11 Progressive inhibition of neuromusculoskeletal structures (PINS) technique
Progressive inhibition of neuromusculoskeletal structures (PINS) is a manipulative medicine technique that, when properly utilized, can be included in the treatment regimen of patients with neuromusculoskeletal dysfunction. Knowledge of anatomy and neuromuscular physiology, as well as reliance on standard forms of palpatory diagnosis and treatment, are necessary.
As a variant of a technique known as ‘inhibition’, PINS bears some resemblance to other manual medicine techniques. The practitioner must determine any alteration of the related soft tissues due to dysfunction. Then he or she must gauge the direction and amount of treatment based on palpatory evaluation and patient feedback.
Initially, two related sensitive points are located. One is most commonly in the immediate region of the patient’s symptoms, and the other is sometimes at the other end of a structure, such as a muscle, nerve, fascial link or ligament that is anatomically related. The practitioner exerts a mild amount of pressure progressively from one to the other.
Other similar techniques are also discussed. Some theoretical as well as selected practical applications are presented.
Neuromuscular techniques
Manipulative treatments have been used throughout history, although the aetiology of musculoskeletal dysfunction, as well as the processes by which dysfunctions are maintained, have been poorly understood until recently. What is obvious to anyone who practises palpation is that the soft tissues, including the skin, muscles, fascia and ligaments, may be involved. Dysfunction of each of these result in, result from, or both in relation to other structures such as the joints, nerves and viscera. With knowledge of anatomy, separate hypertonic individual muscles, as well as groups of muscles, can usually be discerned in association with somatic dysfunction. While many skeletal muscles are capable of being activated by conscious initiation, many muscular actions operate via reflexive mechanisms.
Clinical experience shows that injured muscles may remain in a state of hyperresponsiveness, as evidenced by their hypertonicity, due to unconscious mechanisms that maintain them in a dysfunctional state. Looking past the usual concepts associated with intent and activity, attention most logically turns towards reflex activity as a maintaining factor. With the capability of being enhanced or inhibited by higher neurological functions, the stimuli that maintain undesirable hypertonicity operate at a spinal cord level. Often, a reflex that seems to be programmed for the purpose of protection is inappropriately maintained afterwards. Muscles innervated by segmental nerves may become activated consciously or reflexively. When the latter occurs, possibly following injury, there can be maintenance of a dysfunctional hypertonic state. The potential for the central nervous system to inhibit or eliminate such activity may have been overridden reflexively.
Understanding these patterns suggests that the process of manipulative treatment should involve more than the ‘prodding’, ‘kneading’ or ‘folding-and-holding’ of dysfunctional tissues. Through a combination of observation, assessment and diagnosis, the manipulative specialist may postulate the causes as well as the most appropriate treatment choices. Appreciation of the connection between the musculoskeletal and the neurological influences involved in somatic dysfunction allows for the therapeutic manual interventions that follow to be designated as neuromuscular techniques.
Many neuromuscular modalities have been developed. Some practitioners and physicians apply these in a narrow regional manner involving localized dysfunction. Others learn to apply the concepts and principles behind any particular technique more widely, involving global appreciation of the interactions between body regions and systems. Jones’ strain/counterstrain system, for example, started as a form of treatment for low back pain in an individual patient (Jones et al 1995). It is almost certain that in treating low back pain, others had practised locating a local tender point and then holding the region until it dissipated. The crucial leap beyond these limitations occurred when Jones postulated the underlying principles involved, and then developed the practical methods that flowed from this hypothesis, to locate tender points throughout the body in a similar way. Similarly, as later discussion in this chapter will elaborate, understanding the basic principles involved in manual methods, such as applied pressure, allows for a variety of different methods of application, all of which are neuromusculoskeletal, by definition.
Background
Osteopathy has been practised since the late 1800s. Many osteopathic treatment modalities have been delineated and refined in the 100 or more years of the profession. Several are adaptations of other methods. There are many other modalities developed before or since in other related fields of manual medicine as well. Sometimes, the similarities are greater than the differences. Appropriate clinical selection of any one depends upon experience, skill, suitability, efficacy, ease of use and expected outcome. As a new technique, PINS is a variation of the technique known as inhibition.
Having suffered from headaches over 30 years ago, the author was frustrated with the treatments that were offered. Having little knowledge of anatomy, early attempts involved the application of pressure on various portions of his scalp. The related symptoms involved pain at and near the right eye, increased lacrimation (tearing), facial pain, nasal stuffiness and scalp pain. There were also suboccipital symptoms, which appeared to be distantly related to the periorbital pain. As the symptoms appeared to progress following a great deal of reading, eye strain was a typical initiating condition. Exposure to bright sunlight without the benefit of sunglasses could also precipitate the cephalgia. Each of the symptoms could occur independently and was worsened by stress.
By trial and error, manual pressure was exerted at several sensitive points. There appeared to be a temporary beneficial effect when any point was pressed singly, but sometimes, within seconds, secondary adjacent regions of the scalp developed pain. When these secondary points were likewise pressured, patterns seemed to appear.
Treatment of these patterns as a succession of points was the most successful approach – more so than addressing any individual point or pair of points. When similar symptoms of headache that developed in others were likewise treated, the results were equivalently successful.
Later, after beginning osteopathic medical education at the New York College of Osteopathic Medicine, the author began to integrate knowledge of osteopathic manipulative medicine theory along with clinical observations. As it was utilized more and more, and taught to others, the rationale as well as further expansion of use of this inhibitory technique beyond just headache was determined. During this exploration, similarities and differences were noted in relationship to other methods of ‘point therapy’.
Inhibition
PINS is most closely related to the osteopathic modality of inhibition. According to the Glossary of Osteopathic Terminology (American Osteopathic Association 1998), inhibition is ‘a term that describes steady pressure to soft tissues to effect relaxation and normalize reflex activity.’ Inhibition, or this use of ‘steady pressure to soft tissues’, is perhaps one of the oldest methods of manual treatment, regardless of the name applied. Typically, inhibition is performed by pressing the fingers or other body parts at a constant mild-to-moderate amount of force on regions of persistent hypertonic muscle. Even though the patient may complain of pain or decreased function, the objective of the treatment is to decrease the tonicity of the muscles. The symptoms that the patient has are directly related to this increased dysfunctional muscular tone (Dowling & Scariati 2005).
Large superficial muscles are most easily identified in both the normal relaxed and hypertonic states. A series of regional muscles can be identified and treated in pairs or individually. The supine or prone positions may facilitate the process as the patient will not need to use some of these muscles for postural support of the trunk and neck. With the patient in the supine position, a muscle, such as the trapezius, can easily be located in the cervical, shoulder and upper thoracic regions. The body of the muscle can be grasped, pressed or pinched. A hypertonic muscle is usually found to be firmer, but not necessarily larger, than its counterpart on the other side. An initial response of the tissue to pressure may be an increase in tonus and perhaps sensitivity. Gradually, with sustained pressure, the structures relax.
Another consideration is the relationship between musculoskeletal structures and the underlying organs. The viscera receive innervation from the spinal cord via nerves that originate from the same segments as the nerves that service the more superficial structures. As the sympathetic chain lies just anterior to the rib heads, dysfunction of the vertebra may result in increased sympathetic activity, or stimulation, to the innervated visceral target organs and the segmental musculoskeletal region (Ehrenfeuchter 1997).
The sympathetic system is often referred to as the ‘flight or fight’ response mechanism. It allows for rapid response to perceived danger or injury. The organism’s reactions are channelled towards self-preservation. The heart rate increases, pupils dilate, blood is shunted to the skeletal muscles and away from the internal organs, and the respiratory rate increases. Gastrointestinal activity, among other visceral concerns, effectively shuts down. This normal reaction to stresses becomes abnormal when it does not abate. Inhibition also has a specialized purpose in the thoracic region. In theory, constant pressure to an area, which is the source of increased sympathetic activity, will result in reduction of the autonomic activity. Raised blood pressure, ischaemic changes, arrhythmias, tachycardias or myocardial infarction secondary to vasospasm of a congested coronary artery may result from the effect of the stimulation on a visceral organ such as the heart. Musculoskeletal response includes spasm, decreased circulation due to vasoconstriction, impaired drainage of waste products, sensitivity changes and trophic alterations. Acute responses to this activity are the same as those to any new injury: redness (rubor), pain (dolor), swelling (tumor), heat (calor) and decreased function (functio laesa) (Robbins et al 1984).
• The skin and subcutaneous tissue may have a ‘doughy’ consistency and the pain sharp and throbbing.
• As the state persists without relief, the alterations reflect the chronicity of the dysfunction. Muscles and the surrounding fascia become more fibrotic (‘ropy’).
• The skin responds to the chronicity of the dysfunction by becoming thinner, paler and cooler.
• Pain responses may be more variable from insensitivity (‘anaesthetic’) to altered sensitivity (‘paraesthesia’) to hypersensitivity.
External pressure, such as is provided by inhibition, may initially result in a transitory increase in spasm or sensitivity. However, subsequent reduction of some or all of these components can be readily appreciated. Research regarding the visceral responses has indicated reduction of the undesirable autonomic responses (Hermann 1965). However, the persistence may be more dependent on the aetiology. If the visceral organ’s structure or function were somehow altered, either primarily or secondarily, then the benefits of surface inhibition might be short lived. The more observable musculoskeletal signs and symptoms might represent a viscerosomatic reflex. When a musculoskeletal injury is the origin, a somatovisceral reflex may occur. Manipulative treatment of the musculoskeletal structures may result in a more persistent reduction of all elements.
In the suboccipital and sacral regions, the intention switches from the sympathetic half of the autonomic system towards resetting parasympathetic activity, the other half of the autonomic nervous system. Rather than being reactive to external danger such as the sympathetic system, the parasympathetics comprise nerves affecting the modifying reconstructive processes. Upgrading of parasympathetic activity coordinates increased gastrointestinal motility, decreased sphincter closure, reduction of heart rate, constriction of pupils, and sleepiness, to name just a few of the reactions.
Parasympathetic fibres travel only to the head and trunk, not to the extremities. Any region that has a visceral organ will have parasympathetic innervation. Although there are other cranial nerves (III, V, VII and IX) with some parasympathetic fibres, the vagus nerve (cranial nerve X) is the major influence to the head, neck, and thoracic and abdominal cavities. The origin of the vagus nerve is in the upper spinal cord and lower brainstem. The pelvic organs and the terminal portions of the gastrointestinal system are influenced by branches of nerves originating from the terminus of the spinal cord and exiting from foramen in the sacrum (S2, S3 and S4). The parasympathetic centres also receive sensory information from the target organs.
Persistent conditions such as nausea, vomiting, diarrhoea, dysmenorrhoea and dyspepsia are parasympathetic in nature. Dysfunction of the upper cervical, occipital and sacral regions may reflect or result in inappropriate parasympathetic activity. Inhibitory treatment results in reduction of the more superficial representation (increased musculoskeletal tone and congestion) and theoretically downregulates the more internal mechanisms. A thorough understanding of the structure and function of all of the factors related to dysfunction should guide accurate treatment.
Andrew Taylor Still first developed the concepts of osteopathy in 1874. An American medical practitioner primarily trained through apprenticeship with his father, a Methodist missionary and itinerant practitioner, Dr. Still practised what could be called conventional medicine until he suffered personal loss as a result of its inadequacy. Despite calling in other practitioners to assist, he watched as members of his family succumbed to meningitis. Realizing that the approaches utilized in the ‘heroic’ era of medicine, which were the primary tools of the allopathic profession at that time, were often more dangerous than the diseases they were meant to combat, and seeking other means, Still began using manipulative treatments. He found these were quite effective in managing or facilitating his patients’ health.
Theorizing that the body was a unit, structure and function were interrelated, and the body had the ability to heal and defend itself, he set about reorganizing medical theory. In 1892, he established the first school of osteopathy in Kirksville, Missouri. As a rural institution, osteopathy spread slowly and experienced much prejudice. In the United States, there are currently 26 medical schools of osteopathy and approximately 66 000 osteopathic practitioners with full medical practice rights. Brought to England at the turn of the century by J. Martin Littlejohn, osteopathy spread to the rest of Europe, and the Empire (now Commonwealth).
The origins of some of Still’s treatments apparently predate his professional separation from his allopathic colleagues. When he was a young man suffering from chronic headaches, Still treated himself with a rope-swing. He lowered the rope to a few inches above the ground and slung a blanket across it. Lying on the ground, he positioned himself with the contraption supporting his neck at the base of the skull, and subsequently fell asleep. He awakened refreshed and pain-free. This method may represent inhibition as well as a positional intervention (Still 1908). Some descriptions of both inhibition and stimulation methods were included in Still’s early writings (Still 1902).
Some of Still’s early students likewise described inhibitory techniques as well as their rationale. Eduard Goetz, one of Still’s earliest students, described and illustrated inhibition for various conditions, both somatic and visceral, in his book A Manual of Osteopathy (Goetz 1905). Selected photographs in this small handbook clearly demonstrate and detail inhibitory treatment of several regions. Two such areas are the orbital and suboccipital regions of the head. In one such approach, pressure is applied individually to each of these areas for a few minutes.
Dain L. Tasker delivers a more extensive description in Principles of Osteopathy (Tasker 1916). Tasker describes a rationale as to the effectiveness of inhibition and that it is a natural phenomenon. Activities such as defecation and urination could not come under conscious and unconscious control without the ability of the individual to perform inhibition. In discussing the ability of externally applied inhibitory pressure, applied by a practitioner of manual medicine, to lessen hyperactivity, Tasker states that it is not the palpation itself but the initiation or alteration of the reflex arc that occurs. Observation reveals that placing a pressure should be a form of stimulation because it is impacting on the soft tissue. The effect of inhibitory pressure is to produce neural resetting of tone, modification of the dysfunction, and a beneficial modulation of distant or deeper reflexively linked structures. In citing Hilton’s law ‘that the skin, muscles and synovial membrane of a joint, or the skin, muscles of the abdomen and contents covered by peritoneum, are innervated from the same segment of the cord’, Tasker states that the ‘over-stimulation’ caused by inhibition brings about a diminution or elimination of the overreactivity.
Osteopathic point and/or pressure techniques
Strain/counterstrain (see also p. 196)
Several passive direct and indirect systems of osteopathic treatment of somatic dysfunction exist. Standard points and diagnoses are used as fulcrums, or monitoring locations, in practically all. Monitoring by constant palpation at the points allows both practitioner and patient to experience feedback as to the success of the treatment when performing Jones’ strain/counterstrain treatment (Glover & Yates 1997, Jones 1981, Jones et al 1995).
The practitioner determines a tender point, such as those that have been identified and mapped by Laurence Jones and his followers. The pressure on the point is designed to create a mild degree of discomfort, which the patient reports on as the tissues are positioned to remove the discomfort. The positioning of the region or the whole patient into a direction of ease is the actual therapeutic intervention. Although the diagnostic points are named for spinal segments, bony landmarks, ligaments or muscles, it appears that the treatment positions bring about shortening, and therefore relaxation of the muscles and ligaments.
In theory, during the period spent in a position of ease, muscle spindle resetting occurs. The muscle spindle apparatus is a sensory organ embedded into the larger muscle. Small, almost primitive, fibres exist in parallel within the larger extrafusal muscle. Two distinct shapes of the muscular fibres, as well as two of the sensory ends of the nerve fibres, exist. The nuclear bag muscle spindle fibre has all the nuclei collected in the centre. Nuclear chain fibres have the nuclei set almost in line. The primary type of sensory fibres to the nuclear bag appear almost like a coiled spring, and are termed annulospiral. The descriptive name ‘flower spray’ is applied to the endings of the fibres that primarily service the nuclear bag fibres. The muscle spindle fibres, unlike the other large extrafusal muscle fibres, do not have a great deal of contractile ability.
The sensory nerves to these intrafusal spindle fibres are stimulated by stretch of any kind. The annulospiral is more responsive to rate of stretch, and the other to constant stretch. This assists in the regulation of muscle tonicity as stretch brings about reflexive muscular contraction. Ordinarily, this is short in duration and recovery is quick. Sometimes, the reflex persists longer than is appropriate. The signals from the spindle continue as if the tissue were being stretched too rapidly, or overstretched, even though the length may be normal.
Increased neural activity is evidenced by increased sensitivity of a ‘tender point’. Applied pressure elicits a report of tenderness. The positioning process during application of strain/counterstrain technique shortens the whole muscle, allowing the spindle reflex mechanism to be reset. The position that relieves the tenderness in the palpated point is typically held for 90 seconds and is then slowly returned to neutral. When successful, the previously hypertonic muscles relax and the sensitivity disappears.
Facilitated positional release
Facilitated positional release (FPR) (Schiowitz 1997) is similar in many respects to strain/counterstrain. It differs in its use of an activating force, usually compression or torsion, after initially positioning the region in neutral (ease). By comparison, strain/counterstrain is a form of positional release, whereas FPR utilizes an additional facilitating force. As with most manipulative techniques, the efficacy is directly proportional to the accuracy of diagnosis. The diagnosis includes relative motion freedom in the sagittal plane (flexion/extension), coronal plane (lateral flexion/abduction/adduction) and horizontal plane (rotation). Any increase in tissue tension in the surrounding tissue is also noted by means of palpation.
Initially, at least with spinal dysfunctions, the region is brought into a neutral position relative to the sagittal (anterior–posterior) plane. The lordosis of the cervical spine and the kyphosis of the thoracic spine are flattened. The practitioner then further brings the somatic dysfunction into the directions of relative ease. A facilitating force, usually compression and/or torsion, follows this. Release of the dysfunction and localized tension is noted almost immediately, as shown by the practitioner’s monitoring finger.
Both strain/counterstrain and FPR theoretically utilize the same neurophysiological mechanism. However, because of an inverse myotactic reflex caused by the facilitating force, a release occurs within seconds instead of in 1.5 minutes. The muscle spindle has a specialized motor nerve known as the gamma motor neuron. Even though the nuclear chain and bag fibres are weakly contractile, increased gamma activity causes the ends to contract and the central regions become stretched. Regardless of whether the whole muscle is stretched or not, the spindle will react as if it were. The reaction results in overall protective contraction. The gamma gain, as it is known, tends to persist longer than is necessary and is modified by many factors including stress, pain, anxiety, endocrine alterations, medications and food substances. FPR, with its initial manoeuvres to flatten curves and adding a facilitating force, addresses the gamma activity component as well as the spindle stretch response. Diagnosis for FPR is less reliant on the localization of a tender point, but when such a point is found it is used solely for the purpose of monitoring.
Still technique
The recently described Still technique (van Buskirk 1996) shares many similar applications with these two previously described techniques. Richard van Buskirk attributes the writings of Charles Hazzard (Hazzard 1905), as well as those of Still himself, as the sources for the method. The descriptions revolve around the palpatory diagnosis of dysfunctions followed by motion into the directions of freedom/ease, and finally by movement past the neutral point into the barrier directions. A low-velocity, relatively low-amplitude articulatory movement towards the barriers follows positional treatment and the utilization of forces into the directions of ease (freedoms).
Functional technique
Functional technique (Johnston 1997) utilizes the diagnostic tender points to define the somatic dysfunction that exists at that level relative to the two adjoining vertebrae, the one above and the one below. Detection is typically made by percussion testing to scan and screen the regions. Once an anomaly is determined, the practitioner tests the dysfunction more specifically. The practitioner guides the region into a compound position of freedom (‘ease’, comfort) along various axes. Fine tuning to achieve release of the dysfunction includes side-bending and lateral translation, flexion/extension together with anterior or posterior translation, as well as rotation combined with compression or distraction. Breathing is then held in either exhalation or inhalation, dependent upon which phase is associated with greatest sense of tissue freedom.
Additional osteopathic methods using palpated points
Monitoring points as sites where some form of pressure is exerted to relieve dysfunction is used in other osteopathic techniques. The intent goes beyond monitoring.
Elaine Wallace developed Torque unwinding (Dowling 2005) and has taught this on a limited basis. She advises that the body can be imagined as a collection of adjacent or overlapping cubes. Injuries place forces into a whole ‘cube’. Even though the vector force may be straight initially, after entry into the complex body it rarely remains so fixed. The pathway, because of bodily composition, motion or twists, becomes arced or more twisted. The tissues, especially the fascia, maintain memory for these injurious forces. The practitioner’s fingers direct rhythmic, balancing, pressures centrally from two opposing cube faces. Placed on the contralateral sides of the head, trunk or extremity, the therapeutic forces negate the residual traumatic ones. A light percussive test on one side that is monitored on the other yields a sense of resonance that confirms the correct selection of the connected points.
Osteopathic literature is filled with many other variations of myofascial or fascial release techniques (Chila 1997, Ward 1997) that utilize point contacts as references, contact points and/or diagnostic reflections. Steven Typaldos (1994) has written about trigger band technique – a method intended to change the pathological cross-linkages of fascial bands. Using an instrument or fingers, the practitioner exerts significant pressure along certain connective pathways. This occurs along involved tissue in a basically linear fashion from an area of relative dysfunction towards the more involved region. Leon Chaitow (Chaitow 1980, 1996) describes the development of neuromuscular technique by two of his relatives, Stanley Lief and Boris Chaitow. Consisting mostly of point localization, reflected dysfunctions are treated by pressure followed by deep stroking and/or rolling of the tissue.
Standardized patterns of Chapman’s point treatment (Owens 1937) reflect a neurological/endocrine/lymphatic internal alteration to the surface. The palpatory finding has been described as a lenticular (bean-shaped) subcutaneous structure. Although they may not be tender or sensitive to pressure, clinical correlation should raise suspicion either to locate Chapman’s points or possibly to search for a latent visceral correlate. Apparently developed independently, some of the specific points are similar to those of acupuncture. Circular pressures are applied rhythmically by the pad of the manipulator’s finger(s) to the nodular findings that are related to visceral conditions.
Non-osteopathic point and/or pressure systems
There are some similarities between typical inhibition technique and some other manual medicine systems of treatment. These include the Cyriax method (Cyriax 1959), trigger point therapy (Chaitow 1990, Travell & Simons 1983), acupressure (Kenyon 1988, Cerney 1974), reflexology, rolfing and shiatsu (Schultz 1976, Weil 1995). Some of the common elements include the practitioner providing the treatment by pressing the patient’s soft tissue with the intent of bringing about a persistent alteration. Another similarity is the reliance upon a system of diagnosis and/or treatment points.
James Cyriax was most noted as a medical orthopaedist who practised joint mobilization and massage. He discussed the use of a ‘pinching’ technique on several locations (Cyriax 1959). The end goal was relaxation and stretching of tissue, as well as a relative hyperaemia. Triggerpoint therapy, developed by Janet Travell, recognizes the relationship between a remote referral point and a damaged myofascial nexus. Manual pressure can be used, but more commonly dry needling, vapocoolant spray, or a combination of anaesthetic and/or steroid agents are injected into the trigger point. By these means the practitioner locates and interrupts the aberrant patterns. Regardless of the method, theoretically restricted soft tissue is released by means of deep pressure applied to the selected points. Another manual version of the triggerpoint concept, Bonnie Prudden myotherapy, consists of primary points, as well as satellite points. Both are treated for short intervals several times a day over several sessions (Burton Goldberg Group 1994, Prudden 1980). After the treatment, stretching is also incorporated.
Like the better-known acupuncture, acupressure utilizes similar surface points that represent reflections of visceral changes. Traditional Oriental concept meridians align the specific point locations. Generally, one or two points are treated at any given time and the technique generally involves the application of pressure as well as circular motions.
Injured in a horse-riding accident as a young girl and treated by an osteopathic practitioner, Ida Rolf developed the eponymous system, Rolfing (Burton Goldberg Group 1994). She proposed utilizing deeply applied pressure on regions of the body as the tool to re-establish symmetry and more normal function. The actual force of deeply applied pressure used in this modality exceeds that which is commonly applied in inhibition. Some initial discomfort to the patient usually results. There is a great deal of emphasis placed on approximating ideal symmetry and alignment. Modifications to this basic theme were made by followers of Rolf, and integrated into other modalities involving movement patterns (Hellerwork, Aston-patterning).
One of the oldest forms of manual therapy, shiatsu, usually involves relatively heavier pressures applied for short intervals. Increases in ‘the circulation of vital energy’ (Schultz 1976) are reflected by a reduction of the tissue tension. The amount of force, especially in the hands of a traditional practitioner, is intense and brief (10 lb for 10 seconds), as opposed to the lower, steady and unrelenting force used in inhibition. Specific conditions dictate the sequencing of points based on energy flows throughout the body. Some points are adjacent, and others are quite distant to the primary location.
Reflexology correlates treatment points with certain visceral organs that are hypothesized as reflecting onto resonant areas located on the hands, feet and ears. In theory, the name has more to do with the functional contribution to the integrity or energy component of the organ than to the actual physical structure.
Progressive inhibition of neuromusculoskeletal structures (PINS) method
There is no doubt that practically all modalities of manual pressure treatment have merit, given the appropriate circumstances. PINS shares some commonality with several of these, including the localization of points and the application of pressure. The PINS system allows for versatility that is based on the practitioner’s ability to utilize anatomical and clinical knowledge to determine treatment. A thorough knowledge of the typical and variant courses of nerves, fascial bands and muscles must be augmented by clinical decision-making skills for efficacy and accuracy. Treatment of contiguous muscles, which is modified by an understanding of ‘watershed’ areas of innervation (the overlapping zones where more than one nerve can be contributing to sensory and motor innervation), leads to the sequencing of PINS treatment.
Anyone can locate a sensitive point in the region of a patient’s chief complaint. The practitioner must also be fully aware of anatomically normal, as well as variable, connections. For example, shoulder pain invites attention to the glenohumeral joint, and when treatment is successful, as evidenced by increasing mobility and decreasing discomfort, investigation can end. However, when localized attention is unsuccessful, more of the same treatment is not the answer. This will prove frustrating to both the patient and the practitioner. Restriction of motion of the shoulder into flexion, abduction and external rotation, as well as reduction of scapulothoracic motion, should instigate further investigation. For example, latissimus dorsi muscle, originating from the mid to lower back and attaching at the bicipital groove of the humerus, would merit assessment. Expanding the focus, in this example, might also incorporate treatment of the upper ribs, pectoralis muscles, lower cervical spine, clavicle, thoracic spine, lumbar spine, pelvis and lower extremity. Fascial planes – and therefore fascial stresses – overlap and influence one another.
In PINS, patients participate in the treatment by describing the amount of pain or other sensitivity. As the treatment proceeds, changes that occur, as well as the comparison of symptom intensity, are evaluated. Frequently, PINS is not the only treatment modality employed. It can be used before or after other methods of treatment, manipulative or otherwise.
Procedure
The development of an appropriate and specific diagnostic and treatment protocol using PINS requires:
1. In examining the patient, any relationship between the presenting symptoms, somatic dysfunctions and soft tissue findings should be determined.
2. The components comprising a somatic dysfunction must be determined. The mnemonic ‘S-T-A-R’ (Dowling 1998) can be used to track the different aspects:
S –
Sensitivity changes are the patient’s subjective experiences in response to the palpation performed by the practitioner at the sites of dysfunction. These sensations include tenderness, numbness, radiation, warmth, irritation, throbbing, etc.
T –
Tissue texture changes are the soft tissue conditions as found by palpation by the practitioner. They can be
chronic (prolonged blanching of the skin, ropy or fibrous texture of the muscles and fascia, coolness, dryness, vascular changes) or
acute (increased redness, swelling and oedema, moist and/or increased temperature). The findings may worsen with palpation, to a slight degree.
A –
Asymmetry is the utilization of the non-dysfunctional side of the patient in comparison with the dysfunctional side. An area of dysfunction should be compared to the analogous structure on the other side of the body. An imaginary line down the middle of the body should reveal an almost mirrored ideal functional symmetry of one side to the other in a non-dysfunctional person.
R –
Restriction of motion is the most important determinant of dysfunction, especially when motion testing demonstrates asymmetry. The restriction can be by quantity (number of degrees of motion) and quality (stiffness, tremors, cogwheel rigidity, extraneous movement, etc.). Although one or more elements may be present, and the patient may or may not complain of a decrease in available motion, abnormal movement is perhaps the most sensitive and specific determinant of somatic dysfunction (see also
p. 196).
3. Complaints of pain can be deceptive and may actually not help in the localization of the patient’s true problem. They are, however, a very good indication that there is a problem. Often, spasmed muscles on one side may be relatively pain free while the contralateral muscles that are being stretched are more ‘attention seeking’. Exclusive attention to the symptoms may distract treatment from the more needy locations. Pain, or any other symptom, suggests that there is a problem, although the site of pain may or may not correlate with the site of dysfunction.
4. A ‘primary sensitive’ point is determined by examination of the tissue in the region of the patient’s complaint. If a significant one is not found, the practitioner utilizes knowledge of anatomical relationships and widens the search to contiguous areas.
5. Using knowledge of anatomical structures, another point, designated as the ‘end point’, is located distal or proximal to the primary point. Knowledge and understanding of muscle and ligamentous origins and insertions is a good beginning concept in determining this pair of points. If the primary point is at the origin, the end point may be at the insertion. The reverse can also be true.
Sometimes the primary point is located in the belly of the muscle. In that case, exploration of both ends of the attachments to bone may reveal the location of an end point. Ligaments, which are generally shorter and more fibrous, have points that are probably also fairly close to one another. Fascia encompasses all structures, and the path between one point and another may seem to traverse other structures. Generally, the more specialized the fascia, the more palpable and tendinous it is.
Tracing superficial and deep pathways of nerves is useful when determining paths that do not correlate with the other structures. Primary and end points may be found where a nerve passes out of a foramen, between or through muscles, or over and around bony protrusions. Sometimes, if more than one nerve innervates a region, the primary point can be found at the beginning of one nerve and the end point at the beginning of the other. In the case of nerve distribution of an extremity, one point will be found closer to the body while the other will be closer to the end of the extremity.
There is no substitution for an excellent working knowledge of functional anatomy. Regardless of the aetiology, the chosen primary point will most probably be near to the patient’s symptoms. The end point may also elicit symptoms, but to a lesser extent. As the two ends of the same problem, both (and all intervening) points must be addressed. In any case, the practitioner makes the determination of the two ends of the pattern. Sometimes the clue for the practitioner is that the patient relates what appears to them as unrelated complaints. Assuming patient knowledge of anatomy is small, it is left to the practitioner to draw the conclusions necessary to begin treatment. For the purpose of proceeding in a logical fashion, the point that is more sensitive is designated as the initial ‘primary’. The other point, which is found distant from it but on a related structure that links the points, is considered as the ‘end point’.
A few examples of primary and end points are shown in Table 11.1.
6. Conceptually, a muscular, fascial and/or neurological pathway is drawn between the primary sensitive point and the end point. The line may be curved rather than straight. The direction of treatment may be from distal to proximal, or vice versa.
7. The physical connection between the two points may involve:
(i)
Direct connections (The connection of a point near the medial epicondyle at the elbow to a point along the medial arm near the wrist – ulnar nerve.)
(ii)
Overlap or ‘watershed regions’ of innervation – The ophthalmic division of the trigeminal nerve travels from the supraorbital notch over the frontal region and to the top of the head. The greater occipital nerve exits the suboccipal region in the occipital sulcus and travels over the occiput to the top of the head. Rather than have a region of nerve-free scalp, there is an area at the top of the head that is innervated by both the trigeminal and greater occipital nerves.
(b)
Muscle origins and insertions
(i)
Typical – A sensitive point may be found at the medial aspect of the clavicle and another at the mastoid process representing involvement of the sternocleidomastoid muscle.
(ii)
Overlap – The location of a sensitive point medial to the scapula and another in the upper cervical spine might represent splenii, levator scapula and/or trapezius muscles.
(iii)
Contiguity – The tensor fascia lata and iliotibial band actually form a continuity for two possible tender points located, respectively, at the greater trochanter and the fibular head. If a terminal point were actually found near the lateral malleolus instead of the fibular head, there might be a tensor fascia lata, iliotibial band, peroneal muscle connection.
(i)
The interosseous ligaments are actually specialized fascia connecting the radius and ulna in the arm, in the same way that the fibula and tibia are connected. These ligaments should be suspected when the pattern appears to overlie their locations. When analysing the line of connection between the two points, there may be no obvious neural, muscular or other ligamentous analogues. For the lower extremity, the symptoms may be of ‘shin splints’ where forearm symptoms may appear radicular without involving the hand.
(ii)
Septa – Although it contains muscular components to a greater extent, the central tendon and crus of the thoracoabdominal diaphragm are fascial in nature. The diaphragm supports the thoracic viscera, and separates the thoracic and abdominal cavities. Points found around the lower costal cartilage, the 12th rib and T10–T12 may represent a diaphragmatic involvement.
(iii)
Overlaps – The common fascia in the lumbar region acts as an attachment for muscles such as the latissimus dorsi and overlaps muscles such as the quadratus lumborum, iliocostalis and other erector spinae muscles. Points may be found anywhere within the region and may extend to the lateral edge of the 12th rib (quadratus lumborum) or even to the bicipital groove of the humerus (latissimus dorsi).
(d)
Ligamentous attachments
(i)
Typical – Points can be found at the attachments of either end of the collateral ligaments in the elbow and knee.
(ii)
Relationships to muscles – Surface of the points found on the superior C7 spinous process and the base of the occiput may represent spinalis muscles or the nuchal ligament.
(iii)
Relationships to nerves – The flexor retinaculum and palmar aponeurosis are key components to treat when the median nerve in the forearm is involved. There may actually be a need to treat the articular relationships of the four carpal attachments (pisiform, hamate, scaphoid and trapezium) of the retinaculum as well.
(e)
Bones – Although the bones are the deepest of the musculoskeletal structures, they and their components should be considered as connective tissue as well.
(i)
Construction of joints – The joint capsules represent encompassing connections of two or more bones. At joints such as the elbow and the knee, the capsules are stronger and reinforced on their medial and lateral surfaces by collateral ligaments. The anterior and posterior surfaces tend to be more flaccid in one direction of motion or the other. Points may occur in the middle of the capsule and at the bony attachments.
(ii)
Lever action – The mechanical activity of the bones is more of a concern for the analysis of the aetiology of strains and somatic dysfunctions. The bony prominences are relatively strong extensions of the bones. Muscle tendons and ligaments attach to bone and, as a result of frequent usage, lead to the development of enlargements including tubercles, trochanters and other processes. Points theoretically located at tendinous insertions may also represent a contribution from the periosteal anchors.
8. Both the primary point and the end point are pressed simultaneously using the pad region of a finger on each hand (for the sake of simplicity the practitioner can identify the primary point as the ‘first point’ for the patient). The pressure exerted is a few ounces, enough to elicit the patient’s symptoms, and should be of equal degree on both points. The patient may experience a mild to moderate increase in sensitivity. The practitioner should also determine the soft tissue response to pressure by sensing changes in the tissues:
(a)
Dysfunctions that are acute may be more sensitive than chronic ones. A muscle that has been hypertonic will usually be more sensitive to pressure than the same muscle on the contralateral side.
(b)
Muscles that are used excessively will hypertrophy and be bulkier than their contralateral pairs.
Table 11.1 Examples of primary and end points
| Primary point |
End point |
Connection |
| Supraorbital notch |
Suboccipital region |
Frontalis–occipitalis muscles
Trigeminal–greater occipital nerves |
| Medial elbow epicondyle |
Scaphoid wrist region
Pisiform at wrist |
Flexor carpi radialis muscle
Ulnar nerve |
| Greater trochanter of femur |
Fibular head |
Iliotibial band |
| Sternum at 2nd rib |
Upper humerus |
Pectoralis major |
| Temporomandibular joint |
Side of head |
Temporalis muscle |
| Gluteal region |
Greater trochanter
Popliteal region |
Piriformis muscle
Sciatic nerve |
| Xiphoid process |
Public ramus |
Rectus abdominis |
| Maxillary |
Angle of mouth |
Trigeminal nerve |
| Temporomandibular joint |
Maxillary region |
Facial nerve |
Larger muscles do not necessarily indicate dysfunction. When muscles have been subjected to increased usage or there is preference to one side being used more, such as in sports activities that preferentially utilize muscles in an asymmetrical manner (e.g. bowling, archery), the dominant side will typically be larger, but not necessarily dysfunctional.
Whether dysfunctional or not, hypertonic muscles that have been so for some time may not be quite so sensitive to pressure. This may be due to the chronicity of usage. A more sensitive, but less hypertonic, muscle indicates a problem. This does not necessarily indicate the laterality of the problem. Both sides can be dysfunctional. One may be more symptomatic than the other, but to varying degrees. Given a choice of examined findings versus symptoms, the findings take precedence. The practitioner should initially treat the more dysfunctional tissue, re-examine, and treat the less involved side as well.
(c)
Whenever possible, the patient should be in a comfortable position, which generally means one where the muscle is not actively being utilized. Because postural muscles do not fully relax while the patient is seated or standing, a supine or prone position is preferred.
(d)
The pressure exerted on both the primary point and the end point should be equal:
(i)
Patients may assume that the more sensitive location is receiving more pressure. They should be reassured that the reason for the asymmetrical degree of sensitivity is because of the dysfunctional state of the involved tissue.
(ii)
Occasionally, patients will direct the practitioner to apply greater pressure. Increased pressure does not accelerate the treatment. It is not necessary to increase the pressure, and doing so may be counterproductive.
(iii)
Pain or tenderness may not be the only sensations experienced as a result of the applied pressure. The chronic nature of some dysfunctions may result in the patient reporting other sensations such as paraesthesia, which may occur alone or in combination with pain.
(e)
Maintain constant pressure on the end point throughout the treatment (this can be identified as the ‘end point’ or ‘final point’ for the patient).
9. Initiate pressure on the point that produces the greatest sensitivity (primary point). A series of points will be located for application of inhibitory pressure between this ‘primary’ (i.e. the more sensitive) point and the end point during the course of the treatment.
10. Request that the patient report the initial amount and type of sensitivity. Feedback should be given if the sensation at any sensitive point decreases or increases. When inhibition is utilized properly, the sensitivity will usually have a transient initial increase followed by a typical subsequent decrease in sensitivity as the tissue accommodates to the irritation of the inhibition. Ultimately sensitivity may disappear totally. The duration can vary from several seconds to minutes.
11. The practitioner maintains simultaneous contact with the two points for 20–30 seconds and then seeks another point:
(a)
A finger of the same hand that has a finger applying pressure to the primary point is used to locate a ‘secondary point’. If the index finger is on the primary point, then the middle finger can be used to palpate for the secondary point.
(b)
Usually the secondary point will be approximately 2–3 cm (approximately 1 inch) away from the primary point in the direction of the end point. (The practitioner can identify the secondary point as the ‘second point’ for the patient.) This will typically follow the predicted course of an anatomical structure (innervating nerve, along the direction of the muscle fibres, or following fascial planes).
12. Equal pressure is exerted onto both the primary and secondary points while maintaining pressure on the end point.
13. The patient is requested to determine which of the two points (primary versus secondary or ‘first versus second’) is more sensitive. The practitioner can state: ‘I am pressing on two points that are close together. Please tell me which of the two, the “first” (practitioner may move the finger slightly) or the “second” is more sensitive.’
(a)
If the second point is more or equally sensitive than the first:
(i)
pressure is relieved and removed from the first point (primary);
(ii)
and then constant pressure is maintained on the second (secondary) sensitive point for 20–30 seconds. It becomes the new ‘first’ point.
(iii)
The sensitivity at any point does not have to abate completely before moving on to the next point. It is only important that the next point is more sensitive.
(iv)
The initial pressure on a new ‘secondary’ point will usually cause a response of both increased tension and sensitivity. This typically returns to a baseline after a few seconds, as noted above; the amount of time depends on the soft tissue response.
(b)
There are a few considerations if the primary point persists as the more sensitive of the two contiguous points:
(i)
Maintain pressure at the location of the primary point.
(ii)
The practitioner moves the finger pressing on the secondary point more laterally or medially in an arc 2–3 centimetres from the primary point and into the direction of the end point. A point may be found that has more or the same sensitivity as the primary point by searching slightly out of line with the targeted end point. (The anatomical structure, which is being inhibited, may have slight variations in the specific course in this individual.)
(iii)
Once a secondary point that is equally or more sensitive (compared with the primary point) is located, pressure is released from the primary point and maintained on the new secondary point, as described above.
(iv)
The secondary point then becomes the new ‘first’ point in the continuing sequence of treatment towards the end point.
14. Before searching or inhibiting any subsequent points, the practitioner should wait approximately 20–30 seconds.
15. If no secondary point can be located despite searching in a 2-cm radius from the primary point, the clinician maintains pressure on the primary point (or the new ‘primary’ point) for an additional 30 seconds. Sometimes certain points require further inhibition before progress can be made. After doing so, a new secondary point may be located where previously there was less sensitivity.
16. The end point will have received inhibitory pressure throughout. Often the patient will forget that this point is being inhibited and it may lose all sensitivity.
17. The process is continued successively until the ultimate ‘second’ point is 2 cm from the end point.
18. Once there are the two final points being inhibited, the practitioner determines the amount of dysfunction that persists at the end and secondary point locations. The dysfunction may have reduced or disappeared totally.
19. If the dysfunction, including the end point, remains persistent, the practitioner can choose to treat the dysfunction with whatever additional modality is deemed necessary and appropriate. The end point and dysfunction, having been recalcitrant to treatment previously, may now be more amenable. Strain/counterstrain, facilitated positional release, Still technique, muscle energy technique, balanced tension techniques or some other modality may be used. Single-segment somatic dysfunctions that were difficult to position or resistant to thrust technique may now be more responsive to articulatory techniques such as high-velocity, low-amplitude thrust.
20. PINS technique can be the sole approach to the somatic dysfunctions that were found, or may be used in conjunction with any other modality of manual treatment. Determining this is:
(a)
The persistence of the dysfunction or related components after treatment.
(b)
The ability of the practitioner to perform other modalities of treatment.
(c)
The need or capability of the patient to accept additional treatment.
(i)
After any treatment, some soreness or other symptom may persist despite sufficient treatment. The practitioner should determine extent of treatment based on the findings for the individual; it should not be based on the patient’s subjective complaints. Overtreatment can cause as many problems as undertreatment.
(ii)
Based on previous experience or misconceptions, patients may limit types of treatment. This may be due to fears or reactions that they have had to previous types of treatment.
Application
The following two case studies are illustrative of the use of PINS to common myofascial conditions.
Case study 1
The patient was a 25-year-old married female osteopathic medical student who presented with a chief complaint of ‘migraine headache’. She had been followed for her musculoskeletal complaints by another osteopathic practitioner who was unavailable on the day of presentation to the clinic. The headache was sharp and focused near the right orbit with radiation to the right frontal and temporal region. The patient had some nausea, blurring of vision, increased lacrimation and neck stiffness. The pain had started a few days beforehand and was unrelieved by the use of non-steroidal anti-inflammatory drugs, sleep or frequent doses of sumatriptan succinate, which she took orally. The patient stated that she takes between 21 and 30 pills of this drug per month (recommended usage is 2–3 per month). Loud sounds, light and certain food smells appear to worsen the chief complaint. There were no other visual, auditory or olfactory complaints or other associated symptoms with the presence of headache. The current episode appeared to be unrelated to the patient’s menses, since her last menstrual period had been 2 weeks previously.
Past medical history relevant to the chief complaint was significant for paraesthesias to the upper extremities secondary to a motor vehicle accident 2 months earlier. She was the driver of a vehicle that was stopped at a traffic light, when it was struck from behind. She saw the other vehicle in the rear-view mirror and had braced herself for impact. She had had a fall at age 12 years, in which she struck the top of her head, and had migraines since that time. Family history was significant in that other members of the family have had migraines, a brother has allergies, and her mother has ‘colon problems’. The patient drank two glasses of wine once per week, during religious observations, and denied use of recreational drugs or tobacco. She had a tonsillectomy, rhinoplasty and sinus cauterization. Other medical history was non-contributory.
Other medications included fexofenadine hydrochloride, oral contraceptives, Excedrin® PM (paracetamol (acetaminophen), aspirin and caffeine) and ibuprofen, as well as the sumatriptan. The last three drugs were taken episodically for headaches. At times in the past, she had gone to the emergency room for treatment of unrelieved migraine headaches.
Cranial nerve, sensorimotor and reflex testing as well as other neurological and orthopaedic evaluation findings for the patient were essentially normal. Although she had several tender points, there was not a pattern that would suggest fibromyalgia as a component of the patient’s condition.
Examination of the head, neck, chest and abdomen were essentially normal, with the exception of photophobia. Vital signs were stable and the patient was alert and oriented for all modalities. Examination resulted in findings of somatic dysfunctions, as described below.
Cranial. Cranial examination revealed restrictive patterns on the right side with relative freedom of left cranial motion.
Cervical. Several single somatic dysfunctions were found in the cervical spine including ones at OA (C0–C1), AA (C1–C2), C2, C3, C6 and C7. There was also hypertonicity of the right trapezius and right sternocleidomastoid muscles.
Thoracic and rib. Hypertonicity of the right levator scapula and of the left scalene muscles; right first rib elevation; myofascial restriction of the hyoid and anterior strap muscles; multiple thoracic type II somatic dysfunctions.
Lumbar. A somatic dysfunction was found at L5 on the right accompanied by thoracolumbar paravertebral muscle spasms.
Sacrum and pelvis. Restrictions of the right sacroiliac joint and the related myofascial structures were noted.
The primary diagnosis for the office visit in question included cephalgia (migraine). Other diagnoses included cervical, thoracic, head, lumbar, sacral and pelvic somatic dysfunctions and strain. Although they were present, the areas other than those related to the patient’s head were more chronic in nature and not as crucial to the patient’s chief complaint. The patient was clearly anxious regarding her condition.
Much of the treatment that was performed on this single visit was similar to that which had been performed previously for the patient. Many modalities of treatment were utilized to address all related and apparently unrelated strains and dysfunctions. All of these interventions were successful, to some extent, in relieving most of the somatic dysfunctions and complaints, with the exception of the chief one – the cephalgia. The complaints of the ‘migraine headache’ persisted unabated.
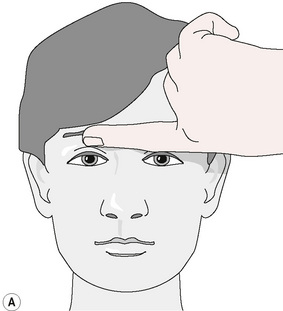
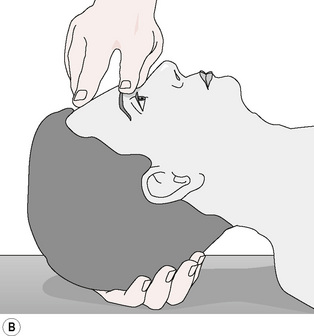
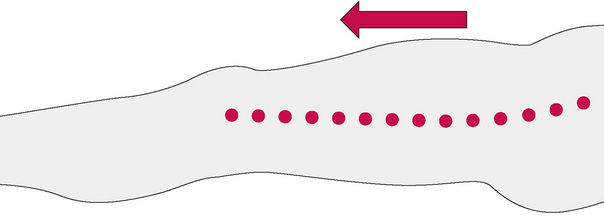
PINS, as a modality, was added to the other customary treatment. Sensitive points at the right supraorbital ridge at the trochlear notch and in the suboccipital region were identified. Placing his left hand beneath the patient’s head and neck, the author inhibited the suboccipital point with his left index finger (‘end point’). Simultaneously, the author’s right index finger (Fig. 11.1A,B,C) exerted pressure on the right orbital sensitive point (‘primary point’).
Figure 11.1 Pressure is exerted on the end point at the right suboccipital region and the right supraorbital ridge by using a finger of each hand.
Redrawn from Dowling (2000), with permission from The American Osteopathic Association.
The patient indicated that the orbital point was the more sensitive of the two. The pressure also seemed to increase her ophthalmic symptoms (nausea, blurring of vision, increased lacrimation). Pressure was maintained for approximately 30 seconds on the anterior, primary point. After this interval, a second point superior to this was simultaneously pressed, with the same amount of pressure as the first, utilizing the author’s right middle finger (Fig. 11.2A,B). The patient was asked to identify which of the two anterior points was more sensitive. She stated that the second was more so. Pressure was then maintained on this second point and released on the first.
This was then maintained for 30 seconds before a third point was identified approximately 2 cm above the second point. This now was reported as more sensitive than the second point. Pressure was then relieved from the second point and maintained on the third. The same pattern was followed progressively along a parasagittal line over the frontal, parietal and occipital bones until a final point was identified. This was 1 cm above the end-point location that was being constantly inhibited in the suboccipital region throughout the whole process. The somatic dysfunctions were treated with a combination of other modalities such as cervical strain/counterstrain, facilitated positional release, low-velocity and then high-velocity, low-amplitude techniques to the suboccipital region. These techniques had previously, during this session, either been unsuccessful or could not be performed, because of the patient’s symptoms. All the patient’s symptoms resolved completely.
Note: Placement and movement of the fingers often requires that the practitioner move the whole hand when selecting subsequent points. This ‘finger walking’ may mean that the second, third and fourth fingers are primarily used in sequence. Sometimes, the first finger (thumb) can be utilized temporarily to locate a new secondary point. Once it has been selected, one of the other fingers can be substituted.
Because she understood the process and her own particular patterns, the patient also tried the technique on herself, with positive results. When used early in the onset of subsequent headaches, it could be quite effective in aborting a migraine headache. When the results were less than optimal, she reported that she could then take a single sumatriptan pill and the symptoms would usually improve to a greater extent. Instead of the 21–30 pills per month, her use of this medication reduced to a more acceptable 2–3 monthly. This remained constant for several months and ultimately she was able to not require the prescription medications.
Cephalgia or headache is complex and complicated by overlapping symptoms and findings. The same symptoms can represent multiple aetiologies. A consideration is that all headaches have elements of muscle contraction, regardless of the cause. When initiated during the prodromal phase or during relatively symptom-free intervals, manipulative treatment of migraine headaches appears to be most successful. Migraine headaches, in particular, are vascular with arterial constriction, dilatation and inflammatory phases nearly paralleling the aural, pain and refractory phases. When considering irritation and inflammation of the cranial dura, one must keep in mind that the first branch of the trigeminal nerve innervates the frontal region. The posterior fossa receives a good portion of innervation from the upper cervical region. Generally, treatment during the full-blown sickening headache component of migraine may be more effective in reduction rather than complete elimination of the symptoms.
Other types of headaches, such as muscle tension/contraction and cervicogenic headaches, can mimic some of the more typical migraine symptoms. Because all headaches have muscle contraction as a component, there is no reason why migraine and muscle contraction headaches cannot occur in the same person. Patients with chronic headaches of any sort may seek many means of intervention.
It is well documented that pharmacological interventions, such as non-steroidal anti-inflammatory drugs and vasoconstrictive medications, are frequently the initial and/or most frequently attempted interventions. Caffeine is an ingredient in many other self-treatments, including beverages, foods and pills. Because of their vasoconstrictive effects, they are successful in limiting or eliminating headaches. However, paradoxically, they have also been implicated in recurrences. It is possible to experience a rebound effect once the medication level goes below a critical point. Rather than eliminate headaches as intended, frequent use of anti-inflammatory and/or vasoconstrictive substances may encourage recurrences.
Cephalgia of this type can be approached from a neuromusculoskeletal model by inhibiting discovered sensitive points by using the PINS technique. The location of the initial point, in this particular case, was at the exit of the ophthalmic division of the trigeminal nerve, above the orbit. The same nerve innervates both the dural lining of the brain and the pain-sensitive structures of the forehead. The dura, one of the layers of the meninges, is also a pain-sensitive structure. The attachment of the superior oblique muscle at the trochlear notch of the orbit, as well as sympathetic influences from the upper cervical spine postganglionic fibres, must also be considered.
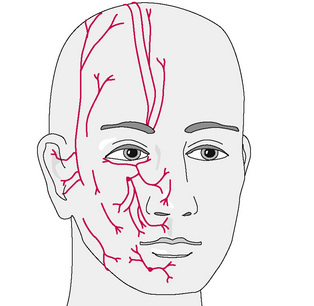
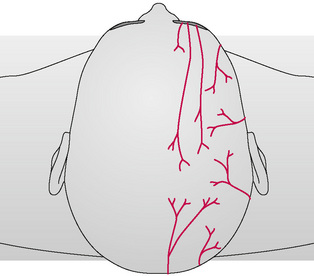
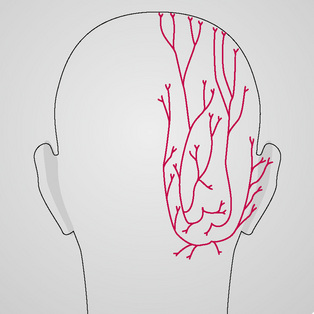
There are several branchings of the ophthalmic division of the trigeminal nerve (Fig. 11.3), and all project more superiorly along the frontal region. Basically, they track upwards unilaterally into the parietal region and are responsible for sensory appreciation from this region. Near their terminations on the top of the head there is a ‘watershed’ region at the galea aponeurotica (Fig. 11.4). The greater occipital nerve (Fig. 11.5) begins to also innervate the skin and musculature in this region (Moore 1980). This nerve is derived from C2 and C3 nerve roots and perforates the fascia and suboccipital muscles. These nerve roots control the majority of sensory and motor innervation to most of the occipital region. Fibres also travel anteriorly upwards through the foremen magnum to the dura of the posterior fossa. Without inhibition and other treatment of the subocciptal region, resolution of the headache may not occur. With limited treatment, some of the symptoms may abate but the presence of multiple untreated regions may result in fairly rapid recurrence.
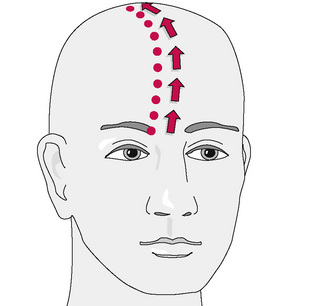
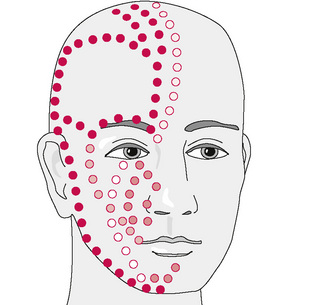
The typical direction of treatment of frontal headache utilizing PINS (Fig. 11.6) proceeds in a pattern that progresses from orbit to occiput along a typical parasagittal line. The direction may vary in some cases and include other divisions or subdivisions of the trigeminal nerve (Fig. 11.7). The approach may be more anterograde, beginning in the suboccipital region and proceeding to the frontal–orbital region depending on the findings. This depends on the clinical complaints of the patient as well as the experience of the practitioner. Generally, the more sensitive of the points is selected as the beginning location. Sometimes, pressure placed onto the suboccipital region reproduces the symptoms and pain in the region of the eye. Although it is infrequently a terminal point, it is also not unusual to find that one of the intermediate points near the vertex of the head also refers pain towards the initial primary point, either to the eye or to the base of the head. Finding this symptom-referring point should be taken as a positive sign in that the procedure is locating and treating the component factors of the dysfunction. In any case, sometimes a ‘search and test’ approach determines the location of several involved points. Two or more found points may give an indication of the involved structures by tracing a line and identifying the structures that link them.
Case study 2
The patient was a 72-year-old man with chief complaints of pain in the left lower extremity, specifically in the hip area. He also had a history of Parkinson’s disease and osteoarthritis. He described the primary symptom as sharp, almost constant, and with radiation of the pain from the left hip towards the knee and ankle. His Parkinson’s disease had progressed slowly and was expressed primarily by stiffness. When added to his arthritis, some activities had become difficult to perform. His posture and gait were stooped, with head forward and moderate bradykinesia. The recent onset of the hip pain added a limp to his already shuffling gait. Shortly after the examination, radiography revealed apparently symmetrical moderate degenerative joint disease of both hips. The patient denied any changes in bowel or bladder habits.
Range of motion examination revealed equal restriction of motion of both hips. Fabere (Patrick test) and Fadir (Flexion, Adduction and Internal Rotation) ranges of motion, as well as pure flexion, were equally limited and equivalent for both hips. Sacroiliac motion was likewise limited with asymmetry. The left side demonstrated slightly less motion than the right. A left unilateral sacral shear was noted. Equal mobility, or relative lack thereof, of ilia motion was demonstrated. The legs appeared to be of equal length. Moderate somatic dysfunctions were noted throughout the lumbar, thoracic and cervical regions as well. Neurological examination revealed that sensorimotor and deep tendon reflex testing of the lower extremities were equal and normal. Strain/counterstrain tender points were noted in the left gluteal, piriformis, midpole sacral and iliotibial band. Left posterior fibular head somatic dysfunction was also noted.
Manipulative treatment based on these findings was performed on one occasion using techniques such as strain/counterstrain, muscle energy, balanced ligamentous tension, and other means of fascial release. Attempted mobilization utilizing high-velocity, low-amplitude (HVLA) thrust of the posterior fibular head was unsuccessful. Ultrasound modality was utilized along the iliotibial band, both during that office visit and during the twice-a-week physiotherapy sessions, along with other physical medicine modalities. Despite all this, the patient’s chief complaint symptoms persisted.
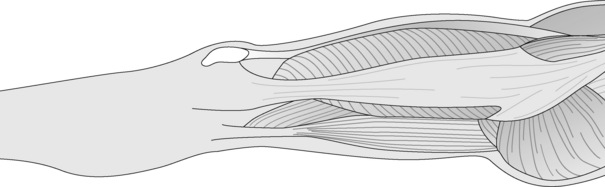
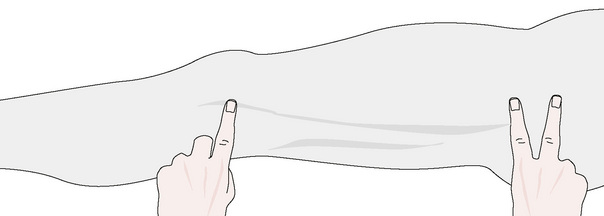
One week later, the same clinical and palpatory findings were noted. PINS technique was then utilized. A sensitive primary point was located at the greater trochanter. The end point was found overlying the fibula head. Location of this point took some trial and error. End points could have been located at the ankle, medial knee, popliteal space, buttock, or even more centrally above the iliac crest. In this case, successive points were also found along the tensor fascia lata/iliotibial band (Figs 11.8-11.10). Following a process of sequential inhibition of these points utilizing PINS, the final ‘primary’ point that was located close to the end point was approximately 2 cm proximal to the end point. Pressure was maintained for half a minute simultaneously on the two points. Inhibition alone resulted in a reported reduction of at least 50% of the lower extremity pain and radiation. The fibula head was then mobilized successfully with HVLA mobilization. The patient stated he had only a small amount of residual discomfort after this was performed. Previous attempts at performing HVLA thrust to the fibula head had been unsuccessful.
At the next visit, the patient reported that the improvement had persisted for at least 1 week. Some of the findings were again present, but to a much lesser degree, and were limited to a single tender point near the left greater trochanter. This was easily treated with only strain/counterstrain technique. PINS was not necessary to the treatment protocol on this visit.
Possible mechanism of action
The mechanism of action by which the technique of inhibition works can only be postulated. Unfortunately, this is the status with many other modalities of osteopathic manipulative technique: insufficient research has been performed for many manipulative modalities. However, the clinical outcomes have been reported anecdotally many times. Understanding the processes of injury as well as treatment is typically based on the most likely combination of relevant physiological and anatomical components.
One of the important components of inhibition is the use of a low-level (but using a constant amount of force) pressure applied to a dysfunctional tissue.
Accommodation or habituation is a process wherein a stimulus of a constant level, even if initially irritating, becomes less noticeable over time. At first, the subject may be acutely aware of the intrusion or pressure. The patient may state that there is pain, sensitivity, increased pressure or some other sensation. The practitioner may also note that the local tissue reacts by initially increasing in tension. Firm, spasmed muscle may become more so. When the pressure is maintained constantly, these reactions decrease and may disappear altogether as the system adapts (Bailey 1976). The reticular formation as a screen is but one component involved in the process. There are many other occasions where the body accommodates to stimuli. These are evidenced by the relative non-awareness of body contact with eyeglasses, tight belts, stiff clothing, uncomfortable shoes, as well as constant extraneous auditory and visual stimuli. It is only when attention is called to them by a new, probably irritating, event that awareness resurfaces. A refrigerator in the kitchen or the sounds from a nearby railway often fail to attract the attention of someone accustomed to them – unless the sounds deviate from the usual. Persons who have worn eyeglasses since infancy may be oblivious to their presence and may even casually adjust the positioning with almost unconscious effort. However, someone who has recently developed the need for visual aids, such as a middle-aged presbyopic adult, may be all too aware of every aspect from the points of contact to the change in appearance of objects. Gradually, this diminishes. This filtering process may also involve lower components, such as the spinal cord, to act as a mediator. Its contribution in this habituation process is to act as a ‘brake’ when sensory overload occurs (Patterson 1976).
Direct pressure placed upon areas of greatest sensitivity or symptoms may act as a counter-irritant. Rapid, conducting, large nerve afferents gate transmission in the dorsal horn of the spinal cord. Collateral fibres in the substantia gelatinosa or adjacent interneurons then inhibit the transmission of pain to the central nervous system via the spinothalamic tract (Ganong 1995). Pressure acts as a stimulant to the neighbouring tissue, reducing the sensitivity of the original tender point. Scratching in the region of an itch would be an example of this phenomenon. An ischaemia theory concerning the use of a sustained pressure, such as that used in inhibition, describes an effect in the immediate tissue. When a muscle is maintained in prolonged contraction, metabolites are released that were produced from the local tissue damage (Stoddard 1969). Damaged tissue ordinarily demonstrates a decrease in circulation in a progressive fashion. Immediate or acute injury results in hyperaemia and congestion. This is followed by infiltration of vasoactive substances. These appear primarily for the theoretical purpose of dealing with tissue injury. If the injury persists or there is a prolonged reduced function, trophic tissue changes occur. The muscles, ligaments and fascia may develop fibrotic changes. The chronic nature of the dysfunction demonstrates decreased circulation by blanching following any pressure. Normally, the skin shows a brief blanching followed by redness, which also fades. When muscle is maintained in a chronically tightened state, circulation is impaired. The use of further pressure in a therapeutic fashion to cause a relatively increased ischaemia does not initially make sense from the standpoint of nutrient deprivation. One way of appreciating an effect is to postulate that, following pressure, the increased ischaemia reduces the capacity of the nociceptive receptors to process. Once this pressure is removed, the resultant hyperaemia produced after release results in flushing of the waste products from the region. The local vessels are dammed temporarily, there is a build-up of pressure, and then sudden washing away as the compression is released.
Although there may be no visible abnormality, a dysfunctional muscle may appear to be in its neutral position but still be hypertonic. Any further stretch from the shortened attitude increases activity of the muscle spindle mechanisms. Slight increases in length, even if the muscle is halfway between fully shortened and extended, may result in a reflexive and prolonged contraction. Within skeletal muscle, sensory muscle fibres ‘monitor’ length changes. These specialized muscular fibres lie deep within the larger extrafusal fibres. Set in parallel, the sensory nerve fibres to these small muscles track back to the spinal cord. Specific motor nerves (gamma motor neurons) modulate muscle spindle contractions. The sensory fibres, the annulospiral and flower-spray afferents, react to either contraction of the nuclear bag and chain fibres or the stretching of these. This is an intrinsic means of protection. A rationale for this is the prevention of tearings of the muscle. Factors that increase the sensitivity and gain of these fibres include stress, anxiety, pain, cold and other general components. Sudden, unexpected stretching, as well as overstretching of the intrafusal fibres, also increases activity of the special sensory flower-spray and annulospiral fibres. Mediated by the spinal cord segment, this results in a reflex action by activation of the alpha motor neuron. This causes contraction of the larger extrafusal muscle fibres. When the gamma motor neuron gain is set too high, the muscle spindles react earlier in the stretch, to a greater degree than is usually necessary, or are inappropriately maintained for longer than is necessary (Becker 1976, Buzzell 1967, Ganong 1995, Korr 1976).
Slow stretching is encouraged, especially before and after exercise, to prevent contractions as a means of ‘training’ the extrafusal muscles, but also to lower the reactivity of the muscle spindles. Pressure applied during inhibition introduces a gentle stretch while allowing re-setting of the stretch receptors (Korr 1979b). This localized pressure may add a stretch in a region of only a few centimetres without challenging the whole muscle. The component that is initially irritating is at a subcritical level. Once the small, localized component is overwhelmed, any affected adjacent area can subsequently be inhibited, with similar results. The use of digitally applied pressure along the muscle, such as is used in PINS, may be a very effective method as it deals with a series of irritated parts. In this way, the practitioner completes the treatment by progressively treating all of the involved elements.
Myotendinotic changes, which are usually characterized by increased tone, thickening, resistance and decreased plasticity, have been described by some authors (Dvorak & Dvorak 1990). These occur within the muscle. They are particularly tender when the muscle is palpated perpendicular to the direction of the fibres. The tenderness may be elicited when using pressure that should not ordinarily be irritating. Along with the increase in sensitivity, changes in these fibres can be palpated from the origin to the insertion. Other non-pathological fibres that are located in the same or nearby muscles do not evidence the same pattern of irritation. The pathological and physiological fibres can be parallel to one another. However, the pathological aspects of the fibres may occur in relatively isolated bundles from the neighbouring unaffected ones. These tender bands can be found in patterns that are similar to trigger points. The appearance may be related to relatively non-traumatic events. After a variable latency period in which only one site is irritable, the rest of the muscle and attachments become irritable. This phenomenon may explain some of the correlation between locations of Jones’ strain/counterstrain tender points and Travell’s trigger points (Travell & Simons 1983). Jones’ points tend to be related to muscle bands, are sensitive to light pressure, but elicit only tenderness at the site of pressure. The Travell points themselves may be sensitive or not, but the hallmark of their existence is the pain patterns that radiate when they are compressed. The differences in quality between the two types of point may represent a matter of duration and degree of the dysfunction.
A complementary muscular reflex system to the muscle spindle is that of the Golgi tendon system. The Golgi tendon organs are set in series and located in a net-like fashion in the tendon, unlike the muscle spindles, which are set in parallel with the extrafusal muscles. Tendons are the least contractile element of a muscle. The Golgi unit has sensory fibres that become relatively stretched during muscular contraction. This is unlike the activation of the muscle spindles, which occurs during muscular stretch. The Golgi tendon organs can also become activated by passive stretch of the whole unit. Unlike the muscle spindle, increased Golgi tendon organ activity brings about reflex relaxation of the muscle as a whole. The sensory neuron from the Golgi apparatus influences the alpha motor neuron indirectly through the mediation of an inhibitory interneuron. The reflex is also known as the clasp-knife reflex, and the results can be quite dramatic and sudden. The progressive tightening of muscles recruits more and more Golgi tendon activity. Therefore, the signals bring about greater inhibition of the muscular contraction. When muscles are hypertonic, an intervention whereby initial stretch results in further contraction is then followed by resultant relaxation (Ganong 1995). This reflex system is the one most probably involved in direct active techniques (i.e. muscle energy technique) and in passive stretch interventions where the region is held at a pathological barrier for a significant amount of time.
A narrow view of compression is that only blood flow is impeded. Impaired flow can be of vascular, lymphatic or neuronal origin. Pressure on the axons can impair the transport of necessary neuropeptides and other substances when considering nerves (Korr 1979c). According to Korr & Appeltauer (1979), the speed with which this flow naturally occurs is quite slow at 40 to several hundred millimetres per day. These rates would therefore not easily explain any immediate effect of inhibitory pressure. The reduction in the soft tissue hypertonicity and the persistence of this effect in response to soft tissue treatments such as PINS may be due in some part to alleviation of the pressure upon nerves (Korr 1979a).
The persistence of somatic dysfunction, as has been expressed previously, can occur despite adequate treatment. Sometimes the breakthrough in successful treatment comes with the recognition of the connection of various apparently unrelated elements. Beginning with the postulate that some dysfunctions support others, failure to recognize and initiate improvement of some aspects allows for continuation or recurrence. The more symptomatic elements may receive the attention, while the supportive ones remain relatively silent in the background: the ‘noisy’ ones are treated while the ‘quiet’ ones are not. After treatment, the whole problem may resolve, the secondary components may assert themselves, or they may instigate a recurrence of the original problem. Using the analogy of a reverberating circuit, all elements should be ‘shut down’ to eliminate the process entirely. It is tempting, on first presentation, to focus solely on the region of the patient’s chief complaint. If there is good resolution, there may be no need to search further. However, when limited results are obtained, there is a need to search further. As a treatment modality, the PINS approach offers an additional means of analysing and treating persistent or difficult dysfunctions.
References
American Osteopathic Association 1998 Glossary of Osteopathic Terminology. American Osteopathic Association Yearbook and Directory of Osteopathic Practitioners. Chicago, Illinois: AOA, 1998.
Bailey H.W. Some problems in making osteopathic spinal manipulative therapy appropriate and specific. J Am Osteopath Assoc. 1976;75:486-499.
Becker R.F. The gamma system and its relation to the development and maintenance of muscle tone. In: 1976 year book of the American Academy of Osteopathy. Colorado Springs: American Academy of Osteopathy; 1976:26-40.
Burton Goldberg Group. Alternative medicine: the definitive guide. Puyallup, Washington: Future Medicine Publishing, 1994.
Buzzell K.A. The potential disruptive influence of somatic input. In: The physiological basis of osteopathic medicine. New York: Insight Publishing; 1967:39-51. Postgraduate Institute of Osteopathic Medicine and Surgery
Cerney J.V. Acupuncture without needles. West Nyack, New York: Parker Publishing, 1974.
Chaitow L. Neuro-muscular technique. Wellingborough, UK: Thorsons, 1980.
Chaitow L. Osteopathic self-treatment. Wellingborough, UK: Thorsons, 1990.
Chaitow L. Modern neuromuscular techniques. New York: Churchill Livingstone, 1996.
Chila A.G. Fascial – ligamentous release: an indirect approach. In: Ward R.C., editor. Foundations for osteopathic medicine. Baltimore: Williams & Wilkins; 1997:819-830.
Cyriax J. ed 6. Text-book of orthopaedic medicine. vol. II. New York: Harper & Row; 1959. Treatment by manipulation and message
Dowling D.J. Myofascial release concepts. In: DiGiovanna E.L., Schiowitz S., Dowling D.J., editors. An osteopathic approach to diagnosis and treatment. ed 3. Philadelphia: Lippincott Williams & Wilkins; 2005:95-102.
Dowling D.J. S.T.A.R.: a more viable alternative descriptor system of somatic dysfunction. American Academy of Osteopathy Journal. 1998;8(2):34-37.
Dowling D.J. Progressive inhibition of neuromuscular structures (PINS) technique. J Am Osteopath Assoc. 2000;100(5):285-297.
Dowling D.J., Scariati P.D. General physiologic considerations. In: DiGiovanna E.L., Schiowitz S., Dowling D.J., editors. An osteopathic approach to diagnosis and treatment. ed 3. Philadelphia: Lippincott Williams & Wilkins; 2005:38-52.
Dvorak J., Dvorak V. Manual medicine: diagnostics, ed 2. New York: Thieme, 1990.
Ehrenfeuchter W.C. Soft tissue techniques. In: Ward R.C., editor. Foundations for osteopathic medicine. Baltimore: Williams & Wilkins; 1997:781-794.
Ganong W.F. Review of medical physiology. Lange, 1995.
Glover J.C., Yates H.A. Strain and counterstrain techniques. In: Ward R.C., editor. Foundations for osteopathic medicine. Baltimore: Williams & Wilkins; 1997:809-818.
Goetz E.W. Manual of osteopathy, ed 5. Ohio: Cincinnati, 1905.
Hazzard C. The practice and applied therapeutics of osteopathy. 1905.
Hermann E. The D.O. October. 1965. 163–164
Johnston W.L. Functional technique: an indirect method. In: Ward R.C., editor. Foundations for osteopathic medicine. Baltimore: Williams & Wilkins; 1997:795-808.
Jones L.H. Strain and counterstrain. Newark, Ohio: American Academy of Osteopathy, 1981.
Jones L.H., Kusenose R., Goering E. Jones strain–counterstrain. Idaho: Boise, 1995. Jones Strain–Counterstrain Company
Kenyon J. Acupressure techniques: a self help guide. Rochester, Vermont: Healing Arts Press, 1988.
Korr I.M. Proprioceptors and somatic dysfunction. In: 1976 year book of the American Academy of Osteopathy. Colorado Springs, Colorado: American Academy of Osteopathy; 1976:41-50.
Korr I.M. Neurochemical and neurotrophic consequences of nerve deformation: clinical implications in relation to spinal manipulation. J Am Osteopath Assoc. 1979;75:409-414. (reprinted in: The collected papers of Irvin M Korr) American Academy of Osteopathy, 1979a, Colorado Springs, pp 196–199
Korr I.M. Proprioceptors and somatic dysfunction. J Am Osteopath Assoc. 1979;74:638-650. (reprinted in: The collected papers of Irvin M Korr), American Academy of Osteopathy, Colorado Springs, 1979b. pp 200–207
Korr I.M. The nature and basis of the trophic function of nerves: outline of a research program. J Am Osteopath Assoc. 1979;66:74-78. (reprinted in: The collected papers of Irvin M Korr), American Academy of Osteopathy, 1979c, Colorado Springs, pp 96–99
Korr I.M., Appeltauer G.S. Continued studies on the axonal transport of nerve proteins to muscle. J Am Osteopath Assoc. 1979;69:76-78. (reprinted in: The collected papers of Irvin M Korr), American Academy of Osteopathy, 1979, Colorado Springs, pp 100–101
Moore K.L. Clinically oriented anatomy. London: Williams & Wilkins, 1980.
Owens C. An endocrine interpretation of Chapman’s reflexes, ed 2. Chattanooga, Tennessee: Chattanooga Printing and Engraving Company, 1937.
Patterson M.M. A model mechanism for spinal segmental facilitation. J Am Osteopath Assoc. 1976;76:62-72.
Prudden B. Pain erasure: the Bonnie Prudden way. New York: Ballantine Books, 1980.
Robbins S.L., Cotran R.S., Kumar V. Pathologic basis of disease, ed 3. Philadelphia: WB Saunders, 1984.
Schiowitz S. DiGiovanna, Schiowitz S., An osteopathic approach to diagnosis and treatment. ed 2. Philadelphia: Lippincott-Raven; 1997:91.
Schultz W. Shiatsu: Japanese finger pressure therapy. New York: Bell Publishing, 1976.
Still A.T. The philosophy and mechanical principles of osteopathy. Kansas City, Missouri: Hudson-Kimberly, 1902.
Still A.T. Autobiography of AT Still, Revised ed. Kirksville, Missouri: Self-published, 1908.
Stoddard A. Manual of osteopathic practice. London: Hutchinson Medical, 1969.
Tasker D.D. Principles of osteopathy, ed 4. Los Angeles: Bireley & Elson, 1916.
Travell J.G., Simmons D.G. Myofascial pain and dysfunction: the trigger point manual. vol. I. Baltimore: Williams & Wilkins; 1983. The upper extremities
Typaldos S. Introducing the fascial distortion model. American Academy of Osteopathy Journal. 4(2), 1994.
Van Buskirk V.L. A manipulative technique of Andrew Taylor Still as reported by Charles Hazzard, DO, in 1905. J Am Osteopath Assoc. 1996;96(10):597-602.
Ward R.C. Integrated neuromusculoskeletal release and myofascial release: an introduction to diagnosis and treatment. In: Ward R.C., editor. Foundations for osteopathic medicine. Baltimore: Williams & Wilkins; 1997:846-849.
Weil A. Spontaneous healing. New York: Ballantine Books, 1995.