3 Principles of contemporary mental health practice
• To demonstrate an understanding of how the principles of recovery apply to a mental health context
• To analyse the role of values in influencing the decisions made in mental health practice
• To critically reflect upon your own values base in relation to the attitudes and beliefs which underpin your understanding of the role of a mental health nurse
• To critically discuss how a range of understandings of mental health problems can inform creative approaches to mental health practice
• To describe the relevance of health policy for nursing practice
• To identify key policy drivers for the delivery of mental health care
• To explain the role of the NICE guidelines
• To introduce the relevant mental health law and how this impacts on the role and responsibilities of the nurse
Introduction
This chapter will introduce the key areas of learning which you can engage in while on mental health placements. A range of contemporary theories and debates will be presented which are currently underpinning the direction of mental health service provision internationally. The picture is not straightforward and many students find the complexity of mental health care difficult to unpick. This section will aim to help you make sense of the practice you observe, and become involved in, by providing you with explanations of the theory, language and concepts and philosophies of mental health care. The activities and reflective exercises will help you to apply these concepts to your own practice in order to prepare you and make the most of your mental health placement experience.
The first of these is the concept of recovery in the context of mental health. You might think of recovery as returning to a state of health which is normal for you, or as a cure to your health problems. This way of understanding recovery has been challenged by many service users who see it quite differently. For them, recovery is more about coming to terms with their experiences and finding a way of moving beyond them to achieve a quality of life which is more acceptable to them. This might mean for some people that their mental health problems will continue, but that they will find a way of getting nearer to achieving their goals, despite them. Other people may view their mental health problems as a spiritual experience or as offering them an insight into a deeper awareness of themselves which they value and build upon. In contrast, some people may have been severely disabled or traumatised by their experience of mental health problems. It is therefore important to begin with how the person views their experience and the sense they are making of it. The history, development and impact of what has now become known as the “recovery movement” will be discussed and you will be encouraged to think about how this might influence the approach you adopt in your own clinical practice.
For many students, this conceptualisation of recovery is quite challenging as it contradicts their understanding of the nurses' role. Students often say that they are initially attracted to nursing because they wish to care for people and help to relieve their health problems. Therefore, the idea that people may not “get better” and that they might address their problems with little or no intervention from professional services is a challenge. What is required is a shift in the way nurses see their role so it is less about caring for people to address their problems and more about working with people towards increased independence.
The values you bring to your practice will influence the way you work with people. This is known as values-based practice (VBP) and is the second concept we will introduce in this chapter. VBP provides us with a framework to consider how the varied values we hold can influence the way we reach decisions in mental health practice. It recognises that if we are to truly promote recovery as a therapeutic intention then an awareness of our personal values is essential. This will enable us to be open to discussing and acting upon the values of the people we are working with to deliver mental health services and those who are receiving them.
The final section of this chapter will introduce the different explanations for causes of mental distress. It will contain discussion of the psychological, social and biological approaches to working with service users. You may already have an idea about what you think might contribute to a person's mental wellbeing and there is valid evidence to support each of the explanations we discuss. What we suggest is that by having an awareness of these approaches you can work with the person to help them come to their own understanding of the element of their recovery.
Recovery-orientated mental health care
History
Recovery has predominantly emerged from the stories of service users and has been discussed by professionals or academics.
Definition
… a deeply personal, unique process of changing one's attitudes, values, feelings, goals, skills, and/or roles. It is a way of living a satisfying, hopeful and contributing life even with the limitations caused by illness. Recovery involves the development of new meaning and purpose in one's life as one grows beyond the catastrophic effects of mental illness.
Underpinning principles of recovery
• Recovery is possible for everyone and will mean something different to every individual.
• The continuation or recurrence of symptoms of a mental health problem does not preclude the person from recovering a meaningful and valued life. Therefore, support should focus on the person's whole life and working towards wider goals.
• Recovery is something a person achieves for him or her self and, while it can be supported by professionals, it should not be dependent on professional intervention and can occur without it.
• It is often the effects of prejudice and discrimination that restrict people's opportunities and not the people themselves. This can stem from the consequence of receiving a psychiatric diagnosis which usually has negative associations.
• The starting point of recovery is the individual's experience and facilitating an understanding of what they have been through.
• Recovery does not have an end point but is a continuous journey of growth and adaptation. This may not be a linear journey and it may well involve setbacks.
• Carers, relatives, friends and colleagues are often a part of a person's recovery and they may face the challenges of recovery themselves.
Barriers to recovery
• Prejudice and discrimination, which prevent people who have experienced mental health problems from participating in everyday life. This obstructs people from engaging in roles, activities and relationships which give life its meaning and is often referred to as social exclusion.
• The lack of belief or reluctance that people may have in their own ability to take control and responsibility.
• The attitudes of people who deliver mental health services who may portray a hopeless picture of the person's future. This is often based on a belief that mental health problems will disable the person for the rest of their life and that they will be incapable of achieving their goals.
• The attitude within organisations that maintenance of mental health is good enough and therefore service users should be discouraged from taking risks which may not have a predictable outcome. This is sometimes called defensive practice and can be as a result of professionals' fear of litigation.
• The nature of the mental health problem itself which has a negative influence on people's mood, motivation to change or perception of themselves.

1. Make a list of the 10 things that you most value in your life.
2. Do they fit into categories or themes?
3. Would this be different from or similar to people who experience mental health problems? If so, how? Evidence suggests that when service users are asked this question, the following are commonly prioritised:
4. How does your list relate to this list?
5. What have been the barriers for you in achieving these things?
6. What do you think might be the barriers for people who experience mental health problems in achieving these things?
Recovery models
Despite the supposition that recovery from mental health problems does not always necessarily require professional intervention, it has been identified that some elements of professional practice can obstruct the person's attempts to move forward in their journey. Therefore a number of models, frameworks and approaches have been developed in order to encourage recovery-orientated practice in mental health care. The principles stated above consistently underpin these models, however the language used and ways in which they are applied are slightly different. You may or may not see one of these models being implemented in your placement area or hear your mentor talk about the approaches supported by the authors cited here. The evidence to support the impact of implementing some of the models on changing ways of working has emerged (e.g. Stevenson et al 2002, Cook et al 2005, Gordon et al 2005, Berger 2006, Lafferty & Davidson 2006). However, it has been recognised that due to the uniqueness of the recovery experience, traditional outcome measures, such as readmission rates and levels of medication use, are too narrow to appreciate the complexity of the process of recovery.
The following will describe three examples of recovery models or approaches which are currently being implemented in mental health practice. There are other examples, however these are the most commonly adopted in the UK.
Social inclusion and recovery: components of a model for mental health practice – Julie Repper and Rachel Perkins
This model emphasises the potential impact mental health services can have on a person's opportunities for recovery. It draws upon personal accounts of people's experiences of using mental health services and identifies that the stigma that results from contact with mental health services, the side effects of some psychotropic medication and disempowering practices which are present within organisational culture can act as barriers to recovery. Repper and Perkins (2003) maintain that significant change is required in the attitudes of professionals and the ways they perceive their role if recovery-orientated mental health services are to become sustainable. This model identifies three interrelated components which are proposed to promote the principles of recovery among mental health professionals. These include: developing hope-inspiring relationships; facilitating adaptation which enables personal understanding and opportunities to take back control; and promoting inclusion by helping people to access the roles, relationships and activities that are important to them.
Tidal Model – Phillip Barker and Poppy Buchanan-Barker
The Tidal Model has been developed by mental health nurses in collaboration with service users. It is a philosophical approach to the discovery of mental health. This means it is a way of thinking about how people might reclaim their personal story, as a first step towards recovering their lives. It is maintained that the Tidal Model is an approach to recovery as opposed to a rigid system or a set of prescribed procedures. You can learn more about the Tidal Model at http://www.tidal-model.com.
The model adopts a number of metaphors which aim to challenge the authority attached to professional language and promote common understanding. It compares life to a voyage which will inevitably involve some storms and may leave the person feeling that they are drowning. People who negatively influence the person's selfhood are described as pirates and may include an abuser or the instigator of trauma. In these circumstances a person may need guiding to a safe haven where they can repair their ship and regain their sea legs in order to re-embark on their life course.
The key difference between the Tidal Model and other recovery models is the principle that in order for the person to retain their selfhood during periods of crisis, recovery needs to start as soon as possible and should not wait until the crisis has passed. The model refers to this period as ‘the lowest ebb’. This may well require support from others including mental health services due to the challenge of exercising the level of self-exploration which is required to understand experiences during periods of significant distress.
The core values which underpin the Tidal Model are defined in the ‘Ten Commandments’. In essence, these include a focus on the person's story. This is captured from the person's perspective and told in their own language. It is not rephrased into a ‘patient history’ and translated into professional speech. It requires the professional to express a genuine interest in the person's view of their experiences and be willing to learn from their expertise as opposed to completing the exercise because it is a routine requirement. The person may not recognise their expertise in their experience and therefore find it difficult to tell their story. It is essential, therefore, that nurses communicate their belief in the person and value their point of view. This requires one-to-one time and it is maintained that this should be prioritised within organisations as opposed to being viewed as a luxury.
The ‘Ten Commandments’ recognise that the person's story will contain insights into what has helped them in the past. This could inform the types of evidence-based intervention that you draw upon to inform the way you help the person. This requires nurses to hold their personal view of what is the best way to help the person back and redefine their approach based on the person's definition of effective approaches to care. The first step in moving forward is seen as a crucial element of the recovery journey as it allows the person to see what can be done now and gives optimism for the future. It is acknowledged that although the person's circumstances may change, personal growth is challenging and will require the person to be aware of the changes that are occurring and influence the direction of their care. Many people may find this challenging, particularly if they have been excluded from decisions which influenced their life in the past. It is, therefore, the professionals' role to support the person to input into decisions and advocate for their view during the decision-making process. This will be aided by adopting a transparent approach to practice which includes documenting interactions together and continuing to adopt language which allows for mutual understanding.
Values-based mental health nursing practice – K Woodbridge and B Fulford
The influence of personal values on the way we practise as nurses has recently gained recognition in mental health care (see Department of Health (DH) 2004, Woodbridge & Fulford 2005, Cooper 2009). This school of thought identifies that the decisions we make and the way we work are not only influenced by research evidence but also by our values. This recognition prompts us to be aware of what influences our response to a particular person, their behaviour and how this might impact the direction of their care.
Definition
Values-based practice (VBP) is the theory and skills base for effective healthcare decision making where different (and hence potentially conflicting) values are in play (Fulford 2004).
The term ‘values’ is difficult to define. To help you start to understand this concept, use the thought bubble in Figure 3.1 to identify any words, phrases or terms you link with the term ‘values’. We have started you off with some suggestions.Now try and put this into a definition.
Values are ……………………………………………………………………………………………………………… …………………………………………………………………………………………………………………. …………………………………………………………………………………………………………………. …………………………………………………………………………………………………………………. …………………………………………………………………Cooper (2009, p. 22) offers a definition of values: The worth, desirability, importance, or emotional investment (either for or against) we attach to something.
Complexity of values
You may have found that your definition of values is different to Cooper's. This does not mean that it is wrong but it does tell us that values are complex. Woodbridge and Fulford (2003) suggest this is for the following reasons:
Values come in many different varieties
You may have found that your definition is more about ethics, human rights or virtues. Values often encompass all of these things and also go beyond them to take into consideration your own wishes, desires and dreams.
Values vary with time and place and are also eternal
Some values relate to the core beliefs that we tend to think of as with us from childhood and guiding us throughout life. These could be religious beliefs, family values or understanding of what society accepts as right or wrong. However, they can be expressed in different ways or be fluid and changeable depending on life experiences which challenge our values and cause us to question them.
Values vary from person to person
We may have some consensus in what the term ‘values’ means to us but the individual values we hold may be very different. Also, the importance we place on certain values may be unlike a colleague, service user or friend. For example, you might feel that the value of honesty is highly important to you. However, a colleague may believe that honesty is less important than protecting the person from harm. In this situation you may want to give a person all the information but your colleague may want to withhold it if it could potentially lead to the person becoming distressed.
Values applied to mental health practice
It is important to explore the values that you bring to your work as a student nurse in order to recognise how they are influencing your practice and identify why you may feel in conflict at times with people you are working with. This can include service users, their carers and also your mentor or other professionals. A good way to start this process is by completing the activity in the reflection point box below. This activity will aim to help you clearly define the values you bring to your work. It can become part of your portfolio and you may wish to reflect on it throughout your programme to identify when your values are challenged or reinforced in your practice and how you respond to this.
The values which have been advocated in relation to mental health care were formally brought together in a document called The Ten Essential Shared Capabilities (DH 2004). This document was developed in collaboration with service users, carers and mental health practitioners in both the voluntary and statutory sector. It represents a set of overarching principles for the whole of mental health care which aim to promote a recovery-orientated service. These principles were further reinforced in the Chief Nursing Officer's review of mental health nursing which was named From Values to Action (DH 2006). This policy sets the direction for the future of mental health nursing practice and emphasises the importance of adopting person-centred values in order to facilitate and promote recovery. A description of these documents and their application is given on Chapter 4.
Principles of values-based practice
Woodbridge and Fulford (2003) have developed the framework of VBP which is defined as:
… the theory and skills base for effective health care decision making where different (and hence potentially conflicting) values are in play.

Developing your nursing philosophy statement (NPS)
A nursing philosophy is a personal statement that describes your own views, beliefs and theories about how nurses should practise and care for service users. There is not necessarily a ‘right’ or ‘wrong’ way to write your NPS. However, there are certain issues that you should probably consider when making the connections between what you believe about nursing, how you nurse and how you evaluate your practice.
This framework recognises that in order for mental health practitioners to work with values, they should do the following:
• Raise awareness of values. Often, we are not aware of our values until they come into conflict or we feel our values are being ignored. As a professional, our values are usually advocated as a result of the power that is given to us in our role. However, service users often feel their values are dismissed or viewed as less valid as a consequence of their mental health problem. Therefore, it is important to consciously explore values in order to consider how they influence practice. This involves exploring personal values and creating forums for the discussion of values within teams.
• Adopt strategies for reasoning about values which enable the exploration of values which are influencing a situation and justify the outcome of a decision.
• Gain knowledge about the values which are likely to be influencing a situation. For example, gathering the past experiences of people involved, considering how the media may have portrayed a similar situation or exploring research which has been published on the issues arising.
• Adopt communication skills which enable people to give their views and feel listened to. This may involve some negotiation skills or resolution skills where there is conflicting values. This is important in order to ensure that each person's values are given equal attention.
• Start the decision-making process from the perspective of the service user to ensure that practice and policy are applied to the individual.
• Attend to the values of all others involved including the service user's family, friends, informal carers, support workers and all mental health practitioners. This is known as multidisciplinary practice. This will enable potential sources of misunderstanding or conflict to be converted into opportunities for discussion and creative working.
• Consider the influence of both the values and the facts when making decisions. This challenges the assumption that decisions made based on science, such as diagnosis, are not influenced by values of the person conducting the assessment. Values are, in fact, relevant to these decisions and can account for some of the inconsistencies in how different diagnoses are applied to the same symptoms or behaviours.
Barriers to implementing VBP and helpful strategies to facilitate VBP are listed in Table 3.1.
Table 3.1 Barriers and strategies for facilitating VBP
| Barriers to implementing VBP | Helpful strategies to facilitate VBP |
|---|---|
| Forums for the discussion of values are not routinely in place in practice | Clinical supervision, care reviews or multidisciplinary team meetings can be reformatted to enable this discussion |
| Decisions are sometimes made in an emergency situation which limits the time given to collaboration or effort to involve all parties. Also, when the service user is in crisis, they may be seen as unable to contribute to decisions made about their care | Crisis planning can allow for people to express their values in anticipation of an emergency situation. Therefore, you can be assured that action taken is in line with a pre-agreed plan. This is where a wellness recovery action plan (WRAP) or alternative relapse prevention plan can become very useful! |
| Some people you are working with may not see the value of considering other people's views or be unwilling to listen to alternatives which limits opportunities for negotiation | This will require you to step into their shoes and question why they may find this way of working challenging. The individual may have personal support or professional development needs |
| The wider organisation of mental health services places the responsibility and accountability of a decision with the professional. This may mean that some professionals are reluctant to consider others' views due to their accountability | A multidisciplinary approach to the decision-making process helps to share this responsibility as it enables concerns to be discussed, explored and strategies to be put in place which the whole team agrees upon. It also allows for the service user to take some responsibility for their actions and feel an increased sense of control |
Models of mental health
There are a number of models of mental health which attempt to explain or understand how mental health problems are caused and the ways they are viewed by society. This section will give a brief introduction to the key models which currently influence our understanding and practice in mental health care. What is unusual about mental health problems is that there is no one explanation. Each individual we meet has their own unique experiences, responds to different approaches and has varied journeys through and within their mental health problems. This can be challenging for students and service users because there is no simple explanation or answer. What is important is that the person develops an understanding of their experience which is acceptable to them and therefore the mental health nurses' role often involves supporting them during the periods of uncertainty, offering possible explanations and helping them to apply this to their own understanding.
Biological
Biological explanations of mental health problems have consistently dominated approaches adopted within mental health services in the UK since psychiatry was first established. This school of thought is sometimes known as the medical model or disease model and views mental health problems as a disease of the brain. It assumes that mental health problems can be assessed and treated in the same way as physical health problems. This involves the identification of a set of symptoms which are grouped together to inform a diagnosis and a plan of treatment. This process is led by a psychiatrist and can require admission to hospital. It often incorporates the use of medication which affects the central nervous system and the ways in which specific neurotransmitters work within the brain. This area of mental health nursing practice will be explored in more detail in Chapter 9.
There are some observable changes in the brain which can influence behaviour. A good example of this is dementia or brain injury resulting from physical trauma. However, the medical model has extended beyond these organic conditions to explain mental health problems such as depression and schizophrenia. These disorders are attributed to factors such as the following:
• A change in the levels of neurotransmitters which can be detected in urine and saliva (Plant & Stephenson 2008).
• Physiological differences such as the size of the temporal lobe in the brain (Gournay 1996).
• A genetic predisposition which is inherited from a family member.
Some people find this approach helpful because it offers them an explanation for their problems and a way of classifying a complex experience. It provides reassurance that others have similar problems and that there are evidence-based treatments which can potentially minimise or eradicate symptoms. However, there are significant criticisms posed at this model of mental health, particularly from service users. These include the following (Norman & Ryrie 2009):
• The assumption that the problem is due to a dysfunction which automatically places the person in a disabled position and therefore at a disadvantage.
• The power that is associated with medical language which can only be understood by those who are educated in the specialist area.
• The tendency for people to become passive recipients of treatment which is prescribed by professionals as opposed to partnerships in their care and recovery.
Psychological
There are a number of schools of thought which fall under the umbrella of psychological models. These include the following.
Psychodynamic
This approach has a primary focus on the ideas and feelings which are behind behaviours, words and actions. It assumes that a significant level of behaviour is determined by mental functioning which we are not aware of. This is influenced by early experiences which occur during childhood and go on to influence the way the person views themselves and the strategies they use to defend themselves as adult. Intervention therefore involves developing an understanding of the different levels of mental functioning known as the conscious and unconscious and addressing negative defence mechanisms.
Cognitive
The cognitive approach is based upon the assumption that the way people interpret their thoughts will subsequently determine their behaviour. The ABC model developed by Ellis (1962) describes this process:
Interventions within this model attempt to identify and alter beliefs about the activating event which are often described as dysfunctional thinking patterns.
Behavioural
The behavioural model is underpinned by learning theory which assumes behaviours are learnt responses that are influenced by external events, stressors and individual personalities. The learnt response is thought to be developed by two key types of conditioning:
1 Classical conditioning (Pavlov 1927)
This term refers to a natural stimulus that becomes associated with an unrelated stimulus response sequence. For example, Pavlov's seminal work illustrated this. In this famous experiment, a dog was conditioned to salivate in response to a bell as opposed to food. Initially the dog was given food at the same time as the sounding of a bell. After a few trials, the dog would salivate at the sound of the bell without the food.
2 Operant conditioning (Skinner 1972)
This results from gaining positive outcome from a behaviour and then applying it to other scenarios (positive reinforcement). For example, Skinner found that rats would initially press levers in a box due to natural curiosity. One of the levers would release food and therefore, after a few tries, the rats learnt to press the lever that released food until they were full, and not to press the other levers.
The behavioural model focuses on changing or replacing a behaviour which is causing the person distress with a more helpful response. This is usually achieved by gradually exposing the person to a stimulus which would normally evoke a negative response and supporting the person to alter how they behave in reaction.
Cognitive and behavioural approaches are often used in combination (cognitive behavioural therapy; CBT). These approaches attempt to address the thinking which underpins a behaviour in combination with changing the behaviour itself. It is recognised that each element can reinforce the other and therefore it is important to address both. This approach is currently gaining increasingly favourable outcomes and has been recommended widely within the National Institute for Health and Clinical Excellence (NICE; 2010) guidelines for a range of mental health problems. Interventions used within this approach will be described in Chapter 11.
Psychological understandings of mental health problems are often positively regarded by service users. They offer the opportunity to build a therapeutic relationship with a professional in order to explore the feelings, thoughts and behaviours which are affecting their mental wellbeing. People often describe feeling genuinely listened to and there appears to be a higher potential for a collaborative working partnership. However, there are limitations to these approaches:
• There is limited evidence which is viewed as ‘scientific’ to support these approaches due to the many variables that can influence the outcome of the interventions.
• There are often long waiting lists to receive this type of support which limits its accessibility in practice.
• They often require a significant commitment from the individual to the approach. This might include homework, an acceptance that their thinking style or behaviour is problematic and the ability to articulate complex thought and behaviour patterns.
• These requirements are sometimes unrealistic for people who have complex problems and therefore they may be labelled as lacking motivation to change and excluded from psychologically-based therapy on this basis.
Social
The social model focuses on the person in the context of society and considers the influences of social forces on mental wellbeing. Social forces are factors such as isolation, limited relationships, poor living circumstances and unemployment. These factors are suggested to lead to a loss of social role and subsequent alienation from mainstream society which is viewed as the precipitant for mental health problems (Pilgrim & Rogers 1999). When combined with major life events, such as bereavement and divorce, these factors become even more of an issue because people are not able to draw upon social support or resources to help them cope. Interventions within this model are focused on supporting the person to maintain or re-establish an acceptable role in society through support with employment, relationships and social skills.
According to the social model, all behaviour should be understood from within its social context and the boundary between normal and abnormal should be challenged. The social model is very critical of the medical model because it views the stigma and discrimination which can arise from being given a diagnosis of a mental disorder as significantly damaging to the person's position in society.
The challenges associated with this model are grounded in the difficulties with shifting social beliefs and attitudes in order to challenge social exclusion. This prospect can be extremely overwhelming for the service user and mental health practitioners working in isolation. There has been significant political recognition and investment in strategies to challenge social exclusion for service users. However, research into public attitudes suggests that these interventions have had limited impact on society's core perceptions (Crisp et al 2005).
Integrated approaches
This discussion has briefly outlined the key principles and assumptions associated with the various models of mental health. Each one has advantages and limitations, largely due to their attempts to reduce complex emotional experiences into one explanation. We suggest that each model offers helpful ways of thinking about the possible cause of the person's mental health problems and approaches adopted in mental health nursing are often informed by a combination of each. The approach that you adopt may be influenced by the philosophy of the organisation or team you are working within, the resources available to you and your own personal values and beliefs about mental health problems. However, we would discourage you from discounting the ideas of a particular model on the basis of personal preference or prejudices. It is helpful to think of these models as the tool box which you can draw upon to inform your practice depending on the individual you are working alongside.
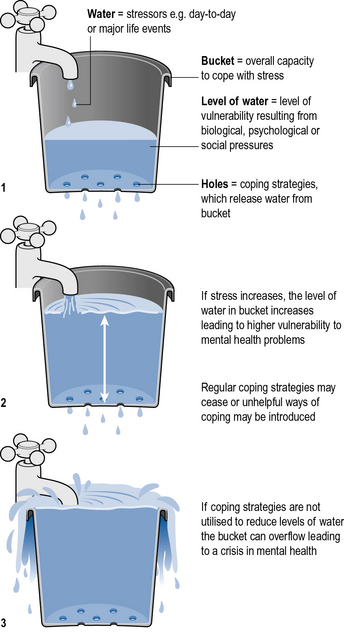
An example of how these models have been brought together is the Stress Vulnerability Model developed by Zubin and Spring (1977). This model is known as a biopsychosocial model. It assumes that we all have a vulnerability to mental health problems, however, for some people, the level of vulnerability is higher. This is as a result of genetic predispositions (biological) and disruptions during childhood (psychodynamic) which can lead to problematic learnt behaviours (behavioural) or a negative perception of self (cognitive). If vulnerability is high, low levels of stress can lead to the experience of mental health problems and major life events are more likely to result in a crisis of mental health. The coping strategies that are employed to deal with stress are suggested to be less well developed due to the impact of negative social circumstances which may have led to poor role modelling or a lack of opportunity to develop supportive social relationships (social). The leaky bucket analogy illustrated in Figure 3.2 can be helpful to explain how each of these factors connect to contribute to a person's vulnerability to mental health problems.
This model continues to be influential in current mental health practice and often informs approaches to working with people who hear voices or have unusual beliefs, such as psychoeducation, relapse prevention and coping skills enhancement. Each of these interventions will be discussed in more detail in Chapter 13.
Mental health policy and law
Policy and law are important areas within mental health care that can impact on the structures and values of service delivery. The following section provides a brief outline of the role of mental health policy and summarises the central mental health policy documents from recent years. While you are a student nurse, it may feel that legal and ethical responsibilities lie with your mentor who is supervising your practice. However, the Nursing and Midwifery Council (NMC) code (2008) states that you are personally accountable for your actions and omissions, regardless of advice or directions from another professional. Therefore, an awareness of the legal frameworks which underpin practice which you are involved in are extremely relevant to you. Furthermore, the mental health nursing skills which are described in this book are underpinned by a requirement to deliver them ethically and in accordance with the law.
Mental health policy
In order to consider the application and relevance of mental health policy in contemporary services, it is useful to briefly explore what is meant by ‘policy’. The term is one that to a certain extent defies a definition as there is not a specific agreement about what constitutes policy. However, Lester and Glasby (2006) suggest that policy relates to a series of decisions, acknowledging that those who make the decisions are not necessarily those who will be implementing them into practice. Rogers and Pilgrim (2001) highlight that mental health policy relates to the directives, financial resources and legal frameworks developed for mental health care. They also highlight the sometimes competing functions that this serves in terms of policy being aimed at responding to distress but also controlling behaviour.
Within your practice experiences you will have been directed at some point to the local policies within the organisation where you are working. These local policies provide guidance and direction for specific practices within the local area such as a ‘lone worker’ policy guiding how to maintain your safety when working in the community. Policy on a national level provides guidelines for the direction of services. This helps to outline and agree the priorities, values and philosophy for care delivery. Certain policies may also be accompanied by financial investment and directives that alter the structure of service delivery. For instance, the National Service Framework for Mental Health (DH 1999) supported the development of assertive outreach, early intervention and crisis home treatment teams. This created a path for the services to be delivered nationally.
Table 3.2 contains a summary of some key policies impacting on mental health care.
Table 3.2 Summary of key mental health policy documents
| Policy document | Key themes |
|---|---|
| DH (1999) National service framework for mental health | Developing national standards for health care relating to: mental health promotion, primary care, access to services, care for people with severe mental illness, carers and suicide prevention |
| DH (2001) Journey to recovery; the government's vision for mental health care | Services should support people to work towards recovery. They should work with individuals as partners in their care and be responsive to their needs. These reflect the new government priorities |
| DH (2002) Women's mental health: into the mainstream. Strategic development of mental health care for women | Highlights that policy, research and services need to recognise the potential differences in the needs of men and women. This includes identifying the need for gender-sensitive and gender-specific services |
| DH (2004) National service framework for children, young people and maternity services | Focuses on standards for care relating to young people and families. This includes that care provided is person centred and that young people with mental health needs should have an effective assessment. Therapeutic relationships should be developed with young people to promote effective care |
| DH (2004) National service framework for older people | Outlines set of standards for care relating to older people, including: promoting independence, person-centred care, tackling discrimination. Considers older people and mental health |
| DH (2004) National suicide prevention strategy for England | Policy to support reduction in suicide through: reducing risk in high-risk groups, mental health promotion and wellbeing, reducing access to methods, promoting research, impact on media reporting and monitoring targets for prevention |
| DH (2004) Ten essential shared capabilities | Outlines core capabilities for the entire mental health workforce to inform training, continuing professional development and direction of mental health care. Includes focus on: values, social inclusion and recovery, diversity, positive risk taking |
| DH (2005) Delivering race equality in mental health care; a summary | Recognises inequalities in the care received by black and minority ethnic groups. Outlines action plan to address this through enhancing quality in services and ensuring they are more responsive, that there are better relationships between services and local communities and more effective communication and information sharing |
| DH (2006) From values to action. Chief Nursing Officer's review of mental health nursing | Provides recommendations for the future direction of mental health nursing in terms of practice and education. This document is centred on recovery and commits to embedding this within training. Also highlights the significance of providing effective support and leadership |
| DH (2009) New horizons; a shared vision for mental health | The key aims of the policy are to improve the general mental health and wellbeing of the population alongside enhancing the quality and accessibility of support provided to those with poor mental health. This includes recognising need to tackle stigma and discrimination, that mental and physical health care are linked and that there is a need to provide help early |
Further details regarding mental health policy may be found at http://www.dh.gov.uk where most of these policies can be downloaded. The approaches to policy across the UK have been similar. For instance, the review of mental health nursing in Scotland was conducted separately and published by the Scottish Executive (2006) but focused on recovery as the driving philosophy for mental health care. However, the structures and impact of these policies may be different within Scotland, Wales and Northern Ireland as each country has legislative powers for policy development in health (Williamson et al 2008). As the publication of mental health policy is linked to national government through the Department of Health, this means the direction of health policy and therefore health services are particularly sensitive to changes in the political views of the ruling government. All of the examples of policy included here were published during a previous government. New health policy will constantly evolve to provide new and a potentially changing direction for health care.
National Institute for Health and Clinical Excellence guidelines
NICE provides national guidelines on the treatment of different health problems. These guidelines are based on a review of the relevant evidence and outline priorities for suggested treatments. They also include an appraisal of the costs and benefits of the interventions, therefore taking into consideration value for money (http://www.nice.org.uk/).
Using the information from Table 3.2 and any further reading about policy on your next placement:
As with any piece of evidence, the NICE guidelines should be viewed critically. It offers evidence-based guidelines that recommend specific standards of practice. However, it has received some criticism for how the evidence it uses is defined. Also some service users and carers feel that some recommendations are driven by cost alone rather than health benefits and quality.
It may be useful for you to read one of these pieces of evidence from NICE prior to your placement, in particular one that relates to the care of the client group in that placement.
Relevance to practice
Policy has a powerful impact on practice delivery. This is important in terms of working towards national standards, promoting equity of access to care as well as addressing gaps in provision and quality. The start of this section suggested policy is defined as the decision-making process. Recently, there has been a drive towards involving stakeholders in the development of policy, including consultation with professionals and service users, although there have been a number of barriers to these stakeholders having their voices heard, in particular people who have used services (Trivedi 2001). As a mental health nurse, there is an expectation that, beyond initial registration, you will be committed to keeping up to date with changes in evidence and research. This also includes being aware of policy developments and their potential impact on mental health practice.
Given that policy development should include the contribution of key stakeholders such as mental health nurses, there is also a key role for the nurse in shaping as well as responding to mental health policy. This was evidenced in the contribution of mental health professionals as part of the ‘Mental Health Alliance’ in challenging the government's amendments to the Mental Health Act (see http://www.mentalhealthalliance.org.uk/).
This section has outlined the relevance of policy to mental health practice and linked this to the significant policy documents influencing mental healthcare delivery since 1999.
Mental health law
Law refers to a set of rules or norms of conduct which mandate, prescribe or permit specified relationships among people and organisations. They provide methods for ensuring the fair treatment of people, and provide punishments for those who do not follow the established rules of conduct. The combination of those rules and principles of conduct originate from court decisions and are established by local custom. Practitioners are accountable in law as well as to professional bodies via codes of ethics or conduct.
There are two types of law in England:
Negligence
Negligence is the breach of a common law duty of care owed to one person by another which results in damage being caused to that person. Clinical negligence is concerned with claims against doctors, nurses and other healthcare professionals and their employers. In order to succeed in a claim for negligence, the claimant needs to prove the following:
Legal documents can often be difficult to understand and apply to practice. There are a number of helpful guides which come from reliable sources and help to explain complex law to practitioners and service users. The following links are examples of these:
 National Mental Health Development Unit (http://www.nmhdu.org.uk/nmhdu/)
National Mental Health Development Unit (http://www.nmhdu.org.uk/nmhdu/)
Mind (http://www.mind.org.uk/)
Use the information provided at these links and the remainder of this chapter to answer the following questions relating to the 2007 Mental Health Act:
• That the doctor or other healthcare professional owed a duty to take care of the claimant and not cause injury.
• That there was a breach of that duty to take care.
For there to be a breach of the duty to take care, it is necessary to show that whatever the healthcare professional, for example the nurse, did or did not do fell below the standard of a reasonably competent nurse in that particular field of health care. This is known as the Bolam Test.
Confidentiality
Service users are legally entitled to expect that information which a healthcare professional learns during the course of clinical practice will remain confidential. The principal legislations concerning the protection and use of personal information are listed below.
• Human Rights Act 1998 – the right to respect for private and family life.
• The Freedom of Information Act 2000 – gives individuals the rights of access to information held by public organisations.
• Data Protection Act 1998 – governs the protection and use of personal information about a living person.
• Mental Capacity Act 2005 – gives individuals who must be involved in decision making on behalf of a person without capacity the right to relevant information.
• The Common Law Duty of Confidence – requires that information that has been provided in confidence may only be used for purposes of which the subject has been informed and given their consent unless there is a legal obligation to disclose. The circumstances making disclosure of confidential information lawful are:
In the NHS, all healthcare professionals are bound by a legal duty of confidentiality in their contracts of employment and breaching this will lead to disciplinary action and can lead to dismissal. All healthcare professionals are held to an ethical duty of confidentiality by their professional bodies and any breach can lead to disciplinary action. This is stated within The Code: Standards of Conduct, Performance and Ethics for Nurses and Midwives (NMC 2008).
Disclosures may be made only in the following circumstances:
Consent
The ethical principle that each person has a right to self-determination and is entitled to have their autonomy respected finds its expression in law through the notion of consent. For consent to be valid it must be ‘real’, that is, certain criteria must be met. The service user must:
– have the capacity to give consent
– know in broad terms what they are consenting to
– give their consent freely without being misled, placed under duress or subject to undue influence.
If an adult person meets the criteria to be able to consent to treatment then they also have the right to refuse treatment both at the time it is offered and in the future. Such a refusal of treatment must be respected even if it may lead to the death of the service user. The Mental Health Act 1983 can be used to override a person's competent refusal of treatment for a mental disorder in certain circumstances.
Capacity
Competence is a pivotal concept in decision making about medical treatment. Competent decisions about accepting or rejecting proposed treatment are respected. Incompetent patients' choices, on the other hand, are put to one side, and alternative mechanisms for deciding about their care are sought (Grisso & Applebaum 1998). The legal mechanism for making decisions about the care and treatment of people who lack capacity to make decisions has been governed by statute law since 1 October 2007, due to the Mental Capacity Act 2005.
Statute law
Mental Health Act 1983
This legislation allows service users to be admitted to mental hospitals and detained in appropriate circumstances. Action may only be taken if there is clear evidence that the medical condition of a service user justifies such action. Admission to hospital under the civil sections of the Act (Part II) may only be made where there is a formal application by either an approved mental health professional or the nearest relative. An application is founded on two medical recommendations made by two qualified medical practitioners, one of whom must be approved for the purpose under the Act. Different procedures apply in the case of emergencies.
The most commonly used sections of the Act are the following:
• Section 2 – detention in hospital for assessment for a maximum of 28 days.
• Section 3 – detention in hospital for treatment for up to 6 months which is renewable for a further 6 months and then for 1 year at a time.
• Section 4 – detention in hospital for assessment in cases of emergency for 72 hours maximum.
• Section 5(2) – compulsory detention of informal service users already in hospital for 72 hours.
• Section 5(4) – nurses holding power leading to compulsory detention of informal service users already in hospital for 6 hours.
• Section 17 – leave of absence from hospital: can be given at the order of the responsible clinician (RC), at any time and with any conditions.
• Section 37/41 – detention in hospital which is not time limited. Discharge and leave is restricted by the Home Office as opposed to the resident medical officer.
• Section 58 – treatment which requires consent or a second opinion after 3 months in order to continue. If continued treament is agreed, a form 39 (certificate to treat) is issued.
• Section 117 – under this section, health authorities and local social services authorities have a legal duty to provide aftercare for service users who have been on sections 3, 37, 45a, 47 or 48, but who have left hospital.
Mental Health Act 2007
The Mental Health Act 2007 made changes to the Mental Health Act 1983 through a number of amendments.
Definition of mental disorder
The new Act changes the way in which the 1983 Act defines mental disorder so that a single definition applies throughout the Act and abolishes references to categories of disorder. Section 1(2) states that ‘mental disorder’ means any disorder or disability of the mind; and ‘mentally disordered’ shall be construed accordingly. The effect is to widen the application of the provisions in question to all mental disorders.
There is a single exclusion stating that dependence on alcohol or drugs is not to be considered a disorder or disability of the mind for the purposes of the definition of mental disorder.
Appropriate treatment test
This replaced the ‘treatable test’ and aims to ensure that a service user is only detained if appropriate medical treatment is available to them. However, the definition of medical treatment has also been widened to include psychological intervention and specialist mental health rehabilitation.
Professional roles
The role of responsible clinician (RC) replaces the role of responsible medical officer. The RC could be any professional with the appropriate skills and training. The new legislation also replaces the approved social worker (ASW) with an approved mental health professional (AMHP). The AMHPs will take on the functions of the ASWs and may be suitably skilled and experienced nurses, occupational therapists and psychologists.
Supervised community treatment
The supervised community treatment provisions will allow some service users with mental disorder to live in the community while still being detained under the Mental Health Act. Only those service users who are detained in hospital for treatment will be eligible to be considered and an AMHP needs to be in agreement. Also, to be considered for a community treatment order (CTO), it must be judged that it is necessary for the patient's health or safety or for the protection of other persons that the patient continues to receive their treatment when discharged from hospital. There is a power of recall to hospital for up to 72 hours during which treatment can be imposed under Part IV of the Act. The order lasts initially for 6 months, can be renewed for another 6 months and thereafter for periods of 1 year at a time.
Mental health review tribunals
A maximum period is being introduced during which managers can refer service users to the mental health review tribunal. Managers will be required to refer a service user at 6 months from the day that he/she was first detained and take into account the fact that a patient may have been detained for assessment.
Restricted patients
Section 41 of the Mental Health Act 1983 is amended to remove the power of the Crown Court to make time-limited restriction orders.
Deprivation of liberty
This makes it lawful to detain someone in hospital under the condition that it is an emergency, the person is reliably shown to be suffering from a mental disorder or the disorder is of a nature that warrants compulsory confinement.
Additional safeguards to service users
The new Act gives service users the right to make an application to court to displace their nearest relative and adds the criterion of being ‘otherwise not a suitable person to act as such’ to the existing criteria for displacement. Civil partnerships will now be recognised as equivalent to marriage under the list of nearest relatives.
The Act also provides the following safeguards:
• Electroconvulsive therapy (ECT) cannot be given to a detained patient who refuses consent except in an emergency situation.
• ECT cannot be given to a person who lacks capacity if it conflicts with an advance decision refusing treatment.
• ECT can only be given to a detained patient under Section 62 when it is immediately necessary to save the patient's life or prevent a serious deterioration in his condition.
• Service users detained under the Mental Health Act 1983 are to be given statutory rights to an advocacy service.
• Trusts must provide age-appropriate accommodation for the treatment of informal and detained service users under the age of 18 with mental health disorders (subject to their needs).
Mental Capacity Act 2005
This Act provides a statutory framework to empower and protect people who lack the capacity to make some decisions for themselves. It generally applies only to people aged 16 or over. It also brings in legal mechanisms that a person with capacity can use to make preparations for a time when they may lack capacity in the future.
The whole Act is underpinned by a set of five key principles set out in Section 1 of the Act:
1. A resumption of capacity – every adult has the right to make his or her own decisions and must be assumed to have capacity to do so unless it is proved otherwise.
2. Individuals being supported to make their own decisions – a person must be given all practicable help before anyone treats them as not being able to make their own decisions.
3. Unwise decisions – just because an individual makes what might be seen as an unwise decision, they should not be treated as lacking capacity to make that decision.
4. Best interests – an act done or decision made under the Act for, or on behalf of, a person who lacks capacity must be done in their best interests.
5. Least restrictive option – anything done for, or on behalf of, a person who lacks capacity should consider options that are less restrictive of their basic rights and freedoms if they are as effective as the proposed option.
Assessing lack of capacity
The Act sets out a single clear test for assessing whether a person lacks capacity to take a particular decision at a particular time. It is a ‘decision-specific’ and ‘time-specific’ test. No one can be labelled ‘incapable’ simply as a result of a particular medical condition or diagnosis. Section 2 of the Act makes it clear that a lack of capacity cannot be established merely by reference to a person's age, appearance or any condition or aspect of a person's behaviour that might lead others to make unjustified assumptions about capacity. If a doctor or healthcare professional proposes treatment or an examination, they must assess the person's capacity to consent. In settings such as a hospital, this can involve the multidisciplinary team but, ultimately, it is up to the professional responsible for the person's treatment to make sure that capacity has been assessed. A person's capacity must be assessed specifically in terms of their capacity to make a particular decision at the time it needs to be made.
How to assess capacity
Capacity is assessed by asking the following questions:
1. Does the person have an impairment of the mind or brain, or is there some sort of disturbance affecting the way their mind or brain works?
2. If so, does that impairment or disturbance mean that the person is unable to make the decision in question at the time it needs to be made?
A person is unable to make a decision if they cannot:
– understand information about the decision to be made
– retain that information in their mind
– use or weigh that information as part of the decision-making process
– communicate their decision (by talking, using sign language or any other means).
The first three points above need to be applied together. If a person cannot do any of these three things, they will be treated as unable to make the decision. It is sometimes assumed that service users lack capacity as a result of their altered perceptions, unusual beliefs or poor memory.
Consider the following scenario in light of the criteria outlined above.
Brenda is an 87-year-old lady with a diagnosis of early dementia. She is beginning to find it difficult to manage in her home and her children are extremely worried about her safety. Brenda is adamant that she does not want to leave her home and is willing to have help with her day-to-day activities. Brenda's children are not satisfied with this option and are telling your mentor that her mental state is far worse than it appears and that she is not capable of making a decision about her safety.
An act done or decision made for or on behalf of a person who lacks capacity must be in that person's best interests. A person can put his/her wishes and feelings into a written statement if they so wish, which the person making the determination must consider. In addition, people involved in caring for the person lacking capacity have to be consulted concerning a person's best interests.
Acts in connection with care or treatment
Section 5 offers statutory protection from liability where a person is performing an act in connection with the care or treatment of someone who lacks capacity. This could cover actions that might otherwise attract criminal prosecution or civil liability if someone has to interfere with the person's body or property in the course of providing care or treatment.
Restraint
Section 6 of the Act sets out limitations on Section 5. It defines restraint as the use or threat of force where a person who lacks capacity resists, and any restriction of liberty or movement whether or not the person resists. Restraint is only permitted if the person using it reasonably believes it is necessary to prevent harm to the person who lacks capacity, and if the restraint used is a proportionate response to the likelihood and seriousness of the harm.
Lasting powers of attorney (LPA)
The Act allows a person to appoint an attorney to act on their behalf if they should lose capacity in the future. It allows people to empower an attorney to make personal welfare decisions, including healthcare and consent decisions. Before it can be used, an LPA must be registered with the Office of the Public Guardian.
Court-appointed deputies
The Act provides for a system of court-appointed deputies who are able to be appointed to take decisions on welfare, healthcare and financial matters as authorised by the Court of Protection but are not able to refuse consent to life-sustaining treatment. They are only appointed if the Court cannot make a one-off decision to resolve the issues.
Court of Protection
This court has jurisdiction relating to the whole Act. It has its own procedures and nominated judges. It is able to make declarations, decisions and orders affecting people who lack capacity and make decisions for, or appoint deputies to make decisions on behalf of, people lacking capacity. It deals with decisions concerning property and affairs, as well as health and welfare decisions. It is particularly important in resolving complex or disputed cases involving, for example, whether someone lacks capacity or what action is in their best interests. The court is based in venues in a small number of locations across England and Wales and is supported by a central administration in London.
Public guardian
The public guardian has several duties under the Act and is supported in carrying these out by the Office of the Public Guardian. The public guardian and his staff are the registering authority for LPAs and deputies. They supervise deputies appointed by the court and provide information to help the court make decisions. They also work together with other agencies, such as the police and social services, to respond to any concerns raised about the way in which an attorney or deputy is operating. A public guardian board has been appointed to scrutinise and review the way in which the public guardian discharges his functions.
Independent mental capacity advocate (IMCA)
An IMCA is someone instructed to support a person who lacks capacity but has no one to speak for him or her, such as family or friends. They have to be involved where decisions are being made about serious medical treatment or a change in the person's accommodation where it is provided or arranged by the NHS or a local authority, and may be involved in abuse cases. The IMCA makes representations about the person's wishes, feelings, beliefs and values and, at the same time, brings to the attention of the decision maker all factors that are relevant to the decision. The IMCA can challenge the decision maker on behalf of the person lacking capacity if necessary.
Advance decisions to refuse treatment
The Act creates statutory rules with clear safeguards so that people may make a decision in advance to refuse treatment if they should lack capacity in the future. The Act sets out two important safeguards of validity and applicability in relation to advance decisions. Where an advance decision concerns treatment that is necessary to sustain life, strict formalities must be complied with in order for the advance decision to be applicable. These formalities are that the decision must be in writing, signed and witnessed. In addition, there must be an express statement that the decision stands ‘even if life is at risk’ which must also be in writing, signed and witnessed.
A criminal offence
The Act introduces a new criminal offence of ill treatment or wilful neglect of a person who lacks capacity. A person found guilty of such an offence may be liable to imprisonment for a term of up to 5 years.
The Mental Capacity Act Deprivation of Liberty safeguards
The Mental Capacity Act Deprivation of Liberty (MCA DOL) safeguards (formerly known as the Bournewood safeguards) were introduced into the Mental Capacity Act 2005 through the Mental Health Act 2007.
The MCA DOL safeguards apply to anyone:
– who suffers from a mental disorder or disability of the mind, such as dementia or a profound learning disability
– who lacks the capacity to give informed consent to the arrangements made for their care and/or treatment
– for whom deprivation of liberty is considered, after an independent assessment, to be necessary in their best interests to protect them from harm.
The safeguards cover patients in hospitals, and people in care homes registered under the Care Standards Act 2000, whether placed under public or private arrangements. The safeguards are designed to protect the interests of an extremely vulnerable group of service users and to:
Conclusion
The material presented in this chapter is complex and should be considered in preparation for a mental health placement and then reconsidered in light of day-to-day experiences which you have encountered. The scenarios in practice which challenge us often expose the contradictions and dilemmas which exist within ethical and legal frameworks. The answer is rarely obvious and the decision is unlikely to be black or white. The use of clinical judgement is therefore highly important along with the opportunity to discuss and explore with colleagues.
Anderson R., Oades L., Caputi P. The experience of recovery from schizophrenia: toward an empirically validated stage model. Australian and New Zealand Journal of Psychiatry. 2003;37:586–594.
Anthony W. Recovery from mental illness: the guiding vision of the mental health service system in the 1990s. Psychosocial Rehabilitation Journal. 1993;16:11–23.
Berger J.L. Incorporation of the Tidal Model into the interdisciplinary plan of care – a program quality improvement project. Journal of Psychiatric and Mental Health Nursing. 2006;13(4):464–467.
Cook N.R., Phillips B.N., Sadler D. The Tidal Model as experienced by patients and nurses in a regional forensic unit. Journal of Psychiatric and Mental Health Nursing. 2005;12(5):536–540.
Cooper L. Values-based mental health nursing practice. In: Callaghan P., Playle J., Cooper L. Mental health nursing skills. Oxford: Oxford University Press, 2009.
Crisp A., Gelder M., Goddard E., Meltzer H. Stigmatization of people with mental illness. A follow up study within the Changing Minds campaign of the Royal College of Psychiatrist. World Psychiatry. 2005;4(2):106–113.
Department of Health. National service framework for mental health: modern standards and service models. London: HMSO; 1999.
Department of Health. Journey to recovery;. DH, London: the government's vision for mental health care; 2001.
Department of Health. Women's mental health: into the mainstream. DH, London: Strategic development of menatl health care for women; 2002.
Department of Health. The ten essential shared capabilities. DH, London: A framework for the whole of the mental health workforce; 2004.
Department of Health. Delivering race equaligy in mental health care; a summary. London: DH; 2001.
Department of Health. From values to action: the Chief Nursing Officer's review of mental health nursing. London: DH; 2006.
Department of Health. New horizons;. London: a shared vision for mental health. DH; 2001.
Ellis A. Reason and emotion in psychiatry. New York: Stuart; 1962.
Fulford K.W.M. Ten principles of values-based medicine. In: Radden J., ed. The philosophy of psychiatry: a companion. New York: Oxford University Press, 2004.
Gordon W., Morton T., Brooks G. Launching the Tidal Model: evaluating the evidence. Journal of Psychiatric and Mental Health Nursing. 2005;12(6):703–712.
Gournay K. Schizophrenia: a review of the contemporary literature and implications for mental health nursing theory, practice and education. Journal of Psychiatric and Mental Health Nursing. 1996;3:7–12.
Grisso T., Appelbaum P.A. The assessment of decision-making capacity: a guide for physicians and other health professionals. Oxford: Oxford University Press; 1998.
Lafferty S., Davidson R. Person-centred care in practice: an account of the implementation of the Tidal Model in an adult acute admission ward in Glasgow. Mental Health Today, 2006:31–34 (March)
Lester H., Glasby J. Mental health policy and practice. Basingstoke: Palgrave Macmillan; 2006.
National Institute for Health and Clinical Excellence. Guidance. London: NICE; 2010.
Norman I., Ryrie I. The art and science of mental health nursing. A textbook of principles and practice, 2nd ed. London: Open University Press; 2009.
Nursing and Midwifery Council. The code: standards of conduct, performance and ethics for nurses and midwives. London: NMC; 2008.
Pavlov I. Conditioned reflexes. Oxford: Oxford University Press; 1927.
Pilgrim D., Rogers A. Sociology of mental health and illness. Oxford: Oxford University Press; 1999.
Plant J., Stephenson J. Beating stress, anxiety and depression. London: Piatkus Press; 2008.
Repper J., Perkins R. Social inclusion and recovery: components of a model for mental health practice. Edinburgh: Baillière Tindall; 2003.
Rogers A., Pilgrim D. Mental health policy in Britain, 2nd ed. Basingstoke: Palgrave; 2001.
Scottish Executive. Rights, relationships and recovery: the report of the review of mental health nursing in Scotland. Edinburgh: Scottish Executive; 2006.
Skinner B. Beyond freedom and dignity. London: Jonathan Cape; 1972.
Stevenson C., Barker P., Fletcher E. Judgement days: developing an evaluation for an innovative nursing model. Journal of Psychiatric and Mental Health Nursing. 2002;9(3):271–276.
Trivedi P. Never again. Openmind. 2001;110:19.
Williamson G., Jenkinson T., Proctor-Childs T. Contexts of contemporary nursing, second ed. Exeter: Learning Matters; 2008.
Woodbridge K., Fulford K.W.M. Good practice? Values-based practice in mental health. Mental Health Practice. 2003;7(2):30–34.
Woodbridge K., Fulford K.W.M. Whose values? A workbook for values-based practice in mental health care. London: Sainsbury Centre for Mental Health; 2005.
Zubin J., Spring B. Vulnerability – A new view of schizophrenia. Journal of Abnormal Psychology. 1977;86:103–126.
Barker P., Buchanan-Barker P. The Tidal Model: a guide for mental health professionals. London and New York: Brunner-Routledge; 2005.
Brooker C., Repper J. Mental health; from policy to practice. Edinburgh: Churchill Livingstone; 2009.
Copeland M.E. Wellness recovery action plan. USA: Peach Press; 1997.
Lester H., Glasby J. Mental health policy and practice. Basingstoke: Palgrave Macmillan; 2006.
• WRAP: http://www.mentalhealthrecovery.com
• The Tidal Model: http://www.tidal-model.com
Influential writers in recovery:
• Patricia Deegan: http://www.patdeegan.com
• Rufus May: http://www.rufusmay.com
• Dan Fisher: http://www.power2u.org/who.html