Chapter 1 Ruminant History, Physical Examination, and Records
OBTAINING THE HISTORY
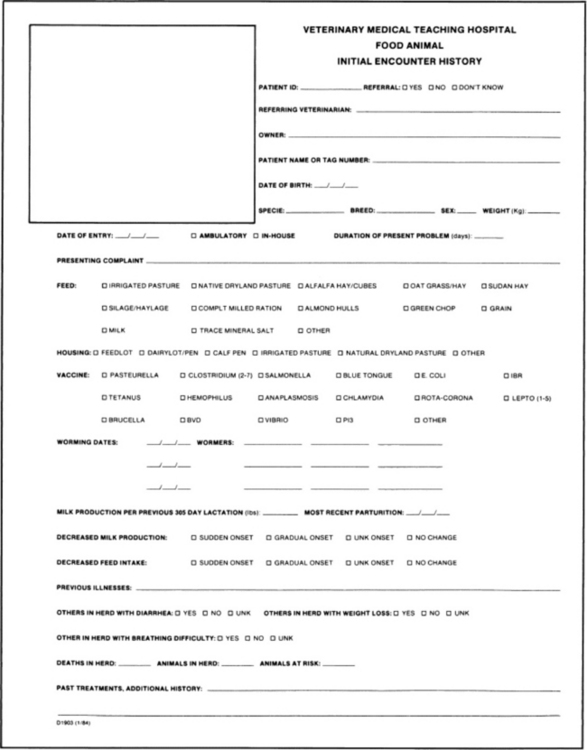
The initial and often the most important step in the diagnostic approach to the sick ruminant is the physical examination. Throughout this process an anamnesis is obtained by asking questions of the owner or manager during the examination of the animal. The examiner should obtain the signalment either by observation or by questioning the owner. The information that one wishes to obtain while taking the history is that related to the chief, or presenting, complaint—that is, the complaint, the duration, whether the onset was gradual or sudden, and any associated signs that have been noted. For females, one must know when the last parturition occurred, and for dairy cows, what the production parameters were in the previous lactation as well as in the current lactation. With dairy cows a drop in milk production is often the only sign noted by the owner. Weight can be either approximated, via heart-girth measurements, or determined exactly if facilities exist to do so. What and how the animal is fed are questions to be asked. Does the animal refuse any or all of the feed offered? Is there more than one ration or feeding regimen for this particular operation? If so, are these same signs noted in animals exposed to different feeding practices? The examiner also obtains vaccination and worming history and inquires about pasture or housing practices to determine the influence that management factors have on the incidence of the disease. Previous diseases noted in the herd, therapeutic regimens used, and resolutions of previous problems are pertinent aspects. Finally, the examiner should note the treatment history of the patient. An example of a history questionnaire that can be used for ruminants is included (Fig. 1-1). Specific problems that are noted in the history or physical examination can be looked up on pp. 21 and 22, and lists of differential diagnoses considered.
EXAMINATION
A complete examination should always be performed even if the presenting complaint is easily recognizable. The physical examination provides the veterinarian with information that is used to assess the health status of the patient. This information, combined with that obtained while taking the history, enables the practitioner to determine which specific signs of disease are present and often to localize the disease process to specific organ systems. The physical examination also helps to determine which ancillary diagnostic tests must be performed. Additional information gathered during the examination may reveal disorders other than the presenting complaint that warrant further attention and may have a profound influence on the prognosis of the case. Realistically, economic and temporal constraints preclude full examinations in some cases. In these situations the veterinarian must be familiar enough with the complete physical examination to know which aspects can be excluded and which should be performed.
A systematic approach to the animal must be developed and used in every physical examination. The first step is to form an initial overall impression by observing the animal from a distance. The animal is then restrained and examined topographically, beginning on one side, moving to the other, then evaluating the rear and finally the head and neck. Thus individual organs and systems are examined completely, although disjointedly, and the information gained is correlated to form the complete diagnosis.
Visual Examination
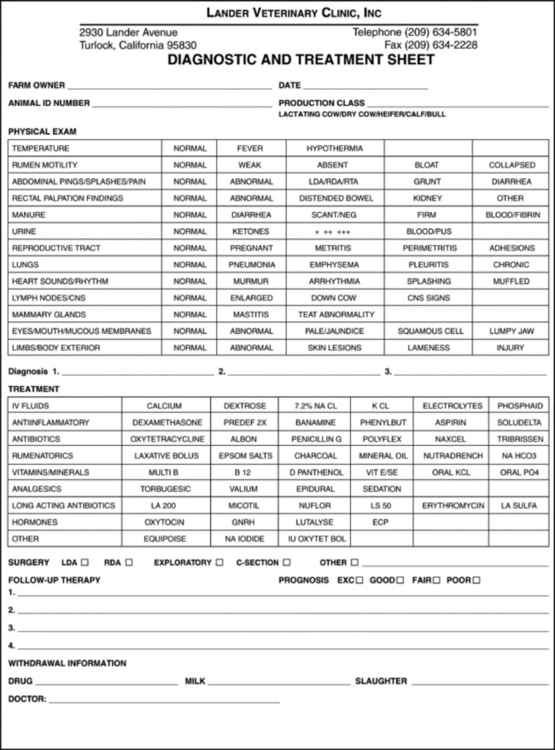
As observations are made and a physical examination performed, it is important to follow a systematic approach and to record findings. A checklist has been found to be extremely useful (Fig. 1-2). While observing the animal from a distance, the examiner should assess its posture, gait, behavior, and physical condition. Observation of the other members of the flock or herd helps to differentiate normal from abnormal characteristics under each particular management system because normal may vary from farm to farm and because what is considered “normal” for a farm by the owner or herdsman might actually be abnormal; this information is valuable for assessing the incidence of a disease or disorder that is caused by management. As more animals in more herds are observed, a background of knowledge is gained that allows the practitioner to assess these management deficiencies more reliably.
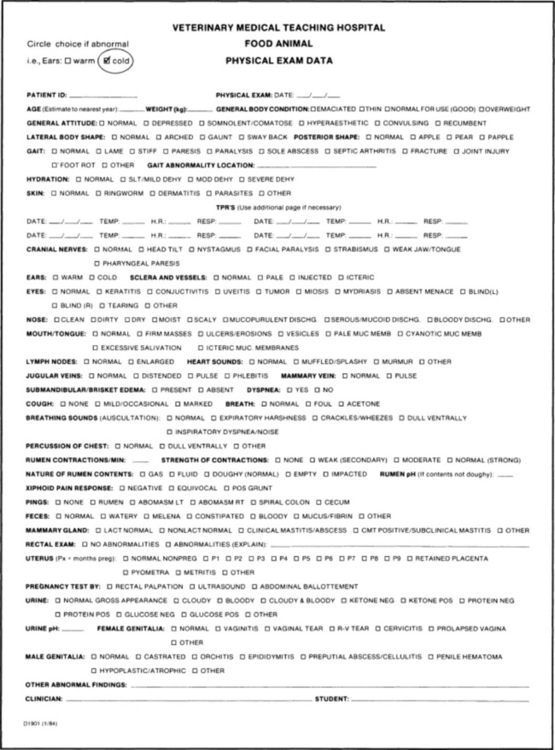
Fig. 1-2 Example of a data sheet for the recording of the pertinent findings from the physical examination.
The general appearance and conformation of the animal are included in determining posture. These are assessed in light of the age and breed of the patient. Determining abnormalities in posture can be difficult; however, noting these subtle changes can contribute greatly to the diagnosis of a disease process. Conformation is recognized by looking at the overall size and shape with particular regard to height, width, and relationship of the head, neck, and legs to the trunk. The general appearance of the patient in light of overall conformation can then be assessed. Determining a body condition score and correlating it with stage of lactation can offer insight into the course of the presenting complaint. Is the young, growing animal within breed standards for size and weight? (See Chapters 9 and 13.) The condition of the hair coat and presence of external parasites can be noted during the physical examination (e.g., frank hair loss, as seen in louse infestation, or dander and scruffiness of the hair coat, as seen in chronic debilitating diseases).
Observe the animal for signs of abdominal splinting or arching of the back, as can be seen with peritonitis. This posture can also be noted with other disease processes when these produce pain in the ventral abdomen. Lateral curvature of the spine could indicate a congenital defect or a chronic spinal lesion. Carrying the tail up away from the body is seen with conditions resulting in pain or irritation in the perineal region, vagina, or rectum. Standing with all four legs in the classic “saw-horse” stance with the neck and tail held erect is typical of tetanus. Abduction of the elbows is seen in disorders that cause thoracic pain. Lameness can be noted by observing unwillingness to bear weight fully on the affected limb, while either standing or walking. Loss of extensor or flexor capabilities of the joints is seen in nerve paralysis or paresis; it can also be caused by tendon and/or joint contractures, in which case joints are rigid. Walking as if all four feet are sore may indicate laminitis. With bright and alert recumbent animals, a thorough examination to rule out fractures or severe joint trauma is essential. Once these have been ruled out, inability to stand may be indicative of generalized muscular paresis or paralysis. These can be of a primary nature, as with lesions within the spinal column causing cord compression, or secondary to mineral or electrolyte deficiencies (e.g., hypocalcemia, hypomagnesemia, or hypokalemia).
To be able to judge the behavior of the animal as being normal or abnormal, the observer must call on a large amount of experience. Observing the animal from a distance allows assessment of eating and drinking behavior, as well as assessment of the subject as it is ruminating, urinating, and defecating. How the animal gets up or lies down and how it ambulates are important. Signs indicative of estrus or signs commonly seen with calving might be considered normal or abnormal, given the history and behavior of the animal during these events. Observing the patient during the milking process may also be beneficial. The influence of the manager on animal behavior is very important, as is the overall temperament of the particular breed or herd in question. Normal animals react to the approach of a human being by moving away; however, those that have had extensive contact with people may be more inquisitive. Within a herd one can note animals that are more tolerant than others, more stubborn, more restless, and more anxious. These traits are not necessarily abnormal and need to be differentiated from behavior that would be considered secondary to disease. In general, one must determine whether the behavior is one of a depressed or apathetic animal or of a hyperexcitable or frenzied animal.
Nutritional status and physical condition are assessed by means of observation and palpation. Special attention is paid to the dewlap, the spinous processes of the thoracic and lumbar vertebrae, the shoulder area, and the area around the tailhead. Determination of body condition will then result in a classification of the animal as being anywhere from severely emaciated or cachectic to extremely overconditioned or fat (see Chapters 9 and 13 for body scores). Next it must be determined whether the condition is of a primary or nutritional nature or the result of disease. Disease processes can influence or be influenced by the animal’s body condition. Extremely thin animals are seen in primary undernutrition and also with chronic disease. Females carrying multiple fetuses and lactating animals with metabolic abnormalities secondary to abomasal displacements would also show signs of weight loss. Overconditioned animals are at greater risk for a wide variety of disorders primarily related to the accumulation of fat in the liver and excessive fat storage in the omentum.
Physical Examination
With the animal properly restrained, the physical examination can now progress to specific palpation, auscultation, and percussion. Obtaining a sample of urine for urinalysis is of great value if incorporated into the physical examination; it is easy to perform with the use of dipsticks such as N-Multistix. Stroking the perineal region can aid in eliciting urination in the bovine; however, even this is futile if the animal is apprehensive. Consequently, it is recommended that this be done first, while the patient is still fairly relaxed. In the male, elicitation of urination is slightly more difficult and requires massaging of the preputial orifice. Another method is to wash the outside of the prepuce with warm water, but this is less successful. In the female sheep and goat, stroking the perineal area can be attempted, but positive results are rarely achieved. A method that is more reliable but that causes the animal much greater stress is to prevent it from breathing until urination is stimulated. In male or castrated male sheep and goats, gentle massage of the prepuce sometimes results in urination. If that fails, the breath-holding technique can be used. It is recommended that this not be attempted on patients that are severely compromised because of any disease process. (See Chapter 22 for further information on interpretation of the urinalysis.)
Body temperature is then measured with a rectal thermometer. Normal values for each species are given in Table 1-1. There are no absolute values, and the upper and lower limits should be adjusted as necessary to account for ambient temperature and housing. For example, if the ambient temperature is greater than 37.5° C (100° F), a body temperature of 39.5° C (103° F) may still be considered normal for the adult bovine, especially if the animal is not allowed access to shade. When body temperatures approach 41° C (106° F), as a result of very high ambient temperatures, heat stroke may occur. Keep in mind that the animal tries to maintain its body temperature within these normal limits, and marked deviation from the norm would be indicative of a disease process. A markedly elevated temperature is seen in acute, severe inflammatory processes. Pathologic lowering of the body temperature is seen in disorders that cause an inhibition of metabolism such as postparturient paresis, neonatal hypoglycemia, the end stages of a chronic disease, or severe septicemia resulting from gram-negative bacteria. There is a normal diurnal variation in body temperature of as much as 0.5° to 1° C. In the female there can also be a slight increase in temperature in the days preceding estrus. Neonates are poor thermoregulators and often have a normal body temperature that is 0.5° to 1° C higher than that of adults.
Table 1-1 Normal Values for Temperature in the Ruminant1-3
| Animal | Degrees Celsius | Degrees Fahrenheit |
|---|---|---|
| CATTLE | ||
| Adult | 38–39 | 100.5–102.5 |
| Calf | 39–40.5 | 101.5–103 |
| SHEEP | ||
| Adult | 39–40 | 102–103.5 |
| Lamb | 39.5–40.5 | 102.5–104 |
| GOAT | ||
| Adult | 38.5–39.5 | 101.5–103.5 |
| Kid | 39–40.5 | 102–104 |
In the evaluation of the thoracic and abdominal cavities, the initial step is the ballottement of the abdomen on the right side. An increase in fluid being sequestered intraabdominally could be related to some degree of intestinal or ruminal stasis or associated with an increase in peritoneal fluid, as with peritonitis or ruptured bladder. Ballottement can also reveal whether any firm mass such as a fetus, impacted abomasum, abscess, or tumor is located in the abdomen. In goats the abdominal fat pad is quite prominent and tends to obscure any significant finding on ballottement. Deep palpation of the paralumbar fossa can sometimes reveal masses in this region, including lymphomas, fat necrosis, or abscesses. In goats, lambs, and calves, two hands are used to deeply palpate the abdomen; the normal freely movable left kidney is usually readily palpable. On the right side an enlarged or painful liver or kidney can be noted. Palpation of an abnormal swelling or firmness, especially with the elicitation of pain, indicates a problem that must be further evaluated.
The spinal column and ribcage are then palpated; the presence of fractures, enlargement of the costochondral junctions, or the elicitation of pain is noted. Enlargement or fractures of the costochondral junctions are commonly seen in young animals with deficiencies of calcium, copper, or vitamin D.
Auscultation with concurrent percussion by snapping the finger against the thoracic and abdominal walls is the next procedure. Gas trapped within abdominal viscera elicits a “pinging” sound that can be heard with the stethoscope. Localization of these gas pings to certain areas within the abdomen is helpful in determining which alimentary structure is involved (Figs. 1-3 to 1-5). If the cecum is enlarged and gas filled, an abdominal ping can be heard. This can extend caudally to the tuber coxae and cranially through the paralumbar fossa and under the ribcage on the right side (see Fig. 1-3). The diameter of this area can be variable and range from 6 inches (15 cm) in a cecal displacement to 3 feet (1 m) horizontally in cecal torsions. Spiral colon pings are generally localized to the right dorsocranial paralumbar fossa and rarely extend farther forward than the tenth intercostal space. They tend to be round areas 10 inches (25 cm) or less in diameter centered high under the last rib (see Fig. 1-3) and are commonly found in sick cattle that are anorectic. These pings have no specific diagnostic significance. Gas pings associated with a right-sided displacement or torsion of the abomasum can extend as far cranially as the ninth intercostal space and caudally into the paralumbar fossa (see Fig. 1-4). The diameter of displacements is usually 18 inches (45 cm), whereas that of torsions can be up to 3 feet (1 m). In cases of abomasal volvulus, the animal is usually exhibiting other systemic signs such as increased heart rate, dehydration, depression, scleral injection, and mild colic. In simple right-sided displacements or dilations of the abomasum, the only significant finding may be the small gas ping localized to the abomasum in a cow with depressed appetite and decreased milk production.
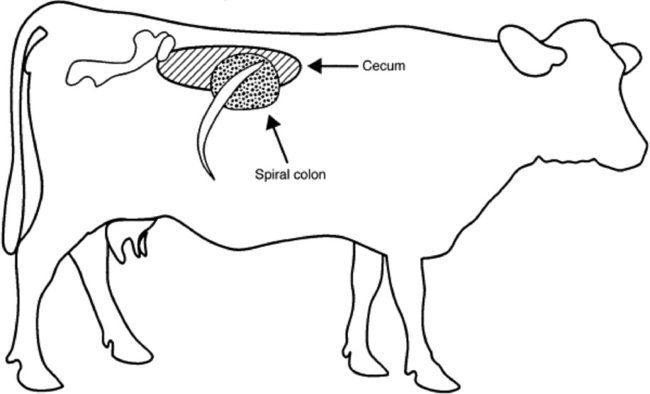
Fig. 1-3 Schematic representation of areas of gas pings elicited by percussion of the cecum and spiral colon.
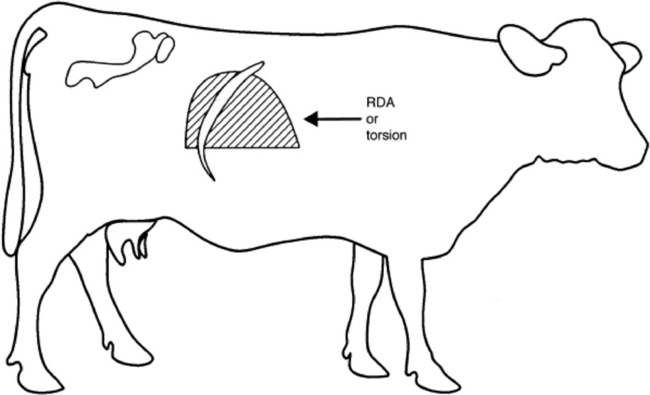
Fig. 1-4 Schematic representation of the area of the gas ping percussed in association with a right displaced abomasum (RDA) or abomasal torsion.
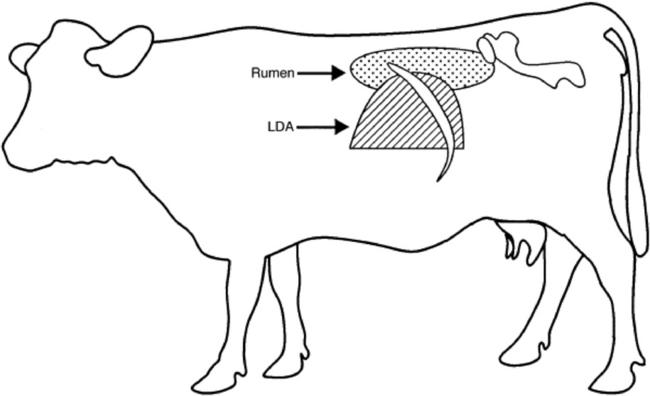
Fig. 1-5 Schematic representation of the area of the gas ping percussed in association with a left displaced abomasum (LDA) or gas ping in the rumen.
On the left side, gas pings can be noted as originating from the rumen, the peritoneum, or a left displaced abomasum (LDA). The auscultation of a gas ping that is primarily localized to the dorsal aspect of the paralumbar fossa and auscultable on both sides of the spinal column would be indicative of a pneumoperitoneum. The extent of these pings can be from the thoracolumbar junction caudally to the retroperitoneal space. Pings associated with ruminal tympany occupy the whole of the paralumbar fossa and can extend dorsally to the spinal column but generally do not extend over to the right side (see Fig. 1-5). LDA results in a gas ping that is localized, easily outlined, and approximately 12 to 18 inches (30 to 45 cm) in diameter. Caudal extent of the displacement is generally the thirteenth rib; however, it can extend into the paralumbar fossa, in which case the outline of the abomasum can be easily palpated. The LDA should ping over the eleventh rib on a line from the hip to the elbow (see Fig. 1-5). Rumen gas associated with a left-sided ping will rarely ping at this location. Identification of a fluid line within the displacement can aid in diagnosis and is accomplished by ballotting the left paralumbar fossa while auscultating the area of the gas ping concurrently, a process known as succussion. LDA often gives a pitch that changes in tone as it is percussed, as a result of movement of the rumen behind the abomasum. Often with LDA, intermittent gas bubbling or “sloshing fluid” sounds are heard. Rumen gas can be further differentiated from gas trapped in an LDA by rectal palpation of the rumen. One can also differentiate rumen gas from that trapped in an LDA by passage of a stomach tube into the rumen. Blowing into the rumen yields obviously auscultable sounds unless an LDA is present, in which case the sounds are muffled as the practitioner listens over the area of the ping. Performing a rumen or abomasal tap, the Liptac test, can further differentiate whether the ping originates from an LDA or the rumen. Fluid collected from an LDA would have a pH of less than 4, whereas that of the rumen should be 6 or higher.
The rumen is examined by both auscultation and palpation. It should have a doughy texture with a small gas cap in its dorsal regions and usually is not distended above a plane formed by the coxofemoral joints. Increased accumulation of gas within the rumen would be seen with acute primary frothy bloat and also with free gas bloat. The rumen contractions should be counted, observed, and auscultated. Normally, primary ruminal contractions occur one and one-half to three times per minute, and the force of the contraction should displace the lateral body wall at least ½ to 1 inch (1 to 2 cm). When auscultated, the ruminal contraction sounds like a dull roar that starts quietly, rises to a peak, and dies away. Hypocalcemia and peritonitis are examples of disorders that result in weak or absent ruminal contractions. Hypermotility is rarely seen but can occur and has been described in association with vagal indigestion.
The cardiac region of the thorax is auscultated next. Heart rate and rhythm are determined at this time. Rate varies among species, and age differences within species are noted. In general, older or larger animals have a slower heart rate. Table 1-2 lists the ranges of heart rate that are considered normal for the ruminant species, depending on age. Tachycardia can be seen in animals that have been stressed or excited, as in the process of restraint. However, with time the rate should return to within a more normal range. Any deviation from the normal heart rate in a quiet, relaxed animal implies a general disturbance of the normal health of the animal. Increased heart rate can be seen with fever, inflammation, pain, hypocalcemia, or metabolic disturbances that result in hypovolemia. Bradycardia is seen with conduction disorders within the heart muscle and with some metabolic disorders (uremia, hypokalemia). The most common causes of arrhythmias are atrial fibrillation in adult cattle and hyperkalemia in diarrhetic neonates. Location and intensity of the heart sounds are also important to note, because muffling or displacement of the sounds can indicate space-occupying lesions within the thorax, pericardium, or mediastinum. With pericardial effusion the heart sounds are initially dull but develop splashy washing machine sounds as a gas-fluid interface develops. This often takes weeks. Normally the heart occupies a space on the ventral thorax between the third and sixth ribs. Most of the heart mass is located on the left side of the chest; thus the heart sounds should be louder on that side. However, if the heart is muffled on the left side and louder than normal on the right, one should consider the possibility of inflammation of the pericardium or lung lobes on the left side of the chest. Displacements of the heart sounds caudally are an indication of a space-occupying lesion in the anterior thorax or mediastinum, such as an abscess or neoplasm. Cranial displacements of the heart sounds would be noted with distention of the ruminoreticulum, eventration of abdominal viscera into the thorax through a diaphragmatic hernia, or other space-occupying lesions as noted previously. If any murmurs are noted on auscultation, an attempt should be made to localize the murmur to a specific heart valve. While the heart is auscultated, the pulse should also be palpated. The easiest point to fine a pulse while the heart is being auscultated is at the vascular notch of the mandible where the facial artery is easily palpated. Pulse deficits in conjunction with an increase in heart rate are seen in arterial fibrillation and premature ventricular contractions. The heart rhythm is also noted. Dropped beats, gallop rhythm, and sinus arrhythmias should be compared with other clinical signs to determine importance.
Table 1-2 Normal Resting Heart Rates (Beats/Min) for Adult and Young (<30 Days of Age) Ruminants1-3
| Animal | Average | Range |
|---|---|---|
| CATTLE | ||
| Adult | 60 | 40–80 |
| Calf | 120 | 100–140 |
| SHEEP | ||
| Adult | 75 | 60–120 |
| Lamb | 140 | 120–160 |
| GOAT | ||
| Adult | 85 | 70–110 |
| Kid | 140 | 120–160 |
The prefemoral and prescapular lymph nodes are palpated. Enlargements would be seen with inflammatory processes occurring in the regions that they drain. The skin is then palpated, starting along the top line and moving down over the abdominal and chest walls to the ventral midline. The presence of subcutaneous gas or edema is noted, as is any elicitation of pain. Emphysema can have iatrogenic causes (e.g., be secondary to abdominal surgery) or result from pulmonary alveolar rupture, gas gangrene, or puncture wounds. Edema, if noted, is usually ventral and is the result of lowered plasma oncotic pressure or increased venous pressure. Right-sided heart failure, as seen in traumatic retic-ulopericarditis, pericarditis, mediastinal masses, or severe pulmonary disease, results in increased venous pressure. If this is the case, a distention of the jugular veins with jugular pulse should also be evident. Protein-losing enteropathies or nephropathies are causes of lowered oncotic pressure, as is liver failure, which results in a lack of synthesis of plasma proteins. Fluid and gas from subcutaneous injection of large volumes of medications such as calcium gluconate can sometimes be confusing.
The thorax is then auscultated and percussed. Respiratory rate (Table 1-3) and pattern are determined at this time, and the lungs are auscultated. If increased inspiratory or expiratory effort is noted, it should be correlated with auscultatory and percussive findings in an effort to determine lung pathology. Normal ruminant lung sounds vary greatly among species. In calves, sheep, and goats the relatively thin chest wall allows one to hear inspiratory sounds ventrally and over the large airways, whereas expiratory sounds are minimal (except in sheep, where they are frequently audible because of the large amount of mucus in sheep airways). In larger cattle, only very faint inspiratory sounds are normally heard. Lung sounds can be classified as normal or harsh (tubular) or as wheezes or crackles. These sounds can vary over the different areas of the thorax or can be found singularly over the entire lung field. Significant pulmonary pathology may be present in ruminants without any auscultable abnormalities. Total absence of lung sounds ventrally indicates pleural effusion or pulmonary abscessation with loss of airways. When ventral consolidation of the lung occurs, airway sounds are transmitted well and easily heard ventrally as pipestem sounds similar to those heard over the trachea, whereas percussion reveals a marked increase in ventral lung density. The trachea should also be auscultated. Inspiratory dyspnea and stridor are usually the result of extrathoracic obstructions to airflow (nose, pharynx, larynx, extrathorac-ic trachea). Pneumothorax can also result in loss of auscult-able airway sounds, which may be absent dorsally or entirely over the entire side if the lung has collapsed completely.
Table 1-3 Normal Resting Respiratory Rates (Breaths/Min) for Adult and Young Ruminants1-3
| Animal | Average | Range |
|---|---|---|
| CATTLE | ||
| Adult | 24 | 12–36 |
| Calf | 48 | 30–60 |
| SHEEP | ||
| Adult | 36 | 12–72 |
| Lamb | 50 | 30–70 |
| GOAT | ||
| Adult | 28 | 15–40 |
| Kid | 50 | 40–65 |
Place the middle finger in the intercostal space and slap the finger with the opposite hand or use a tablespoon and rubber hammer to accomplish percussion of the chest wall to determine the ventral lung border. Percussion is most useful in goats and calves. In sheep the wool precludes effective use of the technique, and in adult cattle the chest wall is often too thick to effectively evaluate changes in percussion tones. The chest is percussed in a dorsal-to-ventral direction, moving caudal to cranial on the chest wall. A change in resonance is noted when the ventral border is reached; a line demarcating this change in resonance is the junction of the diaphragm to the thoracic wall. In the ruminant this line should be described by joining a point at the junction of the eleventh rib and the epaxial musculature dorsally to a point at the middle of the ninth rib, then cranially to the point of the olecranon. The cranioventral portion of the percussed thorax is dull because of the heart field (approximately 3 inches [7.5 cm] above the olecranon in adult cattle; 1 to 2 inches [2.5 to 5 cm] in calves, sheep, and goats). Finding an increased area of dullness in the cranioventral lung field associated with harsh lung sounds would be an indication of lung consolidation as seen in Pasteurella pneumonia. Pulmonary emphysema (atypical interstitial pneumonia) should be considered when the lung field is larger than expected, the animal is dyspneic, and airway sounds are minimal. A ventral border that is markedly elevated and in a straight line could be an indication of pleural effusion. In this case auscultation would reveal decreased lung sounds ventrally and possibly the presence of pleural friction rubs. Acoustic percussion of the lung field can extend into the chest only to a depth of 2 to 2½ inches (5 to 6 cm). Lesions within the thoracic cavity that lie deep-er than this cannot be percussed.
The next step in the physical examination is to assess for evidence of pain in the ventral portion of the abdomen and thorax. This can be accomplished through the use of the withers pinch test or by ballottement of the xiphoid region. The withers pinch test involves auscultating the trachea while the withers are simultaneously squeezed and pushed ventrally. Painful lesions result in the ruminant resisting normal ventral movement of the spine and/or emitting a grunt or holding its breath when this test is performed. Ballottement of the xiphoid is also done while the trachea is auscultated. The xiphoid region is pushed with a knee or struck with a closed fist, and an elicitation of a grunt would indicate pain in this region. The examiner can then ballotte the remainder of the ventral abdomen and thorax to classify the lesion as localized or diffuse. If localized, the region affected should be identified. It should be noted that the animal may kick the examiner during the xiphoid ballottement test; thus proper precautions should be taken.
The subcutaneous abdominal veins are assessed next and palpated along their length for the presence of thickened walls, distention, or pulses. Distention and pulses may be abnormal if they correlate with other clinical evidence of right-sided heart failure. Thickening of the wall or evidence of thrombosis is often a consequence of faulty intravenous injection of irritating substances or of injuries that result in hematomas or abscesses.
If the animal is lame or has postural abnormalities, the feet and legs are palpated next. If the animal is uncooperative, it may be necessary to sedate and/or cast it. If sedation is necessary, it should be performed at the end of the physical examination. Care should be exercised for obvious reasons. The examination consists of comparing one foreleg with the other then comparing both with the expected norm. The same procedure is followed for the hind legs. Abnormalities in the shape of the claw may be hereditary or may be caused by nutritional deficiencies, poor leg conformation, poor housing, or as a sequela to laminitis. The coronary bands should be palpated for evidence of pain or increased heat. An attempt should be made to pick up all four feet individually and observe the soles and interdigital regions for necrotic areas, areas of bruising or swelling, draining tracts, or presence of foreign bodies. The fetlock, carpal and tarsal, stifle, and elbow joints are all easily accessible and should be examined for swelling, tenderness, edema, heat, instability, and crepitation. Each joint should be tested over its full range of motion, and any elicitation of pain should be noted. Physical findings should be consolidated into a decision as to whether the joint problems are infectious or traumatic. Sheep or goats with acute polyarthritis most commonly have mycoplasma or chlamydial infection. Chronic joint pain in goats (often with soft-tissue thickening and enlargement caused by synovitis) is frequently attributable to caprine arthritis encephalomyelitis. Conformation of the legs should be analyzed because this could contribute to a joint or foot problem. The pelvic girdle does not lend itself to extensive examination; however, one can note symmetry or asymmetry and further evaluate during the rectal examination. Fractures of the tuber coxae, subluxation of the sacroiliac junction, acetabular fractures, fractures of the head or neck of the femur, and dislocation of the coxofemoral joint may all be diagnosed by evidence gained during palpation and observation of the pelvic area. The dislocated or fractured limb is frequently shorter than the normal opposite limb. The tail can also be examined for evidence of fractures, paresis, or paralysis.
The perineal region is examined by noting the external condition of the genitals and rectum. Anal sphincter tone can be assessed, and the presence of vaginal discharge can be noted. In males the testicles, spermatic cord, and epididymis should be palpated for the presence of nodules or areas of fibrosis. The testicular circumference can be measured and compared with what is expected for age and breed. These measurements are noted in Tables 1-4 and 1-5. The perineal part of the penis can be palpated for the presence of hematoma or swelling and pain (cellulitis or abscess). In the female the supramammary lymph nodes can be felt at the attachment of the udder to the perineum. Enlargement of these nodes occurs with mastitis or lymphosarcoma. The udder is palpated for the presence of fibrotic areas, commonly seen secondary to staphylococcal mastitis or associated with Arcanobacterium (Actinomyces) pyogenes abscesses. The presence of a swollen quarter or quarters with pain and heat may be associated with mastitis caused by gram-negative bacteria. Cold damp areas of skin on the udder that are discolored, necrotic, and possibly sloughing are evidence of gangrenous mastitis. In lactating animals, milk should be present in each quarter, and some of this milk should be expressed for examination. The milk should be of normal color and consistency and should not have any appreciable smell. The presence of leukocytic flakes or clots (garget) is an indication that the udder is mounting an inflammatory response. This response can be measured qualitatively by using the California Mastitis Test (CMT). One should also collect individual quarter samples from those quarters showing garget or those that test positive on the CMT for bacterial culture and sensitivity.
Table 1-4 Expected Values for the Scrotal Circumference of the Bull at Different Ages4
| Age (Months) | Scrotal Circumference (cm) |
|---|---|
| 12–14 | 30–34 |
| 15–20 | 31–36 |
| 21–30 | 32–38 |
| 31 | 34–39 |
Table 1-5 Expected Values for the Scrotal Circumference of the Ram at Different Body Weights5
| Body Weight (kg) | Scrotal Circumference (cm) |
|---|---|
| <45 | 23–27 |
| 45–70 | 27–33 |
| 70–90 | 30–36 |
| 90–115 | 31–37 |
| 115–135 | 33–38 |
| 135–160 | 36–40 |
The next step is to evaluate the head and neck regions. The head should be symmetric in appearance, and any asymmetry should be evaluated to determine whether the deviation is caused by a neuromuscular or a skeletal defect. Facial nerve paralysis results in one type of asymmetry, whereas a frontal sinusitis with concurrent displacement of the frontal bone appears differently. Discharges from the eyes, ears, nose, or mouth are noted and correlated with other physical findings. The oral cavity is examined by grasping the tongue with the hand and extending it out through the interdental space. Muscular tone of the tongue is evaluated at this time. The normal animal will resist extraction of the tongue and will quickly retract the tongue into the oral cavity when released. Increased ease of extraction and delayed retraction are indicative of diseases resulting in flaccid paralysis or paresis of skeletal muscle, such as seen in botulism, for example. The tongue and oral mucosa are examined for the presence of erosions, ulcerations, foreign bodies, or areas of necrosis. The dental arcade is evaluated for age of animal, absence of teeth, loose teeth, or necrotizing gingivitis. The color of the mucous membranes is noted. Icterus, pallor, hyperemia, cyanosis, excessive reddening, or brown “mud-colored” mucous membranes can all be noted, depending on the underlying disorder. Mucous membrane color is best evaluated in the eyes and/or vulva because of the presence of pigments in the oral mucosa of many ruminants. The smell of the breath is noted and, if fetid, might be an indication of a retropharyngeal abscess caused by trauma, lung abscess, or gangrenous pneumonia. If the breath is foul, deep palpation within the oral cavity for an abscess or necrotic area is indicated.
The mucous membranes of the nares are examined, and erosions and ulcerations are noted. Nasal discharges can be an indication of a pulmonic problem but can also be seen with sinusitis. Bilateral discharge is most commonly associated with pneumonia, and unilateral discharge is more often an indication of a sinus problem. However, percussion of the sinuses is necessary to fully evaluate the presence of a discharge. Normal sinuses percuss with a hollow sound, much like that of a hollow tree, and dullness on percussion might indicate sinusitis, sinus cyst, or other fluid or mass in the sinus.
The eyes are examined next. The sclera and mucous membranes are evaluated in much the same manner as the oral and nasal mucous membranes. The corneas are examined for the presence of opacities, discolorations, ulcerations, and lacerations. The position and size of the corneal opacities or ulcerations can be helpful in determining the cause. Foreign bodies such as plant awns and seeds beneath the third eyelid often cause opacity of the medial aspect of the cornea. Infectious bovine keratoconjunctivitis (pinkeye) is usually localized to the central cornea and causes severe corneal ulceration. When the mucosal diseases cause corneal opacities, they generally do so at the junction of the cornea and sclera and usually do not ulcerate the cornea. The anterior chamber should be examined for the presence of hyphema or hypopyon. These can sometimes be seen in animals with severe bacteremia, especially in neonates with failure of passive transfer. The animal should be evaluated for the presence of a menace reflex (absent in normal neonates for up to 2 weeks), and the pupillary light responses should be observed. Nystagmus and strabismus should be characterized, if present, because the direction is important in localizing the lesion. Nystagmus or strabismus or a deficit noted in the pupillary light reflex or menace reflex is indicative of underlying neurologic or ophthalmologic disease.
The ears should be palpated and evaluated as to their temperature and the presence of skin lesions. They should be warm to the touch. Ears that are cold are an indication that there is decreased blood flow to the periphery, as seen in hypocalcemic states, with decreased cardiac output, or in severe toxic states caused by peripheral vasoconstriction. The presence of small crusty areas or erosions of the skin of the pinna is seen in some of the mucosal diseases such as bluetongue or bovine virus diarrhea. In sheep with acute bluetongue, edema of the face and ears sometimes occurs. If aural discharge or head tilt is present, the ear canal should be examined grossly and with the use of an otoscope for the presence of foreign body or parasites. Purulent discharge can be noted and is an indication of otitis externa. Noting that the eardrum has ruptured along with the purulent discharge is diagnostic of otitis media (and possibly otitis interna). Animals that have suffered trauma to the laryngeal or throat latch region and have a basisphenoid fracture can have bloody discharge from the aural canal. Correlation of the otoscopic findings with other clinical findings is necessary to arrive at a definitive diagnosis.
The palpable lymph nodes of the head and neck include the parotid, the submandibular, and the deep retropharyngeal. The deep retropharyngeals can be palpated externally, if enlarged, in the sheep, goat, and calf. They can be examined in the adult bovine by extending the hand through the mouth and palpating the pharynx. By keeping the animal’s mouth open with one hand and guiding the other hand along the dorsum of the tongue to its base, the examiner can then extend the hand aborally into the pharynx. Enlargements of the deep retropharyngeals, abscesses, or other masses can then be palpated. The most common causes of masses or abscesses in the pharyngeal region are infectious or iatrogenic (e.g., secondary to trauma from a balling gun, paste wormer gun, or other instrument). The submandibular nodes are located in the intermandibular space and are identified by slipping the skin and underlying tissue through the fingers. These nodes are oval and about the size of a walnut, or 1 to 2 inches in diameter (2.5 to 5 cm). The parotid lymph nodes are almond shaped and are located just caudal to the ramus of the mandible and about 4 inches (10 cm) ventral to the ear.
The skin of the neck is palpated, with attention paid to the presence of abscesses, lacerations, or other lesions. Skin turgor can be assessed by tenting the skin and measuring the time it takes for the skin to return to normal shape. This is used to determine the state of hydration. In normal, hydrated animals the skin returns to normal position within 1 second. Using other factors such as sunken eyes, dryness of mucous membranes, abnormal heart rate, and degree of illness, an estimation of percent dehydration is made. Dehydration is first noted clinically when the animal is approximately 5% dehydrated, and death occurs at 12% to 15% dehydration.
The larynx should be palpated for enlargement and the presence of pain. The trachea should also be palpated for the presence of fractured tracheal rings, collapsed areas, and pain on palpation. The jugular veins are examined for the presence of distention and pulses. Thrombosed veins should also be noted because this condition may alter the desired course of therapy and often prevents placement of a catheter. The venous stasis test is performed on the jugular by holding off the vein in the midcervical region. Normally the vessel fills above the point of occlusion and remains collapsed below. With restricted venous blood flow, as seen in cases of right-sided heart failure, a positive stasis test can result. In these cases the vessel below the occluded point fails to collapse or takes a prolonged time to do so, and a jugular pulse is frequently present.
The final step in the physical examination is rectal palpation. This cannot be accomplished in small ruminants, so this section is directed primarily toward the bovine. The pelvic area is evaluated for the presence of retroperitoneal abscesses or fractures of the pelvic bones. The left kidney can be palpated for overall size and shape, which is normally lobulated in cattle, and the kidney can be gently squeezed to determine if pain is evident. The rumen should be palpated and the findings compared with those noted on percussion and auscultation. If there is any evidence of intraabdominal gas pings, an attempt should be made to palpate the suspected organ. This can provide information that may be helpful in determining therapeutic or diagnostic directions. The rectal palpation can reveal the presence of masses that were not palpable externally, such as fat necrosis or tumors. Adhesions and evidence of peritonitis can also be palpated rectally, and attempts should be made to localize them to a specific area of the abdomen to establish potential cause. The preiliac (or internal iliac) lymph nodes are located by sweeping the hand along the craniodorsal face of the ilium. These nodes normally have the size and shape of a walnut. Enlargements are noted with lymphosarcoma, peritonitis, and severe limb inflammation. The lymph nodes of the aortic bifurcation are very small and not easily palpated. Their ability to be palpated would be evidence of abnormal enlargement. Palpation of the genital tract is directed toward establishing size, shape, and presence of abnormalities. These contents could be normal, as with a pregnant animal bearing a fetus, or abnormal, as seen with a pyometra. If it is determined that a cow is not pregnant, the ovaries and oviducts should be palpated for structures and abnormalities. In the bull, particular attention should be paid to the prostate, seminal vesicles, and bulbourethral gland.
Diagnostic imaging using an ultrasound probe in conjunction with rectal palpation can add to the information already gathered during the physical examination to further refine the problem and aid in prognostication and development of the therapeutic plan. Proper manipulation of the probe can allow for imaging the kidney, the uterus, the bladder, and the rumen wall. Abnormal structures noted on palpation of the abdominal cavity can also be imaged. The accessory sex glands in the male can be visualized also.
MEDICAL RECORD
The information gathered by means of the physical examination (see Fig. 1-2) is compiled and correlated with the data obtained during the history (see Fig. 1-1). A problem list should be formulated through the physical examination and anamnesis, leading to the development of a specific diagnostic plan, diagnostic ruleouts, and a proposed course of therapy (Fig. 1-6). Prognosis can also be assessed with the information now in the examiner’s hands. Accurate recording of the abnormalities noted during the examination should become part of the medical record and can prove valuable in following the course of the case. In addition, with each complete and accurate physical examination performed, the practitioner becomes more skilled in the procedure, adapting it to fit his or her needs, and using his or her time more efficiently. With the number of diagnostic tests available to the profession today, the information gained from the physical examination will allow the examiner to pick the tests that are specific for those disorders suspected, which saves the practitioner time and the client money.
DIAGNOSTIC TESTS THAT CAN BE APPLIED IN THE FIELD
There are laboratory procedures that can be performed in the field, the results of which would prove beneficial in the development of a diagnostic plan. These include the CMT, partial urinalysis (dipsticks), ruminal pH determination, and milk or blood progesterone tests. In addition, some serum chemistries can be performed cowside with the use of the i-Stat.*
The CMT is a simple procedure that aids in the detection of clinical or subclinical mastitis (see Chapter 36). This procedure is done routinely during all physical examinations of lactating cows. Partial urinalysis is accomplished by collecting the urine and using any one of a number of urine dipsticks that can be commercially obtained. With a suspected case of lactic acidosis, a rumen sample can be collected through the stomach tube or via percutaneous needle puncture, and rumen pH can be determined. Most drugstores carry pH paper that can be used for this procedure. Be certain that the paper has a standard range, because there are papers that are specific for the acidic or the alkaline range. A rumen pH below 4.5 would be indicative of lactic acidosis. Numerous cowside progesterone assays that use either milk or blood as substrate have recently been developed. These can be relatively easy to use and interpret or they can be difficult, so discretion should be used when making initial purchases. These ancillary diagnostic procedures are explained in greater detail later in this text.
INSURANCE, INTERSTATE, AND PREPURCHASE HEALTH EXAMINATIONS
The complete physical examination as described in the preceding sections is necessary for a proper prepurchase or insurance examination. For insurance purposes a more complete accounting of the examination must be done. This means that all findings, whether normal or abnormal, have to be recorded. A specific form is generally provided by the insuring agent, and this should be used. Potential for future legal action also exists whenever an animal is insured; therefore it is in the practitioner’s best interest to complete the insurance form accurately.
The prepurchase examination is similar to the insurance examination. The physical examination form (see Fig. 1-2) can be used to record findings. The prepurchase examination could be performed on the highly pedigreed female that is being consigned to sale, but it is more often performed on the male scheduled for use as an artificial insemination stud. Occasionally one could be asked to examine an animal under consideration for purchase. Experience indicates that the veterinarian should be employed by the potential buyer in these cases. This arrangement avoids any potential accusations of conflict of interest on the part of the examining veterinarian. A complete blood count and a chemistry panel should be run. Generally it is prudent to certify that the animal is healthy and to test for tuberculosis, brucellosis, and bovine leukosis (using agar gel immunodiffusion). Additional laboratory tests for anaplasmosis and bluetongue may be indicated. Often an animal being consigned to sale or one going into artificial insemination service is required to meet federal regulations for interstate shipment. This information can be obtained from the federal veterinarian in charge in your area or from the office of the state veterinarian in the state of destination.
A problem arises when the number of animals submitted for interstate health examination is large. Economic and temporal constraints usually preclude complete examination of all the animals presented. At such times the visual examination described earlier can prove helpful in determining which animals are to be singled out for the more complete physical examination. The examination of individuals is less complete than for prepurchase or insurance examinations, because such factors as fertility are not at issue when filling out an interstate health certificate. Choosing animals with abnormalities in behavior, physical condition, gait, or posture allows the practitioner to concentrate on those that have the most potential to be diseased. Also, one can be fairly confident that if all the animals appear normal on the general examination, they are healthy and would be suitable for interstate shipment as long as the results of the intradermal tuberculosis test and required serologic tests prove negative. To sign an interstate health certificate, a veterinarian must be accredited and licensed in a state. It is essential that a veterinarian signing an interstate health certificate have examined the livestock sufficiently and diligently enough to be confident that no infectious or contagious diseases are present in the consigned group. A call should be placed to the office of the state veterinarian in the state of destination to be sure that all current requirements are fulfilled before shipment is scheduled.
1 Stöber M. General examination. In: Rosenberger G, editor. Clinical examination of cattle. ed 2. Philadelphia: Saunders; 1979:73.
2 Anonymous. Clinical values and procedures. In: Fraser CM, editor. Merck veterinary manual. ed 6. Rahway, NJ: Merck; 1986:910.
3 East NE. Personal communication. Davis, Calif: University of California, 1982.
4 Chenoweth PJ, Ball L. Breeding soundness evaluation in bulls. In: Morrow DA, editor. Current therapy in theriogenology. Philadelphia: Saunders; 1980:330.
5 Braun WF, Thompson JM, Ross CV. Ram scrotal circumference measurements. Theriogenology. 1980;13:221.