Chapter 18 Footwear
INTRODUCTION
The examination of a patient attending for podiatry treatment cannot be considered complete until assessment has been made of the footwear. It must also be remembered that footwear worn on the day of the examination may not reflect that which is typically used by the patient, and it is therefore necessary for the podiatrist to question the patient about their footwear preferences and habits.
To establish the cause of a foot complaint a thorough case history and examination of the feet during stance, gait and non-weight bearing is required (see Ch. 1). Application of podiatric skills and knowledge, including the normal parameters of gait and the range and direction of joint motion, leads to a clinical judgement to determine the presence, or absence, of any abnormality that accounts for the patient’s symptoms. The outcome of this examination process may lead the practitioner to determine that no significant abnormality is present. The conclusion may then be made that there is no intrinsic cause of the patient’s symptoms, and therefore attention must be focused on what extrinsic influences are placed on the feet and consideration given to the effects of these influences on normal foot function and gait. Frequently, footwear plays a major extrinsic role in the development of, or contribution to, a patient’s foot symptoms. Failure to formally appraise the footwear presented renders the practitioner incapable of fully understanding what can be a complex source of foot discomfort. Footwear appraisal also provides the ideal opportunity to discuss with the patient the relationship between the dynamic foot and footwear.
For the patient to receive maximum benefit from the consultation, and gain an understanding of how they can positively contribute to the management of their own foot condition, discussion regarding footwear must take place. This also allows the podiatrist to advise the patient regarding specific features they require in footwear to achieve maximum foot function and comfort. While this point is easily made, the issue of the provision of footwear advice can present with one of the greatest patient education and communication challenges of the podiatrist’s professional life.
Examination of footwear necessitates the podiatrist to reflect on how the normal foot functions in footwear. When managing the abnormal foot the podiatrist must consider how any identified abnormality within the foot being examined may manifest itself within the footwear during stance and gait. To achieve a successful management outcome it is often necessary to address the issue of the presenting intrinsic structural pathologies with the prescription and application of functional or accommodative orthoses while also making specific recommendations about footwear.
Examination of the wear marks appearing on footwear often reveals information about the gait of the wearer. This can significantly contribute to the practitioner’s understanding of the patient’s symptoms. In addition, comparing the wear marks on the patient’s footwear with that which is considered ‘normal’ can often assist in early diagnosis of conditions that previously have been asymptomatic.
FUNCTION OF FOOTWEAR
Primary function
The wearing of footwear by man at an early stage of civilisation is confirmed (McDowell 1989) by the discovery in Spain of paintings dated between 12,000 and 15,000 BC that depict a man wearing boots made of skin and a woman wearing boots made of fur. The existence of footwear can be traced back to the Ice Age, when basic foot coverings were made from animal skins. In the early and simple form this footwear provided protection principally to the plantar aspect of the foot. With the development of more sophisticated foot coverings the protection provided to the plantar aspect of the foot was extended to the dorsal aspect of the foot and the lower leg. This dorsal extension provided greater protection to the lower limb from extremes of weather, barbed plants and rough terrain. Today, even with the many influences on shoe design and manufacture, protection is still regarded as the primary function of footwear.
Secondary functions
Footwear is also considered to have a number of secondary functions. Appreciation of the secondary functions of footwear enables the podiatrist to question the patient and establish to what extent these secondary functions influence footwear selection, style and wear time. The shoes worn to attend the podiatrist for consultation may not typify those worn on a day-to-day basis. It is extremely important that the podiatrist has a clear understanding of each patient’s footwear preference and wear habits before consideration can be given to any influence the footwear choice may have on the patient’s presenting symptoms. In addition, the full footwear history and habits can have a significant influence on the clinical examination outcome and the management plan. Failure on the part of the podiatrist to establish a clear and current footwear history may cause significant disadvantage when conducting a clinical examination, and may result in an inability to adequately manage the patient.
Completing a fashion
There are many functions of footwear that may be considered secondary to the primary function of protection. The fashion industry plays a major role in dictating what style of footwear is in vogue. Female footwear styles are particularly influenced by the fashion industry. A cursory look into any woman’s fashion magazine will confirm the close relationship between clothing style and footwear style. The frequent changes in fashion clothing trends invariably dictate a change in the height and breadth of the heel and the shape of the toe box of the shoe. Footwear therefore plays a significant role in completing a fashionable ‘look’. This function of footwear is also applicable to specific occupations where the wearing of a particular style of shoe is a requirement of a company on its employees in order to comply with a particular corporate image. For example, some companies within the airline industry require both male and female employees to wear a particular style of shoe in order that corporate identity is preserved. This preservation of image is often at the expense of efficient foot function and the comfort of the employee.
Conducting specific tasks
Specific types of footwear are worn in order that the wearer can perform particular tasks. It would be impossible for a ballet dancer to perform on stage without wearing custom-made ballet shoes that allow the dancer’s foot to adopt precise positions and rapidly change direction of motion while looking graceful and elegant. Similarly, the ability of the combat soldier to march long distances would be impaired if the typical army boot were not worn. Incorporated within the construction of the army boot is a high toe spring and rigid outsole. The combination of these two features minimises foot fatigue when walking long distances and reduces the motion required at the metatarsophalangeal joints during propulsion. A further function of footwear can therefore be identified as a means of assisting the foot to perform a specific task.
Compensating for an abnormality
Footwear may also assist the wearer to overcome a lower-limb abnormality. Significant limb-length discrepancy may be overcome through adaptation of traditional footwear with the addition of a raise to the outsole to the value of the discrepancy. For example, a limb-length discrepancy of 4 cm may be compensated for through the addition of a 4-cm raise to the outsole of the shoe. The rigidity and consequent inflexibility of the modified outsole would be offset by the incorporation of an exaggerated toe spring to facilitate a more natural and efficient toe-off during the propulsive phase of gait. Simple adaptations may be carried out by a traditional cobbler, while more sophisticated adaptations will be provided by a bespoke shoe maker.
PARTS OF A SHOE
Shoes and footwear in general are made in a variety of styles and are manufactured using a wide selection of natural and synthetic materials. Shoe design is largely dependent on the function for which the shoe is intended. A significant influence on the design of the shoe is the targeted retail market and the anticipated price range of the shoe. Although shoes vary immensely in appearance and function all shoes have some common features which, when combined during the manufacturing process, create the completed footwear.
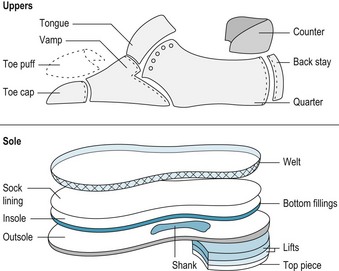
To gain an appreciation of the relationship of one part of the shoe upper to another, examination of the traditional Oxford shoe provides a good example (Fig. 18.1). The Oxford shoe exhibits the many individual shoe parts that are combined during the shoe manufacturing process. In its traditional format, the Oxford shoe is proven to be a robust, hardwearing and long-lasting shoe. Although not singularly reserved for males, historically the Oxford shoe was the favoured shoe worn by professional men. Today, with the influence of fashion and cheaper shoe manufacturing techniques, the Oxford shoe is no longer reserved for businessmen and the style, or variations of it, is frequently seen in high-street shops. Variations in style, shoe manufacturing processes and the cost of footwear will undoubtedly alter the manufacturing process and ultimately the final appearance of the shoe. However, all footwear examined by the podiatrist will display some of the elements seen in the Oxford shoe.

Shoes are traditionally made on lasts that are developed by shoe designers. The last can be made of wood or plastic and is the mould on which the shoe is made. The design of lasts varies depending on the style of footwear to be manufactured. Traditionally, the various parts of the shoe used in the manufacturing process are grouped under the headings of upper, sole and subsidiary parts (Fig. 18.2).
The upper
The upper of the shoe comprises the shoe parts brought together during the shoe manufacturing process to form that part of the shoe which embraces the dorsal aspect of the foot and the medial, lateral and posterior borders of the foot. Depending on the design of the footwear, uppers may consist only of single or multiple straps, as seen in some women’s sandals. At the other extreme, where greater protection is required or as dictated by fashion, uppers may extend to the leg in the form of knee- and thigh-length boots. The typical upper of a shoe comprises all or many of the parts detailed below.
The toe box
The toe box is the space found at the most anterior part of the shoe. This provides accommodation for the toes, and any inadequacy in the design of the last results in poor breadth or depth of the toe box, which can lead to lateral compression of the digits or compression on the nail plate. The toe box is often lined with a ‘toe puff’ or ‘stiffener’. The object of the toe puff is to maintain the shape of the toe end of the last within the shoe following its production. This preserves the final appearance of the shoe and, with care, will maintain the anterior shape for the lifespan of the shoe. In this context, the toe puff does not offer toe protection properties; this can be achieved only by the incorporation of steel toe protectors, as seen in some industrial footwear.
The toe cap
The toe cap is the layer of material in the upper that is applied to the toe end of the shoe. This forms the most anterior part of the upper and encloses the toes within the toe box of the shoe. In the traditional Oxford shoe, the toe cap is an additional piece of hard-wearing leather that is applied to the anterior end of the upper at the toe box and stitched posteriorly to the vamp. It is used to provide decoration and added strength and wear to the area. As with the toe puff, it should not be confused with the protective steel toe cap that is incorporated in industrial shoes to provide protection for the toes against impact. In traditional, everyday footwear the protection provided by the toe cap is negligible.
The vamp
The term ‘vamp’ refers to the upper piece of material that forms the part of the shoe immediately above the metatarsophalangeal joints. In the Oxford shoe it is attached anteriorly to the toe cap and posteriorly to the medial and lateral quarters.
The metatarsophalangeal joints form the fulcrum point of the foot during propulsion; therefore, the vamp is frequently subjected to much flexion during gait – particularly during propulsion to allow the necessary dorsiflexion at these joints. The vamp is required to be made of a flexible but hard-wearing material capable of withstanding repeated stress. Good-quality flexible leather is ideal for this purpose. Cheaper shoes made from synthetic materials frequently show early signs of wear and tear at the vamp, which becomes cracked and eventually may break under the strain.
The tongue
The tongue of a shoe, incorporated in lacing shoes, is an important part of the design. This is a shaped piece of material, usually leather. In the Oxford shoe it is attached on the inside of the shoe to the posterior surface of the vamp. In other styled, lacing shoes (e.g. the Derby shoe) the tongue is formed through a posterior extension of the vamp. In either case, the tongue is positioned in such a way that the dorsal aspect of the foot, particularly the area of the tarsometatarsal joints, is protected from the pressure of the laces and eyelets in the medial and lateral quarters of the shoe. This protection is particularly necessary when the foot is held firmly within the shoe and is efficiently tied with the laces, thereby effectively retaining the foot within the shoe. To successfully perform this protective function, the tongue of the shoe should be well positioned over the dorsal aspect of the foot. It should also be thick enough to provide the necessary absorption of pressure. Some manufacturers incorporate a robust cushioning material between the outer leather of the tongue and its inner lining. This additional piece of material maximises the protection to the dorsal aspect of the foot and encourages an effective lacing technique by the wearer. The absence of an effective tongue in lacing shoes discourages the wearer from lacing the shoes firmly on the feet – mainly because of the uncomfortable pressure of the laces and eyelets on the dorsal aspect of the feet. In response to this discomfort the wearer either discontinues wearing lacing shoes altogether or prefers to wear them loosely tied. The former option may result in the alternative style offering, at best, inadequate retention of the foot within the shoe and, at worst, a shoe that is too small. The latter option results in the creation of physical stresses within the foot as it is no longer held securely during gait and stance. Due to the poor retention, the foot is permitted to move mediolaterally and anteroposteriorly. Over a period of time this repeated motion and lack of security of the foot within the shoe can result in a plethora of foot conditions and strain on the joint ligaments and tendon insertions, giving rise to chronic foot strain and other soft-tissue pathologies.
The quarters
The quarters form the posterior part of the shoe. The medial and lateral quarters of the shoe cradle the hindfoot and should provide a close fit of the shoe to the tarsal and metatarsal regions of the foot. The quarters are joined anteriorly with the vamp and are stitched together at the back of the shoe. To accommodate the medial longitudinal arch of the foot the medial quarters are higher than the lateral quarters. In lacing shoes, the anterior part of the quarters gives rise to the facings that accommodate the eyelets of the shoe. The material from which the quarters are made needs to be hard-wearing and must be able to endure the strain placed on it by the laces while maintaining the eyelets in their correct position. In good-quality footwear the quarters are reinforced to add strength to the area with the addition of a counter located between the quarters and its lining. The combination of close-fitting quarters, the counter and the correct use of the laces serves to hold the foot firmly within the footwear and to minimise any undesirable anteroposterior movement of the foot within the shoe during gait. Similarly, the elimination of mediolateral movement of the heel of the foot within the rear of the shoe is vital to maximise normal foot and joint function during stance and gait. Failure of any shoe to minimise these movements results in stress that can, in time, produce a variety of bone and soft-tissue pathologies within the foot.
The sole
The composition of the sole of shoes varies greatly and is controlled by numerous factors. Sole construction is influenced by the quality and style of the footwear, the material used during manufacture, the manufacturing process and the projected cost of the footwear. Varied use of the basic sole unit components may be seen in modern footwear. Typically, the men’s Oxford shoe consists of the elements detailed below.
The insole
The insole of the shoe is the innermost part of the sole unit and is the platform upon which the foot rests. The material used in insole manufacture must be robust while providing a smooth surface. Any irregularities in the surface of the insole are potential irritants to the plantar aspect of the foot and can result in discomfort to the wearer and the formation of skin pathology. The importance of the quality and integrity of the insole is well demonstrated when considering the effects of a poor-quality, rough insole on the neuropathic foot. While the traditional material for the insole is leather, a variety of synthetic materials is also used. The insole is usually lined with a fine ‘sock lining’, which serves to provide extra smoothness and improve the appearance of the inner part of the shoe. The sock lining may be full length or only three-quarter length, covering the waist and heel seat of the insole. It is usual for the manufacturer to incorporate their name or logo on the sock lining.
In modern footwear, manufacturers often incorporate removable full-length insole liners, many of which are manufactured from synthetic foam materials. The removal of the manufacturer’s insoles permits replacement with commercially available or bespoke insoles.
Bottom fillings
Traditionally made Oxford shoes incorporate bottom fillings within the sole construction of the shoe. The bottom fillings are an infill material used to level out the surface of the lasted shoe once the shank is positioned between the insole and the attached outsole. The bottom fillings found in traditionally manufactured Oxford shoes are typically made from granulated cork. With wear of the shoe, the bottom fillings sustain a mild compression that permits an accommodative depression in the tread area of the insole immediately below the metatarsal heads. Many modern shoe manufacturers do not need to incorporate bottom fillings as they rely on the direct moulded method of sole construction to eliminate irregular contours on the undersurface of the lasted shoe.
The welt
Incorporated in the outsole of the traditional Oxford shoe, and in many other more expensive shoes, the welt serves as a joining material uniting the lasted upper to the outsole. The welt is a narrow piece of leather sewn to the perimeter of the upper of the lasted shoe and projecting slightly outwards. The outsole is then attached to this projection and then attached by a further stitch around the entire surface of the welt, providing a strong attachment of the outsole to the upper of the shoe. The use of the welt in shoe sole construction provides a means of easily removing the outsole when it is worn and attaching a new one, thereby significantly increasing the lifetime of the shoe.
The outsole
The outsole of a shoe is the section that is in direct contact with the ground. Traditionally, it is made of specially treated hard-wearing leather; current methods of sole construction utilise rubber, crepe or other synthetic hard-wearing material. The outsole is required to withstand much wear and tear, and must be tough while retaining the necessary flexibility to permit propulsion during gait.
Leather outsoles are typically found on Oxford shoes. They are hard-wearing and flexible enough to achieve efficient propulsion; they are not, however, particularly good for shock absorption. Manufacturers have commonly replaced the use of leather with hard-wearing synthetic materials that are light in weight and adequately flexible. They will provide shock absorption and protect the foot and skeletal tissues against impact and ground reaction force from hard unyielding surfaces.
Outsoles are attached to the lasted upper by a variety of methods of sole construction, the most commonly used being direct moulded, cemented and welted.
The subsidiary parts
In addition to the main parts of the shoe that are found within the upper and the sole, the subsidiary parts may be incorporated in the manufacture to enhance shoe structure and function; they are not necessarily found in all examples of footwear.
The heel
The heel of the Oxford shoe consists of layers of leather, termed ‘lifts’, attached together providing the required heel height. On the outermost part of the heel, which is in direct contact with the ground when the shoe is worn, a top piece is applied. The top piece is so named because as the lasted shoe reaches its final stage of manufacture it is presented to the shoemaker in the inverted position with the sole facing upwards. This is the final component placed on the shoe before the last is removed. This top piece is made of hardwearing leather and is easily removed when worn and can be replaced. Frequently in modern day shoe manufacture the heel unit is fully integrated with the sole unit and is a composite part of the outsole created through the direct moulding method of sole construction.
The shank
The shank is inserted between the insole and the outsole at the waist of the shoe to form a reinforcing bridge between the heel and the forepart of the shoe. Shanks are traditionally made of a narrow strip of steel or wood and provide support to the non-weight-bearing part of the outsole of the shoe. The former is usually reserved for women’s shoes and the latter for men’s shoes. The shank is particularly necessary in women’s shoes that incorporate a higher heel, preventing the shoe from snapping at the waist during wear.
The counter
The heel counter is a moulded cup-shaped piece of leatherboard or thermal plastic material that may be inserted at the rear of the shoe between the medial and lateral quarter and its lining. The counter is responsible for preserving the shape of the rear medial and lateral quarters during wear and preserving a close relationship between the quarters and the rear part of the foot.
The backstay
The backstay is a narrow strip of leather that is attached to the rear of the shoe and acts as reinforcement to the joint of the medial and lateral quarters. The backstay protects this vulnerable part when the last is removed from the completed shoe and also during wear when the foot is placed in the shoe. The backstay is recognised as an additional strip of leather attached externally at the junction of the rear quarters; alternatively, it may simply comprise a discreet overlay of the upper part of the rear lateral quarters on the medial quarters.
FEATURES OF A GOOD-FITTING SHOE
To achieve maximum benefit from podiatric treatments, patient compliance with footwear advice and a commitment to wearing appropriate shoes on a regular basis is fundamental. It is necessary for the practitioner to be aware of footwear fashion trends, the quality and characteristics of footwear manufactured by individual companies, and local suppliers of footwear. Unfamiliarity with such information renders the podiatrist ill prepared to provide important advice to patients. This may result in a significant reduction in the benefit from both short- and long-term care received by the patient and the full treatment potential will not be realised. Achieving patient compliance with footwear advice is fraught with difficulty. Female patients may present particular resistance to the adoption of footwear advice. They often, incorrectly, anticipate that the podiatrist is recommending ‘old ladies’ ’ shoes and, as a consequence, reject the advice and quickly respond with an excuse as to why they cannot wear that type of shoe. There may be an incorrect perception of the type of shoe that the podiatrist is recommending. As a result, the patient invariably interrupts the delivery of the advice and fails to hear accurately the facts within the information given. Male patients tend to be more receptive to footwear advice. Male footwear styles are less varied and, in general, provide better accommodation for the foot and permit a more natural foot function.
The delivery of footwear advice may be more successfully achieved if it is provided through the podiatrist exploring with the patient what qualities and level of comfort they would like to achieve when purchasing footwear. Careful questioning of the patient can provide the podiatrist with information that can later be reflected back to the patient when recommending specific features about an appropriate shoe. An explanation of how specific footwear features will meet the individual patient’s requirements suggests to the patient that they have remained in control of the footwear selection. The information supplied by the podiatrist regarding specific features of footwear and relating the desirable features to specific manufacturers and styles is invariably more positively received than is a more dictatorial, uncompromising approach.
Normal foot function is described (Merriman & Tollafield 1995) as being pain-free and energy-efficient. Rossi (2003) distinguished between the terms ‘normal gait’ and ‘natural gait’. The former term may be applied to shoe-wearing societies, while the latter can be applied to barefoot societies. It is suggested that the use of the term ‘normal’ may be defined as the accepted standard, mean or average. In contrast, the term ‘natural’ is reserved for what is ‘pristine, the ideal state, the ideal form and function stemming from nature itself’. The difference between the two terms is summarised by: ‘The difference between normal and natural is essentially the difference between what is and what can or ought to be.’ (Rossi 2003).
When this definition is applied in the context of wearing footwear, it can be considered that those who wear shoes will not have a natural gait, as is seen in those who live within shoeless societies, but they will have the potential for a normal gait, the features of which will demonstrate the accepted parameters of normal shoe-assisted gait. Ideally, therefore, any footwear worn to assist walking on hard unyielding surfaces should function in a manner that maximises the potential for more natural gait and that ensures natural foot function is subjected to the minimum of interference. It is desirable that any shoe will work in harmony with and permit the foot to function as naturally as it can.
When advising patients on footwear, attention should be drawn to the desirable features discussed below. Footwear advice must take into account the function for which the footwear is to be used. The features required in footwear to be worn for a busy working day differ from those used for less-active social occasions.
Good retaining medium
A ‘good retaining medium’ refers to any device that retains the foot within the shoe and eliminates undesirable forward movement of the foot within the shoe. Lacing devices are the best means of achieving this. A minimum of three pairs of eyelets with laces is recommended. Although lacing devices are the retaining mechanism of choice, unless the shoe is laced correctly retention can be significantly compromised. The correct way of lacing a shoe is to hold the foot at approximately 45° from the floor surface with the heel of the foot firmly pressed into the rear of the shoe (Fig. 18.3). While maintaining this position the laces should be firmly adjusted from the lowest pair of eyelets to the uppermost and then tied firmly. This method mimics the position the foot adopts when it is placed on the fitting stool used by reputable shoe retailers. For patients with back pain or those who find it difficult to stoop down to lace shoes in this manner, the heel of the foot may be placed on a stool or step. Any discomfort anticipated from the firmness of tied laces should be removed by ensuring that the shoe has a good pressure-absorbing tongue. Shoes that do not have this feature may be adapted through the application of a cushioning tongue pad applied to the inner surface of the shoe’s existing tongue and extending to a point just anterior to the vamp.

Figure 18.3 (A) Incorrect foot position when tying shoelaces. Note the poor security of the heel at the posterior counters. (B) Correct foot position when tying shoelaces, with the heel secured.
An alternative to laces, particularly in women’s shoes, may be the incorporation of a strap that is attached anteriorly at the shoe quarters crossing the forefoot from the medial to the lateral quarters. It is typically held in position using a buckle or hooks and loop attachments. To be effective in retaining the position of the foot this strap must be broad enough and must be attached when the foot is held in the same position as when lacing. In women’s footwear a variation of the forefoot strap is the T-bar strap. The monk-style shoe for men, in which the shoe is retained in position by a side buckle attaching an extension of the medial quarter to the lateral quarter, may be a suitable alternative to lacing shoes (Fig. 18.4).

Close-fitting medial and lateral quarters
A comfortable close fit of the medial and lateral quarters of the shoe will complement the retaining mechanism provided by either laces or strap. The close fit of the quarters around the tarsal region of the foot will also reduce the incidence of the heel sliding medially or laterally and creating frictional stress on the plantar and posterior aspects of the heel. The quarters, ideally reinforced with counters, are required to embrace the rear of the foot and permit normal subtalar, midtarsal and ankle joint function. When examining the weight-bearing foot, with the shoe correctly retained on the foot, the examiner should not be able to identify any gap between the medial and lateral aspects of the foot and the quarters. The medial quarters are positioned slightly higher on the foot than the lateral quarters. This reflects the higher medial longitudinal arch and ensures a good fit around the anterior tarsal and metatarsal region of the foot. They should be shaped to reflect the narrower shape of the hindfoot below the medial and lateral mallelous when compared to the relatively wider plantar aspect of the heel. On the shod foot the quarters should be shaped and positioned in order not to cause irritation to the malleoli or the Achilles tendon. In a shoe that is worn correctly there should be no mediolateral or anteroposterior drift of the foot during gait. Similarly, there should be no evidence of the rear part of the shoe slipping off the heel area of the foot.
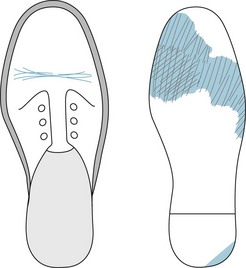
The quarters of the shoe must be robust enough to withstand the frequent insertion and removal of the foot from the shoe. This is achieved by the selection of good-quality materials, the incorporation of an effective counter and the utilisation of a backstay. It should be noted that poor, slovenly habits used to insert or remove the foot from the shoe without undoing the retaining mechanism rapidly result in destruction of the quarters. This results in poorly fitting footwear with inadequate retention of the foot, giving rise to potential foot strain and many other pathologies (Fig. 18.5).

Figure 18.5 Habitual insertion and removal of the foot from the shoe without untying laces leads to breaking down of the quarters and poor retention of the foot in the shoe, and results in chronic foot strain.
CASE STUDY 18.1 THE IMPORTANCE OF ESTABLISHING TYPICAL EVERYDAY FOOTWEAR HABITS AND PRACTICE
A retired woman aged 67 years attended the clinic complaining of a pain in both feet of at least 6 months duration. She stated that she felt less able to carry out her domestic chores and physical activities, and had become reliant on her husband to do the shopping and tend to the garden, etc. The pain was initially described as ‘aching all over both feet’. On questioning, it was established that, while the pain was now present on weight bearing and at rest, at the time of onset the pain was localised to the medial aspect of the rearfoot of both feet and occurred only after weight bearing. Further questioning established that the ‘general’ pain was now bilaterally focused in the region of the talonavicular joint, plantar heel pad, metatarsal heads and posterior aspect of the lower leg. Rest provided mild relief, but further weight bearing increased the intensity of the pain. Using a visual analogue scale (VAS) the pain was reported to be at its best 4 and at its worst 8.
The patient’s general health was good; all pedal pulses were steady, strong and palpable. There were no sensory or motor deficiencies; the skin was mildly anhidrotic. Non-weight-bearing examination revealed some hypermobility of the subtalar joints. The metatarsophalangeal joint motion was unrestricted and within the normal range. Examination of the ankle joints revealed a bilateral ankle equinus, and a maximum dorsiflexion of the ankle being restricted to approximately 3° of plantar flexion. There were no other significant structural abnormalities.
Weight-bearing examination revealed lowering of the medial longitudinal arch, with associated abduction of the forefoot, mild clawing of the lesser toes and prominence of the talonavicular joint. Current medication consisted of an anti-inflammatory drug that had been prescribed by the patient’s family doctor when she presented with her initial symptoms. The footwear worn was lacing, with adequate heel height, shock absorption and toe-box accommodation. It was noted, however, that the shoes had been removed prior to the examination without undoing the laces.
The patient reported that prior to developing the symptoms she enjoyed walking, participated in weekly swimming sessions and was a keen gardener. As a result of her foot pain she had noticed that she had increased in weight, and she blamed this on her relative inactivity. Her main activity now was housework; leisure walking was now minimal due to the pain. On asking the patient what she wore on her feet when working in the house she explained she always wore her slippers as they were ‘roomy’ and felt very comfortable. Frequently, to avoid having anything on her feet, she would be barefooted and conduct her household chores in this manner, as she assumed it was better to have nothing on her feet rather than be restricted in footwear.
Following the examination and history taking, a diagnosis of chronic foot strain was made. It was concluded that the presence of ankle equinus, in the absence of any other significant structural abnormality, had resulted in compensatory pronation at the subtalar joint. This rendered the feet inefficient, not only as a lever during gait but also as a mobile adaptor. Initially this resulted in a local tensile stress on the calcaneonavicular ligament. In association with the hypermobility of the subtalar joints, this resulted in poor foot posture during stance and gait, rendered the forefoot hypermobile, and gave rise to overloading of the metatarsal heads in addition to chronic ligamentous strain in the rearfoot and forefoot joints. The failure of the patient to lace correctly the shoes worn outside resulted in rearfoot instability and forefoot hypermobility, giving rise to chronic ligamentous strain. A further contributing factor was the wearing of slippers that offered no significant support to the hindfoot and offered little to compensate for the ankle equinus or permit functionally uncompromised weight bearing for the heel. This was compounded when the feet were unshod during significant weight-bearing indoor activity.
The first line of management was to explain, in lay terms, the cause of the foot strain and have the patient understand that a significant cause of her discomfort was a result of poor use of what were satisfactory outdoor shoes and the inappropriate wearing of slippers, or going barefooted, while in the house. The poor lacing practice was addressed by demonstrating the correct method of shoe lacing, with the foot on the ground in a dorsiflexed position and the heel firmly at the back of the shoe with the quarters closely fitting. The need for the foot to be supported while indoors and performing household chores and activities was emphasised. It was recommended that the patient used a pair of shoes, similar to the ones she wore to the consultation, but dedicated to wearing in the home when working and weight bearing. Reinforcing this recommendation, she was advised that slippers should be worn only when physically resting or when weight bearing for only a very short interval.
The patient was reviewed 6 weeks later and having followed the advice given stated that the pain had all but resolved (when present it was only after significant period of activity) and was scored as 1 on the VAS. She was now doing her shopping and other outdoor activities in comfort, and habitually kept shoes on while carrying out her chores indoors. She reported that she no longer went barefooted and reserved her slippers for relaxation while watching television or reading.
This case demonstrates the need to consider not only the appropriateness of the footwear presented to the podiatrist at consultation, but also to confirm that footwear is being used and retained on the foot correctly. It also demonstrates the importance of questioning the patient with regard to footwear habits while indoors, and making appropriate recommendations. Finally, the case highlights the importance of identifying and managing the source of the patient’s complaint.
Adequate width and depth in the toe box
Normal toe function during gait with efficient intrinsic and extrinsic muscle action requires unrestricted toe movement. During stance and gait the toes should not be in direct contact with the toe end of the shoe and the toe puff should not exert pressure directly onto the nail plate. Adequate toe-box width and depth is often difficult to ascertain, and in used shoes is best examined by the practitioner feeling directly into the toe box of the shoe to identify any depression or wear of the lining material within that area. If wear or tear is present this is often the result of direct and repeated impact of a toe into the toe box. When width and depth are inadequate, examination of the outer toe box also reveals a distension of the upper material as the toe presses on the upper of the toe box. The presence of these abnormal features may confirm inadequate width and depth of the toe box, but consideration must also be given to the possibility that shoes that are too long, or poorly retained in position, may result in a forward shifting of the foot within the shoe during gait and may result in toe box impact. A similar outcome may also result from wearing shoes that are too short.
There is no standard amount by which any shoe should extend beyond the longest toe. The amount of room provided by shoe manufacturers is variable and is dependent on many factors, including the style and shape of the forepart of the shoe. It is important that the practitioner, through examination of the foot and questioning of the patient, can establish that during gait under normal walking circumstances the shoe provides the necessary accommodation to ensure that the toes are not in direct contact with the toe box.
Correct length
Shoe designers and manufactures consider many factors that influence the length of shoes, including the style of the shoe, the toe shape and the growth allowance for children’s shoes. The podiatrist is interested in the length of shoe relative to the adequacy of the accommodation it provides relative to normal foot function. The result of wearing shoes that are too short or too long is particularly seen in the digits, where impact within the toe box gives rise to toe abnormalities, hypertrophic nail pathologies, an increase in the transverse curvature of the nail plate and articular damage to the joint surfaces of the toes and metatarsophalangeal joints.
The appropriate length of a shoe is determined by the use of a shoe-fitting device (a variety of which are currently in use), the skill and knowledge of the experienced shoe fitter about the footwear, and the response of the wearer of the shoes on trial. People may have subtle differences in the length of the right and left feet, and the shoes provided should accommodate the larger foot unless significant size differences are encountered. The smaller foot may be better accommodated within the shoe through the use of a pad applied to the inner surface of the tongue. Commercially available heel grips are of limited value as they may cause a widening of the quarters, reduce the close fit at the rear foot and serve to push the foot forward into the toe box of the shoe.
The use of a measuring device is not considered by reputable shoe retailers as the definitive means of identifying the correct size of shoe required. Similarly, it is unwise to consider that if one pair of shoes of, for example, a size 7 provides a comfortable fit then all shoes sized 7 will also give a comfortable fit. Subtle differences in the shoe and last design, manufacturing process, the sizing system in use and the country of origin of the shoes may all influence the ability of the shoe to accommodate the foot adequately. It is recommended that when purchasing footwear some time should be spent on ensuring that the correct length (and breadth) is achieved and that the services and advice of a reputable shoe retailer and fitter are sought.
The podiatrist may test to confirm that the length of a shoe is satisfactory by examining the shoe on the foot of the patient. When the shoe is correctly applied and laced there should be no gaping at the medial, lateral and posterior quarters. On palpation, the position of the metatarsophalangeal joints should coincide with the broadest part of the shoe at the tread line. The toes should be able to move freely within the toe box and the hallux should be able to be extended before pressure from the inner surface is noted. The toes should not be in direct contact with the end of the shoe. Finally, gentle depression on the toe box area should reveal approximately 10–12 mm of available toe space beyond the longest toe (Fig. 18.6). To assist in determining the suitability of the length of the shoe, examination of the hosiery worn by the patient whose shoes are too short frequently reveals a hole in the area accommodating the apex of the longest toe. Questioning of the patient may also reveal that the appearance of holes in hosiery occurs rapidly and repeatedly. It must be remembered that in many cases the longest toe is the second toe.

Correct width fitting
Adequate width fitting is of equal importance to length fitting. The correct width fitting of a shoe is achieved when the foot is accommodated in such a way that the toes are straight, unrestricted and maintain the normal relationship of one to the other during gait.
Many foot-measuring devices give a fitting scale measurement based on the measurement seen between two parallel lines that represent the widest part of the foot. This measurement is usually given an identifying letter. For example D is considered to be an average width. while B is narrow and G is broad. (Between each increase in full size of shoe there is a corresponding increase of approximately 6 mm in the girth measurement of the shoe. Some manufacturers produce shoes of the same size but with a range of girth measurements or fittings that accommodate both the narrow and broad foot within one length fitting.) The widest part of the foot is normally transversely between the first metatarsophalangeal joint and the fifth metatarsophalangeal joint. This measurement, when used in association with the length measurement, suggests the most appropriate width fitting for a particular pair of feet. While this is an important measurement, attention should also be drawn to the part of the shoe distal to the metatarsophalangeal joints. If this part tapers too greatly, the first and the fifth toes, and the other lesser toes can frequently be subjected to damaging pressure.
Examination of the foot relative to the width available in the forepart of the shoe will indicate whether there is any inadequacy on the medial, lateral or both aspects of the forepart. This will dictate the shape of the forepart of the shoe best suited to the foot in question. It is often found that the recommendations made by the podiatrist regarding the shoe shape and shoe width are in stark contrast to the shape preferred by the patient.
Examination of the forepart of the shoe when on the patient’s foot to establish the appropriateness of the width should not evidence medial or lateral forced stretching of the quarters and vamp over the outsole of the shoe. Similarly, neither the hallux nor the fifth toe should be seen to exert undue pressure on or distort the upper of the shoe. Tightness to the vamp is suggestive of inadequate width. Examination of the shoe internally may reveal an indentation of the upper where the compressed digit is forced to stretch the upper in an attempt to achieve better accommodation. Conversely, if the vamp area is loose, excessively creased and puckers easily when the thumb is run across the forepart of the shoe, the shoe is too wide.
Adequate heel seat
Shoes are largely reliant on the retaining mechanism and the close fit of the quarters to ensure security on the foot. To function in harmony with the foot and eliminate undesirable movement shoes must be firmly attached around the rear of the foot and the tarsometatarsal region, and permit the toes at the metatarsophalangeal joints to function normally in an unrestricted manner.
The rear quarters must be narrow enough to hold the rear of the foot firmly. It is necessary for the designer of the last to ensure that the heel seat of the shoe is wide enough to accommodate the relatively broad heel of the foot. The relationship of the heel seat to the posterior medial and lateral quarters on cross-section forms a triangular-like shape when correctly designed. This acknowledges the narrowness of the foot below the malleoli and the breadth at the plantar surface of the heel. This shape at the rear of the shoe, which may be described as ‘wedging’ the rearfoot in position, contributes to the retention of the foot within the shoe.
The heel seat must accommodate the heel of the foot. If it is too wide it may allow the heel to drift during wear, making the foot insecure within the shoe. This repeated drifting of the heel may result in the formation of diffuse callus on the plantar aspect of the heel or, in severe cases, the development of plantar calcaneal bursitis. Poor retention of the hindfoot within the shoe may lead to chronic strain on the joints and ligaments of that area, and may contribute to the development of chronic foot strain. In time, secondary to the poor retention of the foot within the shoe, a variety of symptoms may be experienced in the forefoot. A heel seat that is too narrow will cause the soft tissue on the plantar aspect of the heel to be effectively wedged into the junction of the heel seat with the quarters, and may cause a ridge of tightly packed callus to form on the peripheral aspect of the heel.
Examination of the foot within the correctly applied shoe where the heel seat is too broad may reveal a gaping of the medial and lateral quarters. The examiner’s finger may be able to be inserted between the rear foot and the quarters, making contact with the heel seat. Where the heel seat is too narrow, a tightness and forced stretching of the rear quarters will be noted and the patient will describe a feeling of fullness in the rear of the shoe. Dense callus may form on the peripheral borders of the heel.
Heel height no greater than 2 inches (5 cm)
Heels are a fashion accessory to footwear, rather than contributing to ‘natural gait’ during wear. No other part of a shoe is subjected to such change and variety by shoe designers as the heel. Examination of footwear available from shoe retailers reveals a variety of heel heights, widths and shapes. Shoe heel height is variable. Consideration of the concept of ‘natural’ gait opposed to ‘normal’ gait leads to the realisation that the presence of a heel is not necessary for natural foot function. Any footwear worn should allow the foot to function as naturally as possible, and therefore the conclusion is that the absence of a heel from a shoe could be a distinct advantage. The inclusion of heels on footwear is well established and today they are considered to be an integral part of footwear design. Heels can contribute to an imbalance in body-weight distribution between the forefoot and the hindfoot. An increase in heel height can transfer greater body weight to the forefoot. An increase in heel height causes an increase in the angulation of the heel seat from the horizontal, which causes an increase in the thrust of the forefoot into the toe box of the shoe. The higher the heel the more anteriorly positioned is the centre of gravity of the body. As a consequence, the wearer of high-heeled shoes must extend the lumbar spine to maintain upright posture and good balance. This can result in lower back discomfort in addition to the local foot pathologies (e.g. ankle equinus) that may result from the modified, unnatural way the foot is required to function if held in this abnormal position.
To prevent significant overload of the forefoot it is recommended that the heel height should not exceed 5 cm.
Broad heel base in contact with the ground
It is vital to consider the surface area of the heel in contact with the ground during stance and gait. Many women’s shoes may have an acceptable height of heel but a narrow heel breadth offers little stability to the body due to the small area of the heel in contact with the ground at heel-strike. Some women’s fashion shoes offer as little as 1 cm2 of heel contact area. In such cases the outer part of the heel in contact with the ground is made of steel or other hard-wearing plastic material. During heel-strike the efficient transmission of body weight to the weight-bearing heel is significantly jeopardised due to the poor traction properties of the outer part of the heel coupled with the inadequate ground surface contact provided by the narrow heel. Frequently this type of heel results in inversion strains and can lead to fractures at the styloid process of the fifth metatarsal or to more severe ankle fractures.
Ideally, the ground contact surface of the outer part of the heel should be broad and, where possible, extend beyond the parameters of the heel seat of the shoe.
Upper material made of leather or other natural material
The upper of any shoe is subjected to flexion and extension, particularly over the area of the vamp corresponding to the metatarsophalangeal joints. To withstand the wear at this area the material must be hard-wearing and maintain the necessary flexibility to permit the required movement. The plasticity of the material during the shoe-making process (i.e. its ability after distortion, or moulding around a shoe last, to retain the new shape produced) makes leather the most suitable material from which to manufacture the shoe upper. Leather provides the benefits of being plastic when moulded; however, when stretched over the last only a residual amount of the plasticity remains within the material. The remaining plasticity allows for minor adaptations by the material when the shoe is worn and effectively accommodates the foot allowing the shoe to ‘give’ or ‘break-in’.
Leather also provides elastic properties during wear (i.e. the ability to completely recover shape after distortion such as stretching and compression). Bending of any material, as occurs on the vamp of the shoe, requires the stretching of the layers on the outside of the bend and the compression of the layers on the inside of the bend. Failure of the upper to provide elastic properties results in a shoe that does not provide a close fit around the foot and rapidly loses its shape and proportion.
The permeability of shoe leather is important. The ability of the upper to transmit water, air and vapour is an important quality to achieve maximum foot comfort. The perspiring foot relies on the absorption and evaporation of moisture to ensure maintenance of healthy skin. Many synthetic materials are not permeable and therefore result in the accumulation of perspiration on the foot. Prolonged use of footwear incorporating this type of material frequently leads to local hyperhidrosis and the associated skin pathologies that result from a reduction of the skin’s natural resistance to tensile stress. Failure to perform rigorous foot hygiene may result in the decomposition of the sweat and sebum and give rise to bromidrosis.
FOOTWEAR AND LAST TERMINOLOGY
When examining or recommending footwear it is necessary to consider important elements of last design and footwear construction that may influence how well or naturally the foot functions when shoes are worn.
Tread line
The term ‘tread line’ refers to the part of the shoe that is in direct contact with the ground surface at the forepart of the shoe when the heel height, pitch and the toe spring are correct (Fig. 18.7). The tread line lies at an oblique angle across the forepart and runs from the first metatarsal head to the fifth metatarsal head. As the term suggests, the tread line corresponds to the widest part of the forefoot at the metatarsal heads. With normal wear, and in a well fitting shoe, it is this area of the forepart of the outsole where the greatest amount of wear occurs. It is at this point the foot bends when walking. The vamp is the part of the upper subjected to flexion and extension as the foot bends at the metatarsophalangeal joints and is located in the upper above the tread line.
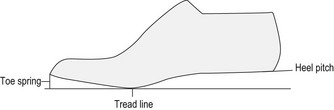
Figure 18.7 A last standing correctly on the tread line, displaying the corresponding heel pitch and toe spring.
It is important that, where possible, the mildly oblique angle created by the position of the first relative to the fifth metatarsophalangeal joint of the foot matches that of the tread line of the shoe. In reality this often differs slightly, which results in compression of the fifth toe by the upper of the shoe distal to the tread line. This is due to a reduction in the angle of the tread line relative to that of the metatarsophalangeal joints. The dynamic foot flexes slightly distally to the tread line, and this may contribute to compression of the lesser toes. Similarly, people with a relatively long medial longitudinal arch may find that in some shoes the tread line is positioned too far posteriorly and that, while the shoe appears to be the correct length in relation to the toes, accommodation within the shoe is poor across the metatarsophalangeal joints and as a result compression of the forefoot occurs.
Toe spring
The toe spring of a shoe or last is defined as ‘the elevation of the toe end of the last from a horizontal surface when the seat is raised to its correct height (pitch) so that the last is standing correctly on its tread line’ (Ceeney 1958). The toe spring of the shoe will reflect the same elevation as that incorporated in the design of the last on which the shoe is made.
The toe spring reduces the resistance to flexion that the shoe will place on the foot when it is flexed at the metatarsophalangeal joints and while the heel is raised during the propulsive phase of gait. Effectively, the presence of the toe spring at the toe end of the shoe serves to reduce the amount of flexion required at the metatarsophalangeal joints to produce propulsion and reduces foot fatigue when walking a distance. The toe spring also helps to reduce the amount of wear and tear that occurs at the vamp.
The amount of toe spring incorporated in the design of a last (and shoe) is dependent on the level of resistance to flexion that will be encountered by the shoe when worn. A number of factors influence the height of the toe spring, including the rigidity of the outsole, the style of shoe, heel height and heel pitch.
Rigidity of the outsole
The more rigid the outsole of a shoe the greater the effort required for the foot to flex the outsole to permit propulsion. Footwear incorporating rigid outsoles (e.g. the army boot) always incorporates a high toe spring to reduce the effort required by the foot to flex the outsole and to compensate for the shoe or boot’s resistance to flexion (Fig. 18.8). An extreme example of a high toe spring is seen in the traditional wooden clog where no flexion is available. The incorporation of an exaggerated toe spring allows the wearer to effectively ‘rock’ forward on the shoe using the forward shift of the body’s centre of gravity to create the rocking effect on the outsole of the clog and permit propulsion. In contrast, shoes with thin outsoles that offer little resistance to flexion have significantly less toe spring incorporated in the design of the shoe.

Style of shoe
Court shoes and slippers usually incorporate flexible outsoles that offer little resistance to flexion. This suggests that there is no need to incorporate a toe spring in the design of the shoe. However, in the absence of any retaining mechanism in these types of shoe the manufacturer often incorporates a higher than necessary toe spring. This is done to ensure that downward pressure of the toes within the toe area of the shoe during wear will effectively reduce the toe spring and result in the quarters of the shoe being pulled against the rear foot and ankle, thereby providing a more secure fit. This tends to work best when the shoes are new.
Heel height
The height of the heel also dictates the height of the toe spring. The foot subjected to a higher heeled shoe is automatically placed in a position where the metatarsophalangeal joints are held in a dorsiflexed, propulsive position. The lasts created to manufacture high-heeled shoes only incorporate a small elevation as a toe spring, the function of which is to prevent the toe end of the shoe scuffing against the ground during gait.
Heel pitch
The term ‘heel pitch’ refers to the angle of elevation of the heel seat of the last from the horizontal surface, when the last is standing correctly on its tread line. The heel pitch is largely dependent on the heel height, and fluctuates relative to the heel height of the shoe. An overshort heel relative to the heel pitch results in an increased toe spring, and causes the shoe to fall backwards during stance or when the shoe is standing on a horizontal surface. When the foot is placed in such a shoe the metatarsophalangeal joints flex and extend at a more posterior position relative to the tread line of the shoe. If the heel is too high, the shoe is tilted forward, with a corresponding decrease in the toe spring. When the shoe is worn, the metatarsophalangeal joints flex and extend in a more anterior position than the shoe’s tread line. An incorrect relationship between the heel pitch and the heel height results in an unbalanced shoe and a reduction in comfort during wear.
During stance the centre of the body weight falls slightly anterior to the ankle joint. Any significant increase in heel pitch, and consequently the height of the heel, results in the centre of the body weight being positioned more anteriorly. To compensate for this and to maintain balance there is a need to extend the lower back. The greater the heel pitch or height, the more the ankle joint is held in plantar flexion and the subtalar joint in an inverted position during the stance phase of gait. The potential for normal foot function is compromised, and prolonged walking in this position may give rise to a variety of foot pathologies and skeletal symptoms affecting the lower back.
Flare
The term ‘flare’, sometimes referred to as ‘form’, refers to the shape of the last or shoe relative to the position that the centre of the heel seat occupies in relation to the forepart. Examination of the relationship between the undersurface of the forepart of the shoe to the centre of the heel in a last or a shoe produced for an adult shows that there is a greater forepart tread width on the inner medial side of the shoe compared to the lateral side. A line from the centre of the heel seat projected forward to bisect the tread line in the forepart reveals the relationship between the medial and the lateral aspect of the tread (Fig. 18.9). A greater tread area on the medial border of the line indicates that a shoe is ‘in-flared’. Tread width that is equal on either side is ‘straight-flared’, and if the lateral tread has a greater surface area the shoe is ‘out-flared’.
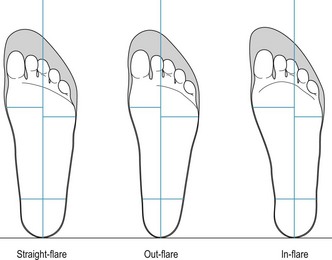
Figure 18.9 Examples of the variety of flares incorporated in footwear. Note the relationship of the centred heel to the accommodation available in the forepart of the shoe relative to the forward extension of the centred heel line.
If a similar examination is made of feet it will be noted that there can be a wide variation in the relationship of the forepart to the central heel. This variation is clearly shown when comparing a pes plano valgus with a pes cavus. The former reflects an out-flared structure, while the latter is more suggestive of a straight-flared structure. A typical healthy adult foot displays little variation on either side and is more in keeping with a straight-flare or a slight in-flare.
If a foot is subjected to a shoe that does not have a corresponding flare it is poorly accommodated and is subjected to considerable stress. If a pes plano valgus foot is subjected to an in-flared shoe, in addition to the distortion that will occur at the hind part of the shoe, the lesser toes, due to the abduction of the forefoot, will be subjected to considerable pressure from the lateral aspect of the forepart of the shoe. This abnormal pressure will be seen in the shoe by distortion of the lateral aspect of the toe box, which may overhang the outsole.
The podiatrist should always consider what extrinsic influences might affect the foot. Frequently, footwear, and in particular the flare of the shoes being worn, is unsuitable and may be directly responsible for the patient’s symptoms.
DESIRABLE FEATURES OF FOOTWEAR FOR SPECIFIC FOOT CONDITIONS
The podiatrist is required to make footwear recommendations according to the specific foot condition with which the patient presents. The standard recommendations stated above may require to be supplemented with some additional and specific features associated with the nature and severity of the patient’s complaint.
It is acknowledged that the severity of some foot conditions necessitates the provision of bespoke or semi-bespoke footwear. Before the patient’s condition advances to this stage it is often possible to recommend specific commercially available shoes that will offer the required level of comfort and accommodation for the foot without the expense of custom-made shoes. Below are listed a variety of foot types and the desirable features that may be incorporated within the footwear worn by the patient. The podiatrist must have good knowledge of the various suppliers of a wide range of commercially available specialist footwear and advise patients on how this may be acquired.
Hallux abducto valgus
Hallux limitus/rigidus
The highly arched foot
SIZE SYSTEMS AND SYSTEMS OF MEASUREMENT
A size system is a method of measuring the length of feet, lasts and shoes using a specific unit of measurement. When measured a descriptive size number is allocated; this is known as the ‘notation’. In the UK two principal size systems are in use: the English size system and the Continental size system. Each has its own unit of increase between sizes and its own notation.
A measurement system that facilitates a regular increase in girth measurements relative to an increase in length measurements, and provides a range of girth measurements for individual sizes, is known as a ‘girth measurement system’. Where shoes of one size are available in different girth measurements this is known as ‘fittings’. Fittings are identified by letters; for example, A denoting a narrow fitting and E denoting a broad fitting. There are significant design, manufacture and production costs to providing shoes in different fittings, and consequently the availability is limited to some of the more established manufacturers of both children’s and adults’ shoes.
A ‘heel-to ball’ measuring system measures the distance from the posterior aspect of the heel to the first metatarsophalangeal joint in addition to the heel-to-toe measurement. The scale used in this system gives a shoe size that is considered appropriate for feet with the particular heel-to-ball measurement. This system is based on the observation that the length of the typical foot from the heel to the first metatarsophalangeal joint is seven-tenths that of the heel-to-toe length. When using this system the desirable outcome is that feet measured from heel-to-toe and heel-to-ball should arrive at the same measurement, albeit from the different scales used for each measurement. When this ideal outcome is achieved, the corresponding shoe size fitted will accommodate the widest part of the foot and will bend correctly at the tread line. Problems may arise when the heel-to-ball measurement of the foot is longer than the heel-to-toe measurement. If the heel-to-toe measurement is used to fit the shoes, the widest part of the shoe will not correspond to the widest part of the foot and this will result in pressure on the forepart of the foot beyond the metatarsal heads. In addition, the shoe is designed to bend at the tread line, which, in the case highlighted, will be positioned slightly posteriorly to the corresponding widest part of the foot. This may lead to undue pressure on the foot and give rise to discomfort.
The English size system
This well-established size system has a unit of increase of one-third of an inch (8.5 mm) between full sizes. Therefore, within a 1-inch measurement there are three full sizes. The English size system includes half sizes, one-sixth of an inch (4.25 mm) between that of the full size. The notation that allocates a size number to the measurement made commences at size 0 (zero), which is four inches (102 mm) in length. Size 1, therefore, is four and a third inches (110 mm) in length, size 2 is four and two-third inches (118 mm) and size 3 is five inches (127 mm). The notation is continuous up to size 13, following which it is repeated from size 1, giving rise to the adult sizes. The repetition of the notation can give rise to confusion in sizes and it is usual to identify the size with the prefix ‘children’s’ or ‘adult’s’.
The Continental size system
The Continental size system is arguably the simplest system and is commonly used. The unit of increase in this system is two-thirds of a centimetre; this unit is referred to as the ‘Paris point’. Within a measurement of 2 cm there are three Paris points. Due to the smallness of the unit of increase there are no half sizes in the continental size system. The notation is simple in its application, with size 1 being 1 cm in length. It is continuous, without any repetition in the adult size range (Table 18.1).
Table 18.1 Adult shoe size conversion table
| English | Continental |
|---|---|
| 5 | 38 |
| 6 | 39 |
| 7 | 41 |
| 8 | 42 |
| 9 | 43 |
COMMON FOOTWEAR STYLES
Examination of the stock held by any shoe retailer will confirm that the choice of shoe style is varied in the ranges for both men and women. Cost, fashion and proposed activity frequently dictate the type of footwear selected. Within each broad category of footwear are assortments of styles and designs from which a particular pair of shoes may be selected. These variations permit the manufacturer to reflect fashion trends. For example, court shoes, so popular with women, may be manufactured with high heels, low heels, backless and sling-backed.
Tie lace
The tie-lace shoe, although worn more frequently by men for business, is also available to women. The adjustable retaining mechanism offered by the laces, when correctly used, serves to minimise undesirable drift of the foot within the shoe and makes this the preferred style of shoe recommended to patients by podiatrists.
The Oxford shoe
The Oxford shoe is distinctive by a decorative toecap attached to the distal end of the upper over the toe box. The vamp is stitched posteriorly to the quarters. The anterior medial and lateral quarters of the shoe, when laced correctly, closely oppose each other over the dorsal tarsal area of the foot. The quarters house the eyelets through which the laces are threaded. Typically, the Oxford shoe has five pairs of eyelets. The potential for pressure on the dorsal aspect of the foot from the laced quarters is reduced by the provision of a tongue. In the Oxford shoe this is attached separately and is stitched anteriorly to the undersurface of the vamp. A more decorative variation of the Oxford shoe is seen in the brogue. The upper of this shoe is pinked and has numerous perforations. The more fashionable brogue shoe worn today is derived from the practical origins of the shoe. Originally a footwear style favoured by Irish land workers, the perforations in the upper material allowed for the evacuation of water when walking in the wet marshy ground of the Irish bog lands. The brogue shoe is very popular and is styled in versions for both men and women. The need for a close apposition over the tarsal region of the foot of the anterior end of the quarters when the shoe is laced means that the Oxford shoe may not be suitable for a foot with a high arch.
The Derby shoe
Often referred to as a ‘Gibson shoe’, the Derby is a variation of the tie-lace shoe. It is simple in design, with the vamp extending under the anterior medial and lateral quarters to form the tongue of the shoe. Unlike the Oxford shoe, the anterior quarters of the Derby do not directly oppose each other when tied correctly. When untied and the quarters are loosened and pulled back there is greater accessibility for the foot to the inside of the shoe. These features are important when shoe recommendations are made for people with broad feet or highly arched feet. In contrast with the Oxford shoe, it is usual for the Derby shoe to have only three pairs of eyelets (Fig. 18.10).

The moccasin-style shoe
This popular style of shoe is based on the traditional North American Indian footwear. Typically made of buckskin, the sole of the shoe and the medial and lateral borders are composed of one piece of material drawn from the plantar aspect of the foot over the dorsal aspect of the forefoot. An ‘apron’ front, which is attached by stitching, covers the toes and the dorsal aspect of the midfoot.
Modern tie-lace and slip-on shoes made in the moccasin style (e.g. loafers) are popular and tend to be worn for more casual occasions. Many people with healthy good functional feet find the shoes comfortable, as they can exhibit many of the desirable features of a good-fitting shoe. However, care should be taken when recommending this style of shoe. If worn by individuals who have prominence of joints, as in hallux abducto valgus or lesser toe abnormalities, care must be taken that the stitching of the apron front to the upper of the shoe and the resultant internal seam does not cause pressure on the skin over the prominent joints (Fig. 18.11). In quality moccasin style shoes, manufacturers frequently incorporate linings that protect the forefoot from the seam of the apron attachment.

The sandal
The sandal, with its simple design and openness, was the standard footwear style of warm Mediterranean countries. The basic sandal provided a simple method of protecting the sole of the foot. As the use of the sandal moved further north with the advancement of the Roman Empire, adaptations were made to provide greater protection to the foot and lower leg, and gave rise to the development of the shoe and boot. The first crafted foot covering, the simple sandal, has provided shoe designers with an opportunity to create endless variations of this basic shoe design. Sandal design can be very simple, creating a means of protecting the sole of the foot. Retention is achieved by the incorporation of various foot and ankle straps that arise from the sole. In contrast, the basic sandal design can be transformed by fashion shoe designers to an elegant foot covering worn by fashion-conscious women as an integral part of a designer outfit. While sandals vary widely in appearance they can be categorised into three distinct styles.
The court shoe
The term court shoe (referred to in North America as a ‘pump’) is thought to have originated in the reign of Henry VIII who had chronic gout and needed to wear footwear that readily and easily accepted a swollen and painful forefoot. Royal courtiers were commanded to wear a similar style of footwear when in the King’s presence in order that attention was not drawn to the King’s foot disorder. The consequence of this royal decree was shoes that slipped onto the feet with a typically squared off broad forefoot, referred to as ‘court shoes’, which are commonly worn today. Male versions are slip-on style shoes, while women’s court shoes have various styles and appearances, ranging from simple slip-ons to more elegantly designed and expensive dress shoes.
Court shoes must rely on a close fit to the foot for retention; many have a higher than necessary toe-spring that is depressed by the pressure from the toes, resulting in a closer, although temporary, fit of the shoe around the posterior, medial and lateral borders of the heel (Fig. 18.12). Prolonged wearing of a slip-on shoe often results in poor retention of the shoe on the foot because of the tendency of the quarters to stretch and gape away from the medial and lateral borders of the foot.

Sports shoes
Sports participants require footwear with a range of features that permit performance of activities with maximum efficiency. A wide variety of sports shoes are commercially available, each with particular features specific to the sporting activity for which they are intended. In general, sports shoes have many desirable features that the podiatrist would recommend for regular wear. It must be remembered, however, that sports shoes suit more leisurely attire. When making footwear recommendations the podiatrist should be conscious that not all patients will accept the concept of wearing trainers nor be realistically expected to wear them to business. It is necessary for the podiatrist to consider what features of the sports shoe are required for the individual patient, and be knowledgeable about current footwear styles and trends in order to direct the patient to an appropriate traditional footwear brand that also exhibits desirable features. (See the discussion of sports shoes in Ch. 13.)
Boots
Boots were originally reserved almost exclusively for wear by men, with the exception of riding boots. Fashion boots are now popular with both sexes, but are also utilitarian and worn by the armed forces, land workers, tradesmen, and fire service and police personnel. Wellington boots are worn by many and are frequently worn by farmers or are reserved for wear in inclement weather or for walking in wet and marshy ground.
The various styles of boot, including the ankle boot and the knee-length boot, are usually retained on the foot and lower limb by a variety of mechanisms. To be retained in position fashion boots frequently rely on the proximity of the material of the upper around the foot and lower limb. Frequently in the more fashionable women’s knee-length boots the inclusion of a zip, usually found on the inside of the boot, may contribute to retention of the foot and lower limb. The more practically styled boots invariably have laces to provide firm retention of the foot.
WEAR MARKS AS AN AID TO DIAGNOSIS
Examination of the wear marks occurring on the upper and the sole of shoes can give the podiatrist an insight to the structure and function of the foot and the features of the gait adopted by the individual. Careful examination of the shoe worn by the patient can serve to confirm a diagnosis of structural abnormalities of the foot. Often by the examination of shoe wear a diagnosis can be made of a potential abnormality before it becomes clinically apparent.
When examining the wear marks occurring on a shoe the practitioner must consider normal foot function and gait and how they influence the development of normal wear marks. This benchmark reference must then be contrasted with the wear observed on the shoes of patients with foot and gait abnormalities. Examination of the shoe should give consideration to the wear on the outsole and heel, the insole, the lining of the upper and the upper itself. No clinical examination should be considered complete until the footwear worn by the patient has been fully examined. The podiatrist must also ascertain that the footwear presented is that which is normally worn by the patient. Questioning the patient should reveal whether any other style of shoe is regularly worn. It is not unusual for patients to wear their ‘best’ shoes for the first visit to a podiatrist, which can be misleading when relating the footwear to the subjective symptoms. With experience and the application of anatomy and biomechanics theory the podiatrist can examine shoe wear and identify areas of abnormality and relate abnormal wear to gait alterations and presenting symptoms.
Wear marks should not be considered as standard; however, certain abnormalities and gait patterns do tend to present with typical patterns of wear. As a guide, typical wear patterns seen in the ‘normal’ foot and contrasted with those seen in association with common foot abnormalities are summarised below.
Normal wear
The outsole and heel
The insole (sock lining)
The lining of the upper
The upper
Wear marks seen in association with common foot disorders
Hallux limitus/rigidus
The outsole and heel
The insole (sock lining)
The lining of the upper
The upper
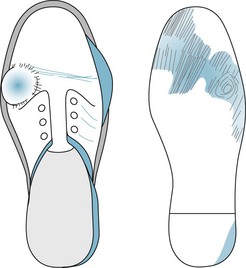
Pes cavus
The insole (sock lining)
The lining of the upper
The upper

Pes plano valgus
The insole (sock lining)
The lining of the upper
The upper
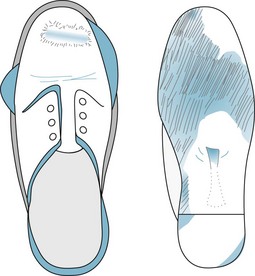
THERAPEUTIC FOOTWEAR
Introduction
Footwear is a valuable aid to any therapy designed to improve foot health. Footwear alone can resolve the consequences of many biomechanical anomalies, aid joint function, and reduce friction and pressure to which the foot might otherwise be subjected.
Effective footwear advice and prescription requires an understanding of the presenting foot pathologies and how footwear features are used to meet the needs of management. Assessing the foot for signs of trauma, deformity and limitation in function is part of the podiatrist’s professional role, and that expertise is employed when prescribing orthoses. The same criteria should be applied to the appropriateness of footwear with consideration of the features of the individual component parts of the shoe. Practitioners automatically examine footwear for signs of abnormal wear, creasing and suitability, but must also evaluate the fit and functionality of footwear and the way in which the various elements contained within the shoe or boot may be modified to improve foot function.
Indications for therapeutic footwear
The need for therapeutic footwear is indicated by a number of local or systemic conditions or if the feet are outside the normal size and fitting range of retail footwear. Therapeutic footwear is costly but often is the only option available or the most effective way of treating a condition (White 1994). Therapeutic footwear is indicated for a wide range of foot pathologies and many respond positively to the prescription of therapeutic/orthopaedic footwear. These vary from localised pathologies, including digital deformities, to multisystem conditions, such as diabetes mellitus. The diagnosis of pathologies does not necessarily indicate that therapeutic footwear prescription is required, rather the extent and severity of the condition is the guide for prescription.
Conditions that may benefit from therapeutic footwear prescription include:
Prior to prescribing therapeutic (orthopaedic) footwear, foot size, foot shape and biomechanical function is assessed. Footwear purchased from a retail outlet should be considered for modification. If the footwear is of a suitable style and material, a number of adaptations can be made. For example, a ball-and-ring stretcher can be used to stretch leather uppers to accommodate problems such as toe deformities and hallux abducto valgus; tongue pads and heel grips can be included to improve fit. Despite these options, there will be a small number of patients whose foot health needs can only be accommodated in specialist footwear (Fig. 18.17).

Figure 18.17 A ball-and-ring stretcher being used to stretch the upper of a shoe to accommodate a hammer toe deformity.
CASE STUDY 18.2 ROLE OF FOOTWEAR IN MANAGEMENT OF CHRONIC HALLUX LIMITUS
An otherwise healthy 52-year-old man presented complaining of pain from both first metatarsophalangeal joints. On questioning he confirmed that the joints had sustained no significant trauma and that the onset of the pain had been some considerable number of years prior to his attendance. Previously a keen walker, walking was now uncomfortable, mainly because of the pain in the affected joints. At its worst, the patient scored the level of pain as 8 on a visual analogue scale (VAS). In addition, he complained of pain from corns that had developed on the plantar aspect of both second metatarsal heads, and from callus on the plantar aspect of both fifth metatarsal heads and on the plantar surface of the interphalangeal joint of the first toes. On questioning, the patient stated that he experienced muscle pain in the posterior aspect of his lower leg, and occasionally strained the lateral border of both his ankles. These symptoms were experienced particularly when he walked a distance. A previous recommendation for orthopaedic surgery had been declined, and the patient was keen to explore what conservative methods of treatment were available.
On examination, the relaxed calcaneal stance position revealed long, narrow feet, excessive subtalar joint pronation with associated lowering of the medial longitudinal arches, abduction of the forefoot, and clawing of the lesser toes. Both first metatarsophalangeal joints were enlarged on the dorsal aspect. Non-weight-bearing examination of passive joint motion revealed a range of motion of 40°, with a direction of motion of only 20° dorsiflexion from the neutral position of the right first metatarsophalangeal joint. The left first metatarsophalangeal joint was similarly affected. Subtalar neutral examination revealed no significant hindfoot to forefoot structural abnormality; however, hypermobility of the joints of the rearfoot and at the lesser metatarsophalangeal joints was evident.
Examination of the patient’s footwear revealed a pair of Derby, lacing shoes. It was established that when wearing lacing shoes they were never laced firmly, the patient preferring to be able to slip them on and off. The upper at the toe box was both narrow and shallow, and a bulging of the upper, coinciding with the enlarged first MTPJ, was noted (see A). The outsole was thin, well worn and showed little evidence of a viable toe spring. Excessive wear was demonstrated on the lateral aspect of the heel. Examination of the forepart of the outsole displayed heavy tread wear at the second to fifth metatarsal heads and at the interphalangeal joint area of both first toes. In contrast, reduced wear was noted under the first metatarsal head (see B). The patient stated that an alternative shoe style was a slip-on shoe that he tended to wear for leisure.

The conclusion was made that the patient suffered from chronic hallux limitus. In view of the general joint hypermobility, the excessive subtalar joint pronation and the patient’s preference to wear either poorly tied or slip-on style shoes, it was considered that, combined, these elements served to cause repeated minor damage to the first metatarsophalangeal joints, which resulted in the chronic hallux limitus. The pain experienced in the posterior compartment of the leg was a result of overuse of the tibialis posterior muscle inverting the hindfoot during midstance and propulsion in order to direct load away from the painful first metatarsophalangeal joint, thereby overloading the fifth and second metatarsal heads and causing lesions. This avoidance gait and the continued use of inappropriate shoes also contributed to the lateral ankle strains. An overpull of the flexor hallucis longus provided the patient with a distal fulcrum point during the modified propulsive phase of gait, leading to a heavy callus on the plantar aspect of the interphalangeal joint of the hallux.
The inadequacy of the retaining medium on the footwear permitted the hypermobile foot to slip forward during use, resulting in repeated impact of the first metatarsophalangeal joint into the toe box of the shoe, causing osteoarthritic lipping on the dorsal aspect of the joint. The narrow and shallow toe box served to irritate the dorsal lipping and contributed to the clawing of the lesser toes. The thin outsole failed to provide any significant protection to the plantar aspect of the metatarsal heads, while the less than effective toe spring served to exacerbate the painful first metatarsophalangeal joint symptoms. The reduction in toe spring height negated any protective function, and it may have contributed to the painful first metatarsophalangeal joint in reducing the extent of dorsiflexion necessary for normal gait.
Careful explanation was given to the patient regarding the complexity of the causes of his symptoms and lesions. Conservative care was provided, with bespoke neutral casted orthoses to manage the hypermobility and excessive subtalar joint pronation. To accommodate the joint abnormality and promote a more normal gait, plain-fronted footwear incorporating laces, a broad and deep toe box, and a firm thick outsole with a high toe spring was advocated. It was stressed that, to receive maximum benefit from the proposed orthoses and footwear, the correct method of lacing must be adopted. The advice was well received.
At review, following the purchase of appropriately styled footwear and the fitting of the orthoses, the patient reported a significant improvement in symptoms and foot comfort. Posterior compartment muscle pain had been eliminated and no further lateral ankle sprains were reported. On questioning regarding the level of pain, a score of 2 was now reported on a VAS.
CLASSES OF THERAPEUTIC FOOTWEAR
Therapeutic footwear may be grouped into several categories:
Stock surgical, modular and bespoke footwear is also often referred to as ‘orthopaedic’ footwear.
Stock surgical footwear
Several manufacturers provide stock ranges of therapeutic footwear available for immediate delivery at a relatively low cost. Colours are basic, usually black or brown, but shoes are made in a wide range of sizes and fittings. Catalogues are provided by each manufacturer, with fitting details. The measurements given include size length, width at the metatarsophalangeal joints, girth at the metatarsophalangeal joints and instep girth. The width and girth measurements are in millimetres, and the length is given usually in the English size system. When measuring length, the gauge used must correspond to the manufacturer’s length units. Measuring sticks are available as foot-length sticks or as shoe-size sticks. Shoe-size sticks should correspond to the shoe size provided by the manufacturer, although each make of stick varies slightly in the readings given. Foot size sticks require that an additional allowance (generally two sizes) is added to the reading to establish the required shoe size. The sticks should be calibrated against the manufacturer’s sizing system prior to measuring.
Stock surgical footwear is available on a sale or return basis. This allows the practitioner to fit and advise without a commitment to purchase. A high percentage of patients requiring therapeutic footwear are fitted from stock. When a good-fitting shoe is identified, further pairs from the same last may be ordered in a different style and colour, but these are non-returnable and require to be paid for on ordering. Stock surgical footwear may be used when a raise is required to compensate for a limb-length discrepancy if the raise required is 1 cm or less. A higher raise requires alteration to the heel-height/toe-spring relationship on the last, and a bespoke prescription is required to meet individual requirements.
Modular and bespoke footwear
Feet outside the dimensions of shoes available from stock ranges require prescription of modular or bespoke footwear. Complex prescription is required and precise, detailed instructions must be given to the shoe manufacturer. Modular footwear relies on the modification of a manufacturer’s existing last, but modifications are limited to ensure that the existing shoe upper pattern pieces are large enough to include modifications. Additional width, girth (up to a total of 2 cm can be accommodated within existing patterns), height and length can be added to an existing last at specific points. Examples are: the inclusion of additional girth to accommodate an exostosis of the first metatarsal head, additional toe-box depth to accommodate deformed toes, the inclusion of additional depth in the tarsal region, an alteration in the height of the quarters to prevent irritation on prominent malleoli.
A range of foot deformities can be accommodated within the modular approach but, despite this facility to adapt lasts, there will be foot shapes or deformities so severe that modification to existing lasts will not suffice. Fully bespoke footwear requires a last to be made by taking plaster of Paris impressions of the feet and lower legs and charting a diagram of the foot outline, with length, width and girth measurements identified at specific points on each foot. British Standard 5943 exists for this process (British Standards Institution 1980) and the measurement system provided in the Standard must be followed for a successful outcome.
Modular and bespoke footwear is available at a fitting stage, and footwear can be fitted to the feet before the shoes are completed. At this stage, the uppers have been prepared and attached to the innersole, and excess upper material is wrapped under the innersole and is available for re-lasting and modification if required (Fig. 18.18).

Figure 18.18 Footwear received at the fitting stage. Note the upper material attached to the innersole and the temporary heel. The upper material can be adjusted to include any change required in the dimensions of the shoe before the outsole is attached.
Any modifications required are illustrated by marking the upper material at the exact location where modification is required using a special effaceable pen. If required, the footwear can be refitted once the modifications have been completed, but once the outsole has been added no further modifications can be made. It is essential to obtain an exact fitting with modifications before the outer sole is attached.
Features of the therapeutic shoe upper
Once foot measurements have been taken and the dimensions of the ‘frame’ of the footwear derived, the features of the footwear components need to be considered. This is true for each of type of footwear – stock, modular or bespoke. The shoe should contain a fastening capable of holding it onto the foot, preferably laces but a Velcro fastening is acceptable when mobility is a problem.
The vamp (the front part of the upper) should be seam-free, and any pattern or decoration should be added externally as internal seams may irritate. The quarters (the back part of the upper) should be made from one piece of material with no back seam, which might irritate the retrocalcaneal area. Leather is the most popular material and the one that suits most foot pathologies, but occasionally there is a need to use an extensible material such as neoprene. Lining material may be leather, nylon, cotton, synthetic fabric or shearling (sheepskin). Selection of the lining depends on the internal climate of the footwear during wear and the external environment in which the footwear will be used. Shearling is indicated for cold climates; nylon is cheap but wears quickly; cotton or cambrelle is best for moist feet, as these materials have a wicking property; and leather is good in temperate climates but not for hot weather. Sweaty feet may cause leather linings to become hard and crack, as the foot moisture level affects the tanned leather.
Without any stiffening the shoe will collapse, crease and cause damage to the feet. Without heel counters the shoe quarters will collapse and the shoe may slip off the foot. The extent of the heel counter and the degree of support offered by it should be evaluated. Patients with ankle instability may find a boot helpful, with heel counters additionally stiffened and extended proximally through the quarter. In a midfoot deformity, particularly a valgus deformity, the quarters may be extended distally through to the waist of the shoe. This will minimise deformation of the shoe during gait and can also be used to reinforce the action of an orthotic device.
The properties required in the toe puff should be carefully considered. A toe rim that holds the shoe up over the toe area is required. This may be a standard toe puff that covers the area at the front of the vamp as far proximally as the interphalangeal joints, or a reinforced toe puff to give additional protection against trauma from external objects. In the presence of toe deformities, sensory neuropathy and the environment in which the footwear will be worn should be considered and should inform the prescription. Where there is sensory neuropathy and deformed toes, a rim toe puff is indicated. This will hold up the front of the shoe but will not extend proximally over the dorsum of the toes. In this case the stiffening of the vamp provided by the toe puff in the very front part of the shoe will stop short of the position of the toe deformities in order not to irritate them. The toes will be protected by the upper and lining material without the added hardness of toe puff material in this area. However, if a patient works in an environment where materials may possibly drop onto the feet, a full-size, reinforced toe puff will be beneficial, provided the toe box is of adequate depth to accommodate the toes.
Features of soling in therapeutic footwear
The type of sole and heel required is also significant. Historically, outsole and heel units were made of leather. However, leather has some disadvantages: it has poor slip resistance, especially in wet conditions; it tends to have little effect in reducing the magnitude of ground reaction force against the foot (Perry 1995); and it absorbs and retains water when wet underfoot conditions are present. Advances in technology have made available a range of materials more suitable for outsole units with varying properties specifically indicated for certain types of activity. Modern sole materials include polymers, most commonly polyurethane, thermoplastic rubber and EVA. The construction of these materials makes them particularly good at shock absorption due to air flow through interconnecting air cells within the materials. These materials are viscoelastic, but the overall effectiveness in reducing plantar pressure is dependent on the thickness of the material, the durability of its elasticity and the speed of recovery of the outsole following deformation under body weight during gait (Even-Tzur et al 2006). Both viscosity and elasticity are important factors in reducing the magnitude of the ground reaction force against the foot. A highly elastic interface will return stored energy to the foot, generally resulting in an increased force between the foot and the ground, whereas a highly viscous interface will absorb most of the energy of the impact caused by the foot hitting the ground. However, if a material is too viscous and is not elastic, it will fail to recover its previous shape after impact and remain flattened, and thus be ineffective during subsequent strides. An element of elasticity is required in soling material to promote material recovery before the next step is taken (Whittle 1999).
All sole materials should keep the foot dry, tolerate a range of external temperatures, be durable and possess a coefficient of friction high enough to prevent slipping but low enough to allow movement across the ground surface without any adherence to it. This coefficient of friction of the outsole material is important. The sole material should allow the foot to move easily across the surface without slipping but also without gripping too firmly to the ground surface, when the body’s momentum is likely to cause the body to continue to move forward while the feet stay still, causing a fall.
EVA is generally the preferred sole and heel material. Occasionally, polyurethane or leather topped with rubber to prevent slipping is used. The durability of EVA is determined by its shore value; with a low shore value EVA wears out very rapidly. Footwear made with extra-durable material may be requested from any manufacturer. Recent developments include the use of injection moulding and preformed sole and heel units in polyurethane and thermoplastic rubber for therapeutic footwear. However, because of the costs involved, these sole and heel units are in predetermined sizes and can be used only where the sole required is within a specified length and width range. It is generally unavailable for bespoke footwear, which may be well outside the normal size range. When prescribing bespoke footwear, soling units may need to be cut from sheets of material and the choice is limited to certain grades and sole patterns of EVA and leather.
The sole material should be appropriate for the lifestyle and activity levels of the wearer. Footwear success is dependent on the choice of sole material and the type of environmental conditions in which it is worn. Studies on safety footwear (Rowland et al 1996) have shown that the wear characteristics of the floor–sole combination must be considered. The wearer’s occupation and activities must be considered when prescribing. A rough terrain requires commando soles with additional grip. Some chemicals may damage soling materials, and advice needs to be given if the shoes may come into contact with chemical spillage on the work floor. A lightweight and smooth-surfaced outsole and heel is ideal for a lightweight person with a shuffling gait (Menz et al 2001). Heel and sole prescription is required when combating postural instability. A wide heel base provides greater stability than narrow heels, which are implicated in falls (Rubenstein et al 1988). Certain features can be added to the heel to increase stability. A leg-length discrepancy may require a raised sole on the shorter side. Rocker- or roller-bottom soles increase the rapidity of the midstance phase of the gait cycle and limit the movement at the metatarsophalangeal joints (Wu et al 2004). A rocker or roller sole is beneficial only if the sole of the shoe is inflexible.
HEELS
Heel height
There is a relationship between forefoot loading and heel height. The higher the heel, the greater the forefoot loading and the lighter the heel loading. This must be taken into account when considering footwear as a therapy for the treatment of foot pathologies (Broch et al 2004). Normal heel height for therapeutic footwear is 2–4 cm and averages at 2.5 cm (1 inch). Certain pathologies require the prescription of a higher than normal heel height. Consideration is given to the effect of surgical intervention on ankle mobility. Ankle joint fixation may vary from the normal 90°, and the required heel height will be determined by the angle of fixation.
HEEL MODIFICATIONS
In the solid ankle cushion heel (SACH) the posterior portion has been replaced by a softer material (Fig. 18.19). This reduces shock at heel-strike and is used to compensate for reduced ankle joint motion. A SACH can add a cushioning effect at heel-strike if ankle joint motion is restricted (Wu et al 2004).
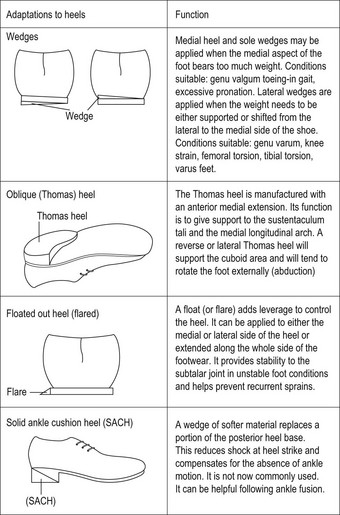
A lateral SACH (the lateral portion of the heel is softer) is sometimes used in cases of hyperpronation to bring the subtalar joint to the neutral position, particularly in adolescents.
Thomas heel
The Thomas heel (Fig. 18.19) is extended anteromedially by 0.5 inch. It is designed to give additional support to the sustentaculum tali and medial longitudinal arch. A lateral or reverse Thomas heel supports the cuboid and tends to rotate the foot externally.
If additional support is needed, the heel can be wedged on either the medial or lateral side only, or across its width. The wedges stabilise the weight distribution and, when used on one side only, offer added support to a given area.
Flared heels (floats)
A flared heel (Fig. 18.19) adds leverage to control the heel. A grossly inverted heel-strike may be helped by a lateral flare to stabilise the ankle and subtalar joint. A medial heel flare will help if the strike is too everted. A flared heel will add to that stability and can prevent excessive pronation (with a medial heel flare) or excessive supination (with a lateral heel flare).
Combined heel and sole modifications
Flares (floats)
Flares may be extended along the entire length of the sole and heel unit, but in order to achieve this a wedged sole and heel unit is preferred (see below). These combined sole and heel flares are useful if the foot is excessively inverting (lateral flare) or everting (medial flare). They increase the ground surface contact area and stabilise the foot.
Wedges
Medial heel and sole wedges (Fig. 18.19) are prescribed when the medial aspect of the foot bears too much weight, and are considered in cases of hyperpronation or depression of the medial longitudinal arch.
Lateral heel wedges with anterior extensions transfer weight off the fifth metatarsal shaft. The apex of lateral heel and sole wedges should not extend beyond the fifth metatarsal head as this stiffens the shoe and causes two main problems: in time the toe will curl upwards, causing the foot to roll more to the lateral side; and the stiffness of the shoe encourages the shoe to slip off the heel during gait.
MODIFICATIONS TO THE SOLE
Lateral sole wedges
These are used when weight needs to be transferred from the lateral to the medial side of the shoe.
Bars
Metatarsal bars may be added posterior to the metatarsal heads on the outer sole of shoes in a line that reflects the angle between the first and fifth metatarsal. This helps to offload pressure from the metatarsal heads and moves the tread line more proximally.
Rocker soles
The rocker shoe is characterised by a rigid sole that restricts movement at the joints, particularly dorsiflexion of the metatarsophalangeal joints. This limitation of movement decreases plantar pressure by preventing anterior displacement of the soft-tissue cushioning of the submetatarsal head and distributes forefoot load over a larger area (van Schie et al 2000). Walking in the rigid shoe is possible because the shoe tips forward when the centre of pressure moves distal to the rocker fulcrum.
Rocker soles eliminate the propulsive phase of gait. Schaff and Cavanagh (1990) suggest that the mechanism of unloading in the rocker-soled shoe may be a combination of the following effects:
Adding rockers to existing footwear
When adding a rocker sole to existing footwear the effect on the heel height of the shoe must be considered. The typical metatarsal rocker added to the tread-line area of the shoe significantly raises the height of the toe spring, which in turn distorts the balance of the shoe and reduces the relative heel height. In some cases this can lead to a negative heel, where the heel is functioning at a lower level than the tread-line foot position.
Shoe raises
Shoe raises added to the outer sole are the most effective means of compensating for limb-length discrepancy (Alexander 2004). Length discrepancy may be caused by congenital anomalies, traumatic injuries, or nerve or muscle damage (Fig. 18.20). Measurement of the length of both limbs is essential to establish the discrepancy and to calculate the height of the raise required. Measurements are taken from the anterior superior iliac crest to the medial malleolus, with the patient supine. Additional measurements should be taken from the ziphoid process to the medial malleolus of each limb, and both these measurements are used to check the discrepancy, which should be used as the first basis for calculation of the raise required. Other factors to be taken into account are hip flexibility, knee flexion and the available range of motion at the ankle, all of which have an effect on functional limb length and must be accounted for in the final calculation of the raise height required.

Figure 18.20 A patient with a limb-length discrepancy. Note that the left foot (longer leg) is pronated and the knee is flexed, while the right foot (shorter leg) is supinated, with the patient failing to make heel contact.
Individuals with a limb-length discrepancy may use specific strategies to improve ambulation. Commonly they may:
Once the discrepancy has been quantified, blocks of material equating in height to the estimated difference in limb length are placed under the shorter limb. A pelvic levelling tool, placed to rest on both iliac crests and containing a spirit level, is used to evaluate the symmetry between the length of the two limbs. Comfort relating to the height adjustment is confirmed, and any necessary adjustment made. Full compensation is not always acceptable or comfortable initially, and it is better to underprescribe the raise height and evaluate again at a later prescription.
Measuring for the raise
The height of the heel raise required should always be measured in the sagittal plane directly underneath the position of the malleoli and not at the back of the heel (Fig. 18.21). Raises over 1 cm in height should be tapered through the remainder of the sole of the footwear to prevent excessive pelvic tilt. The gradation ratio through the sole should be: heel raise = 1 unit; tread line (metatarsophalangeal joint) = 0.5 units; toes = 0.25 or 0 units.

A limb-length discrepancy of 4 cm should have a raise of 4 cm placed under the heel, and 2 cm under the metatarsophalangeal joints tapering to either 1 cm or 0 cm at the toe, depending on the length of the foot and the degree of angulation required for forward propulsion.
In cases of ankle joint fixation it is unwise to use a tapered raise and the ratio here will be: heel = 1 unit; joint = 1 unit; toes = 0.5 unit.
Types of raise
Heel elevation contained inside footwear may be used where the elevation required is <1cm. The cosmetic effect of internal raises is preferred, as the raise is not obvious, but where retail footwear is being used there is seldom enough depth in the heel quarter of the shoe to use a raise of more than 5 mm. Raises may be made of cork, EVA of high shore value (70 shore) or of materials of similar density. Surgical footwear may be manufactured with deeper quarters to include the raise, but it is difficult to disguise the difference in elevation between the two shoes when raises of more than 1.5 cm are involved. It is possible to use an internal and external raise on the same shoe, splitting the height of the raise required between the internal and external raises.
External raises can be added to existing soles if the soling and heel material is suitable. They may be added to the outside of the existing unit, or the existing unit may be removed and the raise added between the shoe and the outsole. It is not advisable to add a heel raise only, as this will affect the heel-height/toe-spring relationship and the shoe will no longer stand correctly on its tread line. The shoe then acquires additional toe spring in wear, causing the front part of the shoe to become upturned and the vamp to become excessively creased. This creasing may irritate the dorsum of the foot, causing superficial lesions.
Where external raises are integrated as part of a surgical shoe they must be made of lightweight material to prevent the shoe becoming too heavy for the wearer. They can be covered with the same material as the upper of the shoe or be made to appear as part of the outer-sole unit. Limb-length discrepancy can have serious consequences for mobility. Accurate measurement and careful prescription of a shoe raise can restore relatively normal function and reduce trauma on the knees, hip and lower spine.
ASSESSING THE FIT OF THERAPEUTIC FOOTWEAR
Whether fitting new therapeutic footwear or evaluating existing therapeutic footwear, the effectiveness of the fit should always be assessed.
Therapeutic footwear is normally provided with a selection of inlays that match the width and length of the shoe, and these provide a useful tool for assessing the dimensions of the shoe in comparison with the foot. Place the foot on the inlay, leaving a small area of the inlay visible behind the foot to allow for the heel curve. Check the overall length of the inlay, from the back of the heel to the longest toe. The inlay should be about 12 mm longer than the longest toe to allow for elongation on walking. Check the proportional length of the foot segments against the inlay. First, check the heel-to-ball length. Then, with the inlay remaining in position under the foot, check that the metatarsophalangeal joints are positioned at the widest part of the inlay, where the shoe is designed to flex. Check the ball-to-toe length to ensure that this is adequate.
If the above lengths are not appropriate the shoe will never fit properly (Fig 18.22). The point at which the shoe flexes (the tread line) must agree with the point at which the foot flexes. If the foot flexes too far proximally the shoe will acquire additional toe spring, the vamp will crease and the shank contained in the shoe will break through the outsole, destroying the integrity of the sole unit. The creased vamp material will cause trauma to the dorsum of the foot, possibly leading to lesion development. If the foot flexes too far distally, the toe spring will be depressed and the toes will be compressed within the shoe.
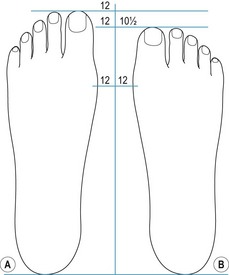
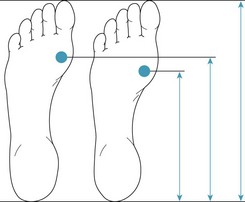
Figure 18.22 (A) Feet of different overall length but the same heel-to-ball measurement; the right foot will be difficult to fit properly. (B) Feet of the same overall length feet but different heel-to-ball measurement; shoes will need to be of different lengths to suit the heel-to-ball lengths.
The inlay is also used to check the width of the shoe at the heel, the instep, the metatarsophalangeal joints and the toes.
The next assessment must be done with the shoe on the foot and containing any orthoses that are to be worn in it. The following should be noted:
CONCLUSION
Footwear is not only a fashion item or only a protection for the feet. In its various forms footwear can facilitate activity, improve mobility, become an effective therapy, reduce morbidity, and improve and extend quality life. To ensure that footwear is optimal, the podiatrist needs to understand how the normal foot functions when shod, how the shoe may have contributed to any pathology present and, conversely, how the various components of the shoe may be used to remedy any pathological state. Footwear should be regarded as part of both the diagnostic and the therapeutic strategy.
Alexander N, Goldberg A. Gait disorders: search for multiple cause. Cleveland Clinic Journal of Medicine. 2004;72(7):586-600.
British Standards Institution. BS 5943: Methods for measurement and recording for orthopaedic footwear. Milton Keynes: BSI; 1980.
Broch NL, Wyller T, Steen H. Effects of heel height and shoe shape on the compressive load between foot and base. Journal of the American Podiatric Medicine Association. 2004;94(5):461-469.
Ceeney E. An introduction to shoe fitting, 1st edn. London: Pitman; 1958.
Even-Tzur N, Weisz E, Hirsch-Falk Y, Gefen A. Role of EVA viscoelastic properties in the protective performance of a sports shoe: computational studies. Bio-Medical Materials and Engineering. 2006;16(5):289-299.
McDowell C. Shoes fashion and fantasy, 1st edn. London: Thames and Hudson; 1989.
Menz H, Lord SR, McIntosh AS. Slip resistance of casual footwear: implications for falls in older adults. Gerontology. 2001;47:145-149.
Merriman LM, Tollafield DR, editors. Assessment of the lower limb, Ch. 8. Churchill Livingstone, 1995.
Perry JE. The use of running shoes to reduce plantar pressures in patients who have diabetes. Journal of Bone and Joint Surgery. 1995;77(12):1819-1828.
Rossi WA. Why shoes make ‘normal’ gait impossible. How flaws in footwear affect this complex human function. Available at http://www.unshod.org/pfbc/pfrossi2.htm, 2003. (September 2009)
Rowland FJ, Jones C, Manning DP. Surface roughness of footwear soling materials: relevance to slip resistance. Journal of Testing and Evaluation. 1996;24(6):368-376.
Rubenstein L, Robbins A, Schulman B, et al. Falls and instability in the elderly. Journal of the American Geriatrics Society. 1988;36:266-278.
Schaff P, Cavanagh P. Shoes for the insensitive foot: the effect of a ‘rocker bottom’ shoe modification on plantar pressure distribution. Foot & Ankle. 1990;11(3):129-140.
van Schie C, Ulbrecht JS, Becker MB, Cavanagh PR. Design criteria for rigid rocker shoes. Foot and Ankle International. 2000;21(10):833-844.
White JM. Custom shoe therapy. Clinics in Podiatric Medicine and Surgery. 1994;11(2):259-270.
Whittle MW. Generation and attenuation of transient impulsive forces beneath the foot: a review. Gait and Posture. 1999;10:264-275.
Wu WL, Rosenbaum D, Su FC. The effects of rocker sole and SACH heel on kinematics in gait. Medical Engineering & Physics. 2004;26:639-646.