Chapter 14 Considerations of Mobility
1. Discuss the Omnibus Budget Reconciliation Act regulations pertaining to the use of physical restraints.
2. Describe the steps in the establishment of a restraint reduction program.
3. Describe the role of the certified occupational therapy assistant in restraint reduction.
4. Outline the basic steps in evaluating the fit of a wheelchair.
5. Describe the major precautions to consider when elders should use wheelchairs.
6. Describe essential considerations when evaluating and fitting a bariatric person with a wheelchair.
7. Identify three reasons that elder adults are at a greater risk for falls than the general population.
8. Identify environmental, biological, psychosocial, and functional causes of falls.
9. Describe key considerations during the evaluation process for elder adults at risk for falls.
10. Describe recommended and evidence-based interventions to prevent falls.
11. Discuss potential desired outcomes of fall prevention interventions.
12. Discuss ways elders may gain access to public transportation.
13. Describe ways elders may become safer pedestrians.
14. Describe a driving evaluation, and identify criteria for this assessment.
15. Describe visual and physical changes in elders that may affect their ability to drive.
restraints, restraint reduction, environmental adaptations, psychosocial approaches, activity alternatives, fall prevention, aging in place, environmental hazards, mobility, transit, driving, pedestrian, paratransit, wheelchair assessment, wheelchair selection, bariatric wheelchair assessment
PART 1 Restraint Reduction
TRACY MILLIUS, CANDICE MULLENDORE, AND IVELISSE LAZZARINI
The use of physical restraints in health care practice has been common for many years.1 The American health care system has used physical restraints throughout the continuum of care ranging from hospital emergency rooms, psychiatric units and med-surgical units, to nursing homes and other institutions. However, there continues to be mounting evidence of patient safety risks related to the use of physical restraints.2
In 1987, the Omnibus Budget Reconciliation Act of 19873 (OBRA) was implemented, and it forbid the use of physical restraints for the purposes of discipline or staff convenience in nursing homes. However, the use of physical restraints continues in nursing homes in the United States, but it is declining. In 2006 the Centers for Medicare & Medicaid Services (CMS) tightened the regulations regarding the use of restraints by requiring health care workers to undergo more extensive training about the appropriate use of restraints to help ensure patient safety.4 CMS also launched a 2-year campaign to reduce the use of restraints in nursing homes because of the high risks of harm associated with restraint usage.5 According to the U.S. Department of Health and Human Services Agency for Healthcare Research and Quality, the amount of long-stay nursing home residents who have physical restraints has decreased from 10.4% in 2000 to 5% in 2007 (Box 14-1).6
BOX 14-1 Negative Effects of Restraints
| Psychosocial | Physical |
|---|---|
Omnibus Budget Reconciliation Act Regulations
OBRA was drafted to protect elders from abuse and to promote choice and dignity. The ultimate goal of OBRA is that each person reaches his or her highest practical level of well-being. A reduction in the use of restraints is only a small part of this intent. OBRA requires caregivers to develop an individualized plan of care that supports each elder in the least restrictive environment possible.4,7,8 Certified occupational therapy assistants (COTAs) should become familiar with OBRA guidelines regarding restraints.
OBRA defines two types of restraints: chemical and physical. “Physical restraint can be any manual method, such as any physical or mechanical device, that restricts the patient’s freedom of movement.”4 Some examples of physical restraints with the elderly may include restrictive chairs with full lap trays and small wheels that limit mobility, vests used to secure patients to their chairs or beds, wrist or ankle restraints, or bedrails. “Chemical restraints are described as a drug or medication when it is used as a restriction to manage the patient’s behavior or restrict the patient’s freedom of movement and is not a standard treatment or dosage for the patient’s condition.”9
Restraints are permitted only when they enable greater functional independence, restrict the elder from interfering with the provision of life-saving treatment, or are necessary because less restrictive devices have failed. A documented medical need and physician’s order for restraints must exist. Clients must be released at least every 2 hours, and the restraints can be used as a temporary intervention only.4
Despite these guidelines, the improper use of restraints continues in the United States. COTAs have an ethical and legal obligation to report elder abuse, which includes using restraints as punishment for clients or as a convenience to staff. COTAs should also participate in educating others about restraints and may wish to initiate a restraint reduction program in their own facility and offer restraint alternatives.
Establishing a Restraint Reduction Program
Reducing restraints is a complex matter. COTAs must evaluate and appropriately address ethical considerations, regulatory and professional standards, legal liability concerns, and health care team members’ education regarding restraint use. It is also important to identify areas for, and participate in, research concerning physical restraints to assist staff nurses and other members of the health care team with making informed decisions regarding patient care.10
Philosophy
The philosophical premises of an educational program aimed at restraint reduction include beliefs about quality of care, commitment to understanding the meaning of behavior, and desire to shift practice from control of behavior to individualized approaches to care. If a change is to occur, an educational program aimed at restraint reduction must recognize the potential contributions of all staff members, use an interactive teaching style, and promote discussion and problem solving. Results of testing a restraint education program suggested that altering staff beliefs and increasing knowledge produced a change in restraint practices, at least in the short-term.11
A fundamental philosophical concept in the care of elders is the empowerment of both elders and staff. This empowerment is expressed in collaborative solutions to problems. The ability to contribute to solutions allows elders their dignity and adds meaning and quality to their lives.12 Making choices, including the choice to take a risk, is an essential part of life and contributes to maintaining self-respect.
In addition, it is also paramount to teach family members about the potentially harmful effects of restraint use and the regulatory restrictions and oversight on using restraints. While family members may incorrectly believe that a restraint prevents injury, COTAs or other health care provider plays an important role in educating family members on the aspects of patient autonomy and freedom of movement.
Policy
Health care providers’ written policies and procedures should be consistent with each of the requirements listed in the regulations. Yearly mandatory training for staff should be provided, and all training and education programs should be documented. Documentation of events of restraint use should meet required regulations.10
When a facility makes a philosophical decision to reduce restraint use, education must be incorporated to help change the organizational culture and to provide strategies for the successful removal of restraints.13
Education
Practitioners must teach these concepts not only because they have been mandated by federal regulation, but also because, as Brungardt14 indicates, elders’ function cannot improve “if they are tied down or drugged up.” Physical restraints are generally harmful to residents because of the negative effects on multiple body systems and interference with normal functioning, including a resident’s capacity to walk, get food, get fluids, change position, toilet, and socialize. Specific physical consequences of restraint use are numerous as well and may include death, injuries, falls, physical deconditioning, incontinence, malnutrition, dehydration, and bone demineralization. Muscle atrophy, skin tears, pressure ulcers, contractures, cardiac rhythm disturbances, and infection can be other consequences of being restrained.15
An effective education program includes an experiential component, such as applying a variety of restraints to participants. Few individuals can imagine choosing restraints as an appropriate intervention for themselves. Feeling the helplessness and degradation of being restrained sensitizes staff to the use of restraints on elders. Education should use and affirm participants’ life experiences. Including board members, volunteers, and all facility employees (kitchen workers, bookkeepers, administration, chaplains, and maintenance workers) in this educational program has been identified as a factor leading to the decreased reliance on restraints.16,17 The CMS Federal Register18 indicates that staff must be trained regarding restraint use and regulations, and all training must be documented.
Steps for Success
The key to eliminating the use of restraints is individualized care, which depends on staff knowing the resident as a person. One strategy for fostering staff-resident relationships is the consistent assignment of staff to residents, which may help promote individualized care. Staff members responsible for care planning should try and document various options to avoid the use of restraints (Box 14-2).15
BOX 14-2
Suggestions to Facilitate a Successful Restraint-Free Environment
 Develop a restraint committee involving all disciplines and departments in the facility.
Develop a restraint committee involving all disciplines and departments in the facility.
Determine the goal for the restraint reduction program. Is it to minimize restraints or completely ban restraints?
Develop a strategic plan including protocols for specific restraint cases.
Recruit specialists (gerontological nurse specialist, occupational therapy personnel, etc.) for consultation.
Determine a protocol for how restraints are ordered by physicians.
Limit restraint usage to a 24-hour trial. If the restraint usage exceeds that time period, consult with the physician.
Provide documentation of both alternatives and reasons for restraint usage when requesting physician’s orders.
Implement a gradual process of change when starting the restraint reduction program.
Start with the easiest cases first and move on to more difficult cases once initial success is achieved.
Complete ongoing resident assessments. Provide restraint alternatives and interventions based on an individualized resident-specific approach. Include family participation. Learn from others who have successful restraint reduction programs.
From Joanna Briggs Institute. (2002). Physical Restraint—Part 2: Minimization in Acute and Residential Care Facilities, Best Practice, 6(4). Asia, Australia: Blackwell.
All members of the team, including families, staff from each shift, consultants, contract personnel, ombudsmen, state surveyors, physicians, and elders themselves, should be included in all stages of the program. Dialogue between these participants from the beginning makes the transition to restraint-free care much smoother. All team members play an important role. Family members can, for example, describe the elder’s previous routines and preferences. Kari and Michels12 assert that certified nursing assistants (CNAs) have essential knowledge of elders and that their usual lack of influence in decision making negatively affects the quality of care.
CNAs may be the team members who first notice behavioral changes and the need for removal of restraints in elders.16 Strumpf and colleagues11 indicate that respect for the dignity of the CNA’s work is vital for any significant reduction in the use of restraints. An interdisciplinary team assessment of the need for restraint is helpful in reducing reliance on restraints.17,19
The most successful restraint-free programs have adopted permanent staffing.20 This model assigns daily a “primary” CNA (and registered nurse, housekeeper, therapist, among others) to each elder. When these staff members are not working, they should have regular replacements. Permanence in staffing fosters relationships between elders, families, and staff who contribute to feelings of safety and connectedness. Permanent staff are particularly important to elders with cognitive impairment. Initial success will help staff members feel confident about continuing restraint reduction. Family involvement that ranges from simply being notified of the restraint reduction to formal family educational programs has proven effective in a reduction program.13
Rader21 has found that the biggest obstacles to eliminating restraints are fears, biases, and unwillingness to change. She proposes that caregivers, clients, advocates, and regulators work together to create new interventions on the basis of the elder’s perspectives and wishes. Reducing restraints should be only the beginning of providing safe care in a dignified and less restrictive environment that promotes the elder’s abilities.22,23
Role of the Certified Occupational Therapy Assistant
In collaboration with a registered occupational therapist (OTR), COTAs may assess the need for restraints, consult with staff about alternatives to restraint, and provide intervention to eliminate restraint use. The type or technique of restraint used must be the least restrictive intervention that will be effective to protect the patient, staff member, or others from harm.4
Assessment
Once the need for intervention is documented and an occupational therapy (OT) order has been received, the OTR/COTA team performs an evaluation. Specific assessments of posture, alignment, balance, strength, and visual acuity are necessary. Assessments of head control, trunk stability, upper extremity support, and the ability to self-propel are added to evaluate seating needs.24,25 Perceptual and cognitive assessments should be included only as appropriate. Practitioners should not embarrass or agitate cognitively impaired elders by assessing areas already documented as deficient.
Consultation
The assessment may reveal minimal intervention needs, perhaps consultation only. Patterson and colleagues26 include the roles of advocate, observer, teacher, information specialist, team problem solver, and identifier of resources and alternatives in their definition of consultant. They also report that the combination of consultation with formal restraint reduction training significantly reduces the use of restraints. COTAs are uniquely qualified to function as consultants in developing alternatives to restraints, especially if they are familiar with restraint reduction principles, OBRA regulations, and the basic principles of positioning. For example, an elbow air splint may be all that is necessary for an elder who continually scratches at sutures on a healing incision. Although an air splint is certainly restrictive, it allows more movement than wrist restraints, thereby meeting the criterion for “least restrictive environment.” Because wound healing is temporary, the air splint is a temporary measure. A protocol for use of the air splint should be provided. The care plan should document the reason that the splint is being used, the way it will be used, and the way it will be reassessed by the nursing staff.
COTAs may recommend other environmental, psychosocial, and activity-related alternatives (Table 14-1). The alternatives outlined are not a complete list. Options are limitless, depending on the COTA’s creativity. Each measure considered should provide as much free choice and control as possible for elders. Eigsti and Vrooman27 claim that the basic ingredient in reducing restraint use is teaching the staff to understand and believe that alternatives exist.
TABLE 14-1 Alternatives to Restraints
| Environmental alternatives | Chairs | |
| Beds | ||
| Monitoring Systems | ||
| Signs | ||
| Safety Adaptations | ||
| Personalized Room | ||
| Other Adaptations | ||
| Psychosocial alternatives | Behavioral Strategies | |
| Decrease or Increase | ||
| Activities |
 to
to  length bed rails (instead of full length)
length bed rails (instead of full length)Environmental Adaptations
There are several strategies that can be used to modify the environment to move toward making it restraint free. For example, using chairs that are at the right height, depth, and level of backing for each resident to have comfortable and safe seating can reduce the risk and need for restraints. Furthermore, individualizing the chairs each resident uses in the dining room or other public areas can help provide a match with the residents’ needs.15
An inexpensive and less restrictive alternative for the confused elder who rises unsafely from a chair might be a personal alarm. Several such alarms are on the market. They do not prevent the elder from rising, but they do alert staff. An elder’s attempt to rise usually occurs for a reason and warrants attention from the caregiver. However, a personal alarm may frighten or agitate the elder or surrounding residents. Therefore, the use of the alarm should be with caution and take into account the environment, elder, and other residents.
Many facilities have discovered that nursery intercoms are an inexpensive and effective way to monitor safe ambulators who wander. Directional signs may help these elders locate their rooms and deter them from entering someone else’s room. An alternative to direction signs are signs with familiar pictures instead of words.
Providing cues to help orient residents who wander may also be helpful. Cues can include memory boxes by a resident’s door, personal furnishings that residents will recognize, or large visual signs or pictures for bathrooms and other frequently sought areas.15 Simple velcro signs can be placed across doorways that wandering residents should not enter (i.e., exit doors). These signs are generally red or yellow and may read “Stop” (Figure 14-1). These visual cues help the wandering resident return to another area of the building.
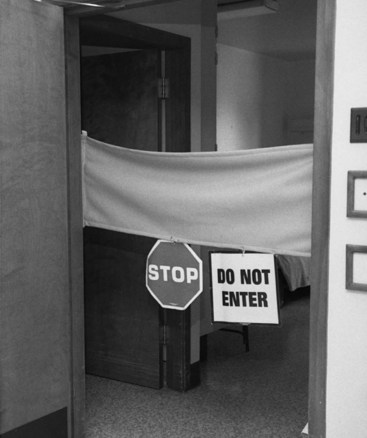
FIGURE 14-1 Environmental adaptations should help restrict elders with Alzheimer’s disease from wandering into other people’s rooms without restricting access to corridors.
There are many new types of beds on the market that will allow a facility to reduce bed rail use and decrease incidence of falls. For residents at a higher risk for falls, the new beds can be adjusted from standard height to 7 inches off the floor, so that when falls do occur, they will not cause serious injury. Safety alarms, special mattresses and pillows, and thick rubber bedside mats can also be installed. Placing squeak toys between the sheets and mattress pads reminds residents when they are getting too close to the edge of the bed. When side rails must be used, staff can set foam “swim noodles” between the mattress and side rail to reduce the risk of a resident getting trapped against the rail.29
Psychosocial Approaches
Qualitative studies1 and other literature15 indicate negative experiences of people who have been restrained, including emotional distress, loss of dignity and independence, dehumanization, increased agitation, and depression. Residents may experience emotions ranging from frustration and anxiety to anger and terror when restrained. Therefore, psychosocial approaches to reduce restraint use are important.
Wandering or attempts to get up from a chair may be part of an elder’s agenda behavior and may lead to agitation if the elder is restrained. Evans and colleagues30 indicate that the keys to responding successfully to agenda behavior are to allow elders to act on their plans, identify a point at which they may accept a suggestion or guidance, and allow them to keep their dignity throughout an incident. The important difference in the result of this approach compared with others is that allowing the elder to play out the behavior provides a sense of identity and promotes feelings of belonging, safety, and connectedness. This diminishes the elder’s need to seek those feelings elsewhere. Further incidences of wandering are subsequently decreased or eliminated.31 Brungardt14 adds that this method works well if the elder’s welfare is considered before the needs or routines of the facility.
Activity Alternatives
Activity zones with recreational activities, such as multisensory theme boxes, and offering substitute physical activities that interest residents such as dance, exercise, or rocking, may be ways to engage residents in something of interest and reduce the occurrence of wandering. Providing cues to help orient residents who wander may also be helpful. Cues can include memory boxes by a resident’s door, personal furnishings that residents will recognize, or large visual signs or pictures for bathrooms and various frequently sought areas.15
Providing meaningful activity alternatives can decrease behavior such as restlessness that has traditionally led to the use of restraints. An activity kit, perhaps in the form of a sewing basket, briefcase, fanny pack, or tackle box, may be helpful. The kit may be assembled by family members who are familiar with the elder’s interests.21,32 The idea is to provide something familiar, comfortable, and safe that engages the elder’s attention.
Intervention
Although not all referrals require intervention beyond consultation, the assessment may identify a need for ongoing intervention. Examples of intervention to eliminate the need for restraints include the development of self-care techniques, upper body positioning, and seating adaptations.
Because restraint use is associated with the inability to perform self-care, elders and their caregivers should be taught strategies for accomplishing this goal. Determining the routines the elder followed in the past to maintain a sense of continuity and predictability is particularly important. Because part of the objective is to reduce anxiety and agitation, self-care must be done according to the elder’s agenda and routine rather than those of the COTA or facility.
Elders with hemiplegia are often provided with half-tray style lapboards to assist with upper body positioning. Because these elders need the best support possible for their upper extremities, this is one of the few cases in which it may be advantageous to begin with the most restrictive device, a full lapboard, and adapt if necessary. If a full lapboard causes agitation or seems too restrictive (perhaps the elder is unable to use a urinal independently), a swing-away half lap tray may be used. Another solution is a foam wedge or cylindrical bean bag, which can extend the width of the armrest for safe positioning without a lapboard. As with any restrictive device, however, less than perfect positioning may be necessary to accommodate the elder’s choice.
Another specific OT intervention aimed at reducing the need for restraints is a positioning assessment for elders who are wheelchair-bound. Ill-fitting wheelchairs contribute to restraint use, which can lead to an abnormal sitting posture and the eventual loss of function.33 For example, wheelchairs usually found in nursing homes were not designed for independent mobility or long-term sitting. Necessary adaptations for comfort and function include dropping the seat so that elders can reach the floor with their feet, replacing the sling seat with a firm seat and cushion, and replacing the sling back with a firm back. A narrower chair may help elders propel themselves more comfortably.34 Knowledge of the principles of positioning is essential. (Basic alignment principles applicable to any elder are outlined in Chapter 19.) Once adaptations have been designed and implemented, the elder’s verbal, behavioral, and postural response must be observed. The system should be reassessed and adapted as necessary until the positioning goals have been met. Documentation should accompany every step of this process, especially if the elder declines the intervention. With very difficult cases, consultation with a seating expert may be helpful. However, even the nonexpert can make many “low-tech” foam supports. More detailed information on wheelchair positioning is included in Part 4 of the chapter.
Relatively inexpensive foam is available in large sizes at the local building or craft store and can easily be cut and shaped with an electric knife. This type of foam works well for the addition of width to an armrest, the fabrication of forearm wedges to elevate edematous upper extremities, or the provision of lightweight lateral trunk support. Egg crate foam is another inexpensive material suitable for limited purposes. Neither of these low-density foams is adequate to support entire body weight while sitting or during episodes of spasticity. For long-term positioning, manufactured cushions of mixed density foam, gel, or air cushions are more durable and are recommended for both comfort and maintained skin integrity. The therapeutic role of orthotic devices in achieving proper body position, balance, and alignment and improving overall functional capacity without the potential negative effects of restraint use is recognized by the Health Care Financing Administration (HCFA).7,8 This recognition does not provide the license to use wedges, reclining chairs, or seat belts as restraints, even for cognitively intact elders. However, it does allow the legitimate use of positioning devices to increase function, given a demonstrated necessity. Any adaptation should maintain the dignity of elders and augment their quality of life.
Case Study
Mary, a 79-year-old woman with the diagnosis of dementia resides in a long-term care facility. Other medical history includes multiple transient ischemic attacks (TIAs) and skin breakdown on the buttocks area. Mary requires total assist transfers from the bed to the wheel chair. Her current wheel chair positioning includes a pressure relief cushion and a self-release pelvic belt to prevent sliding forward in the wheel chair. Mary is able to self-release the pelvic positioning belt; therefore, the belt is not considered to be a restraint. However, when she releases it because of agitation or trying to take herself to the bathroom, she tends to slide forward in her chair and is at risk for falls. To prevent this from happening, the nursing staff have requested that the pelvic belt be replaced with one that Mary is not able to release herself. The new pelvic belt then becomes a restraint. The nursing staff order the OTR/COTA team of Marc and Diana to address this case.
Because Marc and Diana are aware of restraint reduction guidelines, they provide interventions to promote optimal positioning using the least restrictive methods. They install a manual tilt pack on the wheel chair to reduce sliding forward and remove the pelvic positioning belt. They also install a drop seat to allow Mary’s feet to touch the ground and self-propel throughout the facility. They provide a wedge cushion for optimal positioning. To involve the other members of the health care team, they educate nursing on proper positioning devices and techniques.
Finally, they focus on the resident and encourage Mary to self-propel her wheel chair for increased independence. They talk with staff about engaging Mary in various activities throughout the day and evening and suggest moving her to various interesting areas during the day (high traffic areas, such as nursing stations or activity room, or near windows to see outside). As a result, Mary is able to make her needs known when placed near the nursing station and enjoys increased independence with mobility. The pelvic belt is replaced by a recliner back, drop seat, and wedge cushion. These interventions collectively position Mary correctly and reduce her incidences of sliding forward and fall risk. Most importantly, Mary does not have a restraint.
Questions about Case Study
1. How is addressing Mary’s wheelchair positioning in this study related to restraint reduction?
2. How did Marc and Diana help maintain Mary’s dignity and quality of life?
3. How did the OTR/COTA team work as part of the interdisciplinary team to eliminate Mary’s restraint and improve her functional abilities?
Conclusion
COTAs have a responsibility to clearly state their professional opinion and recommendations regarding restraint reduction. Clients must choose whether to act on that advice. True restraint reduction requires an examination of attitudes about the rights of elders, especially those with cognitive impairment, to make choices and take risks. COTAs must be willing to become advocates for elders. An understanding of OBRA regulations and positioning principles and the ability to be flexible and creative within a team framework permit COTAs to contribute effectively to restraint elimination programs. If COTAs have honestly attempted to increase function and honor the dignity of the elders they serve, they will have followed not only the letter of the law, but also the intent and spirit.
PART 2 Wheelchair Seating and Positioning: Considerations for Elders
In 1997, approximately 19% of individuals age 65 years and older relied on a wheelchair for their mobility within the household and community.35 As the population in this age range continues to grow, this percentage is expected to increase rapidly. More recent data indicate that 2.2 million community dwelling people use wheelchairs, of which 58% use manual wheelchairs.36 Persons age 65 years or older and living in nursing homes or facilities are reported to be greater than 50% of the total population.37 The highest rates of manual wheelchair use is in the elderly. People greater than age 65 years (57.8%) use manual wheelchairs. Of note, more than two-thirds of power chair users are not the elderly.38 The use of assistive devices, such as wheelchairs for mobility, has increased with the population growth, technological advances, and initiatives in public policies.35 Public policies such as the Technology Related Assistance for Individuals with Disabilities Act (1998) and the Rehabilitation Act Amendments of 1986 have contributed to the increased access to wheelchairs by elders. The use of a wheelchair for mobility in the home or community, or both, is important in improving individuals’ level of independence and their ability to participate in chosen occupations.
Health professionals frequently have a “one size fits all” approach to wheelchair seating and positioning. This is often true with elders because Medicare has strict guidelines regarding wheelchair rental and purchase. However, elders have numerous conditions associated with aging that increase the likelihood of complications from improper wheelchair seating and positioning. Such conditions include joint replacements, osteoarthritis, osteoporosis, musculoskeletal changes, including kyphosis and scoliosis, cerebrovascular accident, Alzheimer’s disease, amyotrophic lateral sclerosis, Parkinson’s disease, dementia, chronic obstructive pulmonary disease, diabetes, congestive heart failure, and hypertension.39
A wheelchair should be selected with the unique needs of the individual person in mind. The overall outcomes for a person in a proper position in his or her wheelchair include increased independence, prevention of skin breakdown, decreased need for caregiver(s), and a general overall improvement in quality of life.40 The result of an elder seated improperly in his or her wheelchair can be fixed or flexible deformities, as well as a decrease in overall function.41
A proper wheelchair seating and positioning assessment should be conducted by an OTR. The COTA may collaborate in this process. Areas considered in such an assessment include diagnosis, prognosis, age, cognition, perception, level of independence with activities of daily living (ADL) and occupations, functional mobility, body weight distribution, posture, sensory status, presence of edema, skin integrity, and time spent in the wheelchair. It is important that the elder be involved in the decision about a wheelchair.
Until recently, there were not much data on outcome satisfaction of wheelchair use. It has been found that the utilization of wheeled mobility devices depends on a number of factors such as the user’s demographics, health factors, wheelchair characteristics and environmental factors, and the quality of service and delivery.42-44 The involvement of the user in the selection process and the satisfaction related to the mobility device play a significant role in the use or the abandonment of the device.45,46
Proper assessment and selection of a wheelchair are paramount for the satisfaction and utilization of the device. There are a number of key components to a proper assessment.36,47 They are pre-mat assessment and interview, mat physical assessment, objectives and goals, determine the parameters of options (clinical reasoning), possible options, trial of equipment, prescription and letter of necessity, delivery and fitting, and follow-up.47 The interview with the elder and caregiver and the gathering of background information help get a complete picture of the clinical situation and the elder’s goals for the use of the wheelchair along with the concern of whether the elder already has a wheelchair.36 There are future considerations when positioning a person of any age and size. They include tilt versus recline, is the elder agitated or cognitively impaired, clinical indicators/medical necessity, and bariatric client considerations.47
Key issues to address when assessing and selecting a wheelchair for a bariatric elder are center of gravity, additional assessment measurements, and specific issues of the bariatric elder, such as stability and mobility, overall width, adjustability for changing shapes, and transportability.47 The one-size-fits-all approach will not work with bariatric elders because of the varying weight distribution. Dr. Kevin Huffman, a bariatric consultant and board certified bariatric physician, indicates that generally bariatric women carry weight below the waist, whereas men carry weight above.48
The center of gravity of bariatric individuals tends to be more forward than that of a non-bariatric person.48 The axle is often of the rear wheel on a number of wheelchairs. When working with a bariatric elder, it is important to have an axle that moves to allow for the center of gravity to move forward to accommodate the elder’s center of gravity.47
Seat depth is also important because of the posterior redundant tissue that often makes it difficult for bariatric elders to sit all the way back in their chair. They often appear to be tilted as they are leaning back to touch the back of their chair. There are specific measurements needed to accommodate the posterior redundant tissue and posterior shelf of the client.49 The OT practitioner needs to look at the back support and determine how to accommodate the shape and space of the buttock.49 It is also important to ask how and where the wheelchair will be used. A significant issue is environmental access.49 The OT practitioner will need to access the environment so as to ascertain the accessibility of the wheelchair in the elder’s environment.
Wheelchair abandonment is more likely to occur when the individual’s needs are not addressed.50,51 Once a proper wheelchair has been determined, the COTA must help monitor the patient in all of the areas previously assessed.
Certain aspects of wheelchair seating and positioning are of particular importance to elders. Because of musculoskeletal changes, the elder’s posture needs to be monitored continuously. In addition, elders are more at risk for skin breakdown. Therefore, the COTA should help monitor this and educate the elder about the need for pressure relief on a regular schedule. The COTA may also be responsible for making sure the components of a wheelchair are working properly. If a needed repair is identified, the COTA can help facilitate a follow-up visit with the wheelchair vendor.
Skin breakdown can occur quickly with elders. There are several types of skin breakdown related to improper seating, including abrasion, pressure, and shearing. Abrasion occurs when the skin rubs against a surface and causes damage to the tissue.41 An example of this may be when an overweight individual sits in a standard-size wheelchair, and his or her hips rub against the armrest. In addition, rubbing against any sharp areas can cause an abrasion. Elders generally have fragile skin, and an abrasion can occur with very little rubbing.41 A COTA should be aware of this risk and evaluate if any abrasions occur.
Pressure occurs when the forces of two surfaces act against each other. In an optimal wheelchair seating system, pressure will be equally distributed between the person and the seating system. Unfortunately, this equal distribution can be difficult to achieve and maintain, and therefore pressure sores may develop. A pressure sore occurs when the blood circulation to an area is decreased. Subsequently, oxygen does not flow to those cells and death of the cells may occur. After death of the cells occurs, necrosis takes place, and a pressure sore results. Pressure sores develop from the inside out, generally in areas with bony prominences. The ischial tuberosities and sacrum are areas in which pressure sores commonly occur because of improper seating. A COTA should be aware of this risk and continually monitor whether an elder is at risk for pressure sores. Elders who are particularly slender may be at more risk for a pressure sore. All elders should be seated on some type of wheelchair cushion after a proper OT evaluation.
Shearing is another cause of skin breakdown. Shearing also occurs when two surfaces rub against each other. It is not uncommon for shearing to happen with elders seated improperly in sling wheelchairs. The sling does not adequately support the pelvis, and elders may slump in their chair, causing shearing at the ischial tuberosities and sacral areas. In addition, the risk for shearing in those same areas and in the spinous processes increases with a chair that reclines.41
The COTA can help elders learn how to monitor their skin for potential breakdown. Any areas of redness, particularly over bony prominences, can quickly turn into an abrasion or pressure ulcer. The COTA can advise the elders and their caregivers about how to complete a skin inspection. The COTA also can help adapt or modify mirrors to help elders view their skin.
The COTA should also be mindful that a bariatric client has redundant tissue that may get pinched or stuck in crevices, and hence the COTA will need to check for potential areas and consult with the OTR on how to accommodate this. Oftentimes the bariatric client has skin integrity issues in regards to the legs. A padded articulating calf support that is adjustable will help.48 The COTA needs to make sure to protect the client from all sharp objects and parts with the addition of padding in strategic locations on the chair.
It is important for the COTA to be aware of the optimal seating position. The most important element of proper seating is the position of the pelvis. The pelvis is the base of support when one is sitting. The pelvis should be in a neutral position with weight equally distributed between the left and right ischial tuberosities. The trunk should have slight lordosis in the lumbar area, slight kyphosis in the thoracic region, and a small amount of cervical extension.41
The elder’s femurs should be in neutral position, with a slight abduction of the hips and 90 degrees of flexion at the hip, knee, and ankle. The arms should be supported by the armrests with the elbows slightly forward of the shoulders.41 The armrests should be an adequate height to support the arms but not to elevate the shoulders (Figure 14-2).
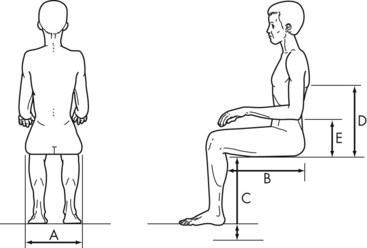
FIGURE 14-2 General guidelines for wheelchair measurement. A, Seat width. B, Seat depth. C, Seat height. D, Backrest height. E, Armrest height.
(Adapted from Wilson, A. B. Jr. (1992). Wheelchairs: A Prescription Guide. New York: Demos.)
Improved posture in a wheelchair can help physiological functions such as breathing, swallowing, and digestion.40 In addition, adjusting posture can improve socialization by simply changing the elder’s eye gaze to allow for more interactions in the environment. Comfort is often improved with proper seating, which may also impact elders’ tolerance and endurance to sit in their wheelchair for longer periods.
The COTA can observe the posture of elders in their wheelchair and make note of any abnormalities such as posterior tilt of the pelvis, sliding forward in the wheelchair, leaning to one side, inadequate arm support, and the inability to self-propel in the wheelchair. If a COTA identified problems in an elder’s current wheelchair system, a referral to an OTR would be indicated for the reevaluation of the seating system. The negative impact of poor seating on frail elders is summarized in Table 14-2.40
TABLE 14-2 Negative Impact of Poor Seating on Frail Elders
| Seating problem | Result on body | Potential negative impact |
|---|---|---|
| Wheelchair too tall | ||
| Poor back support | ||
| Wheelchair too heavy | ||
| Wheelchair too wide | ||
| Hammocking effect | ||
| Foot rests too high |
From Rader, J., Jones, D., & Miller, L. (2000). The importance of individualized wheelchair seating for frail older adults. Journal of Gerontological Nursing, 26, 24-32.
Because of insurance restrictions, elders often find themselves in rental wheelchairs with sling upholstery. Sling-upholstered wheelchairs were not designed to be primary or long-term seating systems; they were designed to transport people through short distances.40 People seated for long periods in sling-upholstered wheelchairs often develop poor posture, including posterior pelvic tilt and kyphosis, in the thoracic and lumbar regions. This type of posture increases the possibility of skin breakdown and limits elders’ ability to engage in their occupations. Simple remedies, such as inserting a solid seat or back, or both, can significantly improve the situation for elders. COTAs can help identify problems associated with poor wheelchair seating and positioning and help recommend changes to improve independence.
Pain and agitation also have been associated with improper positioning of elders in wheelchairs.52 As a result, elders with these symptoms may find themselves with restraints in their wheelchairs. Unfortunately, this usage of restraints can cause further agitation and can decrease the elder’s level of alertness and ability to participate in occupations. Other elders may find themselves sliding or leaning in the wheelchair. Caregivers often use seating restraint to help with posture.40 The use of a restraint to correct posture does not address the cause for the misalignment, which is poor seating and positioning. Therefore, the COTA should be careful when monitoring the elder’s posture in a wheelchair. See Part 1 of the chapter for a review of the proper usage of restraints, and see Box 14-3 for common seating observations.40
BOX 14-3
Observations That Should Trigger a Seating Assessment
From Rader, Jones, & Miller. (2000). The importance of individualized wheelchair seating for frail older adults. Journal of Gerontological Nursing, 26, 24-32.
COTAs can also help determine elders’ functional levels in their current seating system. Because of insurance restrictions from Medicare noted earlier, elders often are set up with heavy, standard-sized wheelchairs that can impede their ability to participate in activities. A study of nursing home residents by Simmons and colleagues53 indicated a positive correlation between hand-grip strength and wheelchair endurance. This study revealed that simple modifications, such as extending brake handles, modifying seat-to-floor height, and prescribing lightweight wheelchairs when appropriate, would increase the elder’s participation within the nursing home.
If a COTA notices a decrease in an elder’s functional activity, it would be important to determine whether the seating system is impairing the elder’s ability to participate in certain activities. Of particular importance would be to determine whether the elder’s strength has decreased. A decrease in any level of strength may also mean a decrease in the elder’s ability to transfer to and from a wheelchair and/or self-propel to activities. The COTA can discuss with elders what factors are impeding their participation in activities. It may be that a simple solution, such as extending the hand brakes or oiling the flip-up footplates, can facilitate increased participation in an activity.
Conclusion
A good wheelchair seating system can support improvements in posture, comfort, independence, and endurance, while preventing skin breakdown. Furthermore, a good system can help elders increase their tolerance for being in the wheelchair, increase socialization, and decrease the burden on caregivers.40 The COTA should work closely with elders, caregivers, the OTR, and the interdisciplinary team to ensure an optimal wheelchair seating system for each elder, no matter their size or shape.
PART 3 Fall Prevention
LOU JENSEN AND SANDRA HATTORI OKADA
Elsa is a 74-year-old woman who was recently widowed. Elsa is independent in most of her basic ADL but had required her husband to assist her in getting into and out of her bathtub. Since his death, Elsa has attempted this task by herself but has had several near falls. She was accustomed to relying on her husband Robert for many instrumental activities of daily living (IADL) such as housework, yard maintenance, shopping, and driving. Elsa has the reputation among her friends as being a wonderful cook, but, in recent years, she was finding herself relying on her husband to be her “eyes in the kitchen” as Elsa’s macular degeneration was progressing, making it increasingly difficult to read the dial on the stove and to see while she prepared meals. After her husband’s death, Elsa has had increasing difficulty keeping up with her home maintenance. Additionally, she does not want to burden her friends and neighbors for transportation, so she has drastically decreased time spent in activities outside of her home such as medical appointments, church activities, and other social events. This decrease in physical activity coupled with situational depression has left Elsa feeling isolated, weak, and fearful of the future.
Recently, Elsa was visiting on the phone with her daughter who lives out of state and admitted that she has fallen inside her home twice in the last week. Elsa’s daughter is quite concerned and encouraged her mother to visit with her physician. Elsa is hesitant, stating, “The next thing you know, I’ll have to move into a nursing home, and I can’t bear to leave my house. If I leave here, I’m afraid my memories of Robert will quickly fade away.”
Falls among the elderly are a complex and significant health problem that can lead to participation restrictions, activity limitations, altered living situations (e.g., premature nursing home admissions), injury, and even death. A fall is “an unexpected event in which the participant comes to rest on the ground, floor, or lower level.”54 Roughly one out of every three adults age 65 and older experience at least one fall per year.55,56 This ratio increases to one half of elders age 80 and older.57 Accidental falls are the leading cause of nonfatal injuries treated in hospital emergency departments in all adult age groups and account for 40% of hospital admissions for older adults.58 Of those elders hospitalized for injuries related to a fall, about half are discharged to nursing homes.59 Elders who sustain a hip fracture as a result of a fall have a 34% mortality rate within 1 year of the fracture.60 Falls are the leading cause of death from injury in those age 65 and older.58 Falls that do not cause physical injury often cause a fear of falling that results in a decrease in occupational participation and independence,61 and impairments in client factors such as strength and balance because of a decrease in overall activity level.62
The effect of a fall on the life of an elder alone emphasizes the importance of including fall prevention into the care plan of any elder. However, the financial impact of falls on the health care system and society adds additional justification for addressing this important health problem. The estimated total direct cost annually of all fall injuries for people age 65 and older exceeds $19 billion.63
On an individual level, costs associated with a fall-produced fracture are $58,120 for the first year and $86,967 for a lifetime.64 As the elder population increases in the next 30 years, so will the incidence of falls and the costs associated with them. Therefore, it is important for COTAs to be knowledgeable about the risk factors and causes associated with falls, as well as how the OT process can be used to effectively reduce falls in the elderly.
Risk Factors and Causes of Falls
Falls are multifactorial in nature and can have a variety of precipitating causes (Box 14-4). Elders are particularly vulnerable to falls because of the increased prevalence of intrinsic risk factors such as comorbid clinical conditions, multiple medication regiments, and age-related physiological changes (e.g., decreased vision and decreased muscle strength). More important, a delicate balance exists between intrinsic factors and common environmental hazards; even a small disruption in this dynamic system can lead to a devastating fall. For example, a so-called accidental trip over a new throw rug may cause a fall that could be attributed to the throw rug (i.e., the environment). However, the fall could have been more likely because the elder had impaired vision, lower extremity weakness, and balance deficits (i.e., intrinsic risk factors). Falls in the elderly population can occur in a variety of environments, including the home, community, hospital, or nursing home, although numbers are higher for those in institutional settings.65
BOX 14-4
Causes of and Risk Factors for Falls in Elderly Persons
| Cause | Risk Factor |
|---|---|
Data from Rubenstein and Josephson. (2006).
Environmental Causes
Accidents related to the environment are the primary cause of falls among elders, comprising 31% of falls.65 Over one-third (39%) of falls occur in the home.66 Disease processes associated with aging are often strong determinants for falls, but environmental factors in the home may be a more common cause.67 About 30% of older adults are aging in place (growing old at home), a 32% increase from previous decades.68 A poorly kept home or yard may be an environmental sign of age-related changes. As people age, they may lose the endurance, strength, and cognitive ability to structure tasks and deal with their environment. Common environmental hazards in the home include poor lighting or glare, uneven stairs, lack of handrails by stairs, and uneven or unsafe surfaces (frayed rug edges, slippery floors in the shower and tub, polished floors, cracks in cement, high doorsteps, and so on). Other hazards may involve old, unstable, or low furniture (chairs, beds, or toilets); pets; young children; clutter or electric cords in walkways; inaccessible items; and limited space for ADL functions (Figure 14-3). New, used, or improperly installed equipment and unfamiliar environments may also be hazardous.

FIGURE 14-3 Common potential hazards that may cause falls include rugs and pets that may get under foot.
According to Carpenter and colleagues,66 approximately 55% of falls in the elderly population occur outside of the home. Common areas in the community where falls occur include public buildings, streets, sidewalks, transferring to or from transportation, or another person’s home. In addition, the greatest proportion of persons with repeated falls occur in the community, specifically on the street or sidewalk. The most common activities that elderly persons engage in when they fall include walking on uneven ground, tripping (over curbs, rugs, or objects), and slipping on wet surfaces. Other examples of activities associated with falls include lifting heavy objects, reaching, balancing on items of unstable support (overturned box), or turning quickly. Therefore, the COTA should take into consideration the context and environment, as well as the activity engaged in during a fall when determining a fall prevention plan.66
Biological Causes
Sensory
Visual changes associated with aging that may influence falls include decreases in depth perception, peripheral vision, color discrimination, acuity, and accommodation. Approximately 30% of persons age 65 and older have visual impairments.69,70 As the elderly population grows, so will the number of persons with visual impairments. A visual impairment can affect a person’s ability to participate in functional mobility in the home and in the community.
Stairs may become more difficult to maneuver. Knowing the location of the next step and judging its depth can become a big challenge. That 75% of all stair accidents occur while descending the stairs, most in the second half of the flight, is also noteworthy.25,71 New bifocals or trifocals may require adjustment time, and looking down stairs requires constant head and eye adjustments.
Medical conditions affecting vision include macular degeneration, cataracts, diabetic retinopathy, glaucoma, and stroke.69 These conditions may manifest as scotomas (blind spots), which impair safety in mobility. Objects on the floor, such as pencils and telephone cords, may not be apparent. Elders with visual impairments may also run into furniture. Decreased visual input caused by disease processes may result in a decrease in postural stability.72 In turn, this affects an elder’s balance and may contribute to the greater incidence of falls among this population.
A disorder involving spatial organization or figure ground may cause an elder to perceive a change in rug color or flooring as a stair and glare on the linoleum as spilled liquid. A dark stairway may be perceived as a ramp. Misinterpreting this information may cause a misjudged step and a fall. (Chapter 15 provides more detailed information on age-related changes in vision and recommended adaptations.)
Vestibular disorders that cause dizziness and vertigo may also contribute to falls in the elderly. Benign paroxysmal positional vertigo (BPPV) is a mechanical vestibular problem caused by displaced otoconia in the inner ear as a result of trauma or age.73 BPPV can cause severe dizziness and vertigo, especially with changes in position or head movements. An elder, particularly one who has a history of falls, may be susceptible to this disorder. Indeed, BPPV is the most common cause of vertigo in persons over age 65 years.73
Neurological/Musculoskeletal
Conditions that affect posture and body alignment cause changes in center of gravity, gait, stride, strength, and joint stability, all of which increase the risk for falls. Age-related changes in postural control include decreased proprioception, slower righting reflexes, decreased muscle tone, and increased postural sway.72 Changes in gait include decreased height of stepping. Men tend to have a more flexed posture and wide-based, short-stepped gait, whereas women tend to have a more narrow-based, waddling gait.74 Medical conditions that affect instability include degenerative joint disease, deconditioning, malnutrition, dehydration, and neurological disorders such as neuropathy, stroke, Parkinson’s disease, and dementia.25,71,74 Elderly women are more susceptible to brittle bones, with a greater incidence of osteoporosis after menopause. In the case of brittle bones, it may be a fractured bone that causes the fall rather than vice versa. However, falls in the elderly cause 90% of the incidence of hip fractures.75 Musculoskeletal conditions that contribute to falls in the elderly include osteoarthritis, spondylosis, and a general decrease in joint range of motion.74
To compensate for changes in gait and decreased balance, elders may “furniture glide” by holding on to furniture for support while they walk (Figure 14-4). They may also drag a foot or lose their balance toward their weaker side (stroke), have a shuffling gait (Alzheimer’s disease), or fall forward (Parkinson’s disease) during ADL training. Older adults may hold onto faucets or towel racks to get into the tub or shower or lean against the shower wall for stability while bathing.

Cardiovascular
Age-related changes include orthostatic hypotension, which affects approximately 30% of the elder population.71 Other medical conditions that cause blood pressure changes include hypertension, neuropathy, and diabetes. In addition, these changes can occur as side effects of certain medications. Arrhythmias may cause up to 50% of syncopal episodes in elders.71 Elders may experience a greater incidence of dizziness or light-headedness, with lower cardiac output, autonomic dysfunction, impaired venous return, and prolonged bed rest. Underlying cardiac disease is the most common cause of syncope that may result in a fall.57 Together with extrinsic or environmental factors, these biological or intrinsic factors are the primary causes of falls among elders.25,65,76
Cognitive/Psychosocial Causes
Psychosocial and cognitive risk factors that may influence falls include poor judgment, insight, and problem-solving skills; confusion; and inattention resulting from fatigue, depression, and dementia. Other factors may include reactions to psychotropic medications, fear of falling, unfamiliarity with a new environment or caregiver, and a strong drive for independence. Elders and their families may not comply with recommended safety modifications because of cultural or personal preferences, aesthetic values, and limited financial or social resources. Consequently, both the caregiver and the client are at greater risk for having a fall.
Depression and psychotropic medications have both been associated with an increased fall risk. Depression increases the risk of falling twofold,65 presumably because of an inattention to the environment and a disregard for safety. A systematic review and meta-analysis of drugs and falls revealed an increased risk of falls when associated with psychotropic drug use in elders.77 A later meta-analysis concluded similarly, noting that not enough has been done in the past decade to address this fall risk factor.78
Functional Causes
Performing ADL functions becomes increasingly challenging for elders. About 18% of the elder population report difficulties with ADL, and 26% report difficulties with IADL.79 Functional mobility problems that may lead to falls include difficulty with performing transfers (to or from a lounge chair, bed, toilet, tub or shower, wheelchair, and car), dressing and bathing (especially the lower body), reaching, sitting, standing, and walking unsupported. Other factors may include the lack of assistive aids for ambulation or an inability to use them. Elders with dementia may forget where they left a cane or walk carrying their walker rather than using it for support. Old, lost, borrowed, or smudged glasses may impair vision. Poorly fitting shoes, loose pants with dragging hems, and flimsy sandals with nylons can affect balance. Falls most commonly occur in places where elders perform most self-care activities: by the bed and in the bathroom.25,76
Knowledge of the most common risk factors and causes of falls in the elderly can significantly inform the OT process, as described in the second edition of the Occupational Therapy Practice Framework: Domain and Process.80 COTAs are important team members in all parts of the process and therefore must understand components of a comprehensive fall risk assessment, fall prevention and reduction interventions, and meaningful ways to measure the outcomes of interventions designed to reduce falls in the elderly.
Evaluation
Because falls in the elderly typically result from a combination of several intrinsic and extrinsic risk factors, multiple precipitating causes, and in a variety of environments, fall prevention is an issue for the entire health care team. Team members, including the COTA, can collaborate to perform an accurate evaluation of the client and to obtain a detailed fall history before designing a fall prevention program. Shumway-Cook and colleagues81 found that only half of older adults who fell claimed to have discussed the fall with their health care provider. In this same study, only three-fourths of elders who did discuss their fall with their health care provider were questioned about the cause of the fall, and less than two-thirds received information on fall prevention. Reasons for this communication breakdown may be varied. Elders may be ashamed to admit that they have fallen, or may fear they will be forced to leave their home or lose their independence if they disclose a fall. Conversely, elders may not consider it important or relevant to report a fall in which no injury was sustained. However, open and honest communication is important to successfully address fall prevention. The OTR/COTA team can collaborate to obtain a complete occupational profile that includes fall-related history and must make the establishment of therapeutic rapport a priority to ensure that the information is complete and accurate.
COTAs, in collaboration with OTRs, are well-equipped to assess elders’ fall risk, educate on fall prevention strategies, and provide other resources. In addition to assessing client risk factors related to body structures and functions and performance skills, an interview to obtain an accurate history of falls is necessary. Clients should be asked to describe the frequency, timing, and location of their fall(s), the activities they were involved in during their fall(s) and any devices or equipment used, their medical history and symptoms, and medications taken and their side effects.25,82 If the elder reports no history of falling, care should still be taken to identify risk factors. When asking about functional status, COTAs should not only ask whether the elder is able to perform ADL functions but also observe the way these are done. In other words, the OT evaluation process includes obtaining a detailed occupational profile and analyzing occupational performance.80 For example, when the COTA asked Elsa whether she could get off the toilet by herself, she responded that she was independent with toileting. When the COTA asked her to demonstrate this transfer, Elsa hooked her cane on a towel rack to pull herself off of the toilet. The COTA was able to determine a high risk for falling only because the transfer was observed. If the COTA had simply accepted Elsa’s report of independence, she would not have been able to recommend a raised toilet seat and toilet rails or replacement of the towel racks with sturdy grab bars.
The extensiveness of the evaluation process and team members involved depends on the planned fall prevention strategy. A team approach may be the most beneficial method to address fall prevention. For example, OT practitioners are well-suited to address safe performance of daily occupations. A referral to physical therapy may be indicated to address weakness, balance and coordination deficits, and overall endurance. A nutritionist or dietitian may be included to determine the adequacy of a client’s diet and whether modifications that would improve overall health and strength need to be made. Pharmacists can review medications and potential side effects that may lead to an increased risk of falling. Referrals to any number of medical specialists could be indicated if a client has an underlying medical condition that affects their fall risk. Once the necessary referrals are made and the team has established goals with the client, intervention can begin.
Fall Prevention Interventions
Rubenstein and Josephson65 have classified current fall prevention interventions for the elderly into five broad categories: multidimensional fall risk assessment and risk reduction; exercise-based intervention; environmental assessment and modification; institutional approaches; and multifactorial approaches, including medical management of the elder. COTAs can be involved, in varying degrees, in each of these interventions.
Review of the Evidence
Several Cochrane systematic reviews of the available evidence for preventing falls in older people have been conducted in recent years. In a review of 111 trials involving 55,3030 community-dwelling participants, exercise-based interventions (group or individual) that targeted two or more performance skills (e.g., strength, balance, flexibility, or endurance) reduced the rate of falls and risk of falling in the elderly.56 Multifactorial interventions also reduced the rate of falls in older community-dwelling adults. Interventions designed to improve safety in the home were found to be effective in reducing falls in high-risk elder populations only, such as persons with visual impairment.
A separate review, using 41 trials (25,422 participants), was conducted by Cameron and colleagues83 for older people in institutions. For elders in nursing homes, exercise-based and multifactorial interventions produced variable results on reducing falls. These interventions were most successful when implemented by a coordinated health care team. The evidence did suggest that the prescription of vitamin D and a medication review by a pharmacist reduced falls. For elders in hospitals, interventions that targeted multiple risk factors and supervised exercise were effective in reducing falls.
Multidimensional Fall Risk Assessment and Risk Reduction
The goal of the multidimensional approach for fall prevention in the elder population is to target the multiple risk factors associated with falls to reduce fall risk. This approach can be used for both individuals and populations. For example, a multidimensional fall prevention program can be offered to a population of community-dwelling well elders to educate them on ways to prevent falls and to screen elders to determine their fall risk. Health fairs and community educational programs are two examples of a population-based multidimensional approach for fall prevention. Conversely, an individualized multidimensional fall prevention program may be instituted for an elder who has a history of falls or is at high risk for falling. In either case, fall risk assessment precedes intervention and consists of a fall history, general medical and medication history, and an assessment of client factors and performance skills.
Exercise-Based Intervention
As mentioned previously, exercise-based interventions have been found to effectively reduce falls in elders.56,84 General strengthening programs incorporated in the elder’s daily routine can help decrease deconditioning, especially that caused by a sedentary lifestyle. In addition to OT-led exercise programs, COTAs may also refer elders to physical therapy for general lower extremity strengthening and balance exercises.72 Community exercise programs, such as dancing, water aerobics, swimming, and walking clubs, are also appropriate recommendations.
Activities that target balance can be incorporated into the OT treatment plan. A careful balance of activities designed to remediate balance with those that allow compensation needs to be considered. Tai Chi is a form of exercise that has been shown to be effective in reducing falls and improving balance.56,85,86
Gradual increases in activity are recommended for people with conditions that affect endurance (such as cardiac conditions and deconditioning). Strategically located sturdy chairs may be useful for elders who require rest periods when going from one room to another. Sitting while bathing and avoiding long hot baths are also recommended. A commode chair by the bed may save energy. Activities that involve straining and holding one’s breath (such as during toileting, strenuous transfers, or exercise) can cause light-headedness and should be monitored.
Environmental Assessment and Modifications
OT practitioners, with their focus on the importance of the environment on occupation, are well-equipped to perform home assessments and make modification to improve safety and reduce fall risks in elder populations. Home safety checklists can be provided as a preventive measure for well elders. Often, however, home safety assessments are more beneficial in detecting potential environmental hazards and making individualized recommendations to clients to improve safety.
Bathroom modifications may include a tub or shower bench with armrests and back, a handheld shower hose, grab bars, or a raised toilet seat. Throw rugs should be removed, or nonskid backing should be applied under them. Nonskid stripping or rubber mats can be placed on tub or shower floors. Sliding glass doors should be removed to allow for wider access into the tub. A shower curtain may be hung from a pressure mounted bar to provide privacy if the glass doors are removed. Heat-sensitive safety valves also can be installed to prevent scalding. If the elder uses a wheelchair and the door to the bathroom is too narrow, a rolling shower bench or commode chair with wheels may help. Placing a commode chair by the bed may eliminate unsafe night transfers to the bathroom toilet. A three-in-one commode chair is an inexpensive solution. This type of commode is light and can be used at bedside, over the toilet, or in the tub or shower. Caregivers should remember, however, that emptying the commode bucket and lifting and relocating the commode can be difficult for elders. They should be discouraged from using soap dispensers, towel racks, and toilet paper holders for support. Hygiene items should be placed within reach. Mirrors may be tilted or lowered for better viewing during ADL functions. Doors under the sink should be removed to give the elder more leg room while sitting in front of the sink.
Similar precautions should be taken in the kitchen. Step stools should be avoided, and frequently used utensils and dishes should be rearranged so they are within safe reach. Use of energy conservation techniques during meal preparation may decrease the risk for falling because of fatigue or orthostatic hypotension. Simple meal preparation packages are widely available in grocery stores. Use of a microwave can help decrease the amount of time an elder spends standing at a stove to prepare a meal.
About 30% of all falls in the elderly occur in the home.66 Of those elders who fell during ADL, 22% had falls that occurred when they tried to get out of bed or up from a chair. The height of seats (beds, sofas, chairs) can be increased with firm cushions. Worn mattresses or cushions should be rotated. Chairs with armrests are recommended to facilitate rising from the chair. Chairs with wheels should be avoided, and the brakes of wheelchairs and commodes must be secured before transfers are attempted. Elders should lean forward in the wheelchair only when both feet are flat on the floor (not on the footrests). Electronic lift chairs are typically available in furniture stores.
Caregivers must ensure that stairs are well lit, with no glare, and equipped with railings running along the entire length of the stairwell on both sides. Stripping of various colors can be used at the edge of each step to distinguish them from each other. Safety grip strips may be placed on each step as well. Light switches should be within reach at both the top and bottom of the stairway. COTAs should discuss with elders safe ways to change a light bulb. User-friendly, touch-sensitive, and motion-sensor light switches are also available. Transition areas such as doorways, garages, and patios are common sites for falls. COTAs should look at the outdoor environment, transition areas, and the indoor environment to help prevent falls.
Interventions to compensate for visual loss include increased lighting with limited glare, improved contrast for steps and furniture, decreased clutter in walkways, and well maintained flooring. COTAs should anticipate elders’ performance at different times of the day, with varied natural lighting and indoor lighting. Referrals to vision specialists may be appropriate to ensure that elders are wearing the appropriate eyewear.
Environmental modifications can also include modifications of the objects commonly used during ADL by the elder. COTAs should encourage elders to wear sturdy, comfortable, rubber-soled footwear (e.g., tennis shoes) to help obtain a more secure footing. Some elders may wear slip-on shoes because tying or fastening shoes is difficult. Assistive devices such as elastic laces or Velcro closures may help address this difficulty and provide the elder with more stable footwear to help prevent falls. When dressing, elders should pull pant legs above their ankles before standing. Pants should be pulled down after transferring from the wheelchair to the toilet to avoid tripping.
Elders with a reach of less than 6 to 7 inches are also limited in their mobility skills and are the most restricted in ADL functions.74 Older adults who have difficulty reaching and carrying objects may require reachers, extended handles on bath brushes or shoe horns, carts, walker trays or bags, and sock aids. COTAs play an important role in educating elders in the proper use of these assistive devices so that the devices themselves do not become fall hazards. COTAs can also help the elder problem-solve unique situations. For example, they can determine the best way to attach the reacher to the walker or rearrange items around the living space so they are within reach. Higher electrical outlets also could be recommended to limit the need to reach and bend. Redesigning or rearranging an elder’s environment is often an inexpensive and effective fall prevention technique. However, it is important to consider that rearranging furniture may disorient an elder, which could increase the possibility of a fall. Environment redesign should occur only with the consent of the elder, and follow-up visits are recommended to assess the transition.
Difficulty with transfers and mobility during ADL functions may require safety training with the cane, walker, or wheelchair. This is particularly important because many falls occur in transit during transfers. Elders with nocturia, a normal age change involving increased frequency of urination at night, have a particular need for night lights and a clear passage to the toilet. Before rearranging furniture to provide wider walkways, COTAs must first make sure elders do not need the furniture for stability when ambulating. A consultation with a physical therapist may help clarify the most appropriate and safe assistive device for ambulation.
Institutional Interventions
Institution interventions are fall prevention strategies implemented in institutions such as hospitals, nursing homes, and assisted living facilities. Hospitals often have screening procedures for all patients, which include assessing patients for their fall risk. Often, these screens include an evaluation of cognition and balance by a physician and/or OTR. For those patients found to be at high risk for falls, bed or chair alarms, increased supervision (e.g., a sitter in the room or room placement close to the nursing station), low hospital beds, and the judicious use of restraints (e.g., bed rails, wrist restraints, and restraint vests) are all viable options for keeping the patient safe from falls. Additionally, early mobilization and participation in familiar ADL are recommended to address fall risk.
Nursing homes and assisted living facilities can also implement programs in addition to those mentioned previously to reduce fall risks. Examples include dedicated fall-reduction staff who can provide more supervision and multifaceted fall reduction interventions,87-89 walking and other exercise-based programs to improve client factors, staff education and policies related to fall reduction and reporting, and so on. Previously discussed in the chapter were methods of restraint reduction and proper seating and positioning. Addressing these issues can also reduce falls among elders in institutional settings.
Multifactorial Interventions
Multifactorial interventions are those that incorporate several strategies into a coordinated fall prevention program. This is a useful approach for COTAs who want to ensure they are using a holistic, client-centered approach. Included in the OT plan of care should be referrals to other health professionals who are educated on managing the often complex medical issues of elders. Elders who report dizziness with a change in position may be experiencing a decrease in blood pressure that could result in a fall with or without syncope. A referral to the elder’s physician would facilitate medical management of this problem. Meanwhile, the COTA should monitor the elder’s blood pressure, and elders should be allowed to make slow transitions from supine to sitting or sitting to standing positions. A few minutes may be necessary to allow the blood pressure to accommodate to the change in head position. By teaching elders different techniques for dressing and bathing and instructing them in the use of long-handle devices, COTAs can help elders limit and modify their bending. A typical recommendation is that the elder get dressed while seated to help accommodate for orthostatic hypotension. The rest of the health care team should be informed of reports of dizziness and unstable changes in blood pressure.
COTAs, elders, family members, and caregivers should work together to identify activities important to elders that can be modified to prevent falls. Family members should be included because elders may depend on them to help with preparation and assistance. Elders may prefer to perform toileting activities independently but may not mind assistance with feeding. COTAs should identify personal and shared spaces in the elder’s living environment. If family members do not want to modify the only bathroom in the home with a raised toilet seat and grab bars, a commode chair by the elder’s bed may be appropriate. COTAs should help elders and their family members address safety concerns and practice giving assistance in a safe environment.
Additional areas to consider are the frequency and occurrence of falls. If elders experience repeated falls, their confidence levels may decrease, which could result in a decrease in participation in ADL and IADL.67 The time of day that a fall occurs is also important information to obtain. About 64% of elders in a study reported falls in the afternoon to late afternoon period.67 The afternoon is generally a time of increased activity for elders, and the assessment of ADL and IADL should address the time factor.
COTAs should make sure that strategies exist for emergency situations. Typical questions include the following: If a curtain is not drawn, will the neighbor know that this may be an indication of trouble? If an elder falls, will he or she know the proper way to get up from the floor if no injuries are apparent? Is a telephone within reach? Is a list of emergency phone numbers placed by the phone? If the elder is at home alone, are there emergency alert systems available to signal for help? Is a telephone reassurance program available in which a volunteer calls daily? Is it safer to soil clothes than risk an unassisted transfer to the toilet? All of these questions should be addressed to ensure the elder’s safety before discharge from OT. See Box 14-5 for additional safety tips.
BOX 14-5
Safety Tips
Consider referrals to others on the health care team. Periodic medication reviews by a pharmacist and medical check-ups by a physician are important safeguards against falls.
Exercise has been shown to reduce falls in the elderly. Be sure to proceed with exercise programs that take into account individual elder’s comorbidities and functional status.
Consider issuing and educating on adaptive equipment (e.g., grab bars, tub benches or shower chairs, and bedside commodes) when full remediation is not possible.
Home safety assessments are beneficial to address occupations in context and to reduce environmental hazards such as poor lighting, excessive clutter, and unsafe walking surfaces.
Address safety measures and recommend that a cellular or cordless phone always be within reach of an elder at risk for falls (e.g., in a walker bag, fanny pack).
Outcomes
Identifying outcomes that are important to the client and that can be measured to demonstrate the effectiveness of OT intervention is an important step in the occupational therapy process. Ideally, outcomes are selected collaboratively by the client and OT practitioner(s) early in the therapy process. COTAs, with guidance from OTRs, can contribute to outcomes identification and use. The Framework80 describes nine broad outcomes for any OT intervention, any of which may be appropriate, depending on which fall prevention strategy is used.
Prevention is an obvious outcome to select in fall prevention programs. The number of falls experienced by the client can be counted during a specified time frame and compared to the number of falls experienced by the client before intervention. These data can provide evidence of the effectiveness of the fall prevention intervention. However, not all clients have experienced falls before OT intervention but may have risk factors for falls. Therefore, this outcome alone may not be an adequate measure of success.
Adaptation, health, and wellness can be measurable outcomes in fall prevention programs. Secondary effects of such interventions may be a positive change, or adaptation, in body functions and performance skills such as strength, balance, visual acuity, or endurance. If deficits in these functions and skills were intrinsic risk factors for falls, an improvement may help decrease fall risk. For example, if a client had poor muscle strength and balance, and strengthening and balance activities were included in the intervention plan, appropriate outcome measures would be manual muscle testing or a balance or fall-risk assessment. Many valid and reliable balance assessments are available and can be easily administered.
Occupational performance and role competence are commonly used outcomes in OT practice and may be the client’s desired outcomes for fall prevention interventions. For example, if safety with bathing or showering is addressed through environmental modifications, a client’s occupational performance may improve from needing assistance with tub transfers to being independent with tub transfers as long as a tub transfer bench is used.
Self-advocacy may be a selected outcome. If a client discovers, through guidance from an OT practitioner, that he or she is no longer safe to ambulate in the community because of high fall risk, the ability to self-advocate for community transportation services may be an appropriate outcome.
Participation and quality of life should always be overarching outcomes for any intervention, including fall prevention. Simply helping a client improve endurance and balance does not ensure that he or she can safely and comfortably participate in desired life events and believe that he or she has an improved quality of life. COTAs must be sure to carry out interventions in their natural contexts and ensure that clients are able to participate in these contexts. Many standardized measures of participation and quality of life exist, as well.
Finally, occupational justice is defined as “access to and participation in the full range of meaningful and enriching occupations afforded to others.”80 Care must be taken to design fall prevention interventions such that clients have a reasonable balance between freedom from falls and participation in meaningful occupations. Fall prevention may be extremely challenging if a client has irreversible risk factors such as dementia or blindness. However, if the only answer to fall prevention appears to be a drastic reduction in physical activities so that falls are minimized, the client may potentially sacrifice or be denied access to meaningful living.
Case Study
Let us revisit the case of Elsa. Elsa’s daughter finally convinced her to visit with her physician about her recent falls. The physician ordered home health occupational and physical therapy services for Elsa. Based on what you know about effective fall prevention, answer the questions below.
1. What risk factors does Elsa have that contribute to her falling?
2. What further information would you want to have before designing a fall prevention intervention plan? Specifically, what further questions would you want to ask Elsa, and what assessments and/or functional observations would you want to observe?
3. Which fall prevention approach(es) would be most appropriate for Elsa? Describe two intervention activities for each approach.
4. Finally, consider what outcomes would be most appropriate for Elsa. What specific measures would you, along with the OTR and client, choose?
PART 4 Community Mobility
PENNI JEAN LAVOOT, MICHELE LUTHER-KRUG, AND MARY ELLEN KEITH
Most elders prefer the freedom of traveling by automobile (Figure 14-5). Driving is an important factor in their independence and mental health.90 By the year 2030, one in five American drivers will be age 65 years or older.91 In 2008, elders represented 15% of all licensed drivers in the United States and accounted for 15% of all traffic fatalities.92 Most of these fatalities involving older drivers occur during the daytime (80%), on weekdays (72%), and involve other vehicles (69%).92 Elders are becoming increasingly more reliant on automotive transportation. The reason could be that the majority of elders live in rural or suburban communities. Often in these communities there are limited or no resources available for transportation options for seniors. COTAs can help elders assess the resources within the elders’ local communities.93

Elders may experience age-related changes that can negatively affect their ability to drive, including decreased visual acuity, color discrimination, depth perception, figure ground and peripheral vision, and increased sensitivity to glare.94 Other factors that may influence driving and mobility include unrecognized disease processes, physical changes, psychosocial issues, medications, cognitive changes, reduction in hearing ability, and environmental issues such as small print on signs. Physical changes contributing to driving abilities of elders also include changes in sensation, range of motion, decrease in reaction time, and decrease in decision-making abilities.95
Age-related changes affect the mobility of elders, whether they are pedestrians, drivers, or users of public transportation. For example, pedestrians may have difficulty stepping up or down from curbs or crossing streets within the time allotted by crossing signals (Figure 14-6). Drivers may have difficulties merging, yielding the right of way, negotiating intersections, backing up, handling quick maneuvers, reading traffic signs, and making left turns.96 Physical barriers may make public transportation inaccessible. All of these challenges may rob elders of the freedom and independence they may have enjoyed throughout their lives.

A common goal of OT is to assist elders in being as independent as possible in their homes and communities.97 As with most adults, an elder regularly goes to the doctor’s office, grocery store, places of worship, bank, salon/barber, and pharmacy. These places may be around the corner or many miles from the elder’s home. The role of the COTA in helping identify realistic goals and treatment plans for elders often includes increasing their ability to move in the community. To do this effectively, COTAs must explore as many options as possible for community mobility (Box 14-6). Community transportation options vary greatly among rural areas and cities.
BOX 14-6 Information-Gathering Questions
1. What method of transportation do you typically use to get around in the community?
2. Have you driven before, and do you currently drive?
3. Do you own and drive a car? What kind?
4. Have you noticed any difficulties operating a car?
5. When was the last time you were tested at the Department of Motor Vehicles?
6. When was the last time you had your vision tested?
7. Do you have any conditions that might affect your ability to operate a motor vehicle?
8. Are you familiar with your community?
9. Do you have difficulties driving at night or with glare?
10. How many miles do you drive a year?
11. In the past 5 years have you had any accidents? Moving violations? Please describe.
12. Have you ever used public transportation?
13. Would you be willing to use public transportation? If not, why?
14. Do you need any assistance to get in and out of a car or public transportation?
15. Do you know how to read a bus schedule?
16. Are you familiar with any community resources for transportation?
Pedestrian Safety
Walking safely is an important factor in community mobility. Elders account for 18.3% of all pedestrian fatalities.92 COTAs should evaluate the ability of elders to walk outdoors. Box 14-7 lists precautions for safe walking in an elder’s community.
BOX 14-7
Pedestrian Safety Tips
2. Use the pedestrian push button and wait for the WALK sign to appear.
3. Before stepping into the roadway, search for turning vehicles, look left-right-left, and keep looking while crossing.
4. Wear bright (fluorescent) colors during daylight and wear reflective material and carry a flashlight if walking at night.
Adapted from the American Automobile Association. (1993). Walking through the years. Heathrow, FL: Traffic Safety and Engineering Department.
Elders who use wheelchairs, walkers, and scooters usually have more difficulty and require more time conquering crosswalks, curbs, and uneven sidewalks. These elders need training to negotiate cutout curbs because electric scooters or wheelchairs may overturn when descending. Electric scooters with three wheels tend to tip more often than those with four wheels. A mobility expert should conduct an evaluation to determine the type of equipment needed. This evaluation should take into consideration the elder’s cognition, physical impairments, home environment, seating and positioning needs, and the progression of disease. Whenever possible, COTAs should provide safety training with the exact type of mobility equipment that elders will be using in the community. COTAs also can help elders advocate for curb cuts or longer crossing times at various intersections to ensure independence and safety in the community. To this end, the city’s Traffic Commission or the Architectural and Transportation Barriers Compliance Board can be of assistance.
Elders who fatigue easily or are unable to walk long distances may consider using an electric scooter or wheelchair (Figure 14-7). Golf carts can be especially helpful for elders who live in a planned retirement community and stay within the closed community area. An obstacle course can be set up to determine the elder’s ability to maneuver before this expensive device is purchased. An evaluation in wheelchair and scooter prescriptions by a specialist is also recommended before purchase.
If elders need to transport a wheelchair or scooter in their personal vehicles, community mobility becomes much more complicated. Wheeled power mobility devices should be transported only in a van fitted with an electric lift or ramp of the appropriate size and weight. A driver rehabilitation professional should evaluate each case before a van or lift is purchased to prevent expensive mistakes such as incompatible equipment. A driver rehabilitation professional takes into account many factors, including the type of wheelchair or scooter that must be transported, whether the person needing the equipment will be a driver or passenger, and the length of time that the equipment will be needed. They can also determine the ability of the elder to operate the prescribed equipment. The diagnosis of the elder is also important. An elder with a progressive illness has different needs than an elder without a progressive illness. A driver rehabilitation professional can be found by contacting the Association of Driver Rehabilitation Specialists (ADED) (http://driver-ed.org) or the AOTA Older Driver Initiative.
The driver rehabilitation professional can also provide resources for vendors who install adaptive equipment for vehicles in a particular geographic area. The National Mobility Equipment Dealers Association is a resource for locating these qualified vehicle modifiers/dealers. Before an electric lift, ramp, or scooter carrier is purchased, the prospective user should demonstrate an ability to perform the entire loading process using the recommended equipment. COTAs can assist elders by providing information on driver rehabilitation specialists in the area.
In contrast to power wheelchairs, power scooters can be transported in a variety of ways. They can be stored in the trunk of some cars or on the back of the vehicle. The COTA can refer the elder or caregiver to a driver rehabilitation professional to assist with assessing the safest loading devices, based on the balance and function of the elder client. The elder and caregivers must practice every step of this process before the equipment is purchased. The mobility device and personal vehicle must be compatible for safety reasons. Checking with the manufacturer of the vehicle to see whether it can handle the extra weight of a scooter carrier is necessary.
COTAs can assist the elder driver in applying for a disabled parking placard, usually issued by the Department of Motor Vehicles (DMV) of each state. This entitles the driver of the car to park close to buildings and may also include assistance at the gas station. Some elder drivers do not apply for this placard because they do not understand the application procedure. Other elders may not apply because of a perceived social stigma. It is important for the COTA to help the elder determine the requirements for a disabled parking placard. In many states, the form must be filled out and signed by a licensed physician.
Alternative Transportation
When planning OT intervention, COTAs must take into consideration the individual’s lifestyle and needs.97 This is especially true for elders who have never driven, are now unable to drive because of impairments, voluntarily decide not to drive, or want the option of using community transportation in addition to their personal vehicles. Elders who relied on others for transportation may need to learn to drive, especially if those people are no longer available. COTAs should help the elder investigate community transportation resources available where the elder currently resides or is planning to live. Information on alternative transportation can be obtained by calling city hall, a local senior citizens’ center, the local DMV, local transportation agencies, the area’s Office on Aging, and the local American Association of Retired Persons (AARP) offices. Independent living centers in the community may also be good sources of information. When calling these agencies, COTAs should help the elder obtain information about application procedures, cost, distance traveled, eligibility requirements, and the type of additional equipment available on the vehicles.
Title II of the Americans with Disabilities Act (ADA) addresses many needs of elders with disabilities. This act states that no qualified individual with a disability shall, by reason of that disability, be excluded from participating in or be denied the benefits of the services, programs, or activities of a public entity. According to the ADA, a qualified individual is defined as a person with a disability who meets the essential eligibility requirements for receiving services or participating in programs or activities provided by a public entity. The individual may meet these qualifications with or without reasonable modifications to rules, policies, or practices. They may also qualify with or without the removal of architectural barriers or the provision of auxiliary aids and services. Public entity refers to any state or local government or instrumentality of a state or local government. The paratransit and other special transportation services provided by public entities are designed to be usable by individuals with disabilities, be they physical or mental, who need the assistance of another individual to board, ride, or disembark from any vehicle on the system. Individuals for whom no fixed and accessible route transit (usually a public bus) is available are also eligible for paratransit and special transportation services. However, a fixed, accessible route transit should be used if available (Figure 14-8).98

FIGURE 14-8 Elders may need to learn to use community transportation in addition to their personal vehicle.
Elders who have impairments that prevent them from traveling to or from a boarding location for fixed transportation may also be eligible for special services. Under the law, any individual accompanying the person with the disability may be eligible for paratransit services, provided that space is available and other people with disabilities are not displaced (Figure 14-9).99 This means that if elders with a disability cannot use the available bus system, another transportation system that can pick them up directly from their home must be provided. COTAs working with elders who have a disability must know the ADA as it relates to transportation and accessibility. COTAs also should become knowledgeable about the paratransit services in the local community.

FIGURE 14-9 Public transportation may be a viable option for elders who may no longer be able to drive.
As good as paratransit services may be, they almost never help elders in leaving their homes. Regardless of whether elders are using a bus, paratransit service, or personal vehicle, their ability to safely exit their homes is of critical importance and must be evaluated to determine whether available services should be used. Information regarding this issue can be found in Part 2 of the chapter. The elder may be unable to climb stairs or even unlock or lock the door. COTAs should consider these factors and include them when training in the use of transportation services.
Some elders find the process of applying for special transportation services overcomplicated and confusing. COTAs should have applications available and know the eligibility requirements for these services. If possible, COTAs should schedule an outing with elders to use particular services and help them resolve any difficulties that arise. Elders may need encouragement to be assertive when they require assistance. If the outing is successful, elders are more likely to use the service independently or with a friend or family member.
Safe Driving
Aging is a highly complex process that varies tremendously among individuals. Chronologic age alone is not a good predictor of driving performance. The physical effects of aging in combination with a disability make driving safety an important issue. Although driving may seem simple because so many people do it, it is an extremely complex occupation that requires constant attention and concentration.100 Driving involves a number of abilities. The abilities of sensing, deciding, and acting are critical in operating a vehicle. Drivers must perform a series of coordinated activities with their hands and feet while using input from their eyes and ears. Drivers must make many decisions on the basis of what they see and hear in relation to other vehicles on the road, other drivers, traffic signs, signals, and road conditions. These decisions result in the actions of braking, steering, and accelerating, or a combination of all three to maintain or adjust the position of the vehicle in traffic. Because fluctuations in traffic occur quickly, the coordination between decisions and actions must be smooth. Drivers make about 20 decisions for each mile traveled, demonstrating that the occupation of driving is complex and fast paced.96,100 Age- or disability-related decreases in sensorimotor skills may compromise driving safety by reducing the speed with which an elder can sense, decide, and act in traffic.
The sense dimension of driving includes visual acuity, visual accommodation, field of vision, dark adaptation, color vision, visual searching, and hearing. Glare and illumination, as well as certain diseases of the eye, may also affect the way the driver senses environmental changes. Integrity of muscles and joints and reaction time are also intimately related to driving. Elders may not perceive, interpret, and react to sensory stimulation as acutely or quickly as younger people. Approximately 60% of all persons age 65 years and older have a visual impairment.101 As the size of our elder population increases, the number of people with visual impairments will increase significantly. Visual impairments are a primary consideration in safe driving and should be assessed accordingly.
Vision is usually defined as visual acuity or the ability to see fine details. Static acuity (such as looking at an eye chart) is tested in driver licensing examinations. Dynamic acuity (subject or target moving) is more closely related to traffic accidents but is seldom tested. Up to age 40 or 50 years, little change occurs in visual acuity, but visual acuity declines markedly in individuals older than age 50.102 By age 70 years, most elders have poor acuity without correction. The implications of this decline for driving are that drivers find distinguishing between objects increasingly difficult and need to be closer to objects to clearly perceive them.103 To compensate for this, elders may drive slowly to distinguish hazards on the road in time to avoid them. Some diseases of the eye, such as macular degeneration or diabetic retinopathy, can be improved with devices such as a bioptic telescope system. Bioptic systems combine prescription eyewear with a small telescopic system. The eyewear lens portion is deemed the carrier that provides general vision, whereas the telescope aids in quick spotting of detail for the visually impaired patient. The telescope can be fabricated for one or both eyes.104 COTAs should be aware that not all states approve bioptic driving and therefore should be aware of their state’s visual standards.
Accommodation is defined as the ability to focus the eyes on nearby objects. With aging, changes in the lenses of the eyes and in the muscles that adjust them decrease their capacity for accommodation. For this reason, many elders need bifocal or trifocal eyewear, which affects driving because more time is required to change focus from near to distant objects, such as when looking from the instrument panel to the road and vice versa. A younger person can change focus in about 2 seconds, whereas adults older than age 40 years take 3 seconds or more. This delay is potentially hazardous. The retina of the normal eye receives about one half as much light at age 50 as at age 20 years and about one third as much at age 60 as at age 20 years.105 This change is primarily because of a decrease in the size of the pupil. Elders who complain of night blindness have good reason not to drive at night because less light is available. Choosing well-lighted highways and instrument panels and keeping headlights, windows, and eyeglasses clean are helpful measures. A driver rehabilitation professional may recommend changes in the enhancement of the instrument panel to improve use such as marking various speeds on the odometer or modifying the speedometer with a magnifier.
Field of vision decreases with age, and this decrease can contribute to the possibility of collisions. For example, people who can see only directly ahead confront a greater risk for accidents at intersections because they cannot see vehicles approaching from the sides. Compensations for a decreased field of vision can include the use of special panoramic mirrors and the habit of turning the head more often to check for traffic. Many elders may also not be aware of their blind spot on the side of the vehicle. Reminders to look over the shoulder before all lane changes may be necessary.
Glare occurs when too much light or light from the wrong direction or source is present. If excessive light shines on a highway sign, the elder may not see it. Quick recovery from oncoming headlights is necessary for safe driving. In the elder driver, eye recovery is slower and sensitivity to glare increases. The windshields of a vehicle produce glare, and one way to reduce dashboard glare is to place a black cloth over the dash.
Dark adaptation is the process whereby eyes adjust for better vision in low light. Elders not only see less clearly in darkness but also require more time to accommodate to it.106 This can be a particular problem when driving in and out of tunnels. Many elders decide on their own not to drive at night for this reason.
Elders may not identify the color of traffic signs or signals as well as younger people, especially when the light is dim or glare is present. This can be a problem because elders require additional time to read road signs, which diverts their attention from the road and traffic.102
Uncontrolled glare may mask oncoming traffic and limit the ability to see traffic lights, signs, and brake lights. Not controlling glare can make the driver less safe on the road. Some conditions can require more stringent control of light and glare. The color and properties of the filter are important, and the low vision specialist and the driver rehabilitation specialist can help determine the degree of glare problems and appropriate treatments, including sun filters, hats, adaptive visors, and other adaptive steps. A driver rehabilitation specialist may advise some patients to avoid driving just after sunrise and just before sunset, where low-lying sun might cause significant glare problems.
According to the AARP,107 elders may be able to compensate for some visual limitations. They should have their vision checked at least yearly and avoid eyeglass frames that obstruct peripheral vision. Learning the general meaning of traffic signs by their shapes and colors and avoiding driving at night whenever possible are useful precautions. Various lens tints may be used to improve color recognition or the detection of objects, signs, and road users in low contrast areas.
Approximately 37% of people older than age 65 years experience some hearing loss.108 This loss can cause problems during driving because horns, sirens, and train whistles may be difficult to hear. It may also prevent elders from realizing that the turn signal indicator is on when no turns are being made. Elders should have their hearing tested by a qualified professional. When adjusting to any hearing assistive device, elders should keep the volume of the car radio as low as possible, leave the air conditioning or heating units on the lowest possible setting, and visually check turn signals. Alerting systems and mirrors may also be used to improve awareness. (Resources for drivers with hearing difficulties are listed in the Appendix.)
The aging process also affects muscles and joints in ways that may affect driving. Elders may experience back pain, making it difficult to sit for long periods. Special cushions may be helpful. Arthritis may cause stiffness in the neck, which makes it painful when turning to check for traffic. Fatigue and discomfort are also problems that may distract elders and lessen their awareness of traffic conditions. Power steering and power brakes can help tremendously. A wide variety of mirrors is available to compensate for stiffness in the neck. Using tilt steering and arm rests may also help. A driver rehabilitation specialist can help determine whether modifications to their vehicle will help the elder who is experiencing a decrease in strength or in range of motion. Reaction time is extremely important in safe driving. Reaction time is the time required by the eyes to see and the brain to process, decide what to do, and transmit the information to the proper body parts. For example, after seeing that the traffic ahead has stopped, a driver extends the right leg and pushes on the brake pedal. The ability to respond quickly may decrease with age, but specific safety measures can be used to compensate for the loss. One strategy is to maintain a safe distance from the car ahead. When stopping, the driver should be able to see the tires of the car in front. Other strategies are to avoid rush hour traffic and to take someone else along, especially when traveling to a new destination. If elders are upset or ill, they will probably have a slower reaction time. Education on compensatory techniques can help elders change unsafe habits. The AARP and the AAA offer various programs and courses for elder drivers (Figure 14-10). The driver safety course offered by the AARP covers many issues, including decreased reaction time, visual and hearing losses, the effects of certain medications, and hazardous situations.107 The fee for these courses is nominal, and many insurance companies will offer a rebate on automobile insurance after successful completion of a driver safety course. However, these classes do not include behind-the-wheel testing. COTAs should discuss any concerns about the elder’s ability to drive safely with the supervising OTR and physician whenever possible.
A behind-the-wheel evaluation is the best method for determining driver safety. A driving evaluation program that specializes in working with persons with disabilities can determine safety and equipment needs. The AOTA Older Driver Initiative and the ADED assist COTAs in locating driver evaluation programs. These programs can also instruct COTAs in the proper procedures for reporting unsafe or questionable drivers to the DMV of each state. COTAs should clearly document all recommendations to elders. For example, if the COTA recommends that an elder’s driving ability be evaluated after a stroke, this recommendation must be clearly stated in the medical chart. To demonstrate thorough care, COTAs are advised to document the names of at least three resources given to the client.
A wide variety of equipment is available to help elders continue driving. This equipment is available from a variety of sources, including equipment catalogs, vendors, and automobile manufacturers (Table 14-3). (Refer to the Appendix for addresses of organizations to contact for additional resources.)
TABLE 14-3 Adaptive Equipment Ideas
| Difficulty | Effect on driving | Resources to assist elder drivers |
|---|---|---|
| Decreased neck ROM or pain when turning head | Limited scope of view of traffic around car | Install panoramic mirrors (Brookstone) or convex mirrors (can be installed by vendors); refer to driving program for evaluation; instruct client in use of head support |
| Decreased shoulder ROM or pain in shoulders | Difficulty steering, reaching for seat belt, and adjusting rearview mirror | Use arm supports already in vehicle; automobile upholsterer can build up existing arm supports to support elbows, which usually decreases client’s shoulder pain; client may need effort of steering reduced, which can be determined by driving evaluation (driving program can refer to appropriate vendor for this modification); instruct elder in use of stick to adjust rearview mirror and tilt steering wheel |
| Decreased ROM or pain in fingers and hands | Difficulty turning key, opening door, adjusting radio, air conditioning, and so on; possible difficulty holding onto steering wheel safely | A wide variety of key holders and door openers is available from medical supply catalogs; knob extensions can be made by car vendors; refer client for driving evaluation to determine need for steering device or built-up steering wheel |
| Back pain | Decreased concentration caused by pain; difficulty turning to check traffic | A wide variety of cushions and lumbar supports is available from medical supply companies and vendors; these should be tried before purchase; driving programs can also evaluate and provide resources |
| Impairment or loss of both lower extremities | Inability to operate gas and brake pedals | Refer to driving program for evaluation of ability to use hand controls |
| Impairment or loss of right lower extremity | Difficulty using gas and brake pedals | Refer to driving program for evaluation of ability to use left foot accelerator |
| Impairment or loss of left upper extremity | Difficulty using turn signal and turning | Refer to driving program for evaluation of ability to use right crossover directional and spinner knob |
| Impairment or loss of right upper extremity | Difficulty steering, shifting gears in automatic or manual cars | Refer to driving program for evaluation of ability to use spinner knob |
| Hearing impairment | Inability to hear emergency sirens; failure to turn off turn signal | Elder drivers can purchase equipment to amplify sound of blinker; hearing aids can help clients better hear sirens |
| Cognitive impairment | Decreased judgment and decision making; slow reaction time; unsafe driving | Refer to driving program for detailed evaluation; discuss concerns with occupational therapist; document recommendations clearly |
| Visual impairment | Compromised ability to read signs; overly slow driving; generally unsafe driving skills | Refer to optometrist for vision checkup; if elder has low vision, refer to ophthalmologist or neuro-optometrist that specializes in low vision. Neuro-Optometric Rehabilitation Association (NORA) is a good resource for locating this area of specialty. |
ROM, range of motion.
Adapted from Lillie, S. (1993). Evaluation for driving. In T. T. Yoshikawa & E. Lipton (Eds.). Ambulatory Geriatric Care. St. Louis, MO: Mosby.
Case Study
Mr. Thomas is 62 years old. One year ago he had a right cerebrovascular accident and has a nonfunctional left upper extremity. For long distances, he uses a manual wheelchair, which he pushes with his right lower extremity. For short distances, he slowly ambulates using a quad cane. Other medical conditions include a seizure disorder controlled by medication and a left hip joint replacement that causes pain and discomfort with prolonged sitting. A former physical education teacher, Mr. Thomas enjoys working with students at the high school level and is anxious to return to work in some capacity. His wife works full-time, and he receives occasional assistance in transportation from friends. Mr. Thomas believes he is ready to drive, but his wife is very concerned for his safety.
Mr. Thomas received a driving evaluation, during which he exhibited difficulties such as weaving out of the lane and forgetting to turn off his turn signal. After driving for 20 minutes, he drifted across two lanes and lost his concentration. The driving instructor had to take over the steering wheel to pull the car over to the side of the road. Mr. Thomas stated that his “leg hurt.”
After the evaluation, the deficits observed during driving were discussed. Mr. Thomas demonstrated insight into his difficulties and expressed the desire to begin training to improve his driving skills. Equipment needs included a spinner knob to allow him to steer with one hand and a right crossover directional device that enabled him to use his right hand for directional use. Training strategies included asking Mr. Thomas to tell the driving instructor when he was starting to have pain in his leg and to pull over when it was safe. He was reminded to turn off his directional signal after use and to look ahead while driving. After three training sessions, Mr. Thomas was able to demonstrate safe driving skills. He received a driving test from the DMV and passed. He is now able to return to part-time work and independent living.
Case Study Questions
1. Considering the case of Mr. Thomas, identify some relevant recommendations for driving if he had experienced a spinal cord injury rather than a cerebrovascular accident.
2. Identify alternatives for transportation appropriate for Mr. Thomas if he had failed the driving evaluation.
3. Identify possible funding resources such as Vocational Rehabilitation Services for adaptive driving equipment and driver rehabilitation sessions.
1. Explain the reason that Omnibus Budget Reconciliation Act regulations involving the use of restraints were drafted, and discuss related requirements for health providers.
2. Explain the steps to be taken in establishing a restraint reduction program.
3. Explain the role of the COTA in consultations regarding the use of restraints.
4. Describe at least three environmental adaptations that may help reduce the use of restraints.
5. Identify psychosocial approaches to reducing the use of restraints with an elder who wanders.
6. Explain the ways that activity aids in the reduction of restraints.
7. Describe the ideal position in which an elder should sit in a wheelchair.
8. Describe at least three additional considerations when monitoring the appropriate fitting wheelchair for a bariatric client.
9. List five precautions to consider when monitoring the appropriate fit of a wheelchair for an elder.
10. Identify three reasons that many falls go unreported.
11. Explain the reason that some elders and their family members are reluctant to change the environment when personal safety and prevention of falls are a concern.
12. Explain the need for assessment of an elder’s nighttime toileting skills.
13. Describe ways the home can be modified to prevent falls if elders have vision impairments and poor standing balance.
14. Identify three emergency strategies for an elder who lives alone and has a history of falls.
15. List the issues that must be considered when recommending community transportation.
16. Describe strategies to alleviate the elder’s fear of using transportation.
17. Describe the actions of the COTA when the client’s ability to be a safe driver is in question.
1 Joanna Briggs Institute (JBI). Physical restraint—part 1: Use in acute and residential care facilities. Best Practice. 2002;6(3):1-6.
2 Mott S., Poole J., Kenrick M. Physical and chemical restraints in acute care: Their potential impact on the rehabilitation of older people. International Journal of Nursing Practice. 2005;11(3):95-101.
3 OBRA Omnibus Budget Reconciliation Act, Pub. L. No. 100-20, 101 Stat. 1330 (1987).
4 Centers for Medicare & Medicaid Services. CMS publishes final patients rights rule on use of restraints and seclusion: Better, more extensive training of staff required. Retrieved March 18, 2010, from http://www.cms.hhs.gov/apps/media/press/release.asp?Counter=2057, 2006.
5 U.S. Department of Health & Human Services, Centers for Medicare & Medicaid Services. Release of report: Freedom from unnecessary restraints: Two decades of national progress in nursing home care (Ref: S&C-09-11). Retrieved from http://www.cms.gov/SurveyCertificationGenInfo/downloads/SCLetter09-11.pdf, 2008.
6 U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality. National Healthcare Quality Report. (AHRQ Publication No. 10-0003). Retrieved from http://www.ahrq.gov/qual/nhqr09/nhqr09.pdf, 2009.
7 Health Care Financing Administration. Interpretive guidelines Rev. 250: Part II guidance to surveyors for long-term care facilities tag #s f221-241. Washington, DC: U.S. Department of Health and Human Services; 1995. pp. 44-53
8 Health Care Financing Administration. 42 Code of Federal Regulations, Part 483 Subpart B, Requirements for long-term care facilities. Washington, DC: U.S. Department of Health and Human Services; 2001.
9 Morris K. Issues and answers: Restraint use. Ohio Nurses Review. 2007;82(4):14-15.
10 Kleen K. Restraint regulation: The tie that binds: Break free of potential litigation by recognizing patient rights related to physical restraints. Nursing Management. 2004;35(11):36-38.
11 Strumpf N.E., Evans L.K., Wagner J., Patterson J. Reducing physical restraint: Developing an educational program. Journal of Gerontological Nursing. 1992;18(11):21.
12 Kari N., Michels P. The Lazarus project: The politics of empowerment. American Journal of Occupational Therapy. 1991;45(8):719.
13 Joanna Briggs Institute (JBI). Physical restraint—part 2: Minimization in acute and residential care facilities. Best Practice. 2002;6(4):1-6.
14 Brungardt G. Patient restraints: New guidelines for a less restrictive approach. Geriatrics. 1994;49(6):43.
15 Reed P., Tilly J. Dementia care practice recommendations for nursing homes and assisted living, phase 2: Falls, wandering, and physical restraints. Alzheimer’s Care Today. 2008;9(1):51-59.
16 Janelli L.M., Kanski G.W., Neary M.A. Physical restraints: Has OBRA made a difference? Journal of Gerontological Nursing. 1994;20(6):17.
17 Strumpf N., Evans L., Bourbonniere M. Restraints. In: Mezey M., editor. The Encyclopedia of Elder Care. New York: Springer; 2001:567-569.
18 Medicare and Medicaid Programs; Hospital Conditions of Participation: Patient Rights; Final Rule. 71 Fed. Reg. 71294 (2006) (to be codified at 42 C.F.R. pt. 483.13).
19 Mion L.C., Mercurio A. Methods to reduce restraints: Process, outcomes, and future directions. Journal of Gerontological Nursing. 1992;18(11):5.
20 J. Rader, personal communication, 1996.
21 Rader J. Individualized Dementia Care: Creative, Compassionate Approaches. In: Tornquist E., editor. Individualized Dementia Care: Creative, Compassionate Approaches. New York: Springer, 1995.
22 Werner P., Koroknay V., Braun J., Cohen-Mansfield J. Individualized care alternatives used in the process of removing restraints in the nursing home. Journal of the American Geriatrics Society. 1994;42(3):321.
23 Neufeld R.R., Libow L.S., Foley W.J., Dunbar J.M., Cohen C., Breuer B. Restraint reduction reduces serious injuries among nursing home residents. Journal of the American Geriatrics Society. 1999;47(10):1202-1207.
24 Ericson L.L. Restraints in the nursing home environment. Occupational Therapy Forum. 1991;6(4):1.
25 Tideiksaar R. Falls. In Bonder B., Wagner M., editors: Functional Performance in Older Adults, second ed, Philadelphia: FA Davis, 2001.
26 Patterson J.E., Strumpf N.E., Evans L.K. Nursing consultation to reduce restraints in a nursing home. Clinical Nurse Specialist. 1995;9(4):231.
27 Eigsti D.G., Vrooman N. Releasing restraints in the nursing home: It can be done. Journal of Gerontological Nursing. 1992;18(1):21.
28 Reference deleted in chapter.
29 Maine care center reduces use of bed rails. Health Progress. 2004;85(6):32.
30 Evans L.K., Forceia M.A., Yurkow J., et al. The geriatric day hospital. In: Katz P., Mezey M., Kane R., editors. Emerging Systems in Long-Term Care. New York: Springer, 1999.
31 Gallo J.J., Busby-Whitehead J., Rabins P.V., et al, editors. Reichel’s Care of the Elderly: Clinical Aspects of Aging, fifth ed, Philadelphia: Lippincott Williams & Wilkins, 1999.
32 Plautz R., Camp C. Activities as agents for intervention and rehabilitation in long-term care. In Bonder B., Wagner M., editors: Functional Performance in Older Adults, second ed, Philadelphia: FA Davis, 2001.
33 Greenberg D. Geriatric seating and positioning: Definitely a therapy task. Gerontology Special Interest Section Newsletter. 1996;19(3):1.
34 Jones D.A. Seating problems in long-term care. In: Tornquist E.M., editor. Individualized Dementia Care: Creative Compassionate Approaches. New York: Springer, 1995.
35 Russell J.N., Hendershot G.E., LeClere F., Howie L.J., Adler M. Trends and differential use of assistive technology devices: United States, 1994. Advance Data. 1997;292:1-10.
36 Sabol T.P., Haley E.S. Wheelchair evaluation for the older adult. Clinics in Geriatric Medicine. 2006;22,:355-375.
37 Brechtelsbauer D.A., Louie A. Wheelchair use among long-term care residents. Annals of Long Term Care. 1999;1999(7):213-220.
38 Kaye H.S., Kang T., LaPlante M.P. Mobility Device Use in the United States. Disability Statistics Report 14. Washington, DC: U.S. Department of Education, National Institute on Disability and Rehabilitation Research; 2000.
39 Krasilovsky G. Seating assessment and management in a nursing home population. Physical and Occupational Therapy in Geriatrics. 1993;11:25-38.
40 Rader J., Jones D., Miller L. The importance of individualized wheelchair seating for frail older adults. Journal of Gerontological Nursing. 2000;26:24-32.
41 Perr A. Elements of seating and wheeled mobility intervention. Occupational Therapy Practice. 1998;3(9):16-24.
42 Hoenig H., Landerman L.R., Shipp K.M., George L. Activity restriction among wheelchair users. American Journal of Geriatrics Society. 2003;2003(51):1244-1251.
43 Hoenig H., Landerman L.R., Shipp K.M., Pieper C., Pieper C., Richardson M., et al. Clinical Trial of a Rehabilitation Expert Clinician Versus Usual Care for Providing Manual Wheelchairs. Journal of American Geriatrics Society. 2005;53:1712-1720.
44 Hoenig H., Pieper C., Zolkewitz M., Schenkman M., Branch L.G. Wheelchair users are not necessarily wheelchair bound. Journal of Geriatrics Society. 2002;50:645-654.
45 Scherer M.J., Sax C., Vanbiervliet A., Cushman L.A., Scherer J.V. Predictors of assistive technology use: The importance of personal and psychological factors. Disability Rehabilitation. 2005;27:1321-1331.
46 Phillips B., Zhao H. Predictors of assistive technology abandonment. Assistive Technology. 1993;5:36-45.
47 Fontein J., Mundy P. Wheelchair positioning for all ages and sizes. PowerPoint presentation at Care Medical Care Fair. November 2008 www.pdgmobility.com, 2008.
48 Brackens L. All bariatric patients were not created equal: Mobility Management Newsletter (10/01/2008). www.mobilitymgmt.com, 2008.
49 Fontein J., Tanguay S. Measurement, positioning and mobility considerations for bariatric customers. PowerPoint presentation at Care Medical Care Fair. November 2009 www.pdgmobility.com, 2009. and www.mobilitymgmt.com
50 Kittel, A., Di Marco, A. & Stewart, H. (2002). Factors influencing the decision to abandon manual wheelchairs for three individuals with a spinal cord injury. Disability & Rehabilitation, 24 (1-3), 106-114.
51 Batavia, M., Batavia, A. & Friedman, R. (2001). Changing chairs: anticipating problems in prescribing wheelchairs. Disability & Rehabilitation, 23 (12), 539-548.
52 Feldt K.S., Warne M.A., Ryden M.B. Examining pain and agitation in aggressive cognitively impaired older adults. Journal of Gerontological Nursing. 1998;24(11):14-22.
53 Simmons S., Schnelle J., MacRae P., Ouslander J. Wheelchairs as mobility restraints: Predictors of wheelchair activity in non-ambulatory nursing home residents. Journal of American Geriatrics Society. 1995;43:384-388.
54 Lamb S.E., Jorstad-Stein E.C., Hauer K., Becker C. Prevention of Falls Network Europe and Outcomes Consensus Group. Development of a common outcome data set for fall injury prevention trials: The Prevention of Falls Network of Europe Consensus. Journal of the American Geriatrics Society. 2005;53:1618-1622.
55 Centers for Disease Control and Prevention. Self-reported falls and fall-related injuries among persons aged > or =65 years—United States, 2006. Morbidity and Mortality Weekly Report. 2008;57:225-229.
56 Gillespie, L.D., Robertson, M.C., Gillespie, W.J., Lamb, S.E., Gates, S., Cumming, R.G., et al., 2009. Interventions for preventing falls in older people living in the community. Cochrane Database of Systematic Reviews, 2. Art. No.: CD007146.
57 Rubenstein L.Z., Josephson K.R. The epidemiology of falls and syncope. Clinics in Geriatric Medicine. 2002;18:141-158.
58 Centers for Disease Control and Prevention. Fatalities and injuries from falls among older adults—United States, 1993-2003 and 2001-2005. Morbidity and Mortality Weekly Report. 2006;55:1222-1224.
59 Rubenstein L.Z., Solomon D.H., Roth C.P., Young R.T., Shekelle P.G., Chang J.T., et al. Detection and management of falls and instability in vulnerable elders by community physicians. Journal of the American Geriatrics Society. 2009;57(9):1527-1531.
60 Min L., Yoon W., Mariano J., Wenger N. The vulnerable elders—13 survey predicts 5-year functional decline and mortality outcomes in older ambulatory care patients. Journal of the American Geriatrics Society. 2009;57(11):2070-2076.
61 Jung D., Lee J., Lee S. A meta-analysis of fear of falling treatment programs for the elderly. Western Journal of Nursing Research. 2009;31(1):6-16.
62 Laird R.D., Studenski S., Perera S., Wallace D. Fall history is an independent predictor of adverse health outcomes and utilization in the elderly. American Journal of Managed Care. 2001;7(12):1133-1138.
63 Stevens J.A., Corso P.S., Finkelstein E.A., Miller T.R. The costs of fatal and nonfatal falls among older adults. Injury Prevention. 2006;12:290-295.
64 Frick K.D., Kung J.Y., Parrish J.M., Narrett M.J. Evaluation the cost-effectiveness of fall prevention programs that reduce fall-related hip fractures in older adults. Journal of the American Geriatrics Society. 2010;58:136-141.
65 Rubenstein L.Z., Josephson K.R. Falls and their prevention in elderly people: What does the evidence show? Medical Clinics of North America. 2006;90:807-824.
66 Carpenter C., Scheatzle M., D’Antonio J., Ricci P., Coben J. Identification of fall risk factors in older adult emergency department patients. Academic Emergency Medicine. 2009;16(3):211-219.
67 Chang J., Ganz D. Quality indicators for falls and mobility problems in vulnerable elders. Journal of the American Geriatrics Society. 2007;55(S2):S327-S334.
68 Administration on Aging. A profile of older Americans: 2002. Washington, DC: U.S. Department of Health and Human Services; 2003.
69 Desai M., Pratt L.A., Lentzner H., Robinson K.N. Trends in vision and hearing among older Americans. Aging Trends. 2001;2:1-8.
70 Good G., LaGrow S., Alpass F. An age-cohort study of older adults with and without visual impairments: Activity, independence, and life satisfaction. Journal of Visual Impairment & Blindness. 2008;102(9):517-527.
71 Light K., Thigpen M. Geriatric Rehabilitation: Evidence and Clinical Application. New York: McGraw-Hill; 2010.
72 Naqvi F., Lee S., Fields L. Appraising a guideline for preventing acute care falls. Geriatrics. 2009;64(3):10-33.
73 Nolte J. The Human Brain: An Introduction to its Functional Anatomy, 6th ed. Philadelphia: Mosby Elsevier; 2009.
74 Costarella M., Monteleone L., Steindler R., Zuccaro S. Decline of physical and cognitive conditions in the elderly measured through the functional reach test and the Mini-Mental State Examination. Archives of Gerontology and Geriatrics. 2010;50(3):332-337.
75 Carter N.D., Kannus P., Khan K.M. Exercise in the prevention of falls in older people: A systematic literature review examining the rationale and the evidence. Sports Medicine. 2001;31:427-438.
76 Tideiksaar R. Fall prevention in the home. Topics in Geriatric Rehabilitation. 1987;3:1.
77 Leipzig R.M., Cumming R.G., Tinetti M.E. Drugs and falls in older people: A systematic review and meta-analysis: I. Psychotropic drugs. Journal of American Geriatrics Society. 1999;47:30-39.
78 Woolcott J., Richardson K., Wiens M., Marin J., Khan K., Marra C. Meta-analysis of the impact of 9 medication classes on falls in elderly persons. Archives of Internal Medicine. 2009;169(21):1952-1960.
79 Fuller-Thomson E., Yu B., Nuru-Jeter A., Guralnik J., Minkler M. Basic ADL disability and functional limitation rates among older Americans from 2000-2005: The end of the decline? Journals of Gerontology; Series A. Biological Sciences and Medical Sciences. 2009;64(12):1333-1336.
80 American Occupational Therapy Association. Occupational Therapy Practice Framework: Domain and Process. second ed. American Journal of Occupational Therapy. 2008;62:625-683.
81 Shumway-Cook A., Ciol M.A., Hoffman J., Yorkston K., Chan L. Falls in the Medicare population: Incidence, associated factors, and impact on health care. Physical Therapy. 2009;89:324-332.
82 Tideiksaar R. Geriatric falls: Assessing the cause, preventing recurrence. Geriatrics. 1989;44(7):57.
83 Cameron, I.D., Murray, G.R., Gillespie, L.D., Robertson, M.C., Hill, K.D., Cumming, R.G., et al., 2010. Interventions for preventing falls in older people in nursing care facilities and hospitals. Cochrane Database of Systematic Reviews, 1, Art. No.: CD005465.
84 Sherrington C., Whitney J.C., Lord S.R., Herbert R.D., Cumming R.G., Close J.C. Effective exercise for the prevention of falls: A systematic review and meta-analysis. Journal of the American Geriatrics Society. 2008;56:2234-2243.
85 Kim H., Han J., Cho Y. The effectiveness of community-based tai chi training on balance control during stair descent by older adults. Journal of Physical Therapy Science. 2009;21:317-323.
86 Mihay L.M., Boggs K.M., Breck A.J., Dokken E.L., NaThalang G.C. The effect of tai chi inspired exercise compared to strength training: A pilot study of elderly retired community dwellers. Physical and Occupational Therapy in Geriatrics. 2006;24(3):13-26.
87 Bouwen A., De Lepeleire J., Buntinx F. Rate of accidental falls in institutionalized older people with and without cognitive impairment halved as a result of a staff-orientated intervention. Age and Ageing. 2008;37:306-310.
88 Detweiler M.B., Kim K.Y., Taylor B.Y. Focused supervision of high-risk fall dementia patients: A simple method to reduce fall incidence and severity. American Journal of Alzheimer’s Disease and Other Dementias. 2005;20:97-104.
89 Shimada H., Tiedeman A., Lord S., Suzuki T. The effect of enhanced supervision on fall rates in residential aged care. American Journal of Physical Medicine and Rehabilitation. 2009;88:823-828.
90 Bartley M., O’Neill D. Transportation and driving in longitudinal studies on ageing. Age & Ageing. 2010;39:631-636.
91 Savoye, C., 2001. States to try to help elderly stay behind the wheel. Christian Science Monitor, 93, 3.
92 National Highway Traffic Safety Administration, n.d. Traffic safety facts 2008 data: Older population (DOT HS 811 161). Author, Washington, DC. Retrieved October 25, 2010, from http://www-nrd.nhtsa.dot.gov/Pubs/811161.PDF
93 American Occupational Therapy Association. Statement: Driving and community mobility. American Journal of Occupational Therapy. 2005;59:666-670.
94 National Institutes on Aging. http://www.nia.nih.gov/HealthInformation/Publications/drivers.htm, 2010. Age page. Retrieved October 25, 2010, from
95 Borowsky A., Shinar D., Oron-Gilad T. Age, skill, and hazard perception in driving. Accident Analysis & Prevention. 2010;42:1240-1249.
96 Hunt L.A., Arbesman M. Evidence-based and occupational perspective of effective interventions for older clients that remediate or support improved driving performance. American Journal of Occupational Therapy. 2008;62:136-148.
97 American Occupational Therapy Association. Occupational therapy practice framework: Domain and process. second ed. American Journal of Occupational Therapy. 2008;62:625-683.
98 Hendrickson C. Changes over time in community mobility of elders with disabilities. Physical and Occupational Therapy in Geriatrics. 2005;23(2-3):75-89.
99 Chia D. Policies and practices for effectively and efficiently meeting ADA paratransit demand: A synthesis of transit practice. Washington, DC: Transit Cooperative Research Board/Transportation Research Board; 2008.
100 Hoggarth P.A., Innes C.R., Dalrymple-Alford J.C., Severinsen J., Jones R. Comparison of a linear and a non-linear model for using sensory-motor, cognitive, personality, and demographic data to predict driving ability in healthy older adults. Accident, Analysis and Prevention. 2010;42:1759-1768.
101 Vitale S., Cotch M., Sperduto R. Prevalence of visual impairment in the United States. Journal of the American Medical Association. 2006;295(18):2158-2163.
102 Ilett G. Functional vision assessment. Optician. 2010;240(6260):24. 25
103 Swamy B. Vision screening for frail older people: A randomized trial. British Journal of Ophthalmology. 2009;93:736-741.
104 BiopticDrivingUSA.com. An introduction: Driving with bioptic glasses. Retrieved November 9, 2010, from http://www.biopticdrivingusa.com/, 2010.
105 Cui Q., O’Neill W., Paige G. Advancing age alters the influence of eye position on sound localization. Experimental Brain Research. 2010;206:371-379.
106 Morrison J., McGrath C. Assessment of the optical contributions to the age-related deterioration in vision. Quarterly Journal of Experimental Physiology. 2008;93:249-269.
107 American Association of Retired Persons. Vision changes and driving: Knowing what to expect and when to get eye exams help mature drivers continue to drive safely. Retrieved October 25, 2010, from http://www.aarp.org/home-garden/transportation/info-05-2010/dsp_article_vision_changes_driving.html, 2010.
108 Huang Q., Tang J. Age-related hearing loss or presbycusis. European Archives of Oto-Rhino-Laryngology. 2010;267:1179-1791.