CHAPTER 27 Vision
What aspects of vision do I need to assess?
Visual testing is usually completed by the medical team as part of the assessment of the cranial nerves (S2.10). Visual acuity should be assessed by an optometrist using a Snellen eye chart. However, there are aspects of vision that are simple and relevant for the therapist to assess:
Visual fields
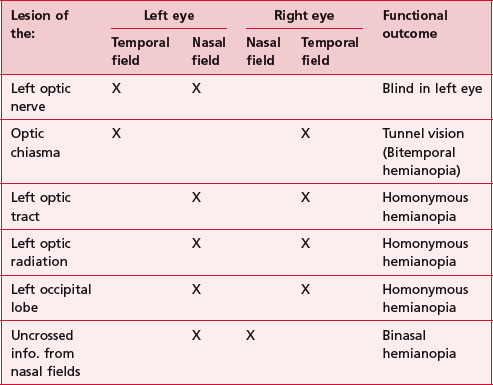
The input from central and peripheral visual fields (S2.10) is important in providing a complete picture of the external environment. Therefore any lesion involving the visual pathway could result in incomplete input, which may hinder functional ability. The presentation of lesions at different points along the visual pathway is shown in Table 27.1.
 Clinical hints and tips
Clinical hints and tipsFixing and scanning
Visual acuity requires coordination between head and body movements to allow the visual stimuli to be picked up by the appropriate part of the retina. This is achieved via fixing (S2.10) and scanning (S2.10). A deficit affecting these abilities may produce poor balance and inaccurate movement during function.
Why do I need to assess these aspects of vision?
Visual deficits are present in as many as 40% of patients with cerebrovascular accidents and 50% of traumatic brain injuries (Kerty 2005). Vision is important in the context of balance and movement and therefore any deficit may have a profound effect on the patient’s ability to function.
How do I assess these aspects of vision?
Visual fields
Therapist
 Caution
Caution
Spatial inattention and neglect (S3.33) may present similarly and may be difficult to differentiate.
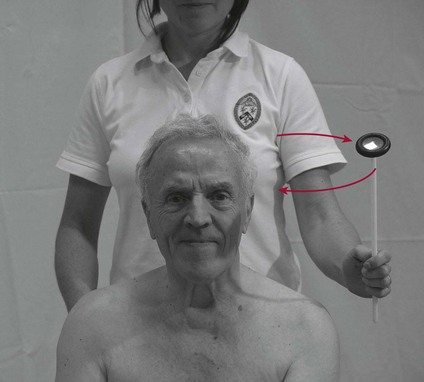
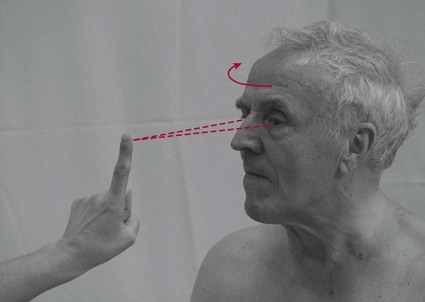
Fixing (Fig. 27.3)
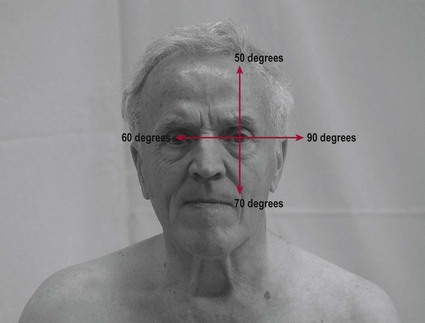
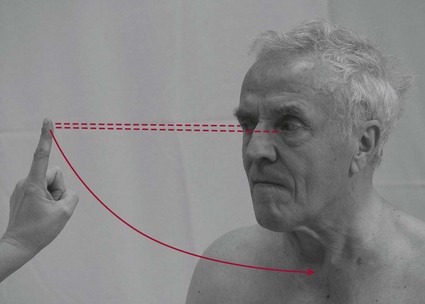
Scanning (Fig. 27.4)
Therapist
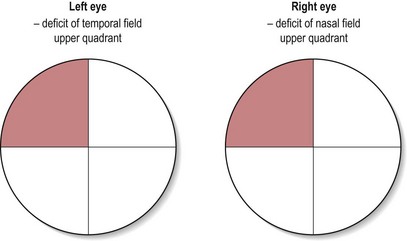
Recording
Recording the findings for fixing and scanning could utilize a simple text description of the deficits noted. However, it may be more efficient to note any visual field deficit in a circle representing the four quadrants tested (Fig. 27.5).