1 Mental health services and nursing
development and practice
• To gain an insight into the historical development of mental health services
• To develop an understanding of the role of the mental health nurse in relation to its origins
• To identify activities that a mental health nurse may be involved in and some of the skills used in these activities
• To gain an understanding of the structure of the multidisciplinary team
Introduction
This chapter aims to give an introduction to mental health nursing, locating this in its historical background to help provide a context for some of the key issues in mental health practice. It is constructed to help develop your knowledge of some of the important structures through which mental health care is delivered and the nature of mental health nursing work. This background helps to provide an introductory understanding of what to expect from your mental health placements.
History of mental health services
The history of mental health care and mental health nursing is both a rich and, at times, traumatic one. This discussion is not able to do full justice to the variety of narratives that are integral to this history, nor is it able to give any great depth of detail on the significant events, experiences and policies that make up this history. Yet the importance of understanding history in mental health nursing lies in the significance of the inequalities in power that still exist between nurses and service users. Gaining an insight into where some of these inequalities come from can be helpful in thinking about how they may be bridged. Additionally, through looking back at the history of mental health services, it may aid in appreciating some of the fears and anxieties that someone may have about using mental health services. Ultimately this can help us in delivering care through how we relate to the people in distress that we are working with. Considering the history of mental health nursing also demonstrates how some of the approaches (such as psychological support) have evolved into the interventions used today.
Through a brief description of the key developments of mental health care it is also hoped that you, as a mental health nurse of the future, will be able to gain an appreciation of the past of mental health nursing and the significance of this past in understanding the rewards and challenges of the role in the present.
Institutionalisation
Following the industrial revolution and the relocation of the population in towns and cities, there was a growth in poverty and ill health (Nolan 1993). This represented an increasing problem for those experiencing mental health problems who were unable to afford the private asylums in operation at the time. Within England, concern over the conditions and treatment within private asylums facilitated a drive for lunacy reform (Porter 2002). Subsequent legislation between 1809 and 1845 allowed for the allocation of funds to build public asylums. This reflects a period of the growth of institutions across Europe and Western societies (Wright 1997). It represented a marked optimism for the benefits of the asylum, underpinned by the growing psychiatric profession and the commitment to institutional care as the vehicle to provide a cure for insanity (Rogers & Pilgrim 2001).
Throughout the history of mental health care, the beliefs and understanding of professionals and the public on the causation of mental health problems have influenced the manner in which people have been treated and the drive for “cures”. In the early days of asylums, treatments were defined by a need for physical restraint on patients. During this period, in the eighteenth and early nineteenth centuries, individuals caring for the inmates of the asylum were termed ‘keepers’. The implications of such a title suggest that those individuals had a role in restricting and controlling the movements of those admitted to the asylum (Nolan 1993).
The optimism for the benefits of a new public asylum system during the mid nineteenth century supported opportunity for the development of pioneering approaches to the management of mental illness developed within the UK and across Europe (Digby 1985, Porter 2002). This included attempts to abandon and reduce the use of physical restraint, examples of which can be seen in the work of Pinel in France, Chiaguri in Italy and Hill and Connelly in England (Porter 2002). 1796 also witnessed the establishment of the York retreat, a Quaker institution founded on the principles of Christian humanism which recognised the humanity of those experiencing mental health problems and promoted moral therapy which attempted to enable individuals to remain included within society (Digby 1985, Nolan 1993).
Within the new public system, after the 1845 Lunacy Act, the role of keeper emerged into one of attendant. The attendant's role was one that involved the most daily contact with people admitted to asylums and they were responsible for their day-to-day care and engagement in work within the asylum. Attendants worked under the direction of the medical superintendent (Nolan 1993). Nolan (1993) notes some early examples of individual superintendents and institutions providing training for attendants but it was not until the very end of the nineteenth century that formalised training was introduced. During this time problems were experienced with the recruitment and conduct of attendants, though pay and conditions were very poor. Pessimism in the asylum system began to spread in the late nineteenth century as asylums became overcrowded and did not deliver the cure for insanity initially hoped for (Porter 2002).
If the history of mental health services and psychiatric hospitals is an area that you are interested in, here is a list of resources that you might find helpful. They include fiction books, video clips and Websites.
Websites
http://www.highroydshospital.co.uk
State of Mind – series of programmes on BBC Radio 4 examining past and contemporary mental health services:
http://www.bbc.co.uk/radio4/science/stateofmind_20090107.shtml (accessed June 2011)
Podcasts of the Institute of Psychiatry debates on a wide range of topics:

Once you have accessed one of these resources:
1. Consider one piece of information that has surprised you.
2. What is it about this that was surprising?
You might want to make a note of some of these issues, in particular the implications for your practice. This can be linked with the activity box on page 21 and included in your portfolio as a record of some of your initial thoughts and reactions at the start of your practice learning journey.
At the turn of the twentieth century, attendants had become known as nurses and the term “mental nurse” was officially instigated on the nursing register in 1923. This reflected the increasing role of psychiatry and the medical approach to understanding mental health problems and therefore nursing was the most appropriate way to care for and treat the mentally ill. During the early part of the century, asylums became known as hospitals. The introduction of the Mental Treatment Act in 1930 represented some attempt to challenge the stigma associated with mental illness that was perpetuated by compulsory treatment through the introduction of voluntary admission. This was underpinned by a desire to treat mental illness within a public health framework (Freeman 1998).
During the twentieth century, further developments in the treatment of mental illness occurred. This included the evolution of a psychodynamic theory pioneered by Freud. However, alongside such developments, treatments were advocated such as psychosurgery which involved removal of parts of the brain thought to be implicated in the symptoms of mental illness. Insulin therapy was also used which involved administering large doses of insulin to cause a coma. These types of treatment, among others, have been heavily criticised as highly dangerous and abusing a population perceived as vulnerable within society. Ion and Beer (2003) warn of the need for us to avoid naively criticising the past without questioning how our own practices may be perceived through the lens of history.
This is particularly poignant given the ethical debates concerning the use of electroconvulsive therapy (ECT) and the damaging impact of psychiatric medication. While there are different perspectives among professionals, service users and families about the use of these interventions today, they are regularly employed to treat mental health problems. The controversies surrounding the use of ECT and psychiatric medication could suggest that their use as treatment may be perceived differently in years to come.
Antipsychotic medication was introduced in the 1950s at a time when the physical state of Victorian asylums was deteriorating and changes in mental health legislation allowed for a more open-door policy within psychiatric hospitals. Public faith in the psychiatric hospital system was diminished through a series of public inquiries and published stories concerning ill treatment, abuse and neglect in hospitals (e.g. Robb 1967). This also occurred within the context of the development of the “antipsychiatry” movement. Key thinkers, such as RD Laing and T Szasz, some of whom were trained psychiatrists, challenged some of the assumptions that mental health problems were a distinct mental illness. A number of antipsychiatrists proposed that mental illness does not exist at all and that people's experiences were the product of an “insane” society. These, combined with other factors, culminated in an announcement by Enoch Powell, in the famous water tower speech, that psychiatric hospitals were consigned to the past and the future of mental healthcare delivery lay in the community. It was also during this time that a humanistic understanding of mental health problems was advocated by Carl Rogers (1967) and the interpersonal nature of nursing was emphasised by the work of Hildegard Peplau (1952).
Over the next 30 years, psychiatric hospitals gradually closed. Historians suggest that care in the community for people with mental health problems has existed for many years including during the asylum era (Wright 1997). However, it is the closure of mental hospitals which contributed to the growth of community nursing and the significant expansion in community services that reflects the model of care delivery we see today. In-patient beds were concentrated in smaller units and district general hospitals rather than distinct large psychiatric hospitals. Many of the service users today who have had long-term needs may have experience of being admitted to an asylum, and this is an area that you might want to explore with them once you have established the therapeutic relationship; particularly considering narratives from people with experience of using services are fairly invisible within the history of mental health care.
This section has highlighted that closure of asylums contributed to a growth in services delivered in the community and that you may have the opportunity to work with people who have experience of being in hospitals such as these.
Make a list of some of the benefits that people who were admitted there, having all mental health services delivered in the asylum, may have had (the Websites listed above may help you). Also make a list of the disadvantages. Review the list and see how this compares to some of the issues that are highlighted in the section below. You might want to revisit this after your first placement to see whether your views have changed.
This historical overview has given an indication of the negative problems associated with the asylum system which has also been criticised for perpetuating stigma and social exclusion through separating people with mental health problems from the remainder of society. However, it is essential to recognise some of the potential benefits of the asylum system, not least as it appeared to offer the best structure for treatment and support to people during their evolution in the Victorian era. Some who have experience of being admitted to psychiatric hospitals speak positively of the peace, quiet and space that were available in the institutions that often had sports grounds, farms and gardens. Social opportunities for connecting with others were also part of the structure of psychiatric hospitals which is important to bear in mind given that isolation remains a barrier to social inclusion and positive mental health for those living in the community.
The majority of mental health services are delivered in the community setting and as a student mental health nurse you will have the opportunity to work in these areas. The evolution of the community teams as the main structures of support for service users provided an important opportunity to challenge the segregation of people with mental health problems and enable people to continue relationships and roles in wider society. This continues to be one of the main areas in which mental health nurses provide support for service users. However, community care has not been without its critics. The closure of psychiatric hospitals and the establishment of community services were chronically underfunded. There was concern that people discharged from psychiatric hospitals were vulnerable to homelessness or ending up as part of the prison population due to a lack of adequate support available in the community setting. During the mid 1990s there were a small number of high-profile incidents of violence related to service users. This led to severe criticism from the press and some charities concerning the appropriateness of supporting people with experience of mental health problems in the community. These incidents and the media and public response to them have been suggested to have had a significant influence on governmental mental health policy at the time, in particular the development of the Care Programme Approach (Hannigan & Cutcliffe 2002). This is explored in more detail in Chapter 8.
The introduction of Modernising Mental Health Services (Department of Health (DH) 1998) and the National Service Framework for Mental Health (DH 1999) outlined the hopes of a new government in tackling these concerns regarding the provision of mental health services and for ensuring the care provided to service users was effective and of good quality. These documents had a significant impact on the structure and development of services and were designed to be underpinned by significant financial investment, though there remains concern that the funding imbalances have not been redressed and mental health care remains a “Cinderella service”.
Over the past 200 years the role of supporting people with mental health problems has evolved from one of keeper of the insane to one of a mental health nurse working alongside people experiencing mental distress. This overview has provided a very brief insight into some of the factors that have informed and shaped this development. An appreciation of the historical roots of the profession is important in order to understand the issues of power and control experienced within mental health services today. In particular, this concerns the contested nature of treatments in mental health alongside the stigma associated with being “consigned to an institution”. Many of these issues bear relevance to today and are picked up in different ways throughout the book. Chapter 3 deals with the philosophies and theories governing contemporary mental health care, some of which you will see have their origins in theories of Rogers and Peplau highlighted here. As you work through this chapter it would be beneficial to think about the similarities and differences between these and what you have read here. Chapter 9 also considers psychiatric medication and enabling people to make choices about their treatment, while Chapter 7 explores the therapeutic relationship and some of the barriers to this. Perhaps more importantly, it is through the professionals and service users that you work with in practice where the relevance of this history may become most apparent, particularly for those who have witnessed and been part of the changes discussed here.
The role of the mental health nurse
What is a mental health nurse?
Mental health nurses work across many diverse settings including GP surgeries, accident and emergency departments, community teams and in-patient psychiatric wards, although there are core skills and values which are integral to this work whatever the setting. This book provides an overview of such capabilities and explores the theory and learning that underpin them in relation to the student practice experience. As you gain familiarity with the literature relating to mental health you may come across debates surrounding the focus and boundaries of the mental health nursing role. This has been influenced by the origin of mental health services, the rapidly changing context of health care over the past 50 years as well as the lack of agreement as to the exact cause and therefore best treatment of mental ill health. This culminates in a situation where it is perhaps more difficult to answer that important question,“what does a mental health nurse do?” than it initially seems.
The last statement has highlighted that it is sometimes difficult to define and identify what is involved in mental health nursing. Often it is a role that can be less visible within media and public information and therefore hard to recognise what it entails until there is the opportunity to gain experience. Some of you may have had this opportunity before starting your first mental health placement.
Think about what you believe mental health nursing is. What does it involve?
It might help you to think about the following:
1. What did you say about the role in your application for your nursing course?
2. What did you say during the selection process about what the role of a mental health nurse entailed?
3. How might it differ from previous experiences that you have had (for instance, as a care support worker)?
To follow this up, make a list of eight roles and responsibilities that you perceive that a mental health nurse is involved in. After this, read the following section and move on to the next activity.
Where might a mental health nurse work?
A mental health nurse can work in a vast variety of different settings. Figure 1.1 is an overview of some of the areas where a mental health nurse may work. This provides some examples of the settings where you could be based (though there may be others that you come across in the course of your training). Chapter 5 goes into more specific detail about each of these areas.
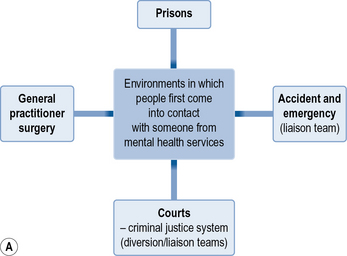
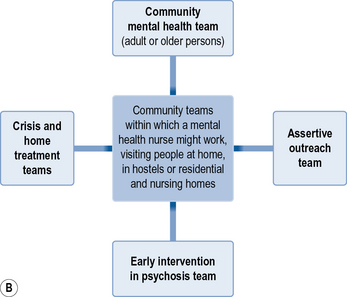
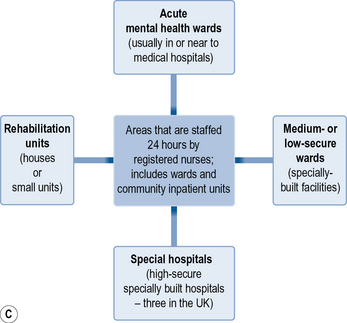
Fig 1.1 Areas of mental health nursing practice. (A) Points of access to service. (B) Community support. (C) In-patient care
The following section defines the nature of mental health nursing work in more detail, aiming to help you begin to answer ‘so what does a mental health nurse do?’
What does a mental health nurse do?
It is important to recognise that the role of a mental health nurse is not a static one and will be developing and changing in response to new healthcare structures, service user and workforce needs alongside new opportunities. In recent years, these changes have included the introduction of mental health nurse prescribers, nurse consultants and the possibility of nurses being involved in the act of sectioning as approved mental health practitioners (explained in more detail in Ch. 4). A key nursing theorist, Altschul (1972), described therapeutic relationships as the core of mental health nursing. In this respect the main tool that the mental health nurse has at his or her disposal to impact positively on an individual's health is his or her self. The relationship that a nurse and service user establish is, therefore, central. This means that communicating effectively and learning to really listen and understand another is one of the most important aspects of being a mental health nurse. Without this, the support a nurse is able to provide is limited.
The contemporary mental health nursing role is a complex one. Mental health nurses are involved in working directly with individuals and families to provide support and deal with the impact of being diagnosed with a mental health problem. They will be involved in promoting the health of the individual, but also increasingly working with schools, colleges and communities to promote mental health and enable people to access opportunities outside mental health services to maximise their potential. Mental health nurses are also involved in managing and leading care (examined in Chs 8 and 14) and contributing to the improvement of health care through research and the development and implementation of strategies for enhancing quality.
Through the therapeutic relationship, mental health nurses assess, plan, implement and evaluate care. This is structured through individual time spent with the person.
Assessment
Through interpersonal interaction, sometimes using more formal assessment tools, the mental health nurse will be involved in a process of assessment with the individual experiencing mental distress. This will entail developing an understanding of who it is to be that person at that point in their life (Barker 1997). Integral to this is gaining a holistic perspective which will incorporate an exploration of their mental distress and current problems but also the impact of relationships, social situation, culture, physical health, spirituality and their strengths and coping strategies on their current experiences and future hopes and goals.
Planning care
The nurse will then work with the individual and potentially their family to prioritise the support that they require and develop a plan of care outlining the nature of that support. What this will entail and the resources that it will incorporate will clearly depend on the individual, their experiences and the context in which care is being delivered.
For instance, in an older persons community team (see Ch. 5), a plan may be orientated towards maintaining activities and cognitive stimulation for a person with dementia. Within an in-patient psychiatric ward it may be orientated towards creating a safe environment to enable individuals to explore and manage their distressing experiences. This process is examined in more detail in Section 2.
Outlined below are the areas where a mental health nurse may provide support, followed by some examples of what this might mean.
Support that is provided by a mental health nurse may include the following:
• Practical: accessing benefit entitlements or supporting someone with an application for an educational course.
• Social: gaining information and helping people to access community resources (such as groups, clubs, courses, gyms) and social opportunities to reduce isolation, extend social networks and enhance self-esteem. It may mean going with them to these activities.
• Psychological: exploring the different ways that individuals may cope with hearing voices, helping them to identify what might trigger or make the voices worse and considering different ways of coping that they may not have tried before.
• Biological: administering medication alongside outlining support for individuals to regularly monitor their blood sugars for diabetes or plan for supporting an individual who may self-harm with dressing their wounds.
• Spiritual: enabling people to access the resources and opportunities that create meaning in their life. This may entail, through the therapeutic relationship, providing a safe space for the person to explore the meaning of their experiences of mental distress.
For the authors, this diversity and breadth of knowledge is integral to building an understanding of individuals in their context. It is also one of the key factors that defines mental health nursing from the other mental health professionals and helps us to be clear about our identity.
The mental health nurse will be engaged in this continual process of assessment, planning, supporting or providing an intervention, evaluating the impact of this and reassessing to inform the next process. This is developed in collaboration with the individual and, where they are involved and consent is given, family and friends. The involvement of the person experiencing mental health problems within this process is essential to ensure that the care provided is meaningful and relevant to them. There are times when this collaboration is challenging, such as when care is enforced through the individual being detained under the Mental Health Act or when a person is so distressed that direct communication about care is difficult. This is a potential tension within mental health services and the role of the mental health nurse.
An introduction to the care programme approach and joint working
One of the main frameworks in the UK, in which this care process is structured in mental health services for adults, is through the Care Programme Approach (CPA). Essentially, this framework was developed to support the increasing amount of care that was delivered in the community in people's own homes. It also aimed to enhance closer working between health and social care services. The CPA sets out the entitlements for the person to have an up-to-date assessment, a care plan that is regularly reviewed and a care coordinator. Mental health nurses are commonly care coordinators although these can also be social workers, psychiatrists and occupational therapists. The role of the care coordinator is to liaise with other professionals to ensure the action in the care plan is being carried out. Mental health services providing care for children and adolescents and older adults (over the age of 65) follow similar processes although they use different terms for these and are being encouraged by the government to introduce the CPA (DH 2008). Refer to Chapter 9 for more detail about using the CPA.
Paperwork and administration are part of a contemporary mental health nurse's role. They are an important part of communication and working effectively in partnership with others. However, it is difficult to achieve the right balance between the requirements of paperwork and the delivery of direct care. It can be frustrating for a nurse as demands of paperwork feel like they may be getting in the way of direct time with service users. A study by the Sainsbury Centre showed that between 27% and 30% of nurses' time was spent on administration and this was the highest of the mental health professions included (Garcia 2006). They also reported too much time doing paperwork contributed to practitioner stress. It is essential that administration systems are not too complex and bureaucratic leading to high demands on resources being concentrated towards paperwork. It is also important that as practitioners we maintain reflective practice in this area to promote efficient working and help avoid paperwork becoming a barrier to spending quality time with services users.
Have a look at the list that you made of the eight roles and responsibilities of the mental health nurse. Consider how this list compares with the outline given above. Is there anything that you would like to add or remove after reading this section?
Keep this list as it will be revisited again in Section 3.
Multidisciplinary team
Within modern healthcare systems, professionals work within multidisciplinary teams. This is perceived as the most effective structure to coordinate the delivery of care and ensures the optimum experience for a service user. Within mental health care, multidisciplinary teams are essential for delivering holistic care which meets the diverse needs and wishes of people with experience of mental distress. It also recognises that the impact of mental health problems can be complex where individuals may benefit from support in a number of areas in their life and that different professionals can offer varied skills and knowledge in these areas.
In response to developing knowledge in mental health care, changing policy and rapidly developing health care, the boundaries of this multidisciplinary team can shift as new roles evolve and change. Figure 1.2 outlines the core roles and professions that you might come across during your mental health placements.
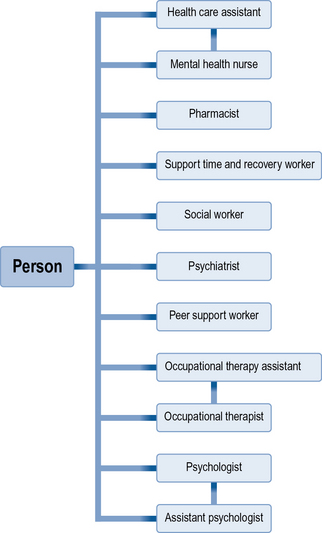
The following discussion considers these roles as they will impact on your experience in placements and the service users you will be working with.
The mental health charity, Mind, have also produced a comprehensive overview of roles in mental health care which can be viewed at: http://www.mind.org.uk/help/research_and_policy/whos_who_in_mental_health_a_brief_guide (accessed June 2011).
Social worker
Social workers tend to be based within community mental health teams. Their background is within the social model (see Ch. 5) and therefore the profession is particularly interested in promoting issues of justice and equality. They have a developing role in relation to personal budgets and direct payments and have played a central role in administering the mental health act.
Occupational therapist
Occupational therapists provide support in areas of occupation. In mental health services this involves assessing and identifying people's interests and capabilities in relation to meaningful activities, often helping people to get access to voluntary work or employment. In some areas this can involve assessing and accessing support aids for activities of daily living within the home environment as well as running social groups. An occupational therapy assistant is an unqualified worker who will provide support for the work of the occupational therapist through direct work with individuals and in groups.
Peer support worker
This is a fairly new role which is rapidly developing. Peer support workers are individuals who themselves have experienced mental distress and provide support to people in a similar situation. Peer support can help people make sense of their experiences and provide inspiration for recovery (Weinstein 2010).
Support time and recovery worker
This role developed with support of the Department of Health to ensure that workers are available with dedicated time to be around service users and provide time and practical support. The introduction of this role promoted an increase in the number of peers employed in this role. Not every team has support time and recovery workers and, in other areas, this role is similar to that of a healthcare assistant.
Psychologist
Clinical psychologists work across different mental health settings. Their focus is on providing psychological support for individuals directed towards their experiences of mental distress and trauma. This tends to be conducted on a one-to-one basis. Psychologists may be involved in delivering different types of psychotherapy such as cognitive behavioural therapy. They may also provide support for service development and facilitate group supervision. Psychology assistants are often individuals gaining an insight into the role prior to undertaking their psychologist training. They will undertake work, with individuals, who experience mental distress supervised by a psychologist.
Healthcare assistant
Healthcare assistants work closely with the nursing team to provide direct care and support to service users. They most commonly work in in-patient settings though increasingly undertake more autonomous roles in community teams. They are involved in developing relationships with service users and providing practical support. They will often spend the most amount of time with service users and be involved in delivering a plan of care. You may actually have been employed as a healthcare assistant prior to commencing your course, or some of you may be working as a healthcare assistant in non-study time. This can give you some valuable insights into mental health care. However, the importance of knowing the difference between qualified and unqualified will be discussed in Chapter 5.
Psychiatrist
A psychiatrist is a qualified medical practitioner who will have undertaken specialist postgraduate training in order to undertake this role. Most areas will work with a consultant psychiatrist who may have a specialist registrar and more junior doctors as part of their team. Psychiatrists often have overall responsibility for the individuals within their care and have specific knowledge and expertise in relation to diagnosing mental health problems, prescribing psychiatric medication and contribute to decisions regarding compulsory admission to hospital under the Mental Health Act.
Pharmacist
Pharmacists are responsible for preparing medication prior to administration. They have in-depth knowledge relating to the biochemical impact of medication. Pharmacists may be involved in reviewing care with other members of the multidisciplinary team and are able to advise on recommended medications and doses.
Approved mental health practitioner
Prior to amendments to the Mental Health Act (1983), only consultant psychiatrists, GPs and social workers who had undergone specialist training could make the decision that an individual was able to be detained under the Mental Health Act, although mental health nurses, doctors and the police had special holding powers (see Ch. 4). Amendments that were introduced by the government in 2007 extended the professionals that could be approved to conduct assessments and make decisions to detain people in hospital. Currently, social workers, mental health nurses, occupational therapists and psychologists can undertake training to become approved mental health practitioners. This has extended the professionals able to take on a role only previously accessible to social workers. The reaction and acceptance of this role among different professions (including nursing) has been mixed.
Partnership organisations
The complexity of the impact that mental health problems can have on people's lives has already been highlighted. This can mean that input is provided by organisations outside of mental health services. This will clearly depend on the individuals' situation and the nature of their needs. However, it is possible that an individual may be receiving support from general healthcare services, from housing, charitable or advocacy organisations. Some people in distress may need ongoing or intensive input with some of these issues and may therefore live in supported accommodation or hostels provided by such organisations. The changing context of healthcare services suggests that these organisations outside of the NHS, in the voluntary or third sector, are likely to take on an increasing role in providing support across care settings, but in particular to individuals who experience mental health problems or who have learning disabilities (Longley et al 2007). Developing relationships and working in partnership with these organisations is an important area for mental health nurses (explored in more detail in Ch. 15). In this respect, as a mental health nurse you may be working as part of a multidisciplinary and interagency team as well as collaboratively with service users and their loved ones. This contributes to the role of a mental health nurse being a complex yet rewarding one.
There will be many opportunities to work with these different professions during your practice experiences. It is likely that you will also meet other students from different disciplines both in practice and theory time. It might be useful to prepare a list of questions that you may have for people from different professional backgrounds, to help you understand their training and role, to aid in future working as part of a multidisciplinary team. Keeping a record of this discussion and reflecting on your responses may contribute to evidence in your portfolio.
Altschul A. Nurse–patient interaction, a study of interaction patterns in acute psychiatric wards. Edinburgh: Churchill Livingstone; 1972.
Barker P. Assessment in psychiatric and mental health nursing. Cheltenham: Stanley Thornes; 1997.
Department of Health. Modernising mental health services: safe, sound and supportive. London: HMSO; 1998.
Department of Health. National service framework for mental health, modern standards and service models. London: HMSO; 1999.
Department of Health. Refocusing the care program approach; policy positive practice guidance. London: HMSO; 2008.
Digby A. Madness, morality and medicine. Cambridge: Cambridge University Press; 1985.
Freeman H. Mental health policy and practice in the NHS: 1948–79. Journal of Mental Health. 1998;7(3):225–239.
Garcia I. A report on the administrative workload of mental health practitioners, amended version. London: Sainsbury Centre for Mental Health; 2006.
Hannigan B., Cutcliffe J. Challenging contemporary mental health policy: time to assuage the coercion? Journal of Advanced Nursing. 2002;37(5):477–484.
Ion R., Beer D. Valuing the past: the importance of an understanding of the history of psychiatry for healthcare professionals, service users and carers. International Journal of Mental Health Nursing. 2003;12:237–242.
Longley M., Shaw C., Dolan G. Nursing: towards 2015. Alternative scenarios for healthcare, nursing and nurse education in the UK in 2015. Pontypridd: Welsh Institute for Health and Social Care; 2007.
Nolan P. A history of mental health nursing. London: Chapman & Hall; 1993.
Peplau H.E. Interpersonal relations in nursing. New York: GP Putnam's Sons; 1952.
Porter R. Madness, a brief history. Oxford: Oxford University Press; 2002.
Robb B. Sans everything. London: Nelson; 1967.
Rogers C. On becoming a person. Constable, London: A therapist's view of psychotherapy; 1967.
Rogers A., Pilgrim D. Mental health policy in Britain, 2nd ed. Basingstoke: Palgrave; 2001.
Weinstein J. Mental health service user involvement and recovery. London: Jessica Kingsley; 2010.
Wright D. Getting out of the asylum: understanding the confinement of the insane in the nineteenth century. Social History of Medicine. 1997;10:137–155.
Callaghan P., Waldrock H. Oxford handbook of mental health nursing. Oxford: Oxford University Press, 2006.
Clarke V., Walsh. Fundamentals of mental health nursing. Berkshire: Open University Press; 2009.
Nolan P. A history of mental health nursing. London: Chapman and Hall; 1993.
Wycroft N. Introduction to nursing. Berkshire: Open University Press; 2009.
Healthcare roles: http://www.mind.org.uk/help/research_and_policy/whos_who_in_mental_health_a_brief_guide (accessed June 2011).
http://www.nhscareers.nhs.uk/index.shtml (accessed June 2011)..