Introduction to Concepts of Pathology
PATHOGENESIS OF DISEASE
Pathology is defined as the branch of medicine that investigates the essential nature of disease, especially changes in body tissues and organs that cause or are caused by disease.36 Clinical pathology in medicine refers to pathology applied to the solution of clinical problems, especially the use of laboratory methods in clinical diagnosis. Pathogenesis is the development of unhealthy conditions or disease, or more specifically, the cellular events and reactions and other pathologic mechanisms that occur in the development of disease.
This text examines the pathogenesis of each disease or condition—that is, the progression of each pathologic condition on both its cellular level and clinical presentation whenever signs and symptoms are manifested. For the therapist, clinical pathology has a different meaning regarding the effects of pathologic processes (i.e., disease) on the individual’s functional abilities and limitations. The relationship between impairment and functional limitation is the key focus in therapy.
Pathology and the Guide to Physical Therapist Practice
The APTA Guide to Physical Therapist Practice4 was developed for clinical use by physical therapists as an expert consensus document. Panels of clinicians were involved in the first step of formulating the Guide, and then more than 1000 therapists across the country participated in reviewing the document.
Three conceptual models are integrated throughout the Guide: the (Nagi) Disablement Model, the Integration of Prevention and Wellness Strategies, and the Patient/Client Management Model. The Guide uses an expanded version of the disablement model to provide therapists with a common language to understand and communicate about our clients. The Guide is currently in its second (revised) edition and being revised for a third edition.
The Guide includes a section of specific diagnostic groups referred to as Preferred Practice Patterns that represent the major body systems and are designed to facilitate a systems approach to patient/client management. The Practice Patterns are described in four sections: musculoskeletal, neuromuscular, cardiopulmonary, and integumentary. It is not possible to place all diseases included just within these four categories at this time. The therapist will encounter multiple medical comorbidities that extend beyond the four categories of the Preferred Practice Patterns outlined in the Guide. However, therapists will not be devising intervention strategies for liver disease, for example, but must be aware of the impact that such diseases may have on the rehabilitation process. The most likely practice patterns associated with each disease or disorder discussed are presented in the Special Implications for the Therapist boxes. These patterns may vary with each episode of care, depending on clinical presentation.
Advances in medicine have resulted in a population with greater longevity but also with a more complex pathologic picture. Orthopedic and neurologic conditions are no longer present as singular phenomena; they often occur in a person with other medical pathology. We must be knowledgeable of the impact other conditions and diseases have on the individual’s neuromusculoskeletal system and the necessary steps that must be taken to provide safe, effective treatment.
CONCEPTS OF HEALTH, ILLNESS, AND DISABILITY
Many people and organizations have attempted to define the concept of health, but no universally accepted definition has been adopted. A dictionary definition describes health in terms of an individual’s ability to function normally in society. Some definitions characterize health as a disease-free state or condition. The World Health Organization (WHO)54 has defined health as a state of complete physical, mental, and social well-being and not merely as the absence of disease or infirmity. All of these definitions present health as an either/or circumstance, meaning an individual is either healthy or ill.
Health is more accurately viewed as a continuum on which wellness on one end is the optimal level of function and illness on the other may be so unfavorable as to result in death. Health is a dynamic process that varies with changes in interactions between an individual and the internal and external environments. This type of definition recognizes health as an individual’s level of wellness.
Health reflects a person’s biologic, psychologic, spiritual, and sociologic state. The biologic or physical state refers to the overall structure of the individual’s body tissues and organs and to the biochemical interactions and functions within the body. The psychologic state includes the individual’s mood, emotions, and personality.
The spiritual aspect of health addresses the individual’s religious needs, which may be affected by illness or injury. The spiritual dimension in health care focuses on the integration of mind, body, and spirit, with the goal of promoting whole-person healing. The sociologic or social state refers to the interaction between the individual and the social environment. A high level of wellness or holistic health is achieved when the biopsychosocial-spiritual needs of a person are met.
Illness
Illness is often defined as sickness or deviation from a healthy state, and the term has a broader meaning than disease. Disease refers to a biologic or psychologic alteration that results in a malfunction of a body organ or system. Disease is usually a term used to describe a biomedical condition that is substantiated by objective data such as elevated temperature or presence of infection (as demonstrated by positive blood cultures).
Illness is the perception and response of the person to not being well. Illness includes disturbances in normal human biologic function and personal, interpersonal, and cultural reactions to disease. Disease can occur in an individual without he or she being aware of illness and without others perceiving illness. However, a person can feel very ill even though no obvious pathologic processes can be identified.
Incidence and Prevalence
When discussing various diseases, disorders, and conditions, incidence and prevalence may be reported. Incidence is the number of new cases of a condition in a specific period of time (e.g., 6 months or 1 year) in relation to the total number of people in the population who are “at risk” at the beginning of the period. Prevalence measures all cases of a condition (new and old) among those at risk for developing the condition. Measures of prevalence are made at one point in time (e.g., on a specific day).
Natural History
The natural history of a condition, disorder, or disease describes how it progresses over time. The natural history of some conditions, such as cancer, can be judged based on the stage of the tumor at the diagnosis and response to treatment. Scientists are actively engaged in identifying predictive factors that help tell what the patient/client’s outcome might be. In medicine, predictive factors are the closest thing we have to a crystal ball.
Even with known predictive factors, the natural history is not always clear; predicting what is going to happen and when it is going to happen can have wide or narrow margins, depending on the condition. For example, individuals with some forms of muscular dystrophy have a more predictive natural history, whereas individuals with cerebral palsy may not be so easy to gauge, especially during the early years of growth and development.
The therapist must develop a plan of care keeping in mind the natural history of the condition and where the individual is in the lifespan cycle. Some thought should be given to dovetailing our view of impairments, dysfunctions, and disabilities with the natural history of the disease, condition, and illness. This is particularly important when working with individuals who have longterm, degenerative or progressive neurologic, or chronic conditions.
Improvements in treatment for neurologic and other conditions previously considered fatal (e.g., cancer, cystic fibrosis) are now extending the life expectancy for many individuals. Improved interventions bring new areas of focus such as quality of life issues. With some conditions (e.g., muscular dystrophy, cerebral palsy), the artificial dichotomy of pediatric versus adult care is gradually being replaced by a lifestyle approach that takes into consideration what is known about the natural history of the condition.
Acute Illness
Acute illness usually refers to an illness or disease that has a relatively rapid onset and short duration; it is not synonymous with “severe.” The condition often responds to a specific treatment and is usually self-limiting, although exceptions to this definition are numerous. If no complications occur, most acute illnesses end in a full recovery and the individual returns to the previous level of functioning.
Subacute refers to how long a disease has been present, but there is no set time that divides subacute from the other time descriptions (i.e., acute and chronic). Subacute describes a time course that is between acute and chronic. A symptom that is subacute has been present for longer than a few days but less than several months. Chronic conditions sometimes flare up and may be referred to as subacute.
Acute illnesses usually follow a specific sequence, or stages of illness, from onset through recovery. The first stage involves the experience of physical symptoms (e.g., pain, shortness of breath, fever), cognitive awareness (i.e., the symptoms are interpreted to have meaning), and an emotional response, usually one of denial, fear, or anxiety.
Subsequent stages of an acute illness may include assumption of a sick role as the person recognizes the problem as being sufficient to require contact with a health care professional. If the illness is confirmed, the individual continues in the sick role; if it is not confirmed, a return to normalcy may occur or the person may continue to seek health care to identify the illness.
A stage of dependency occurs when the person receives and accepts a diagnosis and treatment plan. This type of dependency in the psychologically and emotionally balanced person represents awareness, acceptance, reliance on diagnosis, and care beyond self-help. This definition of dependency differs from dependency associated with dependent personality disorder, in which the affected person lacks self-confidence or the ability to function independently, and allows others to assume responsibility for his or her care. Depending on the severity of the illness, the individual may give up independence and control and assume a more dependent sick role. During this stage, sick people often become more passive and concerned about themselves.
Most people move from acute or subacute to the final stage of recovery or rehabilitation. During this stage, the individual gives up the sick role and resumes more normal activities and responsibilities. Individuals with long-term or chronic illnesses may require a longer period to adjust to new lifestyles.
Chronic Illness
Chronic illness describes illnesses that include one or more of the following characteristics: permanent impairment or disability, residual physical or cognitive disability, or the need for special rehabilitation and/or long-term medical management. Chronic illnesses and conditions may fluctuate in intensity as acute exacerbations occur that cause physiologic instability and necessitate additional medical management (e.g., diabetes mellitus, fibromyalgia, rheumatoid arthritis). A person who has exacerbations of chronic illness may progress through the stages of illness described in the previous section.
Psychologic Aspects
The most important factor influencing psychologic reactions to illness is the premorbid (before illness) psychologic profile of the affected person. For example, a person with a dependent-type personality may become very dependent, perhaps seeking unusually large amounts of advice or reassurance from the health care specialist or expecting attention beyond that required for the degree of illness present. A narcissistic (self-centered) person may be particularly concerned about the need to take medication or the loss of the ability to work. The stoic person (indifferent to or unaffected by pain) may have difficulty admitting to being sick at all.
Other factors that affect a person’s psychologic reaction include the extent of the illness and the particular symptoms that develop. Extremely mild disease may have little effect, whereas completely unexpected and debilitating illness may be very distressing. A common reaction to any illness is fear or anxiety related to the loss of control over one’s own body. Denial is an unconscious defense mechanism that allows a person to avoid painful reality as long as possible. Denial can be a natural part of the process of dealing with illness, which culminates in acceptance.
Noncompliance with treatment may have a psychologic basis (e.g., denial: “There is nothing wrong with me, so I do not need medical treatment.”), but it may also occur as a result of previous experience. For example, noncompliance with prescribed corticosteroid therapy may be based on aversion to side effects experienced during use of this drug in a previous disease flare. With chronic autoimmune diseases (e.g., connective tissue diseases), denial may continue for years as a coping mechanism for the individual who continues to decline in physical functional capacity.
It is important to recognize that psychologic or psychiatric symptoms, such as impairment of memory, personality changes (e.g., paranoia), loss of impulse control, or mood disorders (e.g., persistent depression or elation), can have a functional or organic basis. Functional symptoms occur without significant physical dysfunction of brain cells, whereas organic symptoms can be caused by abnormal physiologic changes in brain tissue. An example of a functional symptom is depression that is considered to be the psychologic consequence of a general medical condition (e.g., myocardial infarction).
Organic symptoms occur as a direct physiologic consequence of a medication or medical condition. For example, onset of corticosteroid-induced psychologic symptoms is often dose-related, and symptoms subside as the corticosteroids are tapered. Another example of an organic basis for symptomatology is the person with systemic lupus erythematosus (SLE) who experiences symptoms of organic mental disorders secondary to SLE-mediated vasculitis, called lupus cerebritis, or the person with end-stage liver disease who develops hepatic encephalopathy when toxic substances in the blood, such as ammonia, reach the brain.
Disability
Disability is a large public health problem in the United States affecting an estimated 54 million people who report disabling conditions. This figure illustrates that nearly 20% of the U.S. population currently lives with a disability. Prevalence of disability is higher among women than men and is reported highest among people 65 years of age and older. One of the national health goals for 2010 is to eliminate health disparities among different segments of the population, including among people with disabilities. National estimates of disability range from 15% to 20% for adults over the age of 18 years, but these figures are most likely underestimated and do not account for severity or duration of disability.13
Disability is often viewed by physical therapists from a biopsychosocial model, which incorporates and integrates the traditional medical model with the less stringent and more flexible social model of disability. The medical model confines disability as a descriptor of the affected individual. In this context, disability requires intervention by others (usually health care providers) to correct the problem. The social model of disability is more likely to see an unaccommodating environment and lack of social response to individuals with disabilities as the problem requiring a social or political response.29
Disablement and Classification Models28
There are several contemporary biopsychosocial models proposed today to describe disability classifications and give us a framework for identifying the consequences of diseases, disorders, and injuries.
Nagi Disablement Model.: The Nagi model represents a system often used by health care professionals to classify the impact of disease or trauma.39 Nagi suggests that pathology produces pain and impairments, which then lead to functional limitations and disability. It works well for clinical practice at the level of impairment in which the therapist works and understands the client’s needs. The major components of this model include the following:
Disease or pathology describes the underlying pathogenesis and abnormal cellular and physiologic processes. Impairment(s) refer to a loss or abnormality at the tissue, visceral, and/or body system level. An impairment can be temporary or permanent and is considered to occur at the organ level. Functional limitations occur at the individual level and restrict that person’s performance of specific actions. Disability is the actual limitation of physical or mental function in a social context. Any restriction or lack of ability to perform an activity in a normal manner or within the normal range may represent a disability.
Not all disease leads to impairment and not all impairment leads to disability. For example, diabetes can result in impairment (e.g., diminished circulation), but not all people with diabetes sustain a disability (e.g., vision loss or amputation). In another example, an individual with a cardiopulmonary condition would have impairment at the level of the tissue or organ system such as ventilation, respiration (gas exchange), and circulation. The functional limitation would be the restrictions in the individual’s ability to perform specific tasks such as climbing stairs or carrying groceries.16 The disability occurs because the functional limitations are severe enough to prevent this individual from holding down a job or caring for children at home.
Nagi proposed that functional limitations were the result of impairments and consisted of an individual’s inability to perform the tasks and roles that constitute usual activities for that individual. According to the Nagi model, disability is defined as the patterns of behavior that emerge over long periods of time when functional limitations cannot be overcome to create normal task performance or role fulfillment.
International Classification of Functioning, Disability, and Health (ICF).: The WHO’s framework to classify and code information about health and provide standardized language is the International Classification of Functioning, Disability, and Health (ICF) established in 2001. The ICF is presented as the international standard to describe and measure health and disability from a biopsychosocial perspective by all health care professionals. The ICF is a good framework for research from a global perspective.
The ICF replaces the International Classification of Impairments, Disabilities, and Handicaps (ICIDH) classification established in 1980.57 While traditional health indicators are based on the mortality (i.e., death) rates of populations, the ICF shifts focus to “life” (i.e., how people live with their health conditions and how these can be improved to achieve a productive, fulfilling life). Most notable in the current structure is the inclusion of “host factors” that impact the behavior of the individual such as demographic background, physical and social environments, and psychologic status. The full description of this model can be found at http://www.who.int/classification/icf. The ICF disablement components (Fig. 1-1) include the following:
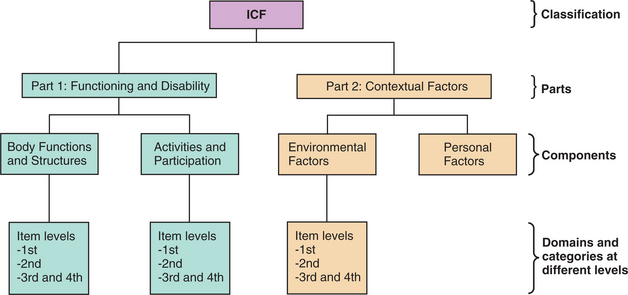
Figure 1-1 Structure of the International Classification of Functioning, Disability, and Health (ICF). (From World Health Organization WHO): Principles and process for including classifications in the Family of International Classifications, Geneva, Revised 2004, WHO.) WHO
The ICF describes how people live with their health condition. The ICF is a classification of health and uses these health-related domains to describe body functions and structures and activities and participation from body, individual, and societal perspectives. Because an individual’s functioning and disability occur in a context, the ICF also includes a list of environmental factors.56
The ICF changes our understanding of disability, no longer presenting disability as a problem of a minority group, or just of people with a visible impairment or in a wheelchair. For example, a person living with HIV/AIDS could be disabled in terms of his or her ability to participate actively in a profession. In that case, the ICF provides different perspectives as to how measures can be targeted to optimize that person’s ability to remain in the work force and live a full life in the community.58
ICF—Language.: The ICF introduces new “enablement” language to replace older disablement terminology that implied distinctions between individuals who are healthy and those who have disabilities. The new language defines body functions and structures as physiologic or psychologic functions of body systems or anatomic parts (e.g., organs, limbs). Impairments are defined as problems in body function or structure.
Activity is defined as the execution of specific tasks or actions by an individual. Activity limitations are the difficulties that an individual might have in executing activities, and participation is the individual’s involvement in life situations. Participation restrictions are problems the individual might have in real-life situations.28,56
Secondary conditions or impairments of body structures can result from limitation of activity and participation. Joint contractures, disuse atrophy, and heart disease are examples of changes from inactivity. If not prevented, these changes can lead to further limitation of activity but are not part of the underlying health condition. It is important to remember that the same impairments may not result in the same extent of activity limitation or that activity limitation may not limit the participation in a life role in the same way in two different individuals.
An example of this continuum could be described this way: a person has survived a stroke in the left side of the brain and has the impairments of hemiparesis and aphasia. This person may not be able to walk or talk but can participate in work with the assistance of a walker and communication board. On the other hand, a person who survived a stroke on the right side of the brain may be able to walk but not be able to participate in work because of loss of executive function and poor judgment.
If the first individual does not have access to a walker and communication board because of lack of funding, he or she may not be able to return to work. In many cultures, it is tradition that if a person is injured or has a medical condition, it is the responsibility of the family to provide passive or palliative care; that person may never have the opportunity to rehabilitate to full potential.
The ICF framework takes a broad biopsychosocial view that looks beyond mortality and disease to focus on how people live with their conditions.28,29 The ICF framework promotes international exchange using a common and consistent framework and universal language to discuss disability and related phenomena.29 Steps are being taken by some to incorporate the ICF into practice. For example, a list of intervention categories relevant for physical therapy according to the ICF has been identified.21
Cognitive Disability53
Problems such as mental illnesses like depression, alcoholism, schizophrenia, and cognitive impairments, although responsible for only about 1% of deaths, are seriously underestimated sources of disabilities that account for 11% of the world’s disease burden.55 These conditions are often undiagnosed, and although therapists cannot diagnose these impairments, recognizing the deficits is important. Only cognitive disability is discussed in this section; common mental illnesses are discussed in Chapter 3. Five types of cognitive deficit are associated with specific areas of brain damage and linked to possible causes that may be barriers to successful treatment (Table 1-1).
Table 1-1

HIV, Human immunodeficiency virus; AIDS, acquired immunodeficiency syndrome.
Modified from Woltersdorf MA: Beyond the sensorimotor strip, Clin Management 12:63-69, 1992.
Executive functions may be described as cortical functions involved in formulating goals and in planning, initiating, monitoring, and maintaining behavior.31 Behavior is defined here in its broadest terms to include not only overt motor behavior but also affective and social behavior. A person with executive function deficits typically appears inert or apathetic. Clinically, these clients typically have a right hemisphere lesion and apraxia, unilateral neglect, or both. When frontal lobe damage occurs, the effects of impaired executive functions may be attributed to depression. Although the two may occur simultaneously, depression is usually characterized by a lack of energy, whereas impaired executive functions are demonstrated by a lack of involvement.
Complex problem solving may be described as the effective handling of new information. Impaired problem solving results in concrete thinking, inability to distinguish the relevant from the irrelevant, erroneous application of rules, and difficulty generalizing from one situation to another. For example, when a client learns how to accomplish wheelchair transfers and then generalizes that information to various settings (bed to chair, chair to toilet, chair to car, in hospital, at home), he or she is using new information in complex problem solving.
Information processing involves the speed with which information travels from one part of the brain to another and the amount of information assimilated at that speed.31 Whereas complex problem solving has to do with the orchestration of information, information processing involves the efficient transfer of information.
As a result of genetic, environmental, and educational factors, some people are more proficient processors than others. As a result of trauma, some people may lose processing ability and speed. Noise levels, external sensory stimulation (e.g., presence of other people and other activities), and presentation of more than one kind of information at a time (e.g., providing a written home program then discussing the time of the next appointment) are examples of distractions to people with reduced information-processing abilities.
Memory deficits result from a failure to store or retrieve information. Before it can be determined that the person is experiencing a memory lapse, it must be established that the material was learned in the first place. Memory problems typically are acquired rather than developmental. Depression may masquerade as memory loss, but the depressed person is usually less attentive or interactive with the environment and therefore registers (or learns) less. For example, a client may appear to be suffering from a memory dysfunction when, in fact, the decreased attention span is a result of depression that has reduced learning.
Learning disability occurs in a person with normal or near-normal intelligence as difficulty acquiring information in specific domains such as spelling, arithmetic, reading, and visual-spatial relationships. Therapists most commonly encounter learning disabilities manifested as noncompliance with written treatment programs, repeated tardiness or absence for treatment sessions, and an overly anxious approach to the physical symptoms that have brought the client to the therapist in the first place.
THEORIES OF HEALTH AND ILLNESS
Many theories exist as to the cause of illnesses. In the latter part of the nineteenth century, Louis Pasteur took medicine out of the Dark Ages. It was not “bad air” or “bad blood” that caused diseases like malaria and yellow fever but pathogens transmitted by mosquitoes.
Pasteur’s germ theory promoted our understanding of infectious disease and helped reduce deaths from infection. Pasteur proposed that a specific microorganism was capable of causing an infectious disease. Infections, such as poliomyelitis, tuberculosis, human immunodeficiency virus (HIV) associated with acquired immunodeficiency syndrome (AIDS), or legionellosis (legionnaire’s disease), are caused by a known agent. Once the causative agent is identified, specific treatment methods can be determined.
Pasteur’s germ theory has been labeled Germ Theory, Part I and has been expounded on by today’s biologists in what is referred to as Germ Theory, Part II. Taken from Darwin’s description of how an organism and its environment fit together, it is now restated that the success of an organism is relative to competing organisms. According to this theory, genetic traits that may be unfavorable to an organism’s survival or reproduction do not persist in the gene pool for very long. Natural selection, by its very definition, weeds them out in short order. By this logic, any inherited disease or trait that has a serious impact on fitness must fade over time because the genes responsible for the disease or trait will be passed on to fewer and fewer individuals in future generations. Common illnesses that cannot be linked to genetics or to some hostile environmental element (including lifestyle) must have some other explanation.
The current germ theory suggests that diseases present in human populations for many generations that still have a substantial negative impact may have an infectious origin. Chronic diseases of the late twentieth century that have been considered hereditary, environmental, or multifactorial may in fact be caused by an infectious pathogen. For example, herpesviruses have been linked to multiple sclerosis, Kaposi’s sarcoma, B-cell lymphomas, Burkitt’s lymphoma, and several other forms of cancer.
Helicobacter pylori, found in the stomachs of a third of adults in the United States, causes inflammation of the stomach lining and can result in ulcers. In most cases, these ulcers can be cured in less than a month with antibiotics. The lymphoid tissue of the stomach can produce a low-grade gastric lymphoma under the influence of this bacterium. Eradication rates of 80% to 90% have been noted with the use of antibiotics, although antibiotic resistance may be decreasing these cure rates. However, this may be the first time in medical history that cancer has been cured with an antibiotic.1,8,34,51
Heart disease is now being linked to infections such as herpes simplex virus (HSV), enterovirus (ES), and Chlamydia pneumoniae, a newly discovered bacterium that causes pneumonia and bronchitis. Several studies have now shown that people who have had a heart attack have high levels of antibodies to one or more of these infections from previous exposure, often during childhood.1,27,29,41
Germ Theory, Part II also hypothesizes that clinical depression or mental illness, such as schizophrenia, may have an underlying infectious basis given how common these conditions are in the general population. According to germ theory proponents, natural selection should have eliminated any genes for these conditions to ensure survival and reproduction. No one has found a depression virus or a schizophrenia virus yet, but research continues in this area. The germ theory cannot explain all diseases, and other more complex theories have been postulated.
Biomedical Model
The biomedical model explains disease as a result of malfunctioning organs or cells. Within this model, conditions can be classified as diseases if they have a recognized cause, if a change occurs in structure or function of an organ, and if a consistently identifiable group of signs and symptoms is apparent. The biomedical model focuses on cause-and-effect relationships but does not take into account psychosocial components of disease, such as varying reactions to a disease because of age, lifestyle, personality, and compliance with therapy.
Neither the germ theory nor the biomedical model can explain the widespread increase in noninfectious chronic diseases that affect modern civilizations. In the past, the high death rate from epidemics of infectious diseases meant that many people did not live long enough for chronic illnesses to develop, especially those that occur with aging. With the development of penicillin in 1928 and the subsequent development of other antibiotics, people in the twentieth century have had reduced mortality from infectious disease. Heart disease and cancer—ailments that plague modern industrialized nations—have become the center of focus.
Multicausal Theory
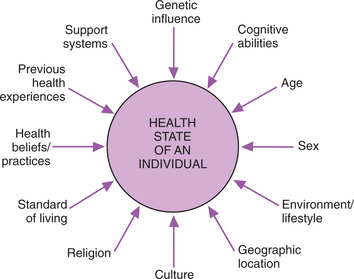
It is now recognized that lifestyle, diet, and stress response contribute to the development of diseases, and treatment interventions are focusing more on the relationship of the individual with his or her external and internal environment. Multicausal theories have been proposed to take into account the many additional factors associated with health and the development of illness (Fig. 1-2). Many of these variables are discussed further in Chapter 2.
Homeostasis Theory
Homeostasis theories developed in the nineteenth century continue to be expanded on through the twenty-first century. Homeostasis is the body’s ability to maintain its internal environment in a constant state of equilibrium despite external influences that promote imbalance. Homeostasis begins at the cellular level in that the cell receives nutrients, oxygen, water, and essential minerals from the environment. It uses these resources to generate energy, maintain its own integrity, and contribute to the body’s internal stability. The body’s ability to maintain temperature, blood pressure, and levels of fluid and electrolytes, serum glucose, blood oxygen, and carbon dioxide within a given range are examples of dynamic homeostasis that begins at the cellular level. External stimuli can alter the body’s equilibrium or homeostasis. External demands may exceed the capacity of the cell to adapt, resulting in a permanent disequilibrium and injury or illness.
Injury occurs when the cells or tissues have been required to adapt beyond their limitations. Like a muscle that has exceeded its ability to stretch, has ruptured, and is no longer able to contract, cells can be irreparably damaged and unable to return to the original steady state. Illness is the result of an imbalance in the body’s (cell’s) ability to regulate the internal environment. The concept of “fight, flight, or freeze” to explain the body’s reactions to emergencies was added to the homeostasis theory and continues to be used today to explain homeostasis as a dynamic equilibrium designed to maintain a steady state.
General Adaptation Syndrome
The general adaptation syndrome continued to build on the homeostasis theory and the concept of fight, flight, or freeze by describing a response to stress that, regardless of diagnosis, has common symptoms such as appetite loss, weight loss, myalgias, and fatigue. The entire body responds to stress in an attempt to maintain or adapt through the autonomic and central nervous systems. If the demand or stress continues, the adaptive capacity of the body can be exceeded, and disease may result.
This theory suggests that stress causes disease by placing excessive demands on the body, which in turn produces high levels of adaptive hormones, such as glucocorticoids, which reduce inflammation, and mineralocorticoid hormones, which regulate electrolyte and water metabolism. These hormones lower the body’s resistance to disease and cause organ damage. When stress is continuous, the adaptive capacity of the body may be exceeded, and disease (or even death) may result.
Psychosocial Theory
Psychosocial theories of disease attempt to integrate physiologic, psychologic, and social factors to explain disease. An individual’s degree of resistance to microbes depends largely on how well he or she is coping with internal and external stresses. Resistance to infectious disease, allergies, and possibly cancer depends on a well-functioning immune system. People who cope poorly with stress have significantly impaired immune responses, as manifested by a diminished activity level in natural killer cells. These are a special type of leukocyte that destroy viruses and cancer cells without having previously encountered them. Biopsychosocial concepts as they relate to health are discussed more fully in Chapter 3.
Psychoneuroimmunology Theory
As new research added important information, the psychosocial theory has been modified to become the Psychoneuroimmunology (PNI) Model first described in the 1980s. PNI is the study of the interactions among behavior and neural, endocrine, enteric, and immune system functions.
Those who founded the research in this area point out that PNI is a misnomer because it reveals only part of the process and redundantly includes the brain as psycho and neuro, leaving out the powerful impact of the endocrine system.32 The literature refers to this theory by a variety of names, such as neuroendocrine immunology, neurogastroimmunology, or psychoimmunology, and is seemingly dependent on the system under investigation.
Illness was once thought of as the result of a breakdown within the immune system alone, but immune function is now recognized as the integrative defense mechanism of multiple systems. This theory has outlined the influence of the nervous system on immune and inflammatory responses and how the immune system communicates with the neuroendocrine systems. This information is very relevant in understanding host defenses and injury/repair processes.
Further, the integration of the hypothalamic-pituitary-adrenal axis and the neuro-endocrine-enteric axis has a biologic basis first discovered in the late 1990s. Physiologically adaptive processes occur as a result of these biochemically based mind-body connections. We now know that each thought and emotion is a message to the rest of the body, mediated by an intricate array of nerve signals, hormones, and various other substances.17
Candace Pert,32,45 formerly a molecular biologist at the National Institutes of Health (NIH), made a groundbreaking discovery when she identified the biologic basis for emotions (neuropeptides and their receptors). This new understanding of the interconnections between the mind and body goes far beyond our former understanding of psychosomatic or psychosocial theories of health and illness.
It is now known that these chemical messengers (sometimes referred to as peptides, neuropeptides, ligands, neurotransmitters, or information molecules) move through the blood stream to every cell of the body. When these chemicals find body cells with receptors that attract them like magnets, they attach and make significant changes in that cell structure and organ system. These information molecules are the messengers the body uses to communicate between all the major body systems. For example, both the digestive (enteric) system and the neurologic system communicate with the immune system via these peptides. These three systems can exchange information and influence one another’s actions.
Knowledge of PNI sheds new light on many of the previously postulated theories of health and illness, whereas understanding dysfunctions in the PNI system may highlight a wide variety of system disorders and diseases. For example, explaining how the body maintains homeostasis through autonomic temperature regulation (Homeostasis Theory) will now have an added dimension when considering the role of these information molecules or understanding that the sympathetic nervous system controls cardiovascular and immune functions, hormones control energy balance, and neurohormones control salt and fluid balance (General Adaptation Syndrome) via the interactions of the PNI.
Continued research in this area has brought new information to light about the effects of variables, such as stress and coping, personality, mental status, socioeconomic status, and work and family life, and their role in the outcome of surgery or the development and progression of disease, morbidity, and mortality (e.g., Multicausal Theory, Psychosocial Theory).6,20,33
Energy Medicine
Many well-known scientists (e.g., Candace Pert, James Oschman, Larry Dossey) with extensive training and research in the areas of biophysics and biology have attempted to bring together evidence from a range of disciplines to provide an acceptable explanation for the energetic exchanges that take place in all therapies.15,43 Studies in biophysics have shown that physical instabilities result in fluctuations, the quantum properties of which can be applied to regulatory control mechanisms in living organisms with promising results. The discovery of the existence of macroscopic quantum coherence in living systems has led to a new field of mind-body medicine and a new understanding of the role of natural “energy forces” within the body in maintaining normal health and well-being.26
At the same time, behavioral scientists have been exploring the concept that consciousness in the form of beliefs, expectations, and intention plays a central role in healing. Studies of prayer and the spiritual aspects of medicine have moved many health care professionals away from a biomedical model of health care to a model of whole-person caring.30 This in turn has led to interest in how these energies or forces may be used to assist in healing and the restoration of normal health. The concept of energy medicine has resulted in a new discipline called complementary and alternative medicine (CAM) or complementary and integrative medicine (CIM).
HEALTH PROMOTION AND DISEASE PREVENTION
The topic of health promotion and disease prevention has taken front and center stage in many arenas within the health care industry. There has been a change in health care focus from intervention for cure and healing to healing, health, wellness, and prevention. Traditional health promotion has not been to take care of the sick and disabled but rather to prevent disease and disability in the healthy.22 Today’s concepts of health place all health on a continuum. The focus is on practicing healthy behaviors, even in the presence of disease and disability. Although disability can increase a person’s risk of or susceptibility to secondary health conditions, the primary disability does not mean that individual is “unhealthy.”
Research has proved without a shadow of a doubt that many of today’s illnesses, disorders, and conditions can be prevented altogether. Diseases of longevity, lifestyle, and health behaviors are prevalent, and more people are living longer with chronic diseases, all of which drive up the cost of health care. The health care industry as a whole and especially third party payers have been slow to respond with ways to change our approach to this information.
The first set of national health targets was published in 1979 in Healthy People: The Surgeon General’s Report on Health Promotion and Disease Prevention. Healthy People 2000 was released in 1990 as a management tool with goals to reduce mortality, increase independence among older adults, reduce disparities in health among different population groups, and achieve access to preventive health services.
This program has become an ongoing comprehensive program of public health planning now called Healthy People 2010 that is a tremendously valuable asset to all who work to improve health. Healthy People 2010 (available at http://health.gov/healthypeople/) has a series of objectives to bring better health to all people in this country and to eliminate disparities among different segments of the population. These include differences that occur by gender, race or ethnicity, education or income, disability, residence in rural localities, and sexual orientation. This program has a built-in means to measure progress toward achieving 10-year targets across a broad range of health behaviors and outcomes.
Health Promotion
Health promotion as a concept and as an active process is built on the principles of self-responsibility, nutritional awareness, stress reduction and management, and physical fitness. Health promotion is not limited to any particular age or level of ability but rather extends throughout the lifespan from before birth (e.g., prenatal care) through old age, including anyone with a disability of any kind.
Health promotion programs that encompass the entire lifespan are applicable to people of both genders and all socioeconomic and cultural backgrounds, to those who have no health problems, and to those with chronic illnesses and disabilities. Many types of health promotion programs are in existence such as health screening, wellness, safety, stress management, or support groups for specific diseases.
Disease Prevention
Even since the last edition of this text, disease prevention has gained momentum and today is at the forefront of the health care industry. It is now recognized and addressed by greater numbers of health care professionals that preventing disease is more cost-effective than treating disease. Many new areas of study have developed as a result of this paradigm shift in focus from treatment to prevention. Scientists are revolutionizing the way we fight infection, manage chronic illness, and stay well. For example, one group has coined the term immunotics to describe this new approach to preventing and treating disease.14
Immunotics is to the twenty-first century what antibiotics were to the twentieth century—but perhaps even better. Whereas antibiotics are used to treat illness after it occurs, immunotics is designed to prevent illness in the first place. Unlike antibiotics, which can have serious side effects, immunotics has no side effects; at the very least it adopts the Hippocratic philosophy of do no harm.14
In another area, cancer prevention strategies to reduce the incidence of cancer occurrence and recurrence have commanded the attention of oncology researchers. Chemoprevention, the use of agents to inhibit and reverse cancer, has focused on diet-derived agents. Another term, preventive oncology, is a relatively new branch of medicine that includes both primary and secondary prevention.
Preventive medicine as a branch of medicine is categorized as primary, secondary, or tertiary. Primary prevention is geared toward removing or reducing disease risk factors, for example, by maintaining adequate levels of calcium intake and regular exercise as a means of preventing osteoporosis and subsequent bone fractures or by giving up or not starting smoking to reduce multiple causes of morbidity. Use of seat belts, use of helmets by motorcyclists and bicyclists, and immunizations are other examples of primary prevention strategies.
Secondary prevention techniques are designed to promote early detection of disease and to employ preventive measures to avoid further complications. Examples of secondary prevention include skin tests for tuberculosis or screening procedures such as mammography, colonoscopy, or routine cervical Papanicolaou smear.
Tertiary prevention measures are aimed at limiting the impact of established disease (e.g., radiation or chemotherapy to control localized cancer). Tertiary prevention involves rehabilitation and may end when no further healing is expected. The goal of tertiary prevention is to return the person to the highest possible level of functioning and to prevent severe disabilities.
Specific therapy interventions are not the focus of this text but whenever possible, risk factor reduction strategies are offered because risk factors are a part of the discussion surrounding each disease and therapists play an important role in disease prevention and health promotion.
GENETIC ASPECTS OF DISEASE
Advances in immunology and molecular genetics have accelerated our understanding of the genetic and cellular basis of many diseases. Remarkable progress has been made in recombinant deoxyribonucleic acid (DNA) technology, making it possible to offer molecular and cellular treatments for infectious diseases, inherited disorders, and cancer. Development of the monoclonal antibody technique is finding ever-increasing uses in the treatment of diseases such as rheumatoid arthritis, cancer, and AIDS.38
At the same time, innovations in gene therapy have advanced the field of vaccine development, especially recombinant vaccine technology. Although the field of vaccination has historically focused on the prevention of infectious diseases, this technology provides a broader base for immune modulation of pathologic responses underlying other conditions.38
The completion of the Human Genome Project just 50 years after the discovery of the structure of DNA, combined with advances in technology, has enabled researchers to begin identifying the actual genes that encode particular disorders.40 It may be possible in the near future to treat altered gene structure (gene therapy) in an attempt to cure or control previously incurable diseases. The laboratory studies and advances in the collection of immune cells made it possible to begin clinical trials of gene therapy in the early 1990s. The recent explosion in biotechnology has advanced the field of genetic testing, which is a necessary component in the genetic treatment of diseases and disorders.
The Human Genome Project
The Human Genome Project, an international project led in the United States by the National Human Genome Research Institute (NHGRI) and the Department of Energy, was completed in April 2003 and provides a reference DNA sequence of the human genome. Researchers identified all 100,000 genes existing in 23 pairs of chromosomes and deciphered the genetic code by sequencing the 3.1 billion base pairs of human DNA and mapping their location in the chromosomes.
The goals of this project have been to identify all human genes, map the genes’ locations on chromosomes, and ultimately provide detailed information from the genetic coding about how the genes function. Because virtually every human illness and even many lifestyle-related conditions have a hereditary component, the Human Genome Project may hold the key to the prevention or cure of many, if not all, diseases and disorders.47
The Human Genome Project dispelled the idea that race or ethnic-based biologic differences existed when they discovered that 99.99% of the genome is the same across the human population, regardless of race or ethnic origin. Individual variations can increase the risk of disease as some people can become more vulnerable to bacteria, viruses, toxins, and chemicals, but the Human Genome Project disproved many previously held beliefs about biologically based racial differences.
Knowing the order in which these chemical units are arranged on each strand of DNA does not tell where the genes are located within the genome, the specific function of each gene in the sequence, or which genes make which proteins. The study of genomes has been labeled genomics, which includes the investigation of an organism’s entire hereditary information encoded in the DNA. The term comes from the words “gene” and “chromosome.”
The genome of any organism (including humans) is a complete DNA sequence of one set of chromosomes. Genomics is different from genetics, which is generally the study of single genes or groups of genes. Genomics with its unfolding of the complete DNA sequences will provide a basis for the study of susceptibility to disease, the pathogenesis of disease, and the development of new preventive and therapeutic approaches.
Additionally, the completion of the Human Genome Project has enhanced the widespread use of prenatal diagnosis and DNA chip technology and will make it possible to analyze a sample of DNA collected from saliva. Drugs designed and prescribed to accommodate individual differences in metabolism may be possible from the data derived from this project. All of these areas of interest will be the substance of future studies.
Information about the genes is made available immediately on the Internet to scientists, clinicians, librarians, educators, and the general public. The cataloging and filing of this information are under the auspices of the Cancer Genome Anatomy Project (CGAP). The Human Cancer Genome Project is another program that is attempting to develop a comprehensive description of the genetic basis of human cancer and specifically the complete identification and characterization of genetic alterations present in a large number of major types of cancer (Fig. 1-3).

Figure 1-3 Example of genetic basis for cancer found in early cervical carcinoma. The gain of chromosome 3q (tumor DNA seen as green) that occurs with HPV16 infection defines the transition from severe dysplasia/carcinoma in situ to invasive carcinoma of the uterine cervix. Genetic testing can help identify chromosomal aberrations such as this that occur during carcinogenesis. (From Heselmeyer K, Schrock E, du Manoir S, et al: Gain of chromosome 3q defines the transition from severe dysplasia to invasive carcinoma of the uterine cervix, Proc Natl Acad Sci USA 93:479-484, 1996.)
Gene Therapy
Genes are the chemical messengers of heredity. Two hundred thousand (200,000) human genes composed of DNA molecules along a double helix and carrying instructions for synthesizing every protein that the body needs to function properly (Fig. 1-4) have been identified. Their order determines the function of the gene. Genes determine everything from appearance to the regulation of everyday life processes (e.g., how efficiently we process foods, how effectively we fight infection).
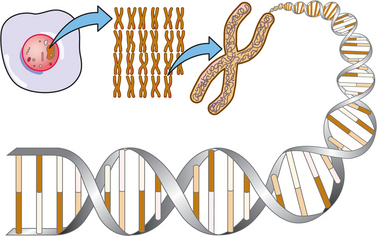
Figure 1-4 Schematic diagram of deoxyribonucleic acid (DNA). Inside the nucleus of nearly every cell in the body, a complex set of genetic instructions, known as the human genome, is contained on 23 pairs of chromosomes. Chromosomes are made of long chains of a chemical called DNA, packaged into short segments called genes. Every cell of every human body contains a copy of the same DNA. Genes contain instructions to direct all body functions written in a molecular language. This molecular language is made up of four letters; each letter represents a molecule on the DNA: adenine, cytosine, guanine, thymine. The As, Cs, Gs, and Ts form in triplets, constituting a code; each triplet of letters instructs the cell to attach to a particular amino acid (e.g., TGG attaches to amino acid tryptophan). Amino acids combined together form proteins. If the DNA language becomes garbled or a word is misspelled, the cell may make the wrong protein or too much or too little of the right one—mistakes that often result in disease.
DNA is composed of different combinations of molecules called nucleic acids. The sequence of nucleic acids provides instructions for assembling amino acids, which are the basic structural units of proteins (Fig. 1-5). A change in the normal DNA pattern of a particular gene is called a mutation. Some illnesses are caused by a tiny change in the DNA of just one gene, whereas others are caused by major changes in the DNA of multiple genes.
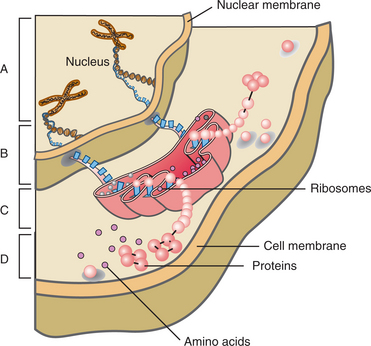
Figure 1-5 The chain of events from DNA; this is how the DNA directs the cell. A, Ribonucleic acid (RNA) receives instructions from the DNA code in the chromosomes. B, The RNA travels from the nucleus to link up with ribosomes (protein-making units). C, Instructions from the code contained within the DNA are used by the RNA-ribosome complex to assemble amino acids. D, Cellular function is now directed by proteins containing the amino acids.
Most illnesses, including most cases of cancer, are caused by acquired mutations. Acquired mutations arise during normal daily life, usually during the process of cell division. Each day the body replaces thousands of worn-out cells. Some genetic errors are inevitable as old cells replicate and pass DNA flaws along to replacement (daughter) cells. When all goes well, daughter cells recognize these mutations and repair them, but the repair mechanism can fail or be disabled by environmental toxins and diet. Although acquired mutations can be passed on to daughter cells, they cannot be inherited.
More specifically, gene therapy (also known as human genetic engineering) is the process in which specific malfunctioning cells are targeted and repaired or replaced with corrected genes (Fig. 1-6). A gene can be delivered to a cell using a carrier known as a “vector.” The most common types of vectors used in gene therapy are genetically altered viruses, but nonviral vectors are being developed as potential gene delivery vehicles as well. Essentially, DNA is used like a drug, allowing it to replace or repair defective genes. It is hoped that the altered cells will yield daughter cells with healthy genes; these offspring cells will help eliminate the diseased cells. Alternately, cells can be genetically altered to contain a toxin-producing suicide gene to treat some cancers.33
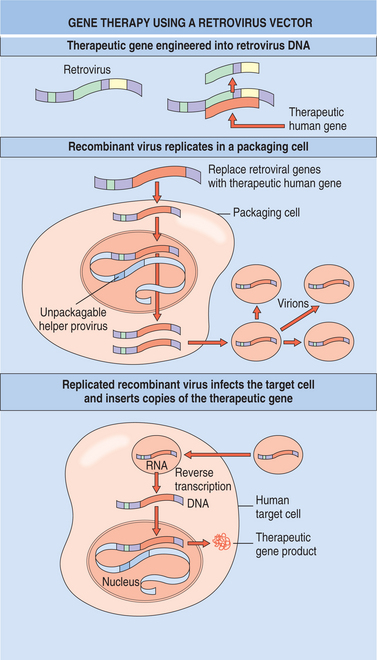
Figure 1-6 Gene therapy. A therapeutic gene is engineered genetically into the retrovirus DNA and replaces most of the viral DNA sequences. The recombinant virus that carries the therapeutic gene is allowed to replicate in a special “packaging cell,” which also contains normal virus that carries the genes required for viral replication. The replicated recombinant virus is allowed to infect the human diseased tissue, or “target cell.” The recombinant virus may invade the diseased tissue but cannot replicate or destroy the cell. The recombinant virus inserts copies of the normal therapeutic gene into the host genome and produces the normal protein product. (From Yanoff M, Duker JS: Ophthalmology, ed 2, St Louis, 2004, Mosby.)
Uses for Gene Therapy
Research is ongoing into such cures for a wide variety of hereditary disorders and diseases caused by aging (Box 1-2); some diseases, such as hemophilia, are being studied as a good model for gene therapy. Gene therapy for the treatment of diseases in children before birth is being actively pursued at many medical centers using animal models. In utero gene therapy (IUGT) could be beneficial for those with genetic diseases if gene therapy is performed before symptoms are manifested.39,52
Gene therapy is being investigated as a means of helping injuries heal, replacing worn-out tissue, reducing scar tissue, or fusing spinal segments together. The gene for bone growth has been injected into the disk space and shown to signal enough bone growth to bridge the bone on either side of the space. Investigational studies using animals may find an injectable method to fuse bone to replace the costly and complicated spinal fusion surgery.48
Gene insertion has been used to successfully treat humans with inoperable coronary artery disease. Researchers injected a gene that makes a protein called vascular endothelial growth factor (VEGF) into the hearts of candidates with severe chest pain caused by ischemia that could not be corrected with bypass surgery or angioplasty.
Tests suggest that once installed, the gene produces blood vessel–promoting proteins for 2 or 3 weeks (enough to grow a permanent new blood supply) before ceasing to work. The heart actually sprouts tiny new blood vessels (therapeutic angiogenesis) too small to be seen but with improved blood flow to the heart readily demonstrated.25,49 Investigations continue to examine gene therapy strategies to deliver genes coding for the angiogens.
Approaches to Gene Therapy
Gene therapy may take a number of different approaches. The original design was to inject one or more genes into the person to replace those that are absent or not functioning properly. A second approach called small-molecule therapy injects a small molecule (i.e., a drug) to modify the function of one or more genes in the body that is making a normal product but just too much or too little of it.
Other approaches include transferring a gene into cancer cells to sensitize them to drugs19 or restoring immune function in HIV by transferring a therapeutic gene into target cells, rendering them resistant to HIV replication. Infusion of protected cells may limit virus spread and delay AIDS disease progression. Efforts are underway to deliver antiviral genes to hematopoietic stem cells to ensure a renewable supply of HIV-protected cells for the life of the individual.11,12,32
Germ-line gene therapy is an approach that delivers genes to sperm or egg (or to the cells that produce them). It might prevent defective genes from being transmitted to subsequent generations by repairing the original genetic defect in germ cells. Gene modification at an early stage of embryonic development might also be a way of correcting gene defects in both the germ-line and body cells. This therapy is highly controversial because it carries an unknown level of risk (interference with another gene, specificity of the insertion). As a consequence, germ-line gene therapy is not being considered for application to humans at this time. In the future, if scientists determine ways to make sure that a transferred gene goes into the cell’s genome at the same position as the already mutated gene, then the safety of germ-line gene therapy procedures might be dramatically increased.
Obstacles to Gene Therapy
Some obstacles to gene therapy must be overcome before this procedure is considered a viable treatment option. Examples include finding appropriate harmless viral vectors to carry the normal gene to the target cells that do not provoke an immune response against them as foreign invaders or cause toxic side effects, engineering the transplanted genes to be efficient and effective, and finding ways to modify retrovirus vectors so they can carry the genes into nondividing cells (presently, genes can only be delivered to actively dividing cells when delivered by retrovirus vectors).
Ethical concerns have also been raised about the use of human genetic engineering for purposes other than therapy (e.g., eugenics). These include the use of genes to improve ourselves cosmetically, increase intelligence (a gene has been discovered that seems to make mice more intelligent), accomplish ethnic cleansing (“designer babies” genetically engineered before birth), or cause permanent changes in the gene pool. Some researchers are advocating the use of human genetic engineering for the treatment of serious diseases only.5
Gene Doping.: Gene therapy in sports athletes, called gene doping, involves transferring genes directly into human cells to blend with an athlete’s own DNA, enhancing muscle growth and increasing strength or endurance. Gene doping is banned in sports, and although there has been no direct evidence yet to prove it, there is some concern that gene doping has already begun.
Concerns have been raised about long-term effects such as leukemia, other forms of cancer, and unknown effects, including the potential harm in passing changes on to the athlete’s children. Although not currently in use, the potential for gene doping to enhance performance has been discussed in the literature.24,50
Gene Testing
The new and rapidly expanding field of genetic testing holds great promise for detecting many devastating illnesses long before their symptoms become apparent. Such testing identifies people who have inherited a faulty gene that may (or may not) lead to a particular disorder. In the last 15 years, such predictive tests have been developed for more than 200 of the 4000 diseases thought to be caused by inherited gene mutations. The result has been earlier monitoring, preventive treatments, and in some cases, planning for long-term care.
However, gene testing is not without its difficulties. For example, the presence of a particular mutation does not mean that illness is inevitable, making the interpretation of test results a highly complex task. The psychologic implications of predictive testing must be considered. Identifying who is a candidate for testing remains to be determined. Inheritance accounts for a limited number of diseases, suggesting that genetic testing should be reserved for people with a strong family history of a particular disease. Safeguards and protocols are not always in place before testing finds its way into general practice. For these reasons, it has been recommended that predictive testing should be confined to research or clinical settings where skilled counseling is available.
Other ethical issues and privacy concerns, such as the potential use of genetic testing to screen job applicants or to qualify for insurance coverage, must also be settled.
References
1. Arcari, CM. Association between Chlamydia pneumoniae and acute myocardial infarction in young men in the United States military. Clin Infect Dis. 2005;40(8):1123–1130.
2. Agaki, T. Gastric mucosa-associated lymphoid tissue lymphoma and Helicobacter pylori infection: evaluation of antibiotic treatment. Intern Med. 2000;39(4):273–274.
3. American College of Sports Medicine (ACSM). Position stand: exercise and physical activity for older adults. Med Sci Sports Exerc. 1998;30(6):992–1008.
4. American Physical Therapy Association (APTA). Guide to physical therapist practice, ed 2. Alexandria, VA: The Association, 2003.
5. Anderson, WF. Gene therapy: the best of times, the worst of times. Science. 2000;288(5466):627–629.
6. Balbin, EG, Ironson, GH, Solomon, GF. Stress and coping: the psychoneuroimmunology of HIV/AIDS. Baillieres Best Pract Res Clin Endocrinol Metab. 1999;13(4):615–633.
7. Baldwin, KM. Research in the exercise sciences: where do we go from here? J Appl Physiol. 2000;88(1):332–336.
8. Belhoussine-Idrissi, L. Helicobacter pylori infection: treatment. Curr Opin Gastroenterol. 2002;18(1):26–33.
9. Boissonnault, WG. Prevalence of comorbid conditions, surgeries, and medication use in a physical therapy outpatient population: a multicentered study. J Orthop Sports Phys Ther. 1999;29:506–525.
10. Bray, MS. Genomics, genes, and environmental interaction: the role of exercise. J Appl Physiol. 2000;88(2):788–792.
11. Bridges, SH, Sarver, N. Gene therapy and immune restoration for HIV disease. Lancet. 1995;345(8947):427–432.
12. Cairns, JS, Sarver, N. New viral vectors for HIV vaccine delivery. AIDS Res Hum Retroviruses. 1998;14(17):1501–1508.
13. Centers for Disease Control and Prevention (CDC). State specific prevalence of disability among adults. MMWR. 2000;49(31):711–714.
14. Coleman, C, Rountree, R. Immunotics. New York: G.P. Putnam’s Sons, 2000.
15. Davis, C.M. Getting from what is to what ought to be: Linda D. Crane Lecture. Combined Sections Meeting, San Diego, February 2005.
16. Dean, E. Preferred practice patterns in cardiopulmonary physical therapy: a guide to physiologic measures. Cardiopul Physical Ther. 1999;10(4):124–134.
17. Dossey, L. The extraordinary healing power of ordinary things. New York: Harmony Books, 2006.
18. Duncan, PW. Evidence-based practice: a new model for physical therapy. PT Magazine. 1996;12(12):44–48.
19. Evrard, A, et al. Enhancement of 5-fluorouracil cytotoxicity by human thymidine-phosphorylase expression in cancer cells: in vitro and in vivo study. Int J Cancer. 1999;80(3):465–470.
20. Feigenbaum, MS, Pollock, ML. Prescription of resistance training for health and disease. Med Sci Sports Exerc. 1999;31(1):38–45.
21. Finger, ME. Identification of intervention categories for physical therapy, based on the International Classification of Functioning, Disability, and Health: a Delphi exercise. Phys Ther. 2006;86(9):1203–1220.
22. Gahimer, J. Health promotion for the physical therapist: concepts, theory, evidence, and application. Annual APTA Conference, Boston, June 2005.
23. Greer, S. Mind-body research in psychooncology. Adv Mind Body Med. 1999;15(4):236–244.
24. Haisma, H.J. Gene doping: a report from the Netherlands Centre for Doping Affairs. Available on-line at http://www.genedoping.com. Accessed April 10, 2007.
25. Hamawy, AH, et al. Cardiac angiogenesis and gene therapy: a strategy for myocardial revascularization. Curr Opin Cardiol. 1999;14(6):515–522.
26. Hankey, A. Are we close to a theory of energy medicine? J Altern Complement Med. 2004;10(1):83–86.
27. Jensen, GM, et al. Expert practice in physical therapy. Phys Ther. 2000;80(1):28–44.
28. Jette, AM. The changing language of disablement (editorial). Phys Ther. 2005;85(2):118–119.
29. Jette, AM. Toward a common language for function, disability, and health. Phys Ther. 2006;86(5):726–734.
30. Jonas, W, Crawford, C. Science and spiritual healing: a critical review of spiritual healing, “energy” medicine, and intentionality. J Altern Complement Med. 2003;9(2):48–55.
31. Lezak, M. Neuropsychological assessment. New York: Oxford University Press, 1983.
32. Li, M. RNAi in combination with a ribozyme and TAR decoy for treatment of HIV infection in hematopoietic cell gene therapy. Ann NY Acad Sci. 2006;1082:172–179.
33. Link, CJ, et al. Cellular suicide therapy of malignant disease. Oncologist. 2000;5(1):68–74.
34. Lochhead, P. Helicobacter pylori infection and gastric cancer. Best Pract Res Clin Gastroenterol. 2007;21(2):281–297.
35. Maas, M, et al. Detection of chlamydia pneumoniae within peripheral blood monocytes of patients with unstable angina or myocardial infarction. J Infect Dis. 2000;181(suppl 3):S449–451.
36. Mosby’s dictionary of medicine, nursing & health professions. ed 7. St. Louis: Mosby; 2006.
37. Muhlestein, JB. Chronic infection and coronary artery disease. Med Clin North Am. 2000;84(1):123–148.
38. Nabel, GJ. Genetic, cellular and immune approaches to disease therapy: past and future. Nat Med. 2004;10(2):135–141.
39. Nagi, SZ. Disability and rehabilitation. Columbus, OH: Ohio State University Press, 1969.
40. National Human Genome Research Institute All about the human genome project, 2007. Available at http://www.genome.gov/HGP/ Accessed April 11, 2007.
41. Pesonen, E. Dual role of infections as risk factors for coronary heart disease. Atherosclerosis. 2006. [[Epub ahead of print.]].
42. Pert, C. Molecules of emotion: the science behind mind-body medicine. New York: Touchstone (Simon and Schuster), 1998.
43. Pert, C. Paradigms from neuroscience: when shift happens. Mol Interv. 2003;3(7):361–366.
44. Pert, C. The wisdom of the receptors: neuropeptides, the emotions, and bodymind. Adv Mind Body Med. 2002;18(1):30–35.
45. Pert, C, Marriott, N. Everything you need to know to feel good. New York: Hay House, 2006.
46. Petry, JJ. The role of the mind and emotions of patient and surgeon in the outcome of surgery. Plast Reconstr Surg. 2000;105(7):2636–2637.
47. Poirot, L. Genetic disorders and engineering: implications for physical therapists. PT Magazine. 2005;13(2):54–60.
48. Riew, KD. Thoracoscopic intradiscal spine fusion using a minimally invasive gene-therapy technique. J Bone Joint Surg. 2003;85A(5):866–872.
49. Rosengart, TK, Patel, SR, Crystal, RG. Therapeutic angiogenesis: protein and gene therapy delivery strategies. J Cardiovasc Risk. 1999;6(1):29–40.
50. Trent, RJ, Alexander, IE. Gene therapy in sport. Br J Sports Med. 2006;40(1):4–5.
51. Vilaichone, RK. Helicobacter pylori diagnosis and management. Gastroenterol Clin North Am. 2006;35(2):229–247.
52. Waddington, SN. In utero gene therapy: current challenges and perspectives. Mol Ther. 2005;11(5):661–676.
53. Woltersdorf, MA. Beyond the sensorimotor strip. Clin Management. 1992;12:63–69.
54. World Health Organization (WHO). Constitution of the World Health Organization. In Chronicle of the World Health Organization. Geneva: WHO; 1947.
55. World Health Organization (WHO). Global burden of disease and injury report. Geneva: WHO, 2007.
56. World Health Organization (WHO) International classification of functioning, disability, and health (ICF), 2001. Available at http://www.who.int/classifications/icf/en/ Accessed April 10, 2007.
57. World Health Organization (WHO). International classification of impairments, disabilities, and handicaps: a manual of classification relating to the consequences of disease. Geneva: WHO, 1990.
58. World Health Organization (WHO) New guidelines to measure health (press release), 2001. Available at http://www.who.int/inf-pr-2001/en/pr2001-48.html Accessed April 10, 2007.
59. Zanjani, ED, Anderson, WF. Prospects for in utero human gene therapy. Science. 1999;285(5436):2084–2088.