5 Removal of unerupted teeth
ASSUMED KNOWLEDGE
It is assumed that at this stage you will have knowledge/competencies in the following areas:
If you think that you are not competent in these areas, revise them before reading this chapter or cross-check with relevant texts as you read.
INTENDED LEARNING OUTCOMES
At the end of this chapter you should be able to:
INTRODUCTION
Teeth fail to erupt into functional positions for a variety of reasons:
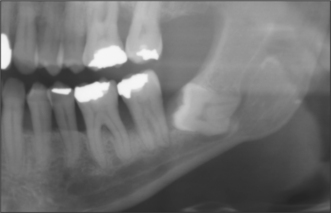
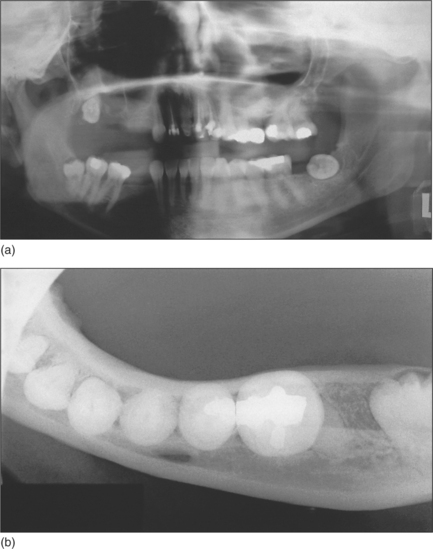
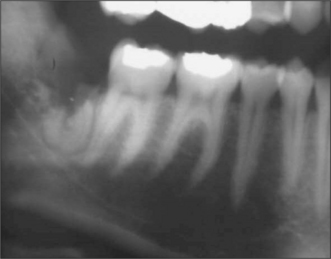
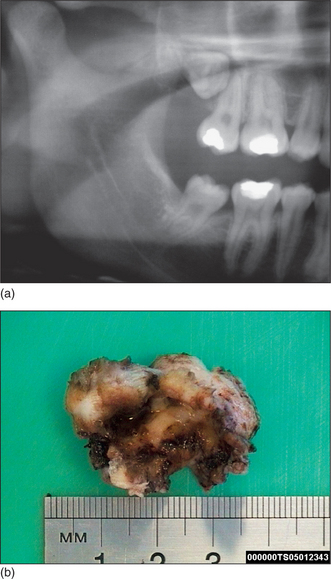
Fig. 5.1 Panoramic radiograph showing impacted lower left wisdom tooth.
Note that the inferior dental nerve canal casts a dark band over the roots of this tooth.
Other reasons include retention or premature loss of deciduous teeth, tumours, cyst formation and certain developmental conditions such as cleft palate or cleidocranial dysostosis.
PREOPERATIVE ASSESSMENT OF THE IMPACTED LOWER THIRD MOLAR
History
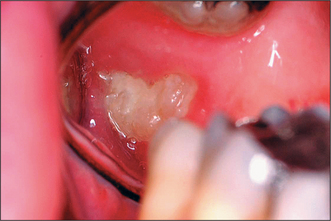
Most patients attending hospital with impacted teeth are referred because of pain and infection, associated with partially erupted teeth (Fig. 5.2); however, many impacted or displaced teeth are unerupted and asymptomatic and therefore an incidental finding following radiographic examination. Occasionally, unerupted wisdom teeth, in the absence of any obvious infection, can give rise to discomfort (often described by patients as ‘pressure’ at the back of the mouth). It is important to exclude other possible causes such as temporomandibular joint pain and pulpitis/periapical abscess from another tooth.
Intraoral anatomical factors that may influence surgical access include size of the tongue and degree of mandibular opening. The position of the impacted wisdom tooth should be noted (unerupted, partially erupted or erupted but non-functional), together with any signs of infection (e.g. caries, pericoronitis). Probing the distal aspect of the second molar will confirm whether the buried tooth is in communication with the mouth.
Pericoronitis
Pericoronitis may be defined as an infection involving the soft tissues surrounding the crown of a partially erupted tooth. It is usually caused by streptococci and anaerobic bacteria, and may be classified clinically as acute (the features of acute inflammation developing over hours to days, possibly with systemic involvement) or chronic (some redness and/or discharge of pus with few acute symptoms, lasting over weeks or months). It may be associated with poor oral hygiene, stress and upper respiratory tract infection.
Signs and symptoms of pericoronitis include swelling, soreness, erythema of the overlying soft-tissue operculum, trismus, facial swelling, raised temperature, regional lymphadenopathy and general malaise. The disorder may be precipitated by trauma from an over-erupted upper wisdom tooth or entrapment of food debris and bacterial infection of the operculum.
Pericoronitis may be treated by removal of the upper wisdom tooth (if this is traumatizing the operculum overlying the lower wisdom tooth), irrigation under the operculum with chlorhexidine, the careful application of a medicament such as trichloroacetic acid beneath the operculum, hot salt-water mouthwashes and analgesics (e.g. ibuprofen). If there is systemic involvement, then antibiotics are indicated (e.g. amoxicillin or metronidazole). Severe infections may require admission to hospital as they can spread through the fascial planes and compromise the airway (see Ch. 7).
Clinical examination assesses the wisdom tooth and excludes other causes of symptoms:
Radiological assessment
The radiographic examination of choice is a panoramic radiograph such as an OPT (Fig. 5.3), although periapical or oblique lateral views of the mandible may be taken as an alternative. When referring a case for treatment all recent relevant radiographs should be included to avoid further exposure to ionizing radiation.
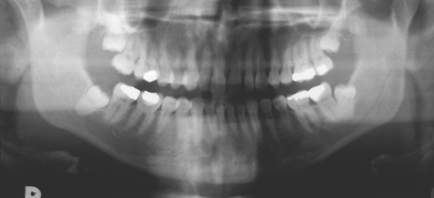
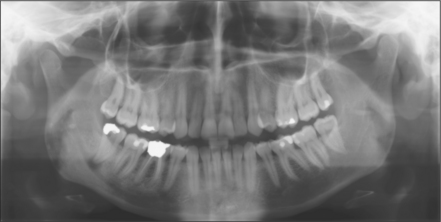
Fig. 5.3 A mesioangular impacted lower third molar on the right and distoangular impaction on the left. (Note the unerupted third molars in the maxilla.)
The following radiological assessment of the lower third molar should be made:
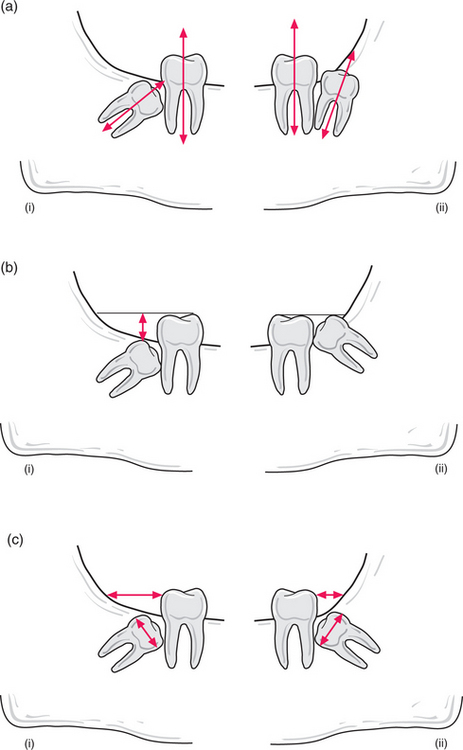
Fig. 5.4 (a) Orientation of third molar: (i) towards second molar; (ii) away from second molar. (b) Increased depth of crown of right third molar (i) from occlusal plane compared to left third molar (ii). (c) Distance between anterior ramus and distal aspect of second molar compared with width of third molar crown: increased surgical access for right third molar (i) but reduced access for left third molar (ii).
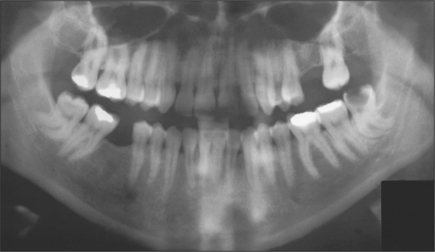
Fig. 5.5 Marked curvature of the roots of the lower third molars. Note gross caries affecting the lower left third molar.
Diagnosis
From the clinical and radiographic examination, a decision on whether to remove the impacted third molar needs to be made (discussed below). If there is pain/discomfort, the cause (e.g. caries) should be identified and treated. Trauma to the operculum of the lower third molar may be eliminated by either extracting or grinding down the cusps of the maxillary third molar. Pericoronitis may require irrigation with chlorhexidine, antibiotics (if systemic involvement) and analgesics. The decision whether to prophylactically remove non-diseased third molars is discussed below in greater detail, although in general their removal is not indicated because they are usually symptomless.
Patient preference should be taken into account when deciding on the form of anaesthesia: local anaesthesia, intravenous sedation, general anaesthesia.
Reasons for removal
The US National Institutes for Health (NIH) consensus on indications for removing wisdom teeth (published in 1980) (see also SIGN 2000 and NICE 2000) listed the following points as definite indications for removal:
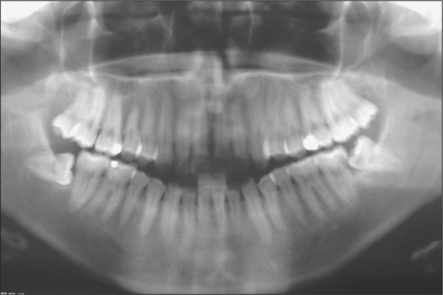
Fig. 5.7 Mesioangular impacted lower left third molar with distal caries on adjacent molar. Note horizontal impacted right third molar.


Contraindications to removal
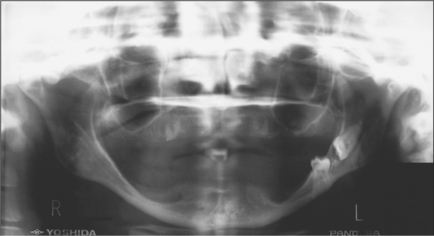
Fig. 5.10 A severely resorbed mandible. The horizontal third molar and impacted second molar occupying the full depth of the mandible show an increased risk of jaw fracture. (Note retained roots in the maxilla.)
There is no strong indication to extract asymptomatic contralateral or unerupted maxillary teeth simultaneously if they are disease-free.
Informed consent for the removal of wisdom teeth
Prior to any surgical procedure the patient should be made aware of the benefits and risks of treatment as well as the possible sequelae of other options (including no treatment).
Thus patients should be warned to expect pain, swelling, bruising, difficulty in opening the mouth and possible damage to the lingual or inferior dental nerve (‘numbness in the tongue or lip’). Effects on ‘quality of life’ issues that may occur (interference with eating, socializing) and time off work, if applicable, should also be mentioned.
Factors influencing the decision to refer to a specialist include:
Type of impaction
Lower third molars may be impacted mesioangularly (Fig. 5.3, right), vertically (Fig. 5.6), distoangularly (Fig. 5.3, left), horizontally (Fig. 5.10) or ectopically placed.
One simple method of determining the type of impaction involves comparing the distance between the roots of the third and second molar (a) with the distance between the roots of the second and first molars (b) (Fig. 5.11). If (a) is greater than (b) it is a mesioangular impaction; where (a) is less than (b) it is a distoangular impaction; where (a) is equal to (b) it is a vertical impaction. If the first molar is missing, the impaction can be determined by comparing a line drawn down the long axis of both the second and third molars: if parallel, it is vertical; if lower 8 leans towards lower 7 it is mesioangular; if the lower 8 long axis diverges from that of the 7, then it is a distoangular impaction.
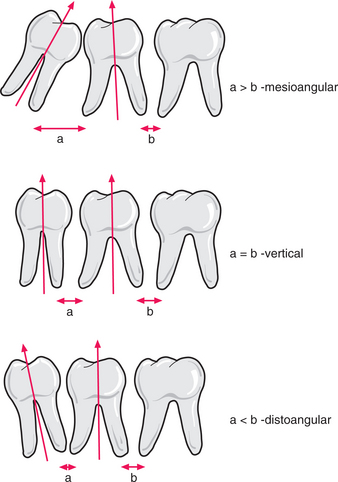
Fig. 5.11 The author’s method to determine the type of impaction of a third molar by reference to spacing between the roots of the molar teeth. See text for details.
The difficulty associated with removing distoangularly impacted teeth should not be underestimated. Although their impaction may appear mild, the path of withdrawal towards the ramus is often associated with more bone removal and reduced surgical access. Horizontal impactions are more difficult to deal with than mesioangular impactions.
A horizontal tooth (i.e. where the line down the long axis of the tooth is roughly parallel with the occlusal plane) usually has its crown facing the second molar but occasionally lies buccolingually (Fig. 5.12). An occlusal view can be taken to identify which way the crown lies. Pell and Gregory (1933) have classified the position of the impacted lower wisdom tooth according to (1) distance between distal surface of lower second molar and anterior aspect of ramus and (2) depth of the occlusal surface of the wisdom tooth in comparison to the occlusal plane of the second molar.
SURGICAL ASSESSMENT
Once the decision has been made that a patient will benefit from removal of a wisdom tooth, the difficulty of the surgery should be assessed in order to determine who should perform it, to select the mode of anaesthesia and to advise the patient concerning the likely outcome. The following method allows the operation to be planned in reverse as the flap size and shape will depend upon the bone removal, which depends upon the position of the tooth. A radiograph is essential before such assessment, and should show the whole tooth and its association to neighbouring structures (e.g. ID canal, adjacent teeth and preferably the lower border of the mandible).
Path of withdrawal/eruption
This depends upon the root curvature, although in practice taking the direction in which the tooth would erupt is probably just as informative.
Obstacles to removal
Those obstacles identifiable on a radiograph may be external to the tooth (extrinsic) or due to the tooth itself (intrinsic).
Extrinsic factors include depth of bone, adjacent teeth and proximity of the inferior dental canal. In addition, the distance between the ascending ramus and second molar influences access. Radiographic signs of intimate involvement between the inferior dental nerve and wisdom tooth include darkening of the root, a break in the white cortical line of the canal and deviation of the canal (Fig. 5.1).
Intrinsic factors include hooked or bulbous roots, roots curving in opposite directions, caries (Fig. 5.5).
Method of overcoming obstacles
Most mildly impacted wisdom teeth can be elevated following removal of sufficient overlying bone. In more severe impactions the whole crown may require sectioning and removal before elevation of the remaining roots.
Sometimes the roots may appear to diverge only to meet again at the apices. The inter-radicular bone can prevent such a tooth being elevated, and thus may require vertical division, allowing the elevation of one root at a time.
Position of instrument to elevate tooth
This is usually on the mesial aspect of the wisdom tooth, although as the tooth moves, a better application point may be obtained buccally. It usually requires bone removal. During the operation it is sometimes necessary to drill such a point into the tooth itself—i.e. to elevate along the path of withdrawal.
SURGICAL REMOVAL OF LOWER THIRD MOLARS
Flap design
A full mucoperiosteal flap should be raised to give adequate access to the site where bone is to be removed. It should be broader at the base to ensure good blood supply and the margins should be capable of being supported on bone following surgery.
Where the tooth is not distoangularly impacted, a triangular flap is preferred. However, with distoangular teeth the proximity to the distal root of the lower second molar argues for the envelope flap.
If the tooth to be removed is partially erupted, then its gingival margin should be included in the flap. If unerupted, the incision starts from the distal aspect of the second molar.
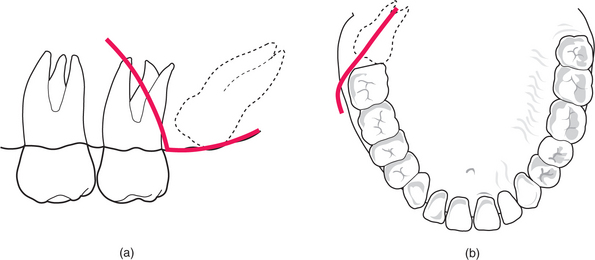
Triangular flap (Fig. 5.13)
Keeping a finger on the external oblique ridge to place the soft tissues under tension and define the bony landmarks, the scalpel blade is inserted onto bone at a point immediately distal to the second molar. The incision is extended down to bone, along the external oblique ridge (upwards, outwards and backwards) for approximately 1 cm. The incision must not be carried directly backwards in the line of the posterior teeth as the mandible flares laterally and there is a risk of damage to the lingual nerve. The lingual nerve may lie on or near the alveolar crest in up to one in five cases.
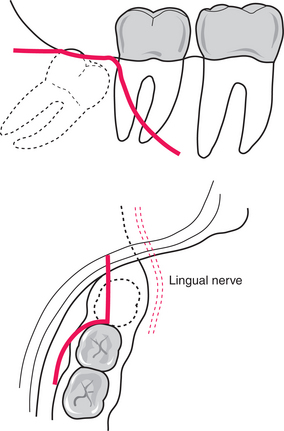
Fig. 5.13 The triangular flap used to gain access for the surgical removal of an impacted lower right third molar.
(Top) Buccal aspect of incision. (Bottom) Distal relieving incision viewed from above. Note the position of the lingual nerve as the mandible flares laterally.
The anterior relieving incision curves down from the distal aspect of the lower second molar towards the buccal sulcus. It should not be extended too far towards the sulcus as this can result in troublesome bleeding. The mucoperiosteal flap is raised (using a Howarth’s or similar periosteal elevator), starting in the anterior relieving incision.
Opinion varies as to whether the lingual tissues should be protected by insertion of a retractor between periosteum and bone. Traditionally this has been done in the UK, although it is less common in Europe and the USA. Where a lingual retractor has been placed, temporary lingual nerve dysaesthesia can be expected in approximately 10% of cases. This is probably due to blunt trauma but also possibly to stretching of the nerve or compression against the mandible if trapped between bone and retractor. There is no evidence that the incidence of permanent nerve injury is higher without a retractor. Avoidance of a lingual nerve retractor may reduce this temporary dysaesthesia although it does not guarantee that the lingual nerve will not be damaged: for example, the nerve may be damaged whilst suturing if it is near the alveolar crest. Although inexperienced operators generally find inserting a lingual nerve retractor difficult (e.g. problems finding the correct tissue plane, or where the lingual ridge is undercut), it does improve visibility by retracting the lingual tissues. A lingually placed retractor may reduce the likelihood of permanent anaesthesia if the lingual plate is penetrated by a bur. However, this may be at the expense of increasing the chances of a temporary paraesthesia due to blunt trauma from the retractor. It is essential to check that there is no soft tissue lying between the retractor and lingual bone. Where there has been infection of the surrounding soft tissues the flap may be more difficult to raise due to fibrous tissue.
Whether a lingual retractor is used or not, it is important to avoid penetrating the lingual cortical plate with the bur because this is often associated with permanent damage to the lingual nerve.
Envelope flap (Fig. 5.14)
Once again a distal relieving incision is made. However, with this flap the incision is taken around the gingival margin of the lower second and first molars to include the papilla between the first molar and second premolar. A Warwick-James elevator is used to free up the interdental papillae and the gingival margin prior to flap reflection with a periosteal elevator.
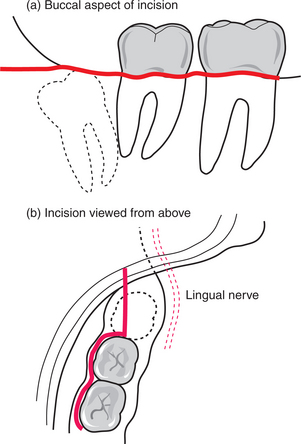
This flap is particularly indicated where it is predicted that much bone will need to be removed just distal to the lower second molar—for example, a distoangular or horizontally inclined third molar—because a triangular flap could leave mucosa overlying a site requiring bone removal. Furthermore, the relieving incision might not rest on bone following removal of the tooth, thus potentially delaying healing. Hence the value of an envelope flap, which has adequate bone support, although it is important to ensure that postoperatively the suture distal to the second molar replaces the gingival margin and papillae with sufficient tension.
Following reflection of the mucoperiosteal flap, if there is insufficient access, then the distal relieving incision may be extended. This is more easily done by inserting a buccal retractor (e.g. rake) and cutting up the external ridge (with either blade or scissors), whilst keeping the flap extended outwards under tension. If there are no obstructions, the tooth may be elevated using a Coupland’s elevator placed mesially and then down the long axis of the tooth, buccally. This displaces the tooth upwards, as the instrument is driven down and rotated.
Bone removal
If the tooth cannot safely be elevated intact, then bone is usually removed using a round bur. If operating under general anaesthesia some prefer the use of chisels.
The bur should rotate in the correct direction and at maximum speed. Cutting instruments that introduce air (‘air rotor’) should not be used because they can result in surgical emphysema. The handpiece should not rest on the soft tissues of the cheek and lips, because burning could occur if it overheats. Adequate delivery of sterile saline through an integral part of the handpiece or from a syringe should ensure that the debris is flushed away and that the bone and bur do not overheat. The patient should be warned to expect the sound of the drill and the assistant should endeavour to keep all excess fluid sucked away. The crown of the impacted tooth should be exposed (usually to the cementoenamel junction) by removal of surrounding bone: (a) mesially (to create a point of application but beware of adjacent root of second molar); (b) buccally (cutting a trough or gutter around the tooth to the root furcation); (c) distally (remember that, even if the lingual tissues are retracted, the lingual nerve may not be adequately protected, hence ideally the lingual plate should not be breached). If lingual tissues are not retracted, access to distolingual bone is severely restricted.
Distoangularly impacted third molars, particularly if partially erupted, may appear relatively straightforward to the inexperienced. However, more distal bone is usually required to be removed than with a mesioangular impaction, and it may be better to remove the crown and roots separately, once the tooth has been mobilized.
Tooth division
If the roots are not fused then a choice between sectioning the tooth in the vertical axis (with a bur or, if operating under GA, an osteotome; thus removal in two halves) or horizontal axis (removal of the whole crown and then elevation of the roots) should be made. The choice will to some extent depend upon the inclination of the crown, and the root apices. When using a drill it is easier to cut at an angle approximating to that which the drill takes on entering the mouth. It is easier to section the crown off a distoangular or horizontal tooth (Fig. 5.15) and to split a mesioangular tooth along its length (Fig. 5.16).
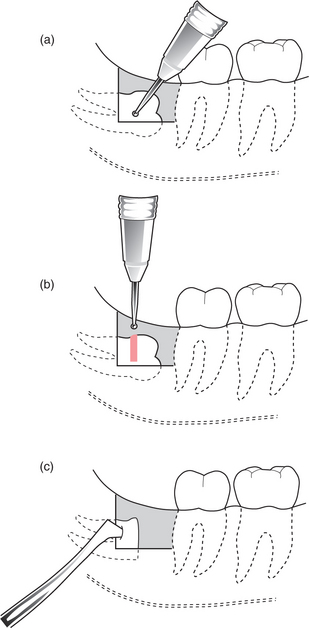
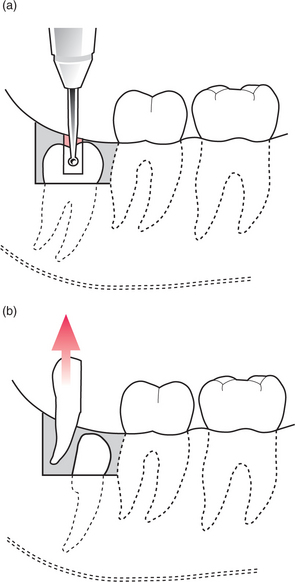
Fig. 5.16 (a) Mesioangularly impacted third molar with separate roots sectioned longitudinally with a bur. (b) The distal half is removed with an elevator before removal of the mesial half.
When cutting into enamel, with practice it is possible to ‘feel’ when the bur has reached the enamel on the lingual aspect of the tooth, which, ideally, should not be breached. The crown can be split and removed from its other half (if vertically sectioned) or from the root (if horizontally sectioned) by inserting a Coupland’s elevator. The patient should be warned to expect a cracking sound due to splitting of the tooth. In older patients there may be an increased risk of mandibular fracture due to possible ankylosis, reduced mandibular thickness and less flexible bone. Where there is a large distal restoration on the second molar, the patient should be warned that it could be dislodged by elevating the tooth (Fig. 5.17).
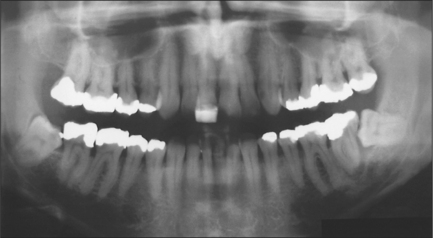
Fig. 5.17 The distal amalgam on the lower right second molar is at risk of being dislodged when elevating the mesioangularly impacted third molar.
Following removal of the crown it may be necessary to remove more bone (buccally, mesially and/or distally) to obtain a point of application for removal of the root. A point of application cut into the root may allow its removal using a Cryer’s or Warwick-James elevator. Sometimes the individual pulp canals can be visualized and a cut made between them buccolingually. This should be deep enough to allow the insertion of a Coupland’s elevator which, when rotated, splits the roots. Do not use the adjacent molar as a fulcrum. Once one root is removed the other may be elevated, by inserting either a Cryer’s or Warwick-James elevator in the space cut around the root.
If the apex (or apices) fracture then they are best removed at the time. Exceptions include a vital tooth in which the fragment is small and the surgeon considers the inferior dental nerve to be at risk by its removal, or where under local anaesthesia the patient would find further surgery unduly stressful (Fig. 5.18). The patient should always be informed of this decision, which should be recorded in the notes, and told to return if symptoms arise. It is wise to take a periapical radiograph after surgery.
Wound debridement
Check that the whole of the tooth, including all roots, has been removed. The buccal and lingual margins of the socket should be smoothed using a round bur, bone file or rongeurs to remove loose, sharp bits of bone or any that has been devitalized. The wound should be irrigated with sterile saline, paying particular attention to the area underneath the soft-tissue flaps. The sequestration of small pieces of bone may cause severe discomfort out of all proportion to their size and can foster infection over a period of months postoperatively.
Mild oozing occurs from the socket immediately following removal of the tooth but brisk bleeding should be controlled before suturing the flap.
Although it is often thought that the follicle and associated fibrous tissue should be removed (‘to avoid cyst formation’), there seems little evidence to suggest that its complete eradication is required, particularly if it would lead to damage to the lingual nerve. If fibrous tissue cannot be easily removed from the lingual soft tissues (e.g. with a scalpel or a pair of Fickling’s forceps) then it is probably best left, although obviously infected or granulation tissue should be removed and submitted for histopathological examination.
Bone removal with chisels (the lingual split technique)
When used by specialists operating under general anaesthesia, this technique may be faster than the use of a bur. However, the extent of bone removal is less predictable than with a bur.
Briefly, a 5-mm chisel and mallet are used to create a vertical step cut at the distal aspect of the second molar. With the bevel facing downwards, a horizontal cut is made from the lowest point of the vertical step cut, backwards to just beyond the third molar. The buccal bone can then be removed, usually in one piece. It is important to ensure that the chisel is not parallel with the internal oblique ridge as this might fracture the mandible. The chisel is placed diagonally across the mandible, distal to the third molar. The angulation of the chisel will determine the depth of lingual bone split (i.e. the more vertical the chisel, the greater the depth of bone). It is not unusual for the lingual plate thus fractured to contain the lingula. The tooth can then usually be rolled out in a lingual direction. Using this technique, the lingual nerve must be protected.
Perioperative drug therapy
Various drugs may be given perioperatively just before, during or at completion of treatment to help to reduce complications.
Analgesics
Despite the availability of a reasonable spectrum of analgesics patients often experience pain. There is some evidence that preoperative analgesia leads to less pain and reduced analgesic consumption. Aspirin or ibuprofen appear effective. When taken postoperatively, soluble aspirin would appear to be better than paracetamol.
Steroids
Steroids (e.g. dexamethasone 8 mg) reduce facial swelling and discomfort if given at the time of operation, although not all surgeons routinely use them. They do not appear to delay wound healing.
Antibiotics
Although some favour the routine use of prophylactic antibiotics there is no strong evidence that it reduces the infection rate. Indiscriminate use increases the risk of unwanted side effects such as allergy/anaphylaxis or emergence of bacterial resistance. Some surgeons reserve the use of antibiotics for an operation which has taken longer than expected, if the bone appears more dense, in older patients and when using chisels.
Prophylactic antibiotics are recommended in a patient who has had radiotherapy involving the jaw bone or who is at risk of infective endocarditis. In general, short courses of high doses appear to be better than long courses of low doses. Preoperative antibiotics appear more efficacious than those given postoperatively. The latter appears not to contribute to better wound healing or less pain.
Closure
Although healing by primary intention is the ideal, in practice this is rarely achieved because the wound margin does not always rest on bone. Where a partially erupted tooth existed, a choice between complete closure or retaining the gap needs to be made. If the gap is retained then food debris may collect, causing pain, halitosis and bad taste. However, whilst primary closure may lead to faster healing there may be more pain and tethering of the cheek.
Sutures may be either resorbable (e.g. polygalactin) or non-resorbable (e.g. silk). A 3/0 suture should be used. The first suture should be placed just distal to the second molar, from buccal to lingual tissue. If a triangular flap is used, the anterior relieving incision rarely requires suturing. However, the distal relieving incision usually does.
POSTOPERATIVE CARE AND COMPLICATIONS OF REMOVAL OF LOWER THIRD MOLARS
In addition to general issues of postoperative care dealt with in Chapter 4, there are certain specific points that relate to third molar surgery (Table 5.1).
Table 5.1 Problems associated with third molar surgery
| Intraoperative | Postoperative |
|---|---|
| Haemorrhage | Pain |
| Fractured root apex | Swelling |
| Damage to adjacent tooth or soft tissue | Bruising |
| Fracture of the mandible | Trismus |
| Anaesthesia of labial or lingual nerves | |
| Infection of soft tissue or bone |
The patient should be reminded of the most common complications—pain, swelling, bruising, trismus and possible alteration of sensation to the lip and tongue.
Other factors that require consideration relate to quality-of-life issues, for example, time off work, enjoyment of food, interference with oral functions, in particular ability to eat. There is a significant deterioration in oral health-related quality of life during the first postoperative week, which should be considered when obtaining informed consent.
Some surgeons do not routinely review patients after third molar surgery if they have used resorbable sutures. It is essential that the patient knows how to contact their surgeon in the event of difficulties and that they are aware that they should return if there is any sensory loss.
The lingual plate of bone can be very thin, with the possibility of displacing the apices lingually. Should this happen, a finger placed lingually can push it back into the socket; failing this a lingual flap can be raised to retrieve it. Transient dysaesthesia of the lingual nerve is highly likely.
If a root should fracture do not try to drill it away: remove more bone and elevate the root whole. If it is very small and near the inferior dental nerve then it is probably best left (see Ch. 4). There is a risk of mandibular fracture in the atrophied (usually edentulous) jaw or where a deeply buried tooth lies near the lower border (Fig. 5.10). In the event of a fracture, repair with miniplates is usually the treatment of choice—this is a task for a hospital specialist. Both hard (e.g. second molar roots) and soft tissues (e.g. lingual nerve) can be damaged. Be especially aware of distal restorations on the second molar when elevating at the mesial aspect of the wisdom tooth.
If any of the above occur, the patient should be informed before leaving the surgery. Ideally the problem should be corrected on the day of surgery and may require referral to a specialist. Such events should be recorded in the notes.
Bruising (ecchymosis) is common, tracking along the tissue planes and resolving usually within 2 weeks. However, pooling of blood within the soft tissue to form a haematoma may require incision and evacuation of the blood clot, which is prone to infection and slow to resolve. Infection of the soft tissues may result in secondary haemorrhage, cellulitis or abscess formation but this seldom occurs before 48 hours after surgery. Where signs of systemic involvement are present (pyrexia, lymphadenopathy) antibiotics should be prescribed and good oral hygiene advised. With persistent infection, check that no root, necrotic bone or foreign body has been retained.
Rarely, osteomyelitis (or actinomycosis) may occur (see Ch. 7).
Delayed wound healing may occur with or without pain. Institute good oral hygiene plus mouthwashes. Ensure that the wound heals (i.e. exclude tumour).
Lingual and inferior alveolar nerve damage may occur. The lingual nerve is at risk from: (1) ‘bruising’ or stretching, following the use of periosteal elevator; (2) a bur through the lingual plate; (3) suturing. It is surprising how infrequently patients complain of buccal nerve dysaesthesia. Loss of fungiform papillae is the only clinical sign associated with lingual nerve anaesthesia, with their return linked to nerve regeneration (Fig. 5.19). Patients with no sign of recovery of sensation should be referred to a specialist with a view to possible nerve repair. Spontaneous recovery is unlikely after 6 months.

Fig. 5.19 The loss of fungiform papillae (on the right) is associated with lingual nerve damage whilst their return is linked to nerve regeneration.
Difficulty in opening the mouth usually resolves over 2 weeks but may require ‘encouragement’ through the use of a trismus screw or wooden spatulas. Swelling also usually resolves within 2 weeks. It can be reduced by perioperative administration of steroids.
Removal of lower wisdom teeth may be associated with bone loss distal to the second molar, with loss of periodontal attachment.
There is little evidence to suggest that the complication rate is significantly higher in any particular group, such as older patients.
MAXILLARY THIRD MOLARS
Indications for removal
Extraction is indicated if the tooth is erupted and causing trauma to the cheek or operculum overlying the lower wisdom tooth. Unerupted third molars are often asymptomatic and unless there is associated pathology (Fig. 5.20) they should be left, regardless of whether the lower third molars are to be removed under general anaesthesia.
Surgical access (Fig. 5.21)
Access is difficult due to the posterior position and further restricted by the coronoid process, particularly when the mouth is fully open. Erupted teeth can be extracted with forceps, rather than an elevator (to reduce the possibility of a fractured tuberosity). Unerupted teeth that are to be removed require a flap in which the incision runs from the distopalatal aspect of the third molar to its mesiobuccal corner, continuing in the same direction towards the buccal sulcus. The flap may be raised using a Howarth’s elevator. The tooth must be prevented from being pushed into the infratemporal fossa by inserting the Howarth’s elevator behind the tuberosity (otherwise a Laster’s retractor may be used). If there is overlying bone it is usually thin and can be removed with a chisel (which may be hand-held rather than being tapped with a mallet); rarely, a bur is needed. A mesial application point is established and the tooth elevated distobuccally using a Warwick-James or Cryer’s elevator. A flat mesial surface is associated with more difficulty in inserting an elevator. The flap falls back in on itself and many surgeons feel it does not normally require suturing. However, sometimes an extensive incision tends to bleed at its limits, and such an incision should be sutured. An envelope flap may be used, which has a distal relieving incision and extends around the gingival margins of the teeth. Access can be extremely good but it may take longer to raise and repair. A flap with both mesial and distal relieving incisions increases access still further but can be difficult to repair.
Complications
Excessive bleeding may occur, from either the buccal sulcus incision or tearing of the palatal tissue as the tooth is elevated. Pressure and suturing should suffice.
Fracture of the tuberosity (Table 5.2) is more likely if a fully erupted tooth is elevated backwards. If the fragment is small and the tooth roots are fused to the bone the tooth should be removed with the bone fragment and the mucosa sutured. Larger pieces of bone, if still attached to periosteum, may be replaced and, if the tooth is erupted and vital, it should be splinted in place and surgically removed at a later date. Check for an oroantral communication after extraction, particularly where the roots are in close proximity to the maxillary antrum.
Table 5.2 Complications associated with other impacted teeth
| Maxillary third molar | Maxillary canine |
|---|---|
| Fracture of tuberosity | Damage to adjacent teeth |
| Oroantral communication | Palatal haematoma |
| Displacement | Perforation of floor of nose |
| Perforation of maxillary antrum |
A maxillary third molar may be displaced either backwards into the infratemporal fossa lateral to the pterygoid plates or, rarely, into the maxillary antrum. Antibiotics should be prescribed to reduce the risk of infection that might spread through the fascial planes. Removal of such a tooth is a task for a hospital specialist. Once located using two radiographic films at right angles to one another, a needle is inserted until it contacts the tooth. The surgeon then blunt dissects down onto the tooth to remove it.
IMPACTED MAXILLARY CANINES
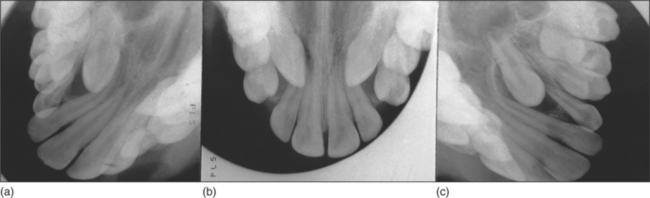
Radiographic examination
The main methods of localization are (1) use of parallax or (2) two films taken at right angles to one another. Parallax movement can be assessed in both the horizontal and vertical planes by taking two periapicals with differing X-ray tube angles or an anterior and an oblique occlusal view (Fig. 5.22). If the unerupted tooth appears to move in the same direction as the X-ray tube, then it is lying palatally. A panoramic radiograph plus an anterior occlusal or lateral skull radiograph may also be used. A vertex occlusal view is best avoided, as it requires a large dose.
Surgical extraction
Canines lie buccal to the arch in approximately one in five cases. If the crown is easily palpable, then a semilunar incision, at least 0.5 cm above the gingival margin of the erupted teeth, may be used. Otherwise an incision is taken around the gingival margin of the erupted teeth. This is cut one tooth behind and one in front of where the unerupted canine is lying, with an anterior relieving incision carried up towards the buccal sulcus. The bone is usually thin and may be removed using a Coupland’s elevator or bur to uncover the crown prior to elevation. Depending on the patient (e.g. maturity), this may be carried out under local anaesthesia.
Most canines are palatally impacted. Where a unilateral canine is impacted the incision may be taken around the palatal gingival margin from the first molar on the impacted side to the canine on the opposite side. Where bilaterally impacted maxillary canines are to be extracted, then the flap margin may extend from the first molar on the left side to the first molar on the right side. This is usually carried out under general anaesthesia.
The flap is raised by inserting the convex surface of a Warwick-James elevator and peeling back the gingival margin. The Howarth’s can then be used to complete the raising of the palatal flap. The neurovascular bundle issuing from the incisive foramen can safely be cut with a blade (bleeding uncontrollable by pressure may require bipolar coagulation) and rarely gives rise to clinically perceptible anaesthesia.
Bone may be removed with a bur to expose the whole of the crown (from incisive edge to coronal aspect of root, taking care not to damage adjacent roots). The tooth may be removed with a Warwick-James elevator, taking care to palpate the adjacent teeth for movement. Occasionally it may be helpful to use both Warwick-James elevators together to alter the direction of displacement. The elevator must be kept against sound bone. If adjacent teeth begin to move, stop and section the crown from the root. Once the crown is sectioned further bone removal may be required to obtain an application point on the root.
Mould the palatal flap back (pressure from an assistant’s finger whilst suturing the papillae may help reduce the likelihood of a palatal haematoma). Ensure there is no bleeding from the flap before suturing. Take deep bites of palatal tissue and place interrupted sutures through the papillae. The knots should lie buccally to avoid irritating the tongue.
Complications
There is a risk of damage to adjacent teeth and roots (Fig. 5.23; see also Table 5.2). A palatal haematoma may occur as the flap is readily displaced downwards into the mouth. If it arises there is a risk of infection.

Perforation of the floor of nose or maxillary antrum may occur with extensive or careless bone removal. Bone loss may lead to periodontal pocketing. This is very rarely a problem clinically but may merit referral to a periodontal specialist.
OTHER BURIED TEETH
These include second premolars, supernumeraries (Fig. 5.24), supplemental teeth and, from time to time, almost any tooth. The tooth is located by palpation and radiography; occasionally parallax views may be required. Treatment options, as for buried canines, include (1) leaving it, if it is not resorbing the adjacent teeth and its removal might damage adjacent structures; (2) orthodontic alignment; (3) removal; (4) transplantation.
Surgical removal
It is difficult to raise a lingual flap in the lower arch, as it easily tears and suturing is difficult. In addition, for both upper and lower premolars lingually inclined, the apex is buccally placed and it is often that part of the tooth which is most troublesome to remove. A buccal approach involves raising a flap one tooth posterior to the impacted tooth to one tooth anterior, using a buccal relieving incision. This should gently curve away from the mental nerve region. In the lower arch the mental nerve should be identified so that it can be protected whilst bone is removed. The crown can be sectioned if necessary, the root elevated, the wound cleaned and sutured. The patient should always be warned of possible mental nerve para/anaesthesia when removing impacted lower premolars.
Supernumerary teeth are relatively common in the anterior maxillary region, lying palatal to or between the permanent teeth. Removal is indicated if they are interfering with the eruption of a permanent incisor. Otherwise mere presence does not warrant removal. Where other unerupted developing teeth are present, great care is needed to remove the correct one.
A decision to remove any buried tooth should involve a balanced judgement of the risk of damage from the tooth itself and the risk of damage from the surgery. Surgery should not proceed unless it is judged that the benefits of removal exceed the risks of surgery.
Carmichael F.A., McGowan D.A. Incidence of nerve damage following third molar removal. British Journal of Oral and Maxillofacial Surgery. 1992;30:78-82.
McGrath C., Comfort M.B., Lo E.C., Luo Y. Changes in life quality following third molar surgery—the immediate postoperative period. British Dental Journal. 2003;194:265-268.
McGurk M., Haskell R. How clinical research changed the habit of a lifetime. British Dental Journal. 1997;183:121.
Mercier P., Precious D. Risks and benefits of removal of impacted third molars. A critical review of the literature. International Journal of Oral and Maxillofacial Surgery. 1992;21:17-27.
National Institute for Clinical Excellence (NICE). Guidance for removal of wisdom teeth. Technical Appraisal Guidance No. 1. London: NICE, 2000.
Ogden G.R. Atrophy of fungiform papillae following lingual nerve damage—a poor prognosis? British Dental Journal. 1989;167:332.
Ogden G.R., Bissias E., Ruta D.A., Ogston S. Quality of life following third molar removal: a patient versus professional perspective. British Dental Journal. 1998;185:407-411.
Ong K.S., Seymour R.A., Chen F.G., Ho V.C. Preoperative ketorolac has a preemptive effect for postoperative third molar surgical pain. International Journal of Oral and Maxillofacial Surgery. 2004;33:771-776.
Orr D.L. Protection of the lingual nerve. British Journal of Oral and Maxillofacial Surgery. 1998;36:158.
Pell G.J., Gregory G.T. Impacted mandibular third molars: classification and modified technique for removal. Dental Digest. 1933;39:330-338.
Petersen L.J., Laskin D. NIH consensus development conference on removal of third molars. Journal of Oral Surgery. 1980;38:235-236.
Robinson P.P., Smith K.G. Lingual nerve damage during lower third molar removal: a comparison of two surgical methods. British Dental Journal. 1996;180:456-461.
Robinson P.P., Smith K.G. A study on the efficacy of late lingual nerve repair. British Journal of Oral and Maxillofacial Surgery. 1996;34:96-103.
Rood J.P., Nooraldeen Shehab B.A.A. The radiological prediction of inferior alveolar nerve injury during third molar surgery. British Journal of Oral and Maxillofacial Surgery. 1996;28:20-25.
Ruta D.A., Bissias E., Ogston S., Ogden G.R. Assessing health outcomes after extraction of third molars: the postoperative symptom severity (PoSSe) Scale. British Journal of Oral and Maxillofacial Surgery. 2000;38:480-487.
Savin J., Ogden G.R. Third molar surgery–a preliminary report on aspects affecting quality of life in the early postoperative period. British Journal of Oral and Maxillofacial Surgery. 1997;35:246-253.
Scottish Intercollegiate Guideline Network (SIGN). Management of unerupted and impacted third molar teeth. Report no. 43, Royal College of Physicians, Edinburgh. [Online]. Available at: URL: http://www.sign.ac.uk, 2000.
Shepherd J., Brickley M. Surgical removal of third molars. Prophylactic surgery should be abandoned. British Medical Journal. 1994;309:620-621.
Thomas D.W., Hill C.M. An audit of antibiotic prescribing in third molar surgery. British Journal of Oral and Maxillofacial Surgery. 1997;35:126-128. (See comment S. F. Worrall (1998) British Journal of Oral and Maxillofacial Surgery 36: 74.)
Von Wowern N., Nielsen H.O. The fate of impacted lower third molars after the age of 20. International Journal of Oral Maxillofacial Surgery. 1989;18:277-280.
Zeitler D.L. Prophylactic antibiotics for third molar surgery: a dissenting opinion. Journal of Oral and Maxillofacial Surgery. 1995;53:61-64.
ACKNOWLEDGEMENTS
Dr D Thomson and Dr E Connor, Dental Radiology, Dundee Dental Hospital for Fig. 5.1.
SELF ASSESSMENT
Answers on page 263.