chapter 6 The Regulation of Public Policy for Elders
1. Describe payment systems that influence practice developed as a result of public policy.
2. Clearly define the role of the certified occupational therapy assistant (COTA) within the Omnibus Budget Reconciliation Act (OBRA) regulations.
3. Describe the prospective payment system and COTA practice in different practice settings.
4. Learn ways that input of the COTA into the various screening measurements and care plans is valuable for an integrated team approach.
5. Learn the importance of advocacy for the occupational therapy (OT) profession.
6. Understand how COTAs can become more aware of public policy trends and changes that impact practice.
advocacy, care planning, Inpatient Rehabilitation Facility Patient Assessment Instrument (IRF-PAI), managed care, Medicare, Medicaid, Medicare Administrative Contractures (MACs), Minimum Data Set (MDS), Older Americans Act, Outcome and Assessment Information Set (OASIS), Omnibus Budget Reconciliation Act of 1987, prospective payment system, skilled services/unskilled services
Marie is a COTA who was invited to speak to a class of occupational therapy assistant (OTA) students about public policy. Marie began her lecture by stating, “Today we are going to discuss the influence of public policies such as Medicare and Medicaid on occupational therapy practice.” Marie scanned the faces of the students. They appeared to look disinterested. She observed students gazing out of the window, using their laptops to access the Internet, and a few stifling yawns. “Okay,” Marie slowly stated as she reorganized her thoughts, “I have decided to first share my story. In 1998 I was working for a rehabilitation company that contracted at several skilled nursing facilities in the area. I was making a very high salary—over $50,000 a year for a COTA just out of school! I didn’t think to question where that salary came from. Later I realized that to pay my salary the contract company must have been getting money from somewhere and that money possibly came from charging large amounts to Medicare for patient interventions. You see, Medicare was paid retrospectively based on what was charged after interventions. Today, as you will learn, cost measures have been established called ‘prospective payment,’ or payments paid ahead of time based on preestablished amounts. Anyway, one day your instructor Sally brought the OTA students to observe patients at the facility where I was employed. During a free moment Sally asked me if I had considered the impact of the Balanced Budget Act on my practice. ‘No,’ I responded. ‘I assume that my contract company will take care of me.’ You see, I never paid much attention to public policy. I found that subject far removed from my life, and, frankly, I was not interested. I was only interested in my patient interventions. My ignorance about public policy ended up affecting me personally, as in 1999, soon after the new law became instituted in skilled nursing facilities, I lost my job. The contract company reorganized because of the changes and I was among several rehabilitation personnel who lost their jobs. In a blink of an eye I went from earning $50,000 a year to being on unemployment, which was difficult as a single mother.” Marie paused and looked around the classroom and observed a group of attentive students gazing back at her. Marie continued, “I found myself reflecting about my career. What was I going to do? Should I enter another area of practice? The more I thought about it I realized that my passion was in working with elders. So I did a huge amount of networking and within 3 months I was lucky to be hired by a skilled nursing facility as an in-house staff therapist. Practice changed so I had to learn the prospective payment system. It was difficult at first but, eventually, I adjusted.
Now I pay close attention to policy trends, I have become involved in the state and national occupational therapy organizations, and I try to influence change by writing letters and making phone calls to the senators and congress people from this district. I even visited my representative while attending a conference in Washington, D. C. I never again want to be uninformed about public policy and its impact on practice. Practice will change again with any health reforms. I urge you to think beyond the classroom to how public policy can impact your lives as citizens and your professional practice.” As Marie continued with her lecture, the class was attentive.
As Susan, a member of the class, listened to the lecture she felt overwhelmed. She was thinking, How can I ever learn all this material so I can apply it in practice? How can I become more aware of changes in public policy that impact practice? These concerns bothered her so much that she asked Marie about them. Marie answered “I am glad that you asked those questions. Pay close attention now and review what I teach. In a year from now when you are out in practice, this information will fall into place. Be sure to learn how documentation and billing is done in your practice setting and don’t be shy about asking any clarification questions. Also, for those of you going into practice settings that receive Medicare payment be aware of the Centers for Medicare & Medicaid Services (CMS) website, which is a good resource, and there are many other resources online that can help you.” A year later Susan is employed as a COTA at a skilled nursing facility (SNF). She is very excited and feels prepared to work with the residents. As she overviews what she will do, she remembers the questions she had asked Marie and decides to review her course notes, study the policy and procedural manual at the facility, and question anything she needs further clarification about.
Introductory Concepts
Public policy develops from legislation at the federal and state levels and represents society’s values. (MacClain, 1996, personal communication) For example, the Medicare Act, which resulted in a national health insurance plan for elders, was enacted in 1965. Medicaid, a combined federal and state insurance program that addresses the health care needs of the indigent, was enacted in 1966. Both measures were enacted at a time when civil rights was valued by society and was reflected in many government acts that passed around that time such as the Developmental Disabilities Act and the Vocational Rehabilitation Act. The language of public policies is meant to be general. The specifics about each public policy are in its regulations, which COTAs need to comprehend because they directly impact OT practice. COTAs working in an SNF should understand the Omnibus Budget Reconciliation Act (OBRA) of 1987 and the prospective payment system (PPS) resulting from the Balanced Budget Act (BBA) of 1997 to provide appropriate care and be effective treatment team members. COTAs also must have a direct understanding of how Medicare and Medicaid is regulated in any setting to ensure that intervention they provide is reimbursed by third-party payers.
In this chapter, COTAs will overview key payment sources and related public policies that they will work with in practice settings. Medicare, Medicaid, OBRA, and the Older Americans Act (OAA) are examples of such public policies. The intent of this chapter is to provide an introduction and overview of these key public policies that influence therapy practice and how they are regulated. New policies are enacted, such as for health reform, and policies can also change with amendments and regulations. Therefore, not every specific detail of changes will be or can be included. For example, in 2010 a new Minimum Data Set (MDS) 3.0 and Resource Utilization Groups (RUG-IV) in SNFs was instituted and newer versions will come out in the future. With each version there are changes. One change with the MDS 3.0 was making it more client centered.1 With the chapter readers will get a strong foundation for practice and then will need to keep updated with changes through resources provided in the chapter. The chapter begins by discussing health care trends in the United States and then goes into specifics about federal public policies that influence OT practice and overviews health reform and Medicare. The chapter concludes with suggestions for COTAs on ways to keep up with public policy trends as well as promote changes with public policy through advocacy.
Health Care Trends in the United States
Health care in the United States is transforming rapidly as a result of a quickly changing society. A knowledge of these health care trends helps with understanding policies that develop. Previously, the family physician was the sole provider of health care. The physician knew individuals throughout their lives and treated them as whole people rather than as illnesses or diseases. Recently, the health care industry has undergone an extensive period of fragmented approaches to service delivery. The current trend, especially for elders, is toward comprehensive, cost-effective health care. Consumers want simplified access to a range of services with predictable costs. This has led to the emergence and growth of various public and private sources of health coverage. With health care reform systems will become even more integrated, and there will be a strong focus on quality, cost-efficient care. Electronic records as a result of public policy (e.g., the HITECH Act [P.L.111-5]2) will become a reality. Because health care is a large part of the gross national product and costs have been consistently increasing along with a growing aged population, ways to monitor costs with the major programs such as Medicare, Medicaid, and Social Security will be continually evaluated and discussed on the national agenda. The following sections describe public regulated sources.
Public Regulated Sources
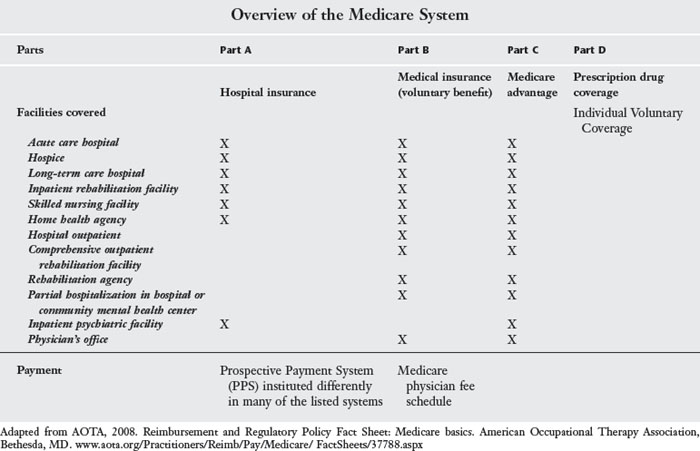
Public regulated sources include Medicare, Medicaid, federal and state employee health plans, the military, and the Veterans Administration. Medicare and Medicaid are often accessed by the elder clients whom COTAs treat and are discussed in the following sections. Please refer to Table 6-1 for an overview of the Medicare system that COTAs may work with.
Medicare
Medicare, or Title 18 of the Social Security Act, was first implemented in 1966. As part of the Social Security Amendment of 1965, the Medicare program was created to establish a health insurance program to supplement retirement, survivors, and disability insurance benefits. Originally, Medicare covered most people age 65 years and older. However, since then the program policy has expanded to cover other groups of people, including those entitled to disability benefits for at least 24 months, those with end-stage renal disease, and those who elect to buy into the program.3 Medicare is the largest entitlement program in the United States, and other insurance companies often follow the same standards as set up by Medicare.
Parts of the medicare program and occupational therapy practice
Medicare is divided into four parts (A, B, C, and D).3 Parts A, B, and C directly influence OT practice. Part A refers to hospital insurance. It covers “inpatient care in hospitals, including critical access hospitals, and skilled nursing facilities (not custodial or long-term care). It also helps cover hospice care and some home health care. Beneficiaries must meet certain conditions to get these benefits.”4 OT practitioners (registered occupational therapists [OTRs] and COTAs) follow Medicare beneficiaries under Part A in many settings both inpatient and outpatient (see Table 6-1). In most settings, therapy is reimbursed under a PPS. PPS are rates established in advance, based on the anticipated resource usage by the Medicare beneficiary and are “a pre-determined fixed amount.”5 These rates can be based by time, such as a per diem amount provided per case or per episode. Rates can also be established by a patient classification system such as with the diagnostic-related groups (DRGs) used in inpatient hospitals or the resource utilization groups (RUGs) used in SNFs.6
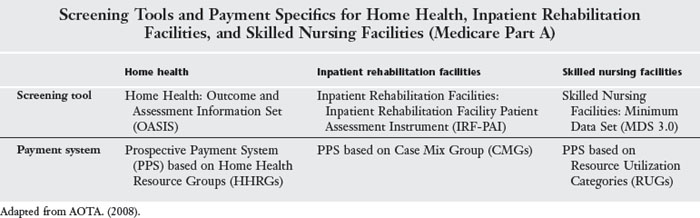
Medicare Reimbursement under Part A as a PPS system was first instituted in inpatient acute hospital settings in 1983 based on a DRG patient classification system, and this system continues today.7 PPS in each system (e.g., hospital, home health, SNF) is instituted differently, so COTAS will need to understand the specific system they work in. For example, in inpatient hospitals costs are bundled into the PPS rate. Some of the systems have a specific screening tool, such as the minimum data set (MDS) in SNFs. For an overview of screening tools and payment systems for Part A in home health, inpatient rehabilitation facilities, and SNFs, refer to Table 6-2.
TABLE 6-2 Screening Tools and Payment Specifics for Home Health, Inpatient Rehabilitation Facilities, and Skilled Nursing Facilities (Medicare Part A)
Medicare Part B is the medical insurance that covers “doctors’ services and outpatient care. It also covers some other medical services that Part A doesn’t cover, such as some of the services of physical and occupational therapists, and some home health care.”8 Part B is a voluntary benefit, which is paid for by monthly premiums. The cost of this premium continues to increase. It is important for COTAs to be aware that Medicare beneficiaries pay 20% of their Part B costs unless they have purchased supplemental insurance.
Therapists can provide therapy and bill under Part B in many outpatient settings, including physicians’ offices, outpatient, home health services, assisted living, SNFs, and comprehensive outpatient rehabilitation.7 Certain regulations are required to be followed with Part B, such as getting physician certification and a plan for therapy that is approved by the physician. Therapy services are billed under a physician’s fee schedule using the Physician’s Current Procedural Terminology (CPT) codes. CPT codes are revised annually, and the amount of reimbursement is calculated on the basis of a number of factors. COTAs in collaboration with the OTR decide how to code delivered intervention. Codes describe outcomes. They may be service codes that are billed only once per day regardless of the amount of time spent in delivering the procedure. Service codes include evaluation, reevaluation, splint application, and most modalities. Timed codes are the majority of the codes applicable to intervention provided by the COTA. Multiple units of timed codes can be delivered during a day of intervention. They are based on 15-minute units, and Medicare regulations guide how to calculate the units. For example, to count as 1 unit therapists follow a client between 8 and 22 minutes. This is also known as the 8-minute rule, and Medicare requires that time be accurately recorded for timed codes. (Please refer to CMS Internet manual 100.4, Chapter 5, Section 20.2. for more information.)
HCPCS Level II are another type of coding used for “products, supplies, and services not included in the CPT codes, such as ambulance services and durable medical equipment, prosthetics, orthotics, and supplies.”9 CMS has also instituted for Part B claims national coding methodologies to avoid misuse of billing procedures based on a policy called the Correct Coding Initiative (CCI).10,11 The purpose of these edits is “to prevent improper payment when incorrect code combinations are reported.”10
Currently Medicare beneficiaries who purchase Part B coverage have a therapy cap, or set financial amount, per year that they can use for all of their outpatient rehabilitation costs (occupational therapy, physical therapy, and speech therapy), except for hospital outpatient costs, which is exempt from the therapy cap. Over the years, the American Occupational Therapy Association (AOTA)12 has advocated for adding an exception process to extend coverage for certain conditions that may warrant more therapy, and AOTA is working on a permanent fix for the therapy cap. (More information on therapy caps can be found in IOM 100-04, Chapter 5, Section 10.2.)
Part C “are health plans offered by private companies approved by Medicare.”13 Part C includes the basic services covered by parts A and B and is covered by a variety of payment types such as managed care, fee for service, and medical savings accounts. Some plans have offered more benefits than the traditional Medicare plans. Medicare Part D is the outpatient prescription drug coverage, an optional benefit. Although this part of the law does not directly influence occupational therapy practice, therapists may want to read more about it on the CMS website.
General Guidelines for OT Payment and Intervention
Table 6-3 overviews examples of justifiable therapy service. Professional therapy intervention should be developed according to client needs relative to the complexity and intensity of required intervention. Intervention plans should be based on function and must integrate the plan of care. Intervention should be reinforced by other disciplines, such as skilled nursing. The client’s prior level of function, mobility, and safety in addition to self-care deficits are primary and essential indicators for professional intervention and must be reflected in assessments.14 COTAs should understand and follow specific guidelines to receive payment and not have a claim denied, such as receiving a denial for not having the physician sign off on the plan of care.
TABLE 6-3 Justification for Professional Therapy Service
| Patient example | Justification |
|---|---|
| Hilde was admitted into an SNF to recuperate from hip replacement surgery. In addition, she was to learn to ambulate with a walker and independently perform ADL functions, particularly her own dressing. Once Hilde learned these skills, she might return to her retirement home apartment and receive home health care to ensure her continued progress and safety. | The immediate or short-term potential for progress toward a less intensive or lesser skilled service area exists. |
| Hilde was depressed and the COTA primarily treated her for depression rather than the total hip replacement. However, intervention may be considered skilled if the COTA could demonstrate that the intervention was directly related to motivating the client to safely perform ADL functions. | The philosophy and plan of intervention must realistically focus on achievement of outcomes for the specific phase of rehabilitation, such as being an inpatient in a skilled facility. |
| The COTA focuses on Hilde’s intervention on going home with safety considerations. | Intervention also must focus on the plan for the next expected phase such as outpatient or home care. |
| During intervention, the COTA should address short-term deficits in safely performing ADL functions. The OT intervention should also take into account the performance component of the client’s difficulty | Intervention is expected to address the type and degree of deficits and effects of other problems in relation to the short-term or interim goals with problem solving. |
| The COTA would thoroughly document changes in Hilde’s status and her motivational level. | The therapist must emphasize variances in the elder’s response to intervention and new developments. |
ADL, activities of daily living; COTA, certified occupational therapy assistant; OT, occupational therapy; SNF, skilled nursing facility.
Refer to the Medicare Benefit Policy Manual 100-0215 for specifics about occupational therapy coverage. Also refer to the personnel qualifications for occupational therapy assistants, which are discussed in the 2008 Physician Fee Schedule.16 See the Federal Register of November 27, 2007,17 for the full text. See also the correction notice for this rule, published in the Federal Register on January 15, 2008.18
Skilled and Unskilled Therapy
The concept of skilled and unskilled therapy must be understood to obtain reimbursement from Medicare for OT intervention. Skilled care involves specific guidelines. For example, in SNFs care is covered if performed under the supervision of a professional and ordered by a physician and provided on a daily basis. Care “must be reasonable and necessary for the treatment of a patient’s illness or injury” and “reasonable in terms of duration and quality.”19 Examples of unskilled services would be exercises that are repetitive in nature, or passive exercises to maintain range of motion or strength that do not require the involvement of skilled rehabilitation. Usage of heat as a “palliative and comfort measure” and routine assistance in dressing, eating, or going to the toilet, and positioning in bed should be considered as unskilled services (Table 6-4).19
TABLE 6-4 Skilled Occupational Therapy Services
| Patient example | Justification |
|---|---|
| Linferd: An 89-year-old client who recently had a stroke. Prior level of function was independent living at home. Because of hemianopsia and problem-solving difficulties, Linferd requires moderate assistance with ADL functions that require use of upper and lower extremities. He is motivated to do OT intervention. | Recent condition Identifiable functional deficits in performance areas with requiring moderate assistance with dressing and grooming upper and lower extremity |
| Gertrude: A 72-year-old client who recently had a total hip replacement. She is unable to safely dress and requires education in hip safety precautions. The COTA provides instructions for lower extremity dressing and other ADL functions. Intervention includes teaching safety precautions. | Recent condition (hip surgery) Safety concerns Identifiable functional deficit in lower extremity dressing |
| Fred: A 92-year-old client who recently sustained a right wrist fracture. He is right hand dominant. The client was independently performing ADL functions before his wrist was fractured. He now requires moderate assistance with ADL functions because of decreased ROM in the right upper extremity. The COTA provides a home ROM program and instruction in ADL functions. | Recent injury Functional deficits with ADL (dressing, feeding, and grooming) caused by difficulty with the performance component of ROM Prior level of independence Skilled expertise of the COTA needed to teach home ROM program |
ADL, activities of daily living; COTA, certified occupational therapy assistant; OT, occupational therapy; ROM, range of motion.
Although a client’s diagnosis is a valid factor in deciding the need for skilled services, it should never be the only factor considered. The key issue is whether the skills of a therapist are needed for the required services. Skilled therapy services cannot be denied on the basis of diagnosis. This was clarified in a CMS Program Memorandum as it relates to therapy services needed by individuals with a diagnosis of Alzheimer’s disease or other dementias.20 Before this memorandum, there had been many denials on the basis of having the diagnosis of Alzheimer’s disease. (Refer to the Internet Medicare Benefit Policy Manual19 for more information about skilled and unskilled services.)
Medicare Administrative Contractures
Since the inception of Medicare, the Centers for Medicare and Medicaid Services (CMS) has contracted out vital program operational functions (claims processing, provider and beneficiary services, appeals, etc.) to a set of contractors known as Medicare Fiscal Intermediaries (FIs) and Carriers. Currently, with contract reform throughout the United States, Medicare claim review and payment are monitored by Medicare Administrative Contractors (MACs). MACs determine local coverage determinations (LCDs). “An LCD is a decision by a Medicare administrative contractor (MAC) whether to cover a particular service.”21 Payment coverage from each MAC can vary, so it is important for COTAs to become familiar with their area MAC and pay attention to LCDs. COTAs can go to their MAC website to determine claims processing information, educational options, and any regulation changes.
Working with Medicare and Related Regulations in Different Payment Systems
COTAs work with Medicare beneficiaries in many different systems, including SNFs, home health, inpatient rehabilitation facility, hospital outpatient, comprehensive outpatient rehabilitation facility (CORF), rehabilitation agency, occupational therapy private practice, partial hospitalization programs, inpatient psychiatric facilities, and physician’s offices. In each setting therapy coverage will be different and “therapists need to conform to the requirements of the PPS” if that is part of the system.22 In this section COTAs will be provided with resources to help them best understand the systems that they end up working in. In addition, some key aspects of a few of the systems that they may practice in (SNFs, home health, and inpatient rehabilitation) will be overviewed.
The best resources for COTAs to understand practice in different systems reimbursed by Medicare is to overview the Internet resources on the CMS website. As stated earlier, regulations change and COTAs need to stay current. The online CMS Manual System is organized by functional areas (e.g., eligibility, entitlement, claims processing, benefit policy, program integrity). The Internet-only manuals address coverage in many systems and are most up to date. It is especially helpful to refer to The CMS, Benefit Policy Manual, Publication, 100-02, Chapter 15 (Covered Medical and other Health Services), Sections 220-230.22 The outpatient regulations in this manual form the basis of coverage for all therapy services. Specific policies may differ by setting. Different policies concerning therapy services are found in other manuals. When a therapy service policy is specific to a setting, it takes precedence over these general outpatient policies. Finally, keep in mind that all Medicare regulations are periodically reviewed and updated. The most current Medicare regulations will always prevail.22 Table 6-5 overviews Medicare resources that COTAS can go to understand different systems they may work in.
TABLE 6-5 Medicare Resources Online
| Resources | Information covered |
|---|---|
| 100-01: Medicare General Information, Eligibility, and Entitlement Manual | Provides general information on program requirements |
| RAI Manual | This manual provides information on how to code therapy sections for the RUGs IV and provides a lot of information about what is included in sections of the MDS 3.0 |
| 100-02: Medicare Benefit Policy Manuals | General coverage criteria and guidelines for various Medicare settings |
| 100-03 Medicare National Coverage Determinations (NCD) Manuals | Describes whether specific medical items, services, treatment procedures, or technologies can be paid for under Medicare |
| 100-04 Medicare Claims Processing Manual | Provides all of the billing and claims processing information |
Working in Skilled Nursing Facilities
As of 2006 the largest employer of COTAs has been in SNFs.12 Practice in SNFs is primarily influenced by the public policies of OBRA, Medicare, and Medicaid.
OBRA, a landmark act of Congress, is not influenced by budgetary concerns. This act focuses on elders’ rights, quality of care, and quality of life in the nursing home setting. OBRA went into effect in October 1990 and was revised with final rules published in 1995.23,24 Compliance with the OBRA regulation is necessary for a nursing facility to receive reimbursement from Medicare or Medicaid. This discrepancy between what is required for good care, rehabilitation, and dignity and what is funded can cause ethical and moral dilemmas for COTAs. Knowledge of the regulations that govern care can help the COTA advocate for the services the patients need.
Minimum Data Set
The OBRA law was the impetus for developing the screening tool of the MDS, as it “called for the development of a comprehensive assessment tool to provide the foundation for planning and delivering care to nursing home residents.”25 Working in SNFs, COTAS need to be aware of the MDS because this screening tool identifies strengths and deficits that are recognized for further assessment. Many sections of the MDS address areas within the scope of OT practice. For example, COTAs might be able to add input to the cognitive patterns section among others. Data from OT practitioners contribute to the section on physical functioning (Figure 6-1). The MDS has been revised, and, with the MDS 3.0, the resident is involved in the assessment process and changes have been made in how data are collected for therapy.26,27
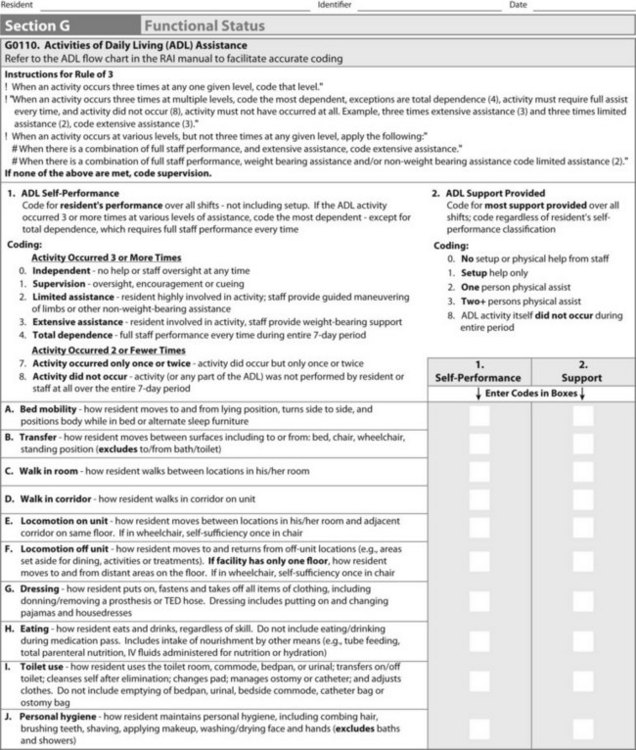
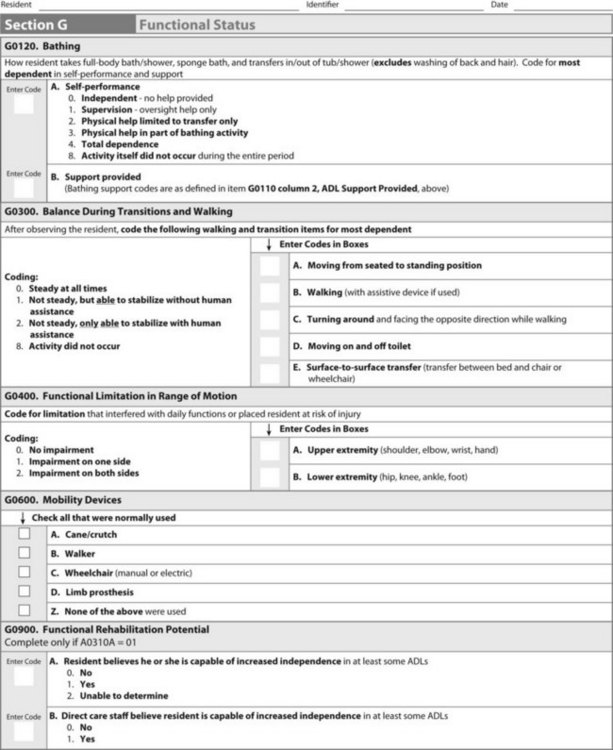
FIGURE 6-1 Example of the Physical Functioning and Structural Problems Section G of the Minimum Data Set 3.0.
Under the regulations for the PPS, a system that regulates Part A payments in SNFs, the MDS is also used to determine Medicare payment for those residents who meet the eligibility qualifications. OT intervention influences that payment system, and COTAs may be responsible for tracking minutes of intervention for sections of the MDS. Even if no intervention has taken place, the data collection and resident interview may help COTAs give the necessary information to others on the interdisciplinary team. If COTAs complete any portion of the MDS assessment, they must certify accuracy of the section(s) they complete by noting their credentials and the date and indicating the portion of the assessment completed. The signature of a registered nurse is required to certify completion of the assessment.
The Prospective Payment System in Skilled Nursing Facilities
COTAs need to be aware of the PPS in SNFs. The PPS was established by the Balanced Budget Act (BBA) of 1997.28 These regulations were created to control the increasing costs of health care with Medicare A in SNFs. Reimbursement occurs prospectively on the basis of a level of care or an anticipated level of care rather than retrospectively on the basis of what was charged. The final rule governing PPS was published in July 1999.29 Under this rule there were significant reimbursement changes in SNFs, and the impact on the delivery of therapy services was monumental. One of the big changes impacting practice was the organization of patients into RUGs. RUGs are determined by the number of therapies providing intervention (physical occupational or speech), therapy minutes that the Medicare beneficiary has used in the first 7-day reference period or is expected to use, need for services (e.g., respiratory therapy), specific medical conditions (e.g., pneumonia), and ADL score based on an index.30 RUGs categories for therapy vary from a low to ultra high categories and can be combined with extensive services (refer to the RAI manual listed in Table 6-5). As regulations change and to learn more about the specifics, COTAs need to refer to the aforementioned Medicare coverage manuals in Table 6-5. Box 6-1 provides some hints for operating in an SNF under a PPS system.
BOX 6-1
Operational Hints for Working in a Prospective Payment System (PPS) in a Skilled Nursing Facility (SNF)
 Communicate well with other members of the interprofessional team to coordinate care.
Communicate well with other members of the interprofessional team to coordinate care.
Know guidelines for PPS and the Resources Utilization Groups (RUGs).
Know approximately how many minutes of intervention are needed to generate desired outcomes and for type of therapy you are providing (individual, concurrent, or group).
Recognize that timing of therapy is critical for working effectively within this system.
Obtain therapy orders before admission for effective planning.
Prioritize care by dividing therapy minutes based on resident needs and desired outcomes.
Begin therapy with treatment minutes as soon as possible using good judgment based on the resident’s health status.
Be organized and track time accurately to the minute. If the number of qualifying minutes is not achieved, the resident’s status with the RUGs will default to a lower category.
Adapted from Flanagan, J. (2009 & 2010). Guide to Prospective Payment System; Linda Spurrell, July 26, 2010, personal communication.
Medicare Coverage for Home Health
The BBA of 1997,28 as amended by the Omnibus Consolidated and Emergency Supplemental Appropriations Act of 1999,31 called for the development and implementation of a PPS for Medicare home health services. The following discussion overviews the Medicare regulations for the home health system.
Eligibility for Medicare Part A home health services does not require a 3-day hospital stay as is required for Part A eligibility in skilled nursing homes. However, the elder must be homebound, have a physician’s referral, and require skilled services. Homebound means that it is not recommended that the person leave the home and leaving the home requires considerable effort and help.32 The elder does not have to be bedridden.33 Visiting a physician is an example of a legitimate reason to leave the home. With revisions of the law home health eligibility has broadened to include “participating in therapeutic, psychosocial, or medical intervention in an adult day-care program and occasional absences from the home for nonmedical purposes, for example, an occasional trip to the barber, a walk around the block or a drive, attendance at a family reunion, funeral, graduation, or other infrequent or unique event.”33 A client does not qualify for Part A home health services based solely on the need for OT. Nursing, physical therapy, or speech-language pathology must first open the case. However, OT may be introduced along with these other services and may continue after the other services have ended.34 The legislative attempts to change these qualification regulations continue but have been unsuccessful so far.
The regulations for HHAs are, of course, quite extensive. With assessment, the Outcome and Assessment Information Set (OASIS) is a key component of Medicare’s partnership with the home care industry to foster and monitor improved home health care outcomes. It represents core items of a comprehensive assessment for an adult home care patient and forms the basis for measuring patient outcomes for purposes of outcome-based quality improvement. Most data items in the OASIS were developed as systems of outcome measures for home health care. The items have use for outcome monitoring, clinical assessment, care planning, and other internal agency-level applications. OASIS data items encompass sociodemographic, environmental, support system, health status, and functional status attributes of adult patients. In addition, selected attributes of health service use are included. Refer to the Medicare online manuals listed in Table 6-5 for more information about current regulations on the CMS website.
Medicare in Inpatient Rehabilitation Facilities
COTAs employed in inpatient rehabilitation facilities (IRFs) will need to be informed about how the system works because there are very unique regulations for this area of practice. An admission regulation is called the “75% rule.”35 Although still called this, legislative changes now require that 60% of the admitted patients have one of 13 diagnoses. Examples of diagnoses are stroke and amputations.35 Similar to other settings, IRFs follow a PPS system for Medicare Part A beneficiaries. This PPS system establishes residents in one of numerous case mix groups (CMG) based on a screening tool called the Inpatient Rehabilitation Facility Patient Assessment Instrument (IRF-PAI) and a customized Functional Independence Measure (FIM). The customized FIM evaluates the client and assigns the client to a CMG. The IRF-PAI is used to establish client categories.11 COTAs can contribute functional information to the assessment process. As in other health care settings (SNFs and inpatient hospitals), there are time limitations that influence therapy. In IRFs, COTAs and OTRs provide intensive rehabilitation in 3-hour time blocks per day along with physical therapists and speech therapists. Patients need to be able to tolerate this level of intensive therapy.35
Medicaid
Medicaid is a health insurance “for low-income individuals and families who fit into an eligibility group that is recognized by federal and state law.”36 Because such a large portion of Medicaid dollars goes toward financing long-term care coverage,37 COTAs should become aware of this important public policy. States must provide basic health services, including inpatient and outpatient hospital services, laboratory and x-ray examinations, nursing facility services, physician and nurse practitioner services, and family planning services. State administrations can choose to cover any of 30 or more optional services, including OT. States also have been required to ensure that descriptions of their services meet federal guidelines and that all Medicaid recipients are treated equally.38
In many states the Medicaid program is administered as a managed care plan. Medicaid pays a high percentage of nursing care expenditures in the nursing home industry. Because of funding restrictions, Medicaid places an emphasis on institutional care rather than on other options that might permit elders to remain in their communities. However, the degree of emphasis varies among states because some have waiver programs and demonstration projects that involve broader funding for innovative programs and nontraditional care management. As Evashwick39 states, “An extremely important feature of the public long-term care system is the lead role that state governments have in shaping the characteristics of local financing and delivery systems for long-term care services.” Thus, the Medicaid program varies considerably from state to state and within each state over time. Because of these variances, the COTA must have access to local information and be an advocate for OT on local and national levels. In addition, COTAs should become aware of major changes that may occur with the health reform law, including expanded Medicaid coverage to populations under age 6537 and other demonstration projects that may influence care of their elder clients.
Managed Care
Elders may be in a managed care plan whether in Medicaid or Medicare Part C. Managed care organizations manage the care given to consumers and often involve the entire range of utilization control tools applied to manage the practice of physicians and others, regardless of practice setting. With Medicare Part C, care may be managed through a health maintenance organization (HMO) or preferred provider organization (PPO). Reimbursement rates to managed care providers are capitated, meaning that a set rate is provided either per intervention or per condition. This payment may sometimes not be enough to include extensive therapy. The OTR/COTA team needs to familiarize itself with the type of managed care services their clients may be receiving, emphasize in documentations the functional intervention they provide, and advocate for services if there are any issues.
Older Americans Act
In 1965 the Older Americans Act (OAA)40 was enacted to provide services for elders. The premise of OAA was that services provided to elders at least 60 years of age would enable them to remain in their homes and communities. Funding was established for nutrition programs, senior centers, transportation, housing, ombudsman, and legal services. Differences in these programs exist among states because administration is at the state level. In addition, more opportunity for OT involvement exists in some regions than in others. The original OAA was designed to foster independence, but rehabilitative services were not included. The act established the Administration on Aging, an agency specifically responsible for developing new social services for elders. COTAs should pay attention to the OAA when it is reauthorized because some of the changes may help their clients. It is also beneficial for COTAs to become aware of services offered by their local office on aging because many of these services can help their clients.
Trends with Federal Health Care Policies: Health Care Reform
As of this writing the Patient Protection and Affordable Care Act,41 as amended by the Health Care Education Reconciliation Act of 2010,42 will result in sweeping changes in our health care system as it is gradually instituted between 2010 and 2020. Parts of the law related to Medicare directly influence the provision of health care of elders. With health care reform the basic benefit package of Medicare will remain unchanged. Medicare beneficiaries will continue to receive their health insurance and physicians and hospitals will continue to be reimbursed per procedure.43 However, new changes with the law involve adding provisions to help elders manage their health care. Examples of these changes are gradually closing up in Medicare Part D, the voluntary prescription drug program that was known as the “donut hole.” The donut hole referred to a coverage gap in which elders had to pay out of pocket for their prescription medications. Another change with health reform is that subsidies will be offered for people with low income for Part D (prescription drug coverage). Preventive services in medical areas, such as Medicare financing annual physicals and regular colon screens will become covered benefits. With Medicare Part C (Medicare Advantage plans), reforms include restructuring and reducing payments and providing bonuses for quality programs. There will be many other cost savings provisions, which are predicted to save the Medicare program billions of dollars. Delivery reforms such as reducing hospital payments linked with needless readmissions or hospital-acquired infections44 will hopefully improve quality of care and decrease unnecessary spending. It is believed that the changes to Medicare will extend the solvency of the Hospital Insurance Trust Fund for Part A in the next 10 years.44
A voluntary long-term care insurance program, or the Community Living and Assistance Services and Support Program (CLASS), will help citizens finance long-term care services and supports.45 It is also important to be aware of pilot programs because they may eventually influence practice. One such pilot program is bundling the costs for delivery of post-acute care for Medicare beneficiaries. Finally this historical legislation is yet to be settled and more changes may occur as the makeup of Congress fluctuates.
Advocacy for Elders
Health care is always in a state of flux that directly affects OT practice. To deal with constant changes advocacy is important to any profession. Eleanor Roosevelt once stated, “Every person owes a portion of his time and talent to the up building of a profession to which he/she belongs.”46
Involvement of COTAs in advocacy for elders and the OT profession can make a difference. Advocacy is clearly discussed in the Occupational Therapy Code of Ethics and Ethics Standards.47 As stated in Principle 4 Part D of the Occupational Therapy Code of Ethics, therapists should “advocate for just and fair intervention for all patients, clients, employees, and colleagues, and encourage employers and colleagues to abide by the highest standards of social justice and the ethical standards set forth by the occupational therapy profession.”47 Part E states that therapists should “make efforts to advocate for recipients of occupational therapy services to obtain needed services through available means.”47
Every COTA and OTR must encourage the benefits of OT and establish the role of the profession within society. COTAs must stay informed about all government decisions regarding health care (Table 6-6). The rapidly changing face of today’s health care economy demands innovative and progressive responses from individuals. OTRs and COTAs must be strong advocates for their profession and the clients that benefit from OT intervention by adjusting to change and adapting to new ways to deliver intervention. An example of a direct benefit of advocacy with CMS was the successful effort to get clarification of coverage for patients with the diagnosis of Alzheimer’s disease.48 Box 6-2 provides suggestions for ways that COTAs can become more involved with public policy and advocacy.
TABLE 6-6 Nonskilled Occupational Therapy Services
| Example | Justification |
|---|---|
| Gwendolyn: A 69-year-old client diagnosed with right cerebral vascular accident. Previously, she performed all ADL functions independently. On initial evaluation, Gwendolyn was able to perform ADL functions independently but slowly. Her status on initial evaluation was independent with ADL, although performance was slow. | Slow performance with ADL functions is not significant enough to require the intervention of a skilled practitioner. The client will likely improve on her own over time without intervention. |
| Sebastian: A 75-year-old client diagnosed with rheumatoid arthritis. OT was ordered to provide an adapted pencil gripper to assist with writing. The COTA provided the gripper. | Intervention does not require the skilled expertise of the COTA. Anyone could provide an adapted pencil gripper. |
| Bob: A 74-year-old client diagnosed with Alzheimer’s disease. He is dependent in feeding. The COTA monitors feeding three times a week for 2 weeks. | The client’s condition is chronic and has not shown significant improvement. Intervention is routine therefore not requiring the skilled expertise of the COTA. |
ADL, activities of daily living; COTA, certified occupational therapy assistant; OT, occupational therapy; ROM, range of motion.
BOX 6-2 Ways for Certified Occupational Therapy Assistants to Become Involved with Public Policy and to Advocate
Be able and ready to articulate a clear definition of occupational therapy (OT) for the public; be visible.
Regularly access the American Occupational Therapy Association (AOTA) website, the Centers for Medicare & Medicaid Services (CMS) website, and their Medicare Administrative Contracture (MAC) website to keep abreast of public policy trends.
Serve on OT task forces and committees on a state or national level.
Become involved in advocacy groups in other associations related to therapy practice with elders, such as the AARP and the Alzheimer’s Association.
Read public (Web-based) and OT literature as much as possible to keep up on trends. Write and submit articles to professional and consumer publications about OT practice and public policy.
Find a mentor who understands public policy.
Write letters or visit people involved with public policy such as legislators, managed care and corporate executives, third-party payers, and case managers.
Learn the legislative process in your state and testify for relevant issues at public hearings.
If questions or concerns cannot be answered or addressed on a local level, network with the legislative division of AOTA.
Keeping Up with Changes
Let us return to Susan the COTA discussed in the opening scenario. On the first day of her job she meets with her boss Sonya. After reviewing some of the documentation and billing aspects of the job, Sonya asks Susan how she will keep updated with the frequent changes in regulations related to payment provision. Sonya challenges Susan to research that question and come up with ideas the next day when they meet. That evening Susan researches the CMS website and the AOTA website. She learns about and plans to follow postings on the CMS website called transmittals, which are used “to communicate new or changed policies, and/or procedures that are being incorporated into specific Centers for Medicare & Medicaid Services (CMS) program manual.”49 She finds manuals on the site that overview different Medicare regulations. Then she goes to the AOTA website. There in the Issues and Advocacy section she finds many resources to keep abreast with policy trends as well as practical suggestions for advocacy. She also finds the MAC site for her area and reads about regulation changes and looks at the LCDs. She searches further on the Internet and finds the AARP website that overviews extensive background related to public policy and advocacy. The next day when they meet again Sonya is pleased to learn about Susan’s efforts and states, “I hope that you make initiative to keep current from now on at least about this area of practice. In this rapidly changing health care environment I expect all my employees to be pro-active. I like to have monthly meetings where along with our practice discussions we educate and share about current health care changes and public policy.”
1. Name and describe the four parts of Medicare and those directly related to occupational therapy practice.
2. How is Medicare billed under Part B?
3. What is a Medicare Administrative Contracture (MAC), and how can it help inform practice?
4. Describe the prospective payment system used in skilled nursing facilities and how it influences therapy practice.
5. What is a resource utilization group?
6. What is Medicaid, and is OT a required or optional benefit?
7. What is home-bound status for clients in a home health care setting under Medicare Part A and allowable reasons for leaving the home?
8. What is the current assessment system used in home health care?
9. What is the current assessment system used in inpatient rehabilitation settings?
10. How can COTAs access the Older Americans Act (OAA) for their clients?
11. How might health reform influence practice?
12. How can COTAs be advocates for the OT profession?
13. How can COTAs stay aware of public policy changes that influence practice?
1 MDS 3.0 for Nursing Homes and Swing Bed Providers. Centers for Medicare & Medicaid Services. https://www.cms.gov/NursingHomeQualityInits/30_NHQIMDS30TechnicalInformation.asp#TopOfPage.
2 Health Information Technology for Economic and Clinical Health Act, 2009. Pub. L. No. 111-5, 123 Stat. 226, 467.
3 “What is Medicare?” Centers for Medicare & Medicaid Services. www.medicare.gov/Publications/Pubs/pdf/11306.pdf, April 2008.
4 . “Medicare Part A.” In Medicare Program: General Information. Centers for Medicare & Medicaid Services www.cms.gov/MedicareGenInfo/02_Part%20A.asp
5 . Prospective payment systems: General information. Centers for Medicare & Medicaid Services www.cms.gov/ProspMedicareFeeSvcPmtGen/
6 Robinson M., Bogenrief J. Introduction to reimbursement and documentation for the new graduate. Retrieved from http://www.aota.org/documentvault/conference/reimbursement.aspx, 2009.
7 AOTA. Reimbursement and Regulatory Policy Fact Sheet: Medicare basics. Bethesda, MD: American Occupational Therapy Association, 2008. www.aota.org/Practitioners/Reimb/Pay/Medicare/FactSheets/37788.aspx.
8 . “Medicare Part B.” In Medicare Program: General Information. Centers for Medicare & Medicaid Services www.cms.gov/MedicareGenInfo/03_Part%20B.asp#TopOfPage%20Part%20B
9 . Healthcare common procedure coding system level II coding procedures. Centers for Medicare & Medicaid Services www.cms.gov/MedHCPCSGenInfo/Downloads/LevelIICodingProcedures.pdf
10 . National correct coding initiatives edits. In Centers for Medicare & Medicaid Services www.cms.gov/NationalCorrectCodiNitEd/01_overview.asp
11 Robinson M. Medicare 101: Understanding the basics. OT Practice. 12(2), 2007. CE-1-7
12 2006 Occupational therapy compensation and workforce report. Bethesda, MD: American Occupational Therapy Association, 2006.
13 Medicare.gov. (n.d). Medicare advantage: Part C. Retrieved from http://www.medicare.gov/navigation/medicare-basics/medicare-benefits/part-c.aspx
14 Lubarsky, M., Swerwan, J.R., Schroeder, E.L., Duffy, J.L., 1995. Medicare resource manual: A guide through the critical steps Life Services Network of Illinois.
15 . Practice of occupational therapy. Section 230.2, Chapter 15: Covered Medical and Other Health Services. In: Centers for Medicare & Medicaid Services: Medicare Benefit Policy Manual https://www.cms.gov/manuals/Downloads/bp102c15.pdf
16 Centers for Medicare & Medicaid Services (CMS). Physician Fee Schedule. Retrieved from. http://www.cms.gov/apps/physician-fee-schedule/search/search-criteria.aspx, 2008.
17 . Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule, and Other Part B Payment Policies for CY 2008; Revisions to the Payment Policies of Ambulance Services Under the Ambulance Fee Schedule for CY 2008; and the Amendment of the E-Prescribing Exemption for Computer-Generated Facsimile Transmissions. Federal Register 72 (27 November 2007):66222-66578 http://edocket.access.gpo.gov/2007/pdf/07-5506.pdf
18 . Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule, and Other Part B Payment Policies for CY 2008; Revisions to the Payment Policies of Ambulance Services Under the Ambulance Fee Schedule for CY 2008; and the Amendment of the E-Prescribing Exemption for Computer-Generated Facsimile Transmissions; Corrections; Final Rule. Federal Register 73 (15 January 2008): 2567-2710 http://edocket.access.gpo.gov/2008/pdf/07-6308.pdf
19 . Chapter 8: Coverage of extended care (SNF) services under hospital insurance. In Centers for Medicare & Medicaid Services: Medicare Benefit Policy Manual www.cms.gov/manuals/Downloads/bp102c08.pdf
20 . Program memorandum intermediaries/carriers: Medical review of services for patients with dementia. Centers for Medicare & Medicaid Services: Transmittal AB-01-135 www.cms.gov/Transmittals/downloads/AB-01-135.pdf
21 . Chapter 13: Local coverage determinations. In Centers for Medicare & Medicaid Services: Medicare Program Integrity Manual www.cms.gov/manuals/downloads/pim83c13.pdf
22 . Chapter 15: Covered medical and other health services. In: Centers for Medicare & Medicaid Services: Medicare Benefit Policy Manual www.cms.gov/manuals/Downloads/bp102c15.pdf
23 Omnibus Budget Reconciliation Act, 1987. Pub. L. No. 100-20, 101 Stat. 1330.
24 Medicare and Medicaid Programs; Survey, Certification and Enforcement of Skilled Nursing Facilities and Nursing Facilities, 60 Fed. Reg. 50115 (Sept. 28, 1995)
25 . MDS long-term care. Continuity of Care Task Group http://continuityofcaretaskgroup.pbworks.com/MDS%20Long%20Term%20Care
26 . MDS 3.0 for nursing homes and swing bed providers. In Nursing Home Quality Initiatives. Centers for Medicare & Medicaid Services www.cms.gov/NursingHomeQualityInits/25_NHQIMDS30.asp
27 Keane Care. Preparing for MDS 3.0. Retrieved from http://www.keanecare.com/products/pdf/mds30-flyer.pdf, July 2010.
28 Balanced Budget Act of 1997, Pub. L. 105-133, 111 Stat. 329.
29 “Medicare program; prospective payment system and consolidated billing for skilled nursing facilities—Update; final rule.” Federal Register, 64(31 July 2001), 39562-39607.
30 Medpac. Skilled nursing facilities services payment section: Payment basics. Retrieved from http://www.medpac.gov/documents/MedPAC_Payment_Basics_08_SNF.pdf, 2008.
31 Omnibus Consolidated and Emergency Supplemental Appropriations Act of 1999.
32 . Medicare and home health care. Centers for Medicare & Medicaid Services http://www.medicare.gov/publications/pubs/pdf/10969.pdf
33 . Chapter 7: Home health services. In Centers for Medicare & Medicaid Services: Medicare Benefit Policy Manual www.cms.gov/manuals/Downloads/bp102c07.pdf
34 Youngstrom J.J. Reimbursement for home health services: Guidelines for occupational therapy in home health. Bethesda, MD: Commission on Practice Home Health Task Force; 1995.
35 . Coverage of inpatient rehabilitation services. Medical Learning Network, Centers for Medicare & Medicaid Services www.cms.gov/MLNMattersArticles/downloads/MM6699.pdf
36 . Medicaid program: General information. Centers for Medicare & Medicaid Services www.cms.gov/MedicaidGenInfo/
37 The Kaiser Commission on Medicaid and the Uninsured. http://www.kff.org/medicaid/upload/7334-04.pdf, 2010. Medicaid: A primer. Retrieved from
38 Sommers F.P., Browne S., Carter M.E. Medicaid: Current law and issues in reform proposals. Bethesda, MD: American Occupational Therapy Association; 1996.
39 Evashwick C.J. The Continuum of Long-Term Care. Albany, NY: Delmar; 1996.
40 The Older Americans Act of 1965, Pub. L. 89-73, 79 Stat. 218.
41 Patient Protection and Affordable Care Act, 2010. Pub. L. 111-148, 124 Stat. 119.
42 The Health Care and Education Reconciliation Act of 2010, Pub.L. 111-152, 124 Stat. 1029
43 Tumulty K., Pickert K., Park A. America’s new prescription: Will it work? Time. 2010;175(13):24-32.
44 Kaiser Family Foundation. Medicare: A primer. Retrieved from. 2010. http://www.kff.org/medicare/upload/7615-03.pdf.
45 Kaiser Family Foundation. Health care reform and the CLASS Act. Retrieved from http://www.kff.org/healthreform/upload/8069.pdf, 2010.
46 Scott S.J., Acquaviva J.D. Lobbying for healthcare. Rockville, MD: Government and Legal Affairs Division, American Occupational Therapy Association; 1985.
47 Occupational Therapy Code of Ethics and Ethics Standards. Bethesda, MD: American Occupational Therapy Association, 2010. www.aota.org/Practitioners/Ethics/Docs/Standards/38527.aspx.
48 Centers for Medicare & Medicaid Services (CMS). Statement of Tom Scully, administrator centers for Medicare & Medicaid services on therapy coverage of Alzheimer’s disease patients [WWW page]. URL http://www.hcanys.org/dementia/ AlzheimerScully4-1.PDF, 2002.
49 . Transmittals. Centers for Medicare & Medicaid Services www.cms.gov/Transmittals/