Behavioral, Social, and Environmental Factors Contributing to Disease and Dysfunction
OVERVIEW
The biomedical model of health care has governed the thinking of most health practitioners for the past three centuries holding to the premise that all illness can be explained based on disorder and disease of bodily anatomy and physiologic processes. This model assumes that psychologic, social, and spiritual influences are independent of the disease process.
By contrast, the biopsychosocial model of health and illness supports the idea that biologic, psychologic, and social variables are key factors in health and illness. The mind and body cannot be separated since they both influence the state of health. The biopsychosocial model emphasizes health and illness, rather than considering illness as a deviation of the healthy state.
During the 1980s, the medical model was influenced by a movement toward what was then called holistic health, the notion that the physical, mental, social, and spiritual aspects of a person’s life must be viewed as an integrated whole. Since that time, it has become well established that social support plays a key role in promoting health, decreasing susceptibility to disease, and facilitating recovery from illness or injury.
During the 1990s, basic scientists and clinicians continued to recognize the healing potential of faith, spirituality, and religious beliefs and started to consider the complex biopsychosocial-spiritual phenomena associated with disease, illness, and injury. Multidisciplinary team and managed care approaches to such conditions address the needs of the client in terms of the emotional and psychologic impact, social and spiritual needs, and comprehensive biologic picture that goes beyond medication and surgical intervention as the primary forms of medical treatment.
Behavioral, Social, and Environmental Factors
Aside from the pathology itself, many behavioral, social, and environmental factors influence health and may mitigate or enhance the effects of disease. The impact of these factors on the disease process or the consequences of disease will be a major focus of this chapter. The influence of selected behavioral, social support, and environmental factors on health will be reviewed separately with models or theories described that integrate these components in defining and characterizing health.
Traditionally, physical therapists have approached rehabilitation from a medical model mediated through the mechanism of physiologic impairments. The medical model generally considers the underlying assumptions that pathology should be treated or cured and that pathology leads directly to consequences, including impairment, limitations in physical function, and diminished quality of life. The medical model is then logically focused on eliminating pathology or the resulting impairments, which would then lead to improved function.
Although this model is important for understanding medical care, it does not address the other factors that influence a person’s physical or mental health. The medical model focuses on factors internal to the individual that directly affect an individual’s health status; however, considerable information now indicates that factors external to an individual also play a significant role in a person’s health status.
During the last two decades of the twentieth century, health care professionals developed a better understanding of the importance of behavioral and social issues and how unhealthy behaviors are linked to many conditions and diseases. This shift in emphasis encourages the development of new treatments or interventions that impact an individual’s health. The Centers for Disease Control and Prevention (CDC) has responded to a growing awareness of these changes and established three new internal units to deal with them directly: (1) the National Center for Chronic Disease Prevention and Health Promotion; (2) The National Center for Injury Prevention and Control; and (3) the National Center for HIV, STD, and TB Prevention. The task of these groups is to focus on conditions, diseases, and injuries with clear behavioral risks.123
Other areas of behavioral and social research have focused on social forces affecting the environment that could impact health and the influence of class, family structure, and ethnicity on health and illness.125 In keeping with these changes in the direction of behavioral and social sciences in public health, the intent of this chapter is to increase the physical therapists’ understanding of behavioral, social, and environmental issues in addition to the pathology that can affect health and physical function.
Much work has been done to develop methods to classify the effects of disease on health at all levels. Using the concepts of health and disease presented in Chapter 1, we recognize that the consequences of disease include effects on tissues (pathology), on organs or organ systems, (impairments), and on the person’s ability to function in daily life (disability, activity limitations) and function in society (handicap, participation restrictions). These categories should be useful to rehabilitation specialists as well, who look to mitigate (i.e., reduce the impact of) the effects of disease by focusing on improving physical function and/or performance of daily activities. In addition, this viewpoint reminds us that the adverse effects of pathology may be mediated by other social and environmental factors.
CLINICAL MODELS OF HEALTH
The principles presented in Chapter 1 regarding disablement or enablement models may also be used in clinical practice. The clinical practice perspectives may be characterized by a broad approach to health. From a biopsychosocial point of view, models of health can be narrowed down to the following three main approaches:
• Biomedical model focuses on the disease process.
• Biopsychosocial model describes the role of biological, psychological, and social factors on a person’s health.
• Social-ecologic model describes multiple levels of interaction that influence health.
Biomedical Model
From our discussion in Chapter 1, we know the traditional biomedical model is based on the premise that health is primarily influenced by the person’s biologic state, or whether there is an abnormality at the cellular (pathology) or organ system level (impairments). In this model, in order to improve health, one must cure or treat the underlying disease process.
Biopsychosocial Model
The biopsychosocial model combines knowledge from the disciplines of behavioral medicine, behavioral health, and health psychology.254 In this model, a person’s psychologic system, including aspects of cognition, emotion, and motivation, interacts with biologic factors to produce various states of health. Likewise, how an individual interacts with family, community, and society also influences health outcomes.
Compared to the biomedical model, the benefit of this approach is that it includes factors other than physical condition that influence health. The negative effect of this approach is to place blame on the individual for his or her health status, while neglecting the influence of social or environmental factors on the individual.
Social-Ecologic Model
From the field of social community health and health promotion, the social-ecologic model was developed on a broader view of health issues. Social ecology is viewed as an overarching framework or a set of theoretic principles for understanding the interrelations among diverse personal and environmental factors in human health and illness.274 Social-ecologic theory, an extension of the biologic concept of ecology, creates a framework in which to place and discuss health at a level beyond the individual.
Four primary assumptions regarding social-ecologic theory have been outlined.235,236 First, intrapersonal, social, and physical environments work jointly to influence health behavior. Second, environmental influences on health are the result not only of physical and social components but also the perception of these variables by the individual. Recognition of various collective levels of human interaction with the environment (e.g., individual-environment, community-environment, or population-environment) comprises the third assumption.
The fourth and critical assumption of social-ecologic theory is the relationship between environmental levels and collections of individuals. In short, altering behaviors among individuals will influence environmental level characteristics, which will in turn further influence groups of individuals within a community or population.
Various models of social ecology have been described and applied in intervention programs. The most common construction of social ecology, provided by Sallis and Owen,219 proposes that behaviors are influenced by intrapersonal, sociocultural, policy, and physical-environmental factors.
Bronfenbrenner’s35 model describes three levels of environmental-individual interaction, the microsystem (i.e., interpersonal interactions), the mesosystem (i.e., interactions among various settings such as work, family, and social networks), and the exosystem (i.e., cultural, political, and economic forces).
The model proposed by McLeroy et al in 1988168 is composed of five classes of factors: intrapersonal factors, interpersonal processes and primary groups, institutional factors, community factors, and public policy. Behavior is the outcome of interest and is determined by the five classes, with four of the five pertaining to the person’s environment and clearly beyond the intrapersonal. Moos’176 ecologic model is geared toward health behavior and constructed of physical settings, organizational factors, human aggregates, and social climate.
The important point in recognizing the diversity of the models used to describe social-ecologic theory is to observe the common threads that run between them. Each reflects the interrelationship between individual level characteristics and large-scale social forces (Fig. 2-1). Increasingly larger social structures influence the indi- vidual and can shape behavior, including the ability to make health decisions such as compliance with regimens or even initial health choices.
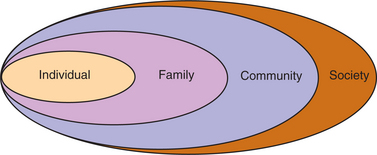
Figure 2-1 Social structures influencing the individual. Aside from the pathology itself, many behavioral, social, and environmental factors influence health and may mitigate or enhance the effects of disease. The individual is influenced in various ways by family, community, and society. Each of these nested social structures influences the individual and can shape behavior, including the ability to make health decisions, compliance with regimens, or even with initial health choices. (Courtesy Ira Gorman, PT, MSPH, Regis University, Department of Physical Therapy, Denver, CO.)
This model attempts to identify the various levels of influence that have an impact on health, from the individual to the environment. This view greatly broadens the types of interventions that can improve health and helps us understand the role pathologic processes have at the cellular level as they interact with the environment to cause disease, impairment, functional limitations, and disability.
VARIATIONS IN CLIENT POPULATIONS
Healthy People 2010110 recognizes the need for all Americans to benefit from advancements in quality of life and health, regardless of race, ethnicity, gender, geographic location, disability status, income, sexual or spiritual orientation, or educational level. Recognizing variations in client populations is important in helping all health care professionals to provide health-promoting and preventive programs.
Sociodemographics
Sociodemographic information and the results of the 2000 census have provided us with a composite picture of America never before so broad based or so complete. Americans are more diverse ethnically, with an estimated ethnic racial mix of 72% white, 12% African American, 12% Hispanic, and 4% Asian and Pacific Islander. By the year 2020 the number of people of Asian descent will double from 10 million to 20 million, and by 2050, whites will comprise only 53% of the U.S. population.
Rapid population shifts to the mountain states and resurgent growth in suburbs have changed the urban/rural configurations. More than 70% of all rural counties gained population in the last decade.
Finally, the percentage of Americans who are married continues to drop—most recently from 58.1% of those age 15 and older in 1992 to 56.4% in 1998.250 Since the census was completed, new reports indicate that the percentage of single heads of households (52%) has now surpassed married households.
Health Status
The health status of the United States is a description of the health of the total population using information that is representative of most people living in this country. However, it must be noted that our current epidemiologic system does not keep data on people who do not obtain treatment; no universal or uniform registry is available in the United States.
Health status of a nation can be measured by birth and death rates, life expectancy, quality of life, morbidity from specific diseases, risk factors, the use of ambulatory care and inpatient care, accessibility of health personnel and facilities, financing of health care, health insurance coverage, and many other factors.
The leading causes of death are often used to describe the health status of a nation. For example, in the United States, obesity, alcoholism, sedentary lifestyle, and tobacco use have contributed significantly to the most common causes of morbidity and mortality in 2000, compared with the year 1900, when infectious diseases ran rampant in the United States and worldwide and topped the leading causes of death. In the year 2000, 65% of all deaths were caused by cardiovascular disease, cancer, and diabetes.172
Deaths, permanent disability, and unnecessary suffering from medical errors are an escalating problem that remains largely unreported. According to the Institute of Medicine (IOM),241 medical errors kill over 44,000 people in U.S. hospitals each year. Statistics are not available for similar errors in other health-related settings such as same-day surgery centers, outpatient clinics, retail pharmacies, nursing homes, and in-home care. Deaths from medication errors that occur both in and out of hospitals (more than 7000 annually) exceed those caused by injuries in the workplace.
Chronic Diseases
Over the last century, a shift from infectious to chronic diseases has occurred. As a result of the control of many infectious agents, eradication of childhood diseases, and the current increasing age of the population, chronic diseases now top the list as causes of morbidity and mortality in the United States (Table 2-1). Many of these illnesses are modifiable through changes in behavior and lifestyle. This trend has led to a new focus in rehabilitation: chronic disease management. In some places, chronic disease management is a new term for rehabilitation.
Table 2-1
Leading Causes of Death in the United States*
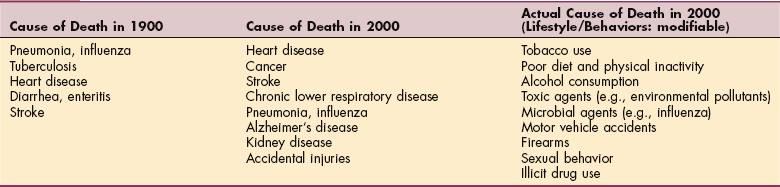
*Listed in descending order of incidence.
Data from Mokdad AH: Actual causes of death in the United States, 2000, JAMA 291(10):1238-1245, 2004.
Cost of health care delivery has increased exponentially with the rise in aging, risky lifestyle behaviors, and associated medical conditions. Chronic conditions, such as heart disease, hypertension, diabetes, and mental disorders, are costing billions of dollars—more than even 20 years ago. Up to half of Medicare patients aged 65 and older have at least three chronic medical conditions, and one-fifth has five or more.245
Medical spending has increased as more people are suffering from chronic disorders with multiple complex comorbidities. In addition, some conditions have become more expensive to treat, and the number of people diagnosed with these conditions has increased.245
With modifiable behavioral risk factors as leading causes of mortality in the United States, identifying trends and gearing prevention strategies and opportunities toward these specific behaviors may help offset escalating health care costs.173
Despite all the evidence supporting the medical and economic benefits of prevention and early detection, current disease control efforts are underfunded and fragmented. While health care costs are skyrocketing, the national investment in prevention is estimated at less than 3% of the total annual health care expenditures.48
Americans with Disabilities
There were 49.7 million Americans reported in the 2000 U.S. Census with some disability. This number increased by the mid-2000s to over 54 million. Rates of disability are higher among older adults who also have higher rates of chronic diseases.
Almost half of all seniors (over age 65) have a physical, sensory, mental, or learning disability of some kind. There is a wide range of definitions for disability used in social research situations. In some cases, disability is any difficulty with activities of daily living or limitations associated with over 30 associated health conditions.169 Other definitions include those receiving federal benefits on the basis of an inability to work or those with any limitation in the ability to work at a job or business, yet over half (56%) of working-age individuals with a disability are employed.248
Until the census in 2000, the number of American veterans was declining. With the American involvement in the Middle East in the new century, 2010 census figures may show an increase in these statistics. Therapists may expect to see a greater number of combat-related disabilities among men and women in the military, as well as in the civilian sector once they are discharged.
With increasing life expectancy and the aging of America, health issues related to disability are likely to increase in prevalence and importance over the next few decades. Living longer means increasing percentages of individuals with disabilities.169
Geographic Variations
The concept of “community” as it relates to where individuals live geographically and the characteristics of that place has a definite impact on the status of people’s health. For example, based on statistics pertaining to crime, divorce, population density, unemployment, and average commuting time, the most stressful cities and jobs have been identified, as well as the least stressful locations and occupations.54
Other factors, such as urban pockets of minority groups (usually associated with increased levels of poverty), access to fresh fruits and vegetables (or lack thereof), and even local smoking ordinances, contribute to the geographic variations people experience that can impact their health.201
The geographic and political climates of countries also play a role in determining how people live and the health problems that commonly develop. A half-century ago, a few physicians cultivated an interest in diseases that seemed to have strict geographic boundaries. As a result, a discipline called geographic pathology developed. Geographic pathology was concerned with diseases endemic (present in a community at all times) to certain areas of the world, most often parasitic and infectious diseases that seemed unique to individual geographic regions. A component called occupational disease was added with the discovery that chemical agents are mediators of a variety of tissue changes and the recognition that many of these causative agents are environmental contaminants. Disease caused by contaminants was included to constitute the field of environmental pathology. For further discussion, see Chapter 4.
One other issue related to geographic variations is the fact that treatment for a single medical condition can vary significantly from one geographic location to another. Rates and types of surgical procedures differ from one geographic location to another, depending on the prevailing health care system, physician and hospital preferences (not client preferences or needs), and where the physician was trained.30,195
Race and Ethnicity
The use of the terms “race” and “ethnicity” are seldom well defined and are generally thought to have less scientific and biologic significance than sociologic and cultural importance. The CDC defines race as “an arbitrary classification based on physical characteristics; a group of persons related by common descent or heredity.” The CDC defines ethnicity as “an arbitrary classification based on cultural, religious, or linguistic traditions; ethnic traits, background, allegiance, or association.”183
Identification of race and ethnicity is widely used when collecting vital statistics and demographic data for documenting health patterns among population groups living in the United States and globally. The National Health and Nutrition Examination Survey (NHANES) I, II, and III (developed in 1959, the 1970s, and the 1980s, respectively) used race and ethnicity data when evaluating the health and nutrition status of the civilian, noninstitutionalized population of the United States. This survey is updated annually.188
The Hispanic HANES (HHANES) was conducted to obtain sufficient numbers to produce estimates of the health and nutritional status of Hispanics in general, as well as specific data for Puerto Ricans, Mexican Americans, and Cuban Americans. Included in the survey were Mexican Americans from Texas, Colorado, New Mexico, Arizona, and California; Cuban Americans from Dade County, Florida; and Puerto Ricans from the New York area, including parts of New Jersey and Connecticut.63,187
In planning for the U.S. Census 2000, the Office of Management and Budget (OMB) revised the Race and Ethnic Standards for Federal Statistics and Administrative Reporting. The revised standards include five minimum categories for data on race: American Indian or Alaska Native, Asian, Black or African American, Native Hawaiian or other Pacific Islander, and White. There are two categories for data on ethnicity: “Hispanic or Latino” and “Not Hispanic or Latino.”196
The CDC has developed unique identifiers for race and ethnicity. The CDC data collection and reporting system is standardized and includes data elements that describe a unique identifier code set for race and ethnicity information and provides guidance for recording and exchanging this type of information. The unique identifier code set combines current federal standards for classifying data based on minimum race and ethnicity categories as defined by the OMB and a more detailed set of race and ethnicity categories from the U.S. Bureau of Census.184
In the past, it was believed that race or ethnic background predisposed people to certain diseases and chronic conditions. However, during the last 50 years, “race” has been scientifically disproved—that is, race is not a real, natural phenomenon. Data on human variation come from studies of genetic variation, which are clearly quantifiable and replicable. Genetic data show that no matter how racial groups are defined, two people from the same racial group are as different as two people from any two different racial groups.
Current information about biologic and genetic characteristics of various groups (e.g., blacks, Hispanics, Native Americans, Alaskan Natives, Native Hawaiians, or Pacific Islanders) does not explain the health disparities experienced by these groups. These differences are believed to be the result of the complex interaction among genetic variations, environmental factors, and specific sociocultural and health behaviors.
Data indicate that some conditions are more prevalent in certain groups; for example, nonwhite people (black, Native Americans, and Asians) are three times more likely to die of hypertension than whites of the same age group. In the past, causes of death were identified that together accounted for more than 80% of mortality in nonwhite people, including cancer; cardiovascular disease and stroke; chemical dependency; cirrhoses; diabetes; homicides, suicides, and accidents; and infant mortality.83
Other conditions that are peculiar to ethnic or racial groups include Tay-Sachs disease (Jewish people of northeastern European origin are most susceptible); cystic fibrosis (incidence is highest in whites and rare in Asians); and sickle cell anemia, which affects blacks, especially Africans.
Health Disparities
Although it is a well-known fact that over the last 100 hundred years health care has dramatically improved the lifespan and the quality of life for many through advances in public health, medical discoveries, and technology, it is less known that not every segment of the population has benefited equally from the advances in health care.
Social factors, such as socioeconomic status, access to health care, language differences, place of birth, residential segregation, and access to nutrition, have all been variables that help explain the disparities in health care that result in higher morbidity and mortality rates among groups of Americans. For example, statistics show a broad gap between the death rates for blacks and whites, but blacks differ more from each other than they do from whites.75 Whites living in higher socioeconomic areas have lower mortality rates than whites living in predominantly black areas for all age groups, and elderly blacks living in black areas (despite their less favorable socioeconomic status) have lower mortality rates for all causes than those living in white areas.76
Although cancer death rates are declining nationally, ethnic groups and medically underserved populations have a higher incidence and lower survival rate. Racial differences in the surgical treatment of blacks as compared with whites have been documented.13
Available education and health care resources are not accessible to minorities and rural residents with limited financial means. Routine programs, such as antismoking campaigns and cancer screenings (e.g., breast, prostate, or colon), tend to be focused on affluent Americans who are better educated and can afford regular medical care.68 The general understanding regarding health care was that those who could afford health care had access to health care and those who could not afford health care did not have access to health care. Thus there was disparity in health care related to access based on socioeconomic factors.
In the 1990s, it became apparent that despite the improved access to health care through the national Medicare health system, there were persistent health disparities. In 1999 the U.S. Congress mandated the IOM to conduct a study to assess differences in the kinds and quality of health care received by U.S. racial and ethnic minorities and nonminorities. The IOM was charged to assess the extent of racial and ethnic differences in health care not otherwise attributable to known factors such as access to care (ability to pay for insurance coverage). The IOM was to evaluate potential sources of racial and ethnic disparities in health care, including the role of bias, discrimination, and stereotyping at the individual (patient and provider), institutional, and health systems level. The IOM was also charged to provide recommendations regarding interventions to eliminate health care disparities.
The IOM committee reviewed over 100 studies that assessed the quality of health care for various racial and ethnic minority groups. The research studies reviewed controlled for variations in insurance status, patient income, and other access-related factors.231
Racial and ethnic disparities remain even after adjustment for socioeconomic differences and other health care access–related factors. According to the IOM report,231 there is a difference in the quality of health care provided to racial and ethnic minorities even when there is equal access to health care.
The IOM report findings indicate “despite steady improvement in the overall health of the U.S. population, racial and ethnic minorities, with few exceptions, experience higher rates of morbidity and mortality than non-minorities.”231 Minorities are less likely than whites to receive needed health services, including clinically necessary procedures.
Racial and ethnic health disparities exist in different disease conditions such cardiovascular disease, cancer, human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS), mental illness, and diabetes. Racial and ethnic minorities are less likely than whites to receive angioplasty, coronary artery bypass graft surgery, mammography, and hip fracture repair.
African Americans are 2.5 times more likely than whites to have radical surgeries, such as bilateral orchiectomy as a result of cancer and limb amputation secondary to peripheral vascular disease, when compared to other racial groups with similar medical conditions. Disparities are found across a range of clinical settings, including public and private hospitals and teaching and nonteaching medical centers. Health disparities result in higher morbidity and mortality rates among minorities.
Disparities in Rehabilitation Services
Specific to health care practices in rehabilitative services, three research studies reviewed by the IOM identified the following information on health disparities:
• Harada, Chun, Chui, et al105 assessed sociodemographic and clinical characteristics associated with the use of physical therapy in acute hospitals, skilled nursing facilities, or both. The records of 187,900 hip fracture patients were reviewed. African-American patients were less likely than whites to receive acute physical therapy, were less likely than whites to receive physical therapy in both acute care and skilled nursing facilities, and were more likely to receive no physical therapy at all.231
• Horner, Hoenig, Sloane, et al124 assessed racial differences in the utilization of inpatient rehabilitation services among elderly stroke patients. The records of 2497 African-American and white Medicare patients hospitalized after stroke at any of 297 acute care hospitals in five states were reviewed. After adjusting for clinical and socioeconomic factors associated with the use of physical and occupational therapy, no racial differences were found in the likelihood of use of therapy or time to initiate therapy. No differences were found in length of physical or occupational therapy in days or as a proportion of hospital stay.231
• Hoenig, Rubenstein, and Kahn120 assessed racial and other sociodemographic and geographic differences in use of physical and occupational therapy in elderly Medicare patients with acute hip fracture. The records of 2762 African-American and white Medicare patients treated in 297 randomly selected hospitals from five states were reviewed. After controlling for clinical factors, African-American patients and dual eligible Medicare/Medicaid patients were less likely to receive high-intensity physical or occupational therapy. No racial differences were found in time to initiate therapy.231
The first National Healthcare Disparities Report (NHDR) issued by the Agency for Healthcare Research and Quality (AHRQ) in 2003 reported: “There are clear disparities in lifespan, health status, and health care use among different racial, ethnic, socioeconomic, and geographical groups. These individuals suffer a disproportionate burden of illness and disability from preventable or treatable chronic conditions.”190
Factors Contributing to Health Disparities
The IOM report identified several factors that contribute to health disparities. First, health systems have financial expectations that influence health care practice. For example, increased productivity demands utilize scheduling practices that often limit health practitioner contact with clients and require health care practitioners to engage in multiple duties at the same time. Health systems also provide financial incentives to physicians for limiting services including diagnostic procedures and interventions.
Second, the organizational structure of health care delivery can contribute to health disparities. Care may be provided by health care professionals, such as nurse practitioners, physician assistants, and physicians in training, who may not be qualified to address the individual’s needs. According to one study, African Americans who do not receive health care from a physician are more likely to feel distrustful.103 More research is needed to compare level of trust with degree of compliance when given advice and recommendations by the health care professional.
Third, clients are not always followed by the same health care provider, and inconsistencies exist when one health practitioner orders certain tests and procedures for a medical work-up while another practitioner does not. There is evidence of this type of fragmentation of health care along socioeconomic lines. Clients in lower socioeconomic groups are less likely to receive a complete array of medical tests routinely ordered for individuals with a higher socioeconomic status.
Other factors contributing to racial and ethnic health disparities include cultural and linguistic barriers, discrimination, bias, stereotyping, and uncertainty on the part of the health practitioner. Despite best intentions to avoid such practices, health practitioners engage in stereotyping and bias that may be conscious or unconscious. The health care provider may experience uncertainty in the clinical encounter and rely on a previous experience as the basis for the clinical decision making. The bias, stereotyping, and uncertainty may be the result of cultural differences and linguistic issues and affect the clinical management and health outcomes.
Strategies to Eliminate Disparities
Every effort must be made to eliminate racial and ethnic disparities in health care. The IOM has recommended the following strategies to eliminate or reduce health disparities:
• Education to address discrimination, bias, stereotyping, and uncertainty that contribute to health disparity; engage health practitioners in reflective practice that can alter conscious and unconscious behavior.
• Cross-cultural education provided to current and future health care practitioners to develop attitudes, knowledge, and skills in working with diverse populations.
• Standardize data collection to include race and ethnicity data for both the client and the provider, primary language data, socioeconomic data, and monitoring of performance outcomes.
The health of individuals within the society directly influences the health of the nation in the collective. Citizens contribute to the culture and the society to create the fabric of national life. Thus the health of the citizens of the nation is of paramount importance and is being addressed through a variety of federal and nonfederal initiatives (Box 2-1).
Beyond Cultural Competence: Transnational Competence
Understanding of cultural diversity and cultural competence has become a familiar topic in the physical therapist’s education. Likewise, some consideration of these topics has become a part of all U.S. medical schools. Cultural competence has been linked with quality assurance and cost-containment programs to help reduce disparities in health care.142 A new goal is to prepare students for multiple (international) practice sites.142
Given rapidly changing global demographics and the continued health disparities, social scientists propose a need to move beyond cultural competence to embrace transnational competence (TC). TC teaches the health care professional how to address issues of physical and mental health along with experiences related to geographic dislocation and adaptation to unfamiliar settings.142
Demographic patterns are changing rapidly in the United States. Disparities in health and health care are increasing. More than 35 million foreign-born persons are living in the United States—more than 12% of the total population. Currently, 6 out of every 10 babies born in New York City have at least one foreign-born parent.29
It is not enough to consider lists of ethnocultural characteristics and single-factor explanations such as health-belief systems. Relevant links between health and postmigration stressors may include employment status and experiences, discrimination, insecurity of immigration status, or family fragmentation.141 TC requires a multidimensional approach that takes into account our current era of globalization and migration and their impact on health beliefs, disparities, and diversity within ethnic groups.
Age and Aging
Age and gender play important roles in the development of most diseases. Age often represents the accumulated effects of genetic and environmental factors over time. Intrinsic cellular mechanisms play a role in aging, though these can be modulated by extracellular factors such as hormones. Discriminating between causes and effects of aging is often impossible. Separating aging from pathology remains a major challenge in our understanding of these two concepts.
There are many theories to explain what changes occur that lead to aging, but no universal theory of aging or consensus over what causes aging or determines the rate of aging exists. Theories of aging that have gathered more experimental support than others are presented here.
Theories of Aging
Senescence, the process or condition of growing old, may be the result of continuous cellular metabolism, cellular damage, and inefficient repair systems throughout the entire lifespan. Some researchers in gerontology (specifically biogerontologists) regard aging itself as a “disease” that may be curable. Understanding aging from this framework is referred to as a damage-based theory. Error theory, the wear and tear theory, the free radical theory, the neuroendocrine theory, and the waste accumulation theory are examples of damage-based explanations of aging. To those who accept the damage-based view, aging is an accumulation of damage to macromolecules, cells, tissues and organs.
Examples of environmentally induced damage range from alterations to deoxyribonucleic acid (DNA), formation of free radicals from oxidative processes causing damage to tissues and cells, and increased cross-linking of tendon, bone, and muscle tissue reducing tissue elasticity and obstructing the passage of nutrients and waste between cells. These concepts are discussed in greater detail in Chapter 6.
An alternate explanation for the aging process is programmed-based, which presumes that aging is a genetically driven process and not primarily the result of ongoing and accumulated cellular or environmental processes. In other words, aging is regulated by a biologic clock. Changes in gene expression are either preprogrammed or derived from DNA structural changes and affect the systems responsible for maintenance, repair, and defenses.39 Examples of the programmed-based explanation of aging include the gene mutation theory, the genetic control theory, and the planned obsolescence theory. Both damage-based and programmed-based theories acknowledge that aging is influenced to some degree by intrinsic and extrinsic factors. It is also possible that elements of both theoretic models apply.
A newer theory in the field of antiaging medicine is the telomerase theory of aging. The basis of this theory is the shortening of telomeres in the process of DNA replication during cell division. Telomeres are sequences of nucleic acids extending from the ends of chromosomes. Telomeres act to maintain the integrity of our chromosomes. Every time our cells divide, telomeres are shortened, leading to cellular damage and cellular death associated with aging.
Researchers also found that the enzyme telomerase is a key factor in rebuilding the disappearing telomeres. Telomerase is found only in germ cells and cancer cells. Telomerase may be manipulating the biologic clock that controls the lifespan of dividing cells. Future development of telomerase inhibitor may be able to stop cancer cells from dividing. The hope is to convert them back into normal cells.
Life Expectancy
Life expectancy at birth is now about 80 years for women and 75 years for men, compared with 48 years at the turn of the last century.186 Until recently, these estimates were expected to continue increasing for both genders. But some researchers predict a decline in U.S. life expectancy later this century based on the dramatic rise in obesity, especially among young people and minorities.198
Whites and blacks have similar life expectancies at age 65, but a higher death rate exists among younger blacks. Once adults reach age 65, men can expect to live an additional 15.8 years, and women can expect an additional 17.6 years. Individuals 75 years of age can be expected to live an average of 11 more years for a total of 86 years.249
The majority of cancers occur in adults over the age of 65, with about 70% of all cancer deaths in this population. For many cancers, a person’s advanced chronologic age is considered a major adverse prognostic factor. Many older adults tolerate cancer treatment, but they experience delayed recovery and are at increased risk of serious infectious and bleeding complications.278
Centenarians
A dramatic extension of longevity has occurred in the last 100 years. In 1900, people over age 65 constituted 4% of the U.S. population. By 1988, that proportion was up to 12.4%, and it is predicted that by 2025, one-third of all Americans will be age 65 or older, and 30% of the over-65 population will be nonwhite by 2050, representing an even greater cultural diversity among the aging.12
The most rapid population increase over the next decade will be among those over age 85 and the “oldest old” over 100 years of age (centenarians). This aging trend of the U.S. population is reflected in the kinds of clients and problems therapists will treat in the coming decades. Confusion; fractures and other injuries related to falls; strokes; infections; and effects of polypharmacy, inappropriate medications, and decline in drug clearance are just a few of the more common characteristic problems this group of older adults faces.
Finally, the older adult can be assessed for modifiable risk factors that contribute to functional decline. Slow gait, short-acting benzodiazepine use, depression, low exercise level, and obesity are significant modifiable predictors of functional decline in both vigorous and basic activities. Weak grip predicts functional decline in vigorous activities, whereas long-acting benzodiazepine use and poor visual acuity predict decline in basic activities. Known nonmodifiable predictors of functional decline include age, education, medical comorbidity, cognitive function, smoking history, and presence of previous spine fracture.223
Children and Adolescents
Research has produced dramatic advancements in children’s health that have an impact on adulthood. The long-term benefits of childhood intervention to prevent adult disease are documented. For example, preventing osteoporosis in the aging adult begins by providing necessary dietary calcium intake during bone development and calcification in childhood.
Preventing tobacco-related cancer and lung diseases begins with educating children about the risks of initiating smoking. Healthy People 2010 leads the country in trying to develop effective and economic self-management strategies and interventions for children and families to prevent disease and improve health.
As the young and the aging continue to garner attention, teenagers are falling between the cracks of medical care. Prenatal and well-child prevention programs have boosted the care given to the under-12 age group, but most physicians do not categorize teenagers as adults and may not be adequately addressing the needs of this group.
Adolescents as a group are the primary users of illicit drugs, tobacco, and alcohol and comprise the largest group with unwanted pregnancies, abortions, and sexually transmitted diseases. Preventive health care and intervention among this age group are the next targets for the Healthy People 2010 campaign.
Gender
Increasingly, research efforts are finding that the differences between men and women go far beyond the reproductive organs to affect every physiologic function and organ in the body, including the aging process. Physiologic or biologic differences between males and females are sometimes referred to as sex-related. Behavioral or social role differences are more often referred to as gender-related.
Gender-Based Biology
Gender-based biology has demonstrated major gender differences in such things as risk factors, response to medications, response to surgical procedures, and response to treatment. Striking physiologic differences exist between men and women. For example, sports injuries linked with neuromuscular imbalance are more common in women, especially young female athletes.
Women’s hearts beat faster, which is now recognized as a result of the configuration and activity of the cardiac cell membrane as they function differently between the genders. Men’s brains are larger than women’s, but women have more brain cells. Diagnostic scanning shows that different areas of the brain light up in response to an identical task between men and women. Age-related changes that differ in men and women are just now coming to the forefront of science.
Men generally experience poorer health than women and have a decreased life expectancy compared with women. Prostate and testicular cancer rates are increasing, while male fertility may be declining; male sexual dysfunction, including erectile dysfunction (ED), is common.15
Gender Bias and Gender Equity
Until the late twentieth century, evidence for gender bias, usually against women, was seen in three areas: (1) the historical use of public monies to fund research predominantly in men, (2) the perpetuation of the view in medicine that the 70-kg man is the norm for representing all humans in medicine, and (3) the use of federal funds through Medicare to provide better reimbursement for conditions more prevalent in men compared with those more prevalent in women.42
The National Institutes of Health (NIH) issued guidelines in 1990 requiring the inclusion of women and minorities in all NIH-sponsored clinical research and revised these guidelines in 1994 to require analysis of clinical trial outcomes by gender. Although most clinical studies since that time have included women as study subjects, only a small percentage of research findings are analyzed by gender.253
New studies evaluating differences between the genders regarding a variety of factors are currently underway.99 The importance of gender equity in health is receiving more attention, with increasing focus on gender roles linked with health-related problems. For example, because men may perform more physically challenging jobs in the workplace, they are at increased risk for work-related accidents.15
Gender-Based Patterns of Disease
It is clear now that men and women experience different patterns of disease. Some gender differences may represent either environmental or genetic factors. Diseases with rates of occurrence that differ between men and women may reflect lifestyle or environmental differences or anatomic and hormonal differences.
Women are twice as likely as men to contract a sexually transmitted disease (STD) and 10 times more likely to contract HIV, in particular during unprotected sex with an infected partner. Women smokers are more likely to develop lung cancer than men who smoke. Women are more likely to have a second heart attack within a year of the first, and nearly one-half of men but only one-third of women survive 1 year after a heart attack.
Women constitute 80% of those who have bone loss (osteoporosis) severe enough to increase fracture risk significantly; women have higher blood alcohol levels than men after both consume the same amount; and women tend to regain consciousness after anesthesia more quickly than men.107 Additionally, the incidence of health risks to women, such as depression, anxiety, alcoholism, and eating disorders, is increasing.64,127
Men, however, face some unique health challenges. Deaths from malignant melanoma are 50% higher in men than in women, despite a 50% lower incidence of the disease in men. In general, men die an average of 5 years earlier than women, develop heart disease a decade earlier, and are more likely to participate in dangerous jobs and recreational activities. Men are two times more likely than women to die from unintentional injuries and four times more likely to die from firearm-related injuries.
Additionally, researchers are now examining whether people are more vulnerable to environmental and biologic challenges during periods of critical biochemical change than in times of relative quiescence. For example, are social, biologic, or psychologic changes that affect health influenced during hormonal fluctuations associated with puberty, premenstrual cycles, pregnancy, and menopause, compared with other periods in a woman’s life cycle?
Gender Roles in Health
Gender expectations play a role in response to health issues in most cultures in the United States. The familiar male stereotype, which places a high value on stoicism and self-reliance, may make asking for medical help a sign of weakness. Men are vulnerable to social pressures that lead to eating disorders, an increasingly prevalent problem among men in the United States. Males are expected to show less expression of pain than females, and in most cultures, men will be less expressive in describing pain. In some cultures, male children are held in higher regard than female children and are more likely to receive any necessary care and follow-up prescribed.
Men also tend to take greater risks with their health: many drink excessively, smoke, practice unsafe sex, drive dangerously, or participate in high-impact sports (competitively and recreationally). Risk-taking behaviors may be intended to prove masculinity. Men are less likely than women to seek medical care or practice preventive medicine, and men are less likely to have a primary care physician. They are more likely to delay medical evaluation until later in the course of an illness compared with women.15
Men who have sex with men (MSM) have health concerns beyond HIV, including a higher rate of suicide, self-harm, problems with alcohol and other drug abuse, tobacco use, and a wide range of other mental and sexual health problems. Expanded knowledge and understanding of the unique health problems of this group are advocated.271,276
Gender and Exercise
Previously, it was taught that few differences between men and women exist in response to exercise, so few adjustments were made when prescribing exercise for the female as opposed to the male. New research results document significant differences that exist in neuroendocrine, metabolic, and cardiovascular counter-regulatory responses in men and women to prolonged moderate exercise.
How these differences will affect exercise programs or recommendations remains to be determined.60 It is important to match the intensity of the exercise to the capacity of the individual. When training heart rate has not been determined through prescreening exercise testing, an exercise protocol should progress in slow stepwise increments.
LIFESTYLE FACTORS THAT INFLUENCE HEALTH
According to the World Health Organization (WHO), the highest number of deaths are attributed to the risk factors of tobacco use, high blood pressure, high body mass index, high cholesterol, low fruit and vegetable intake, alcohol consumption, and lack of physical activity, in that order.202 More than half of deaths from the leading causes in the United States (see Table 2-1) result from behavioral and lifestyle factors such as diet, exercise, smoking, and substance abuse. These factors not only contribute to the number of deaths but also contribute significantly to disability and the burden of disease.
More than any other intervention, changing behavior and lifestyle could help prevent death, enhance the quality of life, and reduce the escalating costs of treating chronic illnesses. For example, although heart disease remains the number one cause of death in the U.S. adult population, the cardiac death rate has been reduced by 52% over the last 2 decades as a result of changes in diet and lifestyle.
Other risk factors in lifestyle affecting health status and health care are considered individually modifiable and include personal habits such as rest and sleep; diet, including calcium, fat, and fiber intake; level of activity and exercise (fitness); stress and coping ability; substance abuse; travel; environmental or occupational status; and high-risk sexual activity.
The gay and lesbian population comprises a diverse community with disparate health concerns. Major health issues for gay men are HIV/AIDS and other STDs, substance abuse, depression, and suicide. Gay male adolescents are two to three times more likely than their peers to attempt suicide. Some evidence suggests lesbians have higher rates of smoking, obesity, alcohol abuse, and stress than heterosexual women. The issues surrounding personal, family, and social acceptance of sexual orientation can place a significant burden on mental health and personal safety.67
This section examines selected lifestyle and behaviors that affect health and directly influence physical therapy practice. Psychologic and behavioral risk factors that influence health outcomes presented include physical activity, nutrition, tobacco use, alcohol and other drug use, stress and coping, and domestic violence. Some current theories about health behavior change that can influence effectiveness of physical therapy interventions will also be discussed.
Cultural Influences
Variations in lifestyle influencing clients’ perceptions of health care may occur as a result of cultural, religious, socioeconomic, or even age factors. Although clinical manifestations of a disease or condition are essentially the same across cultures, how a person (or family member) responds or interprets the experience can vary.
This phenomenon of response based on cultural influence is called cultural relativity—that is, behavior must be judged first in relation to the context of the culture in which it occurs. For example, some groups consider health as a function of luck (good or bad), whereas others see health problems as a punishment for bad behavior and good health as a reward for good behavior.
Cultural factors may also prevent illness. For example, people belonging to religious faiths that forbid drinking or smoking have lower cancer rates than the general population. Religious beliefs related to health must be recognized and respected. Research to study the effects of religiosity as a predictor of outcome in a variety of disorders is beginning to draw definitive conclusions about the efficacy of prayer, religious practices and activities, and philosophic orientation toward health.10,143,229 Research suggests that one of the principal reasons people are attracted to alternative medicine is that they find many of these therapies in keeping with their personal beliefs.11
Demographics by Generation
Generational differences are seen among groups such as the Matures, also known as postwar/depression-era (born from 1900 to 1946); the baby boomers (born from 1946 to 1964); the Generation X-ers (born from 1965 to 1979); and the Millennials, also referred to as Generation Y (born from 1980 to 1999).
Many people born before 1946 tend to assume a passive role in their own health and in receipt of health care by accepting whatever happens to them and whatever treatment is outlined. However, baby boomers have grown up questioning authority, and their offspring are even more likely to consider themselves consumers asking for treatment rationales, seeking second opinions, and combining allopathic treatment with alternative medicine (e.g., naturopathy, aroma therapy, acupuncture, massage therapy).
Socioeconomic Status
The most adverse influence on health is socioeconomic status, with a higher percentage of low-socioeconomic class members experiencing health-related problems than any other group. Adults with higher incomes tend to experience better health and can expect to live more than 3 years longer than those in the lowest income bracket.
The percentage of people in the lowest income families reporting limitation in activity caused by chronic disease is three times that of people in the highest income families.110 Lack of health insurance coverage and/or access to quality health care may result in delayed or postponed diagnosis and treatment of health problems.
Differences in attitudes toward health have been found to be greater between social classes than between races or ethnic groups. Ninety percent of all health care dollars is spent on extraordinary care in the last 2 to 3 years of life. This style of death-based medicine assigns the greatest financial and professional resources to treating the diseases of aging.138
The homeless have become one of the fastest growing populations in need of health care in the United States. Traditionally, the homeless consisted primarily of older, single men, often alcoholics, but now this group includes families and children who are runaways or adolescent throwaways.
Declining public assistance, a shortage of affordable rental housing, and an increase in poverty are additional contributing factors to the rise in homelessness. Although estimates of homeless people vary, the National Coalition for the Homeless188a reports that on any given night, 700,000 Americans are homeless and up to 2 million homeless people are reported in a year’s time. This number includes an estimated 100,000 children in the United States who are homeless; more than half are under age 5.
Adverse Childhood Experiences
Adverse experiences in childhood are linked to the development of problems later in life, including alcohol and other drug use, drug and/or tobacco addiction or addictions, obesity, fibromyalgia, or other autoimmune disorders. Children who have been exposed to four or more adverse experiences in childhood are more likely to have attempted suicide and to have had multiple sex partners, increasing their risk of STDs. Dangerous or apparently counterproductive behaviors can serve a purpose (e.g., coping mechanism, barrier against social contact).
The strong relationship between exposure to abuse or household dysfunction during childhood and multiple risk factors for several of the leading causes of death in adults is beginning to be recognized in the health care setting.8,78 Healthy People 2010 has set goals of primary prevention of adverse childhood experiences and improved treatment of exposed children to reduce self-destructive behaviors, such as smoking, among adolescents and adults. For a more complete understanding of the impact of adverse experiences in general, see Chapter 3.
Physical Activity
The benefits of physical activity have been recognized since the time of Hippocrates, as evidenced by this quote attributed to Hippocrates (460-377 BC): “All parts of the body which have a function, if used in moderation and exercised in labours in which each is accustomed, become thereby healthy, well-developed and age more slowly; but if unused and left idle they become liable to disease, defective in growth, and age quickly.” The importance of physical activity seems to be as relevant today as it was then.
Physical activity is defined as any bodily movement produced by skeletal muscles that results in an expenditure of energy.62 Physical activity behaviors are different than other lifestyle behaviors, in that all individuals have to move, although some move more and some move less. Physical activity contributes both directly and indirectly to health status and outcomes. Physical activity levels appear to contribute directly to disease mortality and morbidity, as well as indirectly by the influence of physical activity on conditions such as obesity, diabetes, and osteoporosis.
Physical fitness may be defined as “a set of attributes a person has in regards to a person’s ability to perform physical activities that require aerobic fitness, endurance, strength, or flexibility and is determined by a combination of regular activity and genetically inherited ability.”62 Physical fitness and physical activity are related since increased physical activity is required to improve physical fitness, although one can perform a modest amount of physical activity without seeing improvements in fitness.
Effects of Physical Activity on Morbidity and Mortality
Much has been learned in the last decade about the adaptability of various biologic systems and the ways that regular physical activity and exercise can influence them. Participation in regular physical activity (both aerobic and strength training) is an effective intervention modality to reduce and/or prevent a number of functional declines associated with aging and to elicit a number of favorable responses that contribute to healthy aging32 (Box 2-2).
The effect of training intensity, psychosocial variables influencing exercise, and the breadth of emotional benefit from physical activity has not been fully determined, although studies in this area are ongoing. The risks and benefits of exercise among people with disabilities remain unknown. As people with disabilities live longer, the need for addressing long-term health issues, assessing the risk for secondary disability, and prescribing exercise from the perspective of disease prevention while reducing the risk for injury is needed.58
Other research to determine the potential links between oxidative stress and physical activity/exercise in the aging adult is ongoing. Exercise, especially when performed strenuously, is associated with increased free radical formation (see Fig. 6-2) that damages key cellular components.210 In the older adult the benefit of exercise is influenced by sedentary lifestyle, nutritional deficiencies, and comorbidities that can all deplete the individual’s antioxidant reservoir.
Aging adults face additional problems of deconditioning or loss of balance and stability as a result of disease or illness. The most successful exercise programs take into consideration the person’s functional capacity, medical status, and personal interests. Some helpful strategies for facilitating an exercise program (whether for a specific body part or as an overall fitness program) are listed in Box 2-3.
Morbidity.: Physical inactivity contributes to the incidence of some chronic diseases. According to the WHO, there is convincing evidence that physical inactivity increases the risk of obesity and type 2 diabetes. In other words, regular physical activity decreases the risk of cardiovascular disease, type 2 diabetes, obesity, and osteoporosis and decreases the risk of some types of cancers (e.g., colorectal).258
Regular physical activity appears to modify or reverse cardiovascular disease severity in individuals with known cardiovascular disease.242 These effects include decreased risk of death from cardiovascular causes,243 decreased atherosclerotic plaque formation,104 and improved health status.200
Aerobic and resistive exercise appear to be associated with a decreased risk for type 2 diabetes, even among people at high risk for the disease.114 In one large study, the risk of type 2 diabetes decreased 6% for every increase in energy expenditure of 500 kilocalories (kcal)/week.113 In addition, moderate physical activity was shown to be as effective as one type of diabetes medication (metformin) in reducing risk of diabetes.140
Osteoporosis is associated with increased disability and frequency of some types of fractures. The greatest benefits to bone mineral density and the incidence of osteoporosis appear to come from resistance training.257 Exercise training programs have been found to prevent the 1% of bone loss per year observed in the lumbar spine in premenopausal and postmenopausal women.268
In regard to cancer, physical activity has an effect on some kinds of cancers.152 Physical activity decreased the risk of colon cancer for men and women by 30% to 40% and also demonstrated a risk reduction of 20% to 30% for breast cancer in physically active women.152
Since there is an association of improved health with increased physical activity, it is important to define how much physical activity is beneficial. There is debate over the optimal amount of exercise needed for health benefits, although the general agreement is that more is better. Current discussion centers on whether the volume or intensity of exercise is most important for health.73 Given that moderate exercise appears to provide significant health benefits and that vigorous exercise is difficult for individuals to achieve, public health policy has emphasized regular moderate exercise as an achievable goal for the greatest number of individuals.
The current recommendation of the U.S. Surgeon General indicates that individuals should accumulate 30 minutes of moderate exercise on most days of the week. Minimum increments of 10 minutes are advised. Additional wording indicates that people who are already active may benefit from more intense levels of physical activity.62
Mortality.: Physical activity patterns appear to have a direct effect on deaths. In the 1990s, activity patterns and nutrition contributed to 14% of all deaths in the United States.166 In addition, 23% of deaths from major chronic diseases were also linked to lack of physical activity.102 Increased levels of physical activity appear to reduce the relative risk of death in both men and women by 20% to 35%.163,164 In addition, increased physical activity by 1000 kcal/week or 1 metabolic equivalent (MET) of fitness is associated with a 20% decrease in mortality, at least among women.126,153
Physical fitness appears to confer a greater benefit than physical activity alone. A clear relationship between fitness and all-cause mortality and deaths from cardiovascular disease has been established.69 These studies demonstrate that death rates are highest in the lowest quartile of fitness. The greatest improvement in mortality occurs between the lowest and next lowest category of fitness, suggesting there is a graded effect of improved fitness on mortality. This is consistent with other research that demonstrates that small improvements in fitness are associated with significant reduction in risk of cardiovascular events and death.258
Occupational Versus Leisure Time Physical Activity
Early investigation of the role of physical activity in mortality compared people in sedentary versus physically active occupations.178 Much of the recent literature, including the Surgeon General’s report, has investigated leisure time physical activity.62 Taking the evidence together, it appears that the overall volume and intensity of physical activity are most important, whether at work or during leisure time. However, there may be additional effects of strenuous work on health status or musculoskeletal pathology. For example, self-reported health was lower in people with active and strenuous jobs.203
In a study of industrial workers over a 28-year period of time, vigorous leisure time activity was associated with low risk of poor physical function, but strenuous work activity increased the risk of poor physical function.154 In addition, low levels of physical activity were associated with higher rates of low back pain.115 Future investigations may clarify the various effects of leisure versus occupational physical activity.
Aerobic Capacity Versus Musculoskeletal Fitness
Physical activity, regardless of aerobic capacity level, appears to provide health benefits. Musculoskeletal performance is increasingly linked to improved physical function and prevents or modifies disability.177 Many activities of daily living (ADLs) require more musculoskeletal performance and rely less on aerobic capacity.258 Furthermore, a decline in physical performance, defined by activities such as rising from a chair and climbing stairs, is associated with dependence in ADLs and assisted living placement.101
Prevalence of Physical Activity Behaviors
Two behavioral strategies for reducing the risk for chronic disease have been identified: (1) consuming fruits and vegetables five or more times per day and (2) engaging in regular physical activity. Despite the importance of physical activity, only a minority of Americans are meeting physical activity guidelines.
Data for the prevalence of physical activity behaviors are available from a variety of population surveys. One common source of information is the Behavioral Risk Factor Surveillance System45 (BRFSS), a population-based, random digit–dialed telephone survey of the U.S. population greater than 18 years of age conducted by the CDC.174 Information regarding health risk behaviors, clinical preventive health practices, and health care access, primarily related to chronic disease and injury, is obtained from a representative sample of adults in each state.174 Respondents are asked to recall the overall frequency and time spent in a variety of leisure time activities, as well as in moderate and vigorous physical activity.
In the Surgeon General’s 1996 report, which used a variety of population-based surveys, most adults were not meeting current physical activity guidelines.62 About 25% of adults reported no physical activity during leisure time. Approximately 22% of adults engaged in physical activity of any intensity for 30 minutes, 5 days a week. Only 15% of adults engaged in vigorous physical activity for 20 minutes, 3 times a week.
An update on physical activity in 2000 to 2001 from the BRFSS indicated that approximately 26% of adults had no form of physical activity during their leisure time, a number that is slightly higher than the 1996 data. The BRFSS lifestyle activity questions were modified in 2000 to 2001. Based on the new wording of the questions, 45% of adults participated in physical activity that met the new guidelines of the Surgeon General. These numbers indicate there is much work to be done to increase physical activity within our country.
There are differences in physical activity and nutrition reported by ethnicity. Among men, engaging in regular physical activity was significantly less common for non-Hispanic blacks, Hispanics, and Asian/Pacific Islanders than for non-Hispanic whites. Among women, regular physical activity was significantly lower among non-Hispanic blacks and Hispanics than among non-Hispanic whites.146
Compared with non-Hispanic white men, the combined prevalence for eating fruits and vegetables five or more times per day and engaging in regular physical activity was significantly higher for men of multiple/other races. Among women, the combined prevalence of eating fruits and vegetables five or more times per day and engaging in regular physical activity was significantly lower for non-Hispanic blacks and Hispanics than for non-Hispanic whites.146
Based on the Surgeon General’s report, which used a variety of population-based surveys, most children and youth are not meeting current physical activity guidelines. About 15% of children reported no recent physical activity of any intensity during leisure time. Inactivity is higher in girls versus boys and in black girls versus white girls.
Approximately 25% of youth reported no vigorous physical activity; however, 25% also report walking or biking nearly every day (equivalent to light or moderate activity). Participation in physical activity decreases significantly as age or grade in school increases.62 Youth Risk Behavior Surveillance System (YRBSS) reports one-third of all students grades 9 to 12 did not meet national guidelines for physical activity in 2003.100
Regular physical activity is beneficial in improving both physical and mental health outcomes. There is evidence that physical activity decreases blood pressure, improves lipid profile by decreasing triglycerides and total cholesterol while increasing high-density lipoprotein (HDL), improves insulin sensitivity, and enhances endothelial function, all of which contribute to decreasing cardiovascular risk.258 In addition, regular physical activity is associated with an increased sense of well-being, can modify the symptoms of depression, and increase self-efficacy (the ability or confidence of a person to implement an effective behavior).267
Interventions for Increasing Physical Activity
Given the benefits of physical activity, it is helpful to know what type of interventions are successful in increasing physical activity. There are a variety of strategies used to encourage physical activity, including self-directed behavior, supervised programs, or combined approaches. However, it is difficult to compare the success of interventions since they are so varied. A review of physical activity interventions examined randomized controlled trials for different interventions for community living adults with a 6-month follow-up and no more than 20% participant loss over the time period.119
All types of interventions were successful at increasing physical activity levels, including individual and positive encouragement and group or individual exercise programs.119 This implies that all medical practitioners, including physical therapists, should encourage individuals to exercise. Cardiopulmonary fitness also improved in people who exercised, as compared to controls. However, few studies were able to demonstrate success for individuals in achieving a predetermined amount of physical activity.160
The interventions that appear to improve physical activity the most include physician advice; counseling from a health educator on action planning and follow-up phone calls, emails, monitoring cards; and a pedometer.119 Adding weekly classes on skills for increasing physical activity and educational materials appears to help women achieve higher fitness goals, though these additions do not significantly influence men.277 Success appears to increase with ongoing support in which there are four or more contacts among exercise participants and staff.119
2-2 SPECIAL IMPLICATIONS FOR THE THERAPIST
Reports indicate that few adults combine consuming fruits and vegetables frequently and engage in regular physical activity, thus missing an opportunity to help reduce their risk for chronic disease. The therapist can participate in promoting healthy behaviors by including each of the following steps.
Physical Activity Recommendations62
• Accumulating 30 minutes of physical activity has been shown to have health benefits; however, the minimum amount of time to be spent in physical activity is 10 minutes.
• Moderate exercise is defined as reaching a certain threshold of energy expenditure. Energy expenditure estimated in METs gives a guideline for energy expenditure. By definition, 1 MET is equivalent to the amount of oxygen consumed at rest, averaged at 3.5 ml/kg−1/min−1. Moderate activity ranges from 3 to 6 METS, or 10.5 to 21.0 ml of oxygen consumed for each kilogram of body weight per minute. This leads to approximately 100 calories burned for 30 minutes of exercise in an individual who weighs 150 lbs.
Table 2-2 provides some estimates of energy expenditure for the average person that can be used in physical therapy settings.

Nutrition
Nutrition is a modifiable risk factor for chronic disease; there is increased evidence that diet has significant effects (positive or negative) on health. Studies by the WHO indicate that diet has an important role in preventing and controlling both morbidity and mortality.272 The chronic diseases most influenced by diet and creating the greatest cost in deaths or disability include obesity, diabetes, cardiovascular disease, cancer, and osteoporosis.
The National Cholesterol Education Program and the American Cancer Society both emphasize lifestyle modifications that include diet and physical activity to reduce disease risk. Diets high in fruits and vegetables combined with participation in regular physical activity are associated with a lower risk for several chronic diseases and conditions. These are also two of the strategies implemented by states participating in the CDC Nutrition and Physical Activity Program to Prevent Obesity and Other Chronic Diseases.146
Significant changes have occurred in the world food economy with profound effects on diets and lifestyles. These shifting dietary patterns include increased consumption of energy-dense foods high in saturated fat and low in unprocessed carbohydrates. Nutritional patterns indicate that in industrialized countries, energy intake averages 3380 kcal per capita per day, with a large increase (26%) from 1969 to 1999 in energy supplied by animal fat. North America remains above the recommended average of fat-to-energy ratio defined as the percent of energy derived from fat in the total number of calories supplied, as well as above the recommended amount of saturated fat per total calories (10%).273
Obesity
Obesity is defined by an excessive accumulation of fat in the body that contributes to numerous chronic diseases and early mortality and morbidity. Bariatrics is a branch of medicine concerned with the management of obesity.233
Body mass index (BMI), a ratio of height to weight, further classifies obesity in a clinically feasible manner as both are easily measured (Table 2-3). The NIH191 clinical guidelines and the WHO275 have stated that overweight is defined as having a BMI equal to or greater than 25 kg/m2. Obesity, defined as a BMI greater than or equal to 30 kg/m2, is further divided into three classes. A BMI greater than or equal to 25 is associated with increased risk for premature death and disability. As one progresses to a higher class of obesity, health risk and morbidity increase.88 The term morbid obesity has been used by some authors to refer to a BMI greater than 40.130
Table 2-3
Body Mass Index (BMI) to Determine Obesity Classification
| NHLBI Terminology | BMI Range (kg/m2) | WHO Classification |
| Underweight* | <18.5 | Underweight |
| Normal | 18.5-24.9 | Normal |
| Overweight | 25.0-29.9 | Preobese |
| Obesity Class 1 | 30.0-34.9 | Obese Class 1 |
| Obesity Class 2 | 35.0-39.9 | Obese Class 2 |
| Obesity Class 3 | ≥40.0 | Obese Class 3 |
NHLBI, National Heart Lung and Blood Institute; WHO, World Health Organization.
To calculate your BMI using pounds (lbs) and inches (in), multiply your weight (lbs) × 700 and divide the product by your height in inches squared. NOTE: you can easily calculate your BMI on-line at http://www.nhlbisupport.com/bmi/bmicalc.htm.
In addition to the use of BMI, medical professionals may still define obesity as weight greater than 20% of desirable weight for adults of a given gender, body structure, and height. A more precise classification has been suggested, with overweight describing someone weighing 10% more than his or her optimum weight; obese describing individuals weighing 15% more; and grossly obese describing persons weighing 20% or more above the optimum weight for height and body type.
BMI, however, is currently the most common measure of obesity and is an internationally accepted and understood definition of the condition. Regardless of the measure used, obesity is a condition that is inherently risky for health and longevity, especially if the distribution of such fat is in and around the abdomen (see Fig. 11-8). Although a highly muscular person may have a higher than desirable BMI, health risk occurs only if BMI is indicative of excess body fat.
BMI varies with age and sex in children and adolescents, necessitating the CDC to develop BMI charts that uniquely account for growth using weight and height. Pediatricians should track growth regularly and confer with parents when a child or adolescent presents with a BMI greater than or equal to the 85th percentile. BMIs greater than or equal to the 85th and less than or equal to the 95th percentile signify a risk for being overweight; BMI greater than or equal to the 95th percentile signifies risk for being obese.
Incidence and Prevalence
Obesity is now regarded as a pandemic with implications for 300 million people across the world.217 Obesity has begun to replace other known causes of mortality (e.g., undernutrition and infectious diseases) as the most significant contributor to ill health. It is second only to cigarette smoking as a leading cause of preventable death in the United States and contributes to 500,000 deaths annually; out of these deaths the CDC reports that 30,000 are premature deaths. In the United States, it is estimated that 65% of adults can be categorized as overweight or obese.82
The prevalence of obesity among adults continues to increase.33 From 1980 to 2002, obesity has doubled in adults and overweight prevalence has tripled in children and adolescents.197 In 2003 to 2004, 17.1% of children and adolescents aged 2 to 19 years were overweight and 32.2% of adults were obese.197 This growth in the percentage of people who are now overweight or obese is occurring across all age groups and of significant concern in the pediatric and geriatric populations.
The U.S. Department of Health and Human Services (DHHS) reports that one out of every five children is obese and the obesity rates have increased 147% from 1971 to 1994 among children ages 6 to 11.46 The increase in numbers of people who are obese is paralleled by a considerable reduction in daily energy expenditure and physical activity that leads to a decrease in aerobic capacity and deficiencies in the ability to perform physical activities.47,166,192,247
Existing evidence indicates that physical inactivity is strongly associated with body weight gain and that the conduct of purposeful and regular exercise and maintenance of a physically active lifestyle can be effective in maintaining a healthy body weight.52,89,265 Although sedentary lifestyles have not been causally linked to BMI, the risk of becoming sedentary increases with BMI.180 Research has confirmed the importance of physical activity to maintain weight loss, especially if exercise commitment reached or exceeded 200 minutes per week.131,134
Etiologic and Risk Factors
The development of obesity depends on an imbalance between energy intake and energy expenditure, with more energy consumed than is expended. Inactivity and a high-fat, low-carbohydrate diet with excess intake of refined sugar are contributing factors to excess adipose tissue and weight gain.
Hill and colleagues,116 using National Health and Nutrition Examination Survey (NHANES)116,185 data over an 8-year period, have determined that the median energy accumulation is 15 kcal/day and that 90% of the population accumulates less than 50 kcal/day. This means that an intervention that reduced energy gain by 50 kcal/day could offset weight gain in about 90% of the population.
In other words, for every excess 100 kcal consumed, at least 50 kcal of energy are deposited in energy stores. On the basis of this information, most of the weight gain seen in the population could be eliminated by some combination of increasing energy expenditure and reducing energy intake by 100 kcal/day, closing the energy gap.64 This can be accomplished by simply walking an extra mile per day or for 15 to 20 minutes, or by reducing intake with smaller portions of food. The reason an energy imbalance leads to obesity remains unknown. However, factors that are associated with the development of the energy imbalance and that may lead to excessive fat deposition and obesity are listed in Box 2-4.
In addition to the failure of aging people to adjust food intake in response to lowered metabolism and diminished activity, weight cycling with fluctuations of body weight produced by repeated cycles of weight loss and gain appears to contribute to the inability to lose weight on a long-term basis.
Medication-induced weight gain may occur as a result of increased appetite, episodes of hypoglycemia, or water retention. Other drugs, such as corticosteroids, make the body less able to absorb blood glucose, leading to increased fat deposits in the trunk. Antihypertensive medications, such as beta-blockers, may produce fatigue or shortness of breath, leading to reduced activity levels and increased weight gain.
A growing body of evidence suggests that some forms of obesity are more likely the result of biochemical defects rather than consumption of excess calories.225 After a 40-year search, scientists originally found three genes linked to obesity (ob, neuropeptide Y [Npy], and the Beacon gene). Npy and the Beacon gene produce a protein that stimulates the appetite, whereas the ob gene produces a protein (leptin) that switches off the appetite. In some obese people, the body does not respond to leptin; in others, the Beacon gene is working in overdrive, producing too much appetite-stimulating protein.57 Preliminary studies show that the Beacon gene is the same across various regions and ethnicities.
More recently, more genes and digestive tract hormones have been found that may influence why some individuals become obese and others do not. Newer genes being investigated are Insig-1 and Foxa-2 and the hormone known as peripheral hormone peptide YY (PYY). Insig-1 blocks the formation of new fat cells and is suspected to be more active in various parts of the body, thus accounting for different body contours and deposits of fat tissue.156 Foxa-2 is known to prevent immature cells from developing into new fat cells.269 Location and lack of Insig-1 and Foxa-2 genes may influence where fat is deposited and if more than normal fat deposits occur.
Peripheral peptide YY or hormone PYY is produced by cells in the stomach and intestines after a meal. PYY is thought to act on the brain to reduce appetite. PYY and many gastrointestinal hormones are being investigated as potential weight loss drug targets.50,215,230
Despite the new discoveries of single-gene mutations resulting in obesity, most cases of obesity are more likely the result of subtle interactions of several related genes with environmental factors, which favor the net deposition of calories as fat resulting in obesity. The increasing rates of obesity cannot be exclusively explained by changes in the gene pool, although genetic variants that were previously silent are now being triggered by the high availability of energy-and fat-dense foods and by the increasingly sedentary lifestyle of modern societies.165
Pathogenesis
The mechanisms proposed to explain the development or effects of obesity on the human body target neurologic, metabolic, and energy regulation systems.
Accumulating evidence indicates that obesity is a central nervous system–mediated neuroendocrine dysfunction. Since the central nervous system plays a key role in the regulation of food intake and energy balance, one explanation may be that either spontaneous genetic mutations or targeted gene deletions that impair central nervous system signaling cause disrupted food intake and body-weight control.25 Researchers are studying the highly complex process of signaling molecules involved in the regulation of food intake and how inherited or acquired defects in the function of these hormonal and neuropeptide signaling pathways contribute to obesity.226,270
Another explanation involves the neuroendocrine system and suggests that hormonal dysfunction affecting the hypothalamic-pituitary-adrenal (HPA) axis results in a complex series of events. Stress stimulates daily, periodic elevations of cortisol secretion and results in impaired cortisol secretion, prolonged stimulation of the sympathetic nervous system, and subsequent hypothalamic arousal. The net effects of this neuroendocrine-endocrine cascade are poorly regulated cortisol secretion, insulin resistance, elevated blood pressure, and visceral accumulation of body fat (central obesity).31 The result can be a collection of metabolic risk factors, referred to as the metabolic syndrome, which includes abdominal obesity, atherogenic dyslipidemia, elevated blood pressure, insulin resistance, and prothrombotic and proinflammatory state of the blood (see further discussion of the Metabolic Syndrome in Chapter 11).
Energy regulation also has been a target for explaining the mechanism(s) of obesity. In this case, the sodium (Na+)/potassium (K+)/adenosine triphosphatase (ATPase) pump is believed to play a major role in the development of obesity. This enzyme pump transports sodium out of the cell and potassium into the cell at the expense of cellular energy in the form of adenosine triphosphate (ATP). Obese people are believed to have fewer ATPase pumps than the nonobese; the obese person uses less energy and expends fewer calories, keeping a state of equilibrium within the body.
The adipose cell theory postulates that some people inherently have an excessive number of fat cells (adipo- cytes) and the size of the fat cells is increased. Similarly, the lipoprotein lipase (LPL) theory suggests that LPL (the enzyme that helps fat to be deposited in adipocytes) is elevated in obese persons and weight reduction stimulates even more production of LPL, causing fat cells to return to their hypertrophic size.
More recently, researchers have proposed the theory that for some people, obesity is the result of intestinal microorganisms. The microbial theory of obesity suggests a biologic cause of weight gain from an altered level of bacterial intestinal microbes called gut microflora, which may be responsible for regulating energy intake, absorption, and storage.14,155
Clinical Manifestations
Regardless of the mechanisms on the condition, the outward signs and symptoms of obesity are readily observable (excess body fat). However, the effects and complications of obesity are less easily identified at onset.
Obesity is associated with significant increases in both morbidity and mortality from many conditions (Box 2-5) and is associated with three leading causes of death: cardiovascular disease, cancer, and diabetes mellitus. The role of obesity in inflammation is discussed in Chapter 11, and fat (adipose tissue) as an endocrine gland and its role in cancer is discussed in Chapter 11.
Other complications may include nephrotic syndrome and renal vein thrombosis; other thromboembolic disorders; digestive tract diseases, such as gallstones and reflux esophagitis; asthma; obstructive sleep apnea; carpal tunnel syndrome; and subsequent pulmonary compromise with decreased gas exchange, vital capacity, and expiratory volume.
Diet accounts for about 35% of all cancers8; obesity is a known risk factor for hormone-related cancers such as breast, cervical, endometrial, and liver cancer in women and prostate, colon, and rectal cancer in men.2,145 Obesity may increase the risk of Hodgkin’s lymphoma, especially among men.262 See further discussion on the influence of obesity on cancer in Chapters 9 and 11.
As discussed, dietary patterns (highly processed and refined foods without fiber) in combination with physical inactivity contribute to obesity and metabolic consequences. Nutritional modulation of growth-enhancing and differentiating hormones is discussed further in Chapter 9.
Some scientists believe that there is a causal relationship of obesity with asthma.51,221 The mechanism for the causality is thought to be related to an inability of the person to take deep breaths, which leads to more reactive airways and, if severe enough, asthma. Research is mixed as to whether the link between obesity and asthma is the same for women and men. One study concluded that independent of age, women with a BMI greater than or equal to 30 kg/m2 were about twice as likely to develop asthma as women of a normal weight.51
Type 2 diabetes mellitus is often associated with obesity. Excessive food intake stimulates hyperinsulinemia. Through a negative-feedback mechanism, excessive insulin levels decrease the number of insulin receptor sites on adipose cells. The decrease in insulin receptor sites decreases the amount of glucose that can enter the cells. This promotes high blood levels of glucose. The excess glucose is stored as glycogen in the liver or as triglycerides in adipose cells, thereby enhancing hypertrophy and hyperplasia of fat cells in the already obese person. Weight reduction does reverse this process.
Obesity also is associated with significant functional deficits or problems that lead to functional impairments. Shortness of breath; fatigue; ADL limitations237; increased risk for falls59; and an increased incidence of hip, knee, and back pain in those who are obese9 are potential problems.
Given a strong association between obesity and osteoarthritis (OA) of the knee, the risk for dysfunction in functional activities, such as walking and stair climbing, has been investigated.55,171 Weight loss has been shown both to reduce the risk of OA, as well as to improve function in the face of this condition.171
Both perceptions and observed measures of functional limitations have been tested and found to be associated with difficulty of accomplishing daily tasks related to housework and self-care.149,150 Thus the clinical manifestations of obesity have broad implications for numerous body systems and health dimensions.
MEDICAL MANAGEMENT
Preventing obesity from occurring or worsening is an important part of achieving a healthier population. Prevention includes maintenance of healthy weight, maintenance of weight loss, and prevention of weight gain. Identifying risk factors that can lead to obesity or cause related health problems and learning strategies toward achieving a healthy weight are the keys to successful prevention.6 See also previous discussions of physical activity and nutrition in this chapter.