CHAPTER 12 The foot
The foot is the athlete’s main contact area with the ground—an obvious point, but one which helps account for the very high number of conditions affecting this area in sport. An athlete’s foot may have to withstand forces two or three times greater than bodyweight, and this may be repeated more than 5000 times every hour when running. Most sports involve some sort of running or jumping, and so the foot is continually called upon to provide both stability and shock attenuation.
The first metatarsophalangeal joint
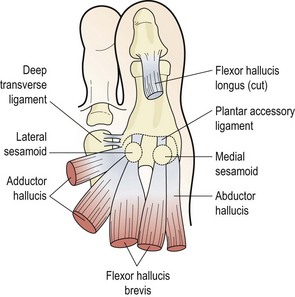
The first metatarsal bone joins proximally to the first cuneiform to form the first ray complex. Distally, the bone forms the first metatarsophalangeal (MP) joint with the proximal phalanx of the hallux. The first MP joint is reinforced over its plantar aspect by an area of fibrocartilage known as the volar plate (plantar accessory ligament). This is formed from the deep transverse metatarsal ligament, and the tendons of flexor hallucis brevis, adductor hallucis, and abductor hallucis. It has within it two sesamoid bones which serve as weight-bearing points for the metatarsal head (Fig. 12.1).
Movement of the joint is carried out by flexor hallucis longus, flexor hallucis brevis, extensor hallucis longus, the medial tendon of extensor digitorum brevis, and abductor and adductor hallucis. This fairly complex structure is often taken for granted but does give rise to a number of important conditions.
Turf toe
Turf toe is a sprain involving the plantar aspect of the capsule of the first MP joint. It is most often seen in athletes who play regularly on synthetic surfaces, and results from forced hyperextension (dorsiflexion) of the first MP joint. Normally this joint has a range of 50–60°, but with trauma the range may be forced to over 100°. The condition is quite common, with studies of American football players showing that 45% of athletes had suffered from turf toe at some stage (Rodeo et al., 1989a).
Forced hyperextension of the first MP joint causes capsular tearing, collateral ligament damage and damage to the plantar accessory ligament. Sometimes force is so great that disruption of the medial sesamoid occurs (Fig. 12.2). Examination reveals a hyperaemic swollen joint with tenderness over the plantar surface of the metatarsal head. Local bruising may develop within 24 hours. Differential diagnosis must be made from sesamoid stress fracture (insidious onset) and metatarsal or phalangeal fractures (site of pain and radiograph).
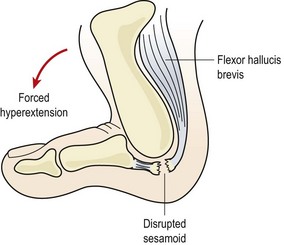
Figure 12.2 Forced hyperextension causes soft tissue damage and possible sesamoid disruption—’turf toe’.
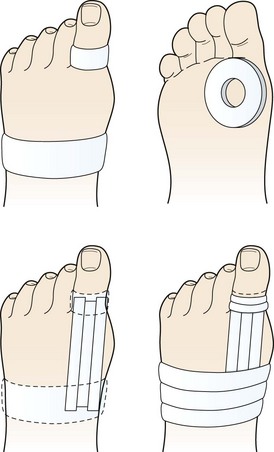
Treatment aims at reducing pain and inflammation and supporting the joint by taping (Fig. 12.3). An oval piece of felt or foam with a hole in the middle is placed beneath the toe, the hole corresponding to the metatarsal head. The first MP joint is held in neutral position and anchors are applied around the first phalanx and mid-foot. Strips of 2.5 cm inelastic tape are applied as stirrups between the anchors on the dorsal and plantar aspects of the toe. In each case the tape starts at the toe and is pulled towards the mid-foot, covering the first MP joint. The mid-foot and phalanx strips are finished with fixing strips.
A number of factors may predispose the athlete to turf toe. The condition is more common with artificial playing surfaces than with grass (Bowers and Martin, 1976). Artificial turf is less shock-absorbing, and so transmits more force directly to the first MP joint. Sports shoes also have an important part to play. Lighter shoes tend to be used with artificial playing surfaces. These shoes are more flexible around the distal forefoot, and allow the MP joint to hyperextend. In addition, shoes which are fitted by length size alone, rather than width, may cause problems for athletes with wider feet. This person must buy shoes which are too long to accommodate his or her foot width. Such a shoe increases the leverage forces acting on the toe joints and allows the foot to slide forwards in the shoe, increasing the speed of movement at the joint.
Preventive measures include wearing shoes with more rigid soles to avoid hyperextension of the injured joint. In addition, semi-rigid (spring steel or heat-sensitive plastic) insoles may be used. Some authors recommend the use of rigid insoles as a preventive measure when playing on all-weather surfaces, for all athletes with less than 60° dorsiflexion at the first MP joint (Clanton, Butler and Eggert, 1986).
An increased range of ankle dorsiflexion has been suggested as a risk factor which may predispose an athlete to turf toe (Rodeo et al., 1989b). However, in walking subjects, when the ankle is strapped to reduce dorsiflexion, the heel actually lifts up earlier in the gait cycle, causing the range of motion at the metatarsal heads to increase (Carmines, Nunley and McElhaney, 1988). This increased range may once again predispose the athlete to turf toe (George, 1989), so the amount of dorsiflexion per se may not be that important. If injury has recently changed the range, the athlete may not have had time to fully adapt to the altered movement pattern, and the altered foot/ankle mechanics in total may be the problem.
As with many soft tissue injuries, if incorrectly managed the condition may predispose the athlete to arthritic changes in later life. In the case of turf toe, this may occur as calcification of the soft tissues around the injury site, presenting as hallux valgus or hallux rigidus.
Hallus valgus
Hallux valgus (hallux abductovalgus or HAV) usually occurs when the first MP joint is hypermobile, and the first ray is shorter than the second (Morton foot structure). When this is the case, the second metatarsal head takes more pressure than in a non-Morton foot (Rodgers and Cavanagh, 1989) (Fig. 12.4). In addition, hallux valgus is more common in athletes who hyperpronate. Often the combination of hyperpronation and poorly supporting fashion footwear exacerbates the condition.
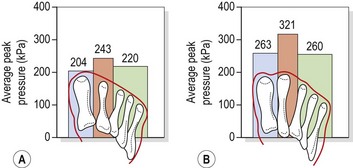
Figure 12.4 Pressure distribution in (A) Morton and (B) non-Morton feet.
From Rodgers, M.M. and Cavanagh, P.R. (1989) Pressure distribution in Morton’s foot structure. Medicine and Science in Sports and Exercise, 21, 23–28. With permission.
Pronation of the subtaloid joint reduces the stabilizing effect of the peroneus longus muscle, allowing the 1st metatarsal to displace more easily. The increased motion leads to the combined deformity of abduction and external rotation of the first toe (phalanges) and adduction and internal rotation of the first metatarsal. Joint displacement occurs at both the MP joint and the metatarsal/medial cuneiform joint (Lorimer et al., 2002).
As the first MP joint dorsiflexes during the propulsive phase of running, the instability allows the hallux to deviate from its normal plane. Adduction and axial rotation occur, and the long flexors which normally stabilize the joint now themselves become deforming influences, causing bowstring effect. As the first metatarsal head adducts, the sesamoids sublux and eventually erode the plantar aspect of the first metatarsal head—this is one source of pain. Compensatory stress is placed on the joints proximal and distal to the first MP and further pain arises through synovial inflammation and capsular distraction. Eventually, secondary osteoarthritis occurs in the first MP joint and sesamoids. High heeled and constrictive footwear may predispose to the condition.
Hallux valgus may occur in one of two types. Congrous hallux valgus is an exaggeration of the normal angulation between the metatarsal and the phalanx of the 1st toe. Importantly the joint surfaces remain in opposition and the condition does not progress. The normal angulation of the 1st MPJ (measured between the long axis of the metatarsal and that of the proximal phalanx) is 8–20°; in congruous hallux valgus this angle may increase to 20–30° (Fig. 12.5A). Once the angle increases above 30°, the joint surfaces move out of congruity and may eventually sublux. This condition is now classified as pathological hallux valgus, and may progress, with the angulation increasing to as much as 60° (Magee, 2002).
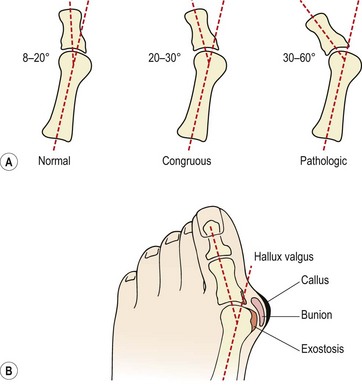
Figure 12.5 Hallux valgus. (A) Metatarsophalangeal angle and (B) appearance.
After Magee (2002) with permission.
Bunion formation to the side of the first metatarsal head is common. The bursa over the medial aspect of the MPJ thickens and a callus develops. In time an exostosis is seen on the metatarsal head and the three structures combined lead to the cosmetic change which is noticeable (Fig. 12.5B). A gel padded bunion shield can help reduce both abnormal shearing and compressive stress to ease symptoms when walking. At night a bunion regulator which resists the abduction forces acting on the 1st toe can help to protect the overstretched soft tissues and reduce inflammation and pain.
Keypoint
A bunion shield is a soft pad placed over the toe joint. A bunion regulator is a firmer splint placed over the forefoot to resist abduction of the 1st toe.
Management of this condition is initially to stabilize the first MP joint by correcting faulty foot mechanics (especially hyperpronation) and advising on correct athletic footwear. If conservative management fails, surgery may be required. If the deformity is purely soft tissue in nature, the bunion may be removed, and the dynamic structures around the first toe realigned. If bony deformity is present, osteotomy (bone realignment), arthroplasty (forming a new joint) or arthordesis (joint fusion) may be necessary.
Hallux limitus/rigidus
A reduction in movement of the first MP joint, hallus limitus, may progress to complete immobility or hallux rigidus where the joint is ankylosed. The condition is more common when the first metatarsal is longer than the second. Pain is generally worse during sporting activities, and occurs especially when pushing off. On examination, the joint end feel is usually firm, and limitation of movement is noted to dorsiflexion. To differentiate between a tight flexor hallucis longus and joint structures, the foot is assessed both with the foot dorsiflexed and everted (tendon on stretch) and then plantarflexed and inverted (tendon relaxed).
Keypoint
In hallux limitus, movement may be restricted by either a tight flexor hallucis longus (FHL) or joint structures. To differentiate between the two, movement range is assessed both with the tendon on stretch (FHL limits) and with the tendon relaxed (joint limits).
Limitation of motion through muscle tightness responds well to stretching procedures, while joint limitation which is soft tissue in nature is treated by joint mobilization. Distal distraction and gliding mobilizations with the metatarsal head stabilized are particularly useful (Cibulka, 1990). Where bony deformity is present, surgery is indicated. A number of surgical procedures are available for hallux conditions, and the interested reader is referred to Horn and Subotnick (1989) for an excellent review.
Taylor’s bunion
A Taylor’s bunion is seen over the base of the 5th metatarsal. It is more common in athletes who have a cavus foot with splaying toes, and may cause abrasion in unyielding sports footwear such as ski boots, cycling shoes and rollerboots. Management is generally conservative, encouraging athletes to select sports shoes with a wide toe box. Severe cases may require surgical intervention.
Plantar fasciitis
The plantar fascia (plantar aponeurosis) is the thickest fascia in the body. It attaches from a point just behind the medial tubercle of calcaneus and runs anteriorly as five slips. As the slips approach the metatarsal heads, they split into superficial and deep layers (Fig. 12.6A). The superficial layer attaches to superficial fascia beneath the skin, while the deep layer divides into medial and lateral portions to allow the passage of the flexor tendons. Each of the five portions attaches to the base of a proximal phalanx and to the deep transverse ligament.
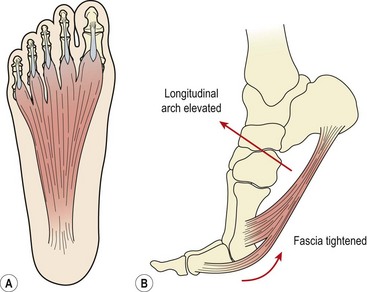
Figure 12.6 Plantar fascia structure and action. (A) Normal tension in fascia. (B) Raising onto the toes tightens the plantar fascia and raises the longitudinal arch.
As the toes dorsiflex and the 1st MP joint is extended prior to toe off, the fascia is wound around the metatarsal head (windlass effect). In so doing the fascia is tightened, shortening the foot and elevating the longitudinal arch (Fig. 12.6B). The combination of these effects supinates the foot and provides a rigid lever for push off. As the foot contacts the ground at heel strike the arch lowers and the foot pronates, becoming a mobile adaptive unit. The plantar fascia is stretched as the foot lengthens.
As we have seen in Chapters 10 and 11 tendon inflammation (patella tendonitis and Achilles tendonitis) is now thought to be an incorrect term based on the pathology of the tissue affected. Similarly the term plantar fasciitis implies tissue inflammation but histological findings do not support this concept. Reviewing 50 post surgical cases Lemont, Ammirati and Usen (2003) found degeneration and fragmentation of the plantar fascia together with bone marrow vascular ectasia (expansion). No inflammatory markers were present, implying that the condition is a fasciosis rather than a fasciitis. This fact is important when treating the condition, as steroid injections (anti-inflammatory) often used to treat plantar pain have a strong association with plantar ruptures (Murphy, 2006). In a study of 765 patients with plantar fascial pain Acevedo and Beskin (1998) found 51 patients who had received corticosteriod injection. Of this subgroup 44 ruptured, with 68% showing sudden onset tearing and 32% gradual onset tearing. At follow-up 26 subjects still showed symptoms 1 year after rupture.
Keypoint
Plantar fasciitis is a non-inflammatory condition (fasciosis) showing degeneration and fragmentation of the plantar fascia.
Pain in the plantar fascia is common in sports which involve repeated jumping, and with hill running. Overuse may cause microtears and degeneration at the fascial insertion, and nodules from the fascial granuloma can occasionally be felt (Tanner and Harvey, 1988).
Normally, during mid-stance the foot is flattened, stretching the plantar fascia and enabling it to store elastic energy to be released at toe off. However, a variety of malalignment faults may increase stress on the fascia. Excessive rearfoot pronation will lower the arch and overstretch the fascia, and a reduction in mobility of the first metatarsal may also contribute to the condition (Creighton and Olson, 1987). In addition, weak peronei, often the result of incomplete rehabilitation following ankle sprains, will reduce the support on the arch, thus stressing the plantar fascia. Congenital problems such as pes cavus will also leave an athlete more susceptible to plantar fasciitis. The condition is exacerbated if the Achilles tendon is tight, or if high-heeled shoes are worn. Pain is often worse when taking the first few steps in the morning until the Achilles tendon is stretched.
Keypoint
Plantar fasciitis can be aggravated if the Achilles tendon is tight or if the patient wears high-heeled shoes.
Sports shoes play an important part in the course of this condition. Inadequate rearfoot control may fail to eliminate hyperpronation, and a poorly fitting heel counter will allow the calcaneal fat pad to spread at heel strike, transmitting extra impact force to the calcaneus and plantar fascia. On a hard surface, the shock-absorbing qualities of the shoe are important, and a patient’s footwear should always be examined.
Pain is usually over the calcaneal attachment of the fascia or its medial edge. Pain may be localized to the heel as though the athlete is ‘stepping on a stone’, or may present as a burning pain over the arch. The problem must be differentiated from rheumatoid conditions which often give bilateral pain, and Sever’s disease which gives pain to the insertion of the Achilles tendon. In addition fat pad pain (see below) will give heel pain over the whole pad rather than a single point as with plantar fasciitis.
Treatment
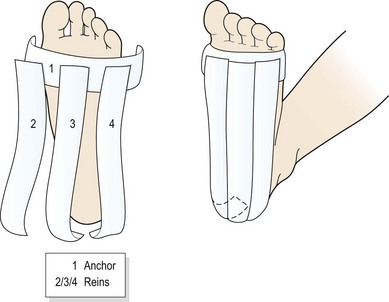
Taping the foot (Fig. 12.7) may often give surprisingly rapid relief. The foot is locked in neutral position and an anchor strap placed just behind the metatarsal heads. Three strips of tape (medial, lateral and central) are then passed from the anchor over the heel to stop on the posterior aspect of the calcaneum. A horseshoe-shaped fixing strip secures the tape behind the heel. Additional strips may be placed transversely across the foot from the metatarsal heads to the calcaneal tubercle.
Trigger point therapy for the plantar muscles (especially quadratus plantae and flexor hallucis) may give excellent results even long term. The thickness of the tissues in this area means that a massage tool should be used to save the therapist’s fingers. The athlete sits with the therapist sitting towards the end of the treatment couch. Ischaemic pressure is placed onto the muscles and fascia in the sole of the foot and the tissues are gradually tightened as pain allows by plantarflexion of the foot and flexing the toes (windlass effect). Specific soft tissue mobilization may be performed by pressing the fascia into the pain producing direction and repeating this action at a lower (painless) grade and holding the fascia stretch for 4−5 seconds. The athlete can be taught self-management by pressing the sole of the foot down onto a hard ball (marble or snooker ball) or crossing the legs and pressing directly into the sole with the thumbs.
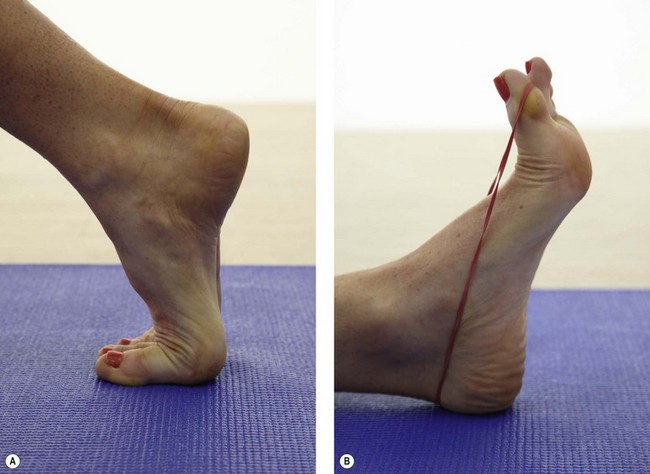
Extensibility of the 1st MP joint is assessed both weight bearing (foot on the floor) and non-weight bearing (patient on the couch), with normal values of 65° quoted (Murphy, 2006). Movement limitation should be categorized as bony requiring joint mobilization or soft tissue requiring stretching. The plantar fascia is stretched by using a combination of 1st MP extension and ankle dorsiflexion (Fig. 12.8).
More permanent management may require rearfoot posting to control excessive pronation. In addition, strengthening the intrinsic foot musculature is important. Although the plantar fascia is inert, stress on the structure may be increased when the intrinsic foot musculature is weak. The role of foot strengthening, including actively increasing the arch height, and ‘gripping’ the floor with the toes, may have a re-education effect on plantar proprioception.
Heel pad
The calcaneus is covered by elastic adipose tissue in the same way as the finger tips. The fat cells are arranged in columns made from fibrous septa which lie vertically. As weight is taken, the walls of the columns bulge and spring back as the weight is released. With age the septa lose elasticity and the thickness of the heel pad reduces.
Athletes who wear poorly padded sports shoes and those who land heavily on the heel when jumping may bruise this area. In more severe cases rupture of the fibrous septa may occur causing spillage of the enclosed fat cells (Reid, 1992). In turn, the loss of the heel pad shock-absorbing mechanism places excessive compression stress onto the calcaneum.
Pain is increased when walking barefoot. Typically, athletes complain of pain first thing in the morning when getting out of bed. The first few steps are exquisitely tender, later subsiding to a dull ache. Pain is brought on by prolonged standing and walking.
Management is by additional padding, and preventing the heel pad from spreading. Non-bottoming shock-absorbing materials are useful, and taping to surround the heel and prevent spread of the pad is effective in the short term (Fig. 12.9). Activity modification is required during the acute stage of the condition.

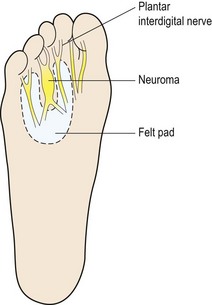
Morton’s neuroma
Morton’s neuroma (plantar neuroma) affects the plantar interdigital nerve between the third and fourth metatarsal heads. The condition is not a true neuroma (nerve tumour), but simply a localized swelling and scarring of the nerve. Symptoms may occur spontaneously and are often described as feeling like ‘electric shocks’ along the sensory nerve distribution. The condition is more common with runners (particularly when sprinting and running uphill) and dancers, and is often aggravated by wearing narrow, high-heeled shoes. The sustained dorsiflexed position of these activities stretches the digital nerve causing inflammation. Once swollen, the nerve is open to entrapment between the metatarsal heads, and eventually the nerve is scarred and permanently enlarged to form a neuroma.
The patient’s pain may be reproduced by direct pressure over the neuroma while compressing the forefoot medially and laterally to shorten the transverse arch (Mulder’s sign). The condition must be differentiated from Freiberg’s disease (see below) which occurs in the younger athlete.
Keypoint
Mulder’s sign is a test for Morton’s neuroma. The test is positive if pain is reproduced by palpating the neuroma while compressing the forefoot in a medial−lateral direction to shorten the transverse arch.
If the condition is caught in its oedematous stage, alteration of footwear (larger toe box and lower heel), ice application and ultrasound are effective. Injection with corticosteroid and local anaesthetic is also used. Padding the area with orthopaedic felt (Fig. 12.10) to take some of the bodyweight off the neuroma can give temporary relief. The arms of the pad rest on the adjacent metatarsals, leaving the area of the neuroma free.
Once the neuroma has formed, surgical excision under local anaesthesia may be required, with some studies showing improvement in 80% of patients (Mann and Reynolds, 1983). There may be a permanent loss of sensation over the plantar aspect of the foot supplied by the digital nerve, but in some cases regeneration can occur between 8 and 12 months after surgery. Follow-up after 2 years (mean 29 months) has shown an 88% reduction in pain with overall satisfaction being excellent or good in 93% of sporting patients (Akermark, Saartok T and Zuber, 2008).
Freiberg’s disease
Freiberg’s disease (lesion) is an osteochondrosis of the 2nd metatarsal head, most commonly seen in young ballet dancers. Pain occurs over the bony head of the metatarsal (contrast this with Morton’s neuroma which gives pain between the metatarsals) and is aggravated by raise onto the ball of the foot. In longer standing cases x-ray reveals flattening of the metatarsal head with damage to the epiphyseal plate. Initially no changes may be apparent on radiographs (Fig. 12.11), with bone scan or MRI being more sensitive. Management is by modification of weight bearing activities and padding over the metatarsal head to offload the joint and reduce direct pressure over the painful area. Orthotic prescription is often required.

Metatarsalgia
The term ‘metatarsalgia’ is often used to describe any pain in the forefoot. Such pain may come from a variety of conditions, including those affecting the hallux, a digital neuroma or even stress fractures. However, in this description we will limit the term to ‘functional metatarsalgia’, where altered foot function causes abnormal mechanical stress in the forefoot, which is symptomatic.
The transverse arch of the foot is supported at the level of the cuneiforms by peroneus longus, which pulls the medial and lateral edges of the foot together (Palastanga, Field and Soames, 1989). More distally, the arch is formed by the metatarsal heads, the highest point or ‘keystone’ being the second metatarsal.
Keypoint
The transverse arch of the foot is supported by peroneus longus. Distally, the arch is formed by the metatarsal heads, the highest point or ‘keystone’ being the second metatarsal.
In mid-stance, the arch flattens and the five metatarsal heads come to lie in the same transverse plane to take the bodyweight. The first metatarsal takes weight through its sesamoid bones, and it and the fifth metatarsal are more mobile than the other three. Stability to the metatarsal heads is provided both passively, by the transverse metatarsal ligament, and actively, by adductor hallucis and, to a lesser extent, the intrinsic muscles. Normally, these structures keep the metatarsals together. However, in cases of hypermobility such as excessive pronation or hallux valgus, the metatarsal heads may splay apart, effectively increasing the width of the forefoot, and allowing the central metatarsal heads to take too much weight.
Hypermobility may cause abnormal shearing forces, especially in an ill-fitting shoe, giving plantar keratosis. As the metatarsal heads splay, the transverse ligament and intrinsic muscles are subjected to tensile stress, giving pain. Rigidity of the foot may also cause problems. If any of the metatarsals are fixed, or if the toes are ‘clawed’, plantar compression will occur, again giving keratoma (Neale and Adams, 1989).
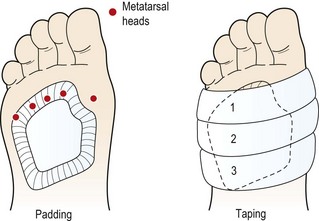
Clearly, successful management of the condition relies to a large extent on the identification of any underlying biomechanical abnormality in the foot. Short-term relief may be obtained by using anti-inflammatory modalities, and padding and strapping to relieve the stress on the forefoot tissues. An adhesive plantar metatarsal pad (PMP), made from orthopaedic felt, is contoured to cover the heads and upper shafts of the three central metatarsals, lifting them above ground level on weight bearing (Fig. 12.12). The pad is cut around the head of the first metatarsal to avoid excessive pressure at this point. To prevent metatarsal splaying, inelastic strapping is placed around the forefoot, encircling the metatarsals just beneath the first and fifth metatarsal heads. If the metatarsals are immobile, a metatarsal bar may be built into the shoe. This has the effect of transferring the bodyweight to the metatarsal shafts and away from the painful metatarsal head.
Coupled with strapping and padding, strengthening the intrinsic muscles is essential. Simple exercises, such as gripping the floor with the toes in bare feet, are effective at building isometric strength and endurance of the intrinsics. Eccentric strength is similarly developed by initially tensing the intrinsic muscles of the foot and increasing the arch with the leg non-weight bearing. The bodyweight is then taken onto the foot and gradually the arch is allowed to flatten under control.
Cuboid syndrome
Pain over the lateral aspect of the foot may represent subluxation of the cuboid. This is more common in dancers, where 17% of foot and ankle injuries have been found to be cuboid-related (Marshall and Hamilton, 1992). The condition is also seen following ankle sprain. At the time of injury, the ligamentous support of the calcaneocuboid joint and the metatarsal cuboid joint may be disrupted. When this occurs in an athlete with a markedly pronated foot, the peroneus longus, travelling through the groove of the cuboid, may pull the medial edge of the cuboid down.
Dull pain is experienced over the lateral aspect of the foot and along the course of peroneus longus tendon. Pain is increased with prolonged standing and exercise on unforgiving surfaces and/or in poor athletic footwear. Typically, the pain is worse for the first few steps in the morning and is lessened when non-weight bearing, and when walking on the toes (foot supinated).
The subluxation may be reduced by manual therapy. Two methods are typically used (Marshall and Hamilton, 1992) with each using passive plantarflexion to reduce the subluxed cuboid:
Accessory movements of the foot
In many conditions affecting the foot and ankle, accessory movements of the joints of the mid-foot and forefoot may be reduced. Mobilization procedures require accurate fixation of one segment while mobilization of an adjacent segment is carried out. Kaltenborn (1989) described a logical series of movements of use for examination and manual treatment.
On the lateral side of the foot a number of movements focus on the cuboid. Initially, the cuboid is moved on the fixed calcaneum. The navicular and lateral cuneiform are fixed and the cuboid is then moved upon them. Finally the cuboid itself is fixed and the fourth and fifth metatarsals are moved.
On the medial side of the foot, movements are around the navicular and cuneiforms. The navicular is fixed and the cuboid and then the cuneiforms are moved. The navicular itself is moved on the talus. Finally, the cuneiforms are fixed and the second and third metatarsals moved (Fig. 12.13). See also Treatment note 12.1.
Figure 12.13 The lateral side of the foot is moved around the cuboid, the medial side around the navicular cuneiforms.
Treatment note 12.1 Manual therapy techniques for the foot
Mobilization of the cuboid bone
The cuboid may become stiff due to lateral ligament sprain where inflammation has been caused to the peroneus brevis tendon connected to the tubercler of the 5th metatarsal. Swelling may then spread on to the cuboid articulations.
To locate the cuboid, find the tubercle on the 5th metatarsal. The cuboid is the flat block-like bone which lies immediately superior to this. Grip the cuboid with the thumb and forefinger of one hand and fix the calcaneous with the other. Move the cuboid on the fixed calcaneous (Fig. 12.14). Secondly, fix the cuboid with the thumb and forefinger of one hand and move the 4th and 5th metatarsals on this fixed point.

Mobilization of the tarsometatarsal (TM) joint of the first toe
To find the first TM joint, palpate the ball of the large toe and follow the metatarsal along its length, tracing it with the knife edge of the thumb. The thumb comes to rest in a shallow hollow between the base of the first metatarsal and the medial cuneiform bone. Stabilize the metatarsal with the thumb and forefinger of one hand while mobilizing the medial cuneiform with the thumb and forefinger of the opposite hand.
Longitudinal mobilization traction of the first ray
Longitudinal mobilization to the first metatarsal phalangeal (MP) joint and the tarsometatarsal (TM) joint of the first toe can be extremely relieving in cases of halux rigidus. Support the shaft of the first metatarsal with one hand while surrounding the proximal phalanx of the great toe with the fingers of the opposite hand (Fig. 12.15). The movement is a distraction force for first MP joint. While maintaining the stabilization on the shaft of the first metatarsal bone, abduction and adduction may be imposed on the first MP joint.

Trigger point massage of the quadratus plantae and the flexor digitorum
These muscles (quadratus plantae is also known as flexor accessorius) become tight and painful in cases of plantar fasciitis and respond well to ischaemic compression. Because of the thickness of the sole of the foot it is difficult to provide sufficient pressure using the practitioner’s thumb.
For this reason, a plunger is used. Pressure is initially applied with the foot slightly plantarflexed and the toes flexed to release the muscle (Fig. 12.16). As pain eases, the plantar fascia itself is stretched by plantarflexion and flexion of the first toe to use the windlass effect. The patient may be taught this technique, using a small marble or ball on the floor and moving the foot up and down over it. Alternatively, massage into the sole of the foot by crossing one leg over the other and using the ball of the thumb (Fig. 12.17).


Skin and nail lesions
Subungual haematoma
In this condition, a haematoma forms directly below the nail plate as a result of direct trauma. Pressure builds up in the space between the nail and nail bed, causing acute pain and throbbing. In some cases the pressure may be great enough to loosen the nail from its bed. Subungual haematoma is often referred to as ‘black toe’ or ‘runner’s toe’. Ill-fitting shoes are a common cause; if the toe box is too small the nail may rub, especially when running downhill.
When the problem is acute, the haematoma is often decompressed by the athlete penetrating the nail with a red-hot needle or paperclip to release the blood (Subotnick, 1989). A less hazardous approach is for the therapist to use a sterile needle, and to then cover the area with a sterile dressing. The best treatment for chronic haemorrhage is to remove the cause, and buy shoes which allow enough room for the toes to spread on weight-bearing and expand with warmth. When standing, a sports shoe should allow one thumb’s breadth between the end of the shoe and the athlete’s longest toe.
Ingrown toenail (onychocryptosis)
Onychocryptosis, or ingrown toenail, is particularly common in the hallux of athletes, especially males. It may occur secondarily to ill-fitting sports shoes, or to incorrect toenail cutting. Shoes are often too narrow, leading to lateral pressure on the hallux, and athletes often cut the toenails too short, causing the underlying soft tissues to protrude. Cutting across the corners of the nail is another common fault in foot care, allowing the nail to embed itself into the nail grooves. Frequently, excessive sweating (hyperhidrosis) causes skin softening, a condition exacerbated by prolonged hot bathing.
A splinter of nail grows into the subcutaneous tissue, and with time, acute inflammation occurs, possibly with infection (paronychia). The skin becomes red, tight and shiny, and the toe swells. There is throbbing pain and acute tenderness to palpation. Normal healing will not take place as long as the nail splinter remains, and so hypergranulation occurs. The combination of granulation tissue and the swollen nailfold overlaps the nail plate itself.
When the condition occurs without infection, the nail splinter may be removed with a scalpel (size 15), avoiding further damage to the sulcus. The edge of the nail is smoothed and the area washed with saline. The nail edge is then packed with cotton wool, allowing some to rest under the nail plate itself. The area is protected with a sterile dressing, and regularly inspected.
When the condition is accompanied by infection, a local anaesthetic is used, injecting at the base of the toe away from the infected area. Oral antibiotics may be used and/or an antiseptic dressing applied. Hypergranulation tissue is excised. If this procedure is ineffective, nail surgery involving partial or complete nail avulsion is required (Neale and Adams, 1989).
Prevention of the problem relies on the use of correctly fitting sports shoes, and on cutting the nails to the shape of the end of the toe while avoiding splintering the nail sides. It is good practice to address basic foot care at the beginning of the season, especially with athletes new to the squad.
Nailbed infection (onychia)
Nailbed infection (onychia) and inflammation of the lateral aspect of the nail (paronychia) is common with the nail of the first toe. The condition occurs through poor foot hygiene and nail management, repetitive trauma, and as a reaction to soaps and nail varnish etc. The infection is usually due to staphylococcus or streptococcus, or as a secondary effect of a fungal infection (see below). There is intense pain, redness and pus formation (suppuration) which may also be accompanied by changes in the appearance of the nail itself.
Management is by antiseptic soaks three times a day with the application of a topical antiseptic cream together with general foot hygiene (clean, breathable socks and disinfect normal footwear which has been worn without socks). Persistent cases may require antibiotics, nail debridement or even nail excision.
Blisters
Blisters occur as a result of compression or shearing on the skin. A narrow toe box may cause blisters over the medial aspect of the fifth toe, and between the first and second toes in the case of hallux valgus. Blisters over the plantar aspect of the foot are common when sports shoes are loose. Shoes should be fitted correctly and friction reduced wherever possible. Petroleum jelly or plastic backed moist gel squares used between the toes are helpful. Proper foot hygiene, which may include powder or astringents to dry the foot, should be observed.
Acute blisters may be drained through a puncture hole. A sterile needle is used and enters the blister at the side, the needle being held parallel to the skin. This will leave a skin flap intact for protection. The underlying cause of the blister should be addressed.
Athlete’s foot
Tinea pedis or ‘athlete’s foot’ is the most common fungal infection of the feet, and is particularly rampant in communal washing areas within sport and where standards of hygiene are poor. Sports shoes create moisture and warmth between the toes, conditions in which the complaint thrives. Three types of tinea pedis are generally seen. First, the lateral toe spaces become macerated due to three organisms: Trichophyton rubrum, Trichophyton interdigitale and Epidermophyton floccosum. Second, the condition may spread to the soles of the feet where vesiculation occurs as a result of T. interdigitale and E. floccosum, and finally a diffuse ‘moccasin type’ scaling appears, usually due to T. rubrum. The condition may also spread to the nails and hands in some cases.
Treatment is initially aimed at removing the scaling tissue by the application of surgical spirit. When the scaling has cleared, antifungal dusting powders, such as tolnaftate, are used. Sprays containing clotrimazole and dusting powders are used by the athlete, and socks and footwear should be changed daily and preferably disinfected. Tea tree oil (Melaleuca alternifolia essential oil) as a 10% cream has been shown to reduce symptoms of tinea pedis as effectively as tolnaftate (1%) in a study of 104 patients (Tong, Altman and Barnetson, 1992). In a randomized controlled double-blinded study of 158 patients Satchell et al. (2002) used a twice daily application of tea tree oil solution (25% and 50%) for 4 weeks and showed a marked clinical response. Mycological cure rate was 64% for the tea tree oil group (50% concentration) compared to 31% for placebo.
While the infection remains, athletes should not go barefoot in public areas (changing rooms and swimming baths), and should not share towels, socks or footwear.
Callus formation (hyperkeratosis)
Keratinization is a normal physiological process which turns the stratum corneum of the skin into a hard protective cover. The process becomes overactive if the skin is continually subjected to mechanical stress, for example on the hands of heavy manual workers or the feet of athletes. Hyperaemia occurs, stimulating a proliferation of epidermal cells, and at the same time the rate of desquamation reduces. This type of keratoma or callus on the foot has a protective function, and providing it is asymptomatic it should be left in place. However, when the bulk of such tissues becomes excessive and causes pain or deformity, treatment is required.
The size and shape of the hyperkeratosis is largely dictated by the stress imposed on the skin. A callus is a diffuse area of thickened skin resulting from stress over a fairly wide area, while a corn is a smaller concentrated area which has formed into a nucleus.
Definition
A callus is a diffuse area of thickened skin resulting from stress over a fairly wide area, while a corn is a smaller concentrated area which has formed into a nucleus.
Corns typically seen in sports medicine are either soft or hard, although vascular and neurovascular types do exist. Soft corns are common in the cleft between the fourth and fifth toes, and appear macerated due to sweat retention. The corn nucleus is generally ring-shaped and the centre of the lesion is very thin. Hard corns occur on the plantar aspect of the foot beneath the metatarsal heads, or on the dorsum of the interphalangeal joints. They develop because of concentrated pressure due to bodyweight and ground reaction forces. The corn nucleus is often associated with surrounding callus due to shearing stress.
The corn or callus may be removed with a scalpel by a therapist and the corn nucleus eradicated. Antiseptic agents such as cetrimide and chlorhexidine are then applied. Moist skin is treated with salicylic acid or aluminium chlorohydrate, and excessively dry skin managed with an emollient containing urea, or soft white paraffin. It is important to remove the underlying cause of the keratoma so that it does not simply return. Examination of foot biomechanics and sports footwear is therefore essential.
Verruca
Verruca pedis is a lesion caused by one of the human papilloma viruses (HPV), of which about 15 have been identified. A benign epithelial tumour which is self-limiting is produced in the plantar skin. The wart is covered by hyperkeratotic tissue, and contains brown or black specks caused by intravascular thromboses within its dilated capillaries. Where the wart is over a weight-bearing site, it is forced into the dermis leaving just the hyperkeratotic area on the surface. For this reason athletes often assume a verruca is simply a corn or callus. However, close inspection will usually reveal the papillary appearance of the verruca. A number of other factors differentiate the two. A wart has a far more rapid onset than an area of callus, and may occur in an area of skin not associated with mechanical stress. In addition, bleeding can occur if the verruca is cut because of capillary dilatation, whereas a callus is avascular.
Keypoint
Differentiation of a verruca from a corn: (i) a verruca forms more quickly than corn; (ii) a verruca is found on skin which is not associated with mechanical stress; (iii) a verruca will bleed if cut, but a corn will not.
The virus normally enters the body through broken skin in the foot, especially if the foot has been wet and the skin macerated. Unfortunately, the virus spreads quickly through a population before the plantar wart becomes obvious. The aim of treatment is to destroy all the cells within the lesion by chemical cautery or cryosurgery. Various preparations are used. The skin surrounding the area is protected, and a liquid or paste of salicylic acid (or monochloroacetic acid) is applied. An aseptic necrosis is produced, and destroyed tissue is removed 1 week later.
Cryosurgery aims at freezing the verruca with carbon dioxide snow, nitrous oxide or liquid nitrogen applied through a probe. Tissue necrosis with blister formation occurs when the skin is cooled to −20°C and bluish colouration results. The rapid cooling causes ice crystals to form in the body cells and interstitial fluids, which in turn ruptures the cells. Liquid nitrogen is perhaps the most common of the cryosurgery techniques, applied by dipping a cotton-tipped stick into the liquid. This is applied to the verruca for about 30–60 seconds. The lesion is protected by a cavity pad if it is over a weight-bearing area.
There is evidence of the effectiveness of tea tree essential oil in the treatment of hand warts (Millar and Moore, 2008), and this treatment is used by some practitioners to successfully manage verrucae.
If the verruca is not painful, treatment may not be required as the lesion will regress naturally in some months (Neale and Adams, 1989). However, cross-infection must still be guarded against by the use of plastic waterproof socks in public areas.
The sports shoe
The design of sports shoes has received a great deal of attention over the last three decades. This interest has to a large extent been market-led due to the massive increase in the number of people jogging. Manufacturers vie with each other to produce a shoe feature which can act as a ‘unique selling point’ to give them an increased market share.
There is little doubt that shoe design has improved, and that athletes have benefited from this. However, many developments are simply variations on the same theme and give little substantial improvement to overall shoe design. In addition, the mounting cost of sports shoes makes it imperative that athletes receive the right advice concerning the shoe which will best suit their foot and be appropriate to their sport.
As most sports involve running, more emphasis will be given to the features of running shoes, as many of these features are carried over into other sports footwear.
Forces acting on the foot
During the stance phase of running, the foot must accommodate to three phases, heel strike, mid-stance and toe off, during which the biomechanics of the foot change considerably. At heel strike the single force of the foot moving downwards and forwards may be resolved into two components. The first is an impact stress acting vertically, and the second a horizontal shearing force, creating friction. Not all athletes strike the ground with the heel when running. For some 80% the initial contact point is at the heel (Frederick, Clarke and Hamill, 1984). The ground reaction force curve in this case shows an initial (passive) peak at heel strike of about half bodyweight, occurring 20–30 ms after heel strike. A secondary (active) peak occurs approximately 100 ms after heel contact as the centre of pressure moves over the ball of the foot prior to toe off (Fig. 12.18).
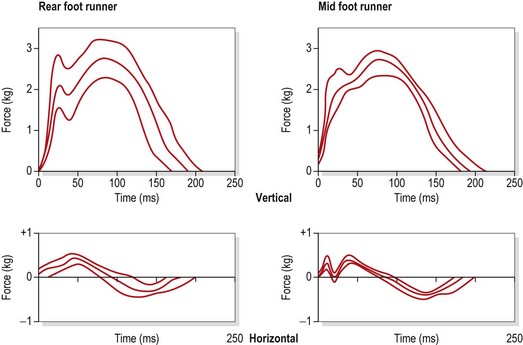
Other runners show a centre of pressure over the mid-foot or rearfoot (Fig. 12.19). The magnitude of the force acting on the foot can be as much as three times bodyweight.
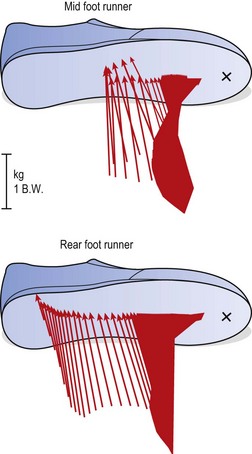
Figure 12.19 Force vector curves for rearfoot and mid-foot runners.
From Segesser and Pforringer (1989), with permission.
The rearfoot runner strikes the ground with the knee locked, and consequently will require more shock attenuation from the sports shoe. The mid-foot or forefoot striker has the knee slightly flexed, and so part of the contact shock is absorbed by the elasticity of the knee structures.
Keypoint
A rearfoot runner strikes the ground with the knee locked, and will require more shock absorption from a sports shoe. Mid-foot or forefoot strikers have the knees slightly flexed, and so some shock is absorbed by the knee.
In some cases, the heel does not touch the ground at all, leaving the stance phase under the control of the posterior leg muscles. With this type of runner, the shock-absorbing function of a heel wedge will be under-utilized.
During mid-stance there can be 5° of abduction of the foot, causing friction between the shoe and running surface. This creates a torsion force which tends to rotate the upper part of the shoe in relation to the sole (Cavanagh, 1989).
Components of a running shoe
Running shoes are manufactured on a model of a foot called a last. Four last shapes are generally used: board, slip, combination and curved.
Keypoint
The last is a foot-shaped model used to form the shoe in manufacture. Four types are used in sport − slip, board, combination and curved.
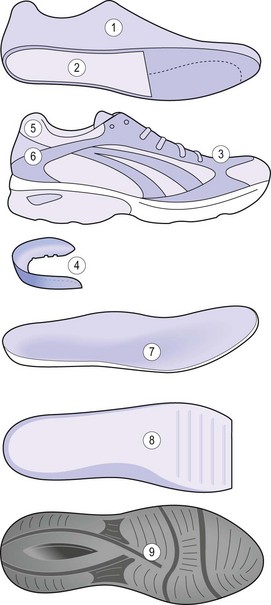
Figure 12.20 Parts of the sports shoe: (1) last; (2) combination last construction; (3) upper—synthetic material and mesh for ventilation; (4) motion control device; (5) Achilles flex notch; (6) heel counter; (7) inner sole—removable; (8) midsole; and (9) outsole.
Adapted from Neale and Adams (1989).
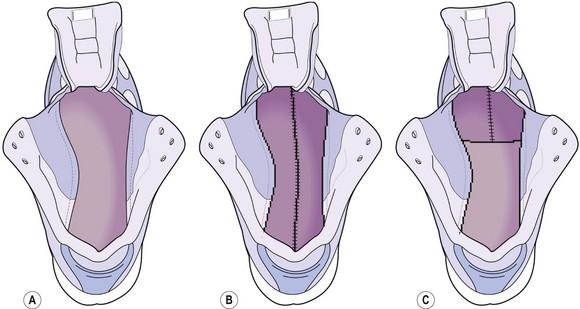
Figure 12.21 Lasts: (A) fully board lasted; (B) slip lasted; and (C) combination lasted.
Adapted from Neale and Adams (1989).
The outer sole (Fig. 12.22) of a shoe is generally a carbon rubber material with treads or studs cut in. The outer sole must provide a combination of four features: grip (traction), durability, flexibility and light weight. Studs provide better cross-country grip while bars are more durable on hard surfaces and so better suited to road shoes. However, the thicker studs or cleats of a cross-country or fell-running shoe will also add weight, so faster road-racing shoes tend to have thin, smoother soles.
Beneath the sole is the mid-sole, extending the full length of the shoe, and the wedge which begins behind the metatarsal heads and extends back to the heel. These take the place of the wooden ‘shank’ of the traditional street shoe. Both the mid-sole and wedge are designed for cushioning, giving good elastic recoil, but they must also maintain good foot control. They are usually two or three layers of different foam materials, such as ethyl vinyl acetate (EVA), or more expensive polyurethane. Thicker materials tend to give better cushioning, but they will also raise the foot off the ground, creating greater leverage forces if the foot contacts the ground at the side of the sole. The mid-sole may be either single density with the same material running through its full length, or dual density where different materials are used for the heal and forefoot sections.
On top of the mid-sole is the insole board, again running the whole length of the shoe. This semi-rigid board stops the foot from twisting and so provides stability. The edge of the shoe upper is usually fastened below the insole board, and the board itself may be chemically treated to resist deterioration from moisture or micro-organism growth.
The heel counter provides rearfoot stability, helping to prevent overpronation and is usually a hard thermoplastic, which will keep its rigidity. Poorer quality shoes may have cardboard heel counters which will feel stiff when the shoe is new, but quickly soften and allow excessive rearfoot motion. Often the heel counter itself will have an additional support.
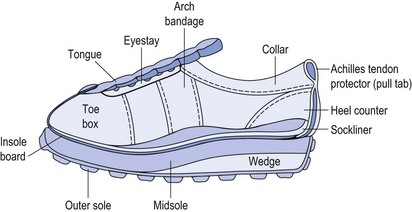
The shoe upper is contoured to the foot, and made from three sections. The ‘vamp’ covers the forefoot, and the mid-foot and hindfoot are covered by the medial and lateral quarters, respectively. The nylon upper provides lightness and breathability, and is supported by the eyestay and arch bandage. The eyestay will normally have eyelets for lacing, and the arch bandage is positioned at the highest point of the longitudinal arch of the foot.
The foot rests within the shoe, directly on top of the sock liner. This should be removable for washing and can also have further padding, such as gel or air sacks, incorporated into it. The liner is designed primarily to reduce friction and absorb sweat, and may be removed when an orthotic device is placed into the shoe.
The ankle collar should be heavily padded and soft, and the heel tab (pull tab) should be notched to prevent friction on the Achilles tendon during toe off. Some older designs of sports shoes still have so-called ‘Achilles tendon protectors’. Unfortunately, the effect of these is usually to injure rather than protect. As the foot is plantarflexed, the Achilles tendon tab will press onto the Achilles tendon causing friction, one cause of Haglund’s syndrome. Shoes of this type may be modified by cutting a slot down each side of the tab or simply cutting the tab off, providing neither of these solutions interferes with the overall shoe structure.
Many shoes have variable lacing systems to accommodate different foot widths and ensure that the shoe fits the foot snugly. With reference to shoe width, it is important to encourage athletes to stand and walk around/jog in sports shoes before they buy them. Obviously the foot spreads with weight bearing, so if the shoe is tried on when sitting it will not give an accurate impression of fit.
Shoe function
Cushioning effects of shoes have been shown to reduce initial impact at heel strike by as much as 50% (Light, McLellan and Klenerman, 1980; Subotnick, 1989). The aim is to reduce or ‘attenuate’ the peak forces to levels which are well tolerated by the human body, and which do not result either in trauma or overuse injury. At the same time, the forces produced at toe off have to be conserved to maintain running efficiency.
Heel materials which are too soft will compress or ‘bottom out’, while those which are too hard reduce cushioning. In addition, the construction of the shoe will also affect shock absorption. A stiff insole board, for example, cemented to a soft mid-sole, will give the shoe a functional hardness usually found only with much firmer mid-sole materials (Frederick, 1989).
The overhand or ‘flare’ of the sole of a running shoe creates leverage force which exaggerates pronation and foot slap (Fig. 12.23). When running barefoot, the subtalar joint axis lies over the ground contact point as does the ankle joint axis (Fig. 12.23A). Wearing a typical running shoe, the leverage force created by the heel flare places the ground contact point further away from the subtalar joint axis, thus increasing the leverage effect by a factor of three (Fig. 12.23B). In the sagittal plane, the heel flare moves the ground contact point back, further from the ankle joint, thus increasing the leverage effect. To compensate, the anterior tibial muscles have to work harder. By altering the heel to a more rounded design, and using a shoe with a dual density mid-sole, overpronation can be limited.
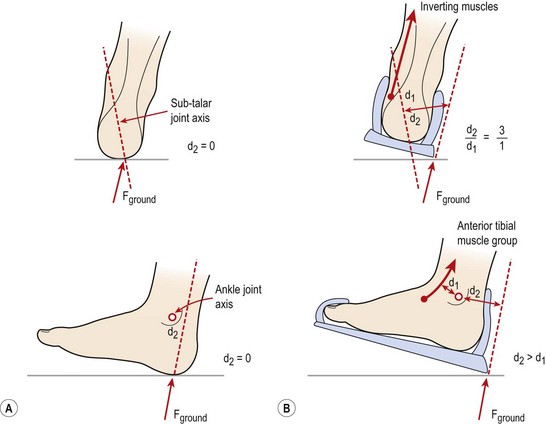
Figure 12.23 Effect of leverage in running shoes. (A) Running barefoot, the subtalar joint axis lies over the ground contact point, as does the ankle joint. (B) The ‘overhang’ of the shoes moves the ground contact point further from the subtaloid and ankle joints, increasing the leverage effect. Muscle action is required to compensate.
From Subotnick (1989).
The sole of a sports shoe should bend at a point just proximal to the metatarsal heads, to an angle of about 30°. Bending a stiffer sole may increase energy expenditure, and could therefore lead to local muscle fatigue. A lighter shoe is more energy conserving. Frederick (1985) showed that carrying 100 g excess weight on the foot increased energy expenditure by 1%; enough, he claimed, to add 1 or 2 minutes on to the time of a competitive marathon runner. Similarly, softer soled shoes are more energy conserving. The same author showed a 2.8% reduction in energy expenditure for subjects wearing soft-soled shoes while running a marathon.
The ideal combination of features in a running shoe is unfortunately not possible. There is always a compromise because many of the attributes are contradictory. Cushioning conflicts with qualities of stability and flexibility. Decreasing the hardness of the sole can increase pronation, so to get adequate cushioning, a thicker more shock-absorbing sole is chosen rather than a softer one.
By combining data from various sources, Frederick (1989) analysed the relationship between heel height, maximum pronation and hardness of a sole to find an ‘ideal’ combination. He concluded that optimum cushioning and rearfoot control are obtained in a shoe with a heel height of 25–35 mm with cushioning values of 40–55 shore A. Hardness is quantified by measuring the resistance of a material to the penetration of a defined object. The shore A scale runs from 0 (softest) to 100 (hardest).
This combination would, however, give a reduction in sole flexibility, as highly flexible soles are usually soft and thin. Fig. 12.24 demonstrates the stresses produced when a sole is bent. The top of the sole is compressed, and the bottom tensioned. To make the sole more flexible, while still maintaining its cushioning effect, a bar of softer material is placed in the top layer of the sole just behind the metatarsal heads. In addition, grooves are cut in the bottom of the sole at the point of bending.
Figure 12.24 Stresses produced when the sole is flexed. The bottom layers are in tension, while the top layers are compressed.
From Segesser and Pforringer (1989), with permission.
Fitting a running shoe
The correct fit of a running shoe is vital. Most individuals have one foot slightly larger than the other, so both shoes must be tried on. Fit the shoe to the larger foot, and use extra padding for the smaller foot. If the shoe is too narrow, extra stress may be placed on the longitudinal arch (Zachazewski, Magee and Quillen, 1996) and callus formation over the metatarsal heads is more likely. To test for correct shoe width, take all of the bodyweight through the shoe and ensure that firstly the shoe does not bulge over the sole (too small) and secondly that creases do not form in the shoe upper (too big).
The toe box must be long enough and wide enough to allow the toes to spread and to enable them to fully extend (flatten out). In general the end of the shoe should be about 1.0 cm longer than the end of the longest toe. It is often easier simply to take the insole out of the shoe and rest the foot on this to assess correct length. Palpate the longest toe when the shoe is on the foot, and also palpate the forefoot at its widest part (first MP joint) to ensure that the toe is not being pushed into a valgus position. Ensure that the highest point of the mid-foot fits well into the shoe.
For running, the shoe should flex at the first MP joint, and this can be assessed simply by holding the main shoe in one hand and pressing the sole with the other. Excessive flare of a shoe heel will introduce dangerous leverage forces on the foot and broadly speaking the flare should not extend beyond the apex of the malleoli.
The shape of the shoe ‘footprint’ is called the last, and this may be straight or curved. A straight last is usually more stable and a curved last less stable. Athletes with a very flexible (pronating) foot will need more control in a shoe and should therefore chose a straight lasted shoe. Several points are summarized in Table 12.1.
Table 12.1 Fitting a running shoe
After Zachazewski, Magee and Quillen (1996).
Is a running shoe necessary?
Robbins and Hanna (1987) argued that habitually unshod humans are not susceptible to chronic overloading of the foot. Locomotion in barefoot adapted subjects (those who regularly run unshod) differs considerably from that of normal shod subjects. When walking, unshod subjects attempt to grip the ground with their toes, and when running the medial longitudinal arch flattens completely during mid-stance. Foot flattening when running unshod is probably a result of eccentric muscle action and elastic deformation of the intrinsic foot musculature and plantar fascia. Robbins and Gouw (1990) claimed that this response is behaviourly induced in the barefoot adapted runner. They argued that the subject was attempting to minimize discomfort by transferring forefoot load from the metatarsal phalangeal joints to the distal digits. This process, they claimed, results in hypertrophy of the intrinsic musculature, and relaxes the plantar fascia (Fig. 12.25).
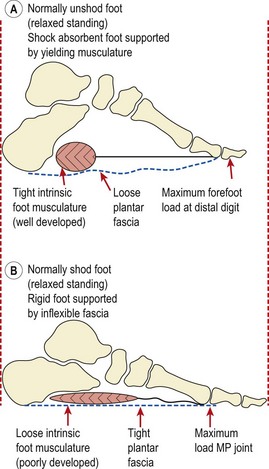
Figure 12.25 Function of intrinsic musculature in the (A) unshod and (B) shod foot.
From Robbins, S.E. and Gouw, G.J. (1990) Athletic footwear and chronic overloading. Sports Medicine, 9 (2), 76–85. With permission.
Robbins and Gouw (1990) argued that this shock moderating behaviour of the foot is related to plantar sensibility. The subject attempts to minimize discomfort by increasing the activity of the intrinsic muscles. However, a running shoe with a thick soft sole will mask sensation to the plantar surface of the foot, and so the subject will not use the intrinsic muscles to their full extent.
The above authors therefore recommended that runners run barefoot, after a progressive period of adaptation. Where a runner is not able to do this each day, or where safety factors prevent it, Robbins and Gouw advised a less yielding shoe which provides adequate sensory feedback.
When assessing proprioceptive function of the foot, foot position error has been shown to be 107.5% poorer with subjects wearing athletic footwear than those who were barefoot. In addition, those who wore footwear were unable to distinguish between a flat surface and a 20° slope angle when blindfolded (Robbins, Waked and Rappel, 1995). These authors argued that the use of footwear was largely responsible for ankle injury, in that it reduced the input from plantar cutaneous mechanoreceptors.
Athletic footwear has also been shown to contribute to falling frequency (Robbins et al., 1994). Using balance beam walking, these authors found that mid-sole hardness was positively related to stability, while mid-sole thickness was negatively related. The authors concluded that shoes with thick, soft soles acted to destabilize an individual whereas thin, hard-soled shoes provided superior stability. Waddington and Adams (2000) compared barefoot conditions, athletic shoes and textured insoles within athletic shoes to determine the effect on ankle movement discrimination. They found that athletic shoes gave significantly worse movement discrimination scores compared to barefoot levels, confirming the work previously quoted. However, the addition of a textured insole improved movement discrimination back to barefoot levels, through enhanced cutaneous feedback on the sole of the foot.
The court shoe
In running, foot movements occur cyclically, but in court games such as tennis, squash and badminton the movements are more varied, both in direction and speed. The casual tennis player makes contact mostly with the heel and less with the ball of the foot. However, when a player is under pressure the situation is reversed. Now contact is more frequently made with the ball of the foot than the heel, and contact with the medial and lateral edges of the foot is increased (Nigg, Luthi and Bahlsen, 1989).
Movement most commonly occurs in the forward direction, but when under pressure, the tennis player moves laterally more frequently. This movement is often combined with contact on the forefoot.
A court shoe must allow all of these movements. The same heel–toe mechanism found in a running shoe is required, but in addition, force attenuation from forefoot contact is needed. The frictional characteristics of the shoe to surface are important. Both translational and rotational movements are needed, translation less so in surfaces which permit some degree of sliding, such as indoor courts or sand/granules.
Because the demands placed on the foot when playing court games are so different to those encountered in road running, athletes must be discouraged from wearing the same shoes for both sports unless they use specifically designed ‘cross training’ footwear. During lateral movements in particular, the leverage involved with the higher (flared) heel of the running shoe makes injury much more likely. Similarly, tennis shoes do not give adequate rearfoot control or shock attenuation for running.
The soccer boot
In football, the ball may reach velocities of 140 km/h (Masson and Hess, 1989). This speed, combined with the weight of the ball, especially when wet, leads to deformation of both the boot and foot with kicking. Forces generated may lead to microtrauma to the foot and ankle. Soccer footwear must therefore be as light as possible to minimize any excessive forces created by kicking. At the same time, the shoe must provide both support and protection for the foot.
Combinations of rotation and flexion with the foot fixed to the ground are particularly taxing on the knee structures. Most boots unfortunately compound this problem by the use of cleats or studs, which, although improving grip on a wet surface, will also increase rotation forces by reducing ‘give’. Indoor surfaces in some cases offer greater grip with similar problems, and shoes need a sole with a greater number of smaller studs to compensate for this.
Shoes must allow the increased range of movement required in soccer, and be flexible enough to accommodate forefoot rocking. Any studs must be placed to avoid pressure irritation to the plantar aspect of the foot. Studs on the heel are placed towards the outside of the shoe to avoid rocking or buckling on weight-bearing.
Acevedo J.I., Beskin J.L. Complications of plantar fascia rupture associated with corticosteroid injection. Foot and Ankle International. 1998;19(2):91-97.
Akermark C., Saartok T., Zuber Z. A prospective 2-year follow up study of plantar incisions in the treatment of primary intermetatarsal neuromas (Morton’s neuroma). Foot and Ankle Surgery. 2008;14:67-73.
Bowers K.D., Martin R.B. Turf toe: a shoe-surface related football injury. Medicine and Science in Sports and Exercise. 1976;8:81-83.
Carmines D.V., Nunley J.A., McElhaney J.H. Effects of ankle taping on the motion and loading pattern of the foot for walking subjects. Journal of Orthopaedic Research. 1988;6:223-229.
Cavanagh P.R. The biomechanics of running and running shoe problems. In: Segesser B., Pforringer W., editors. The Shoe in Sport. Wolfe, London: Year Book Medical Publishers, 1989.
Cibulka M.T. Management of a patient with forefoot pain: a case report. Physical Therapy. 1990;70(1):55-58.
Clanton T.O., Butler J.E., Eggert A. Injuries to the metatarsophalangeal joints in athletes. Foot and Ankle. 1986;7:162-176.
Creighton D.S., Olson V.L. Evaluation of range of motion of the first metatarsophalangeal joint in runners with plantar fasciitis. Journal of Orthopaedic and Sports Physical Therapy. 1987;8:357-361.
Dandy and Edwards. Essential Orthopaedics and Trauma. Edinburgh: Churchill Livingstone; 2009.
Frederick E.C. The energy cost of load carriage on the feet during running. In: Winter D.A., et al, editors. Biomechanics IX. Champaign, Illinois: Human Kinetics Publishers, 1985.
Frederick E.C. The running shoe: dilemmas and dichotomies in design. In: Segesser B., Pforringer W., editors. The Shoe in Sport. Wolfe, London: Year Book Medical Publishers, 1989.
Frederick E.C., Clarke T.E., Hamill C.L. The effect of running shoe design on shock attenuation. In: Frederick E.C., editor. Sports Shoes and Playing Surfaces. Champaign, Illinois: Human Kinetics Publishers; 1984:190-198.
George F.J. Year Book of Sports Medicine. In: Shephard R.J., editor. Year Book of Sports Medicine. Chicago: Year Book Medical Publishers; 1989:75.
Horn L.M., Subotnick S.I. Surgical intervention. In: Subotnick S.I., editor. Sports Medicine of the Lower Extremity. London: Churchill Livingstone, 1989.
Kaltenborn F.M. Manual Mobilisation of the Extremity Joints, fourth ed. Norway: Olaf Norlis Bokhandel; 1989.
Lemont H., Ammirati K.M., Usen N. Plantar fasciitis: a degenerative process (fasciosis) without inflammation. Journal of the American Podiatric Medical Association. 2003;93(3):234-237.
Light L.H., McLellan G.E., Klenerman K. Skeletal transients on heel strike in normal walking with different footwear. Journal of Biomechanics. 1980;13:477.
Lorimer D., French G., O’Donnell M., Burrow J. Neale’s Disorders of the Foot, sixth ed. Edinburgh: Churchill Livingstone; 2002.
Magee D.J. Orthopedic Physical Assessment, fourth ed. Philadelphia: Saunders; 2002.
Mann R.A., Reynolds J.C. Interdigital neuroma: a critical analysis. Journal of Foot and Ankle Surgery. 1983;3:238.
Marshall P., Hamilton W.G. Cuboid subluxation in ballet dancers. American Journal of Sports Medicine. 1992;20:169-175.
Masson M., Hess H. Typical soccer injuries their effects on the design of the athletic shoe. In: Segesser B., Pforringer W., editors. The Shoe in Sport. Wolfe, London: Year Book Medical Publishers, 1989.
Millar B., Moore J. Successful topical treatment of hand warts in a paediatric patient with tea tree oil. Complementary Therapies in Clinical Practice. 2008;14(4):225-227.
Murphy C. Plantar fasciitis. Sportex Medicine October. 2006:14-17.
Neale D., Adams I.M. Common Foot Disorders. London: Churchill Livingstone; 1989.
Nigg B.M., Luthi S.M., Bahlsen H.A. The tennis shoe: biomechanical design criteria. In: Segesser B., Pforringer W., editors. The Shoe in Sport. Wolfe, London: Year Book Medical Publishers, 1989.
Palastanga N., Field D., Soames R. Anatomy and Human Movement. Oxford: Heinemann Medical; 1989.
Reid D.C. Sports Injury Assessment and Rehabilitation. London: Churchill Livingstone; 1992.
Robbins S., Waked E., Rappel R. Ankle taping improves proprioception before and after exercise in young men. British Journal of Sports Medicine. 1995;29(4):242-247.
Robbins S., Waked E., Gouw G.J., McClaran J. Athletic footwear affects balance in men. British Journal of Sports Medicine. 1994;28:117-122.
Robbins S.E., Gouw G.J. Athletic footwear and chronic overloading. Sports Medicine. 1990;9(2):76-85.
Robbins S.E., Hanna A.M. Running related injury prevention through barefoot adaptations. Medicine and Science in Sports and Exercise. 1987;19:148-156.
Rodeo S.A., O’Brian S.J., Warren R.F. Turf toe: an analysis of metatarsophalangeal joint sprains in professional football players. American Journal of Sports Medicine. 1989;17(4):125-131.
Rodeo S.A., O’Brian S.J., Warren R.F., et al. Turf toe: diagnosis and treatment. Physician and Sports Medicine. 1989;17(4):132-147.
Rodgers M.M., Cavanagh P.R. Pressure distribution in Morton’s foot structure. Medicine and Science in Sports and Exercise. 1989;21:23-28.
Satchell A., Sauragen A., Bell C., Barnetson R. Treatment of interdigital tinea pedis with 25% and 50% tea tree oil solution: A randomized placebo controlled blinded study. Australasian Journal of Dermatology. 2002;43(3):175-178.
Segesser B., Pforringer W., editors. The Shoe in Sport. London: Wolfe, 1989.
Subotnick S.I. Sports Medicine of the Lower Extremity. London: Churchill Livingstone; 1989.
Tanner S.M., Harvey J.S. How we manage plantar fasciitis. Physician and Sports Medicine. 1988;16(8):39-47.
Tong M., Altman P., Barnetson R. Tea tree oil in the treatment of tinea pedis. Australasian Journal of Dermatology. 1992;33(3):145-149.
Waddington G., Adams R. Textured insole effects on ankle movement discrimination while wearing athletic shoes. Physical Therapy in Sport. 2000;1(4):119-128.
Zachazewski J.E., Magee D.J., Quillen W.S. Athletic Injuries and Rehabilitation. Philadelphia: Saunders; 1996.