The Psychosocial-Spiritual Impact on Health Care
If we consider our profession to be one of “helping,” it is inconsistent that we should extensively attend to physical pain, dysfunction, and symptoms without recognizing and attending to the non-physical contributors to those physical maladies.
PSYCHOLOGIC CONSIDERATIONS IN HEALTH CARE
Trauma and psychologic contributors to pain and dysfunction cause extensive comorbidity for people seeking resolution through health care. Medical diagnostics and treatment are too often misdirected toward physical causes for the person’s nonphysical, comorbid, emotional, and psychologic symptoms and reactions. Being clinically unaware of psychologic impact on medical care is costly and potentially damaging to both clients and clinicians.61
The cognitive, physical, emotional, and spiritual systems of human beings are intricately intertwined and interdependent. It makes sense that each of these systems can be wounded and thus need care, treatment, and healing. Treatment that comprehensively addresses each of these areas is not always the norm in the medical community.
The more vague and multifaceted the diagnosis and symptoms, the more the clinician must remember that emotional, mental, physical, and spiritual components are intricately interconnected and cannot be separated. Physical therapists are uniquely positioned and equipped to recognize physical and nonphysical contributors to pathology and, in concert with other appropriate professionals, to attend to the rehabilitation of the whole person.
It is important to remember that physical pain and symptoms that have nonphysical roots will not resolve unless the underlying causes of the problems are addressed. It is vital, as health care professionals, that we are sensitive to the effects of our care on the whole person.
Incidence of Underlying Nonphysical Trauma
Whether it is apparent, professionals in all specialties are currently treating people with unseen, devastating pain and wounds beyond their subjective reports of physical signs and symptoms. Some of the noted statistics include the following4,42,52:
• Nearly 900,000 children (12.3 children per 1000) have been identified as victims of abuse or neglect in the United States. More than 500,000 adults over 60 years of age suffer abuse or neglect annually.
• About 1.5 million women and close to 835,000 men are raped or physically assaulted by someone close to them each year. Approximately 2 out of every 3 women reporting rape, assault, and stalking are victims of repeated abuses. Over $5.8 billion every year goes toward health care for victims of rape, physical assault, and stalking.
• Conservatively, 2 million episodes of domestic violence occur in the United States annually—actual estimates may be twice that number. Each year, more than 1000 women (about 4 per day) are killed.
Statistics show that the problem of domestic violence and child abuse is not going away—in fact, the problem is becoming more evident with a continued increase in demand for family violence services every year.56 Many researchers and clinicians suggest that these statistics are low since unreported incidents, events unremembered because of dissociation, and statistics of ritual abuse (sophisticated, carefully hidden, intentional, and repeated torture) cannot be taken into account.
Deliberate, systematic trauma to children and adults is rarely discussed or prosecuted. War and combat trauma is rarely prosecuted, and Satanic ritual abuse and murder only briefly come to light. Medical costs for mental health care, lost work time, and comorbid, unresolved pathology support the fact that we cannot deny the scope and prevalence of trauma in our society and in our world.
Mild-to-extreme trauma and domestic violence are frequently well hidden and closely related to criminal acts. Perpetrators are sophisticated and highly skilled in secrecy, subtlety, and camouflage. The effects of trauma in early development on brain cognition and memory destroy victim credibility and promote denial in the victim. Physicians and therapists who serve as entry points into the health care system need to be aware of and able to care for the most needy and complex of these clients, providing comprehensive and effective care for everyone.
Torture
Torture is a very real part of today’s world events and must be included in any discussion of trauma. Amnesty International reported that torture still occurs in at least 79 of the world’s 183 countries. About 40% of refugees coming to Western Europe have experienced or witnessed torture.191
Considering the ethnic cleansing and warfare from World War II up to the present, as well as current terrorist activity and events in the Middle East, there are many people alive today who have been exposed to trauma in the form of torture. In addition, it is important to include the unknown numbers of children exposed to and experiencing repetitive ritual, sexual, and other kinds of torture.141,145
Combat
The trauma of war can affect not only the warriors but also their partners and children as well. Trauma associated with war can cause problems with self-esteem, communication, sexuality, and parenting. A condition of hyperawareness or hyperarousal is common long after the euphoria of returning home has worn off. Adrenaline rushes from constantly being on alert in war zones do not just get “turned off” once the soldier is home or in a safe environment.
Combat trauma can lead to depression, posttraumatic stress disorder (PTSD), and other forms of emotional pain. The most common problems confronting families of combat veterans include emotional numbing, sexual difficulties, anger, family violence, and guilt. Healing the wounds of war is becoming the focus of new research and clinical attention.159 For further discussion, see the section on Posttraumatic Stress Disorder in this chapter.
World Events and Cultural Trends
Currently, our world is threatened by terrorist activity. Along with our society’s saturation of fear-based marketing strategies and victim mentality, the general public in the United States is a prime target for psychogenic illness. The resulting sequelae directly impact medical care and the clinician’s perspective.
The Department of Homeland Security believes that our country and the world need to prepare for outbreaks of mass psychogenic illness.241 World and U.S. events point to the effects of fear and terrorist attacks on the general public and specifically on people in the real or perceived exposure areas. The number of individuals suffering psychogenic illness could far exceed the number of actual casualties in a chemical, biologic, or radiologic (CBR) or other life-threatening event.
Support for this perception based on real events has been published.176 Distress experienced in populations and various social groups well outside the involved communities included feelings of distrust for authority figures and organizations, anxiety over potential future threats, feelings of grief and loss, a sense of loss of control, and doubting local wisdom that persists for at least 18 months. The study punctuated the importance of open and consistent communication, personal involvement with those perceiving or recovering from trauma, and community support in trauma healing.176
The twenty-first century cultural guidelines in the United States have become more ambiguous and obscure, especially in comparison to the more tangible social constructs of the twentieth century.163 Fear-based living leads to victim mentality and can result in an unrealistic perception of life with associated loss of personal awareness and stress-management potential.
Medical remedies for common concerns serve as back-ups and safety nets when personal management skills are unsuccessful or nonexistent. Loss of confidence in innate coping ability propels us into seeking an external cause and source of remedy. Evidence of this trend is seen in medicine and in everyday life. For example, the field of obstetrics is mirroring fear-based trends, focusing on immediate need without considering future impact. Instead of seeing medical care as a back-up solution for the safety of mother and child, medical intervention for previously accepted and practiced natural labor, delivery, and birth of our children is frequently replaced with drugs to relieve maternal anxiety, prevent pain, and avoid experiencing labor.
Current trends are toward increased use of regional anesthesia and planned cesarean sections to escape the effort and perceived sensations of childbirth, for convenience, and for easing schedules of both physician and client. Many women appear to have lost all confidence in natural abilities and coping potential, putting hope and expectation in medical technology and staff.
Perceptions of Pain
Today, we have more health options and enjoy the benefits of modern medicine, but the effectiveness and scope of these advances can mislead us into thinking that every malady should be quickly curable without effort or pain. The focus of healing is usually on the physical, but healing that results in emotional, mental, physical, and spiritual connection and wholeness must not be minimized.
We have grown more and more dependent on outside sources for self-management and symptom resolution and less and less able to recognize innate abilities to deal with our discomforts and health needs. As such, technology has done both the provider and the client as a consumer a disservice.
The disservice to the clinician is to encourage taking on excessive responsibility as the source and solution of clients’ problems. The disservice is to both client and provider in promoting the idea that another person or a drug is the solution for every discomfort, pain, and problem and that healing equals restoration. Healing can occur incrementally at any time during the rehabilitative process and can involve much more than physical healing.192 Restoration can involve perceptions and expectations of previous abilities, pain relief, and conditions, realistic or not.
There is an expression that “pain is inevitable, but misery is optional.” There appears to be a prevalent belief in society today that there should be no discomfort in life, whether sensory, emotional, or exertional. This belief and current marketing strategies entice people to quickly turn to medications or outside care for uncomfortable feelings, such as grief, and even minor discomforts and pain.
Pain has been defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.168 The nature of the person’s suffering and the psychologic response to the physical or emotional experience is more clinically relevant than the physical pain.102
Ponder this quote: “Culture makes pain tolerable by interpreting its necessity; only pain perceived as curable is intolerable.”113 Belief systems have a potent effect on medical care and client status. Studies have shown that people receiving noxious stimulus and those believing under hypnosis that they are experiencing pain demonstrated the same brain activity of pain perception.
Functional brain imaging and related studies endorse the notion that pain is one-part nociception and three-parts anxiety. Pain is not a thing that can be tangibly identified, pharmaceutically eradicated, or surgically removed. Pain must be addressed at the source contributors, and the clinician is challenged to deal with seen and unseen components.102
Contributors to chronic pain are vast and varied. A recent trend discovered in research of low back pain (LBP) shows that predictors of outcome for LBP treatment are not the presence of degenerative disk disease, herniation, annular rupture, or endplate changes but rather baseline psychosocial variables that strongly predict both long-and short-term disability events, duration, and health care visits.85,208,252
Chronic pain and behavior studies have indicated that the presence of an enabling spouse, not physical pathology, confirms high psychosocial risk and probability that the person will be worse in 5 years.230
The Meaning or Purpose of Suffering
Insight and direction for comprehensive care are gained by listening to and learning from clients about their beliefs of the meaning of their suffering and how those beliefs and messages show up in their lives.
Finding meaning in the midst of suffering may be the most important element in the healing journey.192 Researchers are beginning to examine why some people are broken down by traumatic events, whereas others are broken open. New insights into brain science and genetics, as well as the power of spiritual practice, are being reported.
An individual’s healing and coping potential comes with volitional choice before the “pain with a purpose” event or as the individual comes to terms with the experience, finding meaning or an expanded means of coping through the experience. For example, pain with purpose can help women fight fear and tension and cope more effectively during labor and delivery. Motivation to go through elective surgery and the postoperative pain and effort of rehabilitation comes from acceptance of pain with a purpose. As with athletic conditioning and training, discomfort and healthy suffering can push us out of passivity and apathy into new levels of strength and skill. Healthy suffering does not cause damage but rather motivates us to connect, ask for help, attend to our needs, and empathize with others, and stretches us to grow and develop.
Acute pain serves as a warning system and carries the expectation of resolution. Chronic pain is less well-defined in mechanism and contribution, provides no biological benefit, and by definition, does not resolve. Chronic pain has been shown to dramatically affect neuroanatomy and physiology. Noxious stimuli to dorsal horn neurons cause substance P and glutamate to produce cellular changes, which can enhance pain transmission to the brain.
Prolonged sensitization has been termed memories of pain and kindling. This change in neural excitability eventually requires no external stimuli to be self-perpetuating, becomes internally reinforced, and exacerbates clinical symptoms.
In addition to sustaining cellular changes in the spinal cord, individuals with chronic pain have a more complex brain response to pain experiences than people without chronic pain histories. Studies have shown that mild discomfort or pain experienced by a control population along with those suffering chronic LBP and fibromyalgia activates the secondary somatosensory cortex in all recipients.87 This secondary sensory cortex is not specific for type of pain or area affected but registers general sensation such as touch, pressure, and pain. This was the extent of the brain activity response in the control population studied. In the fibromyalgia and chronic LBP populations, activity was also registered in the ipsilateral primary somatosensory cortex and the contralateral occipital lobe.87
Reliance on Pharmacology
When we scrutinize advertisements on television, we see that the vast number of medications sold are for prophylactic care and minor discomforts. Marketing of pharmaceuticals (both over-the-counter [OTC] and prescription drugs) has a fear-based approach for something that should be optional for many people.
Often the list of potential side effects of medications is equal to or more severe than the problems they claim to relieve. The public is generally willing to put themselves at higher risk to achieve relief for an immediate though minor real or perceived problem.
The broad range of medications available today can appear to be cure-alls to eradicate every discomfort of life. The use of medication by both the medical community and society has changed from the “safety for mother and child” priority to a fear-based priority of pain avoidance in the immediate experience. The perception of medical care and medication has transitioned from support of inherent coping and healing abilities to replacement of innate personal potential.
Before the plethora of medications for every imaginable complaint was available, people were compelled to take time to rest and find respite with family and/or in community. Concerns and symptoms were dealt with as events rather than as long-term conditions. A sneeze was immediately seen as a reason to blow your nose, not as an allergic reaction and permanent limitation.
The faulty perceptions that “life should not have any pain or discomfort” and “a pill will solve my problems” encourage fear-based, quick-fix thinking and damage the concept of self-management and the related stress management skills that would otherwise be cultivated as our first line of defense.
Coping As a Lost Art
Reliance on external sources to identify personal condition and prognosis diminishes self-awareness and discernment, exacerbating the sequelae of real and perceived overwhelming events. Dissociation and other survival coping mechanisms increase the inability to connect with self, both physically and emotionally. This external reliance and internal distancing promotes isolation. In the absence of healthy self-awareness and personal coping skills, isolation is fertile ground for proliferating fear, confusion, and overwhelming stress.
As technologic dependence grows and awareness of inherent human healing and coping capabilities diminish, people are increasingly vulnerable to accepting without challenge a diagnosis and thus the belief that their condition is essentially a “life sentence.”
Technologic advances also foster “instant gratification” and the myopic focus on the immediate discomfort instead of the full healing process. The mounting sense that “I can get what I need instantly from some source, without going through a process” reinforces barriers to healing and cultivates mental confusion for both the individual seeking health care and the provider.
TERMINOLOGY
Along with other professions, the health care profession, including physical therapists, struggles with the use of consistent terminology. Clinicians in each specialty develop intrinsic terminology to portray personal insights. Those terms can be confusing outside of that specialty and sometimes even to peers within the profession.
The best approach in communicating concepts and findings clearly and accurately may be to describe the most basic nature and principle(s) involved. Specific technical jargon can be replaced with straightforward, foundational concepts and widely understood vocabulary. Whether written or verbal, it is always wise to clarify information by reflecting back, in simple language, what you heard or observed and follow up with a written record.
Dangers in developing and applying new terminology include the possibility that definitions may be skewed and vary between specialties or professions or that the terminology becomes a unique “code” for one profession and fails the purposes for which it was developed.
Contained within this chapter are such descriptive and measurement methodologies. To avert dangers and maximize benefits, definitions are included (Box 3-1). In this section, the definition of trauma will be an overwhelming or life-threatening event—experienced or witnessed—resulting in intense fear, helplessness, and horror, with sequelae that will persist until attended and resolved.
Though torture was previously known as a method of punishment or interrogation, we now know that its main purpose is to destroy a person’s identity. Torture is used to cultivate fear and terror. It can be used as a weapon against personal safety, belief systems, and democratic principles.
The use of the words “supposed” and “alleged” in the context of child abuse is a misnomer. Professionals who work with survivors of ritual abuse verify that no person would make up or choose to live the life of a systematically and repeatedly abused child.
Even names given to mental health disorders can be misleading. For example, the concept of dissociation is defined as a detachment of the mind from the emotional state or body. But this condition can be as mild and fleeting as daydreaming as you drive to work, or it can be so severe that the personality is shattered into adaptive “parts” or “alters.”
Dissociation may be accompanied by a void or poor memory of the specific events, which in its severe form is known as dissociative amnesia. Survivors with dissociative identity disorder (DID), previously described as multiple personality disorder, have periods of hours and days that are not remembered, causing the survivor-patient to “wake up” in strange places, alone, and disoriented as to time and place.
EFFECTS OF TRAUMA ON BRAIN DEVELOPMENT
Worry, fear of the unknown, and other anxieties are normal as transient occurrences in life, resolving through the support of caring people who will listen, offer reassurance, point out options for dealing with the event, and provide empathetic support as time passes.214
In the presence of danger, fear is helpful for the purpose of initiating an appropriate short-term survival response referred to as fight, flight, or freeze. Anxiety, or the fear of potential threat but in the absence of real danger, is not helpful. Animal studies confirm that in repeated experiences of overwhelming trauma, freezing becomes the default coping mechanism, even when other options for escape or defense are available. Dissociation is a major component of the freeze response.205
A-Type and B-Type Trauma
Everyone has some trauma, some wound that needs attention. It is not realistic to believe that one can go through life without some pain or wound physically (body), emotionally (heart), or mentally (mind) or without some crisis in faith/belief system (spirit). As such, everyone will benefit from health care providers who attend to their own harbored hurts and practice healthy, sensitive communication that meets the needs of clients suffering the most severe and complex trauma.
It is valuable to recognize two major types of trauma that affect all people including health care providers and clients. In the mid1990s, Lenore Terr, MD, a well-known clinical professor of psychiatry at the University of California San Francisco School of Medicine, introduced the concept of type I and type II trauma that distinguished between single event and multiple occurrence traumas.228
Since that time, the terms type A and type B trauma have been used for what is ordinarily called neglect and abuse.254 Type A trauma results from the absence of good and necessary elements for health and well-being, such as the nurturing by and healthy bonding with parents. Type A traumas most often affect the emotions and are sometimes referred to as “heart breaking.” Physiologically, type A traumas target the limbic and related areas of the brain where strong emotions are processed and stored. Type A traumas will present as painful feelings emerging when the wounded person sees or experiences the good that was absent in his or her own development.
Type B traumas are the things that happen in life that are viewed as “bad” or negative events. Dissociative coping mechanisms and barriers or distortions to memory are more the results of type B traumas. The harbored, unresolved hurts, feelings, and beliefs from type B trauma affect the right orbital prefrontal cortex (ROPC) directly, promoting sympathetic system stimulation and hindering growth of the ROPC and the ability to receive or express joy. After age 3, amnesia (dissociation) is the brain’s coping mechanism for overwhelming, life-threatening trauma.
Both type A and type B traumas increase the individual’s conscious and unconscious need for self-protection, activating the sympathetic system and escalating adrenal activity. A self-perpetuation cycle of mixed messages (the inability of the brain’s two hemispheres to make sense of and resolve the cognitive message and sensory input) results in a persistent sense of helplessness. The unreconciled input causes elevated, sustained cortisol levels, expressed physically as somatic and psychologically as emotional representations of the ongoing internal, mental conflict.
Severe trauma shatters the sense of self, confounding identity and destroying the concept of personal boundaries. Childhood trauma disrupts the course of normal development and perpetuates brain dysregulation, which presents as internal disconnection between the somatic (physical), emotional, and mental “self.”
The person has no or limited self-awareness and is unable to recognize physical status and need. Without comprehensive training and healing, healthy stress management is unknown and regulating physiologic and emotional change or intensity is impossible. Necessary survival, low pain tolerance, and pain-avoidance coping patterns block the person’s ability to hear what his or her body is saying and needing.
Stress Reactions
Data addressing early life stress in humans parallel findings from animal studies. For children, exposure to frequent family conflict and aggression disrupts functioning of the immune system, as well as hormonal systems governing the stress response. Young children who experience abuse or neglect show abnormal cortisol levels, indicative of a dysregulated stress response. These changes often remain after the child has been removed to a safe, caring environment and are persistent in individuals who show clinical or subclinical symptoms of PTSD.93
There is also a negative impact on the brain and sympathetic nervous system as a result of the long-term effects of living in a constant state of anxiety and survival mode. Persistent fear and sense of being unsafe (perceived or real) has devastating effects on every aspect of health. Persistent, long-term cortisol release without resolution is closely related to physical pain and symptoms, excessive fatigue, tension, immune system ineffectiveness, and negative effects on the anatomy and function of the brain.
Brain imaging studies confirm the relationship of chronic pain and brain morphology. Changes in neuroanatomy and neurophysiology include atrophy of the ROPC and destruction of serotonin receptors, secondary to trauma and the resulting sequelae.254,255
Chronic pain results in distinct patterns of cortical degeneration. For example, neocortical gray matter in the somatosensory areas of the brain is lost at the rate of 1.3 cm3 per year in cases of chronic LBP (CLBP). This is a 5% to 11% loss, or the equivalent of gray matter that could be lost normally over 10 to 20 years.102
The most vital fact to remember and convey to clients is that the brain is resilient and has great potential for healing. Most stress and trauma-related pathology can be improved and corrected and affected areas of the brain can heal.
Developmental Deficits and Sequelae
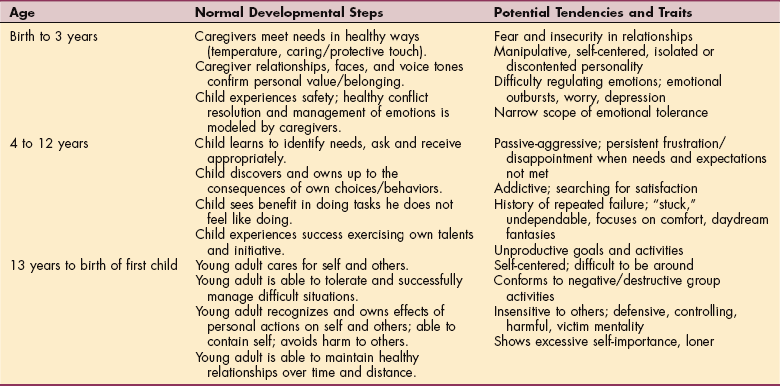
It has been said, “Trauma is an obstacle in normal human development.”201 Developmental trauma initially manifests less as physical pathology and more as emotional, mental, and relational pathology. Physical pain and problems develop from the long-term stresses and continuing sequelae of developmental trauma. Consistent character traits and functional difficulties can be traced from deficits in early development. Major deficits in any of the normal developmental steps can lead to the unhealthy tendencies and traits listed in Table 3-1.
Energy Demand and Trauma Condition Color Codes266
In the early 1990s, the military and police forces used a method of quantifying and describing states of mental awareness developed by Marine Colonel Jeff Cooper. A descriptive method of clarifying status, intensity, and characteristics of trauma severity and energy demand is useful in educating clients and coordinating with other professionals. The color system presented here has been modified from the original model to identify, quantify, and describe energy expenditure and severity of trauma (Box 3-2).117,161,245
Yellow
The client or provider is healthy enough to accurately monitor internal and external condition and status and rapidly adapt, shutting down unnecessary tension, reactions, and energy use in favor of a more appropriate, calm, relaxed, timely response.
The client/provider functions in a state of relaxed well-being and safety with appropriate environmental awareness and readiness, translating smoothly and efficiently to and from lower energy states to higher energy demand. This desired energy demand for normal living is characterized by peace; effective and focused purpose; orderly proficiency; unity of heart, mind, body, and spirit; joy; and sufficient energy in the presence of a chaotic, hurtful, demanding world.
In a world of fear, pain, problems, and limitation, energy demand and trauma condition specified by yellow often seems unattainable, even frightening. Early on, the healing journey depends on trust and observing others successfully exercising healthy stress management skills.
Whatever level of trauma experienced—everyday life or the incomprehensible horrors of repeated torture—every person needs healing and healthy preparation, training, and practice to live in this energy state.
Red
The red color code would correspond to those survivors of trauma who cannot differentiate past threat from current safety, who overreact to normal events in activities of daily living (ADLs), and who live in constant distrust and defensiveness, with all the related physical, emotional, and mental stresses. The red level of energy demand parallels the effort of holding a weight overhead without rest.
Black
Because of the extreme demand on all systems, the black trauma condition cannot last long and will transform one of two ways. The individual at the black level of energy demand and trauma condition may be restored to lower energy and trauma levels as the person gains control, safety increases, and resolution of the event occurs. Otherwise, this state will progress to a white-out level as the person reaches the limits of personal coping abilities and experiences real and perceived loss of control and total helplessness and is completely overwhelmed.
White-Out
In the white-out condition, adrenaline concentration is high, but the person can feel remarkably calm. Retention of the event in procedural memory may rekindle arousal patterns and reactions causing perpetuation of physical, emotional, and mental PTSD symptoms.
Normal, nonthreatening ADLs, especially visits to medical offices and medical procedures, can “trigger” this conditioned freeze/dissociation reaction in the survivor and predisposes the individual to chronic pain, comorbidity, and stress-related diseases.205
In this trauma condition, high levels of endorphins serve as analgesic, allowing the victim to feel numb in the presence of noxious stimuli. Posttraumatic symptoms from an overwhelming event, with accompanying neurologic suppression, can persist for years, prompted by normally meaningless, everyday reminders of the unresolved trauma. Until the person is able to complete the escape or defense process, areas of the brain retaining the survival experience may perceive the threat as ongoing instead of dispatching the event to past experience.205
Many physical, mental, and emotional pain and behavioral problems are common to abuse, trauma, and torture survivors. Although psychologic sequelae are frequently the focus of posttrauma or posttorture experiences, survivors often see their problems as primarily somatic.191 Because of dissociation, amnesia, and survival reactions at the time of trauma, the person may not have any conscious awareness of the abuse and trauma history until adulthood. Clinicians need to know common physical (and related) sequelae of abuse, trauma, and torture to avoid overlooking critical indicators of pathology and to recognize subtle, unidentified contributors of previously failed treatment or comorbidity. Offering the person hope and effective care directed at complete healing promotes clinical and professional credibility and client satisfaction.
Signs of Unresolved Trauma
Many symptoms of trauma are considered “normal” if they are mild and fleeting, but when they interfere with daily living and/or become extreme or persist, then seen and unseen contributors need to be considered. People suffering from unresolved trauma work to cover their severe distrust of people and unfamiliar environments. Safety, real or perceived, is foreign and unidentifiable because of the mixed messages rooted in the abuse. Circumstances of life that remind the wounded person of past trauma through sensation or “meaning” will trigger survival reactions established by the overwhelming events.205
Default coping strategies will surface repeatedly and reinforce the physical, emotional, and mental survival reactions as if past trauma was occurring in the present. This often presents as “freeze” reactions accompanied by shallow breathing or breath holding. Dissociative changes are very subtle, allowing the survivor to conceal tremen- dous turmoil internally and appear normal externally. Practiced observation, attentive listening, and appropriate questions help the clinician to grasp subtle changes that indicate client status.
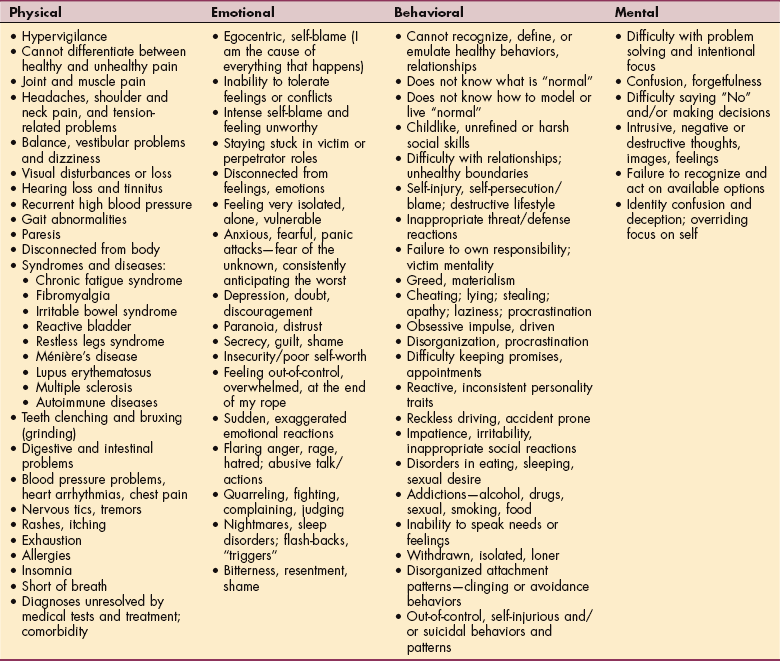
The most common signs and symptoms of unseen wounds are listed in Table 3-2; this list is not exhaustive since there may be other symptoms experienced by some people. The reader may ask, “Why is a list like this, which covers so many common maladies, valuable?” It is important for every health care provider to be aware that deep emotional, physical, and mental maladies can present as common symptoms and contribute to comorbid diagnoses, causing confusion for both the client and the provider.
The astute provider can look beyond the superficial and obvious symptoms to consider the contribution of all systems and underlying pathology. Pain and many other common symptoms are not caused by a single source or element but rather result from complex combinations of experiences, expectations, and perceptions.102 Such awareness allows the clinician to recognize telltale signs of deeper ailments that would otherwise be overlooked or exacerbated.
The effects of past trauma can be expressed physically or emotionally and are often set off by normal daily events, especially medical treatment. Sound, smell, taste, sight, touch, and position or movement similar to the original trauma can elicit physical or emotional reactions, apparently unrelated to the current treatment focus or context. Because these physical or emotional “tags” are apparently unrelated to the current circumstances, the therapist may not know of these reactions unless the affected individual reports them.102,266 Some examples of this phenomenon include the following:
• The client does not progress and has trouble complying with his or her independent self-care program because of past experiences of being victimized and helpless in medical or similar environments.
• The client is not progressing because of a deep-seated belief that anything that causes discomfort is harmful and “healthy” means no pain or discomfort—some level of this belief is pervasive in today’s pregnant populations and labor/delivery settings.
• The client is resistant to treatment and a self-care program because of the belief that somewhere there is a physician, surgery, or drug that will immediately resolve all their problems without work or pain.
• Treatment or touch to a client’s upper back (man or woman) results in reports of thoracic or paraspinal spasms, stabbing or electric-like sensations, pelvic or genital sensations, or sudden fear and the need to protect himself or herself.
• The client perceives that secondary gain from pain, symptoms, and disability is his or her only hope for the future.
These scenarios are common but often remain unnoticed by the provider because of the rushed, sporadic, and superficial contact between client and provider. The provider cannot identify foundational hindrances and barriers to treatment and healing unless time and careful listening are invested, establishing a relationship and drawing out the client’s conscious and unconscious beliefs.
People will not divulge confusing or embarrassing ideas and reactions unless the provider has demonstrated sincere caring and has established an environment of personal safety and trust. At the appropriate time, the client needs to understand that sharing these apparently unrelated reactions is important to successful intervention because thoughts, feelings, and sensations reveal factors contributing to the symptoms and system interplay.
The therapist who knows what to look for and pays close attention to the tension, breathing, and freeze patterns in their clients during positioning and hands-on activities can also glean hints of deeper trauma. Encouraging clients to identify and exercise options and choices and report what they are thinking and feeling can be very helpful.266
BRAIN FUNCTION: A REVIEW OF ORGANIZATION AND HEALING POTENTIAL
When working with patients/clients (or anyone, for that matter), it is important to remember that the message with the most impact is developmentally based. While you, the health care provider, are communicating left hemisphere to left hemisphere with your client, your client’s brain is simultaneously processing a more powerful message. The concept revealed in the following long-circulating saying is worth remembering:
I know you believe you understand what you think I said, but I am not sure you realize that what you heard is not what I meant.
In patient care, the medical community has drifted toward relying more and more on advanced technology to test and diagnose, giving less and less time to listening and making a personal connection with the individual. These trends render the client more dependent on the caregiver, less equipped to deal with his or her condition(s), and less personally invested in the treatment outcome. This inclination is detrimental to and opposes the healing potential of the individual.
Right Hemisphere Communication
As a review, remember that during every interpersonal contact, both hemispheres of each person’s brain are communicating concurrently but differently. While the left hemisphere controls linguistic communication and analytical interpretation, the right hemisphere is responsible for more broad-scope communications (Box 3-3).
Maturation of the right brain in infancy is equated with the early development of self (brain-mind-body). The right hemisphere of the brain, more than the left, develops vast connections with the emotion-processing limbic areas of the brain. The limbic system is a powerful influence on behavior. Right hemisphere-to-right hemisphere communication relays the dominant message when receiving, expressing, and communicating emotional states.209,211
Right hemisphere-to-right hemisphere communication is nonverbal, touching the emotions and the deepest parts of the human heart, mind, spirit, and body. Both brain hemispheres work together to seek and verify consistency and accuracy of information and stimulus. Traumatic experiences interrupt brain function and precipitate conflicting interpretation of sensory and cognitive input.
Facial expressions and tone of voice are subconsciously dictated from past experiences, deep emotions, and base perceptions of the sender. These nonverbal messages are expressed by the right hemisphere of the sender’s brain. They are received subconsciously by the right hemisphere of the receiver’s brain. The receiver’s brain generates a somatosensory, physical representation of how the sender is perceived to be feeling during the interaction and the related “message” or meaning to the receiver.210
Observing the posture of people around us, we can notice the emotional messages presented in the physical bodies such as depression, joy, frustration, contentment, insecurity, confidence, and fear or peace. Whatever the words, the true emotions are stored physically. No matter what words or ideas are verbalized, the strongest, most lasting messages received will be the nonverbal, sensory messages.
The right hemisphere of the brain is also responsible for processing stress and negative emotions and for learning error compensation from the negative experience. People living in chaos, especially those growing up in the midst of chaos and mixed messages, have a much lower tolerance to stressful and real or perceived negative stimulus.
Adaptation to complex, conflicting sensory input is managed in the right hemisphere of the brain, whether negative, nonverbal communication or noxious stimuli. The inability to resolve stressful or incongruous messages and sensory input is accompanied by changes in brain morphology. Recall for example that in the presence of chronic pain, neocortical gray matter is lost at the rate of 1.3 cm3 per year, targeting the right thalamus and dorsolateral prefrontal cortex.102
Potential for Brain Healing
Brain healing occurs when consistent messages are confirmed by both hemispheres, according to the individual’s ability to receive and tolerate healthy reality. This consistency in message is unfamiliar and initially uncomfortable to the person who has lived with mixed messages and emotional, mental, and spiritual wounds.
The clinician must be in touch with, able to successfully process, and model healthy responses to his or her own pain to tolerate the client’s painful experiences and pain reactions. Both therapist and client need to understand that stress can build up, as well as break down, a person and that some uncertainty and discomfort is foundational to a healthy growth and healing process.209
Healing begins with a provider who understands that the ability to tolerate disruption and uncertainty is fundamental to life, health, and growth and who is comfortably able to assist and mentor the individual in exploring that truth during treatment.266
The Development of Joy
We are relational beings. From birth and throughout life, connection with other people or lack thereof impacts every aspect of our health, perspective, and function. Just as neglect and abuse interfere with normal development, nurture and relational joy promote healthy growth and development and a secure, resilient identity.
Joy has been identified as a necessity for human development. You can relate to and remember the effects of joy on your emotions, body, mind, and spirit if you think back to your first “puppy love” experience. That ethereal, consuming feeling of ecstasy is the result of growth in your brain’s ROPC.
The Right Orbital Prefrontal Cortex
The ROPC of the human brain develops between birth and 18 months of age. How much and how fast this area grows depends directly on the nature and quality of stimulation this area receives through interaction with the more mature, caregiver brain. Growth in a person’s ROPC and this feeling of joy are generated by someone communicating, right hemisphere-to-right hemisphere, that they are glad to see you and be with you and that you are accepted and valued for who you are. The sensation and message of joy is the only positive motivation for a child under 12 months old.254,255
The feeling of joy that comes from eye contact, voice tone, and touch that says, “I care for you” is the only experience a child less than 1 year old will seek out. Joy can be defined as the delight of varying intensity that one feels when receiving the right hemisphere messages of “I am glad to see you, I am pleased to be with you and you are valued.” Brain scans confirm that the ROPC grows in response to joy, targeting the left eye.209-211,254,255 For clarity, “joy” is differentiated from “happiness” in that joy is relational and results in positive growth and health beyond circumstances. Happiness can be manipulated and governed by circumstances and by the person’s will.
From childhood, humans will mirror what they receive nonverbally. Interpersonal communication paths are active simultaneously on two levels. Verbal language and cognitive interpretation of the content occur from the sender’s left hemisphere to the recipient’s left hemisphere.
The child will mirror what he or she receives nonverbally from interaction with older children and adults. The child will empathize with the emotions of the more mature being, even to mimicking the mentor’s brain chemistry. The child’s brain will grow according to what is received from exposure to the more mature models.209-211
The attitude and emotions of the sender, conveyed nonverbally, carry the deepest and most lasting message to the receiver. The more healthy and mature a person is, the better able he or she is to accurately understand left and right hemisphere communications and resolve conflicting verbal and nonverbal messages while retaining a solid and consistent self-perception and response stability.209,210,254,255
At the same time, the tone of voice and facial expression are communicating much faster than the verbal communication. Subconscious messages from facial expressions occur as fast as 40 ms or the time it takes for one brain cell to fire. The complete cycle of sent and received nonverbal messages occurs at 6 times per second, right hemisphere to and from right hemisphere.209-211,254,255
Development of the ROPC
Although some growth of the ROPC will occur with even minimal joy experiences, the most favorable growth and healing of the ROPC occurs during frequent and consistent experiences of joy such as genuine smiles back and forth. ROPC function is enhanced when the right hemisphere messages are in agreement with the verbal left hemisphere content and when there is synchrony of communication. In the absence of “joy” stimulation, the ROPC will atrophy and the full growth and potential will not be reached.
Healthy right hemisphere communication between people builds the ROPC areas of both brains. Angry or depressed adult brains will breed angry or depressed child brains, which will also simulate the brain morphology and chemistry of the adult model. Through right hemisphere synchrony, the more immature person will feel what the adult is feeling and communicating nonverbally.
Brain imaging of persons surviving persistent relational trauma, abuse, or neglect will demonstrate major deficits in the number of cells and the size of the ROPC in their brains. These deficits in gray matter are evident in persons with diagnoses such as the following:
• Attention deficit disorder/attention deficit hyperactivity disorder (ADD/ADHD) (which also shows up in many children raised in day care from early ages)209
Research confirms normal growth spurts of the ROPC between birth and 18 months of age, with peaks at 3 months and 9 months of age, between 3 and 5 years of age with the peak at 4 years of age, between 7 and 10 years of age, at 15 years of age, and at the birth of the first child, especially for the mother.209
Biochemical changes during pregnancy prepare the mother’s brain for ROPC growth. The last identified growth spurt of the ROPC occurs at the birth of the first grandchild.209-211 Throughout life, the ROPC retains its ability to grow, and thus its ability to heal, to the same extent as from infancy. ROPC deficits can be restored in persons suffering previous developmental or trauma losses.210,211,254,255
Rope Analogy of Dissociation and Brain Healing266
The purpose of understanding how the brain functions, of knowing about the simultaneous communications of the right and left hemispheres, and the nature of seen and unseen wounds is to be equipped and proficient in serving the most involved of our patients/clients. If the provider is equipped to attend to the most complex and needy individuals, that provider will be better able to comprehensively and effectively serve each person coming for care.
Dissociation
The human survival response to events that threaten existence or that are overwhelming and surpass the individual’s ability to cope is called dissociation. Dissociation is a response to the deepest trauma experienced by humans. Dissociation is the survival mechanism that splits the brain’s left and right hemisphere functions to allow the survivor to store the event, the feelings, and the perceptions unconsciously until the survivor is able to bring the trauma into conscious resolution through right and left hemisphere processing.
But living in the shadow of chronically unresolved trauma and depending constantly on coping systems designed as temporary, short-term defenses for survival take a toll on the survivor—physically, emotionally, mentally, and spiritually. Individuals who use dissociation as a coping mechanism are most often unaware of their fractured state until the coping mechanisms begin to break down and functioning becomes increasingly difficult.
The most severe dissociative pathology results from repetitive childhood trauma and abuse, as in ritual or sexual abuse. The earlier the trauma occurs and the longer the trauma persists, the more severe the sequelae. Specific adaptive “parts” or “alters” emerge to cope with real or perceived threats and unfamiliar circumstances.
Often, when the survivor-patient feels safe enough to risk revealing the conflicts within, “alters” will present verbally or behaviorally as a child of the same age-range as the survivor-patient was when the trauma occurred. The less safety and personal success a survivor-patient remembers experiencing in life, the more severe and complex the dissociative sequelae.
Some people are conscious and aware of their parts, whereas others are unaware of specific “alters” who emerge to deal with perceived threats or stressful events. Individuals who are unaware of their dissociative condition may experience “memory blackouts” when the specific parts are functioning. They may “wake up” in an unfamiliar or even familiar place, not knowing the time or how much time had passed, who has been encountered, or what has happened.
Survivors generally have trouble conceiving what it means to be and function as an integrated whole, beyond the survival coping of their functional parts. Dissociative people see life, self, and others through confusion, fear, insecurity, and helplessness. They are very sensitive to right brain communications and to loss of control.
Since “alters” or “parts” are hidden from the primary presenting personality, the illustration of a rope can depict the fracturing, as well as the healing, of self. Using the colored threads that make up the whole rope, dissociative status, function, and healing can be described and quantified.
Rope Analogy
Portraying psychosocial conditions accurately can be difficult. A rope analogy can be used to help the provider and the client assess the complexity and severity of psychosocial wounds that will affect medical care—for yourself, as the provider, and in your clients.
It is helpful for clinicians and clients to understand what contributes to dissociation and how healing occurs, since healing the physical contributors will be virtually impossible without first addressing the nonphysical contributors to pathology. It is necessary to find an analogy that depicts internal shattering into “parts” or “alters,” unique in personality and function, while still retaining the image of and potential for wholeness. The rope analogy fits all necessary criteria (Fig. 3-1).
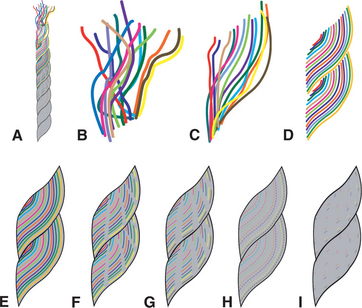
Figure 3-1 Rope analogy to demonstrate how dissociation, function, and healing can be described and quantified. A, Rope shown as a progression from fractured, dissociative, and surviving (top) to functional health—whole, integrated, and thriving (bottom). B, Frayed rope depicts the fractured, wounded condition of the individual existing in “parts” or “alters” used as a coping mechanism before healing. Colored threads represent hidden parts or alters that emerge as needed. In the initial phase, survival coping mechanisms break down and the person recognizes growing physical, emotional, and relational problems, motivating them to seek healing. C, Recognizing options for improvement. As the individual recognizes options for improvement, he or she begins to feel some hope and empowerment. D, Weighing the costs/benefits. Although the healing is challenging and healthy habits are new, the person experiences improved function and order as negative reactions are replaced with positive responses. E, Healing challenges. Difficult healing challenges provide vital opportunities to model and practice problem-solving and stress management skills. F, Healing victories. As the individual experiences the efficiency and success of system healing and integration, difficulties are outweighed by victories. G, System integration. This is a time of personal exploration and rejecting “surviving” habits to practice “thriving” skills. H, Early final phase. The client prepares for independence from the mentor/provider with a new, more tangible sense of identity, discovering how to take ownership of his or her life, choices, and actions. I, Final phase. The client moves into independence with healthy relationships and connection to others—not dependent and not isolated but able to appropriately give and receive (i.e., autonomous). (Courtesy Bonnie Yost. Used with permission.)
Picture of Wholeness and Full Function.: Just as there are many types of people, there are many types of ropes: some for roping cattle or stock, some for climbing mountains and rappelling, some for practice in school, some for securing cargo, some for communicating with and leading a horse, and so on. For the purpose of visually describing health and wholeness before catastrophic events that cause dissociation, we will use a soft, thick lead rope. This lead rope is strong enough, when needed, to protect a horse from hurting himself and softly pliable enough to communicate gently and be a source of trust for the horse.
This rope has hundreds of strands, each a different color, but at first glance, the rope appears to be a uniform gray with hints of color (Fig. 3-1, A). Intact and whole, all strands of the rope are united in place and function to make up the integrated whole. Each strand is unique and vital to the strength and function of the whole. If any of the strands are broken or missing, the rope may not be able to endure the limits of tolerance for which it was designed (Fig. 3-1, B). With internal pathology, the rope will break when challenged by an explosive, powerful pull on the rope. Internal faults cause damage to the whole when, under otherwise healthy conditions, the rope would successfully tolerate these stresses.
If a horse was tethered with one or a few strands, the horse may be able to receive communication accurately if the handler was very skilled and attentive and if the horse was very focused on the handler and even the smallest changes in pressure. The single or few strands would be able to function as the rope in a very limited manner, without the challenge of normal stresses for the rope as a whole.
When a person is internally split by overwhelming events, it is as if the whole begins to unravel and each colored strand disappears or stands out against the background “color” of the prevailing situation. This survival mechanism is vital for the survival of the person when taken beyond their limits of tolerance, but this fractured lifestyle is extremely energy-intensive and inefficient. Sometime during adulthood, this coping mechanism breaks down and the dissociative person becomes aware of missing time and elements in his or her life.
Any “red” event that triggers anger or rage in the person might bring out a “white,” self-destructive part or a “blue,” depressed alter to deal with the event, while the “red” rage part will disappear because of the overwhelming memory, meaning, and pain of the original trauma. The feelings, memories, and meanings must be contained and repressed until the person is appropriately supported and strong enough to face the condition and learn healthy coping strategies. Living day and night in a high adrenaline state causes hypervigilance and exhaustion, and invites a plethora of physical, emotional, and mental symptoms and comorbid diagnoses.
Phases of Healing
With normal living and time away from the trauma, the survival coping mechanisms begin to break down, not only because they are no longer needed but also because of the extreme demand on all systems and the functional limitations of dissociation.
Phase 1: Recognizing the Need for Healing: (see Fig. 3-1, B). The initial phase of healing deep trauma is the recognition that there are other options and the concomitant desire for improvement. The goal of this phase is to help the individual learn how safety feels and looks and to receive care and health that require safety and trust without resorting to habitual survival-coping mechanisms. In this phase, the person begins to see his or her life patterns and to identify destructive thoughts, negative messages, and unnecessary limitations. The individual will begin to recognize and reveal established survival habits and the effects of those old reactions on relationships and daily function. Exhausting internal conflicts become clearer and less functional.
The person will most likely experience feelings of fear. Fear of the unknown, of what may be revealed to self and others, of people, and of what “healing” means can generate feelings of panic, shame, guilt, and hopelessness that may interfere with keeping appointments and the most timely results of treatment.
Sensitive care will help the dissociative, internally shattered person break down the barriers between right hemisphere emotions and perceptions and left hemisphere verbal descriptions and comprehension. Again, this can be a very frightening and confusing time for the individual.
The client may become antagonistic and the connection can be difficult for both the clinician and client, as the client tests acceptance and trustworthiness in this new relationship. In pushing away those who can and want to help, the affected individual is also testing believed and lived lies such as, “No one cares. You are not worth caring about. You are hopeless. There is no way out of this way of life and you cannot improve.”
With patient persistence, both the client and the clinician can disprove these barrier beliefs and open the way to healing. Unwavering, effective nonverbal communication and quiet acceptance of the person in all conditions and emotions, in the presence of healthy, caring, well-established boundaries for the benefit of both, are crucial during this phase of healing.
Phase 2: Recognizing Options for Improvement: (Fig. 3-1, C). In this phase of healing, the client has experienced victory by recognizing that there is help and healing available. The client has experienced some personal control, safety, and respect from others. The client begins to understand how to state needs, ask for help, and see that it is possible to receive without resorting to high-energy survival coping strategies.
The individual’s scope of self-awareness and assertiveness is growing through questioning past beliefs and behaviors and carefully observing those who live out desirable healthy habits that are contrary to the client’s familiar belief and survival habits.
The various parts of the individual are beginning to recognize the various aspects of self and the assigned duties of each survival alter-role. Testing of reality and safety continues in this phase as the person explores healthy, sincere interaction in stark contrast to previous manipulative, abusive, and unsafe involvement.
As the reality of safety grows, the individual risks replacing the escape-focused dissociative tendencies with staying in the present. This step of trust carries the risk of feeling, which can be very frightening for the individual. Past abandonment and betrayal make the person very fragile and hypervigilant.
Previously unknown “alters” and coping mechanisms come to light and more conditioned reactions are revealed. Alters designated for specific functions are identified and the individual begins to grow in internal and external awareness. The person begins to see the various “parts” and their survival-related functions.
The benefits of healthy change and functional harmony are considered. Internally, the conflicting messages and “alter” personality opposition may heighten before it begins to decrease. Learning to trust and receive without fear of repercussion takes time and practice.
Phase 3: Weighing the Cost/Benefits: (Fig. 3-1, D). This phase of healing is challenging because the client sees the healing work ahead and can be overwhelmed. Questions such as, “How long will this take?” and “Must I relive my past abuse or pain?” are common. The clinician’s truthful, open answers are most valuable. The provider’s answer of, “Our work together will touch your pain and deep feelings, but we will strive to avoid retraumatizing you” reinforces the client’s protection and support in the healing process.
“Your healing will take as long as it needs to take, depending on the severity of your condition and how able you are to move through each step of healing” is an accurate answer that helps break an overwhelming process down into manageable steps. Letting the person know that they will not need to walk their healing journey alone, that you and other caregivers will be with them—be specific and name those who are supporting their personal healing—brings deeply needed comfort and hope to the individual.
During this phase, the client will have enough experiences that are different from past trauma that the potential of healing is appealing. Internal parts become more cognizant of each other and more cooperative as the efficiency and strength of unity are revealed. The idea of wholeness and healthy and “normal” interaction is enticing and sought.
Probably the greatest challenge to this healing phase is commitment. Fear of the unknown, of what may be revealed, of abandonment by caregivers, or other anxieties will cause some people to resist or give up this worthwhile effort.
Phase 4: Healing Challenges: (Fig. 3-1, E). During this phase of healing, the client works through progressive steps and deeper hindrances to physical healing with suitable supportive specialists. Repetitive care, such as provided by the physical therapist, allows the clinician to develop a deeper understanding and safe relationship with the individual. Once this relational foundation is set, the provider can coordinate with other involved providers who can offer services such as counseling. It is important to inform the client of options in obtaining those services and the benefits of receiving such services.
Difficulties in this phase can include testing the therapeutic relationship; the fear of losing parts of self by healing; and feeling insecurity, shame, and guilt when receiving joy. Familiar “helpers” or parts that appeared to rescue the client and take care of necessary functions might seem to be disappearing as the previously isolated “helpers” coordinate and integrate.
The rope analogy demonstrates the continued sufficiency and presence of each part and system of the unique individual. The concept of personal distinctiveness, while retaining and improving the strengths and function of all parts, becomes more comfortable.
The client needs to know that healing is worth the effort and that it will take time and practice to adjust to nonfractured thinking and living. The experiences of joy, functionality, and support persuade the affected individual to continue the healing journey through residual thought, image, and emotional intrusions from the past.
Lifestyle options and changes can be discussed and introduced during this phase. The client begins to experience how unity of body, mind, and feelings becomes much less exhausting, much more fulfilling, and more efficient.
Phase 5: Healing Victories: (Fig. 3-1, F). This phase of healing is very rewarding for client and health care provider. Joy is experienced more frequently as the person works through issues that previously blocked ROPC healing and growth. Physical problems stemming from stress reactions, faulty perceptions, and reactive living improve or resolve.
Safe relationships and healthy boundaries are recognized, practiced, and appreciated. The internal hunger that the joy-starved person thought would never be satisfied begins to abate, since joy is no longer feared but welcomed. The client relaxes from the frenzied quest for joy and finds that joy is best received without striving, as a flow, not a flood.
Through testing honest, open relationships in treatment and in personal circles, the client learns that physical and relational discomfort, healthy confrontation, and feelings can be acknowledged and faced, and joy reestablished. Differences between past survival habits and victim attitudes contrast sharply with current healthy proactive problem-solving and choices.
Instead of reacting and being driven by circumstances and other demands, the client is able to identify options and make healthy choices. Taking initiative becomes more comfortable and a proactive way of life. Through continued practice, the client learns that challenges can be addressed effectively and successfully, with less energy, time, and stress. Clients report being surprised by freedom, efficiency, and fullness of life never known before.
Phase 6: Moving Deeper into Health and System Integration: (Fig. 3-1, G). This phase of healing consists of practicing and refining new insights and skills. Realistic, objective assessment of life and situations becomes more routine and efficient, though relationship discernment may still be challenging.
Hypervigilance continues to diminish, but sensory hypersensitivity may increase temporarily. After prolonged periods of avoiding feelings and practicing emotional and sensory numbness, individuals in this phase go through a period of sensory activation and accommodation, even describing more acute hearing, vision, taste, smell, and tactile sensation.
Evidence of healing in mind, body, and spirit is confirmed by the following symptoms diminishing or ceasing:
• Being “triggered” (reacting to nonthreatening daily occurrences as if experiencing past threatening events)
• Reactively driven (impulsive needs to return to unhealthy, unsafe thoughts, habits, places, and people)
• Exaggerated and erratic emotional changes and reactions
• Fear and avoidance behaviors, especially when confronted with unknown or new situations
• Further evidence of emotional, mental, physical, and spiritual connection and health include increasing:
Phase 7: Final Phase of Healing: (Fig. 3-1, H and I). Finally, with evidence of healing and functional victories and with support, mentoring, and practice in healthy thinking, decision making, and living, the person feels healed. The individual may not be totally comfortable with independence but is ready to move out of the caring relationship and experience reinforcing successes and educational failures on his or her own. Continued practice and periodic support are still vital to assist as needed with facing and managing new trials.
People at this stage can be destabilized by brief recurrences of past thoughts or reactions. It is important to emphasize the management skills learned and that these skills helped before and they will help again. Let the client know that healthy does not mean no more pain or problems but rather that the negative occurrences should become less frequent and less intense over time and more efficiently addressed with practice. Issues and areas left unattended may come to light at some point, offering an opportunity for further healing and growth.
Sensory hypersensitivity and habitual hypervigilance decrease and often resolve. The person is better able to quickly recognize negative thoughts and habits and reject them in favor of better options. The client’s sense of personal uniqueness, value, and identity solidifies. Self-control improves while self-centered immaturity transforms into more mature altruism. Appropriate responding and proactivity replace past reactivity.
This final illustration of the rope depicts the rope well integrated, in close association, connected, strong, and functional in the orderly choreography of all elements present and working in harmony. No individual attribute or part is lost or standing alone or apart from the whole.
Although the desire to help others can occur in any phase of personal woundedness, it is in this phase of healing that the person is equipped and healthy enough to reach out to others and share the healing that they have experienced. Volunteer or community programs are excellent opportunities for clients to effectively support and contribute to others in need.
SPIRITUAL DEVELOPMENT IN THE HEALTH CARE PROFESSION
Spirituality can be viewed as one’s search for purpose, meaning, and relationship with the transcendent or others. Spirituality has been defined as a factor that contributes to health in many persons. The concept of spirituality is found in all cultures and societies. It is expressed in an individual’s search for ultimate meaning through participation in, among other things, religion or belief in God, family, work, naturalism, rationalism, and humanism.192
In the last 10 years, the impact of human spirituality and beliefs has come under closer scrutiny in research, secular publications, and clinical education. Studies are beginning to show an association between religion or spirituality and health outcomes such as hypertension, recovery from surgery, coping with illness, and the will to live. Many studies have demonstrated the importance of religion and specifically prayer in the coping process of individuals with cancer.53,67,120,190
According to a Gallup poll, 95% of Americans believe in God or a Higher Power; 3 out of 5 polled said that religion was very important to them.77 Prayer is a common practice in the United States. According to a national survey, more than one-third of Americans pray for good health. Many people who are ill may turn to prayer as a means of coping with their illness. Yet only about 1 in 10 people who pray for health reasons mention it to their health care provider.162
The health care provider’s openness and ability to address clients’ spiritual issues as the person reveals such concerns or beliefs are essential to the health and healing of the whole person. Spiritual care is not in any one provider’s domain. It is the responsibility of everyone on the health care team to listen to what is important to the individual, respect his or her spiritual beliefs, and be able to communicate appropriately with the person as those issues and beliefs are shared. Health care providers can ask patients/clients in a nonbiased, nonjudgmental way about their spirituality for a more holistic approach to health and healing.162
In a 1990 Gallup survey, it was found that 63% of adults surveyed believe it is good for doctors to talk to patients about spiritual beliefs. Sixty-eight percent of patients said they would welcome a spiritual question in a medical history; only 15% said they actually recalled being asked by their physicians whether spiritual or religious beliefs would influence their decisions.76
A study surveying more that 200 hospital inpatients found that 77% said physicians should consider patients’ spiritual needs. Furthermore, 37% wanted their physician to discuss spiritual beliefs with them more frequently, and 48% wanted their physicians to pray with them.131
Spiritual Perceptions and Health
How an individual perceives his or her condition determines how the person will respond to a disease, illness, or other physical or mental health condition. Spiritual experience, beliefs, and perspectives can have a powerful impact on an individual’s understanding of his or her illness. Religious convictions can affect an individual’s scope of options and decision-making process. Spiritual convictions may constitute a foundational need in health care or may cause a person to refuse procedures or treatment altogether.
A person who has experienced spiritual abuse might actively avoid anything with a religious or spiritual connotation. Knowing the pertinent history will allow the caregiver to gather information about words, expressions, and other triggers that might cause a negative reaction in the client. Spiritual health fosters coping beyond normally accepted parameters by giving the following192:
• Sense of control: faith and trust are choices. Making the choice to trust beyond understanding eradicates helplessness, actively engages the person in self-awareness and assessment, and expands coping potential through the experience of empowerment.
• Hope for restoration, for healing, for attaining goals, for a peaceful death: people can find the ability to accept and deal with current conditions through belief in a Higher Power.
• Acceptance: inconceivable stresses and demands can be tolerated when trust in a Higher Power gives meaning and purpose to life and suffering beyond understanding.
• Strength and endurance: a personal faith imparts peace beyond understanding or explanation, strength beyond self, and the ability to focus outwardly instead of being overwhelmed by internal suffering.
Human history is replete with accounts of people going through extreme, incomprehensible, life-threatening experiences or severe loss and finding the resolve to survive and the strength to endure through their faith and trust in God. Healing, beyond medical understanding or imagination, termed miracles or spontaneous healing by both clients and health care providers, is attributed to prayer and supernatural intervention. Although the tangible, consistent differences between those who spontaneously heal and those who do not are still being sought, the impact of spirituality is being considered and studied.
Consistently living in trust beyond circumstances and purpose beyond what we can see and understand relieves stress for many people. Instead of being reactive and allowing external pressures and demands to take control and dictate the results, problem-solving and life choices become responsive in nature. Challenges are addressed responsively, through weighing the options, making reasonable choices, and taking action on those choices.
Unfamiliar situations and apparently threatening events are entrusted to the Higher Power, who is believed to know the big picture beyond the individual’s scope of comprehension and is powerful enough to direct, protect, and provide through any event in life. This type of belief brings the individual an ability to cope and a joy that is above difficult circumstances. The health benefits of preventing damaging effects of persistent stress through abated fears, coming to terms with death and eternity, and knowing place and purpose in life through faith are experienced by many individuals.
Distant Healing
Distant healing, the concept that human beings can intentionally cause healing effects in others, is an ancient concept, but one that has gained much attention in the last decade. Researchers in the field of distant healing cite formal laboratory and clinical studies with reported significant effects.2,12,51,122
Broadly defined, distant healing is a conscious, dedicated act of another person who is physically and emotionally at a distance.20,57,58 Although this concept has come under fire and remains heavily debated, the use of intercessory prayer for patients in a coronary care unit has been established as a landmark study in the areas of both medicine and religion. Limitations of the study have been discussed as well.33,34,60 The relationship between religious activities and lowered blood pressure, improved mental health, and decreased depression in older adults also has been reported.135,136,174
Other researchers have evaluated whether receiving intercessory prayer or knowing intercessory prayer was being offered has any effect on recovery after cardiac surgery. It seems that individuals who know they are being prayed for may have a higher incidence of complications.21
The topic of intentional healing from a distance is not standard conversation among rehabilitation providers. This is a complex and highly emotional subject for many people. The Holistic Nursing Association has brought this topic forward for the nursing profession with a commitment to the well-being of others, integrating intentionality in healing, caring, and communication.196 Research conducted jointly by medical researchers, philosophers, and theologians may bring greater clarity to the topic in future years.
Practicing Sensitive Care
Sensitive care for the spiritual elements of each individual includes the following192:
• Providing a safe environment by giving attention to the physical environment and to nonverbal messages.
• Listening attentively to the client and reflecting feelings and responding appropriately, both verbally and most importantly, nonverbally.
• Accepting the individual as a person whether you agree or approve, verbally and nonverbally respecting and valuing the person as you partner in discovering truth and evaluating options.
• Obtaining a spiritual history or identifying the person’s need for avoidance of discussion of spiritual topics.
• Honoring spiritual practices, as appropriate; each clinician would benefit from discussing this issue and defining the professional, ethical, and personal boundaries involved.
• Recognizing pastors, chaplains, rabbis, and other spiritual leaders as part of the interdisciplinary team.
SPECIAL ROLE OF THE PHYSICAL THERAPIST
It is virtually impossible to discern or identify all of the contributing factors in a person’s pathology. It is to the clinician’s and the client’s benefit to consider the whole person during the physical therapist’s assessment and intervention so as to avoid limiting perspective.
Pathology is never purely physical, mental, emotional, or spiritual. Those systems are intimately connected and interdependent. To believe that comprehensive care can come from treating a single cause or system, while ignoring other components, is naïve and negligent.
Physical therapists are ideally situated to screen for and respond to family violence and all forms of trauma and abuse. As a client is treated over a period of time, and with repeated visits, a relationship is formed that is conducive to growing trust and openness.
The task before us is not easy, but all of our skills and knowledge will matter little unless we bring to our practice the sensitivity that is the right of all of our clients.206 Exercising sensitive, compassionate, and insightful care, the physical therapist is able to identify and attend to situations of abuse, neglect, and domestic violence.52 See Chapter 2 for further discussion of domestic violence.
Other elements that strengthen the position of the physical therapist in identifying and treating underlying contributors to physical pathology include the fact that we monitor a variety of information sources. As the client verbally informs the physical therapist, observations of function, affect, reactivity, receptiveness, and appropriateness can be gathered. Receiving and comparing information from the person’s musculoskeletal, neurologic, verbal, and nonverbal communication provides a wealth of confirming or contradictory evidence.
Physical therapists are primarily involved in the treatment and rehabilitation of most of the signs of unresolved trauma (see Table 3-2), arising from a combination of contributors over time. The importance of listening, observing, and responding carefully to understand the person’s reports of pain, thinking, and living patterns beyond the presenting organic components cannot be overemphasized.
The late Jules Rothstein, PhD, PT, FAPTA and former editor of the professional journal, Physical Therapy, stated that, “Cynics might dismiss the concept of sensitive practice, but reality tells us that only by listening to our clients can we know about them and their condition. The knowledgeable listener who can act on what the patient says needs to couple that skill with keen observations of unspoken messages. All the while, the physical therapist must be wary about receiving messages never meant to be sent, messages that come from within the practitioner, born out of bias and personal agendas.”203
This chapter on nonphysical contributors to physical pain and pathology serves as a practical introduction to the potential we have as physical therapists to integrate neuromusculoskeletal health and function with cognitive, emotional, and spiritual health and function.
As we step out in bridging the gap between medical and psychologic training and treatment, we need to seek insightful resources and competent ancillary professional teammates to partner with us in the rehabilitation of the whole person—heart, mind, spirit, and body.
Boundary Basics for the Provider266
Personal boundaries are critical to a person’s identity and function. Boundaries can be flexible or rigid, open like fences or solid like walls, or versatile like a gate. Whereas positive life experiences promote exploration and testing of boundaries, negative or painful life experiences cultivate avoidance behaviors, especially every real or perceived trauma-related boundary.
People with harbored hurts tend to keep the darker emotions (e.g., anger, shame, fear) in and positive events (e.g., safe connection and trust, joy, helpful support) out of their lives. With healing, the function of boundaries reverses to allow in and keep in good and healthy elements and keep out negative, harmful elements. As health improves, personal boundaries help to monitor internal and external status, which strengthens and magnifies coping ability.
Healthy boundaries maintain an adult-to-adult equality in the caring relationship, prevent the provider from taking on unrealistic responsibility for outcomes, and keep the focus on the needs of the client. Practicing healthy, personal boundaries is critical for the client, as a model of safety, respect, and health, and for the clinician to be above reproach, upholding ethical integrity and moral excellence. Establishing healthy boundaries allows others to know who you are and what to expect, facilitating a safe and trusting relationship.
Guidelines for the Health Care Professional
Initially, the clinician is encouraged to clearly define the clinical relationship with the client, including goals, expectations, roles, policies, and options. The therapist is advised to follow established policies; do not pacify the client by changing the rules. If concessions are made within established policies and healthy boundaries, let the client know what concessions are available and clearly identify the sustaining or limiting parameters.
Appeasing the client may give relief for the moment, but changing the policies can cause confusion and insecurity in the future. Recognize and reflect on what your client is feeling and expressing and then clarify your desire to do the best you can for the individual. Clearly explain the policy and what is expected of both sides and document the interaction well.
Participate in regular supervision and consultation with peers for healthy accountability, support, and perspective. Practice potentially difficult sessions with peers before the session(s). Practice clear statements and interactions that convey empathy, clarity, confidence, and decisiveness. Be objective, not defensive or emotion-laden.
Do not be in a hurry to respond to highly charged, emotional messages or phone calls. Seek counsel from peers and other providers, write out your response, offer options that are “win-win.” Document thoroughly in an objective, nonjudgmental way as if the client, the client’s family, lawyers, and other professionals will read your notes.153
Start and stop each session on time, allowing time for “cool down,” settling, and refreshment, with about 5 minutes dedicated to reviewing victories, independent preparation, and rescheduling.
Avoid rescuing and becoming the “savior.” Know your roles and personal boundaries and make an appropriate referral when necessary. If the client has already been receiving services elsewhere, establish the client’s support list and reflect on healthy options and past management choices. The client should be asked to make a list of at least 5 people who can be contacted by the client in case of depression, crisis, or other emergency. Leaving a message on an answering machine is desirable but do not stop there. Instruct the client to ask for direct contact numbers and continue calling the numbers on their list until they connect with a real person.
Useful Tools
Tools streamline the therapist’s practice and help maintain consistency in treatment. Clinical tools, such as a comprehensive patient/client entry questionnaire, can save time and provide crucial, possibly elusive, pertinent hints as to the individual’s needs, thinking, and status. Have a prepared referral list with contact information for carefully screened interdisciplinary professionals. A list to consider can help smooth the client’s transition in thinking about taking advantage of adjunct services. Specific client worksheets lighten the provider’s load, promote patient/client motivation and participation in the healing process, and equalize responsibility, while providing essential insight into the person’s thinking processes. Materials designed with the therapist in mind are available.266
SPECIFIC PSYCHOLOGIC CONDITIONS
The information in this section is designed to help the therapist recognize the need for referral and to better understand clients with orthopedic and/or neurologic conditions who also have mental health disorders or psychologic issues that can bring many unique challenges to the rehabilitation process.
The information in the first half of this chapter can be applied to all clients with the specific psychologic or psychiatric disorders described in this second half of the chapter. The therapist should keep in mind that psychologic and psychiatric disorders are distinct from but affect behavioral or conscious actions and can often be difficult to differentiate. It is also important to remember that professional, clinical care can either exacerbate pathology or enhance healing. In addition to the benefits of sensitive, insightful care, referral to counseling services and/or pharmacologic intervention may be needed.
Most of the disorders in this chapter can be found in the American Psychiatric Association’s Diagnostic and Statistical Manual, fourth edition, text revision (DSM-IV-TR).6 The DSM-IV-TR is the handbook used most often in diagnosing mental disorders in the United States. The International Statistical Classification of Diseases and Related Health Problems (ICD) is a commonly used alternative internationally. Both texts assume medical concepts and terms and state that there are categorical disorders that can be diagnosed by set lists of criteria.
The first edition of the DSM was published in 1952 and had just slightly more than 100 different disorders. By 1968, the DSM was revised with 140 disorders. Currently, the fourth edition contains eight major areas of disorders (Box 3-4). The fifth edition is expected to be published in 2011. A DSM-V timeline and proposed contents are available.7
In addition to having a copy of the DSM-IV-TR, therapists may want to add to their library a more user-friendly text.175 You can also go to Amazon.com and find “Desk Reference to the Diagnostic Criteria From DSM-IV-TR.” Search inside this reference by typing in the disorder you are interested in and references to appropriate pages will appear.
Substance Abuse
Substance abuse is defined as the excessive use of mood-affecting chemicals (Box 3-5) that are a potential or real threat to either physical or mental health. Substance abuse has become increasingly prevalent in American society among people of every age, social, economic, professional, and educational status.
The reasons for this phenomenon are multifactorial and include changes in social norms and attitudes, easier access, increasing pervasive fears, and life stresses combined with decreasing problem-solving and coping skills. Other contributing factors include personality characteristics, genetic influences, peer pressure, and as a means of self-treatment in PTSD, a syndrome with symptoms resulting from past trauma (defined as a personally overwhelming experience).
The origin of early age onset substance use disorder (SUD), classified as a psychiatric illness, is also considered complex and multifactorial, possibly involving genetic and environmental interactions beginning at conception. Alterations in somatic and neurologic maturation in the presence of adverse environmental variables result in behavioral dysregulation identified at first as difficult or abnormal temperament in infancy, progressing to withdrawal or conduct problems in childhood and substance use in early adolescence, eventually leading to severe SUD by young adulthood.225 Whether to consider substance use/abuse a behavioral condition or psychologic problem remains uncertain. Many psychologists and addiction counselors say it is a condition, illness, or problem with multiple factors, including physical, psychologic, social, economic, and spiritual.
There may be individuals who choose to abuse alcohol and other drugs and think they can stop whenever they want to do so, whether that is true. For those, it is almost always a psychologic issue—peer pressure, the need to get that “feel better” moment, and so on. Then there are those who once they abuse and become addicted cannot stop without behavioral and/or medical intervention. This is both a psychologic issue and in some cases a medical condition. Many people think it is all a psychologic issue; from a substance recovery perspective, this may not be a helpful point of view.110
Addiction
Substance abuse may take the form of both addiction and habituation leading to psychologic craving or dependence, tolerance, and physiologic dependence accompanied by withdrawal symptoms when use is discontinued. The central nervous system (CNS) adapts to the continued presence of a substance by compensating for its effect in a process referred to as tolerance. As a result, the person has to take increased quantities of the substance to obtain the same effect or to feel normal. This phenomenon leads to physical and psychologic dependence and pathologic organ changes.
Withdrawal is the pattern of physical responses that appears when regular drug use is discontinued. When a physically dependent person abruptly stops consumption, signs and symptoms of withdrawal occur. Most withdrawal reactions produce an effect opposite to that of the ingested substance (e.g., a depressant causes hyperactivity during withdrawal).
These substances become necessary to help the individual function normally. The addiction may lead to a lifestyle (e.g., prostitution, theft, violent crime) that puts the person at considerable risk for illness, disease, and injury.
A great deal of research around brain function and addiction has advanced our understanding of addiction. Researchers are looking for ways to stop addiction before it starts, knowing that lasting changes in brain function occur and are difficult to reverse. Twin and adoption studies show that about 50% of individual variation in susceptibility to addiction is hereditary. Stress, depression, anxiety, and mental illness, such as schizophrenia, antisocial disorder, and borderline personality, increase the risk of addiction.
Incidence
Substance abuse is associated with violence, injury, and human immunodeficiency virus (HIV) infection and is estimated to be a factor in half of all highway fatality accidents. Varying center-based statistics show that 25% to 50% of all people with spinal cord injury (SCI) have substance abuse problems compared with an estimated 10% of the general population.
The statistics for alcohol and other drug use at the time of injury are as high as 68% to 80%. Among a sample of people admitted to one center, nearly half of all people who sustained an SCI were intoxicated when injured; although many newly admitted clients with SCI reduce or eliminate alcohol use during their hospitalization, 56% resume drinking after 1 year.172
Alcoholism is the most common drug abuse problem in the United States, affecting more than 15 million Americans, including the adolescent and aging populations. The frequency of binge drinking among college students has increased dramatically in the last decade with an increase in the number of alcohol-related injuries, property damage, and disruption.250
Excessive alcohol consumption kills approximately 75,000 people each year in the United States.236 Alcohol-related deaths outnumber deaths related to other drugs 4 to 1, and alcohol is a factor in more than half of all domestic violence and sexual assault cases.181
Alcohol slows reaction time and impairs judgment, making it a leading cause of all types of accidents, including 40% of all automobile accidents and a large percentage of accidents that occur on the job.125 Alcoholism is extremely prevalent yet underdiagnosed among adults with symptomatic terminally ill cancer.30
The effect of drugs other than alcohol on drivers has been studied but remains inconclusive. Results vary by type of drug. Laboratory studies suggest marijuana and benzodiazepines impair driving performance, but the results of studies of crashes are inconsistent. Marijuana is the most common drug associated with fatally injured drivers, followed by cocaine, benzodiazepines, and amphetamines.125
New users of opioid analgesics likely have impaired driving skills, but again, crash study reports are inconclusive. New users, occasional users, and anyone who has increased the doses of drugs are more impaired than someone who has become tolerant through steady (daily as prescribed) use. Combining alcohol with drugs and the use of multiple drugs increase the overall risk for crashes.125
The injection of illicit drugs has played a central and expanding role in the HIV/acquired immunodeficiency syndrome (AIDS) epidemic. The proportion of new AIDS cases attributable to this risk factor has doubled in the last decade; approximately 30% of people reported with AIDS have injection drug use as their recorded risk behavior. Injection drug use is especially important in the HIV/AIDS epidemic among women and children and represents the major route for heterosexual and perinatal transmission of HIV.72
Tobacco
Tobacco products include all cigarettes (whether they are labeled “light” or other minimizing name), pipe smoking, cigars, and smokeless tobacco, the latter available in two different forms: snuff and chewing tobacco. Snuff, a fine grain tobacco, comes in cans or pouches. Users take a “pinch,” “dip,” or “quid,” and place it between the lower lip or cheek and gum and suck on it. Chewing tobacco comes in pouches in the form of long strands of tobacco that when used are commonly called “plugs,” “wads,” or “chew.”
Approximately 21% of adults in the United States are current smokers; an estimated 70% of those smokers want to quit. After years of steady decline, rates of smoking among adults leveled off in the 1990s but reportedly continue to decline among adults overall.160
Healthy People 2010 has targeted tobacco use as one of its focus areas with the goal of reducing illness, disability, and death related to tobacco use and exposure to secondhand smoke and to reduce the prevalence of cigarette smoking to less than 12%.
American Indian adults have a much higher rate reported by the Centers for Disease Control and Prevention (CDC) as 53% among men and 33% among native women. Epidemiologic data suggest that smoking among high school students peaked in the late 1990s and is now declining. Previously reported rates of 36% in 1997 dropped to 28.5% in 2001 and went down to 20.9% in 2005.43
Smoking appears to be more highly correlated with low income, persons with a GED or formal education less than 12 years, military personnel, and specific groups such as Native Americans and Alaskan Natives. Men have only somewhat higher rates of smoking than women within the total U.S. population.160
Habitual smoking and alcohol dependence frequently occur together. Researchers are exploring a possible genetic link to tobacco and alcohol dependence. The presence of certain genes involved may predispose individuals to both alcohol dependence and habitual tobacco use.96
Tobacco is one of the most addictive agents, with even greater development of dependence than cocaine and heroin. Some researchers suggest that smoking rewires the brain, producing a powerful addiction. Brain imaging studies of addicted smokers suggest that nicotine leads to a rapid increase in dopamine levels, promoting further nicotine use, which is a form of pleasure-seeking behavior.244
People with ADD are five times more likely to become smokers than those without this disorder. Nicotine may help them concentrate. Many smokers are self-medicating with nicotine when they smoke, but the delivery device they are using contains hundreds of cancer-causing chemicals.88
Effects of Tobacco.: Cigarette smoking and the use of tobacco products continues to be the single most preventable cause of disease and death in the United States. Smoking results in more deaths each year in the United States than AIDS, alcohol, cocaine, heroin, homicide, suicide, motor vehicle crashes, and fires combined.40 Tobacco-related deaths number more than 440,000 per year among U.S. adults and direct medical costs attributable to smoking total at least $75 billion per year and an estimated $82 billion in lost productivity.40
Smoking has been linked conclusively to acute myeloid leukemia and cancers of the cervix, kidney, pancreas, and stomach. Smoking is known to cause elevated blood pressure, pneumonia, abdominal aortic aneurysm, cataracts, and periodontitis. Smoking harms nearly every organ of the body, damaging the smoker’s overall health even when it does not cause a specific illness.37 Smokers are at an increased risk of developing diabetes, heart disease,70 major depression,132 and suicide and other problem behaviors.28 Smokers may be at increased risk of LBP.1 Nicotine has also been linked with accelerated disk degeneration. Smoking has a negative effect on wound healing, bone graft incorporation, and pain reduction.101 This is particularly important to some aspects of physical therapy practice. Smoking impairs the normal processes of fibroblasts. In the lung, smoking slows fibroblast proliferation and makes fibroblasts less mobile, leading to slower repair of injured lung tissue.177
Smoking also appears to contribute to increased fibroblast accumulation in some wounds, allowing cells that would normally die to remain alive, but with decreased mobility, therefore accumulating in areas of the wound where they are not needed, inhibiting normal healing,262 and promoting the development of tissue breach or scar tissue.
A study by Brown and colleagues demonstrated an association between smoking and pseudoarthrosis after spinal fusion. Examination 1 to 2 years after surgery revealed that 40% of the smokers had developed a pseudoarthrosis, whereas among nonsmokers, the rate was 8%. It was hypothesized that the higher incidence of surgical nonunion among smokers may be related to blood gas levels.29
Exposure to secondhand smoke has been attributed to increased morbidity and mortality among children and adults. There is a known link between active smoking and cervical cancer; researchers suspect a similar association exists between passive exposure to cigarette smoke and cervical carcinogenesis.238 The Surgeon General’s report on the consequences of involuntary exposure to tobacco smoke reports the following major conclusions36:
• Secondhand smoke causes premature death in children and adults who do not smoke.
• Children exposed to secondhand smoke are at an increased risk for sudden infant death syndrome (SIDS), acute respiratory infections, ear problems, and more severe asthma; smoking by household members causes respiratory symptoms and slows lung growth in children.
• Exposure of adults to secondhand smoke has immediate adverse effects on the cardiovascular system and causes coronary heart disease and lung cancer.
Aging and Substance Abuse
Alcohol is by far the most serious drug problem among the elderly or aging population. Many older people view alcohol problems in a moral context associated with feelings of shame and weakness, which prevents them from seeking help. An older adult is at greater risk for difficulties with alcohol than a young person for several reasons. Both total body water and lean body mass are reduced as a person ages.
Even though ethanol metabolism is not decreased in older adults (unless an underlying condition causes it), blood alcohol levels are less diluted and thus higher in the older person than in the younger person when both are given equivalent amounts determined by body surface area. Thus the same person, as he or she ages, can achieve higher blood alcohol levels with no increase in the amount ingested, all other factors remaining constant. Illness, malnutrition, the administration of other hepatotoxic drugs, or drugs that require breakdown in the liver may all increase an elderly person’s sensitivity to alcohol.
Many OTC liquid cold remedies, mouthwashes, and cough syrups contain alcohol, which the aging person may consume as a substitute for drinking. Signs and symptoms of alcohol abuse may occur, but the person denies alcohol intake. Further questioning may be necessary to uncover these hidden problems with alcohol.
The older person is even more vulnerable to the detrimental effects of alcohol on cognitive function than the younger person. These effects on cognitive function occur even with light social drinking and are similar to those associated with aging. Alcohol can mimic or exacerbate cognitive changes linked both with normal aging and Alzheimer’s disease.
Sleep disorders are common among older people, leading to the use of alcohol and other sedative or hypnotic drugs as chemical management for insomnia. Alcohol does act to decrease sleep latency (the time between falling asleep and the first rapid eye movement [REM] period), which increases with age, but it also tends to further reduce REM and stages 3 and 4 of non-REM sleep, which is already decreased in older adults. The net result is a virtual elimination of the restful and restorative portions of the sleep cycle. This can be further complicated by alcohol withdrawal occurring during sleep with the accompanying sympathetic discharge and arousal.
Abuse of sedative-hypnotics, taken either for sleep or anxiety, is a common form of drug abuse among the elderly. Complications of these drugs may be related to the development of toxic levels from the long half-lives of these compounds along with their slow metabolic breakdown in the elderly. Slowed response, hypersomnia, and increasing confusion are sometimes thought to relate to aging when actually they are symptoms of toxic drug levels.
Withdrawal symptoms may occur when the medication is abruptly discontinued as a result of hospitalization or other change in life circumstances. Symptoms can be severe and may include tachycardia, hyperthermia, hypertension, altered mental states, seizures, and opisthotonos (severe spasm of the body backward into extension). The withdrawal is often not recognized or diagnosed immediately.
Caffeine is included as a substance because it is a chemical stimulant and the most common behaviorally active drug that can result in physical dependence. The most common source of dietary caffeine among the aging is coffee, with average consumption around 200 mg/day. Soda pop and stimulant drinks are a common and growing source of caffeine in younger populations. High consumption or withdrawal from these drinks can present as severe or chronic headaches, joint pain, fatigue, irritability, and other symptoms.
Caffeine is distributed essentially only through lean body mass. Because of the greater proportion of adipose tissue to lean body mass in older humans, a dose of caffeine may result in a higher plasma and tissue concentration in older adults compared with younger individuals. Responses to caffeine may be greater in older adults at doses in the 200-to 300-mm range, and the preponderance of data suggests that caffeine has a greater impact on calcium metabolism and bone in older people.154 Although smoking is less prevalent in older adults, older smokers are at greater risk because they have smoked longer, tend to be heavier smokers, and are more likely to already have smoking-related illnesses.173
Pathogenesis
In recent years, it has been discovered that dopamine, a neurotransmitter, plays a pivotal role in substance dependence by activating channels in the brain that register feelings of arousal, reward, and satisfaction. It is thought to be instrumental in enabling us to identify actions that pay off so that we can appropriately address the underlying need and replace unhealthy habits with healthy, more satisfying practices.
Many substances that create dependence influence dopamine levels. They may stimulate dopamine release, attach to dopamine receptors, or alter the way dopamine receptors respond. Whatever the pathway, the effect of heightened stimulation of neurons in the reward channel is the same. For people who become drug dependent, the pathway becomes more deeply ingrained with each use and becomes linked with cues evoking drug use such as smells, location (e.g., smoky bar, abandoned house), paraphernalia used to prepare and administer the drug, or certain companions.
When a person who is substance dependent encounters a use-associated cue, a spontaneous and overwhelming desire for the substance occurs, triggered by a dopamine release in the brain. These chemical pathways appear to be present even after years of abstinence, making relapses common, along with a new understanding that substance dependence is a chronic medical condition and not a weakness of will.
Illicit drug use or narcotic abuse may damage neurotransmitter receptor sites; the subsequent imbalance produces symptoms that may mimic other psychiatric illnesses such as agitated depression or amphetamine (speed)-induced seizures or paranoia. Repeated stimulation of the brain, called kindling, increases susceptibility to focal brain activity with minimal stimulation until the individual experiences spontaneous effects without the use of chemicals.
The effects of kindling may be manifested as mood swings, panic, psychosis, and occasionally seizures. Behavioral effects are also noted such as poor work performance, job loss, pathologic lying, truancy, paranoia and aggression, violence, marital and relational prob- lems, or erratic behavior. Nonspecific signs such as red eyes; fatigue; signs of upper respiratory infection, especially cough; heart palpitations; avoidance of eye contact; confusion; or evidence of trauma may be present.
Caffeine appears to work not by speeding us up but by keeping us from slowing down. Each time brain cells fire, adenosine is produced that functions as an “off” switch, keeping neural activity in check. Caffeine binds with receptors on cell walls that normally respond to adenosine, overriding the switch so it cannot be turned down. Caffeine along with other stimulants, such as cocaine and amphetamines, mimics the stress response affecting the cardiovascular system and stimulating the sympathetic nervous system to increase production of adrenaline, causing the effects listed in Table 3-3.
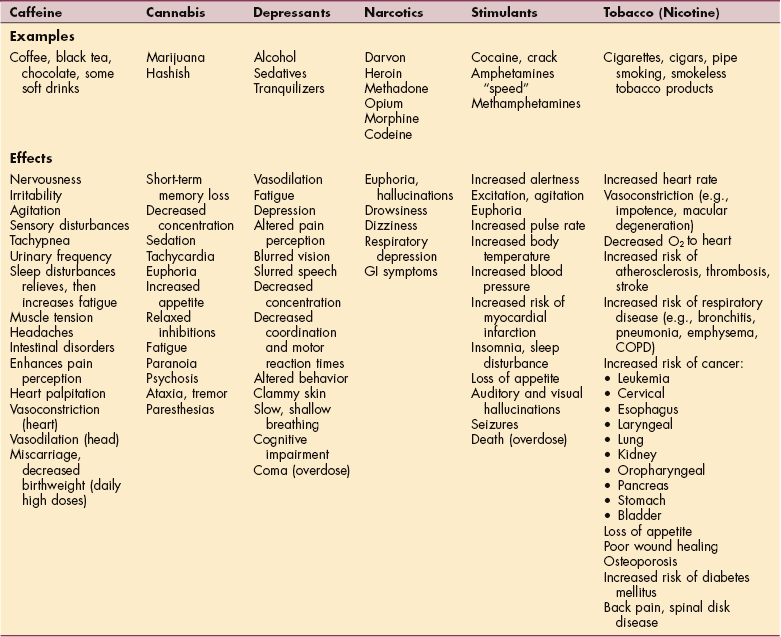
Caffeine in toxic amounts (more than 250 mg/day or 3 cups of caffeinated coffee) may also produce additional symptoms. High daily doses of caffeine in excess of the equivalent of 5 cups of coffee may increase the chance of miscarriage or fetal growth retardation, although it is possible that some of this risk is a result of confounders such as cigarette smoking and alcohol use.133
No data support a link between caffeine and cancer, and no evidence exists showing that caffeine increases the risk of benign breast disease (formerly fibrocystic breast disease). However, cigarettes have been linked to fatal breast cancer. Overall, moderate amounts of caffeine are considered safe, but women are cautioned against substituting coffee for milk or ingesting more than moderate amounts of caffeine during pregnancy or while breast-feeding.
Alcohol and the addictive effects of alcohol may be caused by an enzyme protein kinase C-epsilon (PKC-ε) in the brain responsible for creating a desire to drink. It may be that the channels in the γ-aminobutyric acid (GABA) neurotransmitter system in the brain causing chemical and electrical changes in neurons are kept open longer than normal by alcohol.
This effect results in increased responsiveness to the signals leading to feelings of pleasure, calmness, or sleepiness. Studies involving mice show that in the absence of PKC-ε, alcohol makes the GABA receptor system even more sensitive. Inhibiting this enzyme may remove the rewarding effects of alcohol affected by GABA.105
There is no longer any question that women are more vulnerable to the effects of alcohol than men. Women produce substantially less of the gastric enzyme alcohol dehydrogenase, which breaks down ethanol in the stomach. As a result, women absorb 75% more alcohol into the bloodstream.
Women have a smaller proportion of total body water than men (51% versus 65%), so the alcohol in the blood is less diluted, producing higher blood levels. Women feel the effects of alcohol sooner and more intensely than do men. Similarly, women and older adults of either gender have less water in their tissues than men of comparable height and build. Because alcohol is soluble in water, it tends to dissolve more slowly in older adults and women than in young men, causing intoxication after fewer drinks and longer-lasting effects.
Clinical Manifestations and Health Impact
Alcohol and other drug use are associated with child and spousal abuse; sexually transmitted diseases, including HIV infection; teen pregnancy; school failure; motor vehicle crashes; escalation of health care costs; low worker productivity; and homelessness. Alcohol and other drug use can result in substantial disruptions in family, work, and personal life.
People who use and abuse illicit drugs, any substances mentioned in Box 3-5, or any combination of these substances have special health care needs. Specific effects and adverse reactions depend on the drug type (see Table 3-3) and may vary dramatically from person to person. Death can occur in anyone as a result of interaction between depressants such as alcohol combined with certain medications.
Recently, methamphetamine (meth) has become the most prevalent drug of abuse in many areas. Methamphetamine is also known as “speed” or “crystal” when it is swallowed or sniffed, “crank” when it is injected, and “ice” or “glass” when it is smoked. Users could gain fast access to this drug because it can be manufactured easily from readily available components such as OTC cold medications containing ephedrine or pseudoephedrine. Those OTC medications are now required to be behind-the-counter (BTC) or sold in limited amounts for more difficult access. Addiction is often immediate with the first methamphetamine use—as opposed to a longer period of use required to become addicted to some of the other illicit drugs.
Methamphetamine is a powerful stimulant that activates certain systems in the brain. It is closely related chemically to amphetamine, but the CNS effects of methamphetamine are greater. The CNS actions that result from taking even small amounts of methamphetamine include increased wakefulness, increased physical activity, decreased appetite, increased respiration, hyperthermia, and euphoria.
Other CNS effects include irritability, insomnia, confusion, tremors, convulsions, anxiety, paranoia, and aggressiveness. Hyperthermia and convulsions can result in death. Additionally, the physical damage caused by use of “meth” is more extensive and can be more readily apparent (e.g., rotting teeth). There has been one report of electrode nonadherence when using self-sticking reusable TENS electrodes in a client in a meth recovery program. Chemicals dispersed through the skin seemed to dissolve the adhesive. Even with the use of duct tape to hold the electrodes in place, there was no skin disruption; the duct tape just peeled right off the skin.143 Other unreported effects of meth may be observed but are as yet unreported in a physical therapist’s practice.
Nicotine addiction in tobacco use requires daily use of tobacco products to maintain nicotine levels in the brain, primarily to avoid the negative effects of nicotine withdrawal but also to modulate mood. Nicotine dependence is the single most common psychiatric diagnosis in the United States. Substance abuse, major depression, and anxiety disorders are the most prevalent psychiatric comorbid conditions associated with nicotine dependence. Additionally, regular tobacco users exhibit altered levels of stress, arousal, and impulsivity.22 The many respiratory diseases directly attributable to tobacco are discussed in Chapter 15.
Heavy drinking is associated with an increased risk of several cancers (e.g., mouth, esophagus, pharynx, liver, pancreas).95 There is enough evidence now to support a link between alcohol ingestion and breast cancer, but the exact mechanism(s) remains unclear.140,229,267
Pregnant women are advised to avoid alcohol because no safe level has been identified. Even as little as one drink per day has been shown to cause teratogenic effects in offspring (e.g., developmental abnormalities). Drinking early in pregnancy and binge drinking are associated with the greatest risk to offspring.
The most severe consequences are referred to as fetal alcohol syndrome (FAS), which is characterized by prenatal or postnatal growth retardation; CNS disturbance with neurologic abnormalities, behavioral dysfunction, intellectual impairment, and structural abnormalities (e.g., microcephaly); and a characteristic face with elongated midface, thin upper lip, and flattened maxilla.
Research to identify how alcohol triggers neurodegeneration suggests that the destruction of millions of neurons in the developing human brain could explain the reduced brain mass and associated dysfunction.112
MEDICAL MANAGEMENT
Substance abuse of any kind requires an overall treatment program, including education, counseling, behavior modification, and for some substances, pharmacologic help. Addiction to substances is considered a biochemical disorder that can be arrested by attending to the underlying psychosocial needs and altering behavior(s). Success depends on the individual’s desire to correct the problem and compliance with treatment regimens.
In the rehabilitation of clients with SCI and traumatic brain injury (TBI), pain and underlying emotional and psychologic needs may be undertreated, causing some clients to turn to other, sometimes illicit, drugs to self-medicate. Timely, effective intervention for pain control, along with insightful attention to the psychosocial impact of the condition and resulting needs of the client, are the goals in treatment before substance abuse becomes a problem.
Of the estimated 48 million adult smokers in the United States, approximately 16 million attempt to stop smoking cigarettes for at least 24 hours annually; another 2 to 3 million attempt to stop but cannot abstain for 24 hours. However, 1.2 million people do stop smoking each year, often without the behavioral and pharmacologic aids now available for smoking cessation.
The number of pharmacologically assisted quit attempts per year jumped from 1 to 2 million to approximately 7 million, corresponding with the availability of nicotine gum and the nicotine patch as OTC products. Pharmacologic interventions double the success rates, and all health care workers are encouraged to recommend smoking cessation to all clients while providing appropriate treatment referral.41,44
Prevention is the key to any successful substance abuse program. The American Medical Association has released guidelines recommending that all people over age 60 be screened and treated for substance abuse problems. The Healthy People 2010 goals for substance abuse are to reduce substance abuse to protect the health, safety, and quality of life for all, especially children; to increase tobacco cessation rates; and to increase pregnant women’s rate of abstinence from alcohol from 86% in 1997 to 94% in 2010.
3-5 SPECIAL IMPLICATIONS FOR THE THERAPIST
Impaired Motor Function and Sensory Integrity Associated with Acute or Chronic Polyneuropathies (alcoholrelated)
Primary Prevention/Risk Reduction for Cardiopulmonary Disorders (all substances but especially cocaine and tobacco products)
Impaired Aerobic Capacity and Endurance Secondary to Deconditioning Associated with Systemic Disorders (all substances but especially tobacco products)
Primary Prevention/Risk Reduction for Integumentary Disorders (injection drug use, tobacco use, and delayed wound healing, SCI population)
Substance abuse can impair or slow the rehabilitation process, especially delaying wound healing. The client using any substances discussed in this section should be encouraged to reduce (eliminate if possible) intake of these chemicals during the rehabilitation process. Not only will the healing process accelerate but levels of perceived pain can also be reduced when these substances are eliminated.
Primary intervention or care for the chemically dependent person is essential. However, the realistic picture is more often one of a person who has a pattern of substance abuse and either denies the problem or admits failure in the past. For example, people who smoke or chew tobacco and have repeatedly tried to quit most commonly admit failure. Failure to stop or correct unhealthy habits when the person desires to do so often indicates that (1) the underlying need associated with the destructive behavior has not been addressed or (2) the person may need more equipping or support to attain and maintain the desired correction.
Many people who seek medical attention for seemingly unrelated conditions fail to disclose their use of alcohol or other drugs. Behavioral research shows that most excessive drinkers (79%) are insured and even have contact with health care professionals. Low screening rates among excessive drinkers may be more a matter of missed screening opportunities (i.e., failure of the health care professional to conduct a comprehensive screening examination).
As part of the assessment process, therapists using a systems approach can screen for the presence of chemical substances by asking about the use of prescribed drugs, OTC drugs, and self-prescribed drugs such as nicotine, caffeine, and alcohol or other drugs. Therapists must be alert to alcohol and other drug use and abuse. Recognition of the problem is crucial to successful patient/client management. Since physical therapists generally spend more time with patients/clients than many other health professionals, they may be the ones best able to recognize substance abuse that would be hidden from those who spend less time with the client or who do not have the skills to recognize impairments of the cognitive or motor systems.
It may be helpful to assess the behavioral impact of substance abuse by asking one or more of the following questions:
• When is it that you feel you need these substances?
• How do these activities help you?
• Are you concerned about your dependence?
• Do you have a pattern of cutting back or stopping the use of alcohol, cigarettes/tobacco, sleeping aids, or other substance but then restarting it?
• Have you been concerned or has anyone around you raised concern about your use of these substances?
An appropriate final question may be “Since it is important to the results of your treatment, do you take (use) any drugs or substances that you have not told me about yet?”
The National Council on Alcoholism and Drug Dependence (http://www.ncadd.org or (800) NCA-CALL) has a self-test available for assessing the signs of alcoholism. If the client reports the use of substances, the therapist may want to ask whether the person has discussed this with his or her physician or other health care personnel. Encourage the client to seek medical attention, or inform the individual that this will be addressed as a medical problem in your communication with the physician.
You can take the approach that this situation is no different from a case of undiagnosed or untreated angina. The client’s health is impaired by the use and abuse of substances, and therapy will not be effective as long as the person is under the influence of chemicals.
With the SCI and TBI population, the therapist must be alert to any suspicious signs or symptoms of substance abuse (see Clinical Manifestations in this section). More than half of all people with SCI or TBI incurred their disabilities while under the influence of drugs or alcohol; some studies report as much as 80%. It is estimated that two-thirds of people with disabilities who abuse drugs and/or alcohol did so before their injury, and many turn to substance use afterward to cope with life changes caused by the disability. Medical professionals should also be observant for excessive sleeping and unusual symptoms, such as muscular inflammation and myopathies, which can occur with the use of street drugs.
The health care professional is cautioned against actively or passively encouraging the use of substances out of an attempt to normalize socialization or out of a sense of compassion or pity. This concept is termed entitlement and may take the form of endorsement, subtle agreement with the use of substances, or even active participation with the client (e.g., going out for a few drinks together, providing marijuana and getting “stoned” together).
The concept of moderation is acceptable for some people but for anyone with a past history or current use of substances, the best advice health care professionals can offer is to avoid all substances at all times. The risk of dangerous interactions with medications or further injury from the effects of these chemicals is too great to offer anything but abstinence as an acceptable treatment goal. Considering the predisposing conditions and needs of the client, it is the position of the health care professional to offer, train, and support the individual toward integration of healthy options.266
Interaction of Alcohol with Prescription and OTC Drugs
The therapist should be aware of potential hazards of treating anyone who appears to have been consuming alcohol before coming to the treatment session. Physical therapists must know about all drugs clients are taking on a regular basis.
If the physical therapist suspects the client may be consuming alcohol in excessive amounts, remember that certain medications, both prescribed and OTC, have the potential for adverse reactions when taken with alcohol. Many of these adverse interactions can have a serious, negative impact on the physical therapy plan of care. Many medications, both prescription and OTC, contain significant percentages of alcohol. Some of the medications physical therapy clients may be taking (and their interaction with alcohol) are listed in Box 3-6.243
Smoking may especially exacerbate circulatory problems leading to foot amputation in people with diabetes. The detrimental effects of cigarette smoking on wound healing, ability to cope with pain, and peripheral circulation are well documented.
This population generally has a lower oxygen supply to the lower extremities because they are subject to advanced atherosclerosis. Since good oxygen supply is required for wound healing in soft tissue, it is imperative that people with a history of diabetes and smoking, now presenting with pressure ulcers or other foot complications, receive adequate arterial blood supply to the lower extremities (see Chapters 10 and 11).
Heavy smoking is commonly associated with chronic alcohol abuse, and both addictions have a negative influence on bone formation, probably the result of defective osteoblastosis. Women who smoke are at significantly higher risk of developing osteoporosis late in life and subsequent bone fractures compared with nonsmokers (see Special Implications for the Therapist: Osteoporosis in Chapter 24.)
The relationship between smoking and pain has also been documented, including an association with the incidence and prevalence of back pain in all ages. A link between smoking and back pain in occupations requiring physical exertion was also established possibly as a result of smoking-related reduced-oxygen perfusion and malnutrition of tissues in or around the spine, causing these tissues to respond inefficiently to mechanical stresses.63 Study findings may have implications for targeting at-risk groups for back care education or intervention programs.
The effects of tobacco use (see Table 3-3) have a direct impact on the client’s ability to exercise and must be considered when starting a treatment intervention or exercise program. Smokers are more likely than nonsmokers to suffer fractures, sprains, and other physical injuries even at an early age; these detrimental effects of smoking on injuries appear to persist at least several weeks after cessation of smoking.
All of the detrimental effects of tobacco need to be considered and discussed with women who are pregnant. Many lifestyle improvements occur when a woman and her family are expecting a child. Taking the time to educate your prenatal clients about the negative effects of smoking on fetal development, pain tolerance in labor/delivery, healing postpartum, and potential harm to her own body and family can have a significant positive impact.266
In addition to the overall effects of nicotine, inhaled nicotine has additional pulmonary effects. The combination of smoking and coffee ingestion raises the blood pressure of hypertensive clients about 15/33 mm Hg for as long as 2 hours,71 requiring careful monitoring of vital signs during exercise.
A clear need to increase the frequency of smoking cessation advice and counseling for all tobacco users is evident. However, the difference in receipt of advice to quit among racial/ethnic groups may be influenced by social or cultural factors. For example, among older Hispanic and Asian-American adults, language barriers may affect the lower rates of receiving advice to quit or in understanding the advice. Health care providers should offer culturally appropriate or tailored interventions for racial/ethnic populations.
In 1996 the American Physical Therapy Association (APTA) endorsed the Agency for Healthcare Policy and Research Clinical Practice Smoking Cessation Guideline. This has been superseded by a new, updated Tobacco Cessation Guideline released by the Public Health Service on June 27, 2000. The guidelines recommend that every client who smokes or uses tobacco products should be advised on the known dangers of tobacco use and increased success of smoking cessation programs. A Youth Tobacco Cessation Guideline has also been published.169
The therapist is often in a unique position as the health care professional that the client feels most comfortable with and able to trust for supportive education. Unequivocally, quitting smoking reduces the risk of cancer, cardiovascular disease, and pulmonary disease caused by continued smoking.59 Explaining some of the immediate and long-term benefits of smoking cessation may be helpful (Table 3-4). Younger people benefit the most, but even those who are 65 or older can add years to their life by quitting.227
Table 3-4
| Time Since Last Cigarette | Benefit |
| 20 minutes | Vital signs return to person’s baseline normal level (blood pressure, pulse, temperature) |
| 8 hours | Oxygen levels increase; carbon monoxide levels decrease |
| 1 day | Risk of myocardial infarction (heart attack) decreases |
| 2 days | Increased ability to smell and taste; nerve endings begin repair |
| 2 weeks-3 months | Improved circulation and lung function; reduced shortness of breath; improved exercise capacity |
| 1-9 months | Cilia in lungs regenerate, improving movement of secretions; reduced coughing and sinus congestion; decreased fatigue and increased energy levels |
| 1 year | Risk of coronary heart disease reduced to one-half that of a smoker |
| 5 years | Risk of lung cancer reduced by 50%; reduced risk of cerebrovascular accident (stroke); risk of oropharyngeal cancer (mouth, throat) reduced to one-half that of a smoker |
| 10 years | Lung cancer death rate corresponds to nonsmoker’s rate; risk of other tobacco-related cancers reduced |
| 15 years | Risk of coronary heart disease equals that of a nonsmoker |
From American Cancer Society, 2007 (www.cancer.org/).
Whenever possible, clients who smoke should be encouraged to stop smoking or at least reduce tobacco use before surgery and when recovering from wounds, pressure ulcers, or injuries resulting from trauma (including surgery) or disease. The National Cancer Institute (800-4-CANCER) provides educational materials for health professionals that contain practical steps toward stopping smoking.
Smokers trying to quit may benefit from a medication approved by the Food and Drug Administration (FDA), either nicotine replacement therapy (gum, inhaler, nasal spray, or patch) or a nonnicotine pharmacologic aid (e.g., bupropion [see Table 3-9]). The goal is to wean off of tobacco products and then to decrease and cease the use of pharmacologic aids.
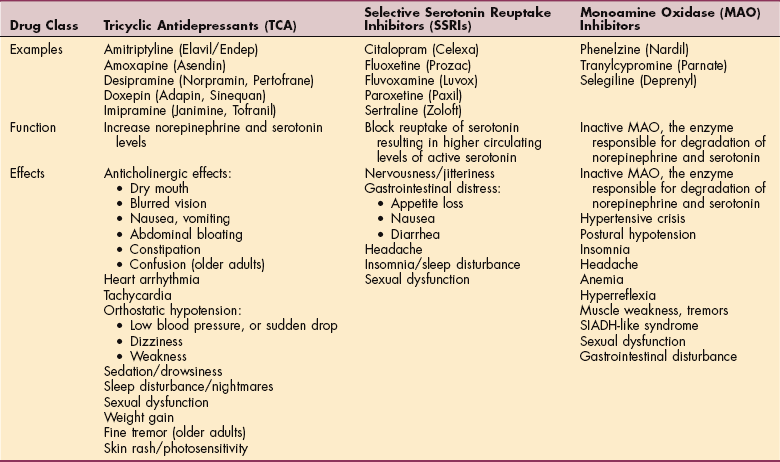
Alcohol; barbiturates; and similarly acting sedatives, hypnotics, and antianxiety agents are CNS depressants. Approximately 30% of hospitalized people, including older adults, are alcohol abusers, and many traumatic injuries occur as a result of excessive alcohol consumption.
Alcohol addiction, a prevalent problem in the acute care setting, often remains hidden until withdrawal symptoms appear. Alcohol withdrawal manifests itself with a wide range of symptoms that usually begin 3 to 36 hours after the last drink. The person may present with delirium, tremulousness, motor hyperactivity, anxiety and hyperalertness, irritability and agitation, diaphoresis, tachycardia, hypertension (to 200/100 mm Hg or higher), pounding headache, abdominal cramping, anorexia, nausea, vomiting, or diarrhea. Withdrawal may be accompanied by behavioral manifestations (e.g., aggression, uncooperative actions) or physiologic complications such as electrolyte disorders, dehydration, polyneuropathy, or myopathy.66
Whenever the therapist observes a cluster of these signs or symptoms, nursing or medical staff should be contacted to confirm the possibility of alcohol withdrawal and to discuss the implications for that individual in a therapy setting.
Alcohol affects many body systems (Fig. 3-2), but the effects on the neurologic and musculoskeletal systems are of particular interest to therapists. Alcoholic polyneuropathy is a degenerative process involving multiple nerves and occurs as a result of nutritional deficiencies associated with chronic alcoholism. It occurs most frequently between ages 40 and 70 and develops slowly over a long period.
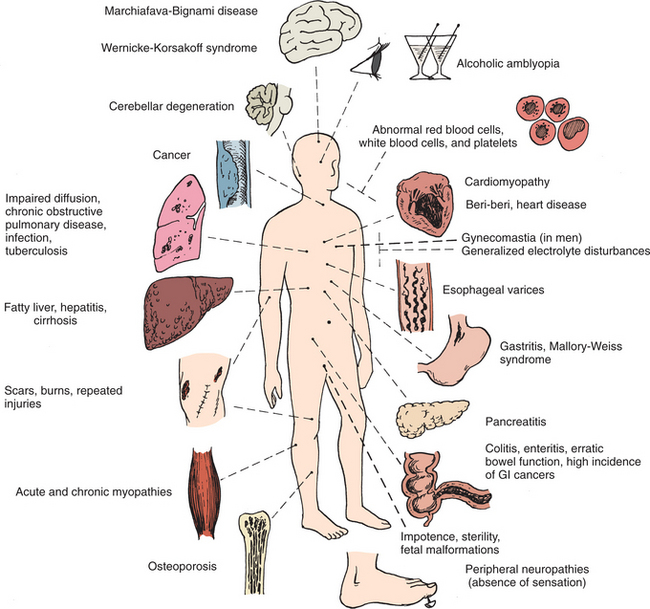
Figure 3-2 Clinical problems resulting from alcohol abuse. Not all of the conditions pictured in this figure are discussed in this text. (From Kneisel CR: Nursing care of clients with substance abuse. In Black JM, Matassari-Jacobs E, editors: Luckmann and Sorensen’s medical-surgical nursing, ed 4, Philadelphia, 1993, WB Saunders.)
Some people with neuropathies are asymptomatic, but neurologic assessment usually reveals varying degrees of motor, reflex, and sensory loss, which typically occur in the feet before the hands, moving distal to proximal. Sensory disturbances usually appear first and are described as tingling, pricking, burning, or numbing sensations.
Safety precautions are very important for people with diminished sensation (see Box 12-14) Calf muscles may be tender to the touch and diminished sensation and weak muscles may result in a wide-stance gait.
Alcohol ingestion may damage skeletal muscle, resulting in subclinical, acute, or chronic alcoholic myopathy. The pathologic process is the same as in alcoholic cardiomyopathy (see Chapter 12). Acute alcoholic myopathy is a syndrome of muscle pain, tenderness, and edema occurring after acute excesses of alcohol ingestion. The proximal muscles of the extremities, the pelvic and shoulder girdles, and the muscles of the thoracic cage are most commonly affected.
Symptoms may subside in 1 to 3 weeks with cessation of alcohol use but may recur with repeated alcohol ingestion. Treatment consists of a well-balanced diet with supplemental vitamins and abstinence from alcohol. Chronic alcoholic myopathy is characterized by muscle weakness and wasting, involving the same muscle groups described in acute alcoholic myopathy. Onset is slow and insidious with no history of pain or tenderness. Treatment intervention is the same as for acute alcoholic myopathy.
Prolonged use of excessive alcohol contributes to three known skeletal complications: a syndrome of nontraumatic hip osteonecrosis, deficient bone metabolism leading to osteomalacia and osteoporosis, and an increased incidence of fractures and other injuries secondary to trauma and falls. Impaired coordination caused by high blood alcohol levels is a contributing factor to falls.
Saturday night palsy, an injury to the radial nerve in the spiral groove, may occur during deep sleep in intoxicated persons. Prolonged compression of the radial nerve results in paralysis of the extensor muscles of the wrist and fingers. The nerve may be injured at or above the elbow; its purely motor posterior interosseous branch, supplying the extensors of the wrist and fingers, may be involved immediately below the elbow, but then sparing of the extensor carpi radialis longus occurs so that the wrist can still be extended. The triceps muscle is spared because of its more proximal nerve supply (see Chapter 39).
The use of chemical stimulants, such as caffeine, cocaine, and amphetamines, has a direct effect on the CNS and may enhance a person’s perception of pain. Pain can be relieved by reducing the daily intake of these chemicals, but care must be taken to avoid the withdrawal syndrome (e.g., symptoms of headache, lethargy, fatigue, muscle pain, and stiffness).
The negative effects of caffeine on TBI are also problematic for the therapist working with the agitation often present in this group. Caffeine may also act on the dopaminergic system of the brain, indirectly enhancing neurotransmission of dopamine and masking the symptoms of Parkinson’s disease. Higher caffeine intake is associated with a significantly lower incidence of Parkinson’s disease.202
The combination of exercise and caffeine can cause elevated blood pressure, especially for people with high blood pressure or healthy people with a family history of hypertension. People who know they have high blood pressure should avoid caffeine for at least 2 hours before a workout or strenuous rehabilitation session.99
Cocaine significantly increases the risk of having a heart attack in the first hour after using it, and this risk applies to people who are otherwise at low risk.170 The role that exercise may have in this phenomenon remains unknown but given the ability of cocaine to increase pulse rate and blood pressure, therapists must monitor vital signs to prescreen all clients in a rehabilitation or exercise program. People taking stimulants, such as cocaine and amphetamines, are easily provoked into aggressive, violent behavior. A calm approach is essential, and realistic goals for client behavior and rehabilitation are important.
Injection drug use is associated with a high rate of skin and soft tissue infections from the use of unsterile intravenous and subcutaneous injection (skin popping). This factor, combined with the presence of pathogenic microorganisms on the skin, results in a wide range of clinical problems from simple cellulitis and abscess to life-threatening necrotizing fasciitis and septic thrombophlebitis.
The clinical appearance is often atypical and subtle because of longstanding damage to the skin and to venous and lymphatic systems, resulting in underlying lymphedema, hyperpigmentation, scarring, and regional lymphadenopathy. The therapist may observe redness, warmth, and tenderness with tender inguinal or axillary lymph nodes. Skin ulcers resulting from skin popping consisting of low-grade foreign body granulomatous inflammation and necrosis are common and easily become superinfected, requiring local wound care, occasionally requiring skin grafting.
The effects of cannabis derivatives usually last a few hours and with repeated use, less of the drug is needed to produce the same effects. The agent persists in the body as an active metabolite as long as 8 days after use, so less of the drug is needed to produce the same effects during this time. As with any substance, clients are encouraged to eliminate the use of cannabis derivatives during the rehabilitation process. Relapse or worsening of symptoms in people with a history of psychologic disorders occurs with the use of cannabis.
Substance (especially alcohol) abuse can be a real problem among our own profession. Physical therapists should be able to recognize and deal with their colleagues who are abusing alcohol and other drugs. The following APTA position statement is directed toward the impaired professional5:
“The American Physical Therapy Association (APTA) recognizes the responsibility of the profession to meet the physical therapy needs of society; to promote the well-being of physical therapists, physical therapist assistants, and students; to uphold the ethical and legal responsibilities of the profession; and to follow the guidelines put forth in the APTA Board of Directors’ document Peer Assistance/Impaired Provider Program. Physical therapists, physical therapist assistants, and students shall address the problems associated with alcohol and substance abuse within the profession.
“APTA recognizes that alcoholism and other chemical dependencies are treatable diseases. Therefore, it is the duty of the physical therapist, the physical therapist assistant, and students to help themselves and their colleagues acknowledge that health and professional roles are adversely affected by these impairments. Additionally, APTA believes that appropriate treatment should continue to be available for impaired physical therapy practitioners and their family members to facilitate re-entry of practitioners into the profession as accountable and reliable professionals. Re-entry should occur when the well-being of the physical therapy practitioner and the patient/client are assured.
“The practitioner’s entry into the recovery process should be confidential and should be instituted in a non-punitive manner. APTA seeks to create a supportive environment for impaired physical therapy practitioners in their recovery and thereby enhance the well-being of its members and the profession.
“APTA encourages chapters to advocate for the establishment of non-punitive programs for impaired practitioners.”
Eating Disorders
Eating disorder is the general term used to describe an obsession with food and weight in adolescence or adulthood, including anorexia nervosa, bulimia nervosa, and binge-eating disorder (BED). According to the Harvard Eating Disorders Center,100 more than five million people in the United States experience these types of eating disorders.
The cause of eating disorders is unknown, although it is likely that a variety of factors (e.g., biologic, psychologic, sociocultural) affect whether an individual may develop an eating disorder. Typically, an underlying dissatisfaction with body image exists that is based on the faulty belief that weight, shape, or thinness is the primary source of self-worth and value.
Whereas an eating disorder is considered an illness, disordered eating is a reaction to life situations or a habit that can be changed through attending to the underlying need, education, self-help, or nutritional or other counseling. Disordered eating does not include persistent thinking and altered behaviors centered around body, food, and eating and does not lead to health, social, school, or work problems as is common with eating disorders. Disordered eating may lead to transient weight changes or nutritional problems but rarely causes major medical complications.
More recently, researchers have described a form of body image disturbance in male bodybuilders and weightlifters referred to as muscle dysmorphia. Previously referred to as “reverse anorexia,” this disorder is characterized by an intense and excessive preoccupation or dissatisfaction with a perceived defect in appearance even though the men are usually large and muscular. The goal in disordered eating for this group of men is to increase body weight and size. The use of performance-enhancing drugs and dietary supplements is common in this group of athletes.17
Risk Factors
Researchers are advocating moving away from female gender as a primary risk factor associated with eating disorders. An estimated 25% of eating disorder cases now occur in boys and men.109 Other more relevant risk factors for both sexes include personality traits or disorders (e.g., perfectionist, rigid, risk-avoidance)98; dieting and family history of eating disorders; and social pressure such as military personnel required to meet certain weight requirements, elite athletic performance, or activities valuing thinness (e.g., dance, gymnastics, modeling, acting).
Several groups of athletes are at greater risk for eating disorders. This includes women who participate in sports that emphasize the importance of low body weight, such as distance running; sports in which judging is based on aesthetic criteria, such as gymnastics and figure skating; and sports where being lean improves performance such as gymnastics or diving.
Men at risk are those who participate in sports that use weight classes such as wrestling and rowing. Horse-racing jockeys of both genders also exhibit these behaviors.223 Gay men tend to be more dissatisfied with their body image and may be at greater risk for symptoms of eating disorders compared to heterosexual men.124
A personal or family history of obesity, drug and/or alcohol abuse, depression, sexual abuse or other forms of trauma, or eating disorders is also a significant risk factor for eating disorders. Family issues, such as separation, divorce, overinvolvement, or abandonment, are also reported risk factors for development of an eating disorder.137
Up to 20% of women with type 1 diabetes mellitus have some kind of eating disorder; this in turn predisposes them to further complications with glucose control. The treatment of diabetes mellitus greatly emphasizes weight control, dietary habits, and food. This focus, combined with stress, poor self-esteem, and altered body image that can result from any chronic illness, contributes to the risk of eating disorders in this population.
MEDICAL MANAGEMENT
More needs to be done in the areas of prevention, early detection, and early treatment of eating disorders. Education efforts should be focused on girls in early middle school or junior high because of the rapid bone formation during puberty that will be necessary for the rest of their lives. Again, physical therapists are uniquely and ideally placed to identify the client’s presenting symptoms, attend to their underlying needs, and refer appropriately to other professionals.
Several national organizations provide valuable educational and prevention information (Eating Disorders Awareness and Prevention (EDAP): http://www.edap.org; National Association of Anorexia Nervosa and Associated Disorders (ANAD): http://www.anad.org). Women identified as meeting the criteria for the female athlete triad (see Clinical Manifestations in this section) should not be disqualified from athletic participation but rather provided with appropriate education and treatment intervention.
The prevention of eating disorders in at-risk college-age women has been demonstrated using an 8-week internet-based cognitive-behavioral psychosocial intervention. Women with high weight and shape concerns participated with follow-up for 3 years with significant weight reduction and decreased risk for eating disorders.226
DIAGNOSIS.
The gold standard for eating disorder assessment is the investigator-based interview: Eating Disorder Examination (EDE).65 Other self-report eating disorder questionnaires are also available based on population (males versus females, adolescents versus adults, acute versus chronic condition).
Diagnostic criteria may be taken from the American Psychiatric Association’s DSM-IV-TR6 (Table 3-5). Various laboratory tests may be performed to evaluate hormone levels in men and women, and imaging studies may include a dual-energy x-ray absorptiometry scan to evaluate bone density.
Table 3-5
Diagnostic Criteria for Eating Disorders
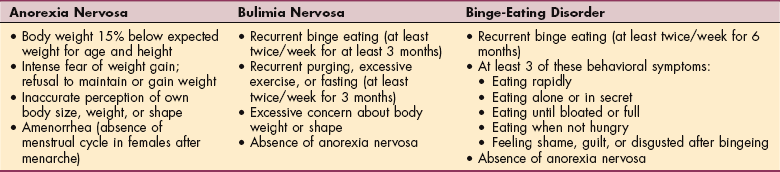
Bingeing is defined as eating large amounts of food at one time or over a short period of time.
Data from Hoffman L: Eating disorders, NIH Publication No. 93-3477, Bethesda, MD, 1993, National Institutes of Mental Health; American Psychiatric Association: Diagnostic and statistical manual of mental disorders-text revision (DSM-IV-TR), ed 4, Washington, DC, 2000, The Association.
TREATMENT.
Eating disorders can be treated successfully, but recovery is often a long process with a high risk of relapse. Overall, degrees of response range along a continuum. With good treatment, 70% of people with eating disorders can be cured. However, it may take years, and the chance of relapse on the road to recovery is as high as 30%.103
Anorexia Nervosa
Definition.: Anorexia nervosa is a refusal to eat. It is characterized by severe weight loss in the absence of obvious physical cause and is attributed to emotions such as anxiety, irritation, anger, and fear. This condition is characterized by distorted thinking, including a fear of becoming obese despite progressive weight loss, accompanied by the perception that the body is fat when it is underweight.
The person may use laxatives, diuretics, fasting, exercise, and self-induced vomiting to achieve additional weight loss. The effects of starvation have psychologic, emotional, and physical sequelae and medical complications that may lead to death.
Anorexia nervosa has been characteristically observed in adolescent and young adult females from middle-and upper-class families, often at or near the onset of menstruation (menarche), but this has spread now to include younger girls, boys, and all economic classes. Experts are exploring the genes that control hormone production as a potential underlying factor in the development of anorexia.
Etiology and Risk Factors.: An increased incidence of anorexia occurs among sports participants, especially sports that emphasize leanness, such as gymnastics, wrestling, diving, figure skating, and distance running, and in ballet dancers. Anorexia occurs in men in approximately 5% to 10% of cases; it is suspected that this figure is a low estimate, since it is likely that more males experience anorexia than what is made aware to health professionals.
Although attributed to psychologic and emotional factors (e.g., the need for control is a common variable; fear of growing up; fear of sexuality; rejection of self), the cause of anorexia remains unknown. During the past several decades, single-factor causal theories have been replaced by the view that anorexia nervosa is a multifactorial biopsychosocial disorder (Fig. 3-3).
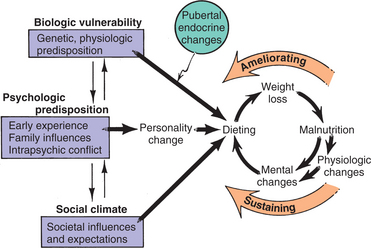
Figure 3-3 Biopsychosocial model for anorexia nervosa. See text discussion. (From Lucas AR: Toward an understanding of anorexia nervosa as a disease, Mayo Clin Proc 56:254, 1981.)
Specific early experiences and family influences may create intrapsychic conflicts that determine the psycho- logic predisposition. The challenges and conflicts of pubertal endocrine changes (biologic factors) may initiate the disorder. Social factors, such as the American cultural obsession with thinness, reinforce the pursuit of thinness.
The cumulative effect leads to dieting (a known risk factor for eating disorders) and other means of weight loss. This in turn results in malnutrition and starvation neurosis. The vicious circle of psychologic dysfunction fostering further dieting and psychologic denial becomes established and may lead to death.
More recently, pilot studies have found higher levels of homocysteine in women with anorexia compared to women with bulimia or healthy controls. Since homocysteine can induce neuronal cell death leading to brain atrophy and has been linked with depressive disorders, this finding has potential significance and remains the topic of further investigation.73,74
Anorexia may have a genetic component and possibly inherited biologic basis. Genetically transmitted variation in gene expression may play a role in vulnerability to anorexia.15,32 Although rare in the general population (2 in 1000), a person with a family history of anorexia has a 1 in 30 chance of developing it; a biologic twin has a 50% increased risk of anorexia when the twin sibling has this condition.219
The biologic basis for anorexia suggests that individuals who lose too much weight may trigger adaptive mechanisms designed for survival when in starvation conditions. Denial of starvation, hyperactivity, and food restriction may be characteristic of ancestral nomadic foragers leaving depleted environments. Genetically susceptible individuals may trigger these adaptations when they lose too much weight.50,97
Clinical Manifestations.: Besides the obvious lack of appetite and refusal to eat with weight loss, other signs and symptoms may occur as a result of starvation, vomiting, and chronic laxative or diuretic abuse (Box 3-7). These practices also lead to alternating periods of dehydration and “rebound” excessive water retention observed as swelling or reported as “puffiness” in the fingers, ankles, and/or face. Edema is usually noticed most immediately after vomiting and laxative abuse have been stopped.
Normalization of food intake and discontinuation of the purging practices will gradually reduce the wide swings in water balance, but the individual often becomes so alarmed at the sudden weight gain or swelling that they repeat the cycle by returning to vomiting or laxatives.80,237
Starvation seriously compromises cardiac functioning and when combined with electrolyte disturbances may result in life-threatening arrhythmias. Mitral valve pro- lapse (MVP) may occur secondary to starvation-induced decrease in left ventricular volume (see Special Implications for the Therapist: Mitral Valve Prolapse in Chapter 12).
Brain scans are abnormal in more than half of all anorexia cases and in some cases of bulimia nervosa. In both eating disorders, this condition appears to reverse itself with renourishment.235 Loss of body fat results in cessation of menstrual cycle (amenorrhea), hypothermia (cold intolerance), and the subsequent development of lanugo (the fine hair sometimes seen on the body of the newborn infant).
Skeletal myopathy with associated proximal muscle weakness from extreme weight loss may have a metabolic basis. This type of metabolic myopathy resolves with improved nutrition.165 Behavioral symptoms are listed in Box 3-8.
Bone density is decreased in anorexic and bulimic women, possibly resulting from estrogen deficiency, low intake of nutrients, low body weight, early onset and long duration of amenorrhea, low calcium intake, reduced physical activity, and hypercortisolism. This type of reduced bone density is associated with a significantly increased risk of fracture even at a young age.94
A new term, female athlete triad, is being used to describe the combination of disordered eating, amenorrhea, and osteopenia or osteoporosis, a situation that often goes unrecognized and untreated.48,204
MEDICAL MANAGEMENT
As mentioned earlier, diagnostic criteria may be taken from the DSM-IV-TR6 (see Table 3-5). Eating disorder assessments are valuable tools. Various laboratory and imaging studies may be performed to identify the effects of anorexia nervosa and plan a management program appropriately.
TREATMENT.
No universally accepted treatment for anorexia nervosa exists. A multidisciplinary approach is needed to normalize eating patterns and increase weight gain. Treatment can be difficult and lengthy if the eating disorder becomes entrenched or if medical complications exist. Treatment may include behavior therapy, demand feeding, behavioral contracts, psychotherapy, family therapy, nutritional counseling, and correction of nutritional status, which may require hospitalization.
Hospitalization is indicated if the body weight or body mass index (BMI) drops below a certain minimum (e.g., less than 16 BMI for adults), treatment-resistant bingeing occurs, or vomiting and/or laxative abuse persist.10 As mentioned, starvation-induced cardiac failure and death are possible.
Estrogen replacement, although beneficial in treating bone loss in menopause, has not been proven to prevent progressive osteopenia in people with anorexia. Recovery from this condition is associated with improved bone density.134,197 Researchers continue to investigate this issue with varied results and recommendations.31,127
PROGNOSIS.
The prognosis for individuals diagnosed with anorexia nervosa is very poor. This illness carries a significant risk of suicide.137 Although 84% of affected individuals achieve a partial recovery at some point in the course of the illness, the rate of sustained full recovery is approximately 33%.103
Bulimia Nervosa
Definition.: Bulimia nervosa is characterized by episodic binge eating (consuming large amounts of food at one time) followed by purging behavior such as self-induced vomiting, fasting, laxative and diuretic abuse, and excessive exercising. Before the 1970s, this disorder was relatively uncommon but since that time, its incidence has increased to exceed that of anorexia.
Etiology and Risk Factors.: The exact cause of bulimia nervosa is unknown, although low tryptophan levels (precursor to serotonin) have been implicated. Several theories include a primary neurologic dysfunction, an electrical disorder similar to epilepsy, disturbance in the appetite and satiety center of the hypothalamus, and a learned behavior for dealing with stress and unpleasant feelings. A vicious cycle of depression, overeating to feel better, vomiting and purging or fasting and exercising to maintain normal weight, and subsequent depression perpetuates this disorder.
Risk factors are the same as for anorexia nervosa, and the bulimic person has a preoccupying pathologic fear of becoming overweight despite the fact that she or he is usually within normal weight standards. The individual is usually aware that the eating pattern is abnormal, and self-recrimination is frequent.
Clinical Manifestations.: Unlike individuals with anorexia nervosa who restricts food as a means of gaining control over problems, people with bulimia react to distress by the binge-purge cycle.217 For many people with bulimia, the binge-purge cycle is initiated by a period of starving or extreme dieting and excessive exercising to lose weight. Periods of normal eating may occur, but the pattern of fasting or bingeing with compensatory behaviors (e.g., vomiting; fasting; use of diuretics, laxatives, or enemas) will resume at some point in time.
Whereas individuals with anorexia nervosa are severely undernourished, the person with bulimia nervosa may appear to be of normal weight or even overweight. The effects of bulimia nervosa are similar to self-induced vomiting in anorexia nervosa: erosion of the tooth enamel and subsequent dental decay, irritation of the throat and esophagus, fluid and electrolyte imbalances, and rectal bleeding associated with laxative abuse. Comorbid psychiatric conditions may include depression, anxiety disorders, substance abuse, and personality disorders.137
MEDICAL MANAGEMENT
In making the diagnosis of bulimia nervosa, the physician relies on physical findings, laboratory testing (e.g., electrolyte abnormalities, increased serum amylase levels), and diagnostic criteria from the DSM-IV-TR (see Table 3-5).
Controlled trials have established cognitive-behavioral therapy as the psychosocial treatment of choice for people with bulimia nervosa.8 Other treatment interventions may include interpersonal therapy, group therapy, antidepressants, and nutritional counseling.