, and the caudal extremity is concave. Adjacent vertebral bodies are connected by intervertebral discs, each of which is a fibrocartilaginous structure composed of a soft center, the nucleus pulposus, surrounded by concentric layers of dense fibrous tissue, the anulus fibrosus. These intervertebral discs will be dissected when the spinal cord is studied.
The vertebral arch is subdivided into basal parts, the pedicles, and the dorsal portion, formed by two laminae. Together with the body the vertebral arch forms a short tube, the vertebral foramen. All the vertebral foramina join to form the vertebral canal. The pedicles of each vertebra extend from the dorsolateral surface of the body. They present smooth-surfaced notches. The cranial vertebral notches are shallow; the caudal vertebral notches are deep. When the vertebral column is articulated, the notches of adjacent vertebrae and the intervening fibrocartilage form the right and left intervertebral foramina. Through these pass the spinal nerves and blood vessels. The dorsal part of the vertebral arch is composed of right and left laminae, which unite to form a spinous process. Each typical vertebra has, in addition to the dorsally located spinous process, or spine, paired transverse processes that project laterally from the region where the arch joins the vertebral body. Farther dorsally on the arch, at the junction of pedicle and lamina, are located the articular processes. There are two of these on each side of the vertebra: a cranial pair whose articulating surfaces point dorsally or medially and a caudal pair whose surfaces are directed ventrally or laterally.
Cervical Vertebrae
There are seven cervical vertebrae in most mammals. The atlas (Figs. 2-65, 2-67), or first cervical vertebra, is atypical in both structure and function. It articulates with the skull cranially. Its chief peculiarities are modified articular processes, a lack of a spinous process, and a reduction of its body half of when become the dens of the axis. The lateral shelflike transverse processes are thick, forming the wings of the atlas. These are united by the body (ventral arch) ventrally and arch dorsally. The two cranial articular foveae articulate with the occipital condyles of the skull to form the atlanto-occipital joint, of which the main movement is flexion and extension. The caudal articular foveae consist of two shallow glenoid cavities that form a freely movable articulation with the second cervical vertebra. Rotatory movement occurs at this atlantoaxial joint. Examine the caudal part of the dorsal surface of the body for the fovea dentis. This is concave from side to side and articulates with the dens of the second cervical vertebra. This articular area blends laterally with the caudal articular fovea. Besides the large vertebral foramen through which the spinal cord passes, there are two pairs of foramina in the atlas. The transverse foramina are actually short canals that pass obliquely through the transverse processes of the atlas and contain the vertebral artery and vein. The lateral vertebral foramina perforate the cranial part of the vertebral arch. The first cervical spinal nerves pass through these foramina.
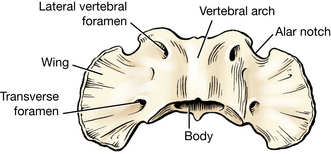
The axis, or second cervical vertebra (Figs. 2-66, 2-67), presents an elongated, ridgelike spinous process as its most prominent characteristic. It is also unlike other vertebrae in that cranially the body projects forward in a peglike eminence, the dens. The ventral surface of the dens is articular, whereas the tip and dorsal surface may be rough because of ligamentous attachment. The cranial articular surface is located on the body and is continuous with the articular area of the dens. The caudal part of the vertebral arch has two articular processes that face ventrolaterally. At the root of the transverse process is the small transverse foramen. The cranial vertebral notch concurs with that of the atlas to form the first intervertebral foramen for the transmission of the second cervical nerve (Fig. 2-67). The caudal notch concurs with that of the third cervical vertebra to form the second intervertebral foramen, through which the third cervical nerve passes. Other features of this bone are similar to those of a typical vertebra.
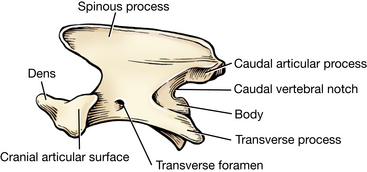
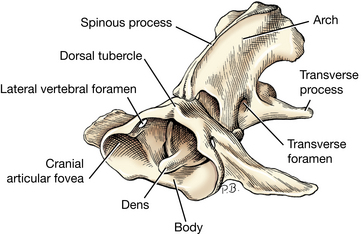
The middle three cervical vertebrae (Fig. 2-68) differ little from a typical vertebra. The spinous processes are low but gradually increase in height from third to fifth. The transverse processes are two pronged and are perforated at the base by a transverse foramen.
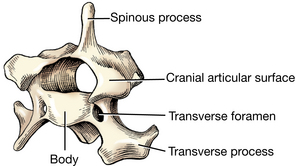
The sixth cervical vertebra has a high spine and an expanded ventral lamina of the transverse process. The seventh cervical vertebra (Fig. 2-69) lacks transverse foramina and has the highest cervical spine.
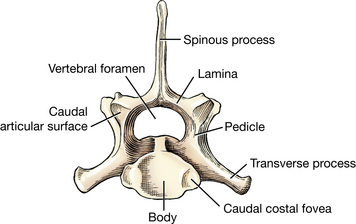
The cranial articular processes of cervical vertebrae 3 to 7 face dorsally and cranially in apposition to the caudal articular processes of adjacent vertebrae. There is a prominent ventral crest on the caudal midventral aspect of the vertebral body.
Thoracic Vertebrae
There are 13 thoracic vertebrae (Fig. 2-70); the first nine are similar. The bodies of the thoracic vertebrae are short. The first through the tenth have a cranial and a caudal costal fovea on each side for rib articulation. Because the foveae of two adjacent vertebrae form the articular surface for the head of one rib, they are sometimes called demifacets. The body of the tenth vertebra frequently lacks caudal foveae, whereas the eleventh through the thirteenth have only one complete cranial costal fovea on each side. The head of the first rib articulates between the last cervical and first thoracic vertebrae. The tubercles of the ribs articulate with the transverse processes of the thoracic vertebrae of the same number in all instances.

Fig. 2-70 A, Sixth thoracic vertebra, left lateral view. B, Twelfth and thirteenth thoracic vertebrae, left lateral view.
The spine is the most conspicuous feature of each of the first nine thoracic vertebrae. The massiveness of the spines gradually decreases with successive vertebrae, but there is little change in length and direction until the seventh or eighth vertebra is reached. The spines then become progressively shorter and incline caudally through the ninth and tenth. The spine of the eleventh thoracic vertebra is nearly perpendicular to the long axis of that bone. This vertebra is designated the anticlinal vertebra. All spines caudal to the eleventh vertebra point cranially; all spines cranial to the eleventh vertebra point caudally (Fig. 2-75).
The transverse processes are short, blunt, and irregular. All contain costal foveae for articulation with the tubercles of the ribs.
The articular processes are located at the junctions of the pedicles and the laminae. The cranial pair are nearly confluent at the median plane on thoracic vertebrae 3 through 10. Similar to cervical vertebrae 3 through 7, the cranial articular surfaces of thoracic vertebrae 1 through 10 face dorsally and slightly craniomedially. Because the caudal articular processes articulate with the cranial ones of the vertebra behind, they are similar in shape but face in the opposite direction. The joints between thoracic vertebrae 10 to 13 are conspicuously modified because the articular surfaces of the caudal articular processes are located on the lateral side and the articular surfaces of the cranial articular processes of thoracic vertebrae 11 through 13 face medially. A similar arrangement is seen in all lumbar vertebrae. This type of interlocking articulation allows flexion and extension of the caudal-thoracic and lumbar region while limiting lateral movement.
The accessory process (Fig. 2-70, B) projects caudally from the pedicle ventral to the caudal articular process and over the dorsal aspect of the intervertebral foramen. It is present from the midthoracic region to the fifth or sixth lumbar vertebra. The mamillary process is a knoblike dorsal projection of the transverse processes of the second through tenth thoracic vertebrae and cranial articular processes of the eleventh thoracic through the caudal vertebrae. Epaxial muscles of the transversospinalis system attach to these processes.
Lumbar Vertebrae
The lumbar vertebrae (Fig. 2-71) have longer bodies than the thoracic vertebrae. The transverse processes are directed cranially as well as ventrolaterally. The articular processes lie mainly in sagittal planes. The caudal processes protrude between the cranial ones of succeeding vertebrae. The prominent blunt spinous processes are largest in the midlumbar region and have a slight cranial direction. The seventh lumbar vertebra is slightly shorter than the other lumbar vertebrae.
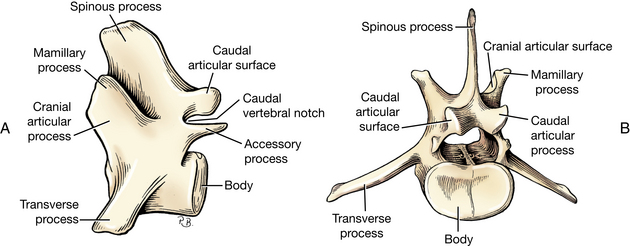
Sacrum
The sacrum (Fig. 2-72) results from the fusion of the bodies and processes of three vertebrae. This bone lies between the ilia and firmly articulates with them.
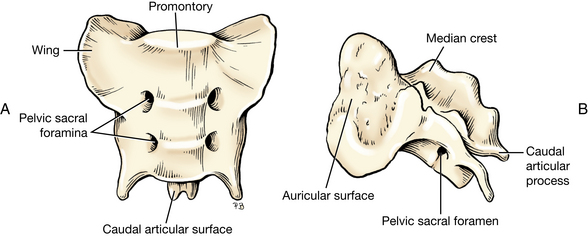
The body of the first segment is larger than the combined bodies of the other two segments. The three are united to form a concave ventral surface.
The dorsal surface presents several markings that result from the fusion of the three sacral vertebrae. The median sacral crest represents the fusion of the three spinous processes. The dorsal surface also bears two pairs of dorsal sacral foramina, which transmit the dorsal branches of the first two sacral spinal nerves.
The pelvic (ventral) surface has two pairs of pelvic sacral foramina. They transmit the ventral branches of the first two sacral spinal nerves. The wing of the sacrum is the enlarged lateral part that bears a large, rough surface, the auricular face, which articulates with the ilium.
The base of the sacrum faces cranially. The ventral part of the base has a transverse ridge, the promontory. This, with the ilia, forms the dorsal boundary of the pelvic inlet.
Caudal Vertebrae
The average number of caudal vertebrae (Fig. 2-73) in the dog is 20. These lose their distinctive features as one proceeds caudally.
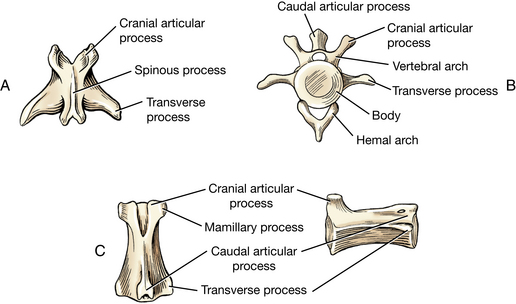
Ribs
All 13 pairs of ribs (Figs. 2-74, 2-75) have dorsal bony and ventral cartilaginous parts that meet at a costochondral junction. This junction may be expanded in rapidly growing animals. The cartilaginous parts are called costal cartilages. The first nine pairs of ribs articulate directly with the sternum. The costal cartilages of the tenth, eleventh, and twelfth unite with one another to form the costal arch. The thirteenth rib often ends freely in the flank. The bony part of a typical rib presents a head, neck, tuberculum, and body.
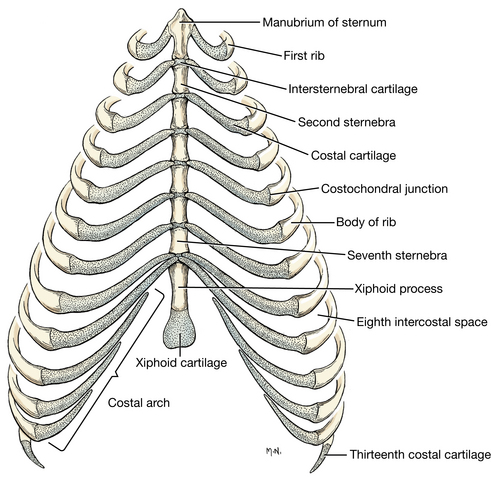
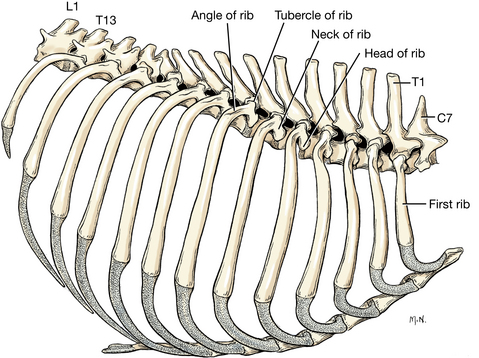
The head of ribs 1 through 10 articulates with the costal foveae of two contiguous vertebrae and the intervening fibrocartilage. For ribs 11 through 13, the head articulates only with the cranial costal fovea on the body of the vertebra of the same number. The tubercle of the rib articulates with the costal fovea of the transverse process of the vertebra of the same number. Between the head and tuberculum of the rib is the neck.
Sternum
The sternum is composed of eight unpaired segments, the sternebrae (Figs. 2-74, 2-75). Consecutive sternebrae are joined by the intersternebral cartilages. The first sternebra, also known as the manubrium, ends cranially in a clublike enlargement. The last sternebra is flattened dorsoventrally and is called the xiphoid process. The caudal end of this process is continued by a thin plate, the xiphoid cartilage.
LIVE DOG
Palpate the wings of the atlas. While holding these firmly, move the head up and down to extend and flex the atlanto-occipital joint. The point at which a transverse line drawn across the cranial edge of the wings of the atlas intersects the median plane is the site for puncture to obtain cerebrospinal fluid. Palpate the spine of the axis. Move each wing of the atlas up and down to rotate the atlantoaxial joint. Palpate the transverse processes of cervical vertebrae 3 through 6. Note their relative positions in the neck and the large volume of epaxial muscles dorsal to them. Feel the ventral edge of the broad transverse processes of the sixth cervical vertebra.
Palpate the prominent spines of thoracic and lumbar vertebrae. Palpate the transverse processes of the lumbar vertebrae. Locate the iliac crests and feel the spine of the seventh lumbar vertebra between them. This spine is shorter than that of the sixth vertebra and is used to locate the site for lumbosacral puncture for epidural anesthesia. Lumbar myelography is usually done between the spines of the sixth and fifth lumbar vertebrae.
Palpate the ribs and compress the thorax, noting the flexibility of the ribs. Palpate the sternum from manubrium to the xiphoid cartilage. Note the costal arch.
MUSCLES OF THE TRUNK AND NECK
The muscles of the trunk and neck, or axial muscles, are classified morphologically into hypaxial and epaxial groups. The epaxial muscles (Fig. 2-81) lie dorsal to the transverse processes of the vertebrae and function mainly as extensors of the vertebral column. The hypaxial group embraces all other trunk muscles not included in the epaxial division. These muscles are located ventral to the transverse processes and include those of the abdominal and thoracic walls.
The superficial fascia of the trunk covers the thorax and abdomen subcutaneously. It is continuous cranially and caudally with the superficial fasciae of the thoracic limb, the neck, and the pelvic limb. Clean this fascia and fat from the thorax and abdomen. It contains the cutaneous trunci muscle and numerous cutaneous vessels and nerves.
The deep fascia of the trunk (Fig. 2-40), the thoracolumbar fascia, is attached to the ends of the spinous and transverse processes of the thoracic and lumbar vertebrae. From its dorsal attachment to the spinous processes and the supraspinous ligament, it passes over the epaxial musculature to the lateral thoracic and abdominal walls, where it serves as origin for several muscles. On each side this fascia closely covers the abdominal muscles and forms the linea alba on the ventral midline. Detach the origin of the latissimus dorsi from the last few ribs and reflect it to the mid-dorsal line, where it arises from the lumbar vertebral spines via the superficial leaf of the thoracolumbar fascia.
Hypaxial Muscles
The longus capitis (Fig. 2-82) lies on the lateral surface of the cervical vertebrae, lateral to the longus colli. It arises from the transverse processes of the cervical vertebrae and inserts on the muscular tubercle on the ventral surface of the basioccipital bone of the skull.
The longus colli (Figs. 3-8, 3-20) covers the ventral surfaces of the vertebral bodies from the sixth thoracic vertebra cranially to the atlas. It consists of many overlapping fascicles that attach to the vertebral bodies or the transverse processes. The most cranial cervical bundles attach to the atlas. Expose this muscle by reflecting the trachea and the esophagus and related soft tissues. Pass your finger into the thoracic inlet dorsally and feel the thoracic part of the longus colli muscle on the vertebral bodies. This portion will be seen in the dissection of the thoracic cavity. The longus colli must be reflected to expose the cervical intervertebral discs for surgical purposes.
Muscles of the Thoracic Wall
1. The scalenus (Figs. 2-76, 2-82) lies ventral to the origin of the cervical and cranial thoracic parts of the serratus ventralis. It attaches to the first few ribs and the transverse processes of the cervical vertebrae and is divided into several slips. It is a muscle of inspiration.
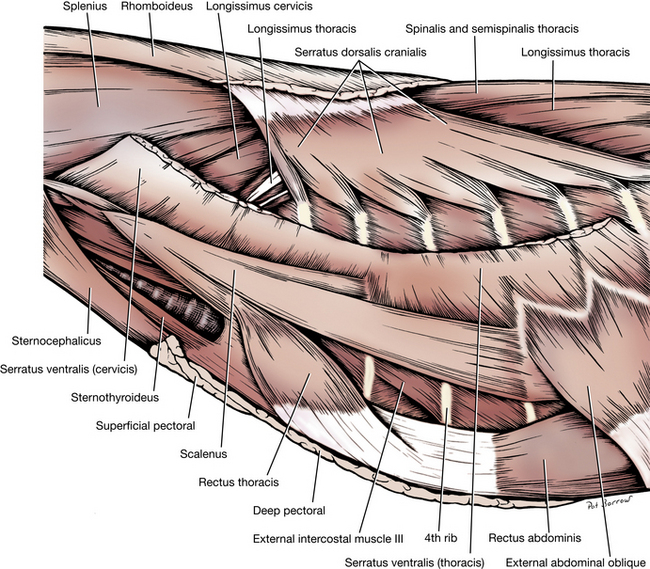
2. The serratus ventralis cervicis and thoracis (Figs. 2-16, 2-76, 2-82) form a large, fan-shaped muscle with an extensive origin on the neck and trunk. Its insertion on the serrated face of the scapula has been observed (Figs. 2-14).
3. The serratus dorsalis consists of cranial and caudal components that arise by a broad aponeurosis from the tendinous raphe of the neck and from the thoracic and lumbar spines and insert on the proximal portions of the ribs. These two components are the serratus dorsalis cranialis and the serratus dorsalis caudalis.
The serratus dorsalis cranialis (Figs. 2-76, 2-82) lies on the dorsal surface of the cranial thorax. It arises by a broad aponeurosis from the thoracolumbar fascia deep to the rhomboideus. It runs caudoventrally and inserts by distinct serrations on the craniolateral surfaces of the ribs. It lifts the ribs for inspiration. Transect this muscle at the begining of its muscle fibers and reflect both portions.
The serratus dorsalis caudalis is smaller and is found on the dorsal surface of the caudal thorax. It consists of distinct muscle leaves that arise by an aponeurosis from the thoracolumbar fascia, course cranioventrally, and insert on the caudal borders of the last three ribs. It functions in drawing the last three ribs caudally in expiration.
4. There are 12 external intercostal muscles (Figs. 2-76, 3-4 through 3-6) on each side of the thoracic wall. Their fibers run caudoventrally from the caudal border of one rib to the cranial border of the rib behind. Their ventral border is near the costochondral junction. They function in respiration by drawing the ribs together, and their overall effect depends on the fixation of the rib cage.
5. The internal intercostal muscles (Figs. 3-4 to 3-6) are easily differentiated from the external intercostal muscles because their fibers run cranioventrally from the cranial border of one rib to the caudal border of the rib in front of it. Medial to most of the internal intercostal muscles is the pleura, which attaches to the muscles and ribs by the endothoracic fascia. The internal intercostal muscles extend the whole distance of the intercostal spaces. These muscles function in a manner similar to that of the external intercostal muscles by drawing the ribs together.
Expose the fifth external intercostal muscle and reflect it to observe the internal intercostal.
Muscles of the Abdominal Wall
The four abdominal muscles (Figs. 2-76 through 2-80), named from without inward, are the external abdominal oblique, the internal abdominal oblique, the rectus abdominis, and the transversus abdominis (Fig. 2-77). When they contract, they aid in urination, defecation, parturition, respiration, or locomotion. These muscles are covered superficially by the abdominal fasciae and deeply by the transverse fascia.
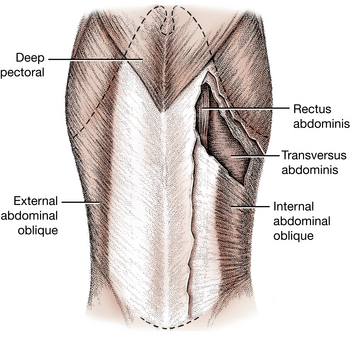
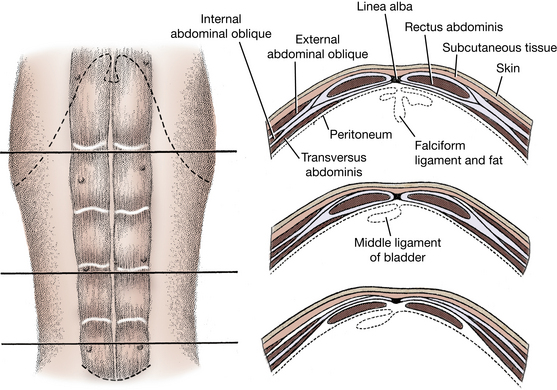
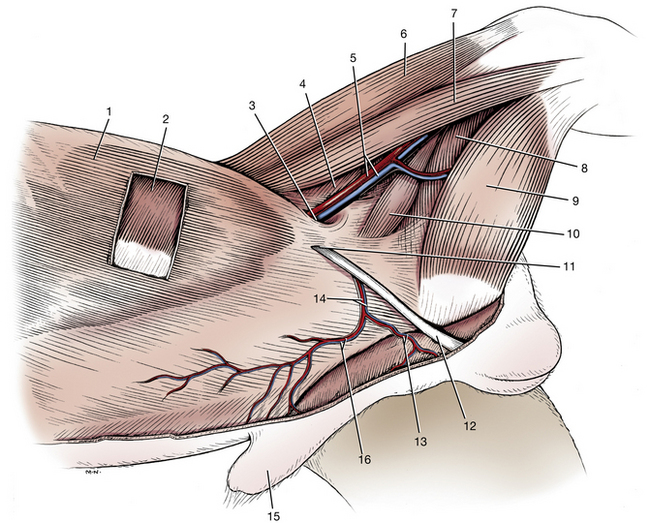
Fig. 2-79 Abdominal muscles and inguinal region of the male, superficial dissection, left side.
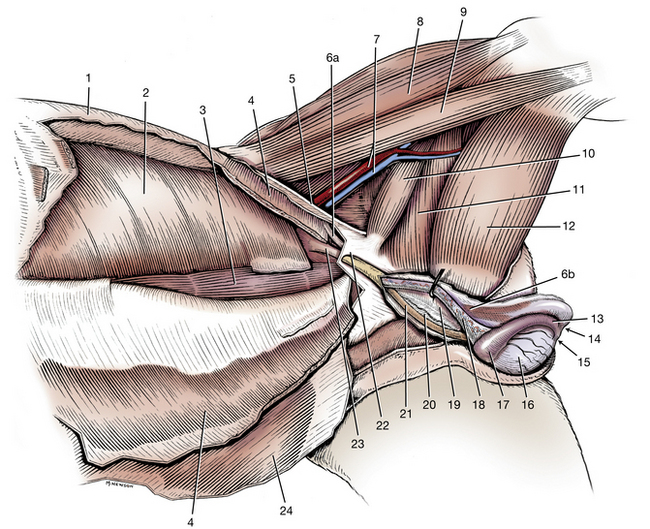
Fig. 2-80 Abdominal muscles and inguinal region of the male, deep dissection, left side.
4. Internal abdominal oblique (transected and reflected)
5. Inguinal ligament (caudal border of aponeurosis of external abdominal oblique muscle)
6a. Cremaster muscle at its origin
6b. Cremaster muscle on external surface of parietal layer of vaginal tunic
14. Ligament of tail of epididymis
16. Testis in visceral vaginal tunic
18. Testicular artery and vein in visceral vaginal tunic (mesorchium)
21. Ductus deferens in visceral vaginal tunic
22. Superficial inguinal ring, lateral crus
1. The external abdominal oblique (Fig. 2-76 through 2-80) covers the ventral half of the lateral thoracic wall and the lateral part of the abdominal wall. The costal part arises from the last ribs. The lumbar part arises from the last rib and from the thoracolumbar fascia. The fibers of this muscle run caudoventrally. In the ventral abdominal wall, this muscle forms a wide aponeurosis that inserts on the linea alba and the prepubic tendon. The linea alba (Fig. 2-78) is the midventral raphe that consists of the fused thoracolumbar fascia and the aponeuroses of the abdominal muscles. The linea alba extends from the xiphoid process to the symphysis pelvis. The aponeurosis of the external abdominal oblique, combined with that of the internal abdominal oblique, forms most of the external lamina of the sheath of the rectus abdominis.
Caudoventrally, just cranial to the iliopubic eminence and lateral to the midline, the aponeurosis of the external abdominal oblique separates into two parts, which then come together to form the superficial inguinal ring (Figs. 2-79, 2-80). This is the external opening of a very short natural passageway through the abdominal wall, the inguinal canal. The superficial inguinal ring is a slit in this aponeurosis with a cranial and caudal angle. The caudal angle is attached to the small palpable iliopubic cartilage that is located in the tendon of origin of the pectineus. Abduct the pelvic limb and follow the pectineus to its origin, where this cartilage can be palpated. The superficial inguinal ring is indistinct because it is covered by thoracolumbar fascia. The internal opening and the boundaries of the canal will be seen when the abdominal cavity is opened. A blind extension of peritoneum protrudes through the inguinal canal to a subcutaneous position outside the body wall. This is the vaginal tunic (Figs. 2-79, 2-80, 4-4, 4-5) in the male and the vaginal process in the female (Figs. 4-2, 4-4). In the male it is accompanied by the testis and spermatic cord, which it envelops. In the female the vaginal process envelops the round ligament of the uterus and a varying amount of fat and ends blindly a short distance from the vulva. In both sexes the external pudendal artery and vein and the genitofemoral nerve also pass through the inguinal canal (Figs. 2-79, 4-2).
Clean the surface of the aponeurosis of the external abdominal oblique and identify the superficial inguinal ring and vaginal tunic or process. Be careful not to destroy the ring and tunic or process in cleaning this muscle. The vaginal tunic or process is covered by the spermatic fascia, which is continuous with the abdominal fascia at this ring.
Transect the external abdominal oblique close to its costal and lumbar origin. Reflect this muscle ventrally from the internal abdominal oblique to the line of fusion between their aponeuroses. The fused aponeuroses cover the external surface of the rectus abdominis.
The inguinal ligament (Fig. 2-80) is the caudal border of the aponeurosis of the external abdominal oblique. It terminates on the iliopubic eminence and prepubic tendon. The ventral portion of the ligament is interposed between the superficial inguinal ring and the vascular lacuna (Figs. 2-79, 4-60). The vascular lacuna is the base of the femoral triangle, the space that contains the femoral vessels that run to and from the hindlimb. The inguinal ligament thus forms part of the cranial border of the vascular lacuna and the caudal border of the inguinal canal. Transect the aponeurosis of insertion of the external abdominal oblique 2 cm cranial to its caudal border and the superficial inguinal ring and reflect the muscle ventrally. Identify these structures.
2. The internal abdominal oblique (Figs. 2-79, 2-80) arises from the superficial leaf of the thoracolumbar fascia caudal to the last rib, in common with the lumbar part of the external abdominal oblique, and from the tuber coxae and adjacent portion of the inguinal ligament. Its fibers run cranioventrally. It inserts by a wide aponeurosis on the costal arch, on the rectus abdominis, and on the linea alba and prepubic tendon. At the rectus abdominis it is fused with the aponeurosis of the external abdominal oblique to form the external sheath of the rectus abdominis.
Transect the muscle 2 cm from its origin (Fig. 2-80) and reflect it ventrally to the rectus abdominis. In doing so, detach its insertions on the ribs. Separate it from all underlying structures except the rectus abdominis. Study the aponeurosis of the internal abdominal oblique, which contributes to the external lamina of the sheath of the rectus abdominis. Note how the caudal border of the muscle forms the cranial border of the inguinal canal. In the male, note that fibers from the caudal border of the internal oblique form the cremaster muscle, which accompanies the vaginal tunic (Fig. 2-80).
3. The transversus abdominis (Figs. 2-40, 2-80) is medial to the internal abdominal oblique and the rectus abdominis. Its fibers run transversely. The muscle arises dorsally from the medial surfaces of the last four or five ribs and from the transverse processes of all the lumbar vertebrae by means of the deep leaf of the thoracolumbar fascia. Its aponeurosis attaches to the linea alba after crossing the internal surface of the rectus abdominis. Except for its most caudal part, the aponeurosis of the transversus abdominis forms the internal sheath of the rectus abdominis. The most caudal portion joins the external sheath and fuses with the linea alba and prepubic tendon.
4. The rectus abdominis (Figs. 2-76 through 2-78, 2-80) extends from the pecten of the pubis, as the prepubic tendon, to the sternum. It flexes the thoracolumbar part of the vertebral column. Observe its cranial aponeurosis from the first few ribs and sternum. The rectus abdominis has distinct transverse tendinous intersections. In the umbilical region the external lamina of the sheath of the rectus abdominis is formed by the fused aponeuroses of the oblique muscles. The internal lamina is formed by the aponeurosis of the transversus abdominis.
Inguinal Canal
The inguinal canal is a slit between the abdominal muscles. It extends from the deep to the superficial inguinal ring (Figs. 2-80, 4-5). The superficial inguinal ring in the aponeurosis of the external abdominal oblique has already been dissected. The deep inguinal ring is formed on the inside of the abdominal wall by the annular reflection of transversalis fascia onto the vaginal tunic or process. This fascia lies between the transversus abdominis and peritoneum. The ring is a boundary and not a distinct anatomical structure. The inguinal canal is bounded laterally by the aponeurosis of the external abdominal oblique, cranially by the internal abdominal oblique, caudally by the caudal border of the external abdominal oblique (the inguinal ligament), and medially by the lateral border of the rectus abdominis and by the transversalis fascia and peritoneum. The vaginal tunic and the spermatic cord or the vaginal process pass obliquely caudoventrally through the inguinal canal.
Epaxial Muscles
The dorsal trunk musculature associated with the vertebral column and ribs may be divided into three parallel longitudinal muscle masses on each side. Each is composed of many overlapping fascicles. These three columns include the lateral iliocostalis system, the intermediate longissimus system, and the medial transversospinalis system (Fig. 2-81). Various fusions occur between these columns, giving rise to different muscle patterns that are difficult to separate. These muscles act as extensors of the vertebral column and also produce lateral movements of the trunk when contracting on only one side.
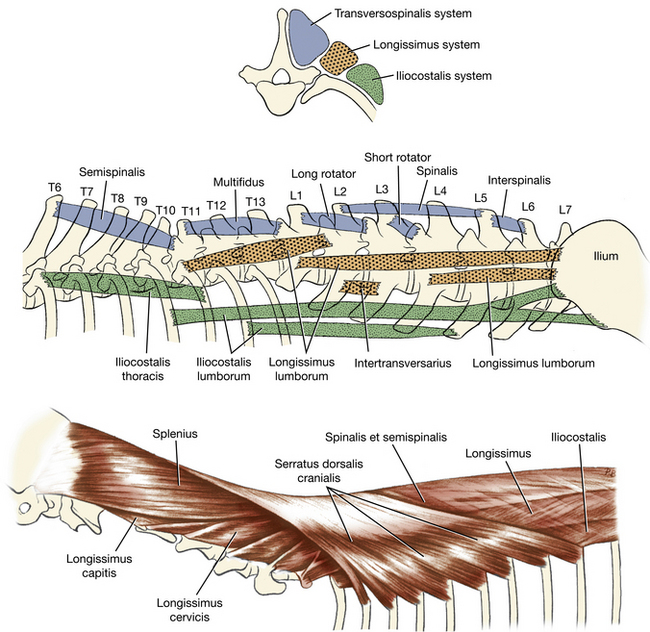
Fig. 2-81 Schema of epaxial muscles. Each of the named muscles shown can be present, spanning other vertebrae, thus overlapping and obscuring their individual nature.
Iliocostalis System
1. The iliocostalis lumborum (Fig. 2-81) arises from the wing of the ilium in common with the longissimus lumborum and inserts on the transverse processes of the lumbar vertebrae and the last four or five ribs. In the lumbar region this muscle is fused medially with the longissimus lumborum. The thoracolumbar fascia covers these muscles. Remove this fascia and any underlying fat to expose the glistening aponeurosis of these fused muscles, which attaches to the crest of the ilium and the spines of the lumbar and last four or five thoracic vertebrae. The cranial end of this iliocostalis muscle is distinctly separated from the longissimus lumborum as it inserts on the ribs. Expose this insertion.
2. The iliocostalis thoracis (Figs. 2-81, 2-82) is a long, narrow muscle mass extending from the twelfth rib to the transverse process of the seventh cervical vertebra. Individual components of the muscle extend between and overlap the ribs. Identify the boundaries of this muscle mass.
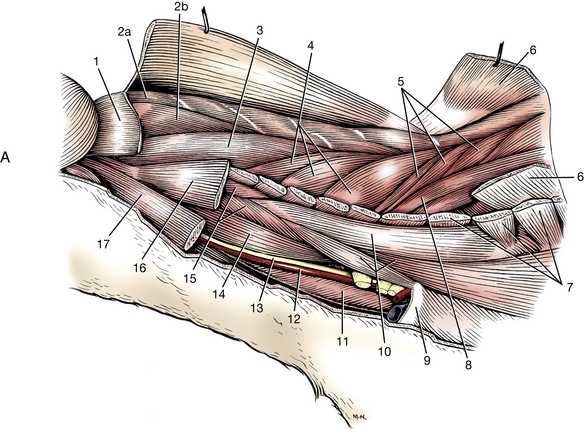
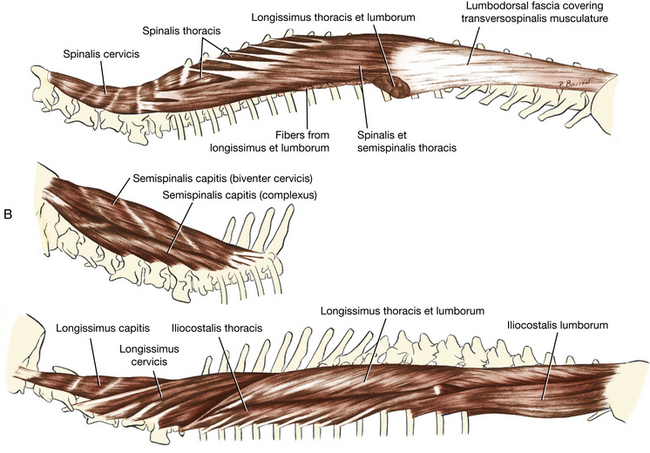
Longissimus System
The longissimus is the intermediate portion of the epaxial musculature. Lying medial to the iliocostalis, its overlapping fascicles extend from the ilium to the head. It consists of three major regional divisions: thoracolumbar, cervical, and capital.
1. The longissimus thoracis et lumborum (Figs. 2-76, 2-81, 2-82) arises from the crest and medial surface of the wing of the ilium and, by means of an aponeurosis, from the supraspinous ligament and the spines of the lumbar and thoracic vertebrae. Its fibers course craniolaterally. Superficially, only a shallow furrow is seen to separate the longissimus and iliocostalis muscles in the lumbar region. This division of the longissimus inserts on various processes of the lumbar aud thoracic vertebrae. The thoracic portion may be seen inserting on the ribs and the seventh cervical vertebra, just medial to the iliocostalis thoracis.
2. The longissimus cervicis (Figs. 2-76, 2-82), the cranial continuation of the longissimus muscle into the neck, consists of four fascicles so arranged that the caudal fascicles partially cover those that lie directly cranioventral to them. They lie in the angle between the cervical and thoracic vertebrae and insert on the transverse processes of the last few cervical vertebrae.
3. The longissimus capitis (Fig. 2-82) is a distinct muscle medial to the longissimus cervicis and splenius muscles. It extends from the first three thoracic vertebrae to the mastoid part of the temporal bone. It is firmly united with the splenius as it passes over the wing of the atlas to its insertion.
Transversospinalis System
The transversospinalis system, the most medial and deep epaxial muscle mass, consists of a number of different groups of muscles that join one vertebra with another or span one or more vertebrae. This complex system extends from the sacrum to the head. Included are muscles whose names depict their attachments or the functions of their fascicles: spinalis, semispinalis, multifidus, rotatores, interspinalis, and intertransversarius. These muscles must be reflected to perform a surgical laminectomy. Only a few of these muscles will be dissected in the neck.
The splenius (Figs. 2-76, 2-82) is a rather large muscle on the dorsolateral surface of the neck, deep to the rhomboideus capitis and the serratus dorsalis cranialis. Its fibers extend in a slightly cranioventral direction from the third thoracic vertebra to the skull. The muscle arises from the cranial border of the thoracolumbar fascia, the spines of the first three thoracic vertebrae, and the entire median raphe of the neck. It inserts on the nuchal crest and mastoid part of the temporal bone. Transect the splenius 2 cm caudal to its insertion and reflect the muscle mass to the median plane.
The semispinalis capitis (Fig. 2-82) is a member of the cervical portion of the transversospinalis group. It lies deep to the splenius and extends from the thoracic vertebrae to the head. It consists of two muscles, the dorsal biventer cervicis and the ventral complexus.
The biventer cervicis is dorsal to the complexus and has tendinous intersections. It arises from thoracic vertebrae and inserts on the caudal surface of the skull. Transect the muscle and reflect it.
The complexus is ventral to the biventer and arises from cervical vertebrae. It inserts on the nuchal crest. Transect this muscle and reflect it.
The nuchal ligament (Fig. 2-84) may now be seen extending from the tip of the spinous process of the first thoracic vertebra to the broad caudal end of the spine of the axis. It is a laterally compressed, paired, yellow elastic band lying between the medial surfaces of the two semispinalis capitis muscles.
The supraspinous ligament continues the nuchal ligament caudally and extends from the spinous process of the first thoracic vertebra to the caudal vertebrae. It passes from one spinous process to another.
LIVE DOG
Palpate the cervical epaxial muscles and note the volume of these muscles dorsal to the cervical vertebrae. Continue caudally and feel the symmetry of the epaxial muscles on either side of the vertebral spines. In racing greyhounds these thoracolumbar epaxial muscles are extremely well developed. Palpate the abdominal wall and visualize the individual layers, the direction of their muscle fibers, and the extent of the aponeuroses of these muscles. Occasionally, the peritoneal cavity is opened by a surgical approach that separates the abdominal muscles in the plane of their fibers—the grid technique. Palpate the rectus abdominis and visualize the aponeuroses that sheath it and the direction of the rectus fibers. Feel the linea alba, where most abdominal incisions are made.
With the dog in lateral recumbency, abduct one pelvic limb. Follow the pectineus muscle proximally toward its origin from the prominent iliopubic eminence. Palpate the iliopubic cartilage just cranial to this eminence. The medial crus of the superficial inguinal ring extends cranially from this cartilage. This crus has a slightly firm feeling, and the spermatic cord in the male and external pudendal vessels in both sexes may be felt passing over this medial crus as the structures emerge from the inguinal canal.
JOINTS OF THE AXIAL SKELETON
Some of these joints will be seen now and others will be observed when the vertebral column and spinal cord are exposed.
Vertebral Joints
The atlanto-occipital joint (Fig. 2-83) is continuous with the atlantoaxial joint through the articulation of the dens with the body of the atlas. The dens is held against the fovea dentis by the transverse ligament of the atlas, which passes dorsal to it and is attached to the body on both sides. Apical and alar ligaments pass from the cranial end of the dens to the basioccipital bone between the occipital condyles. The spine of the axis is joined to the arch of the atlas by a thick dorsal atlantoaxial ligament (Fig. 2-84).
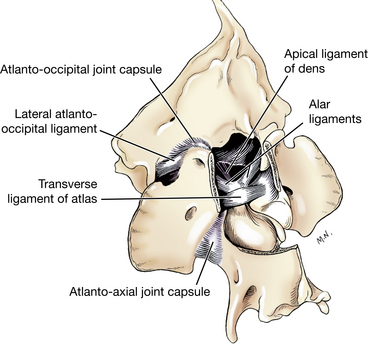
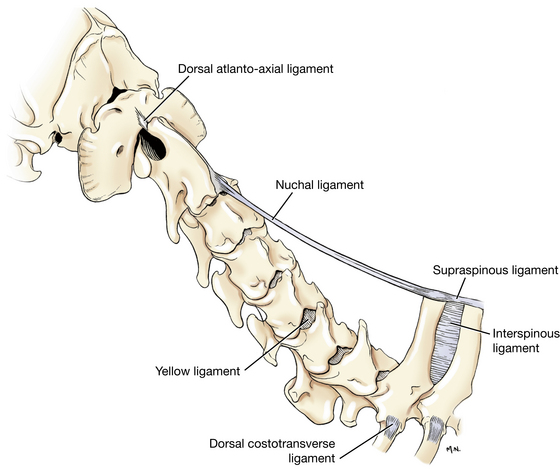
The remaining vertebrae articulate by synovial joints between articular processes and by fibrous joints between the bodies. The latter are intervertebral discs (Figs. 2-85 through 2-87), which consist of outer circumferential collagenous fibers, the anulus fibrosus, and an inner gelatinous core, the nucleus pulposus. The anulus is usually thicker ventrally.
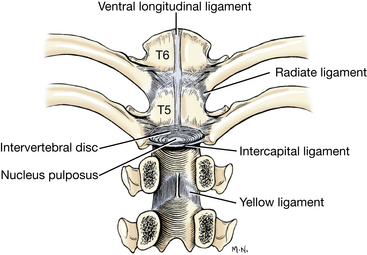
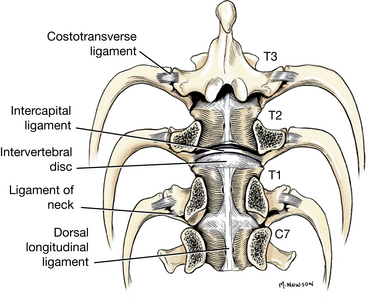
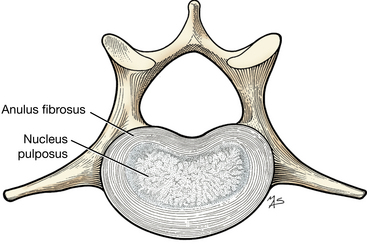
Narrow longitudinal ligaments, one within the vertebral canal and the other beneath the vertebrae, extend across all of the vertebral bodies. The ventral longitudinal ligament (Fig. 2-85) is on the ventral surface of the vertebral bodies and extends from the sacrum to the axis. It is best developed in the caudal thoracic and lumbar regions. The thicker dorsal longitudinal ligament (Fig. 2-86) is on the midline of the floor of the vertebral canal ventral to the spinal cord. It widens where it passes over and attaches to the anulus fibrosus of the intervertebral discs. It extends cranially to the axis.
Yellow ligaments extend between vertebral arches to cover the epidural interarcuate space between the articular processes. Interspinous ligaments (Fig. 2-84) connect adjacent spines above the arches. The supraspinous ligament is a longitudinal band of fibrous connective tissue that connects the apices of all spinous processes from the level of the third caudal vertebra to the first thoracic vertebra. The cranial continuation of this ligament into the cervical region is called the nuchal ligament (Fig. 2-84). The nuchal ligament is elastic and paired. In the dog it extends from the apex of the first thoracic spine to the spine of the axis.
Ribs
The head of each rib articulates in a synovial joint with the craniodorsal aspect of the vertebra of the same number. For the first 10 ribs this articulation includes the caudodorsal portion of the next cranial vertebral body. These adjacent vertebral articular surfaces are cranial and caudal costal foveae. The tuberculum of each rib except the last few has a fibrous articulation with the transverse process.
From the second through the tenth ribs, where the rib heads articulate between vertebral bodies, an intercapital ligament (Figs. 2-85, 2-86) connecting right and left rib heads extends across the dorsal aspect of the anulus fibrosus ventral to the dorsal longitudinal ligament. This intercapital ligament holds the head of the rib in its joint and may provide additional containment for the intervertebral disc, which has a lower incidence of extrusion in this region.
The sternal part of each rib is cartilaginous. The second to seventh ribs join the sternum at modified synovial joints. Other ribs join the sternum as continuous fibrocartilages.