CHAPTER 26 Coordination
What is coordination?
Successful movement involves the complex coordination of multiple joints and muscles which is achieved via the appropriate sequencing, timing and grading of muscle recruitment (Shumway-Cook and Woollacott 2007; Berthier et al. 2005). Even a simple reaching task involves all levels of the central and peripheral nervous system with the integration of these sensorimotor systems occurring primarily in the cerebellum (S2.12) (Fuller 2004). Smooth accurate movement involves the interaction of hand–eye coordination, inter-limb and trunk coordination.
Incoordinated movement
Incoordination presents as a lack of smooth sequenced movement which is often awkward and uneven and may involve both limb and trunk muscles. The incoordination is attributed to a loss of synergistic interplay between muscles as a result of disruption in muscle:
As the control facilitating coordinated movement is highly complex and involves many nervous system structures it follows that incoordination can be a consequence of damage to any one of them. This includes:
Ataxia
Ataxia is a term used to describe the motor incoordination presented by patients with a deficit affecting the cerebellum (S2.12) during voluntary movement. It includes symptoms such as nystagmus, reduced manual dexterity, poor balance and altered gait (Bakker et al. 2006; Ilg et al. 2008), dysarthria and dysmetria (Thoma et al. 2008). Dysmetria, is a problem with judging the distance of movement and is often referred to as intention tremor. The outcome is inaccurate movement with overshooting (hypermetria) and undershooting (hypometria) during the task. Ataxia can affect the trunk (trunk ataxia) or limbs (limb ataxia) or both, depending on whether the lesion is in midline or the cerebellar hemispheres, respectively. The incoordinated movement that is produced affects mobility, when the patient presents with a drunken swaggering gait and all other functional activities. Ataxic movement is thought to occur due to impairment in the timing and duration of muscle activation, or the magnitude and grading of force production (Ausim 2007).
 Caution
CautionWhy do I need to assess coordination?
Incoordinated movement is often inaccurate, effortful and ultimately leads to a reduced functional outcome. This presentation is observed in many neurologically impaired patients whether the pathology affects the central or peripheral nervous system.
How do I assess coordination?
Observation of functional tasks
Assessment of coordination usually begins by observing the patient’s ability to perform simple functional tasks (S3.18) taking note of the accuracy, speed and trajectory of movement.
The activities observed should challenge both the limbs and trunk. To identify a trunk deficit in isolation, the patient could be requested to sit unsupported with upper limbs held in a static position away from the body. Excessive movement of the trunk could indicate incoordination. However, the therapist should be mindful that there is a great deal of overlap between the concepts of trunk coordination, trunk stability (S3.25) and balance (S3.32). The therapist should also be aware that any problems with trunk coordination will also affect the accuracy of limb movements.
Simple tests of limb coordination
A comparison of right and left should be made, allowing for handedness during the performance. If there is an unaffected side this should be tested first to ensure understanding of the procedure.
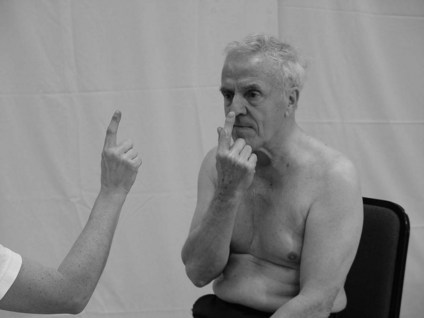
Finger-to-nose test
Therapist
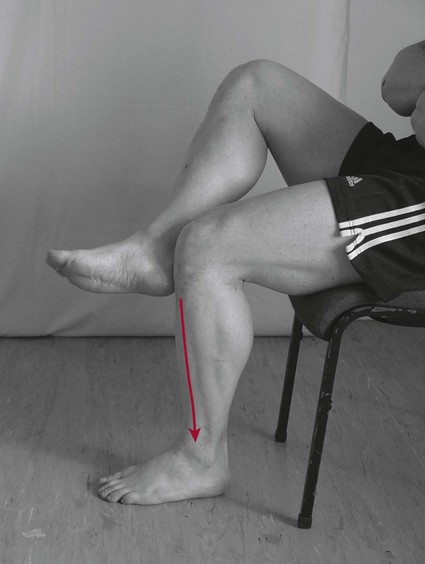
Heel–shin test
Therapist
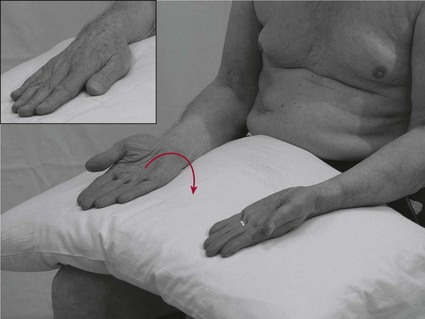
Dysdiadochokinesia
This is the inability to perform rapidly alternating movements.
Therapist
Note: Dysdiadochokinesia is commonly seen as part of ataxia (cerebellar lesion) but is also difficult to achieve for patients with hypertonia and hypotonia (S3.21).
Hand ‘flip’ test (inter-limb coordination)

Analysis
Testing coordination informs the therapist of the existence of a movement dysfunction but not about its cause. Further investigation using other objective assessment tools (S3.19–34), integrated with knowledge related to the patient’s pathological condition will facilitate analysis of the causal factors.
References and Further Reading
Ausim AS. And the olive said to the cerebellum: organization and functional significance of the olivo-cerebellar system. Neuroscientist. 2007;13:616-626.
Bakker M, Allum JH, Visser JE, et al. Postural responses to multidirectional stance perturbations in cerebellar ataxia. Experimental Neurology. 2006;202:21-35.
Berthier NE, Rosenstein MT, Barto AG. Approximate optimal control as a model for motor learning. Psychological Review. 2005;112:329-346.
Crawford JD, Medendorp WP, Marotta JJ. Spatial transformations for eye–hand coordination. Journal of Neurophysiology. 2004:92110-92119.
Fuller G. Neurological examination made easy, ed 3. Edinburgh: Churchill Livingstone; 2004.
Ilg W, Giese MA, Gizewski ER, et al. The influence of focal cerebellar lesions on the control and adaptation of gait. Brain. 2008;131:2913-2927.
Johansson RS, Westling G, Bäckström A, et al. Eye–hand coordination in object manipulation. Journal of Neuroscience. 2001;2117:6917-6932.
Schmitz TJ. Coordination assessment. In O’Sullivan SB, Schmitz TJ, editors: Physical rehabilitation assessment and treatment, ed 4, Philadelphia: FA Davis, 2001.
Shumway-Cook A, Woollacott MH. Motor control translating research into clinical practice, ed 3. Philadelphia: Lippincott Williams and Wilkins; 2007.
Thoma P, Bellebaum C, Koch B, et al. The cerebellum is involved in reward-based reversal learning. Cerebellum. 2008;7:433-443.