23 Colour dilution alopecia
INTRODUCTION
Colour dilution alopecia is a developmental disorder resulting in the weakening of hair shafts and progressive alopecia due to abnormal melanin pigment distribution within hair shafts, and within epidermal and follicular keratinocytes. It is a common condition in dogs with blue or fawn dilute colour hair coats. This case report describes a case of colour dilution alopecia in a collie with a blue hair coat.
CASE HISTORY
The onset of symptoms in colour dilution alopecia is usually between 6 months and 3 years of age and may present initially as gradual onset dorsal alopecia or as dorsal folliculitis. Only hairs in the dilute coat colour area are involved. When dogs present with folliculitis, there is a gradual progression of alopecia following each episode of folliculitis. Unless there is pyoderma, this is a non-pruritic disease and there is no systemic involvement. The history in this case was as follows:
CLINICAL EXAMINATION
General physical examination was unremarkable.
Examination of the skin revealed generalized, partial to complete alopecia over the pinnae and trunk (Figs 23.1 and 23.2). White areas were unaffected.
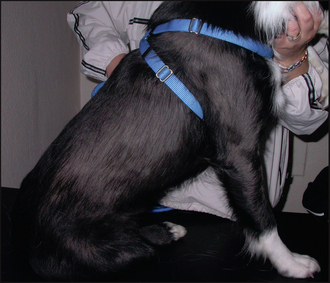

There was loss of primary hair shafts over the pigmented areas, revealing a blue to brown, dilute coloured undercoat.
In this case, the history and clinical signs were strongly suggestive of colour dilution alopecia, although other causes of non-pruritic alopecia were potential rule-outs. The involvement of a staphylococcal folliculitis could be ruled out on the basis of no response to the previous antibacterial therapy. In tardive onset cases, causes of hair follicle arrest, such as hypothyroidism and hyperadrenocorticism, should also be considered as differentials.
CASE WORK-UP
Skin scraping examination and fungal cultures are indicated where a folliculitis is on the list of differential diagnoses. Trichographic examination of plucked hair shafts should show evidence of macromelanosome formation, resulting in distorted, or fractured, hair shafts, and the hair shafts should appear dysplastic (‘deformed’). Histopathological examination helps support the clinical and trichographic diagnosis of colour dilution alopecia. Trial antibacterial therapy would also have been indicated if a staphylococcal infection had still been suspected.
The following diagnostic tests were performed:
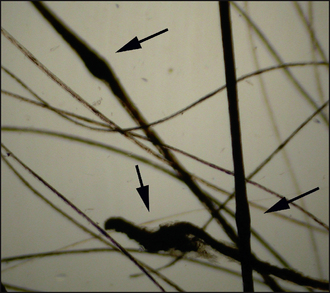
Figure 23.3 Photomicrograph of hair shafts from the dog in Fig. 23.1 showing melanin clumping and dysplasia (arrows).
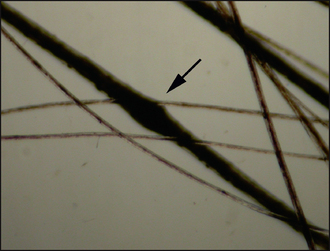
Figure 23.4 Photomicrograph of hair shafts from the dog in Fig. 23.1 showing melanin clumping and dysplasia (arrow).
DIAGNOSIS
The history, clinical signs, trichography and histopathology were consistent with a diagnosis of colour dilution alopecia.
PROGNOSIS
The prognosis for colour dilution alopecia is guarded. Although a purely cosmetic condition, the hair loss is gradually progressive, with complete alopecia developing after a few years. Episodes of secondary bacterial folliculitis are common. Because of the lack of sun protection there may be increased risk of ultraviolet light-induced skin disease and there may be an increased risk of cutaneous neoplasia.
AETIOLOGICAL AND PATHOPHYSIOLOGICAL ASPECTS OF COLOUR DILUTION ALOPECIA
Colour dilution alopecia is a form of hair follicle dysplasia. Dysplastic hair follicle diseases are characterized by abnormal growth and development of the hair follicle or associated glands. Hair follicle dysplasia may result in distortion, abnormal deposits, attenuation, absence, proliferation or degeneration. Colour dilution alopecia is a relatively common condition seen in dogs with a blue or fawn ‘dilute’ hair coat colour. In general, the lighter the hair coat colour, the more severe the disease.
Colour dilution alopecia is a genodermatosis and an autosomal mode of inheritance has been suggested. A colour dilution gene has been linked to the d-locus. It is not known whether this gene is directly responsible for initiating the disease or whether this is a polygenic condition with other genes involved. In colour dilute breeds, there are abnormalities of melanosome storage and transfer from the melanocyte to surrounding keratinocytes. A recent study of black-haired follicular dysplasia (a condition similar to colour dilution alopecia but affecting dogs with black, rather than dilute, hair coat colour) concluded that the condition was analogous to Griscelli syndrome in man. This condition is caused by a defect of melanocytic intracellular transport proteins, resulting in a similar phenotypic appearance.
It should be remembered that all dilute colour hairs contain larger than normal accumulations of melanin, regardless of whether there is evidence of colour dilution alopecia. In dogs with colour dilution alopecia, there is evidence of hair shaft distortion due to the presence of large clumps of pigment (Figs 23.3 and 23.4) that probably weakens the hair shaft, leading to fracture. This is likely to be the main cause of alopecia early in the course of the disease. Folliculitis is also common in these dogs and will lead to further alopecia; however, these factors alone would not usually explain the extent of hair loss. Signals from melanocytes are important in the initiation of anagen, the growth phase of the hair follicle, and it is possible that the abnormal transfer of melanosomes in colour dilution alopecia could result in a lack of stimulation of the hair bulb keratinocytes, leading to resting, non-cycling follicles.
EPIDEMIOLOGY
Colour dilution alopecia is most frequently seen in the blue Dobermann pinscher, but many other dilute coat colour breeds including the Great Dane, whippet, Italian greyhound, Yorkshire terrier, chihuahua, miniature pinscher, chow-chow, silky terriers and mongrels with dilute coat colours are affected. Dogs with light blue coats usually first develop symptoms at around 6 months of age, whereas those with less marked coat colour dilution may have a more tardive onset between 2 and 3 years of age.
TREATMENT OPTIONS
As colour dilution alopecia is a progressive incurable genodermatosis, there is no effective treatment; however, there are some palliative measures that can be taken. Early in the course of the condition the hair coat becomes dry and brittle, and scaling may become evident. The hair loss is due to hair shaft fracture and so excessive brushing and vigorous shampooing should be avoided, but moisturizers may improve the appearance of the hair coat and perhaps make it less brittle and liable to fracture. Episodes of folliculitis should be treated with systemic and gentle topical antibacterial therapy. Some cases develop quite severe scaling and oral vitamin A or synthetic retinoids (see Chapter 13) have been advocated to control the scale, and perhaps help to reduce the frequency and severity of bacterial folliculitis. Anecdotally, melatonin (see Chapter 24), given as a non-specific hair cycling inducer may be effective in promoting hair growth in colour dilution alopecia.
In this case, the following treatments were administered:
Examination of hair shafts is a useful diagnostic technique in colour dilution alopecia. However, large accumulations of pigment will be evident in the hair shafts of all dogs with a dilute coat colour, regardless of whether they have colour dilution alopecia. There should be evidence of dysplastic and distorted hair shafts, as in this case, to make the diagnosis of colour dilution alopecia.
The best sites from which to take samples for histopathological examination are those with complete alopecia. As usual, three to five areas should be sampled.
FOLLOW-UP
Re-examination after 3 months of treatment revealed no progression of the alopecia, with minimal scaling (Fig. 23.5), and so treatment was continued. After a further 2 months, there had been further progression of the alopecia (Fig. 23.6) and the owner elected to stop melatonin therapy on the grounds of lack of efficacy. The topical therapy and essential fatty acid supplement were continued. In a follow-up telephone call a year later, the owner reported that there had been no further progression and there had in fact been an apparent waxing and waning of the degree of alopecia. There had been no evidence of pruritus or folliculitis.
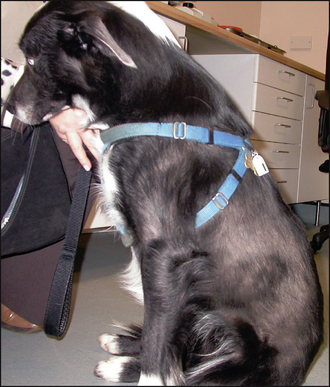
Figure 23.5 Same dog as in Fig. 23.1 after 3 months of treatment. There is some hair regrowth over the trunk.
