8 Associated techniques
Chill-and-stretch (spray-and-stretch) technique
Integrated neuromuscular inhibition technique (INIT)
Ischaemic compression and trigger point release
Muscle energy techniques (MET) – including isolytic stretch
Neuromuscular therapy (soft tissue manipulation)
Percussion technique or spondylotherapy
Proprioceptive adjustment (applied kinesiology)
Pump techniques – lymphatics, liver/spleen, pedal
‘S’ and ‘C’ bends: myofascial release methods for lengthening soft tissues
Stretching fascia – myofascial release
Specific (abdominal) release techniques
Soft tissue approaches
In Chapter 6 a detailed description was given of NMT in spinal, cervical, pelvic and intercostal structures, and abdominal techniques were described in Chapter 7.
In this chapter a number of additional soft tissue approaches/modalities/methods that are frequently employed alongside NMT (listed in Box 8.1) will be outlined in alphabetical order, rather than any other sequence.
Box 8.1 Additional soft tissue approaches
• Active release technique (ART)
• Integrated neuromuscular inhibition technique (INIT)
• Ischaemic compression/trigger point release
• Neuromuscular therapy/soft tissue manipulation discussion
• Pump techniques (liver, lymphatics, spleen, pedal)
• Stretching fascia – myofascial release
Active release technique® (ART)
Active release technique is a registered modality, that is in many ways similar to traditional ‘pin and stretch’ techniques. ART is a soft tissue approach that at its most basic involves the practitioner isolating a contact point close to the region of soft tissue dysfunction, after which the patient is directed to move in a way that produces a longitudinal sliding motion of soft tissues (nerves, ligaments, muscles) beneath the anchored contact point. Alternatively the movements may be initiated by the practitioner, or may be combined with active movements, whichever achieves the best outcome.
There have been relatively few studies to evaluate efficacy, however one pilot study demonstrated no benefit to quadriceps function in athletes with anterior knee pain where ART was applied (Drover et al 2004). While in different pilot studies:
1. Hamstring length was shown to have increased subsequent to treatment (George 2006).
2. Active release technique was found to be beneficial in management of carpal tunnel syndrome patients (George et al 2006).
Elbow (and forearm) technique
Caution – Direct elbow pressure should be avoided, or should be performed with great care:
1. if tissues are inflamed or during the remodelling phase, following trauma, is incomplete
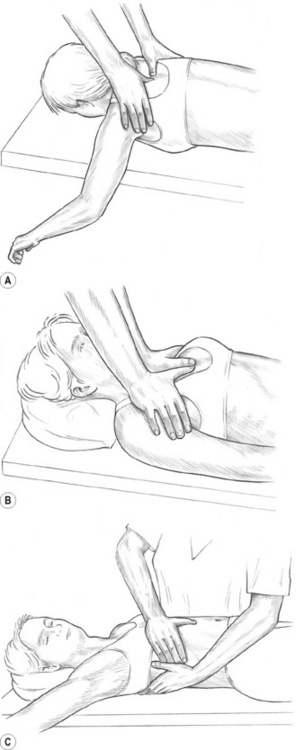
In treating certain muscle groups, notably the gluteals and the sacrospinalis group, it is sometimes difficult, or even impossible, to impart adequate force via the thumb or fingers, owing to the degree of resistance in the tissues involved. Where it is considered appropriate, elbow and/or forearm technique should be applied preparatory to NMT, on a number of occasions, so that NMT can subsequently be applied more effectively.
Sacrospinalis
In treating sacrospinalis, for example, the entire spine should be lubricated, and the practitioner should stand on the patient’s left side (patient supine, pillow under thorax) (Fig. 8.1).
• The right elbow tip should be placed just superior to the sacral base, with the forearm at right angles to the patient’s body, as in Fig. 8.1A (and also Figs 10.13B,C)
• By flexing the knees slightly and allowing weight to be transferred via the elbow, the practitioner can apply controlled pressure to the paraspinal muscles with the broad contact of the forearm, or by raising the hand slightly, more precisely by the elbow itself.
• The more the hand is elevated, the sharper the angle of contact of the elbow, and the more precise strokes will be, at the point of contact.
• The elbow/forearm should be allowed to glide slowly cephalad.
• If pain is reported, pressure should be reduced.
• Several glides or strokes along the full length of the spine will greatly relax even marked contractions.


Chronic shoulder restriction
An example of more focused use of elbow technique involves work on the lateral border of the scapula in cases of chronic shoulder restriction (see Fig. 8.1B).
In order to encourage more normal movement of the humerus in the glenoid fossa, as well as the free glide of the scapula on the rib-cage:
• The patient is side-lying with the side to be treated uppermost, and with the arm abducted, elevated, extended and externally rotated, so that the patient’s hand is close to her head.
• The practitioner should be behind the patient, standing sideways on to the table, facing her head.
• With his non-tableside hand the practitioner grasps the patient’s upper arm, close to the elbow, reinforcing the external rotation, abduction, etc.
• The practitioner’s tableside arm is flexed at the elbow, which should be carefully placed in the patient’s exposed axilla, as close to the lateral border of the scapula as possible.
• Short, slow-moving strokes should be applied along the scapula border, as well as anteriorly and posteriorly, following the curve of the ribs below the axilla.
• If localized contracted tissue is sensed it may be helpful to simply apply sustained, tolerably comfortable, pressure – and wait for a softening to occur.
• The non-treating hand should use any release resulting from the elbow treatment to gradually increase the range of rotation and abduction at the shoulder, to improve humeroglenoid movement.
Treatment of piriformis muscle, and its central trigger points, can usefully be achieved by means of direct elbow pressure, applied to the main trigger point area in the belly of the muscle, while the side-lying patient’s leg is rotated to internally rotate the hip, in order to achieve a lengthening of the muscle. (See illustrated details of the use of the elbow in this way, later in this chapter under the heading Piriformis Technique (see Fig. 8.11)).

 Chill-and-stretch (spray-and-stretch) technique
Chill-and-stretch (spray-and-stretch) technique
Chilling and stretching a muscle housing a trigger point rapidly assists in deactivation of the abnormal neurological behavior of the site. Travell & Mennell have described these effects in detail (Mennell 1969, 1975, Simons et al 1999, Travell 1952, Travell & Simons 1992).
Travell & Simons (1992) and Simons et al (1999) have discouraged the use of vapocoolants to chill the area, because of environmental considerations relating to ozone depletion, and have instead urged the use of stroking with ice in a similar manner to the spray stream to achieve the same effect. The objective is to chill the surface tissues while the underlying muscle housing the trigger is simultaneously stretched. They also point out that the spray is applied before or during the stretch and not after the muscle has already been elongated.
However recently, Gebauer’s Spray and Stretch (prescription) and Instant Ice (non-prescription), both non-flammable, nonozone-depleting vapocoolants, have emerged into a market that has until recently been devoid of environmentally friendly sprays. Spray and stretch techniques can therefore now not only be applied in the treatment room, but also in home care with the patient’s use of the non-prescription version – without environmental risk.
A container of vapocoolant spray with a calibrated nozzle which delivers a moderately fine jet stream, or a source of ice, is needed. The jet stream should have sufficient force to carry in the air for at least 3 feet. Experience suggests that a mist-like spray is less effective. (See Figs 8.2A,B.)
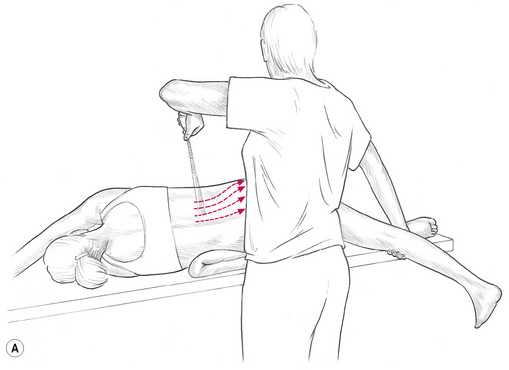
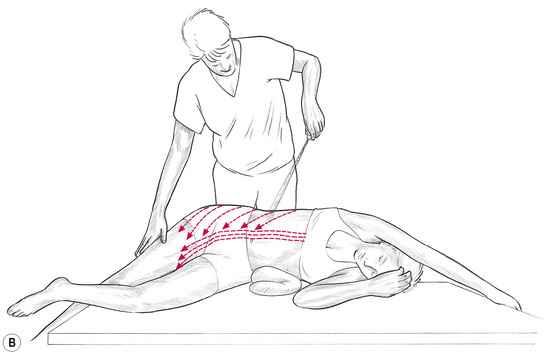
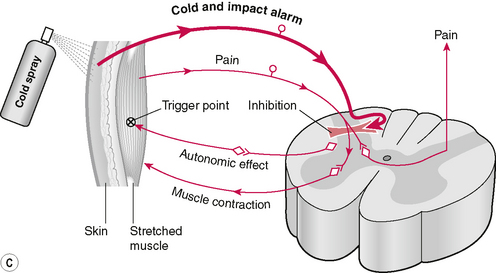
Figure 8.2A,B,C Anterior and posterior view of application of vapocoolant spray to trigger point (quadratus lumborum in this illustration). Muscles housing trigger points are placed at stretch while a coolant spray is utilized to chill the point and the area between it and the target reference area. Schematic illustration of the proposed effects of cold spray application.
Simons & Mense (2003) report that the vapocoolant spray appears to inhibit pain and reflex motor, and autonomic responses in the central nervous system. When the pain stimuli subside a degree of relaxation takes place allowing stretching and lengthening of the muscle to be more effective and less uncomfortable (Lupandin & Kuz’mina 1985). (See Fig. 8.2C).
Ice as an alternative
Ice used to achieve the same effects as the cold spray discussed above, can comprise a cylinder of ice formed by freezing water in a paper cup and then peeling this off the ice. A wooden handle will have been frozen into the ice to allow for its ease of application, as it is rolled from the trigger towards the referred area in a series of sweeps.
The author has found that a cold soft-drink-can, that has been partially filled with water and then frozen, is more suitable, because ice applied directly onto skin melts rapidly and, as Travell & Simons (1992) have pointed out, the skin must remain dry for this method to be successful, because dampness slows the rate of cooling of the skin and may also delay rewarming.
An ice-cold, metal container, can however be rolled over the skin, and will retain its chilling potential for long enough to achieve the ends desired.
Method
Whichever source of cold is chosen, the patient should be comfortably supported to promote muscular relaxation.
• If a spray is used, the container should be held approximately 2 feet (60 cm) away, in such a manner that the jet stream meets the body surface at an acute angle or at a tangent, not perpendicularly (Figs 8.2A,B).
• This lessens the shock of the impact. For the same reason, the stream is sometimes started in air, or on the practitioner’s hand, and is gradually brought into contact with the skin overlying the trigger point.
• The stream/ice massage/frozen canister should be applied in one direction only, not back and forth.
• Each sweep should commence in the tissues overlying the trigger point and be moved slowly and evenly outward over towards reference zone (where pain is reported as being experienced by the patient). The direction of movement of the spray/ice should follow the fibre direction of the muscle.
• It appears that it is advantageous to spray, or ice-chill, both trigger and reference areas, because secondary trigger points are likely to have developed within reference zones when pain is very strong.
• Clinical experience suggests that the optimum speed of movement of the sweep/roll over the skin, is approximately about 4 inches (10 cm) per second.
• Each sweep should be started slightly proximal to the trigger point, and be moved slowly and evenly through the reference zone, to cover it and extend slightly beyond it.
• These sweeps should be repeated in a rhythm of a few seconds on, and a few seconds off, until all the skin over trigger and reference areas has been covered once or twice.
• If aching or ‘cold pain’ develops, or if the application of the spray/ice/canister sets off a reference of new pain, the interval between applications should be lengthened.
• Care should be taken not to frost or blanch the skin.
• During the application of cold the taut fibres should be placed at light stretch, and after the chilling should be further stretched passively.
• Steady, gentle stretching is usually essential if a satisfactory result is to be achieved.
• As relaxation of the muscle occurs, continued stretch should be maintained for 20–30 seconds, and after each series of cold applications active motion should be tested.
• The patient should be asked to move in the directions that were restricted before spraying/chilling, or that were painful to activate.
• An attempt should be made to restore the full range of motion, but always within the limits of discomfort, as sudden overstretching can increase existing muscle spasm.
• The treatment is continued in this manner until the trigger points (often several are present) and their respective pain reference zones have been treated.
• The entire procedure may occupy 15–20 minutes and should not be rushed.
The importance of re-establishing normal motion in conjunction with the use of the chilling is well founded. It may be that the brief interruption of pain impulses is insufficient and that input of normal impulses must also occur for the obliteration of trigger points to be successfully achieved by these means.
Simple exercises that use the principle of passive or active stretch should be outlined to the patient, to be carried out several times daily, after the application of gentle heat (hot packs, etc.) at home. Usual precautions should be mentioned, such as avoiding the use of heat if symptoms worsen or if there is evidence of inflammation.
Deep tissue release
In using NMT it is often helpful to apply a local ‘tissue release’ technique to areas of marked contraction or spasticity. In areas overlying bone, the techniques suitable for use in the abdominal region (see Specific (abdominal) release techniques, later in this chapter) are not applicable.
The method recommended is as follows:
• The contact on the tissues involved is made by extending the digits of either hand and making firm contact with the area between the first and second metacarpophalangeal joints, taking out the slack of the tissues and engaging a resistance barrier.
• This contact is rotated clockwise or anticlockwise in order to increase the tension in the underlying tissues, until the tissues with the greatest resistance are noted and combined barrier is engaged – downwards and in a torsional manner.
• The other hand is then placed over the contact hand so that the downward pressure and rotation are reinforced.
• In addition, a further direction of stretch should be introduced by the second hand –directed laterally/medially or superiorly/inferiorly, whichever offers the greatest resistance.
• The tissues would therefore be receiving a direct downward pressure, a rotational stretch, and a further degree of stretch in another direction, all maintained by the two treating hands.
• The overlying hand should have been placed in such a way that the radial border of the metacarpal base of the thumb is directly over the contact point of the first hand’s contact (i.e. over the second metacarpal joint area). (See Fig. 8.3.)
• The fingers of the overlying hand should be tightly in contact with the lateral border of the contact hand.
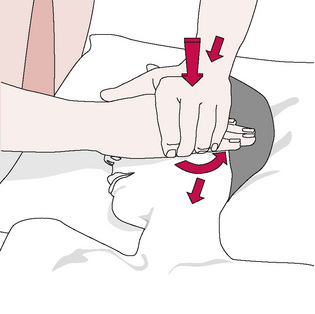
Figure 8.3 Deep tissue release technique applied, in this example, close to the temporomandibular joint area. The soft tissue slack will have been removed (i.e. barriers engaged) by a precise contact from the right hand (the area between the first and second metacarpophalangeal joints) in directions of greatest resistance (a) into the soft tissues, (b) into rotation (counterclockwise in this example) and (c) inferiorly. This contact is supported by the left hand, which then completes the release by means of either a sharp contraction of the contact or a short sharp thrust (see text for further detail).
Redrawn from Fielder & Pyott (1955).
The last stage of the release technique may be performed in one of two ways:
1. The overlying hand executes a short sharp squeeze by flexing the middle finger against the metacarpals of the contact hand. The resulting pressure in the intermetacarpal area provides the ‘thrust’ or release force. The line of force of this squeeze is towards the practitioner.
2. The second method of release, which is more suitable for deeper contractions of tissue, is applied via short sharp thrust by the overlying hand against the contact hand, with a simultaneous medial rotation of the contact hand. The line of force in this technique is away from the practitioner.
This soft tissue approach, which emerged from American naprapathy (a form of soft tissue manipulation popular primarily in Sweden, and the Chicago area of the United States), and an adhesion releasing method (known as ‘bloodless surgery’ between the two World Wars), has been adapted for use in the UK by McTimoney chiropractic practitioners.
Induration technique
Note: This method is suitable even in cases of great fragility (osteoporosis) because pressure is not meant to exceed an ounce or two (30 to 60 grams), at most.
As many patients are too frail, or too ill, to allow the full NMT treatment to be applied, a useful technique exists to aid in normalizing reflex and local areas of the paraspinal musculature. Stoddard (1969) has pointed out that protective spasm in muscle can often indicate underlying pathology (osteoporosis, etc.) and, clearly, deep pressure techniques would be contraindicated in such conditions.
• With the patient sitting or lying, the practitioner, using a very light ‘skin-on-skin’ contact which evaluates ‘drag’ or hills/valleys (see Ch. 5), runs the fingertips longitudinally down the side of the spine (side of spine opposite that on which practitioner is standing) over the transverse processes.
• Any spot or area of ‘hardened’ or indurated tissue, that also palpates as tender to the patient is marked for attention.
• Treatment is applied by palpating the sensitive area with the tip of the thumb (or a finger), of one hand, while applying light pressure towards the painful spot with the soft thenar or hyperthenar eminence of the other hand, which is resting on the spinous process of the vertebra, adjacent to the indurated tissue (Fig. 8.4).
• Direct pressure (extremely light – ounces/grams only) towards the pain should lessen the degree of tissue contraction, and the sensitivity.
• If it does not do so, the angle of light pressure on the spinous process, towards the painful point, should be varied slightly, so that, somewhere within an arc embracing a half circle, an angle of push towards the pain will be found to abolish the pain totally, and will lessen the palpated feeling of tension.
• This ‘position of ease’ is held for around 20 seconds, before moving on to the next sensitive area.
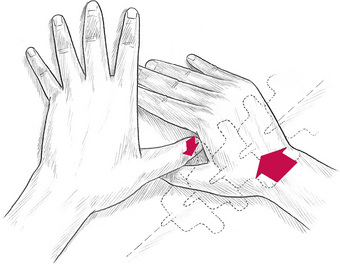
Figure 8.4 Hand positions for induration technique. Pressure used on the spinous process is measured in ounces (grams) at most.
This technique, which has strong echoes of ‘strain/counterstrain’ (described later in this chapter) can be used with NMT or instead of deeper probing measures, that, for practical reasons, may be contraindicated (for example if the patient’s condition involves extreme sensitivity, inflammation or pathology).
Integrated neuromuscular inhibition technique (INIT)
(see Fig. 9.1 and Ch. 9) (Chaitow 1994)
INIT, when used to deactivate a trigger point, involves the application of a sequence that includes:
• Inhibitory (ischaemic) compression (either sustained or intermittent: 5 seconds pressure/2 seconds release/repeated) until a change is reported or noted.
• Place the tissues into a position of ease, to encourage a muscle spindle release of excessive tone (see descriptions of ‘positional release’ below).
• The patient introduces an isometric contraction involving the precise tissues housing the trigger point.
• This is followed by passive stretching of the local tissues.
• Followed by active and passive stretching of the entire muscle (subsequent to another isometric contraction) (see notes on muscle energy technique (MET) below).
• After this activation of antagonists to muscle housing the trigger point may be used to complete the sequence.
This approach achieves a triple effect: inhibition/ischaemic compression, positional release, followed by an isometrically enhanced stretch. The sequence represents a significant advance in deactivating trigger points and the tissues that house them. The initial pressure application (and subsequent positional release and MET) may follow on from identification of the trigger point during NMT evaluation.
Ischaemic compression and trigger point release
Direct inhibitory pressure has a long history of use in many forms of bodywork, including osteopathy, in order to achieve a release of hypertonic, tense tissues, spasm, cramp, etc.
Hou et al (2002) report: ‘Ischemic compression therapy provides alternative treatments using either low pressure (pain threshold) and a long duration (90 s) or high pressure (the average of pain threshold and pain tolerance) and short duration (30 s), for immediate pain relief and myofascial trigger point sensitivity suppression.’
Caution – Direct pressure should be avoided, or performed with great care:
1. If tissues are inflamed, or are in the remodelling phase, following trauma
3. Close to blood vessels and nerves
4. Close to attachment sites (to avoid provoking enthesitis)
Travell & Simons (1983, 1992) have suggested that in treatment of trigger points, these should receive ischaemic compression (‘sustained digital pressure’) for a period of between 20 seconds and 1 minute. The pressure should be gradually increased as the trigger point’s sensitivity (referred sensation, as well as the local discomfort) reduces, and the tension of the tissues housing the trigger (‘taut band’) eases. Stretching techniques should be applied following the compression; see integrated neuromuscular inhibition technique (INIT) described later in this chapter.
Fernández-De-Las-Peñas et al (2006) report on a study that verified these suggestions. ‘Ischemic compression technique and transverse friction massage were equally effective in reducing tenderness in myofascial trigger points.’
The mechanisms involved, as seen from a Western perspective, would include ‘neurological overload’, the release of endogenous morphine-like products (endorphins, enkephalins, endocannabinoids) (McPartland & Simons 2007) as well as ‘flushing’ of tissues with fresh oxygenated blood following the compression. Oriental interpretations would include modulation of energy transmission.
See Chapter 3, Box 3.5, for more detail on compression effects.
Massage
Using standard massage protocols, Field (2000) and others have demonstrated, in hundreds of research projects, that significant benefits occur in the following conditions and patient populations: enhanced growth in preterm infants, cocaine and human immunodeficiency virus (HIV)-exposed infants, pain reduction, during labour, pre-debridement for burn patients, juvenile rheumatoid arthritis, fibromyalgia, premenstrual syndrome, migraine, children with autism, adolescents with attention deficit hyperactivity disorder (enhanced attentiveness), anxiety (e.g. exam settings), depression, post-traumatic stress, adolescent psychiatric patients, adolescent mothers, bulaemia and anorexia, chronic fatigue syndrome, autoimmune and immune disorders, diabetes mellitus (reduced glucose levels), asthma, cystic fibrosis, atopic dermatitis, HIV-positive adults, oncology patients.
Some of Field’s explanations for the benefits of massage are summarized later in this section.
We should also not lose sight of the tried and tested effects of massage on the soft tissues. The degree of that effect will vary with the type of soft tissue manipulation employed, and the nature of the patient and the problem. Soft tissue techniques, apart from those specifically associated with NMT, may include the following.
Safety
There are few modalities that are more universally useful than massage. In its most generic form massage is non-invasive, almost totally safe, and with few contraindications. When massage incorporates techniques based on soft tissue manipulation, or when it becomes ‘deeper’ and has specific therapeutic goals (such as deactivation of trigger points, reduction of fibrosis) universal suitability is reduced and cautions are required – for example when serious pathology (cancer, arthritis), active inflammation and/or vulnerability (osteoporosis for example) are current.
Massage methodology
The various modes of application of massage (e.g. gliding, effleurage, kneading, petrissage, compression) provide the most efficient means of applying variations of therapeutic load to tissues. Each method can be modified, depending on the desired outcome, by adjusting depth of pressure, drag (amount of tensile force applied), direction, speed, rhythm, frequency and duration of contact.
The strokes that make up massage strokes include:
• Petrissage – wringing and stretching movements, across the fibre direction of muscles.
• Kneading – where the hands shape themselves to the contours of the area being treated. The tissues between the hands are lifted and pressed downwards and together.
• Inhibition – which involves application of pressure directly to the belly or origins or insertions of contracted muscles or to local soft tissue dysfunction for a variable amount of time or in a ‘make-and-break’ (pressure applied and then released) manner to reduce hypertonic contraction or for reflexive effects.
• Effleurage – this is a relaxing technique that is used, as appropriate, to initiate or terminate other manipulative methods. Pressure is usually even throughout the strokes, which are applied with the whole hand in contact.
• Vibration and friction – such contacts are used near origins and insertions and near bony attachments for relaxing effects on the muscle as a whole and to reach layers deep to the superficial tissues. It is performed by small circular or vibratory movements, with the tips of fingers or thumb. The heel of the hand may also be used.
• Roulement – this involves skin lifting and rolling, which, as with most massage methods, can be used diagnostically as well as therapeutically (see earlier in this chapter for discussion of skin rolling).
• Transverse or cross-fibre friction – this is performed along or across the belly of muscles using the heel of the hand, thumb or fingers applied slowly and rhythmically or vigorously, depending upon the objectives.
• Tapotement – involves percussive tapping, clapping, drumming and vibrating activities, involving fingertips or the ulnar borders of the hands.
Massage cautions (Wittlinger & Wittlinger 1982)
• In areas that have been recently traumatized (2–3 weeks) and which are in the remodelling phase (including surgery).
• When a person is fatigued the duration and depth of the application should be reduced.
• If a patient has a fragile bone structure, the depth of pressure should be modified.
• When the patient is agitated the rhythm should be modified to create a calming effect.
• Acute infections and acute inflammation (generalized and local)
Physiological effects of massage
The biochemical influences of massage include altered stress hormone (cortisol) production (Field 2000). Perhaps surprisingly, massage fails to increase blood flow through muscle unless it is exceptionally vigorous (Shoemaker et al 1997); however, drainage efficiency is improved when light techniques are employed (Ikimi et al 1996).
• Pain perception is reduced by massage, possibly due to gating of impulses (Clelland et al 1987).
• Massage mechanically modifies soft tissue status (stretching, mobilizing, etc.) depending on the variations in load application (sustained pressure, shearing load, etc.).
• The colloids in fasciae that surround, support and invest all soft tissues respond to appropriately applied pressure and vibration by changing state from a gel-type consistency to a solute, which increases internal hydration and assists in the removal of toxins from the tissue (Oschman 1997).
• Psychological effects include reduced arousal, calmer mood and modified perception of anxiety (Rich 2002).
• Neurological influences include a transient reduction in motor neuron excitability during and following massage (Goldberg 1992).
• Massage also produces a decrease in the sensitivity of the gamma efferent control of the muscle spindles and thereby reduces any shortening tendency of the muscles (Puustjarvi 1990).
Other methods that we would associate with the above techniques of traditional massage might include the various applications of NMT, as described in this text, as well as connective tissue massage techniques, which are used primarily for reflex effects.
Massage effects explained
How are the various effects of massage and soft tissue manipulation explained? Field (2000), discussing her many research findings, states:
In all these studies depression, anxiety, and stress hormones significantly decreased following massage therapy. Because depression, anxiety and stress hormones (particularly cortisol) are notably elevated in autoimmune and immune disorders, we hypothesized that massage therapy might also help these problems.
Field further suggests that the evidence from her studies points to enhanced homeostatic function, in both infants and adults, following massage therapy, as evidenced by improved sleep patterns (and therefore higher levels of somatostatin), as well as increased serotonin levels. These thoughts are supported by the work of other researchers (Ironson et al 1993).
Apart from the undoubted anxiety and stress-reducing influences of massage, a combination of physical effects also occurs (Sandler 1983):
1. Pressure, as applied in deep kneading or stroking along the length of a muscle, tends to displace its fluid content.
2. Venous, lymphatic and tissue drainage is thereby encouraged.
3. The replacement of this with fresh oxygenated blood aids in normalization via increased capillary filtration and venous capillary pressure.
4. This reduces oedema and the effects of pain-inducing substances that may be present (Hovind & Nielson 1974, Xujian 1990).
5. Massage also produces a decrease in the sensitivity of the g-efferent control of the muscle spindles, and thereby reduces any shortening tendency of the muscles (Puustjarvi et al 1990).
6. Pressure techniques, such as are used in NMT, and the methods employed in MET have a direct effect on the Golgi tendon organs, which detect the load applied to the tendon or muscle.
7. These have an inhibitory capability, which can cause the entire muscle to relax.
8. The Golgi tendon organs are set in series in the muscle, and are affected by both active and passive contraction of the tissues. The effect of any system that applies longitudinal pressure or stretch to the muscle will be to evoke this reflex relaxation. The degree of stretch has, however, to be great, as there is little response from a small degree of stretch.
9. The effects of MET, articulation techniques and various functional balance techniques depend to a large extent on these tendon reflexes (Sandler 1983).
Soft tissues at centre stage
We are in the midst of a change in the concepts of manual therapy that has far-reaching implications. One of the major changes is the restoration of the soft tissue component to centre stage, rather than the peripheral role to which it has been assigned in the past as ever more general health problems are found to involve musculoskeletal dysfunction, for example chronic fatigue conditions (Chaitow 1990).
Lewit (1985) discusses aspects of what he describes as the ‘no man’s land’ that lies between neurology, orthopaedics and rheumatology, which, he says, is the home of the vast majority of patients with pain derived from the locomotor system, and in whom no definite pathomorphological changes are found. He makes the suggestion that these be termed cases of ‘functional pathology of the locomotor system’. These include most of the patients attending osteopathic, chiropractic and physiotherapy practitioners.
The most frequent symptom of individuals involved in this area of dysfunction is pain, which may be reflected clinically by reflex changes such as muscle spasm, myofascial trigger points, hyperalgesic skin zones, periosteal pain points, or a wide variety of other sensitive areas that have no obvious pathological origin. As the musculoskeletal system is the largest energy user in the body by far, it is no surprise that fatigue is a feature of chronic changes in the musculature. It is a major part of the role of NMT to help in identifying such areas, and also in offering some help in differential diagnosis. NMT and other soft tissue methods are then capable of positively influencing many of the causative aspects of these myriad sources of pain and disability.
Muscle energy techniques (MET) – including isolytic stretch
Muscle energy technique (MET) involves the use of isometric contractions (Mitchell et al 1998) to assist in modification of muscle and joint behavior. Variations on this basic theme involve the use of isotonic concentric, or eccentric, contractions (Schmitt 1999), or a series of rhythmically pulsating contractions (Ruddy 1961) instead of, or as well as, basic isometric variations.
Definition of MET
MET involves a muscle, or group of muscles, being voluntarily contracted, in a specified direction, for a defined length of time (commonly 5 to 7 seconds), involving submaximal effort, with the contraction being matched by the practitioner/therapist’s effort, so that no movement occurs (Mitchell & Mitchell 1995, Mitchell 1976).
• MET has been shown to improve joint range of motion, including spinal joints (Kamani & Walters 2000, Lenehan et al 2003).
• MET has been shown to improve muscle extensibility more effectively than passive, static stretching – both in the short and long term (Mehta & Hatton 2002, Feland et al 2004, Ferber et al 2002).
• In addition studies offer support for the hypoalgesic effects of MET – for example in relation to spinal pain (Brodin 1962, Cassidy et al 1992, Wilson et al 2003).
• Myofascial trigger point deactivation has been shown to be enhanced by use of MET (Chaitow 1994, Fernández-de-las-Peñas 2005, Simons et al 1992, 1999).
MET origins
Much of the research from which conclusions regarding MET efficacy and mechanisms are taken, relates to studies involving proprioceptive neuromuscular facilitation (PNF) stretching. (Fryer 2006, Schmitt et al 1999) PNF (and MET) application may involve one of 3 variations:
• Contract–relax (CR), in which the muscle being stretched (the agonist) is contracted and then relaxed, before stretching. (See Fig. 8.5A and 8.5B).
• Agonist contract–relax (ACR), in which contraction is of the antagonist, rather than the muscle to be stretched (the agonist). It is suggested that the confusing title of Agonist contract-relax (ACR) should be ignored. The approach relies, it is suggested (see below), on reciprocal inhibition.
• Contract–relax agonist–contract (CRAC), involves a combination of the two methods (CR and ACR) listed above.
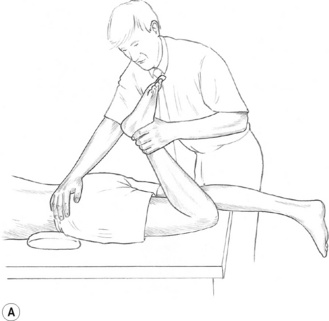
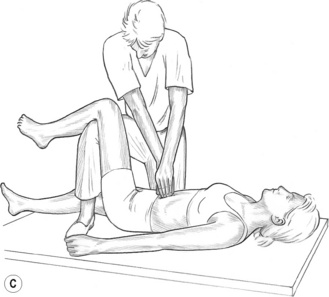
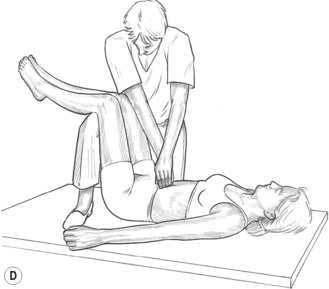
Figure 8.5A MET treatment of left rectus femoris muscle. Note the practitioner’s right hand stabilizes the sacrum and pelvis to prevent undue spinal stress during the stretching phase of the treatment.

Figure 8.5B MET treatment of tensor fascia lata. If a standard MET method is being used, the stretch will follow the isometric contraction in which the patient will attempt to move the right leg to the right, against sustained resistance. It is important for the practitioner to maintain stability of the pelvis during the procedure.
Proposed MET mechanisms
Kuchera & Kuchera (1992) as well as Denslow et al (1993) have speculated on the neurological mechanisms that may follow use of MET (contract/relax version).
• They hypothesize that the effects may result from the inhibitory Golgi tendon reflex, activated during the isometric contraction that leads to reflex relaxation of the muscle, as a result of post isometric relaxation (PIR) (see Fig. 8.6A).
• An alternative reflex effect has been suggested in which an isometric contraction of the antagonist(s) of affected muscle(s) induce relaxation via reciprocal inhibition (RI) (ACR version) (see Fig. 8.6B).
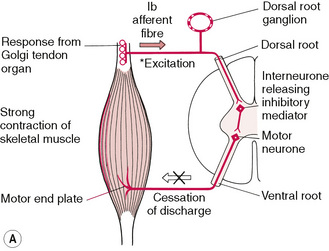
Figure 8.6A Schematic representation of the neurological effects of the loading of the Golgi tendon organs of a skeletal muscle by means of an isometric contraction, which produces a post-isometric relaxation effect in that muscle.
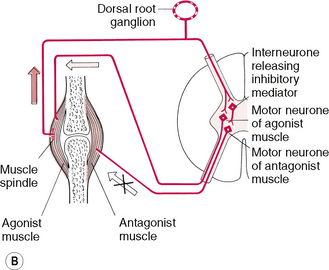
Figure 8.6B Schematic representation of the reciprocal effect of an isometric contraction of a skeletal muscle, resulting in an inhibitory influence on its antagonist.
Some studies support the concept of neurological muscle inhibition, following MET isometric contraction. For example Moore & Kukulka (1991) found that a strong brief depression of the soleus H-reflex occurred, for about 10 seconds, following sub-maximal isometric plantar flexion contractions, probably as a result of pre-synaptic inhibition.
However simultaneous monitoring of the tibialis anterior muscle’s EMG activity revealed minimal activity, so excluding the possibility of reciprocal inhibition operating (Moore & Kukulka 1991).
Since many studies have demonstrated that active motor activity plays a minimal role in producing resistance to stretch (Magnusson et al 1996b) the question remains as to whether low-level motor activity plays a role in limiting the passive stretch of a muscle.
Self-evidently, in order for it to be accepted that MET produces increased muscle length, by means of reflex muscle relaxation, low-level motor activity needs to be shown to play a role in limiting passive stretching of muscle, and this has not been possible (Fryer 2006).
• Ballentyne et al (2003) suggest that the PIR theory is poorly supported by research. Citing EMG evidence they note that ‘various studies have shown that passive stretch does not influence the electrical activity of the hamstring muscle (Klinge et al 1997, McHugh et al 1998) demonstrating that low level muscle contraction does not limit muscle flexibility, disputing the proposal of [such] a neurological mechanism.[i.e. PIR]’
• Lederman (1995) states that the PIR model ignores the complex and dominant influence of the central nervous system.
• Fryer (2000) points to the lack of evidence supporting muscle contraction as a factor in restricted joint ROM, or in spinal dysfunction.
• Magnusson et al (1995) found that low-level EMG activity was unchanged following isometric contractions, or passive stretching.
• Magnusson et al (1996a) have demonstrated that increases in muscle length, following 90 seconds of passive stretching, occurs without any change to the low-level EMG activity of that muscle.
• Fryer (2006) has speculated that although the exact mechanism by which increased muscle extensibility occurs, remains unclear, it probably involves both neurophysiological and mechanical factors, possibly including viscoelastic and plastic changes in the connective tissue elements of the muscle. In fact Fryer maintains that although MET techniques produce greater ROM changes than static stretching, they also produce greater EMG activity in the muscle undergoing the stretch.
• Fryer & Fossum (2008) have hypothesized a neurological explanation for the analgesic effects of MET. A sequence is suggested in which activation of muscle mechanoreceptors and joint mechanoreceptors occur, during an isometric contraction. This leads to sympatho-excitation evoked by somatic efferents and localized activation of the periaqueductal grey that plays a role in descending modulation of pain. Nociceptive inhibition then occurs at the dorsal horn of the spinal cord, as simultaneous gating takes place of nociceptive impulses in the dorsal horn, due to mechano-receptor stimulation (see Fig. 8.6C).
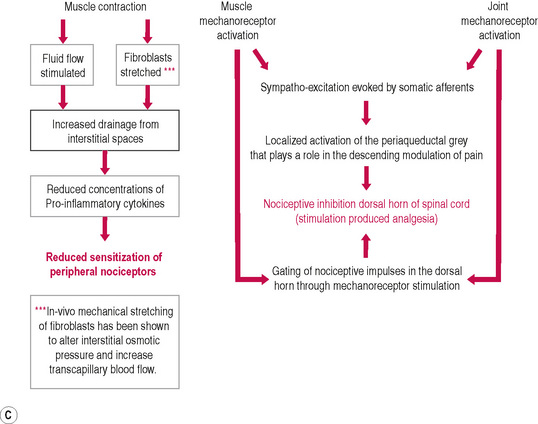
Figure 8.6C Schematic diagram of hypoalgesic effects of MET.
Modified from Fryer G., Fossum C. 2009. Therapeutic Mechanisms Underlying Muscle Energy Approaches. In: Physical Therapy for tension type and cervicogenic headache. Fernández de las Peñas C., Arendt-Nielsen L., Gerwin R. (Eds): Jones & Bartlett, Boston.
Alternative explanations
So if PIR and RI are not the neurophysiological mechanisms that lead to the effectiveness of MET, in increasing joint ROM, or extensibility of soft tissues, and analgesia, what does produce these results?
The phrase ‘increased tolerance to stretch’ has emerged to describe what happens, although it does not explain how it happens.
• At its simplest this explanation observes that if, after an isometric contraction, the same degree of effort is used, as was employed to take the muscle or joint to its end of range, before the contraction, no increase in range or extensibility occurs.
• Magnusson et al (1998, 1996b) measured the degree of applied effort used during passive knee extension, before and after the hamstrings were stretched to the point of pain. They found that both ROM and passive torque were increased following the contraction – because subjects were able to tolerate a stronger stretch.
• Ballantyne et al (2003) confirmed these findings by showing that when the degree of post-test force applied to the muscle remained constant (i.e. the same as used in pre-testing), no change in length took place, suggesting that a single application of MET created a change in tolerance to stretch.
• Fryer (2006) explains: ‘The application of MET would appear to decrease an individual’s perception of muscle pain, and is greater than that which occurs with passive stretching. Stretching and isometric contraction stimulate muscle and joint mechanoreceptors and proprioceptors, and it is possible that this may attenuate the sensation of pain. … MET and stretching appear to produce lasting changes in stretch tolerance, and so the mechanism is likely to be more complex than just gating at the spinal cord, and may also involve changes in the higher centres of the CNS.’
• Hamilton et al (2007) suggest that techniques – such as MET – that stimulate joint proprioceptors, via the production of joint movement, or the stretching of a joint capsule, may be capable of reducing pain by inhibiting the smaller diameter nociceptive neuronal input at the spinal cord level.
What else might produce MET’s analgesic effects?
Brodin (1982), Cassidy et al (1992) and Wilson et al (2003) have all reported that there is a reduction in spinal pain, following application of MET. These reports therefore support the evidence described above, of an increased tolerance to stretch, of muscles treated by MET.
• Degenhardt et al (2007) report that concentrations of several circulatory pain biomarkers (including endocannabinoids and endorphins) were altered following osteopathic manipulative treatment incorporating muscle energy, and other soft tissue techniques. The degree and duration of these changes were greater in subjects with chronic LBP than in control subjects.
• McPartland (2008) and others (Pertwee 2005, Agarwal & Pacher 2007) note that the endocannabinoid (eCB) system, like the better-known endorphin system, consists of cell membrane receptors, endogenous ligands and ligand metabolizing enzymes. Two cannabinoid receptors are known:
Two of the eCB ligands, anandamide (AEA) and 2-AG, are mimicked by cannabis plant compounds. McPartland reports that: ‘AEA and 2-AG are not stored in vesicles like classic neurotransmitters. Rather they are synthesized “on demand” from precursor phospholipids in the neuron cell membrane and immediately released into the neural synapse. (Pertwee 2005). The eCB system dampens nociception and pain, and decreases inflammation in myofascial tissues.’
• Agarwal & Pacher (2007) suggest that cannabinoids mediate analgesia largely via peripheral type 1 cannabinoid receptors (CB1), in pain receptors.
Alternatives to standard isometric contraction versions of MET
• An isotonic eccentric stretch is one in which the practitioner overcomes the effort of the contracting muscle, stretching and simultaneously toning it (Liebenson 2006, Norris 1999, Kolar 1999).
• A rapid isotonic eccentric contraction, the origin and insertion of the muscles involved are taken further apart while the muscle is contracting, due to the greater effort of the practitioner’s counterforce overcoming the muscular effort. When such a manoeuvre is performed rapidly, it is known as an isolytic contraction. Isolytic stretches are useful in cases where a marked degree of fibrotic change is present in the soft tissues. The effect is to create microtrauma during the rapid stretch, subsequently allowing an improvement in elasticity and circulation. To achieve an isolytic contraction (eccentric isotonic), the patient should be instructed to use no more than 20% of possible strength on the first contraction, which is resisted and overcome by the practitioner, in a contraction lasting 2–3 seconds. This is then repeated, but with an increased degree of effort on the part of the patient (assuming the first effort was relatively painless). This continuing increase in the amount of force employed in the contracting musculature may be continued until, hopefully, a fairly strong but painless contraction effort is possible, again to be resisted and overcome by the practitioner. In some muscles, of course, this may require a heroic degree of effort on the part of the practitioner, and alternative methods would need to be found. NMT would seem to offer one such alternative. The isolytic manoeuvre should have as its ultimate aim a fully relaxed muscle, able to reach its normal resting length. This will seldom be possible in one treatment session.
•A slow isotonic eccentric contraction offers various important clinical benefits (Lewit 1999, Liebenson 2001, Norris 1999): To tone postural (type I) muscles that may have lost their endurance potential, a slow isotonic eccentric contraction should be performed, involving increasing degrees of effort. For example, slowly overcome flexion of the wrist forcing it into extension (i.e. the arm flexors, which are postural type I muscles, are stretched while contracting). To relax hypertonic postural (type I) muscles, a slow isotonic eccentric stretch should be performed of their inhibited antagonists (using 40–80% strength). For example, slowly overcome the extended wrist, forcing it into flexion (i.e. the arm extensors, which are phasic type II muscles, are contracting but their effort is overcome).
• A concentric isotonic contraction tones the muscle that is active.
• Ruddy (1961) suggested that the effects of what he termed rapid resisted duction (i.e. pulsed isometric contractions) include improved local oxygenation, enhanced venous and lymphatic circulation, as well as an improved static and kinetic posture, due to the effects on proprioceptive and interoceptive afferent pathways.
• These variations, along with their particular influences, appear to produce identical benefits in terms of increased ROM and extensibility of soft tissues irrespective of which form of MET methodology is employed. For example, in a study of the use of MET in treatment of piriformis dysfunction, it was found that the same results emerged whether the agonist or the antagonist was used in the contraction phase of ME usage (Wright & Drysdale 2008). (See Figs 8.7A,B.)
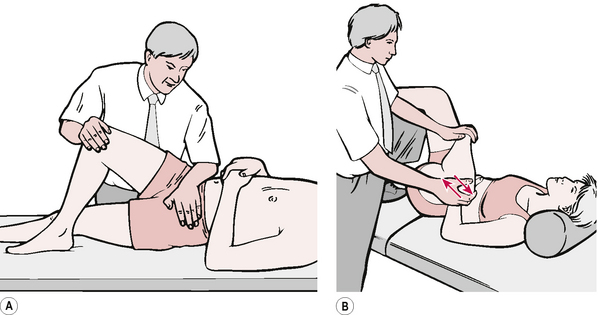
Figure 8.7 Fig. 8.7A shows MET treatment of piriformis using an antagonist contraction. Fig. 8.7B shows MET treatment of piriformis using a stretch following an antagonist contraction.
Update on stretching time in MET
Smith & Fryer (2008) tested the usefulness of extending a hamstring muscle stretch, following a MET Contraction, from 5 seconds (Greenman 1996) to 30 seconds (Chaitow 2002):
Both techniques appeared to be equally effective in increasing hamstring extensibility, and there appeared to be sustained improvement 1 week following the initial treatment. The findings suggest that altering the duration of the passive stretch component does not have a significant impact on the efficacy of MET for short-term increases in muscle extensibility…. both these post-isometric techniques were superior to passive stretching in this group of subjects.
Comment: The study referred to above involved healthy individuals. It may still be the case that sustained (up to 30 second) stretches would be clinically more useful, when treating chronically shortened tissues.
Neuromuscular therapy (soft tissue manipulation)
The term ‘soft tissue manipulation’ (STM) is frequently used to incorporate all manual methods (including massage) that address tissues other than bone, and this phrase (STM) appears to be interchangeable with the term Neuromuscular Therapy, as described by DeLany, in Chapter 10 (as distinct from Neuromuscular Technique – which describes Lief’s approach, explained in detail in Chapter 6).
Neuromuscular therapy therefore incorporates Neuromuscular technique, myofascial release, connective tissue massage, muscle energy techniques and positional release methods (e.g. strain/counterstrain).
These can (with other modalities such as chilling agents), all be used as effective measures to detect, and help normalize, dysfunctional soft tissues, including areas housing noxious trigger points, which can themselves be associated with, and at times be responsible for, the promotion or maintenance of muscular weakness, muscular contraction, pain, vasodilatation, vasoconstriction, tissue degeneration, gastrointestinal, respiratory and a myriad other disorders, including emotional and ‘psychological’ disorders (Baldry 1993, Lewit 1999, Simons et al 1999).
The logical approach to correction of dysfunction involving shortened tight musculature, or weak inhibited musculature, is to identify the reasons for the dysfunction, and to address these. Local application of STM methods then become palliative, as well as creating an environment where more constitutional approaches (postural re-education, for example) can be more effectively achieved.
Is there a ‘correct’ sequence of therapy?
Treatment of dysfunction associated with muscles that have become weakened could involve initial attention to their overtight antagonists, which may be inhibiting them, as well as to isotonic concentric MET methods applied to the weakened muscles, plus exercises specific to the area.
Possible joint influences on dysfunctional soft tissues should be addressed, either through mobilization or, in instances where true joint blockage exists, by active (high-velocity thrust) manipulation.
It is a contention of many practitioners who work with somatic dysfunction that in most instances soft tissue normalization leads to joint normalization; however, the reverse is not a rarity, and at times the joint restriction is the primary feature in an area involving soft tissue dysfunction (Lewit 1996, 1999, Chaitow 2008). General postural re-education and body-toning exercises could follow.
Before such exercise is initiated, however, it is important to discover and treat local dysfunction within shortened or weakened muscles – such as trigger points – and NMT will usefully help towards achieving this.
It is often useful to allow the results of normalization of shortened muscles to unfold without confusing the issue by focusing on the weakened antagonists too soon, as a natural toning effect will occur when inhibitory influences are removed.
If, after several weeks of treatment (and possibly home stretching) of the shortened, contracted, postural muscles and their trigger points, there is not an observable and measurable improvement in the weak antagonists, then MET and exercise could usefully be introduced to these as well.
The use of gentle functional techniques, such as strain/counterstrain, is suitable for combining with NMT and MET methods.
By using MET to help to lengthen shortened structures, and NMT to aid in this, as well as in identifying localized areas of soft tissue dysfunction (myofascial trigger points or other forms of soft tissue dysfunction), the practitioner has a wide range of diagnostic and therapeutic methods, literally at his or her fingertips. Correct sequencing will be individual, but requires a correct (or at least reasonable) understanding of the causes of the dysfunction, so that treatment takes account of local and bodywide biomechanical influences (posture, breathing patterns, etc.), as well as psychosocial and lifestyle features (nutrition, exercise, sleep, etc.).
Percussion technique or spondylotherapy
For soft tissue treatment
Trigger points can be treated effectively using a series of percussive strokes according to Travell & Simons (1992):
1. The muscle is lengthened to the point of onset of passive resistance.
2. The clinician or patient uses a hard rubber mallet or reflex hammer to hit the trigger point at exactly the same place approximately 10 times.
3. This should be done at a slow rate of no more than one impact per second, but at least one impact every 5 seconds; slower rates are likely to be more effective.
Travell & Simons suggest that this enhances, or substitutes for, intermittent cold with stretch (‘spray and stretch’) methods, as described above.
The muscles that they list as benefitting most from percussion techniques include quadratus, brachioradialis, long finger extensors and peroneus longus and brevis.
Caution – It is specifically suggested that anterior and posterior compartment leg muscle should not be treated by percussion, owing to the risk of compartment syndrome, should bleeding occur in the muscle.
TCM percussion
In recent years, Chinese methods involving percussion have added dramatically to our knowledge of the potential of these methods (Zhao-Pu 1991). In traditional Chinese medicine (TCM), percussion methods are incorporated into a broad heading of ‘acupressure’.
Acupressure is based on the same theory as acupuncture and uses the same points and meridians … the therapeutic effect of acupressure technique lies in the way in which it regulates and normalises blocked functions.
Included in these functions (as well as hypothesized energy transmission) are, ‘stimulating circulation of blood … and improving conductivity of nerves.’
In TCM, percussion techniques involve one of three variations (Fig. 8.8):
1. One-finger percussion, using the middle finger braced by the thumb and index finger.
2. Three-finger percussion, using the thumb, index and middle fingers.
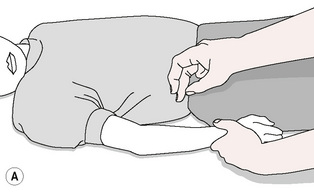
Figure 8.8A One-finger percussion uses middle finger braced by thumb and index finger.
Redrawn from Zhao-Pu (1991), with permission.
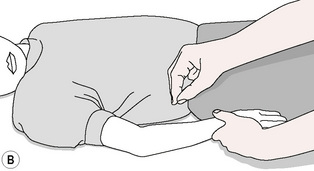
Figure 8.8B Three-finger percussion uses thumb, index and middle finger.
Redrawn from Zhao-Pu (1991), with permission.
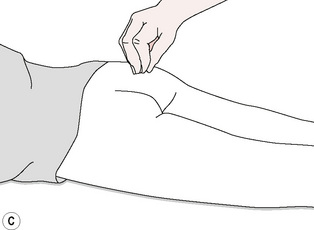
Figure 8.8C Five-finger percussion uses thumb and all fingers.
Redrawn from Zhao-Pu (1991), with permission.
The degree of force applied during percussion is also of three types:
1. Light, which involves a movement of the hand from the wrist joint
2. Medium, which involves a movement from the elbow joint with wrist fairly rigid
3. Strong, which involves a movement of the upper arm, from the shoulder, with a rigid wrist.
Treatment is offered daily, on alternate days or once every 3 days, and a course would involve 20 sessions. Patients often receive three courses or more.
Professor Wang Zhao-Pu (whose work using this approach was based on his extensive experience as an orthopaedic surgeon) describes remarkable clinical results involving patients with paralysis and cerebral birth injuries.
He states (Zhao-Pu 1991):
Research was carried out on the cerebral haemodynamics of patients with cerebral birth injury before and after acupressure (percussion and pressure techniques) therapy. Scanning techniques were used in monitoring the short half-life radioactive materials through the cerebral circulation; in almost one-third of the patients the regional cerebral blood flow was increased after acupressure therapy ranging from 28 to 60 sessions.
In an introduction to Zhao-Pu’s book, Graeme Schofield states:
After cerebral birth injury, significant though the damage may be, there are large areas of the brain and many millions of nerve cells which are still intact. These areas and the cells they contain are the targets of education for future living.
This approach is, therefore, not one that produces instant results, but that influences and gradually harnesses the potential for recovery and improvement that is latent in the tissues of the patient. For more information on oriental bodywork approaches, a complete manual of Chinese therapeutic massage (with many aspects that echo NMT methodology) edited by Sun Chengnan is highly recommended (Chengnan 1990).
Western percussion
In order to stimulate organs via spinal pathways, direct percussion techniques have long been employed by osteopathic and chiropractic practitioners.
Over the past century in the USA, a number of mechanical methods of percussion has evolved (Abrams 1922), as have effective manual systems in which the middle finger is placed on the appropriate spinous process(es) while the other hand concusses the finger with a series of rapidly rebounding blows. This approach is known as spondylotherapy (Johnson 1939) (see Fig. 8.9). One or two percussive repetitions are applied per second. Spondylotherapy percussion is usually applied to a series of three or four (or more) adjacent vertebrae.

Figure 8.9 Percussion technique (spondylotherapy) for reflexive effects or treatment of trigger points (slow percussion).
Examples
• An example of this is the treatment, as above, of the 5th thoracic spinous process, proceeding downwards to the 9th, in the case of liver dysfunction. Treatment would be applied only if the area were painful to palpating pressure.
• Similarly, concussion over the 10th, 11th and 12th thoracic spinous processes would stimulate kidney function.
In order to stimulate an organ, or tissues, using the spinal reflexes, percussion can involve only a short amount of time: 15–30-second applications repeated three or four times, over approximately 4–5 minutes. A mild ‘flare up’ of symptoms and increased sensitivity in the area treated suggests that the desired degree of stimulation had been achieved. In order to inhibit function or to produce dilatation of local blood vessels, Johnson (1939) suggested that percussive repetitions be repeated for prolonged periods, to fatigue the reflex.
Manual spondylotherapy complements NMT because of its reflex influences and its ease of application. A sound knowledge of spinal mechanics and neurological connections is a prerequisite to its usage, which is based on anecdotal and experiential data, rather than any research validation.
Piriformis muscle technique (Retzlaff et al 1974, Wright & Drysdale 2008)
The piriformis muscle syndrome results from contraction of the muscle either due to trauma or repetitive mechanical or postural stress, or due to the presence in the muscle of active trigger points. The effects of piriformis shortening can be circulatory, neurological, reflex or functional, inducing pain and paraesthesia of the affected limb as well as alterations to pelvic and lumbar function, as the muscle anchors the sacrum to the femur. Diagnosis usually hinges on the absence of spinal causative factors for the symptoms.
Piriformis muscle syndrome is frequently characterized by such bizarre symptoms that they may seem to be unrelated. One characteristic complaint is a persistent, severe, radiating low-back pain extending from the sacrum to the hip joint, over the gluteal region and the posterior portion of the upper leg and down to the popliteal space. In the most severe cases the patient will be unable to lie or stand comfortably, and changes in position will not relieve the pain. Intense pain will occur when the patient sits or squats.
A common sign of the piriformis syndrome is a persistent external rotation of the upper leg. This indication, which is known as the positive piriformis sign, is easily detected when the patient is examined in the supine position.
The buttock on the same side as the piriformis lesion is usually sensitive to touch or palpation. Severe pain may occur when pressure is applied to the area over the piriformis muscle and its tendinous insertion on the head of the greater trochanter.
Another diagnostic sign may be the shortening of the leg on the affected side due to contraction of the piriformis muscle. In cases where the leg on the opposite side appears shortened, it is probable that some other dysfunction exists, and that the condition is not directly related to the piriformis syndrome.
The patient may also mention pain that follows the distribution pattern of the sciatic nerve to the level of the popliteal space and sometimes to the more distal branches of this nerve. When the common perineal nerve is involved, there may be a paraesthesia of the posterior surface of the upper leg and some portions of the lower leg.
One of the most perplexing problems arising from the piriformis syndrome is the involvement of the pudendal nerve and blood vessels. This nerve, with its branches, provides the major sensory innervation of the perineal skin and the somatic motor innervation of much of the external genitalia and related perineal musculature in both women and men, with the pudendal blood vessels supplying essentially the same areas.
The pudendal nerve, after passing through the greater sciatic foramen, re-enters the pelvis by way of the lesser sciatic foramen. In a significant proportion of people, the perineal and tibial components of the sciatic nerve actually pass through the piriformis muscle, giving rise in these individuals to a greater likelihood of severe symptoms if the muscle shortens or is stressed (Polstein 1991). Compression of the pudendal nerve and blood vessels can result in serious problems involving the functioning of the genitalia in both sexes. Since external rotation of the upper legs is required for women during coitus, if there is interference with the blood supply and innervation of the genitalia, it is understandable that a female patient might complain of pain during sexual intercourse. This could also be a basis for impotency in men. Ischaemic compression, applied by thumb or elbow, together with stretching of the muscle to its normal resting length (with or without MET), is usually sufficient to remedy the problem.
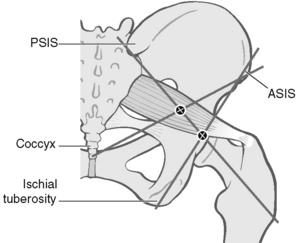
Precise localization of piriformis trigger points/landmarks
The patient is side-lying, tested side uppermost. The practitioner stands at the level of the pelvis in front of, and facing, the patient and, in order to contact the femoral attachment of piriformis, draws imaginary lines between:
Where these reference lines cross, just posterior to the trochanter, is the insertion of the muscle, and pressure here will produce marked discomfort if the structure is short or irritated.
If the most common piriformis trigger point site, in the belly of the muscle, is sought, then the line from the ASIS should be taken to the tip of the coccyx rather than to the ischial tuberosity.
Pressure where this line crosses the other will access the midpoint of the belly of piriformis, where triggers are common. Light compression here, that produces a painful response, is indicative of a stressed muscle and possibly an active myofascial trigger point (Fig. 8.10).
Piriformis treatment
Piriformis method 1
1. The patient is side-lying, close to the edge of the table, affected side uppermost, both legs flexed at hip and knee.
2. The practitioner stands facing the patient at hip level.
3. The practitioner places his or her cephalad elbow tip gently over the point behind trochanter, where piriformis inserts, or on to the central area of the muscle belly, where an active trigger point is common.
4. The patient should be close enough to the edge of the table for the practitioner to stabilize the pelvis against his or her trunk (see Fig. 8.11).
5. At the same time, the practitioner’s caudad hand grasps the ankle and uses this to bring the upper leg/hip into internal rotation, taking out all the slack in piriformis.
6. A degree of inhibitory pressure (sufficient to cause discomfort but not pain) is applied via the elbow for 5–7 seconds while the muscle is kept at a reasonable but not excessive degree of stretch.
7. The practitioner maintains contact on the point, but eases pressure, and asks the patient to introduce an isometric contraction (25% of strength, for 5–7 seconds) to piriformis by bringing the lower leg towards the table against resistance, attempting to rotate the hip externally.
8. After the contraction ceases, and the patient relaxes, the lower limb is taken to its new resistance barrier, and elbow pressure is reapplied.
9. This process is repeated until no further gain is achieved (usually 5 to 7 repetitions of the sequence).
This method is a variation on the method advocated by Te Poorten (1969), which calls for longer and heavier compression, and no intermediate isometric contractions.
Piriformis method 2
1. In the first stage of this alternative method, the patient lies on the non-affected side with knees flexed and hip joints flexed to 90°.
2. The practitioner places his or her elbow on the piriformis musculotendinous junction and a steady pressure of 20–30 lb (9–13 kg) is applied.
3. With the other hand, the practitioner abducts the foot so that it will force an internal rotation of the upper leg.
4. The leg is held in this rotated position, at its elastic barrier, for periods of up to 2 minutes.
5. This procedure is repeated two or three times.
6. The patient is then placed in the supine position and the affected leg is tested for freedom of both external and internal rotation.
Note: See also, earlier in this chapter, Figs 8.7A and B for alternative piriformis treatments, using MET.
Proprioceptive adjustment (applied kinesiology)
(Figs. 8.12 & 8.13) (Walther 1988)
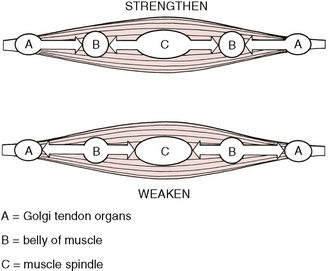
Kinesiological muscle tone correction utilizes two key receptors in muscles to achieve its effects. These are the muscle’s spindles responsible for reporting on muscle length and changes in length, and the Golgi tendon organs that report on the load on, or tension of, the muscle (see Fig. 8.13).
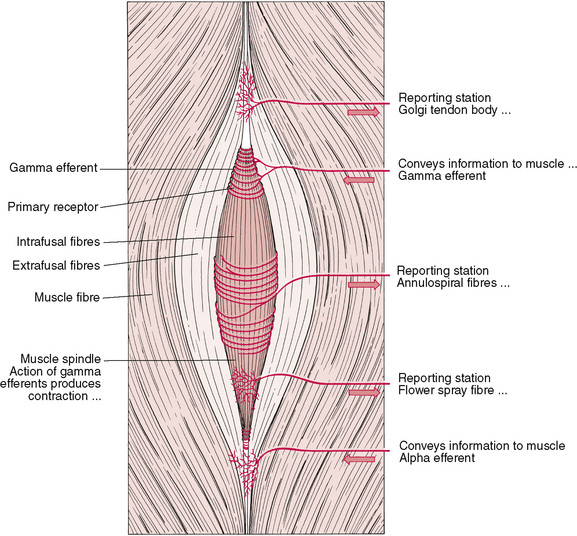
Figure 8.13 Illustration of muscle spindles, showing Golgi tendon organ and neural pathways to and from these reporting stations.
A muscle in spasm may be helped to relax by the application of direct pressure (using 1–7 kg (2–15 lb) of pressure:
• away from the belly of the muscle, in the area of the Golgi tendon organs – and/or
• application of the same amount of pressure towards the belly of the muscle, in the area of the muscle spindle cells (see Fig. 8.12).
The precisely opposite effects (i.e. toning or strengthening the muscle) are said to be achieved by applying pressure:
• away from the belly of the muscle, in the muscle spindle region and/or
• towards the belly of the muscle in the Golgi tendon organ region.
Note that Janda (1990, 1992), in particular, has taught that weakness in a muscle can best be addressed by dealing with hypertonicity in its antagonist(s) – as a primary goal (via stretching, etc.).
• Strength can also be restored to a muscle by slowly stretching it during an isotonic eccentric contraction (which will simultaneously reduce tone in hypertonic antagonist).
• Or, strength can be restored to a muscle by slowly contracting it concentrically against resistance.
(See section on Muscle energy techniques, earlier in this chapter.)
Psoas techniques
In postural distortion, such as scoliosis, or marked lumbar lordosis, as well as in many acute low back and sciatic cases, the iliopsoas muscle is found to be involved (Lewit 1996, 1999).
Contraindications to methods listed below:
• aortic disease (e.g. aneurism, calcification)
• inflammatory bowel or pelvic disease
• pain on application of palpatory pressure, as described below.
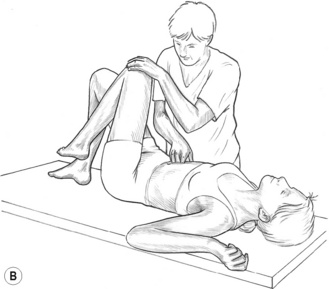
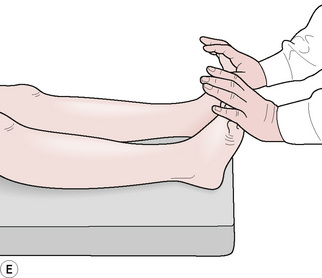
Test for psoas shortness
A simple test involves the patient lying at the end of the bed with the unaffected (non-tested) side leg in full flexion at hip and knee, and the tested leg hanging freely.
• If the thigh is parallel with the floor/table, and has sufficient flexibility to allow for an easy depression into slight extension (10º or so), the iliopsoas is considered normal.
• However, if it is elevated, or is parallel with the floor but has no ‘give’ when pushed lightly into extension, shortness is presumed.
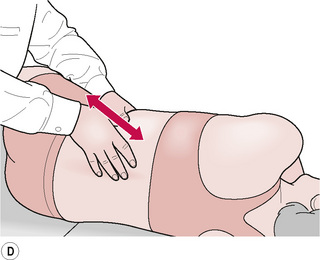
Psoas technique – direct inhibitory pressure
Method (a)
1. The patient lies supine with knees flexed, hands at side.
2. The practitioner stands on the side opposite the contracted psoas.
3. One hand presses down firmly through the linea alba, 3–4 inches (7–10 cm) below the umbilicus, until the gently probing fingers contact the body of the 4th to 5th lumbars.
4. The practitioner then eases fingers over the curved anterior surface of the lumbar body, towards the contralateral side, until the attachment of psoas is located.
5. Firm but gentle pressure is maintained for about 1 minute (Fig. 8.14A,B).

Method (c)
1. Same as method (a), except practitioner places flexed leg on the table to support the patient’s leg on contracted psoas side.
2. In this way both hands are free to support each other as they penetrate heavier abdomens (Fig. 8.14C).
Method (d)
1. Same as method (a), except practitioner’s flexed leg supports both of the patient’s legs.
2. This is especially useful when there is a contraction of both psoas muscles (Fig. 8.14D).
Instead of accessing psoas directly through the linea alba, an oblique contact to the belly of the muscle can be made by applying fingertip pressure towards the spine from the lateral border of rectus abdominis (not illustrated).
In addition, during any of the methods described above, MET may be used by having the patient briefly contract the muscle against resistance (‘bring your knee gently toward your face’), after which easier access, and a more relaxed muscle, should be noted. Additional tactics include having the patient slowly lengthen (extend) and flex the hip, while direct pressure is maintained on the attachment, or the belly, or psoas (‘pin and stretch’).
Note: To apply the methods, as described, the practitioner should stand contralaterally when using the linea alba access, and ipsilaterally when applying the oblique access contact.
A number of additional MET and strain/counterstrain approaches exist for safely treating psoas, and appropriate texts should be consulted for details of these (Chaitow 2006, 2008).
Pectoralis minor release for general upper thoracic mobilization
Release of pectoralis minor by the means described below has been clinically shown to produce an increased range of movement for the upper ribs, and a consequent increase in thoracic volume (Wallace et al 1997).
This allows subsequent pump techniques (see below) to be applied more effectively.
Kuchera & Kuchera (1994) note that ‘a one centimeter increase in the diameter of the chest increases air intake by 200 to 400cc’.
The effect on lymphatic drainage is profound, because the pumping action involved in the breathing process impacts directly on lymph motion. Kuchera & Kuchera (1994) also note:
This is an efficacious technique that can be used with relative ease with patients with brittle bones, with patients in the intensive care unit, where multiple tubes and monitoring devices may be in place, and with post-surgical patients.
In other words, it is a safe procedure!
Method for pectoralis minor release
• The patient is supine with the arms comfortably at the side.
• The practitioner, while standing at the head of the table, places the palms of the hands (having ensured nails are well clipped) into the axilla, palms touching the medial humerus, thumb side of index fingers touching the axilla.
• In this way the dorsa of the fingers are located under the lateral border of each pectoralis minor.
• The practitioner then slowly externally rotates the arms and, using gentle pressure, insinuates fingertips under the lateral border of the muscle.
• The hands, the palms of which are now facing medially, are then drawn lightly toward each other (medially) until all the slack in pectoralis minor has been removed (Fig. 8.15).
• The practitioner’s hands then slowly, deliberately and painlessly lift the tissues towards the ceiling, to their elastic barrier, easing the muscle away from its attachments, until all slack has been removed (i.e. no actual stretching is taking place at this stage, merely a removal of all slack).
• The practitioner should then transfer body weight backwards to introduce a lean, which removes the slack further, by tractioning the muscles in a superior direction (toward the head).
• The muscle fibres will now have been eased medially, anteriorly and superiorly, and should be held at these combined barriers as they slowly release over the next few minutes.
• During this period the patient should be requested to breathe deeply and slowly.
• If correctly applied, this procedure should not be painful.
Hruby & Hoffman (2007) note: ‘The combination of traction and respiratory motion releases the upper anterior thoracic muscle tension.’
Pump techniques – lymphatics, liver/spleen, pedal
Indications for the use of lymphatic pump techniques include all conditions that involve congestion, lymphatic stasis and infection (apart from those listed under ‘Contraindications’).
Wallace et al (1997) report:
Lymphatic pump techniques are designed to augment the pressure gradients that develop between the thoracic and abdominal regions during normal respirations.
The benefits of enhanced lymphatic movement – encouraged by the various techniques described in this section – include (Wallace et al 1997, Knott et al 2005, Sleszynski and Kelso 1993, Hruby & Hoffman 2008):
• increased resorption of fluids
• increased circulation and respiration
• decreased proteins in the interstitium
• facilitation from a more beneficial pH balance
• increase of white blood cell count in peripheral blood (spleen pump)
• increase of lymph flow through the thoracic duct – without changes in mean arterial pressure, heart rate or cardiac output.
Caution – It is important to make sure that the patient has no food, chewing gum or loose dentures in the mouth when these procedures are being applied.
Contraindications to pump techniques:
• malignant or other serious diseases of the lungs, liver, spleen or associated organs
• recent abdominal or thoracic surgery
• fracture, dislocation or other painful dysfunction involving the joints of the thoracic cage or spine
• avoid thoracic pump techniques where the patient has a reduced cough reflex.
Lymphatic pump method (a) – prone
1. Patient is prone, pillow under chest, arms over the side, with the practitioner standing at the head of the table, facing caudad.
2. The practitioner’s thumbs are pressed, bilaterally, onto the intertransverse spaces, starting at the base of the neck (Fig. 8.16A).
3. Pressure is exerted towards the floor as the patient swings the arms slowly forwards (so that arms lie alongside the head at the end of the swing), and simultaneously inhales deeply.
4. On exhalation (slow) the arms are swung slowly down until they lie alongside the trunk.
5. This process of arm movements, linked to inhalation/exhalation, is repeated as the thumbs move down one intervertebral space.
6. This will have a stimulating effect on the lymphatic drainage of the body as a whole.
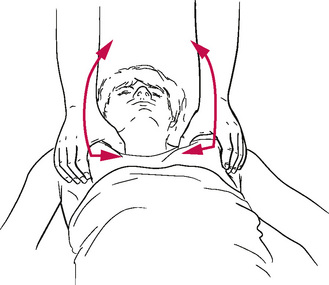
Lymphatic pump method (b) – supine (Sleszynski & Kelso 1993, Wallace et al 1997, Hruby & Hoffman 2008)
1. The patient lies supine, knees and hips flexed.
2. The practitioner is at the head of the table with hands spread across the patient’s chest, with thenar eminences just inferior to the clavicles, with thumbs resting next to each other on the sternum, fingers spread laterally. The arms should be more or less straight for ease of transmission of force from the shoulder to the hands.
3. Rhythmic pumping pressure is introduced by the practitioner, in a downward and caudad direction, which is just sufficient to overcome resistance, by means of a repetitive, minimal, flexion and extension of the elbows.
4. The patient should breathe through the mouth during the treatment and should not resist the repetitive pressure applied by the practitioner, at a rate of 100 and 120 per minute (Fig. 8.16B).
5. This should continue for at least 3 minutes, and for up to 5 minutes.
In babies, the method can be used with one hand over the sternum, the other under the spine, with the baby cradled or seated on the practitioner’s lap. The effect of this is to improve lymphatic drainage markedly.
This method is useful in all cases of oedema and infection. It also has a beneficial effect on immune function (Hoag 1969).
Treatment using Chapman’s reflexes (see Ch. 4) provides additional localized drainage, which supports the general drainage and stimulation of lymphatic function (Washington et al 2003, Owen 1977).
Lymphatic pump method with activating breath (c) – supine
1. The patient, practitioner and the hand positions are as in method (b) above.
2. The patient inhales and exhales fully through an open mouth.
3. As the patient exhales, the practitioner, elbows straight, encourages exhalation by applying pressure to the upper thorax, and maintains the degree of compression achieved at the full exhalation.
4. This process is repeated three or four times, with the degree of sustained compression increasing slightly after each exhalation (i.e. the patient commences each subsequent breath with the upper chest held in compression).
5. Approximately a third to a half of the way through the fourth or fifth inhalation, as pressure builds up against the restraining hands following a request to ‘breathe deeply’, the hands should be removed extremely rapidly, releasing pressure from the chest. A vacuum will have been created and a sound of in-rushing air should be heard. A byproduct of this should be a major shift in lymphatic movement.
Note: Liver and spleen pump techniques are identical, apart from the fact that the spleen is located on the left side of the body and the liver on the right.
Liver/spleen pump method (a) – supine
1. A simple measure, via which function of either the liver or the spleen may be enhanced, involves the practitioner standing on the side opposite the organ that is being stimulated (left side of patient, reaching across for the liver, and vice versa for the spleen).
2. The patient is supine, knees and hips flexed, and the practitioner’s caudad hand is placed under the lower ribs, and the other is placed anteriorly, just medial to the costal cartilages of the lower five ribs (Fig. 8.16C).
3. Bimanual compression should initially be carried out in a direct anterior–posterior direction, in a rhythmic manner in which the hands squeeze the tissues together approximately 20 times per minute, for 1–2 minutes.
4. After this, the direction of the pumping action should be in a more anterolateral direction, for a further minute.
5. The effect, when this is applied to the spleen rather than the liver, is to increase the leucocyte count by an average of 2200 cells per cubic millimetre (Castlio 1955, Wallace et al 1997).
Liver/spleen pump method (b) – side-lying
1. The patient is sidelying with the practitioner standing at hip level, facing the head.
2. The practitioner places both hands on the lower thoracic cage, one hand anterior and the other posterior, thumbs meeting on the axillary line.
3. The patient inhales deeply, and as she exhales the practitioner applies a cephalad directed pressure, combined with a vibratory action, with both hands, to induce a pumping action on the liver (see Fig. 8.16D).
Pedal lymphatic pump method
1. The physician stands at the feet of the supine or prone patient.
2. The practitioner introduces a force that dorsiflexes the feet past neutral, and then releases the pressure, while still holding the feet as they return to neutral.
3. Use the umbilicus to gain a sense of the wave-like motion that develops via the rebound (see Fig. 8.16E).
4. As the rebound wave reaches the feet, a dorsiflexion force is reapplied, repeating the process, and creating an oscillatory pump-action.
Skin techniques
Skin rolling
Skin rolling (see Figs 8.17 and 5.5) is a useful all-purpose approach that involves the use of either or both hands. It can be used for assessment (Jay 1995), as well as for treatment. For example in assessment, Taylor et al 1990) report that: ‘The skin roll technique provides an accurate indication of local areas of decreased pain threshold, along the dorsal spine … [as] … a correlation between tender skin roll areas and spinal joint dysfunction (fixations) does exist’
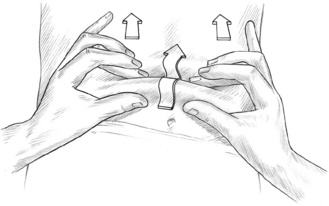
Therapeutically skin rolling is used as a companion approach to Connective Tissue Massage/ Manipulation, as described in Chapter 5.
Method
The fingers draw tissue towards the practitioner, whilst the ball(s) of the thumb(s) roll over the gathered mound of tissue. In this way the tissue is effectively lifted, stretched and squeezed.
The most useful areas of application occur where the tissues lie tight to the underlying structures, such as directly over the shoulder joint and on the lateral aspect of the thigh. The squeezing pressure imparted by the roll of the thumb can be extremely uncomfortable, and care should be exercised during its application.
The angle of stretch, pull and roll may be varied and repeated several times to impart maximum stimulus to the reflex effects and to stimulate circulation and drainage.
The degree of stretch and/or pinch employed during rolling of the tissues is a variable factor that the practitioner may decide upon, depending upon the amount of stimulus called for. Either skin alone, or skin and underlying tissue, may be lifted, stretched and stimulated (pinched) in this way.
Stanley Lief and Boris Chaitow employed this simple, yet effective, manoeuvre as part of their general treatment. The latter described its usefulness as follows (Boris Chaitow ND DC, personal communication, 1983):
One of my favourite techniques to enhance nerve and blood circulation is ‘skin rolling’. Between the skin and the muscular and bony structures it covers, is a veritable network of blood and nerve structures and functions which can, and often do, fail to achieve their full, effective circulation for high efficiency and health because the skin is often so adhered to its lower structures (fascia) that circulation and function is appreciably reduced. This of course adversely affects the efficiency and health of the patient. There is probably no formula that will enhance this aspect of function more effectively than ‘skin rolling’. A specific example of its effective benefit is to skin-roll a major joint such as a shoulder in conditions of articular rheumatism, arthritis, neuritis or frozen shoulder.
Note: Traditional Chinese medicine calls for this procedure to be undertaken, working from the base of the spine upwards, for a tonifying effect, and from the neck downwards, for a sedating effect.
Hyperalgesic skin zones
As noted in earlier chapters, the skin overlying regions or points of reflex activity (such as myofascial trigger points and their referral areas) will frequently be found to have markedly reduced elasticity and to adhere to underlying structures (see Fig. 5.6 and the text that discusses assessment of these areas – including those associated with scars – in Chapter 5) and to be areas of increased sensitivity – hyperalgesic skin zones (HSZs).
Such zones are common in many musculoskeletal conditions, and in chronic pain syndromes. In cases of recurrent headache, HSZs may be found medially below the mastoid process, at the temples and eyebrows, and/or on the forehead above the eyebrows, and on both sides of the nose. These areas correlate with many of Bennett’s neurovascular reflexes, as discussed in earlier chapters.
Some confirmation of the possible neurovascular nature of these areas comes from Ali et al (2000). They conducted studies to evaluate some of the mechanisms associated with HSZs, by injecting norepinephrin (NE), into tissues of individuals with characteristic sympathetically mediated pain (SMP), and concluded that:
NE injections produce pain in SMP patients at doses that are at the threshold for producing vasoconstriction. These studies support a role for cutaneous adrenoceptors in the mechanisms of sympathetically maintained pain.
By altering the degree of hypertonicity, and enhancing local circulation, by methods such as skin rolling (above), or the methods discussed below, hyperalgesia can be modulated by manual therapy. Underlying aetiological factors, of course, also require attention to prevent recurrence.
Stretching, to release overlying tissues of HSZs (Lewit 1992)
1. To treat a hyperalgesic area, the fingertips (for a small area) or the ulnar aspects of the crossed hands (for a larger area) are placed together on the skin surface overlying the affected area.
2. The tissues should then be gently stretched apart, to their easy resistance barrier, as the fingers, or hands, separate.
3. To establish the presence, or lack of, physiological elasticity, the skin would be stretched in various directions.
4. When restriction is noted, the tissues are held in a painlessly stretched position until a degree of release is noted. This commonly takes 10–20 seconds.
5. The same area may be stretched in this manner in various directions, each time being held at its barrier of resistance until a release occurs (see Fig. 5.7A,B).
6. The release of the tissues is itself the therapeutic effort, providing reflex stimulus to underlying structures.
7. The subsequent maintenance of the free elastic state of the tissues is evidence of an improvement in the causative factors. Naturally, if underlying factors maintain the reflex activity, whether this be musculoskeletal or visceral dysfunction, the improvement will be short-lived.
In this way HSZs are used both diagnostically, and prognostically.
Lewit (1992) states:
Treating overlying tissues of HSZs – positional release
1. The practitioner places a contact (finger pad(s) or whole hand) onto the skin, which appears less pliable, more adherent (to underlying fascia; see Ch. 5), or palpates as ‘different’ to, or more sensitive than, surrounding tissues, suggesting that it is a HSZ.
2. The contact hand or finger pad(s) should slide the skin superiorly and inferiorly, medially and laterally, and should turn in a clockwise and then an anticlockwise direction, and with each of these movements should seek the direction of most comfort and least tension/bind.
3. The motion of the contact fingers or whole hand on the tissues is asking: ‘In which direction do the tissues move most easily?’ (Fig. 8.18).
4. When the various positions of ease, evaluated in this way, are ‘stacked’ together, this produces the combined ‘preference pattern’ – the skin and fascia will have been taken in their respective directions of motion away from whatever restriction barriers they currently exhibit.
5. Normal, unstressed, tissues exhibit an equal excursion in all directions of rotation, although this is seldom found in adults, even if surgical trauma has not been a factor (Zink & Lawson 1979).
6. The final position of ease should be held until tension releases spontaneously, usually a period of 30–90 seconds. This will commonly release recently acquired stress patterns in the fascia, possibly revealing older patterns, which can then be treated.
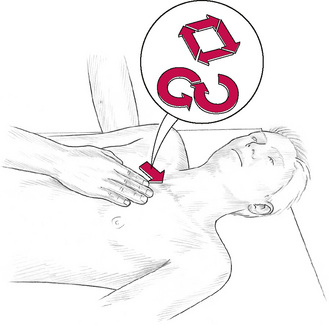
‘S’ and ‘C’ bends: myofascial release methods for lengthening soft tissues
Lederman (1997) has described the relatively few ways in which tissues can be modified by forms of direct therapeutic pressure. These involve:
• Tension loading – including traction, stretching and other lengthening approaches are involved, resulting in changes in connective tissue status (see ‘C’ bends below).
• Compression loading, on the other hand, shortens and widens tissues. See Chapter 3, Box 3.5, for a summary of these effects, which include fluid changes as well (possibly) as changes in length.
• Rotation loading elongates some fibres while compressing others (see ‘S’ bend description below).
• Bending loading combines compression loading (on the concave side) and tension loading on the convex side (see ‘C’ bend description below).
• Shearing loading involves shift or translation movements, and is used primarily in joint mobilization, while elongating and compressing associated soft tissues.
• Combined loading incorporates a variety of the models listed above (see Fig. 8.21).
Figure 8.21 Specific release technique as used in treatment of adhesions and tensor fascia lata restrictions.

Figure 8.21A Both hands release tissue that has been taken to its elastic barrier in various directions: compressed, stretched apart, counter-rotated and finally ‘sprung’.
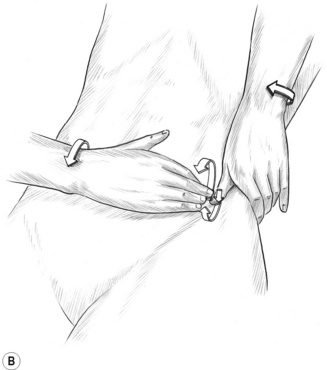
Figure 8.21B The right hand springs the restricted tissues after all slack has been removed and some stretch applied, while the left hand acts mainly to produce a stabilizing contact against which a precisely controlled force is applied.
Other variables to be considered when evaluating therapeutic ‘pressure’ include:
• The degree of pressure (see Box 3.6).
• How great an area of contact is involved and/or how large an area is receiving one or other form of loading.
• How great an amplitude is involved – in other words, how far are the tissues being moved, stretched? (The degree of force largely determines the amplitude.)
• How rapid is the application of force – does it involve high velocity or low velocity?
• For how long are the tissues loaded?
• Is the application of force static or rhythmic, and, if rhythmic, is it rapid or slow, perhaps coinciding with the breathing cycle?
• How steady is the force application, static or moving (gliding)?
• Is the patient participating in the process, actively moving, or resisting the force application?
Examples of the application of force include the ‘C’ and ‘S’ bend techniques.
‘C’ bend technique
In order to lengthen local areas of muscle and/or connective tissue, the tissues may be ‘bent’ (into a ‘C’ shape), to a first barrier of resistance, so that the thumbs engage the barrier, waiting for this to release and retreat, over a period of 5–30 seconds.
Lewit (1996) points out that:
Shortness of the connective tissue is most characteristic for short (taut) muscles, usually overactive muscles. Producing a tissue fold and stretching it is the most effective way to obtain lengthening, because the stretch reflex can be avoided.
See Figures 8.19A and 8.23A for examples of a ‘C’ bend fold. Figure 8.19A shows this being slowly applied to paraspinal muscles, allowing a gentle lengthening to occur. (Lewit 1996). Figure 8.23A (see later in this chapter, under the heading Tensor fascia lata techniques), involves the distal aspects of the iliotibial band, where the method involves a series of rapid, high-velocity, low-amplitude ‘snapping’ bends of the tissues.
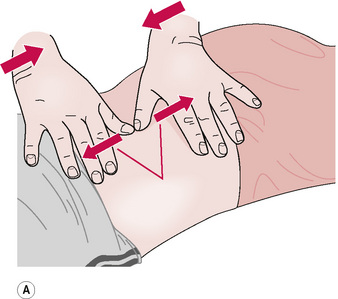

‘S’ bend technique
To achieve a relaxation of a specific area of muscle tension using an ‘S’ bend, the hands should be positioned in such a way as to allow thumb or hand pressure to be applied across the fibres of a contracted or indurated muscle, so that the contacts are travelling in opposite directions to each other (Lewit 1992).
As pressure is applied simultaneously with each thumb or hand (see Figs 8.19B and 8.23B), the tissues between the two contacts will progressively have the slack removed, and be placed in a slightly lengthened situation, in which they can be held until release occurs (or ‘springing’ is introduced).


Figure 8.23B The posterior fibres of the iliotibial band are treated using the heel of one hand alternately to thrust against the band while it is stabilized by the other hand. An alternating sequence of this sort, applied up and down the band, produces marked release of hypertonic and shortened fibres.
This technique can be applied along the course of particularly spastic, and hard unyielding, tissues, in addition to the basic NMT thumb technique (see Chapters 6 & 7).
Additionally, the ‘S’ bend may be used with a flicking action of the thumb to complete the stroke, once effective tension has been created in the tissues by the opposing thumbs. This ‘springing’ has the effect of stimulating local circulation most effectively and, if the tissues are not too sensitive, may assist in breaking down infiltrated or indurated tissues.
The ‘S’ contact is so named because the tissues being treated form that shape, as the strokes are performed. If used in its ‘slow’ mode, the tissues are held in this opposition lengthening state for upwards of 30 seconds, before slightly different fibres are selected to receive the same procedure. Alternatively a rapid, heel of hand, thrust, across the tissues (see Fig. 8.23B), may be used on particularly rigid structures, such as the iliotibial band. That approach is described later in the chapter.
Stretching fascia – myofascial release
Indications for use of MFR include a need to improve movement potential, and/or for the stretching/lengthening of shortened, contracted or fibrosed soft tissues, or for reducing tone in hypertonic muscles. See Fig 8.20.
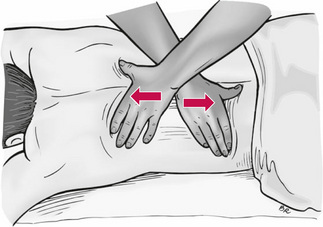
Figure 8.20 Cross handed myofascial release.
© 2007 Elsevier Ltd. Chaitow & Fritz. A Massage Therapists guide to Lower Back & Pelvic Pain.
Fascia is a tough fibroelastic body-wide web of tissue that performs both structural and proprioceptive functions. Because of its contiguous nature, and its virtually universal presence in association with every muscle, vessel and organ, the potential influences of fascia are profound if shortening, adhesions, scarring or distortion occurs as a result of either slow adaptation (microtrauma) or trauma.
Barnes (1997a, 1997b), a leading MFR expert, has said:
Myofascial release is a hands-on soft tissue technique that facilitates a stretch into the restricted fascia. A sustained pressure is applied into the tissue barrier; after 90 to 120 seconds the tissue will undergo histological length changes allowing the first release to be felt. The therapist follows the release into a new tissue barrier and holds. After a few releases the tissues will become softer and more pliable.
Mock (1997) has described a hierarchy of MFR stages or ‘levels’:
1. Level 1 involves treatment of tissues without introducing tension. The practitioner’s contact (which could involve thumb, finger, knuckle or elbow) moves longitudinally along muscle fibres, distal to proximal, with the patient passive.
2. Level 2 is precisely the same as the previous description but in this instance, the glide is applied to muscle which is in tension (at stretch).
3. Level 3 involves the introduction to the process of passively induced motion, as an area of restriction is compressed while the tissues being compressed are taken passively through their fullest possible range of motion.
4. Level 4 is the same as the previous description but the patient actively moves the tissues through the fullest possible range of motion, from shortest to longest, while the practitioner/therapist offers resistance.
For example, the practitioner might apply moderate digital pressure to the involved tissue, in a direction proximal to distal, while the patient actively moves the muscle through its range of motion in both eccentric and concentric contraction phases. This modification of basic MFR has been called Active Release Technique (ART) (Leahy 1999).
Methodology
The basic methodology of MFR requires that it should be applied slowly. Barriers of resistance are engaged, and these are forced to retreat by means of steadily applied load. In this way physiological responses of creep and hysteresis are produced, leading to lengthening. This is a non-violent, direct, approach that has little potential for causing damage (however, see cautions below).
When active or passive movements are combined with the basic methodology, caution is required depending on the status of the patient and the tissues, to avoid excessive irritation. For example enthesitis could occur if localized repetitive stretching combined with compression were applied close to an attachment (Simons et al 1999).
Cautions
• Acute arthritis and other inflammatory conditions (contraindicated during acute stages)
• Bone fractures or acute soft tissue injuries: wait for full healing (6 weeks – 3 months)
• Malignancy with metastasis (or TB) involving bone
• Pain production during procedure
• Patients on cortisone (wait 2–3 months)
Note: The skin stretching methods described above under the heading ‘Hyperalgesic skin zones’ are, in effect, examples of miniature myofascial releases. Whenever skin, or other soft tissues, fails to present symmetrical freedom of movement, either in terms of lengthening potential, range of motion, or ability to glide on underlying tissues, a degree of dysfunction can be assumed (Lewit 1996). Lewit (1996) also describes releasing these tightened, often fascial, tissues as ‘shifting’, rather than stretching. Tissues are taken to their painless elastic barrier, by application of a separation force between the hands or fingers, and held until a lengthening occurs.
Specific (abdominal) release techniques
Boris Chaitow, who worked closely with Stanley Lief, wrote the following about Lief’s ‘adhesion breaking’, ‘bloodless surgery’, techniques (personal communication, 1983):
Using these ‘bloodless surgery’ [specific release technique] methods, Stanley Lief achieved dramatic changes in tissue structure and functional improvements in many types of abdominal stresses, including digestive problems, gall bladder blockage, constipation, spastic colon, colic, uterine fibroids, dysmenorrhoea, postoperative adhesions etc. This was designed to break up deep-seated adhesions and contractions. It also enables the practitioner to improve function and circulation [of the region].
Lief used methods (outlined below) derived from an American system of manipulative or ‘bloodless’ surgery to amplify his abdominal techniques. These ‘release’ techniques can be applied to soft areas of the body, e.g. the throat, as well as to the abdomen. The original concept of ‘bloodless surgery’ was that adhesions were being ‘peeled’ away from their anchorage by the technique, and in some cases this might have been so. However, its current application is to any area of tight, fibrosed, spastic, contracted or adhering soft tissue in the abdominal region, or elsewhere – for example, on the lateral thigh in tense and contracted fascial tissues (Fig. 8.21A,B).
Precisely what takes place after abdominal release technique is open to conjecture. An improvement in tone and circulation, and usually of general function, is the most obvious result. Whether this is because of a release of a long-held contracted state in the soft tissues, or because of an actual breaking of adhesions, or because of some other mechanism, is open to debate.
• A general abdominal neuromuscular treatment (see Ch. 7) should precede application of specific release technique (technique A below).
• This serves both to relax and to tone the abdomen in a general manner, while enabling the practitioner to identify areas that feel indurated or contracted, as well as noting all areas of subjective sensitivity as reported by the patient.
• It is these (a) tight, contracted and (b) sensitive areas that receive the release technique.
Localizing dysfunction
The ability of the practitioner to localize such areas accurately is important, and needs to be practised until the hands and fingers feel such abnormalities as a matter of course. It is suggested that the middle finger of the right hand (in a right-handed practitioner) should be trained to seek and mark those areas where specific release technique is to be applied.
The patient should be supine, with knees flexed, and feet as close to the buttocks as possible, for maximum abdominal relaxation, and with the head on a small pillow. The practitioner should stand facing the patient, on the side opposite that being treated, i.e. to treat the left inguinal area the practitioner stands, knees flexed, leaning across from the patient’s right side. This allows the tissues being manipulated to be drawn towards the practitioner in a controlled manner.
Technique A
1.Having located an area of contracted (often sensitive) tissue, the middle finger locates the point of maximum resistance and the tissues are drawn towards the practitioner, to the limit of pain-free movement. In this description there will be a right hand initial contact, as illustrated in Fig. 8.21A, when working on a left lower abdominal area, while standing on the right).
2. The middle finger (right hand) and its neighbours should be flexed and fairly rigid, and be imparting force in two directions at this stage, i.e. downwards (towards the floor) and towards the practitioner. (In ‘bloodless surgery’ techniques, the right hand is always in contact with the ‘adhesion’/taut area, with the other contact on the organ/tissues to which the adhesion is attached.)
3. With the fingers maintaining the above position, the thumb of the left hand is placed almost immediately – no more than 1/4 inch (6 mm) away – adjacent to the middle finger of the right hand, in such a way that a downward pressure (towards the floor) will provide a fulcrum point, against which force can be applied via the right hand, in order to stretch, or reduce the degree of contraction in, the tissue (or indeed to break or ‘peel’ adhesions).
4. The thumb should also be flexed, and the contact can be via its tip or its lateral border, or a combination of both.
5. The idea of a fulcrum is important because the two points of contact are both on soft tissue structures, and the effect of the manipulation is achieved, not by pulling or twisting these apart, but by a combination of movements that impart force in several directions at the same time.
6. This is accomplished – after all slack has been removed, by a rapid clockwise movement of the right hand (middle finger contact) against the stabilizing anchorage of the left thumb (see Fig. 8.21A).
7. Synchronous movement of the thumb, during this release, is not essential or necessary. However, when using this method Boris Chaitow would impart a degree of additional torsional force, by releasing the thumb contact in an anticlockwise direction, at the moment of manipulation.
8. With both hands in contact, as described, and the contact digits flexed and rigid, the practitioner should be so positioned that he or she is leaning over the affected area, knees flexed with the legs separated for stability, and elbows flexed and separated to 180° separation. The forces operating at the point of contact will be downward, as well as a slight separation of the hands to the soft tissue barrier. The manipulative force is imparted by a very rapid clockwise flick of the right contact, while maintaining the left thumb contact rigid (or simultaneously, rapidly, taking it in an anticlockwise direction).
9. The effect of the right hand movement would be to snap the right elbow towards the practitioner’s side. If a double release is performed, then both elbows come rapidly to the sides.
10. The amount of force imparted should be controlled so that no pain is felt by the patient.
The essence of this technique is the speed with which it is applied. This very high velocity release involves tissues that have been ‘wound up’, by being taken in three directions of distraction – i.e. compression, separation and a degree of torsion. Its success depends upon this speed, as much as on the correct positioning of the hands, and the precise location of the area of tissue restriction.
The same procedure can be repeated several times on the same area, and the release of a number of such areas of contracted or indurated tissue, at any one treatment is usual. The same thumb contact is often maintained whilst variations in the direction of tissue tension are dealt with by slightly altering the angle of the right hand contact and manipulative effort.
If, after manipulation, no objective improvement is noted on palpation, the angle of the contacts should be varied. Nothing will be gained, however, by attempting to use excessive force in order to achieve results. As the degree of soft tissue trauma to the patient is minimal, the after-effects should not include bruising or much discomfort. Any such after-effect would indicate undue pressure or force being used.
Boris Chaitow (personal communication, 1983) described this method as follows:
For the technique of NMT on the abdomen referred to as ‘bloodless surgery’, palpate with the tips of the fingers of the right hand, and having located the area of abnormal feel, place those four fingers as a group at the distal border of the lesioned area, and place the thumb of the left hand alongside the nails of the right fingers. Give a sharp flick with both hands simultaneously, the left hand thumb being twisted anticlockwise, and the fingers of the right hand clockwise (difficult if not impossible to describe on paper). This achieves an appreciable breaking-up, without trauma or hurt to the patient, of tensions, adhesions, congestions etc., both on the wall of the abdomen and structures within the cavity. Obviously these flicks with the hands have to be repeated a number of times to feel a discernible difference in the lesioned tissue.
Technique B
A second method for the release of tense, contracted, indurated connective and muscular tissue is sometimes employed. This requires the same positioning of the patient and the practitioner, as in method A.
It is worth recalling that thickening will occur in fascia in accordance with the degree of stress imposed upon it. As enormous gravitational stress occurs in the abdominal region, as a result of postural embarrassment, it is frequently the case that tight ‘stress bands’ will be felt inferior, superior or lateral to internal organs (e.g. intestinal structures) that have sagged and become displaced. Such contracted tissue is often the source of reflex trigger activity, and is often, in itself, the cause of mechanical interference with normal venous and lymphatic drainage, as well as being a possible source of pain.
Any procedure that helps to normalize such tension should be accompanied by a programme of postural re-education and exercise, if it is to have any lasting beneficial effects.
1. The practitioner’s right hand, fingers flexed and middle finger slightly in the lead, probes through the surface abdominal musculature and attempts to ‘lift’ the structures.
2. In this way, areas of abnormal resistance will be traced, quite easily, by the tip of the middle finger of the right hand. The most inferior point of attachment of such a band is located and held firmly by this flexed digit.
3. The tip and lateral border of the thumb of the left hand is then placed adjacent to this contact, so that the right hand contact is on the tension band and the left contact is on the structure to which it attaches.
4. The manipulative force is achieved by a rapid anticlockwise movement of the right contact, whilst firm, stabilizing pressure is maintained by the left thumb (Fig. 8.21B).
5. The closer the two contacts are to each other at the moment of release, the less force is required and the less danger of injury to the tissues there will be.
6. It is suggested that, by visualizing an attempt to tear an envelope held between thumbs and forefingers, this concept will be better understood. The closer the holding digits are to each other, the easier such an operation would be. As the manipulative effort is attempting to, at least, stretch and, at most, separate the fibres involved, it is necessary to deliver a high-velocity, low-amplitude torsional force, and not a vague stretching effort imparted over a large area of unyielding tissue.
7. The actual manipulative force is imparted by the tip of the middle finger of the right hand, but is, of course, the result of the movement of the whole hand. The wrist snaps medially and the elbow outwards, at the moment of release.
8. This speedy ‘flicking’ action is one that should be practised many times, so that its execution is a matter of routine. A release of contracted tissue will be followed by an immediate freedom of mobility of tissues, or of organs formerly ‘bound’ and immobile.
Such ‘release’ procedures (technique A or B) should be performed throughout the abdominal area and preceded by the general neuromuscular treatment (see Chapters 6 & 7), and be followed by a general procedure to ‘lift’ the abdominal contents back to a physiologically correct position.
Instructions should be given of abdominal and postural exercises, to be performed by the patient, as should improved postural and breathing rehabilitation techniques.
A series of six to ten such ‘specific release’ treatments, over a period of a month or so, is suggested in chronic conditions involving visceroptosis and abdominal congestion. The application of these techniques to the hypogastric and inguinal regions may be of benefit to patients suffering from menstrual irregularities. Local function can often be improved as a result of the structural and circulatory improvements following specific release techniques.
Strain–counterstrain – and other positional release techniques (Fig. 8.22)
We have already seen examples of positional release in the section on treatment of hyperalgesic skin zones, earlier in this chapter (Fig. 8.18). Positional release techniques belong to that class of modalities that invite change, rather than forcing change, when treating dysfunctional tissues. By their nature they are indirect, i.e. the process almost always involves a disengagement from restriction barriers, rather than any direct attempt to engage and overcome such restrictions, as would be the case in HVLA, myofascial release or stretch methodology (Deig 2001). As such, PRT methods are best suited to acute and subacute settings, although they are considered a useful aid in chronic conditions.
Figure 8.22 Application of positional release (strain/counterstrain) to the supraspinatus muscle.
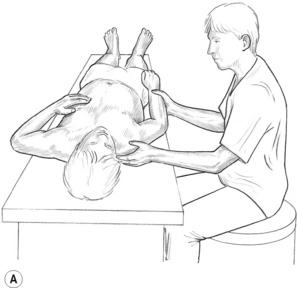
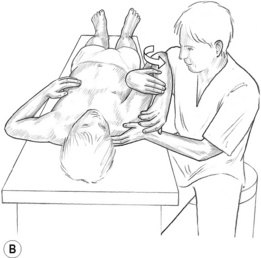
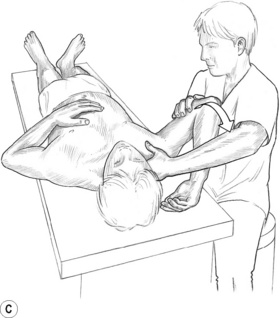
Figure 8.22C A final position of ease is found by fine tuning to relieve pain in the tender point, and the position is held for 20–90 seconds.
Simplistically, PRT methods attempt to create ‘positions of ease’ or ‘comfort’ for shortened and distressed tissues, commonly by taking already shortened (spasm, contracture, fibrosis, etc.) tissues into a supported degree of greater shortness, in the belief that a beneficial change will result, by means of mechanisms including a neurological resetting involving the muscle spindles, and a circulatory ‘flushing’ of previously ischaemic tissues. These and other possible mechanisms are discussed in the ‘Physiological effects’ section below (Chaitow 2002, D’Ambrogio & Roth 1997, Deig 2001, Rathbun & MacNab 1970).
Methodology
The art of applying positional release methods lies in identifying the direction(s) in which a painful joint, or soft tissues, should be moved, so that a spontaneous release occurs (i.e. the position of ‘ease’ or ‘comfort’). When passively placed in such a position, inhibition of painful stimuli results, and the range of motion of the area will usually be significantly enhanced afterwards.
There are two main PRT methods, with a number of variations, that have emerged out of osteopathic methodology.
1. Strain-counterstrain (SCS) utilizes a painful area in dysfunctional tissues (a ‘tender point’) as a monitor to guide the practitioner, as tissues are positioned and fine tuned, until the initial tenderness reduces from a pain score of 10, to 3 or less. The tissues are then held in this position for variable periods (90 seconds is a common recommendation) before being gently released to their resting state (Chaitow 2007, Jones 1981). Jones has compiled lists of specific tender point areas relating to every imaginable strain of most joints, and many muscles, of the body. These are his ‘proven’ (by clinical experience) points, and he provides strict guidelines for achieving ‘ease’ in the tender point that is being palpated (locating the position of ease usually involves a ‘folding’ or crowding of the tissues in which the tender point lies). A number of variations exist as to the use of the concepts that Jones developed, and these are fully explained in Positional Release Techniques (Chaitow 2002). Additional texts by Deig (2001) and D’Ambrogio & Roth (1997) are also recommended (see Figs 4.5A,B,C). An example is offered of the use of SCS positional release in Figure 8.22A,B,C.
2. Functional technique uses palpation of distressed tissues or joints to position them into ‘ease’, without using pain sensitivity as a guide (as in SCS, above). Functional approaches therefore rely on a skilled palpation sense (Johnstone 1997, Schiowitz 1990).
3. A variety of ‘facilitating’ methods are used to encourage functional and pain-reducing changes, including gentle compression, distraction or respiratory strategies (Goodheart 1984).
4. Physical therapy has evolved methods such as ‘mobilization with movement’ and ‘unloading’ taping that incorporate aspects of PRT. McKenzie exercise methods incorporate concepts of movement towards ‘ease’ that are also close to PRT concepts (Horton 2002, Morrissey 2002).
5. In chiropractic, aspects of the use of sacro-occipital technique’s ‘blocking’ methods incorporate placing tissues into an exaggeration of existing distortion (i.e. making whatever is short, shorter) and are also in line with PRT methodology (Blum et al 2003).
6. In craniosacral techniques much of the treatment involves indirect pressure, taking distortions into a ‘crowded’ state, so allowing change to take place spontaneously (Sergueef et al 2002). Upledger & Vredevoogd (1983) give a practical explanation of indirect methods of treatment, especially as related to cranial therapy. The idea of moving a restricted area in the direction of ease is, they say, ‘a sort of “unlatching” principle. Often in order to open a latch we must first exaggerate its closure’.
In normal tissues there exists in the mid-range of motion an area of ‘ease’ or balance, where the tissues are at their least tense. When there is a restriction in the normal range of motion of a joint or an area, whether of osseous or soft tissue origin, the now limited range will almost always still have a place, a moment, a point, which is neutral, of maximum comfort or ease, usually lying somewhere between the new restriction barrier in one direction and the physiological barrier in the other. Finding this balance point – also known as ‘dynamic neutral’ – is a key element in PRT.
Placing the dysfunctional tissues into this ‘ease’ state, for an appropriate length of time (see below), offers restrictions a chance to ‘unlatch’, release, normalize. In this way it is suggested that the positioning/fine-tuning element of the process is the preparation for the treatment to commence, and that the ‘treatment’ itself is self-generated by the tissues (nervous system, circulatory system, etc.) in response to this careful positioning.
Safety
The nature of indirect approaches is essentially safe, since barriers are avoided and tissues are held in comfort. Numerous studies demonstrate that these methods are safe as well as being effective (Cislo et al 1991, Ramirez 1989, Wong et al 2004a,b). Hospital studies involving treatment of recently surgically traumatized tissue validate the essential safety of positional release methods (Dickey 1989).
Proposed mechanisms
Proprioception
Walther (1988) summarizes a ‘strain’ situation as follows:
When proprioceptors send conflicting information there may be simultaneous contraction of the antagonists … without antagonist muscle inhibition, joint and other strain results [and in this manner] a reflex pattern develops which causes muscle or other tissue to maintain this continuing strain. It [strain dysfunction] often relates to the inappropriate signaling from muscle proprioceptors that have been strained from rapid change that does not allow proper adaptation.
Such patterns exist in acute settings such as torticollis, as well as in acute lumbar spasm. It is also recognizable as a feature of many types of chronic somatic dysfunction in which joints remain restricted due to muscular imbalances of this type, occurring as part of an adaptive process. This is a time of intense neurological and proprioceptive ‘confusion’, and is the moment of ‘strain’. SCS appears to offer a means of quieting the neurological confusion and the excessive, or unbalanced, tone.
D’Ambrogio & Roth (1997) state that:
Positional release therapy (PRT) appears to have a damping influence on the general level of excitability within the facilitated segment. Weiselfish (1993) has found that this characteristic of PRT is unique in its effectiveness, and has utilized this feature to successfully treat severe neurologic patients, even though the source of the primary dysfunction arose from the supraspinal level.
Nociception
Bailey & Dick (1992) suggest that strain dysfunction is far more complex than the simple proprioceptive example:
Probably few dysfunctional states result from a purely proprioceptive or nociceptive response. Additional factors such as autonomic responses, other reflexive activities, joint receptor responses [biochemical features] or emotional states must also be accounted for. Nociceptive responses would occur (which are more powerful than proprioceptive influences) and these multisegmental reflexes would produce a flexor withdrawal, dramatically increasing tone in the flexor group.
Korr’s (1976) explanation for the physiological normalization of tissues brought about through positional release is that:
The shortened spindle nevertheless continues to fire, despite the slackening of the main muscle, and the CNS is gradually able to turn down the gamma discharge and, in turn, enables the muscles to return to ‘easy neutral’, at its resting length. In effect, the physician has led the patient through a repetition of the dysfunctioning process with, however, two essential differences. First it is done in slow motion, with gentle muscular forces, and second there have been no surprises for the CNS; the spindle has continued to report throughout.
Other hypotheses
Jacobson et al (1989) have suggested a circulatory hypothesis for the benefits of PRT. Another hypothesis relates to the presumed effects of slackening fascial tissues during positional release. D’Ambrogio & Roth (1997) summarize what may happen to the fascia, during PRT, as follows:
By reducing the tension on the myofascial system, the fascial components of dysfunction may be engaged. The reduction in tension on the collagenous cross-linkages appears to induce a disengagement of the electrochemical bonds and a conversion back [from the gel-like] to the sol [solate] state. Whether proprioceptive, nociceptive, neurological, circulatory or fascial factors are involved in positional release effects remains a matter for further research.
Tensor fascia lata (iliotibial band) techniques
Ober’s test
To test for a tight iliotibial band have the patient lie on the unaffected side, with hip and knee flexed to 90°. The patient is asked to hold that leg to the table. The other leg is supported by the practitioner, who is standing behind the patient. The straight leg is extended, to the point where the iliotibial band lies over the greater trochanter. The practitioner’s cephalad hand supports the leg at the knee, while the caudad hand supports the ankle. The knee is then flexed to 90° and the hand supporting the leg at the knee is removed, allowing the knee to fall towards the table. If the iliotibial band has shortened, this will not occur and the leg will remain suspended. The band will palpate as tender under such conditions, as a rule.
The iliotibial band (ITB) comprises a thick fascial structure that runs from the iliac crest, down the lateral side of the thigh, to insert on the lateral patellar retinaculum, tubercle of the tibia, and proximal fibular head. The ITB provides attaches to the tensor fascia lata (TFL), gluteal muscles, and vastus lateralis (Orchard et al 1996).
ITB friction syndrome is a common source of overuse injury and knee pain, in athletes (Fairclough et al 2006). When the ITB is shortened it is capable of producing or contributing to a range of pelvic (e.g. SI joint), hip, leg and knee and pelvic symptoms.
Fredericson et al (2002) note that a variety of soft tissue problems (including myofascial trigger points, hip abductor muscle inhibition and fascial adhesions) can contribute to increased tension on the ITB making a comprehensive stretching protocol an important component of rehabilitation.
Because of its massive fascial component, the ITB has attracted a variety of treatment approaches, with an abiding question as to whether this structure can itself be effectively stretched at all.
NMT treatment method 1
Treatment may employ a direct approach, as advocated by Mennell (1969) or by use of MET methods, as described below.
‘Twig snap’ method
First the patient is placed side-lying, with both legs flexed comfortably. The first contact is with that part of the band distal to the greater trochanter. The anterior fibres are stretched first to create a ‘C’ bend in the tissues.(Fig. 8.23A). The fingers are laid over the anterior fibres of the band, distal to the trochanter, just above the knee. The thumbs rest, as a fulcrum, and are placed against the posterior aspect of the anterior fibres, and a rapid snapping action is applied. The main force is transmitted through the thumbs, which should stretch the fibres without pressing them against the osseous structures (which would bruise the tissues). A rapidly applied series of ‘thrusts’ such as this, starting at the knee, and working up and down the band, is carried out.
(b) ‘Piston thrust’ method
The posterior fibres are then treated. The heel of each hand is pushed in a piston-like manner against the fibres, alternately. As the heel (thenar or hyperthenar eminence) of one hand thrusts against the fibres, the other stabilizes them by grasping the anterior aspect (Fig. 8.23B). A series of thrusts is made from above the knee to the trochanter and back again. The thrust must be against the fibres and not against osseous structures, or bruising will ensue.
(c) Treatment over the trochanter
The region overlying the trochanter is treated by rolling it backwards and forwards over the bony prominence. The thumbs are the motive force, being pressed downwards and backward or forward, to achieve this. The roll is attempting to take the band posteriorly, and then anteriorly, over the trochanter. As the trochanter rolls backwards, the heel of the foot on the treated leg should rise from the table (but only if the band is tight).
(d) NMT
The area above the trochanter is treated by deep, kneading massage or NMT. This is often easily achieved when the patient is prone, and the tissues are contacted by the fingers of the treating hand, with the practitioner standing on the side opposite the area being treated. The fingers may be insinuated into the tissues, and a degree of lifting, drag, as well as pressure medial-wards, is achieved by the practitioner leaning backwards and drawing the treating hand towards him or her (see Figs 6.8A,B) This may be done as part of NMT treatment. These structures require maintenance stretching, via exercise, if improvement is to be held (see below).
Treatment method 2
MET – involving either isometric or isolytic contraction (see Fig. 8.6B). Note: See ITB Study 1 below, for confirmation of stretch occurring in the positions used in this approach.
Isometric contraction
In the first instance the patient is supine, with the unaffected leg flexed and the affected leg extended (see Fig. 8.24).The practitioner takes the extended leg into maximum adduction, placing a maximum degree of stretch onto the lateral fibres (the abductors and fascia). To achieve this, the leg will be adducted and brought under the other, flexed, leg. Standing on the side of the unaffected leg, against which the practitioner applies stabilizing pressure, the practitioner adducts the treated leg, taking out the slack, and asks the patient to make an attempt to abduct the affected leg using 25% of available strength. This is resisted for 10 seconds as the patient inhales. Release coincides with exhalation, at which time a little more slack is taken out and the affected leg is adducted slightly beyond its resistance barrier. The procedure is repeated two or three more times.

Isolytic contraction
The position is the same as that given above. Should the above method be only partly effective, then, as the patient attempts to abduct the affected leg (commencing with only a portion – say 25% – of available strength, but with increasing degree of effort, if the procedure is repeated several times) the practitioner overcomes this, and forces it further into adduction. This process may be uncomfortable, and the patient should be forewarned. This will produce microtrauma and reduce fibrous contractions. Progressively more effort on the part of the patient should be introduced on subsequent isotonic eccentric contractions.
ITB studies
1. Wang et al (2008) used a combination of MRI scans and real-time ultrasound imaging (RTU) to establish that when placed in a modified Ober’s position, actual stretch occurs in the ITB, and not only in the associated musculature (gluteals, vastus lateralis, TFL). They note that: ‘Band width changes indicated that the ITB was subjected to a significant stretching force during hip adduction.’ Such as is described above (see Fig. 8.24).
2. Using a variety of high-tech instruments, including four cameras to film the positions of skin markers, Fredericson et al (2002), evaluated both the efficacy of three stretching protocols (see Fig. 8.25ABC), as well as the subsequent degrees of lengthening, in the ITBs of the athletes participating in the study. Between 9 and 11% increase in length was noted, following three static, 30 second stretches. Variations on these stretch positions should be given as home self-care to individuals with ITB shortness.
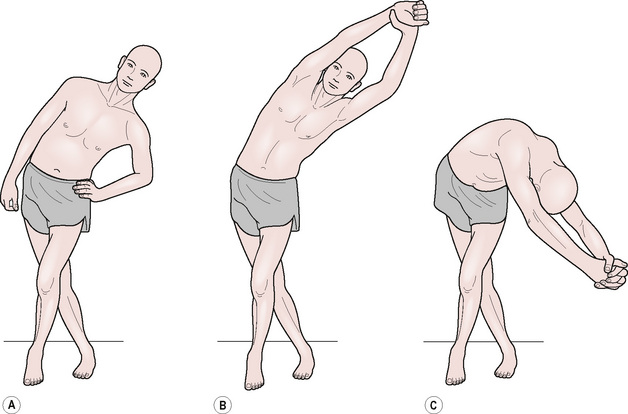
Fig. 8.25 Three stretching positions for ITB. All produced benefits after 3×30 second repetitions, with C the most beneficial.
(Adapted from Fredericson M, White J, MacMahon J 2002 Quantitative Analysis of the Relative Effectiveness of 3 Iliotibial Band Stretches Arch. Phys. Med. Rehabil. 83:589–592, Fig. 2.)
A caution offered as to what is being stretched:
One of the limitations of this study was that we did not directly measure ITB length; rather we estimated changes in length from angular changes in markers. It is possible that extensibility of other tissues such as the gluteals, tensor fascia lata, and vastus lateralis could have contributed to the changes.
Abrams A. New concepts in diagnosis and treatment. San Francisco: Physicoclinical Co, 1922.
Agarwal N., Pacher P., et al. Cannabinoids mediate analgesia largely via peripheral type 1 cannabinoid receptors in nociceptors. Nat Neurosci.. 2007;10:870-879.
Ali Z. Intradermal injection of norepinephrine evokes pain in patients with sympathetically maintained pain. Pain. 2000;88(2):161-168.
Arbuckle B. The selected writings of Beryl Arbuckle. 1977. National Osteopathic Institute and Cerebral Palsy Foundation
Bailey M., Dick L. Nociceptive considerations in treating with counterstrain. J Am Osteopath Assoc.. 1992;92(3):334. 337–341
Baldry P. Acupuncture, trigger points and musculoskeletal pain. Edinburgh: Churchill Livingstone, 1993.
Ballantyne F., Fryer G., McLaughlin P. The effect of muscle energy technique on hamstring extensibility: the mechanism of altered flexibility. Journal of Osteopathic Medicine. 2003;6(2):59-63.
Barnes M. The basic science of myofascial release. Journal of Bodywork and Movement Therapies. 1997;1(4):231-238.
Barnes M., Gronlund R., Little M., et al. Efficacy study of the effect of a myofascial release treatment technique on obtaining pelvic symmetry. Journal of Bodywork and Movement Therapies. 1997;1(5):289-296.
Blum C.S., Esposito V., Esposito C. Orthopedic block placement and its effect on the lumbosacral spine and discs. Three case studies with pre- and post-MRIs. Journal of Chiropractic Education. 2003;17:48-49.
Brodin H. Lumbar treatment using the muscle energy technique. Osteopathic Annals. 1982;10(12):23-24.
Cassidy D., Lopes A., Yong-Hing K. The immediate effect of manipulation versus mobilization on pain and range of motion in the cervical spine: a randomized controlled trial. J Manipulative Physiol Ther.. 1992;15:570-575.
Castlio Y. Effect of direct splenic stimulation in infectious diseases. American Academy of Osteopathy Yearbook. 1955;1955:121.
Chaitow L. Beat fatigue workbook. London: Thorsons, 1990.
Chaitow L. INIT in treatment of pain and trigger points. British Journal of Osteopathy. 1994;XIII:17-21.
Chaitow L. Muscle energy techniques, ed 3. Edinburgh: Churchill Livingstone, 2006.
Chaitow L. Positional release techniques, ed 3. Edinburgh: Churchill Livingstone, 2007.
Chengnan S., editor. Chinese bodywork. Berkeley, California: Pacific View Press, 1990.
Cislo S., Ramirez M., Schwartz H. Low back pain: treatment of forward and backward sacral torsion using counterstrain technique. J Am Osteopath Assoc.. 1991;91(3):255-259.
Clelland J., Savinar E., Shepard K. Role of physical therapist in chronic pain management. In: Burrows G., Elton D., Stanley G.V., editors. Handbook of chronic pain management. London: Elsevier; 1987:243-258.
D’Ambrogio K., Roth G. Positional release therapy. Missouri: Mosby, St Louis, 1997.
Deig D. Positional release technique. Boston: Butterworth Heinemann, 2001.
Degenhardt B., Darmani N., Johnson J., et al. Role of Osteopathic Manipulative Treatment in Altering Pain Biomarkers: A Pilot Study. J Am Osteopath Assoc.. 2007;107:387-400.
Dickey J. Postoperative osteopathic manipulative management of median sternotomy patients. J Am Osteopath Assoc.. 1989;89(10):1309-1322.
Drover J., et al. Influence of Active Release Technique on quadriceps inhibition and strength: A pilot study. J Manipulative Physiol Ther.. 2004;27:408-413.
Fairclough J., Hayashi J., Tounmi H., et al. The functional anatomy of the iliotibial band during flexion and extension of the knee: implications for understanding iliotibial band syndrome. J. Anatomy.. 2006;208:309-316.
Feland J., Marin H. Effect of submaximal contraction intensity in contract-relax proprioceptive neuromuscular facilitation stretching. Br J Sports Med.. 2004;38(4):E18.
Ferber R., Osternig L.R., Gravelle D.C. Effect of PNF stretch techniques on knee flexor muscle EMG activity in older adults. J Electromyogr Kinesiol. 2002;12:391-397.
Fernández-de-las-Peñas C., Sohrbeck-Campo M., Fernández-Carnero J., et al. Manual therapies in the myofascial trigger point treatment: a systematic review. Journal of Bodywork and Movement Therapies. 2005;9:27-34.
Fernández-De-Las-Peñas C., et al. The immediate effect of ischemic compression technique and transverse friction massage on tenderness of active and latent myofascial trigger points: A pilot study. Journal of Bodywork and Movement Therapies. 2006;10(1):3-9.
Fernández de las Peñas C., Arendt-Nielsen L., Gerwin R., editors. Physical Therapy for tension type and cervicogenic headache: physical examination, muscle and joint management. Boston: Jones & Bartlett, 2009.
Field T. Touch therapy. Edinburgh: Churchill Livingstone, 2000.
Fielder S., Pyott W. The science and art of Manipulative Surgery. In American Institute of Manipulative Surgery. Salt Lake City: Utah; 1955.
Fielding S. J Altern Med.. 1983.
Fredericson M., White J., MacMahon J. Quantitative Analysis of the Relative Effectiveness of 3 Iliotibial Band Stretches. Arch Phys Med Rehabil. 2002;83:589-592.
Fryer G. Muscle Energy Concepts – A Need for a Change. J Osteop Med.. 2000;3(2):54-59.
Fryer G. MET: Efficacy & Research. In Chaitow L., editor: Muscle Energy Techniques, ed 3, Edinburgh: Elsevier, 2006.
Fryer G., Fossum C. 2009, Therapeutic Mechanisms Underlying Muscle Energy Approaches, In: George J: The effects of Active Release Technique on hamstring flexibility: A pilot study. J Manipulative Physiol Ther.. 2006;29:224-227.
George J. The effects of Active Release Technique on hamstring flexibility: A pilot study. J Manipulative Physiol Ther.. 2006;29:224-227.
George J. The effects of active release technique on carpal tunnel patients: A pilot study. Journal of Chiropractic Medicine. 2006;5(4):119-122.
Goldberg J. Effect of two intensities of massage on H-reflex amplitude. Phys Ther.. 1992;72(6):449-457.
Goodheart G. Applied kinesiology workshop procedure manual, ed 21. Detroit: Privately published, 1984.
Greenman P. Principles of manual medicine, ed 2. Baltimore: Williams and Wilkins, 1996.
Hamilton L., et al. The effects of high-velocity, low-amplitude manipulation and muscle energy technique on suboccipital tenderness. International Journal of Osteopathic Medicine. 2007;10:42e-49e.
Hoag J. Osteopathic medicine. New York: McGraw Hill, 1969.
Horton S.J. Acute locked thoracic spine: treatment with a modified SNAG. Man Ther.. 2002;7(2):103-107.
Hou C-R., Tsai L-C., Show Cheng K-F. Immediate effects of various physical therapeutic modalities on cervical myofascial pain and trigger-point sensitivity. Arch Phys Med Rehabil. 2002;83(10):1406-1414.
Hovind H., Nielson S.L. Effects of massage on blood flow in skeletal muscle. Scand J Rehabil Med.. 1974;6:74-77.
Hruby R., Hoffman K. Avian influenza: an osteopathic component to treatment. Osteopathic Medicine and Primary Care. 1(10), 2007.
Ikimi F., Hunt J., Hanna G., et al. Interstitial fluid plasma protein, colloid, and leukocyte uptake into initial lymphatics. J Appl Physiol.. 1996;81(5):2060-2067.
Ironson G., et al. Relaxation through massage associated with decreased distress and increased serotonin levels. In Touch Research Institute. Miami: University of Miami School of Medicine; 1993.
Jacobson E.C., Lockwood M.D., Hoefner V.C., et al. Shoulder pain and repetition strain injury to the supraspinatus muscle: etiology and manipulative treatment. J Am Osteopath Assoc.. 1989;89(8):1037-1045.
Janda V. Muscle function testing. London: Butterworths, 1990.
Janda V. Muscle and back pain. Physical Medicine Research Foundation presentation. 1992. Vancouver, British Columbia
Jay G. Sympathetic aspects of myofascial pain. Pain Digest.. 1995(5):192-194.
Johnson A. Principles and practice of drugless therapeutics. Los Angeles: W Straube, 1939.
Johnstone W. Functional technique. In: Ward R., editor. Foundations for osteopathic medicine. Baltimore: Williams & Wilkins, 1997.
Kamani H., Walters N. Muscle energy technique. The effect on joint mobility and agonist/antagonist muscle activity. In: 2nd International Conference on Advances in Osteopathic Research (ICAOR). London: The Law Society; 2000.
Klinge D., Magnusson S., Simonsen E., et al. The effect of strength and flexibility training on skeletal muscle electromyographic activity, stiffness, and viscoelastic stress relaxation response. Am J Sports Med.. 1997;25(5):710-716.
Korr I. Collected papers of I.M Korr. Newark, OH: American Academy of Osteopathy, 1976.
Kuchera M., Kuchera W. Considerations in systemic dysfunction. Columbus, Ohio: Greyden Press, 1994.
Kuchera W., Kuchera M. Osteopathic Principles in Practice. Missouri: Kirksville College of Osteopathic Medicine, 1992.
Leahy P. Active release techniques, Hammer W Functional soft tissue examination and treatment in manual methods, ed 2. Aspen: Gaithersberg Maryland, 1999.
Lederman E. Fundamentals of Manual Therapy. London: Churchill, 1997.
Lenehan K., et al. The effect of muscle energy technique on gross trunk range of motion. J Osteopath Med.. 2003;6(1):13-18.
Lewit K. Manipulative therapy in rehabilitation of the motor system. London: Butterworths, 1985.
Lewit K. Manipulative therapy in rehabilitation of the locomotor system, ed 2. London: Butterworths, 1992.
Lewit K. Role of manipulation in spinal rehabilitation. In: Liebenson C., editor. Rehabilitation of the spine. Baltimore: Williams & Wilkins, 1996.
Lewit K. Manipulative therapy in rehabilitation of the locomotor system, ed 3. London: Butterworths, 1999.
Liebenson C. Manual Resistance Techniques in Rehabilitation. In: Chaitow L., editor. Muscle Energy Techniques. Edinburgh: Churchill Livingstone, 2006.
Liebenson C. Manual resistance techniques in rehabilitation. In Chaitow L., editor: Muscle energy technique, ed 2, Edinburgh: Churchill Livingstone, 2001.
Lupandin L., Kuz’mina K. Interaction of thermoreceptive and vestibular signalling in regulating the activity of flexor and extensor motor nuclei during cold tremor. Fiziol Zh SSSR Im I M Sechenova. 1985;11(71):1433-1438.
McHugh M., Kremenic I., Fox M., Gleim G. The role of mechanical and neural restraints to joint range of motion during passive stretch. Med Sci Sports Exerc. 1998;30(6):928-932.
McPartland J.M., Simons D.G. Myofascial trigger points: translating molecular theory into manual therapy. Journal Manual and Manipulative Therapies. 2007;14:232-239.
McPartland J. Expression of the endocannabinoid system in fibroblasts and myofascial tissues. Journal of Bodywork and Movement Therapies. 2008;12:169-182.
Magnusson M., Simonsen E.B., Aagaard P., et al. Contraction specific changes in passive torque in human skeletal muscle. Acta Physiol Scand.. 1995;155(4):377-386.
Magnusson M., Aagaard P., Simonsen E.B., et al. A biomechanical evaluation of cyclic and static stretch in human skeletal muscle. Int J Sports Med.. 1998;19:310-316.
Magnusson M., Simonsen E., Aagaard P., et al. Mechanical and physiological responses to stretching with and without pre-isometric contraction in human skeletal muscle. Archives of Physical Medicine & Rehabilitation. 1996;77:373-377.
Magnusson M., Simonsen E., Aagaard P., et al. A mechanism for altered flexibility in human skeletal muscle. Journal of Physiology. 1996;497(Part 1):293-298.
Mehta M., Hatton P. The relationship between the duration of sub-maximal isometric contraction (MET) and improvement in the range of passive knee extension. Journal of Osteopathic Medicine. 2002;5(1):40.
Mennell J. Joint pain. Boston: Little Brown, 1969.
Mennell J. The therapeutic use of cold. J Am Osteopath Assoc.. 1975;74(12):1146-1158.
Mitchell F.Jr. Tutorial on biomechanical procedures. Carmel CA: Yearbook American Academy of Osteopathy, 1976.
Mitchell F.Jr, Moran P., Pruzzo N. An evaluation and treatment manual of osteopathic muscle energy procedures. Valley Park: Illinois, 1979.
Mitchell F.Jr, Mitchell P.K.G. The Muscle Energy Manual. vol 1. Michigan: MET; 1995.
Mock L. Myofascial release treatment of specific muscles of the upper extremity (levels 3 and 4). Clinical Bulletin of Myofascial Therapy. 1997;2(1):5-23.
Moore M., Kukulka C. Depression of Hoffman reflexes following voluntary contraction and implications for proprioceptive neuromuscular facilitation therapy. Phys Ther.. 1991;71(4):321-329.
Morrissey D. Unloading and proprioceptive taping. In Chaitow L., editor: Positional release techniques, ed 2, Edinburgh: Churchill Livingstone, 2002.
Morrison M. Lecture notes - Seminar. London: Charing Cross Hotel, 1969.
Norris C. Functional load abdominal training (part 1). Journal of Bodywork and Movement Therapies. 1999;3(3):150-158.
Orchard J.W., Fricker P.A., Abud A.T., Mason B.R. Biomechanics of iliotibial band friction syndrome in runners. Am J Sports Med.. 1996;24:375-379.
Oschman J. What is healing energy? Pt 5: gravity, structure, and emotions. Journal of Bodywork and Movement Therapies. 1997;1(5):307-308.
Owen C. An endocrine interpretation of Chapman’s reflexes. In Academy of Applied Osteopathy. Ohio: Newark; 1977.
Pertwee R. The therapeutic potential of drugs that target cannabinoid receptors or modulate the tissue levels or actions of endocannabinoids. AAPS Journal. 2005;7:E625-E654.
Polstein B. DiGiovanna E., editor. Osteopathic approach to diagnosis and treatment. Philadelphia: JB Lippincott, 1991.
Puustjarvi K., et al. Effects of massage in patients with chronic tension headaches. Acupuncture and Electrotherapeutics Research. 1990;15:159-162.
Rathbun J., MacNab I. Microvascular pattern of rotator cuff. J Bone Joint Surg.. 1970;52:540-553.
Retzlaff E.W., Bemy A.H., Haight A.S., et al. The piriformis muscle syndrome. Journal of American Osteopathic Association. 1974;73:799-807.
Rich G.J. Massage therapy: the evidence for practice. Edinburgh: Churchill Livingstone, 2002.
Ruddy T. Osteopathic rhythmic resistive duction therapy. Yearbook of Academy of Applied Osteopathy 1961, Indianapolis, 1961;58.
Sandler S. The physiology of soft tissue massage. British Osteopathic Journal. 1983;15:1-6.
Sergueef N., Nelson K., Glonek T. The effect of cranial manipulation on the Traube–Hering–Mayer oscillation as measured by laser-Doppler flowmetry. Altern Ther Health Med.. 2002;8(6):74-76.
Schiowitz S. Facilitated positional release. American Osteopathic Association. 1990;90(2):145-156.
Shoemaker J., Tiidus P., Mader R. Failure of manual massage to alter limb blood flow: measures by Doppler ultrasound. Med Sci Sports Exerc.. 1997;29(5):610-614.
Simons D., Mense S. Diagnosis and therapy of myofascial trigger points. Shmerz. 2003;17(6):419-424.
Simons D., Travell J., Simons L. ed 2. Myofascial pain and dysfunction: the trigger point manual. vol 1. Baltimore: Williams & Wilkins; 1999. upper half of body
Sleszynski S.L., Kelso A.F. Comparison of thoracic manipulation and incentive spirometry in preventing postoperative atelactesis. Journal of American Osteopathic Association. 1993;93:834-838. 843–845
Schmitt G., Pelham T., Holt L. From the field. A comparison of selected protocols during proprioceptive neuromuscular facilitation stretching. Clinical Kinesiology. 1999;53(1):16-21.
Simons D., Travell J., Simons L. ed 2. Myofascial Pain and dysfunction: The trigger point manual. vol 1. Baltimore: Williams & Wilkins; 1999.
Smith M., Fryer G. A comparison of two muscle energy techniques for increasing flexibility of the hamstring muscle group. Journal of Bodywork and Movement Therapies. 2008;12(4):312-317.
Stoddard A. Manual of osteopathic practice. London: Hutchinson Medical, 1969.
Te Poorten B. The piriformis muscle. Journal of American Osteopathic Association. 1969;69:150-160.
Taylor P., Tole G., Vernon H. Skin rolling technique as an indicator of spinal joint dysfunction. J Can Chiropractic Assoc.. 1990;34(2):82-86.
Travell J. Ethyl chloride spray for painful muscle spasm. Arch Phys Med Rehabil. 1952;33:291-298.
Travell J., Simons D. Myofascial pain and dysfunction. vol 1. Baltimore: Williams & Wilkins; 1983.
Travell J., Simons D. Myofascial pain and dysfunction. vol 2. Baltimore: Williams & Wilkins; 1992.
Upledger J., Vredevoogd J. Craniosacral therapy. Seattle: Eastland Press, 1983.
Wallace E., McPartland J., Jones J., et al. Lymphatic manipulative techniques. In: Ward R., editor. Foundations for osteopathic medicine. Baltimore: Williams & Wilkins, 1997.
Walther D. Applied kinesiology. SDC Systems: Pueblo, 1988.
Wang H-K., Shih T., Lind K.-H., Wang T-G. Real-time morphologic changes of the iliotibial band during therapeutic stretching; an ultrasonographic study. Man Ther.. 2008;13:334-340.
Washington K., Mosiello R., Venditto M., et al. Presence of Chapman reflex points in hospitalized patients with pneumonia. Journal American Osteopathic Association. 2003;103:479-483.
Weiselfish S. Manual therapy for the orthopedic and neurologic patient. Hertford, CT: Regional Physical Therapy, 1993.
Wilson E., Payton O., Donegan-Shoaf L., et al. Muscle energy technique in patients with acute low back pain: a pilot clinical trial. Journal of Orthopaedic & Sports Physical Therapy. 2003;33:502-512.
Wittlinger H., Wittlinger G. ed 3. Textbook of Dr Vodder’s manual lymph drainage. vol 1. Heidelberg: Karl F Haug; 1982. basic course
Wong C., Schauer-Alvarez C. Effect of strain/counterstrain on pain and strength in hip musculature. Reliability, validity and effectiveness of strain/counterstrain techniques. Journal of Manual and Manipulative Therapy. 2004;12(2):107-112.
Wright P., Drysdale I. Comparison of PIR and RI muscle energy techniques applied to piriformis. Intl Jnl Ost Med.. 2008;11:158-159.
Xujian S. Effects of massage and temperature on permeability of initial lymphatics. Lymphology. 1990;23:48-50.
Zhao-Pu W. Acupressure therapy. Edinburgh: Churchill Livingstone, 1991.
Zink G., Lawson W. An osteopathic structural examination and functional interpretation of the soma. Osteopathic Annals. 1979;12(7):433-440.