chapter 5 Aging Well
Health Promotion and Disease Prevention
1. Discuss how occupational therapy (OT) practitioners—registered occupational therapist (OTR) and certified occupational therapy assistant (COTA)—can influence health through programs and services for individuals, organizations, communities, and populations.
2. Identify methods of screening and assessment used in promoting health and well-being among elders.
3. Describe health promotion activities that can be incorporated into practice with elders.
4. Describe theoretical models that emphasize the importance of participation in meaningful occupations to decrease the negative effects of occupational imbalance, alienation and deprivation, and the promotion and the integration of healthy life patterns and routines.
5. Explain how the Healthy People 20101 goals of increasing quality of life and reducing health disparities may be carried out through OT practitioner services and programs.
6. Discuss the ways in which poor health practices, inadequate nutrition, and lack of self-care contribute to the incidence and prevalence of preventable diseases and disabilities common to elderly populations.
7. Identify factors that contribute most to influencing elders to participate in wellness-focused activities.
8. Describe factors that contribute to poor nutrition and obesity in elderly populations.
9. Name several lifestyle patterns that contribute to the development of preventable diseases in elderly populations.
health, occupation, occupational deprivation, occupational alienation, occupational imbalance, successful aging, wellness, health promotion, occupational form, occupational performance, disuse syndrome, prevention, primary prevention, secondary prevention, health and risk screening, tertiary prevention, nutrition/overweight/obesity, rest
(Adapted from Robert Browning by Ashley Montagu2)
Al is an 87-year-old man who hopes to live to be 100 years old. His wife Irene is 77 years of age and is content to have a few quiet hours each day to read and write letters. Al and Irene have been married for 56 years and have three adult children. They moved into a planned retirement community last year to ensure a safe living arrangement for whoever of the two lives longer. Al and Irene moved from their home of more than 40 years to this new environment with the help of a family friend.
After moving into their new home, Al and Irene often complained of feeling tired because of the demands of adaptation to their new environment. During the next few months, they organized their lives in their new setting. They laughed and talked about the process of getting to know some of their new neighbors. Overall, the move went well, and Al and Irene experienced the usual trials of adaptation to a change in most aspects of their lives: new home, changes in daily habits, patterns of time use and routines, adjusting to a different climate and learning about their neighbors, and availability and access to community services.
Al and Irene are among America’s fortunate well elderly. However, they are not without challenges. Al has been totally blind since he was 22 years of age. He has survived a cranial subdural hematoma, which was removed from the left side of his brain, and was recently treated with radiation therapy for prostate cancer. Irene has experienced many surgeries during the past 15 years, including a heart double bypass, cataract surgery, a hip replacement, a rotator cuff repair, and gallbladder removal.
These two elders enjoy a remarkable level of independence given their ages and medical histories. Some of this level of independence and relatively good health is a result of genetic endowment. In addition, lifestyle changes or other factors contribute to their good health such as regular exercise and a balanced, low-fat diet have influenced independence. Historically, they have not lived without health risk. Al and Irene smoked for some time but eventually quit at ages 55 and 52 years, respectively. They agreed to adjust their diets on the basis of some research that Al had read in his Braille health journals about the positive effects of reducing fat, sodium, and refined sugar intake. Their dietary habits changed approximately 28 years ago. About that same time, Al began walking regularly. Initially, he experienced pain from angina, which required him to stop walking, rest, and take nitroglycerin tablets prescribed by his doctor. After several weeks of daily walking and taking the prescribed medication, Al could finally complete a trip around the block without interruption. He increased the daily walks to eventually complete 2 miles each day, which he continues to maintain. At age 84 years he went to guide dog training school for 3 weeks to be suited with a new guide dog because his previous dog died. His new guide dog, Chelsea, helps Al stay independent and mobile. Irene often accompanies Al and Chelsea on their daily walk (Figure 5-1).
This scenario about Al and Irene’s transition from working to living in a retirement community offers many opportunities to consider how OT practitioners might help elders experience the richness of continued health and well-being with interventions and advocacy aimed at the person in context at the individual, organizational, community, and political levels. Al and Irene are well elders going through an adaptive process involving considerable demand and risk to their health because of the many stressors associated with movement from a familiar surrounding to the unknown of a retirement community situated in a different state. During their transition, the services of an OT practitioner would have been instrumental in facilitating adaptation to this new and unfamiliar community. The stress on Al to learn to navigate in his new home and neighborhood required considerable assistance in orienting his guide dog and familiarizing Al with new routes for his daily walks. Initially, Irene accompanied Al to offer support and guidance and to ensure his safety. Services offered through collaboration with OT practitioners would have been helpful and reduced health risks. To better understand the needs of elders experiencing similar circumstances, OT practitioners should consider evaluating the individual, the organization, and community to formulate a broad public health approach to interventions.
Since Al and Irene moved to a planned retirement community designed specifically to meet the needs of aging clients over age 55 years, some of the architectural and community adaptations needed to encourage and support occupational participation were included in the design of their home and neighborhood. Yet, in their case, little had been considered to accommodate the needs of blind and partially sighted elder residents. The community center and recreational group activities were not accommodating to a person without vision. Al did experience an increased sense of isolation when sighted retirees were unwilling to include him in card games at the community center because playing cards had been a source of pleasure and weekly socialization in his life before retirement. In this case, OT services and advocacy could be very instrumental in easing the transition through evaluation and interventions provided at the levels of person, community, and organization.
Health and well-being are intrinsically linked to participation in occupations that are meaningful. The risk of decline in health in this population emerges when barriers to participation exist. The outcome of occupational imbalance, alienation, or disruption in important life habits, patterns, and routines often lead to a sedentary lifestyle. A shift to sedentary living for well elderly can increase health risks associated with falling, limitations in mobility, increased likelihood of respiratory illness, and increased incidence of depression.
Al and Irene were able to overcome the barriers and challenges presented in their new environment despite increased stress associated with many adaptations. Services from OT practitioners in consultation with this planned retirement community would have improved the ease of their transition and reduced the risk to their health associated with such high demands on this elderly couple. OT practitioners play a vital role in support of elders and can serve as advocates in the development of policy and legislation to enhance life satisfaction and reduction of risk by creating systematic solutions to daily living challenges. Retirement communities designed to meet the needs of elderly populations have many necessary adaptations and safety devices in housing and neighborhood configuration but may lack services that help at-risk elderly continue to thrive once relocated.
This story could be about anyone. The later episodes of a life story itself depend, to some extent, on the self-care choices people make along the way. As health care providers, COTAs and OTRs can offer important health information and propose alternative lifestyle choices to elders. Society will increasingly look to health care providers for guidance and for models of healthful ways of living. This chapter describes the rationale for health promotion and disease or disability prevention programs that can be effective tools for use by COTAs working with elders.
Concepts of Health Promotion and Wellness in Occupational Therapy Practice
The historical roots of OT philosophy and practice demonstrate the profession’s long-standing belief in the value of occupation in promoting health and preventing functional loss caused by disease. Nelson and Stucky3 reviewed important OT values over the decades and wrote, “The potency of occupation in promoting health has long been recognized; this recognition is the basis for the existence of the profession of occupational therapy” (p. 22). Since the inception of OT as a profession in 1917, its premise has been to promote a healthy balance of activities for those persons who seek intervention. Activities perceived by an individual to be meaningful occupations are believed to influence the state of actual or possible health and well-being. Gilfoyle4 stated, “The therapeutic use of occupation to promote fullness of life is the basic value at the heart of our (professional) culture” (p. 400). The concepts of health and occupation are interrelated. Despite the various definitions and societal influences, the concept of occupation has remained centered on the value of activity to maintain enthusiasm about living. In essence, humans find meaning in what they do.4
The value of occupation and the meaning of health are explicitly interrelated.3,5-14 Nelson and Stucky3 described “activation of function (occupation) as a main method of health promotion and disease prevention” (p. 21). Yerxa14 further described this relationship between occupation and health in her working definition of occupation:
Occupations are units of activity which are classified and named by the culture according to the purposes they serve in enabling people to meet environmental challenges successfully. Some essential characteristics of occupation are that it is self-initiated, goal directed (even if the goal is fun or pleasure), experiential as well as behavioral, socially valued or recognized, constructed of adaptive skills or repertoires,13 organized, essential to the quality of life experienced, and possesses the capacity to influence health. (p. 5)
Richard15 suggested that health might be defined as “the ability to live and function effectively in society and to exercise self-reliance and autonomy to the maximum extent feasible, but not necessarily as total freedom from disease” (p. 79). Wilcox11 defined health from an occupational perspective as “the absence of illness, but not necessarily disability; a balance of physical, mental, and social well-being attained through socially valued and individually meaningful occupation; enhancement of capacities and opportunities to strive for individual potential; community cohesion opportunities; and social integration, support, and justice, all within and as a part of sustainable ecology” (p. 110). Wilcox12 advanced our perspective of the relationship between occupation and health by asserting that “occupation is clearly a pre-requisite to health” (p. 195), and that major risk factors to health include problems in occupational performance such as “occupational imbalance,” “occupational deprivation,” and “occupational alienation” (Table 5-1).
| Health risk factors | Wilcox | Brownson and Scaffa |
|---|---|---|
| Occupational imbalance | Occurs when people engage in too much of the same type of activity, limiting the exercise of their various capacities (p. 195) | A lack of balance among work, rest, self-care, play, and leisure that fails to meet an individual’s unique needs, thereby resulting in decreased health, well-being, or both (p. 657) |
| Occupational deprivation | When factors beyond them limit an individual’s choice or opportunity (p. 195) | Prompted by conditions such as poor health, disability, lack of transportation, isolation, unemployment, homelessness, poverty, and so forth (p. 657) |
| Occupational alienation | When people are unable to meet basic occupational needs or use their particular capacities because of intervening sociocultural factors (p. 195) | A sense of estrangement and lack of satisfaction in one’s occupations. Tasks or work perceived as stressful, meaningless, or boring may result in occupational alienation (p. 657). |
Data from Wilcox, A. A. (1999). The Doris Sym Memorial Lecture: Developing a philosophy of occupation for health. British Journal of Occupational Therapy, 62(5), 191-198; and Brownson, C. A., & Scaffa, M. E. (2001). Occupational therapy in the promotion of health and the prevention of disease and disability statement. American Journal of Occupational Therapy, 55(6), 656-660.
Occupational engagement can have a profound and positive effect on the lives of elders who are well and living in the community and can improve life satisfaction among frail elders living in skilled nursing or assisted living environments. Habitual activities, those which are performed with consistency, can have a profound influence on health. “What people do is so much a part of the ordinary fabric of life that it is taken for granted and its health benefits are largely ignored” (p. 194).12 Regular participation in a balance of meaningful daily occupations can prevent the development, occurrence, and progression of most disabling conditions. However, many elders have been typecast by society and health care professionals as being unable to improve their health status. This myth is detrimental to the health and well-being of older adults and dampens motivation to try to make small changes that could provide health improvements with small investments of time and effort.
Only in recent years has the literature associated with aging focused on healthy aging and long-term survival and moved away from medically oriented disease management. Recent literature suggests changing societal views of health and longevity. Promotion of “successful aging” (p. 107)5 will likely replace past views of disease remediation and control. “Shifting the focus from disease management and survival to health through disease prevention, health maintenance, and health promotion provides great promise for occupational therapy practitioners” (p. 10).16 The prevailing diseases contributing to morbidity and mortality among elderly people can be prevented through lifestyle changes.
Although leading causes of death or mortality, these diseases are also leading causes of morbidity or illness (Table 5-2). Morbidity can cause great suffering, occupational disruption, alienation, and cost. OT practitioners can educate clients about how to prevent or to control the long-range and deleterious effects of prevalent hazards to health and well-being. Nutrition, exercise, balance, and decreased stress, along with environmental adjustment for safety and management of medications, are a few examples of minor changes that can make long-range differences in health status. Regardless of age, unhealthy habits and patterns of living can be changed to improve health and to enhance life satisfaction.
TABLE 5-2 Leading Causes of Death by Age Group by Percentage of the Total Number of Deaths: United States in 2002
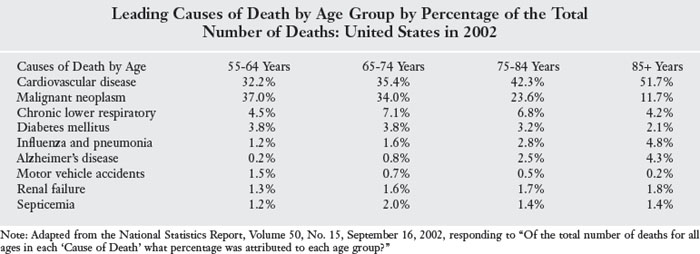
Carlson and colleagues5 asserted that “potentially controllable lifestyle factors play a crucial role in enabling people to experience healthy and satisfying lives well into old age” (p. 107). These authors proposed that an operational definition of aging in the future may in fact be the “disappearance of health” because careful living has such great potential to promote “successful aging” over a lifetime (p. 108).5 Research conducted by Carlson and colleagues5 provides insight into factors that lead to “successful aging” (p. 109) (Box 5-1). The concept that occupational therapy practitioners can “positively enhance lifestyle” (p. 299)17 is in line with the projected goals of the U.S. Department of Health and Human Services (DHHS) for a healthy population as established in Healthy People 2010.1 All OT personnel need to be aware of the major public health initiatives set forth in Healthy People 2010. The goals established in this document emphasize the need for increasing the quality of life of all people and prioritizing efforts leading to the achievement of a longer and healthier life for all citizens. Priority goals call for the elimination of health disparities on the basis of sex, race, ethnicity, disability, sexual orientation, education, income, or residence in a rural or urban setting.1 These goals fit well with the needs of the current elder population. As discussed in this document, the first goal of Healthy People 2010 is to increase the quality as well as the years of healthy life.1 Here the emphasis is on the health status and nature of life, not just longevity. The emphasis on functional capacity and the satisfying productive life of our citizens parallels occupational therapy’s focus on enabling engagement in a meaningful occupation, which supports and leads to productive and satisfying participation in life.18
BOX 5-1
Factors Contributing to Successful Aging
 Experiencing a sense of control over one’s life
Experiencing a sense of control over one’s life
Achieving continuity with one’s past
Participating in a social network of family and friends
Engaging one’s mind in complex cognitive activities
Adapted from Carlson, M., Clark, F., & Young, B. (1998). Practical contributions of occupational science to the art of successful aging: How to sculpt a meaningful life in older adulthood. Journal of Occupational Science, 5(30), 107-118.
OT practitioners have a responsibility and an opportunity to influence change in the quality of the lives of elders at the individual and also at the population levels by the implementation of health-promoting and wellness-centered programs. The 21st century is the time for needed health care reform, prompted by the urgency to reduce cost for care, and the time to return the responsibility for “successful aging” to the individual. Therapists should demonstrate leadership in helping individuals and communities plan health-promoting engagement in meaningful occupations as the path to a long and healthy life. “The organizing promise of occupational therapy emphasizes the important role of everyday activities or occupations in establishing routines and infusing meaning in daily life” (p. 13).19
Society is now better prepared to move toward health-centered, cost-effective approaches to prevention and wellness. Wellness has been defined as “a dynamic way of life that involves actions, values, and attitudes that support or improve both health and quality of life” (p. 656).18 An important projected outcome of health promotion is personal wellness.
Assisting people at all ages to actively participate in taking responsibility for improving the quality of their health is not unique to OT, but it has been a prominent value held by OT personnel since the inception of the profession. Health can be enhanced, and disease can be prevented through occupation. Occupational therapy interventions are provided at the institutional, legislative, and personal level of care, thus encouraging health at the environmental and personal levels. OT practitioners can be instrumental in creating healthy environments through consultation with state, city, and institutional levels of care. Political, economic, and practice environments need health professionals who understand the essential relation between occupation and health. As Mary Reilly20 stated in her Eleanor Clark Slagle Lecture of 1961, “Man through the use of his hands as energized by mind and will, can influence the state of his own health” (p. 2). Wilcox12 further elaborated this association between occupation and health status stating, “Ultimately, health is created and lived by people within the settings of everyday life; where they learn, work, play, and love” (p. 195).
Health Risks and Their Effects on Occupational Engagement and Participation
Substantial research evidence supports the need for increased health promotion and disease prevention activities for elders. Hickey and Stilwell21 maintain that the primary goal of health promotion programs for elders should be focused on prevention of “the progression of disease and the risks of disability and death that health promotion should be designed to help older persons maintain their functional independence and autonomy for as long as possible” (p. 828). Brownson and Scaffa18 define health promotion as “any planned combination of educational, political, regulatory, environmental, and organizational supports for actions and conditions of living conducive to the health of persons, groups, or communities, or—more simply—the process of enabling people to increase control over and to improve their health” (p. 657). Health promotion is focused on preventive efforts. The promotion of health must be considered in the contexts in which people live and relate to others. OT practitioners contribute to health promotion by first identifying those factors at the individual, group, organizational, community, and policy levels that interfere with occupational engagement. Wilcox13 suggests:
What people can do, be, and strive to become is the primary concern and that health is a by-product. A varied and full occupational lifestyle will coincidentally maintain and improve health and well-being if it enables people to be creative and adventurous physically, mentally, and socially. (p. 315)
As described by Fidler and Fidler,22 humans develop through “doing” and through “doing” become individuals. Through occupations, people adapt in both healthy and unhealthy ways. At times people learn maladaptive ways of living through occupational patterns. In daily practice settings, OT practitioners meet elders who can benefit from assistance in making positive choices to improve the quality of their health. Some elders do not recognize that the quality of their lives can change with even minor adjustments in their lifestyles. During daily therapeutic interactions, OT practitioners have an opportunity to influence their clients’ considerations of healthy lifestyles and assist them in improving the quality of their lives. Encouraging exploration of health-promoting activities and providing educational information to elders and their families may help motivate them to take actions that promote health and limit the potential for occupational deprivation, alienation, or imbalance associated with current habits (see Table 5-1). Elders are frequently uninformed or believe that changes later in life may offer few benefits. Helping elders understand the tremendous potential for healthy outcomes associated with small changes in daily routines can make the difference between future independence and debilitating dependence.
Nelson and Stucky3 suggest that “one’s occupational patterns of self-care and interests comprise … occupational situations (occupational forms) that are health promoting and disease preventing” (p. 22). The occupational form to which Nelson and Stucky refer includes the environmental context of the individual’s life. The context is composed of physical and sociocultural characteristics that stimulate the individual to choose an occupational performance. For example, an elder who lives in a retirement village may choose to play golf (occupational form) because there is a golf course on the grounds (physical characteristic), and this is where most people at that village socialize (sociocultural characteristic). The value that the person places on the occupational form gives meaning and purpose to the individual’s choice of actions. This sense of purposefulness is the motivator or stimulus that results in participation in activities such as playing golf. Playing golf on Thursday mornings may involve habituation of many occupational performance skills such as socialization, preparation of refreshments for guests, and the actual performance of playing golf. This involves motor performance, cognition, and other complex functions. Activation of an interest in and performance of a cherished occupation help the person establish a positive and continuous cycle or habit pattern. Fidler and Fidler22 theorize that imagery is linked with purpose. They perceive that actions related to achievement are a result of conceptualizing an image before taking action. Thus, mental imagery adds purpose to occupations. Mental images are constructed before taking action and facilitate the person’s participation (Figure 5-2).

FIGURE 5-2 Purposefulness stimulates participation in activities such as the hobby of playing cards.
The actual enjoyment of participation in chosen occupations or activities is referred to as intrinsic motivation.23 Baking a pie, walking a dog, and gardening are intrinsically motivated occupations. Actions taken toward a goal provide feedback that, if positive, may inspire continued participation in the activity or similar activities. Feedback may take the form of wonderful tomatoes from a well-nurtured garden or excitement from the completion of a small but meaningful project. Recognition from meaningful others can serve as a source of encouragement, and their enjoyment may motivate continued occupational engagement. Each interaction sets up the potential for additional involvement in occupations that ultimately contribute to growth, development, self-confidence, and improved self-esteem. Conversely, negative feedback or experiences may result in a cycle of feelings of fear, helplessness, humiliation, and failure.3
The outcome of an effective health promotion program is the enhancement or maintenance of function in activities of daily living (ADL), instrumental activities of daily living (IADL), and overall life satisfaction. The need for elders to maintain functional capacity, interests, and participation in meaningful occupations has been demonstrated by research findings suggesting that losses occur in the ability to perform ADL functions as a result of the disabling effects of disuse syndrome, a common sequel to physical and cognitive disabilities. Approximately 14.2% of elders living in the community experience difficulty completing one or more ADL because of health-related problems. Approximately 21.6% of elders report difficulties with IADL.24 Research shows that the need for assistance in the completion of ADL and IADL increases with age.1 Recently the U.S. Surgeon General and the Centers for Disease Control and Prevention have reported that limitations in ADL and IADL functions are key indicators of declining health and wellness.25 These authors go on to suggest that OT practitioners’ “prevention-oriented interventions” should include a public health focus by including evaluation data on population health. OT service should reflect population level services and describe population limitations, such as in the area of ADL, by measuring numbers of limits experienced in ADL as reflected in a simple scale of “no problem,” “1-3” difficulties, or “3 or more” difficulties. Measures of this type can be collected and data banked to large scale and multi-site studies reflecting indicators of population health.
McMurdo and Rennie26 report that elders in nursing homes who participated in a seated exercise group for 8 weeks showed significant improvement in grip strength, chair-to-stand time, and function in ADL, and they also experienced decreased feelings of depression. “Even very elderly residents of nursing homes can benefit from participation in regular seated exercise and can improve in functional capacity” (p. 12) (Figure 5-3).26 Unfortunately, research literature indicates that “despite the known importance of and preponderance of media attention to exercise, more than 60% of women over the age of 60 participate in little or no sustained physical activity of at least moderate intensity” (p. 602).27 Studies further indicate a correlation between fear of falling and a loss of physical endurance and strength. Nuessel and Van Stewart28 found that “35% of community dwelling elderly avoided doing things they wanted to do because they were afraid of falling” (p. 4). The fear of falling impaired choices of occupation and life satisfaction. Evidence supports that exercise programs can reduce falls by increasing endurance, improving balance, and improving confidence. Rubenstein and colleagues29 concluded:

A simple program of progressive resistance exercises, walking, and balance training can improve muscle endurance and functional mobility in elderly men with chronic impairments and risk factors for falls. In addition, this study provides new evidence on the complex relationship between physical activity and falls: exercise participants significantly increased their physical activity, yet experienced fewer falls per unit of activity. (p. 319)
Exercise has an effect on the mind and the body. As the body grows stronger, the individual’s self-confidence increases, and with positive changes come greater options for engagement in meaningful occupations.
Nutrition and Overweight or Underweight Elders
Balanced nutrition is essential to health maintenance and prevention of disease, obesity, and malnutrition in elders. OT practitioners can provide elders with important information and encouragement to ensure a balanced intake of foods high in nutrients and low in saturated fats, refined sugars, and sodium (Table 5-3). IADL include the activities of shopping and meal preparation. Selection and preparation of foods with high nutritional value, high fiber content, and portion control contribute to the maintenance of a healthy weight. The intake of a balanced diet can prevent or slow the progression of serious conditions, including diabetes, hypertension, and cardiovascular disease.
TABLE 5-3 Nutritional Standards Based on the Modified Food Pyramid for 70+ Adults
| Original pyramid | Modified pyramid | |
|---|---|---|
| Calcium, vitamin D, and vitamin B12 supplements | Not included | Daily |
| Fats, oils, and sweets | Use sparingly | Use sparingly |
| Milk, yogurt, and cheese groups | 2-3 servings | 3 servings |
| Meat, poultry, fish, dry beans, eggs, and nut groups | 2-3 servings | ≥2 servings |
| Vegetable group | 3-5 servings | ≥3 servings |
| Fruit group | 2-4 servings | ≥2 servings |
| Bread, cereal, rice, and pasta group | 6-11 servings | ≥6 servings |
| Water | Not included | 8 servings |
Note: Food pyramids compared to show differences in nutritional standards for adults and older adults of 70+ years.
Data from Functional performance in older adults. (2009). In B. R. Bonder & V. Dal Bello-Haas (Eds.). Cardiovascular and Pulmonary Function. Philadelphia: FA Davis; and Russell, R. M., Rasmussen, H., & Lichtenstein, A. H. (1999). Modified guide food pyramid for people over seventy years of age. Journal of Nutrition, 129, 751-753.
Table 5-3 provides a contrast of two food pyramids showing a recommended adjustment in the number of servings and balance of food groups for younger adults in contrast to recommendations for persons age 70 years and older. This table highlights the importance of adequate fluid intake and vitamin regimes to support healthy aging for persons 70+ years.
OT practitioner assessment of personal factors associated with nutrition and weight is important in intervening in cases of underweight or overweight. Issues that may impact eating and thus contribute to poor nutrition and underweight status include loss of teeth, low tolerance for textured foods, jaw pain when chewing, and medication side effects such as nausea, dry mouth, and fear of choking. Other issues that contribute to undereating can include impaired cognition and forgetfulness, loss of physical stamina and sufficient endurance to prepare a simple meal, depression and limited vision, or pain due to arthritis. At the environmental level, limited access to a grocery store, lack of transportation either public or private, and limited or declining finances may reduce nutritional intake and cause loss of weight (Table 5-4). OT intervention strategies can be instrumental in helping seniors overcome barriers to adequate nutritional intake through client-centered intervention plans.
TABLE 5-4 Possible Causes of Poor Nutrition
| Changes in senses | Appetite may diminish because of decline in the senses of taste and smell. |
| Effects of medications | Medications may change appetite or cause discomfort because of nausea or other medication effects. |
| Poor dental health | Loss of teeth, sore tongue or lips, chewing endurance, or poor fitting dentures may make eating difficult. |
| Financial burden | Reduced grocery expenses and living on a fixed income may limit the ability to pay for nutritious foods. |
| Lack of transportation | Lack of available private or public transportation, hazardous driving conditions, and winter road conditions coupled with fears of falling while entering and navigating shopping areas may limit access to nutritional foods. |
| Physical difficulty | Seniors may become frail as they age, especially when dealing with conditions such as fibromyalgia, arthritis, vertigo (dizziness), and disability. Physical pain and poor strength can make even simple tasks (opening a can, peeling fruit, and standing long enough to cook a meal) excessively challenging. |
| Forgetfulness | May limit food variations in food choices or reduce intake of adequate amounts of food due to confusion and memory loss associated with Alzheimer’s disease or other cognitive losses. |
| Depression | Loss or decrease in appetite can be due to feelings of loneliness, apathy, or as a result of losses of physical capacity or the death of loved ones. |
Adapted from Beattie, L., & Nichols, N. (2010). Nutrition and the elderly. Retrieved January 4, 2010, from www.resources/nutrition-articles.asp?id=869.
Obesity is another nutrition-related health problem experienced by many older adults and “the leading modifiable risk factor contributing to early mortality” (p. 680).30 High levels of dietary fats, carbohydrates, sugars, and sodium are most associated with the development of obesity. A reported 65% of adults are overweight secondary to diet and a sedentary lifestyle.24,31 Obesity has a significant negative effect on quality of life, self-concept and self-esteem, health, and longevity. Among adults who experience a high rate of obesity are African American women at 53%, followed by Hispanic women at 51%, and Caucasian women at 39%.32 Health conditions that occur as a result of obesity include diabetes, cardiac and peripheral vascular disease, hypertension, and stroke. The sequel of such diseases creates added disability and occupational imbalance as a result of conditions such as peripheral neuropathy, retinopathy, joint pain and weakness, and reduced endurance.
OT practitioners can be vital to interventions at the primary, secondary, and tertiary levels of care. OT practitioners can provide primary prevention of
the onset of weight gain by providing community-based health education and wellness programs. Secondary prevention combines health education with progressive and graded energy expenditure required to perform meaningful occupations (e.g., caloric expenditure during routine activities of daily living) and, at the level of tertiary prevention when the OT practitioner focuses on the occupational needs of the client once the condition becomes chronic.33 (p. 64)
Interventions might include assisting the client in formulating weekly nutritionally balanced menus, shopping for food and encouraging planning of meals that incorporate socialization, pleasant food aromas, and meaningful rituals.
Poorly balanced nutritional intake can contribute to the development of many preventable conditions that affect health and quality of living. As suggested previously, careful assessment of areas of OT practice associated with nutrition can lead to the prevention of serious diseases and limit the progression of existing diseases. Obesity and malnutrition can be addressed through the careful assessment of client factors and environmental contexts.
The benefit of health promotion and disease prevention programs may be best understood by considering the most common risks to the health of elders. Physical and psychological risks to health and well-being, which are common to elders after retirement, are numerous. The DHHS has identified the following chronic conditions as those that most frequently “contribute to difficulty in independently performing activities of daily living (ADL) and instrumental activities of daily living (IADL) functions: arthritis, hypertension, hearing impairment, heart disease, cataracts, diabetes, orthopedic impairments, tinnitus, and diabetes” (p. 12).24
Other authors suggest that the decline seen in aging may not be caused by age but by a condition referred to as disuse syndrome. This term alludes to the detrimental effects of sedentary living and the limited use of capabilities in the development of chronic and debilitating conditions. Approximately 50% of symptoms currently associated with aging, such as increases in body fat and decreases in endurance, lean body mass, and strength and flexibility, are actually a result of hypokinesia, a disease of disuse.34-37 Experimental immobilization has been noted to cause decreases in musculoskeletal, cardiovascular, and metabolic functions similar to those seen with aging. Thus, a portion of the loss of physiological integrity in elders may be attributable to disuse syndrome.38 According to Nied and Franklin,39 “Muscle strength declines by 15% per decade after age 50 and 30 percent per decade after age 70; however, resistance training can result in 25 to 100% strength gains in older people” (p. 421). Jett and Branch40 conducted The Framingham Study of Disability and found that 45% of elderly women age 65 years and older and 65% of women older than age 75 years cannot lift 10 pounds. Loss of strength and endurance among the elderly is most often an outcome of disuse or inactivity and is a serious impediment to daily living function and increased potential for falls. Results of this study identified numerous risk factors and lifestyle habits, which now have led researchers to study how genes contribute to common metabolic disorders such as obesity, hypertension, diabetes, and even Alzheimer’s disease.
Prevention and Health Promotion among Elders
COTAs working with elders should be familiar with categories of prevention used by public health agencies. Many health problems of elders are especially suited for prevention planning. Impaired mobility, injury from falls, sensory loss, adverse medication reactions, disuse syndrome, depression, malnutrition, alcohol abuse, hypertension, and osteoporosis are serious problems of the elderly that can be prevented or postponed through prevention-focused health education efforts.41 Brownson and Scaffa18 assert that “occupational therapy practitioners provide health promotion services, which typically involve ‘lifestyle redesign’ or the development of supports for healthy engagement in occupations as a means of preventing the unhealthy effects of inactivity” (p. 656).
Prevention and health promotion strategies are generally organized into three categories: primary, secondary, and tertiary (Table 5-5). Primary prevention focuses on reducing the risk for disease before its onset. Primary preventive efforts with elders may consist of facilitation of lifestyle changes and the use of necessary medications to reduce the development of life-threatening conditions such as cardiovascular disease and stroke. Primary prevention programs include immunization, accident prevention, exercise, nutritional counseling, and smoking and alcohol cessation.41 A critical primary prevention effort should be focused on the prevention of falls in elders because accidents are the sixth leading cause of death among people older than 65 years.42
TABLE 5-5 Roles of OT Practitioners in Prevention and Primary Health Promotion
| Prevention | Health promotion | |
|---|---|---|
| Primary | “Education or health promotion strategies designed to help people avoid the onset and reduce the incidence of unhealthy conditions, diseases, or injuries. Primary prevention attempts to identify and eliminate risk factors for disease injury and disability (e.g., fall prevention programs for community dwelling seniors).”43 |
“Activities that target the well population and aim to prevent ill health and disability through, for example, health education (often targeting lifestyles and behavioral change) and for legislation (such as smoking policies).”13 |
| Secondary | “Early detection and intervention after disease have occurred and is designed to prevent or disrupt the disability process (e.g., education and training regarding eating habits, activity levels, and prevention of disabilities secondary to obesity).”43 | “Directed at individuals and groups in order to change health damaging habits and/or to prevent ill health moving to a chronic or irreversible stage and, where possible, to restore people to their former state of health. Health promotion practices at this level might involve empowering individuals to take more control of their health and/or community development approaches that encourage structural and environmental changes.”13 |
| Tertiary | “Refers to treatment and services designed to arrest the progression of a condition, prevent further disability, and promote social opportunity (Patrick, Richardson, Starks, Rose, & Kinne [1997]) (e.g., “groups for older adults with dementia to prevent depression, enhance socialization, and improve quality of life).”43 | “Takes place with individuals who have chronic conditions and/or are disabled and is concerned with making the most of their potential for healthy living. This might include client-centered approaches, such as those used in rehabilitation or the management of chronic disease programmes.”13 |
Note: The variation in definitions of prevention and health promotion definitions as adapted from Scriven, A., & Atwal, A. (2004). Occupational therapists as primary health promoters: Opportunities and barriers. British Journal of Occupational Therapy, 67(10), 425; and Scaffa, M. E., Van Slyke, N., & Brownson, C. A. (2008). Occupational therapy services for the promotion of health and the prevention of disease and disability. American Journal of Occupational Therapy, 62(6), 695.
Primary Prevention
OT practitioners may represent the first line of primary prevention for well, homebound, or institutionalized elders. Primary prevention is defined as “education or health promotion strategies designed to help people avoid the onset and reduce the incidence of unhealthy conditions, diseases, or injuries. Primary prevention attempts to identify and eliminate risk factors for disease injury and disability” (p. 696).43 Primary prevention might include fall prevention programs for community dwelling seniors. In this capacity, COTAs have an opportunity to influence change in elders’ awareness of health risks. By assisting elders to develop or to return to interests that stimulate increased activity and mobility, COTAs may help reduce ill effects of a sedentary lifestyle or disuse syndrome. Many disabilities of elders start with disuse and are preventable. Studies have demonstrated the long-reaching effects of regular exercise in the prevention of weakness and fatigue, which interfere with independence in ADL functions.26,29,36,38,44-46 Exercise also has helped prevent obesity, thus reducing consequent hypertension and diabetes. A daily or three times weekly exercise program or regular participation in an activity such as walking or chair aerobics can significantly reduce the potentials for falls,29 which is a serious threat to the health and well-being of elder clients. In addition, exercise is related to improvements in elders’ psychological well-being.47
Noteworthy outcomes exist between clients involved in rote exercise and those participating in personally meaningful occupations. Rote exercise involves the repetition of a particular movement, such as lifting a 10-lb dumbbell 10 times to develop strength, endurance, or skill. Personally meaningful occupations are intrinsically motivated—that is, characteristic of activities that have a purpose in and of themselves, such as picking up a 10-lb infant. Yoder and colleagues48 found that elderly women engaged in significantly more exercise repetitions with intrinsic activities such as food preparation than with a rote exercise program. Riccio and colleagues8 later found that the use of imagery as a cue facilitated more exercise repetitions than a rote exercise program. In this study, elders imagined that they were using first the right and then the left arm to pick apples and place them in a basket.8 In a study of elder women performing a kicking task, Thomas49 found that the subjects who did the task with the actual balloon performed better than those doing rote exercise or those using imagery. He concludes that using actual tasks that have meaning might result in a better performance. A number of other studies have investigated the effects of a purposeful use of materials to facilitate movement beyond the benefits of rote exercise.48,50-56 These studies validate OT beliefs regarding the health-enhancing value of participation in actual occupation and point to the limited effects of simulated activities. Meaningful activities important to the client help generate motivation and excitement that rote exercise cannot. Thus, clients gain more from exercises that are “embedded in meaningful, purposeful occupations” (p. 19)3 than from a rote regimen of exercise, unless such regimen is part of a meaningful daily routine.57,58
Fall prevention is another critical aspect of primary prevention practices that OT practitioners can facilitate. A home or an institutional environmental assessment may identify many fall hazards for elders (see Chapter 14). A Matter of Balance is a well-researched fall prevention program that COTAs can implement in practice. The program uses a multi-model approach that addresses physical, social, and cognitive factors affecting a fear of falling.59 The use of the Fall Risk Factor Screening Checklist60 can contribute significant information to fall prevention.
Secondary Prevention
Secondary prevention efforts consist of “identification and treatment of persons with early, minimally symptomatic diseases to improve outcomes and maintain health” (p. 299).61 Secondary prevention emphasizes “early detection and intervention after disease has occurred and is designed to prevent or disrupt the disability process” (p. 696).43 An example of secondary prevention with elderly might include education and training regarding eating habits, activity levels, and the prevention of disabilities secondary to obesity. Early detection of hypertension and cancers may prevent early disability and mortality. Vision and hearing deficits are also preventable at times if detected early, as are breast and cervical cancers and depressive or substance use disorders. COTAs can contribute to early detection of serious conditions that contribute to disability and interfere with ADL and IADL functions by reminding elders of the importance of annual examinations, such as the mammogram and Papanicolaou (Pap) test. Recommendations for health and risk screening of elder populations can be different in some cases. For example, the DHHS does not provide specific suggestions for upper age limits of Pap testing but suggests recommending discontinuation after age 65 if the woman’s previous regular screenings were consistently normal.62
Minority group and non-ambulatory elderly women are at a greater risk for serious health conditions, including increased incidence of cervical cancer and cervical cancer mortality. “Women age 35 years or older, who are racial or ethnic minorities and low income, are at increased risk for invasive cervical cancer due to lower likelihood of Pap smear screen test” (p. 1).63 Reduced access to health care and to culturally appropriate health care messages has increased the risk for cervical cancers in both Hispanic and Vietnamese women in the United States. “Cervical cancer occurs most often among minority women, particularly Asian American (Vietnamese and Korean), Alaska Native and Hispanic” (p. 2).64
Analysis of invasive cervical cancer incidences by age and stage at diagnosis indicated that, except for women aged 20-29 years, incidences for Hispanic women were significantly higher than those for non-Hispanic women, the incidence for Hispanic women was second only to that of Vietnamese women, which was more than twice the incidence for Hispanics. For Hispanic and non-Hispanic women, approximately 30% of all new invasive cervical cancers diagnosed among women ages <50 years were at an advanced stage; among women who were aged 50> years, advanced stage cervical cancer represented 52% of new diagnoses.65 (p. 1068)
Iezzoni and colleagues66 found that women with lower extremity mobility difficulties are significantly less likely than other women to receive screening and preventive services such as mammograms and Pap smears. Because of the multiple and complex factors that contribute to health disparities among elderly, disabled, and minorities, health care providers at all levels should have an awareness of and a concern for the overall health of their clients. All health care providers should assume responsibility for encouraging and reminding elderly clients to schedule regular physical examinations.
Careful observation of functional capabilities may facilitate early detection of changes in elders’ capabilities. OT practitioners can monitor loss or change of sensory capacity during routine interactions with elders (see Chapters 15 and 16). COTAs also may be instrumental in educating family members to monitor elders for changes in mood or cognitive functioning that may influence independence in ADL and IADL. Changes in mood or cognition can be associated with poor nutrition or dehydration, which can be prevented or remediated (see Chapter 21). Changes also may indicate reactions to or side effects of medications or more serious physiological changes that require medical evaluation and attention (see Chapter 13).
Tertiary Prevention
Tertiary prevention refers to preventing the progression of existing conditions (see Table 5-5). It “relates to functional assessment and rehabilitation both to reverse and to prevent progression of the burden of illness” (p. 3).41 Brownson and Scaffa18 have defined tertiary prevention as “treatment and service designed to arrest the progression of a condition, prevent further disability, and promote social opportunity” (p. 656). An example of tertiary prevention initiated by the OT practitioner could be the intervention of a homebound elder who is experiencing limitations because of the pain of arthritis. The COTA would provide education about self-care activities such as joint protection and energy conservation to prevent further deterioration of arthritic joints. In addition, joint mobility can be facilitated through regular participation in a hobby within the elder’s range of tolerance. Performing energy conservation activities also may assist the elder in feeling in control of his or her daily routine. Control of pain and implementation of environmental adaptations and work simplification could assist the elder and encourage greater involvement in meaningful occupations and engagement with others.
Role of the Certified Occupational Therapy Assistant in Wellness and Health Promotion
OT practitioners play a critical role in promotion of health and prevention of disease among elders. Health education facilitates health promotion, disability reduction, and illness prevention.67,68 Chronic illnesses that affect ADL and IADL functions are more often related to lifestyle, genetic predisposition, and environmental exposure than to age alone. Frequently, elders must change behaviors to prevent disability from developing or progressing. Professional evaluation, intervention, and educational programs implemented by COTAs can foster such life-enhancing changes. A health behavior questionnaire can determine the need for intervention through health education activities (Box 5-2). Hickey and Stilwell21 stated, “The overall goal of health promotion in the elderly should be to prevent the progression of disease and the risks of disability and death” (p. 823). Health promotion should also help elders maintain functional autonomy as long as possible. Glantz and Richman45 proposed guidelines for the development of wellness programs for elders who emphasize goals of “optimum achievement and maintenance of competence and independence” (Box 5-3).
BOX 5-2
Adapted from Lohman, H., & Peyton-Runyon, C. (1991). Intergenerational experiences for occupational therapy students. Physical Occupational Therapy in Geriatrics, 2(10), 17.
Prevention Behavior Questionnaire
1. Name some behaviors in your life that you believe endanger or compromise your health.
2. How much control do you have to change them? (circle one)
3. Do you participate in some form of physical activity on a regular basis? (circle one)
4. What activities do you participate in? (circle all that apply)
5. How often in a week do you engage in these activities? (circle one)
6. How much time do you devote to these activities? (circle one)
7. Rate the level of stress in your life. (circle one)
8. What do you do to relieve stress in your life? (circle all that apply)
9. How many meals do you eat each day? (circle one)
10. Do you usually eat alone or with others? (circle one)
11. What do you consider your weight to be? (circle one)
12. Do you monitor your daily fat intake? (circle one)
13. How many servings do you have each day from the following food groups? (circle your answers)

14. Is it necessary for you to monitor your blood cholesterol level? (circle one)
15. Do you monitor your sodium intake? (circle one)
16. Have you fallen recently? (circle one)
| a. in the past week | b. in the past month |
| c. in the past 3 months | d. in the past 6 months |
| e. in the past 9 months | f. in the past year |
| g. in the past 18 months |
17. If so, how many times have you fallen? (circle one)
18. Have you scalded or burned yourself recently? (circle one)
19. Do you have arthritis? (circle one)
20. Do you have a heart disease? (circle one)
21. Do you have cancer? (circle one)
22. Do you have difficulty catching your breath
| a. when walking? (circle one) | yes | no |
| b. when climbing stairs? (circle one) | yes | no |
| c. when sitting? (circle one) | yes | no |
23. Do you have asthma or emphysema? (circle one)
| a. bending over to remove items from low cabinets? (circle one) | yes | no |
| b. going up or down stairs? (circle one) | yes | no |
| c. getting up from a bed or chair? (circle one) | yes | no |
25. Do you need assistance to walk? (circle one)
26. What distance can you safely walk without assistance or stopping? (circle one)
| a. less than 1 block | b. 1 block | c. 1/4 mile |
| d. 1/2 mile | e. 1 mile | f. other |
BOX 5-3
Wellness Program for Elders
Program goals
Enhance awareness of the positive effect of wellness on health at any age
Promote awareness of the sensory changes that occur as aging progresses
Improve knowledge of food consumption and effects on health
Improve decision-making skills
Encourage self-responsibility for health
Encourage independence and environmental mastery
Heighten awareness of behaviors that inhibit health and perpetuate disease
Possible topics
Adapted from Glantz, C. H., & Richman, N. (1996). The wellness model in long-term care facilities. Quest, 7, 7.
Hettinger69 developed the following ABCs of the wellness model in OT, which may assist COTAs in encouraging their elder clients to learn to improve and maintain their health:
Attitude that includes actively pursuing wellness and ADL that promote satisfaction and quality of life.
Balancing productive activity, positive social support, emotional expression, and environmental interactions.
Controlling health through education about behaviors that lead to wellness.
This model encourages COTAs to serve as mentors, coaches, and educators.
The American Occupational Therapy Association (AOTA) published a position statement entitled “Occupational Therapy Services in the Promotion of Health and the Prevention of Disease and Disability.”43 This statement calls on OT practitioners to be involved with health promotion and disease prevention. Three main roles have been outlined: (1) Promoting healthy lifestyles, (2) Emphasizing occupation as an essential element of health promotion strategies, and (3) providing interventions not only with individuals, but also with populations (p. 696).43
The Well Elderly Study, conducted at the University of Southern California, illustrates a successful model for OT wellness programming.6,70-72 Indications of this well-designed study validate that the lives of elders living in an urban community can be enhanced through reactivation of interests and participation in meaningful occupations. The content of the program, based on elders’ input, provided detailed instructions about areas such as transportation, safety, social relationships, and finances. Interventions through education and self-discovery processes were offered in both individual and group contexts. A key outcome of this study was demonstrating the importance and health-enhancing effects of reengaging elderly participants in meaningful occupations. Elderly participants assigned to a group facilitated by occupational therapists had better outcomes than those participants assigned to the control group or those participants of the group facilitated by a volunteer nonprofessional.6 Overall, this prevention program found that occupational therapist-led groups offered a significant benefit to positive outcomes measures, and that therapy helped the elders improve health and functional ability necessary for community living.72 The results of this program have been sustained over time.70
Health education empowers elders to take increasing responsibility for their health. COTAs have many opportunities across practice domains to provide health education programs for elders. Health promotion can occur through individual or group education efforts.70 COTAs can rely on their knowledge of group skills to facilitate discussion of materials and to encourage group development and cohesion. Generally, health-related topics include awareness building activities to heighten elder valuing and understanding of the benefits of exercise, cardiac risk reduction, methods of management of arthritis, stroke prevention, immunization, osteoporosis, cancer, early detection, home safety, assistive devices, and sensory changes that occur with aging.73 Discussion topics educate elders about leading causes of functional limitation, disability, and death, thereby facilitating the potential to change behaviors and improve quality of life.
In their research of effects of an exercise program for older adults, Hickey and Stilwell21 pointed out evidence to inspire OT practitioners to provide health-promoting activities. “The older adult responds to exercise training in the same manner as a young adult, with a 10% to 20% increase in cardiovascular fitness and strength gain of between 50% and 174%, depending on the extent of reconditioning” (p. 823). Such research shows that it is never too late to begin exercising.
Conclusion
The United States is moving into an era of health care reform that focuses on improving the quality of life for the lowest cost. The OT practitioner’s role in this reform is to promote personal responsibility for health through facilitation of self-discovery activities that can enhance interest and participation in meaningful occupations. In addition, the belief that small adaptive changes can improve the quality of a person’s life regardless of age or disability must be encouraged. As Ashley Montagu2 wrote in Growing Young, “The youth of the chronologically young is a gift; growing young into what others call ‘old age’ is an achievement, a work of art: It takes time to grow young” (p. 194).
1. Give examples of primary, secondary, and tertiary prevention functions of certified occupational therapy assistants (COTAs) working with elders.
2. Name two activity groups that could be used with each classification of prevention and health promotion.
3. Explain how health and occupation are interrelated.
4. How do occupational imbalance, deprivation, and alienation contribute to the development of disease and disability?
5. How can occupation be characterized as health promoting?
6. Describe the role of OT practitioners in wellness and health promotion program implementation.
7. How can COTAs assist elderly in preventing or overcoming occupational imbalance, occupational deprivation, and occupational alienation?
1 U.S. Department of Health and Human Services. Healthy People 2010: Understanding and Improving Health. Washington, DC: U.S. Government Printing Office; 2000.
2 Montagu A. Growing Young. New York: McGraw-Hill; 1981.
3 Nelson D.L., Stucky C. The roles of occupational therapy in preventing further disability of elderly persons in long-term care facilities. In: Levine R.A., Rothman J., editors. Prevention Practice: Strategies for Physical Therapy and Occupational Therapy. Philadelphia: WB Saunders, 1992.
4 Gilfoyle E.M. The future of occupational therapy: An environment of opportunity. In: Ryan S.E., editor. The Certified Occupational Therapy Assistant. Thorofare, NJ: Slack Inc, 1986.
5 Carlson M., Clark F., Young B. Practical contributions of occupational science to the art of successful aging: How to sculpt a meaningful life in older adulthood. Journal of Occupational Science. 1998;5(30):107-118.
6 Jackson J., Carlson M., Mandel D., Zemke R., Clark F. Occupation in lifestyle redesign: The well elderly study occupational therapy program. American Journal of Occupational Therapy. 1998;52(5):326-334.
7 Johnson J.A. Wellness: A Context for Living. Thorofare, NJ: Slack Inc; 1986.
8 Riccio C.M., Nelson D.L., Bush M.A. Adding purpose to the repetitive exercise of elderly women through imagery. American Journal of Occupational Therapy. 1990;44:714-717.
9 Scaffa M.E., Reitz S.M., Pizzi M.A. Occupational Therapy in the Promotion of Health and Wellness. Philadelphia: FA Davis; 2010.
10 Speake D.L. Health promotion activity in the well elderly. Health Values. 1987;11:6-25.
11 Wilcox A.A. Occupation for health. British Journal of Occupational Therapy. 1998;61(8):340-345.
12 Wilcox A.A. The Doris Sym Memorial Lecture: Developing a philosophy of occupation for health. British Journal of Occupational Therapy. 1999;62(5):191-198.
13 Wilcox A.A. An Occupational Perspective of Health, 2nd ed. Thorofare, NJ: Slack Inc; 2006.
14 Yerxa E.J. Occupational science: A new source of power for participants in occupational therapy. Journal of Occupational Science. 1993;1:1-3.
15 Richard B. Workplace literacy technology for nursing assistants. Journal of Health Occupations Education. 1991;6(1):73-85.
16 Hanft B. Promoting health: Historical roots-renewed vision. OT Practice. 2002;2:10-15.
17 Richards S.E. The Carson Memorial Lecture 1998: Occupation for health—and wealth? British Journal of Occupational Therapy. 1998;61(7):294-300.
18 Brownson C.A., Scaffa M.E. Occupational therapy in the promotion of health and the prevention of disease and disability statement. American Journal of Occupational Therapy. 2001;55(6):656-660.
19 Scott A.H., Butin D.N., Tewfik D., Burkhardt M.A., Mandel D., Nelson L. Occupational therapy as a means to wellness with the elderly. Physical & Occupational Therapy in Geriatrics. 2001;18(4):3-22.
20 Reilly M. Occupational therapy can be one of the great ideas of 20th century medicine: Eleanor Clarke Slagle lecture. American Journal of Occupational Therapy. 1962;16:1-9.
21 Hickey T., Stilwell D.L. Health promotion for older people: All is not well. Gerontologist. 1991;31(6):822-828.
22 Fidler G.S., Fidler J.W. Doing and becoming: Purposeful action and self-actualization. American Journal of Occupational Therapy. 1978;32(5):305-310.
23 Florey L. Development through play. In: Schaefer C., editor. The Therapeutic Use of Child’s Play. New York: Jason Aronson, 1976.
24 U.S. Department of Health and Human Services. A profile of older Americans [WWW page]. URL http://www.hhs.gov, 2001.
25 Mallinson T., Fischer H., Rogers J.C., Ehrlich-Jones L., Chang R. The Issue Is—Human occupation for public health promotion: New directions for occupational therapy practice with persons with arthritis. American Journal of Occupational Therapy. 2009;63:220-226.
26 McMurdo M.E., Rennie L. A controlled trial of exercise by residents of old peoples’ homes. Age-Ageing. 1993;22(1):11-15.
27 Caserta M.S., Gillett P.A. Older women feelings about exercise and their adherence to an aerobic regimen over time. Gerontologist. 1998;38(5):602-609.
28 Nuessel F., Van Stewart A. Literary exemplars of illness: A strategy for personalizing geriatric case histories in clinical settings. Physical and Occupational Therapy in Geriatric Medicine. 1999;16:33-46.
29 Rubenstein L.Z., Josephson K.R., Trueblood P.R., Loy S., Harker J.O., Pietruszka F.M., et al. Effects of a group exercise program on strength, mobility, and falls among fall-prone elderly men. Journal of Gerontology Series A, Biological Sciences and Medical Sciences. 2000;55A(6):M317-M321.
30 American Occupational Therapy Association. AOTA’s statement on obesity. American Journal of Occupational Therapy. 2006;60(6):680.
31 U.S. Department of Health and Human Services. Nutrition and overweight. Retrieved December 29, 2009, from www.healthypeople.gov/Document/HTML/Volume2/19NUtrition.htm, 2006.
32 Centers for Disease Control and Prevention. Prevalence of obesity in adults. Retrieved December 28, 2009, from http://www.cdc.gov/nchs/data/databriefs/db01.pdf, 2008.
33 Blanchard S.A. Variables associated with obesity among African-American women in Omaha. American Journal of Occupational Therapy. 2010;63(1):58-68.
34 Drinkwater B.L. Exercise and aging: The female master athlete. Journal of Public Health. Brown C., Voy R.O., editors. Sports Science Perspectives for Women: Proceedings from the Women and Sports Conference. Chicago: Human Kinetics, 1988.
35 Hjort P.F. Physical activity and health in elderly—walk on. Tidsskr Nor Laegeforen. 2000;120(24):2915-2918.
36 Schuster C., Petrosa R., Petrosa S. Using social cognitive theory to predict intentional exercise in post-retirement adults. Journal of Health Education. 1995;26:1-14.
37 Smith M.T. Implementing annual cancer screening for elderly women. Journal of Gerontological Nursing. 1995;2(7):12-17.
38 Fiatarone M.A., Evans J.E. Exercise in the oldest old. Topics in Geriatric Rehabilitation. 1990;5(2):63-77.
39 Nied R.J., Franklin B. Promoting and prescribing exercise for the elderly. American Family Physician. 2002;65:419-426.
40 Jett A.M., Branch L.G. The Farmington Disability Study: ii. Physical disability among the aging. American Journal of Public Health. 1981;71:1211-1216.
41 Webster J.R. Prevention, technology, and aging in the decade ahead. Topics in Geriatric Rehabilitation. 1992;7:4.
42 Centers for Disease Control and Prevention (CDC). Deaths: Final data for 2000. National Vital Statistics Reports. 2002;50(15):1-120.
43 Scaffa M.E., Reitz S.M., Pizzi M.A. Occupational therapy in the promotion of health and wellness. Philadelphia, PA: F. A. Davis; 2010.
44 Butler R.N., Davis R., Lewis C.B., Nelson M.E., Strauss E. Physical fitness: How to help older patients live strong and longer. Geriatrics. 1998;53(9):26-28. 31, 32, 39, 40
45 Glantz C.H., Richman N. The wellness model in long-term care facilities. Quest. 1996;7:7-11.
46 Lohman H., Givens D. Balance and falls with elders: Application of clinical reasoning. Physical and Occupational Therapy in Geriatrics. 1999;16:17-32.
47 Stewart A.L., Mills K.M., Sepsis P.G., King A.C., McLelland B.Y., Roitz K., et al. Evaluation of CHAMPS: A physical activity program for older adults. Annals of Behavior and Medicine. 1998;19(4):353-361.
48 Yoder R.M., Nelson D.L., Smith D.A. Added-purpose versus rote exercise in female nursing home residents. American Journal of Occupational Therapy. 1989;43:581-586.
49 Thomas J.J. Materials based, imagery based, and rote exercise and occupational forms: Effects on repetitions, heart rate, duration of performance, and self-perceived rest periods in well elderly women. American Journal of Occupational Therapy. 1996;50(10):783-789.
50 Bloch M.W., Smith D.A., Nelson D.L. Heart rate, activity, duration, and effect in added purpose versus single-purpose jumping activity. American Journal of Occupational Therapy. 1989;43:25-30.
51 Heck S.H. The effect of purposeful activity on pain tolerance. American Journal of Occupational Therapy. 1988;42:577-581.
52 Kircher M.A. Motivation as a factor of perceived exertion in purposeful versus nonpurposeful activity. American Journal of Occupational Therapy. 1984;38:165-170.
53 Miller L., Nelson D.L. Dual purpose activity versus single purpose in terms of duration on task, exertion level, and affect. Occupational Therapy in Mental Health. 1987;7:55-67.
54 Sakemiller L.M., Nelson D.L. Eliciting functional extension through the use of a game. American Journal of Occupational Therapy. 1998;52(2):150-157.
55 Schmidt C.L., Nelson D.L. A comparison of three occupational forms in rehabilitation patients receiving upper extremity strengthening. Occupational Therapy Journal of Research. 1996;16(3):200-215.
56 Thomas J.J., Rice M.S. Perceived risk and its effect on quality of movement in occupational performance of well-elderly individuals. Occupational Therapy Journal of Research. 2002;22(3):104-110.
57 Wagstaf S. Supports and barriers for exercise participation for well elders: Implications for occupational therapy. Physical and Occupational Therapy in Geriatrics. 2005;24(2):19-33.
58 Fredman L., Bertrand R., Martire L., Hochberg M., Harris E. Leisure-time exercise and overall physical activity in older women caregivers and non-caregivers from the Caregiver-SOF study. Preventive Medicine. 2006;43(3):226-229.
59 Boston University Center for the Enhancement of Late-Life Function. Fear of falling: An emerging health problem. Roybal Program Brief. 2000:1-6. Retrieved December 22, 2003, from http://www.applied-gerontology.org/BUBrief.pdf
60 Carlson A. Fall prevention in Hilo, Hawaii. OT Week. 1996;10(36):14. 15
61 Garner D.J., Young A.A., editors. Women and Healthy Aging: Living Productively in Spite of It All. New York: Haworth Press, 1993.
62 Centers for Disease Control and Prevention (CDC). Cervical cancer and Pap test information. The National Breast and Cervical Cancer Detection Program [WWW page]. URL http://www.cdc.gov/cancer/nbccedp/info-cc.htm, 2002.
63 Washington State Department of Health. Early cervical cancer detection important for women of color and women living in rural areas [WWW page]. URL http://www.doh.wa.gov/Publicat/2002_News/02-06.htm, 2002.
64 Agency for Healthcare Research and Quality. Breast and cervical cancer research highlights [WWW page]. URL http://www.ahcpr.gov/research/breastca.htm, 2003.
65 Centers for Disease Control and Prevention (CDC). Invasive cervical cancer among Hispanic and non-Hispanic women—United States, 1992-1999. Morbidity and Mortality Weekly Report. 2002;51(47):1067-1070.
66 Iezzoni L.I., McCarthy E.P., Davis R.B. Use of screening and prevention services among women with disabilities. American Journal of Medical Quality. 2001;16(4):135-144.
67 Pinch W.J. Health promotion and the elderly. NSNA/Imprint. 1993;40(2):83-86.
68 Poland B., Krupa G., McCall D. Settings for health promotion: An analytic framework to guide intervention design and implementation. Health Promotion Practice. 2009;10(4):505-516.
69 Hettinger J. The wellness connection. OT Week. 1996;10:12. 13
70 Clark F., Azen S.P., Carlson M., Mandel D., LaBree L., Hay J., et al. Embedding health promoting changes into the daily lives of independent-living older adults: Long-term follow-up of occupational therapy intervention. Journals of Gerontology-Series B: Psychological Sciences and Social Sciences. 2001;56B(1):P60-P63.
71 Clark F., Azen S.P., Zemke R., Jackson J., Carlson M., Mandel D., et al. Occupational therapy for independent-living older adults: A randomized control trial. Journal of the American Medical Association. 1997;278(16):1321-1326.
72 Mandel D.R., Jackson J.M., Zemke R., Nelson L., Clark F.A. Lifestyle Redesign: Implementing the Well Elderly Program. Bethesda, MD: The American Occupational Therapy Association; 1999.
73 Mount J. Evaluation of a health promotion program provided at senior centers by physical therapy students. Physical and Occupational Therapy in Geriatrics. 1991;10(1):15-25.