11 Working with people who are anxious or low in mood
Introduction
The interventions and clinical skills described in this chapter are informed by a cognitive behavioural therapy (CBT) approach (see Ch. 3). There is a growing evidence base for the effectiveness of these interventions when working with people who are anxious or low in mood. Additionally there has been strong political support to increase access to psychological interventions in the UK which has led to investment in specific training and service programmes (Department of Health 2008). Efforts have been made to identify the positive elements of a CBT approach and adapt them so that a greater number of practitioners can feel confident using them in mainstream mental health practice. The interventions described here utilise these adaptations and are reflective of the contemporary ways in which CBT is delivered in mainstream services. More information and resources on this approach can be found at http://www.fiveareas.com/resourcearea/ (accessed June 2011). Specialist services do still exist where experienced CBT therapists adopt more traditional approaches and work with people with complex problems.
The interventions described here attempt to improve anxiety and low mood by influencing the way a person perceives and responds to specific situations. This involves conducting a thorough assessment which identifies how a recent life situation alters thinking, behaviour, emotional and physical feelings and how these areas impact on each other to lead to a problematic response. Interventions will commonly focus on changing one of these areas as a way of breaking unhelpful cycles of thoughts, feelings and behaviours. This is based on the fundamental principle of CBT which maintains that what people think affects how they feel emotionally and physically and consequently what they do. Interventions are often short term and tend to focus on a specific problem in the here and now as opposed to past life events which have contributed to the person's current issues. As a student on a mental health placement, you could be involved in delivering an intervention underpinned by this approach.
The Five Areas assessment model
The Five Areas assessment model recognises that when people are feeling anxious or low in mood their thinking can become extreme and unhelpful. For example, people may see themselves as worthless or incompetent which then leads to reduced or avoidant behaviours. The model identifies five domains within which a person's problematic thinking and behaviour can be examined, and the links between each area can be established (Williams & Garland 2002a):
Focused and specific questions are asked to explore the problematic life situation and ascertain how it is impacting on or being maintained by the remaining four areas. For example:
Area 5: altered behaviour
• What things have you stopped doing since you have been feeling this way?
• What things have you started doing to help you cope with the way you have been feeling?
(For a more extensive list of example questions, see Williams & Garland 2002a.)
This approach to assessment aims to inform interventions by identifying clear target areas for change, as making alterations in any one of the domains of the Five Areas model is assumed to lead to improvements in other areas. The model can easily be understood by service users and enables them to recognise their own patterns of thoughts and behaviours from a more objective position. Together the mental health practitioner and the service user can identify how the problem is maintained by specific thoughts, feelings and behaviours which allows them to see the potential for improvement.
The information gathered from the assessment process is summarised under the five domains in a diagram which identifies the relationship between the areas. This can be used to feed back to the multidisciplinary team so that the whole team can gain an understanding of the person's problems and adopt a consistent approach to interventions. An example of when this could be particularly helpful would be if a service user is coping with anxiety through seeking constant reassurance. You may be working with them to change this behaviour and will require other members of the team to support this intervention by not giving reassurance when the service user requests it.
Once the assessment is complete, a plan for intervention is agreed by identifying the area which is likely to have the most significant impact on the defined problem. The following interventions are examples of approaches which are commonly adopted in mental health practice.
Challenging unhelpful thinking styles
The thinking style associated with a problem or behaviour will often become extreme or unhelpful if a person is experiencing anxiety or low mood. You may hear this referred to as negative automatic thoughts, thinking errors or cognitive distortions. They tend to be consistent and lead to misinterpretation of everyday situations. There are common unhelpful thinking styles which lead people to blow issues out of proportion or downplay their ability to cope with a problem. These could include the following:
• A high level of self-criticism.
• A negative attitude towards past and current events.
• Negative predictions about the future.
• Presuming others think badly of them without evidence to suggest that this is the case.
• Feeling responsible for poor outcomes.
• Taking feedback as criticism and personalising criticism which is not directly related to them.
• Holding high standards for self which are likely to be impossible to meet.
It is important to recognise that we all hold some unhelpful thinking styles and you may be able to apply some of the examples given above to yourself at times. These tend to become problematic when these thoughts become frequent and hard to dismiss which then leads to significant levels of distress.
In the following scenario, try to identify the unhelpful thinking styles which are present.

Jane is a 38-year-old single woman who lives alone in a small flat and works as a legal secretary. She has been seeing her doctor for several months complaining of lack of appetite, feeling listless and no longer enjoying her work. After extensive tests revealed no physical health problems, her GP referred her to a psychiatrist for assessment. Although initially reluctant, Jane eventually agreed. The psychiatrist diagnosed Jane with mild depression and prescribed a course of antidepressant medication. Jane was reluctant to take the tablets and enquired whether there was any alternative. She was told about cognitive behavioural therapy which she chose to take up.
During the first meetings, Jane spoke about always feeling different and isolated from other people but things had become worse over the past few months following a date with a work colleague. Jane had never got on well with men and could see nothing in herself that men would find attractive. She had therefore resigned herself to remaining single and had arranged her life accordingly. When a colleague asked her out for a meal, she was flattered and immediately agreed. However, on reflection, she felt her decision had been hasty and was convinced he had only asked her out of pity. Her doubts were confirmed on the date when she acted clumsily and could think of nothing interesting to say. The next day at work her colleague made no attempt to ask her out again. Since that time Jane had found it difficult to talk to men and women. She felt her work colleagues were talking about her behind her back and that she was completely unlikable. She had also lost her desire to play her piano in the local church which was her main hobby.

While on placement you should try to identify these thinking styles among the service users you are working with. You may also be able to recognise them within yourself and friends and family.
Stage 1: recognising unhelpful thinking styles
Interventions which aim to challenge unhelpful thinking styles start with helping the service user to recognise them, identify the impact they have on how they feel and what they do as a response. The follow steps will guide you through this process:
1. Use the list above (p. 165) to talk about if and when the service user has noticed adopting any of these thinking styles.
2. Ask the person to describe the general situations or events when they noticed the thinking style was present. Examples might include:
3. Observe how the person's mood changes while describing the situation and ask them to discuss their current thoughts in relation to the event and how it is making them feel to talk about it.
Stage 2: investigating the thinking style
4. Ask the service user to identify a recent situation where they have felt highly distressed and explore this in depth by considering:
5. Identify together the link between the emotional and physical feelings and the thinking style.
6. Discuss what the service user did to relieve their distress and consider if this involved further unhelpful thinking styles.
(Adapted from Williams & Garland 2002b.)
Before you initiate exploring unhelpful thinking styles with a service user, it is beneficial to consider how you might respond to the questions above based on an event when you have noticed your mood altering. Once you have completed this exercise, consider the following:
1. What did you find challenging about this exercise?
2. How did you find remembering the details of the event or situation?
3. How did you find describing the distressing experience?
4. How did you find distinguishing your thoughts from your feelings?
Discuss with your mentor what you have learnt from completing the task yourself and how this might impact on the way you would broach this with a service user?
Stage 3: challenging unhelpful thinking styles
Once the service user is well practised at identifying their unhelpful thinking styles and is aware of them in day-to-day situations, you can then move onto approaches which challenge them. This is with the view to altering the way a person perceives a situation which will impact on their emotional and behavioural response. This approach is similar to that described in Chapter 13 for testing unusual beliefs and involves encouraging the person to focus on the most emotion-inducing thought (sometimes referred to as the ‘hot thought’) and considering the evidence which supports and challenges their conviction in it.
Williams and Garland (2002b) suggest the following questions can be helpful prompts for facilitating this process:
Evidence against the immediate thought
• Is there anything to make me think the thought is incorrect?
• Are there any other ways of explaining the situation that are more accurate?
• If I wasn't feeling like this, what would I say?
• Would I tell a friend who believed the same thought that they were wrong?
• What would other people say?
• Have others given me different opinions about the thought?
Based on the service user's response to these questions, you can then work together to identify a more balanced conclusion to the thought and consider what can be changed to reinforce the balanced perspective and undermine the unhelpful or extreme immediate response. This change should allow the person to test out the balanced conclusion in everyday life in order to increase their evidence against the immediate thought. It will also move the intervention to a practical task which the person is able to complete outside of the session. Evidence suggests that this is an important aspect of embedding change into day-to-day life.
If we consider the case study above describing Jane's unhelpful thinking styles, the types of changes she might consider would be based upon challenging her thoughts around how others perceive her. Therefore she would need to start by identifying the evidence for and against the thought in order to come to a more balanced conclusion. For example, Jane may conclude that her perceptions of her work colleagues are unfounded because she noticed them respond differently to her immediately and therefore they could not have known how the meal had gone. In order to test this conclusion, she may consider:
• Initiating a conversation with a work colleague to see how they respond to her.
• Confiding in a friend or colleague about her perception of the meal and asking how they might have perceived the gentleman's response the next day.
• Requesting feedback from friends or colleagues on what they value about her during informal conversation.
The outcome of the change should be discussed in depth and may involve further identification and challenge of unhelpful thoughts. The testing of unhelpful thoughts will inevitably be a difficult prospect particularly if the person is more inclined to avoid confronting the situation. It is important to recognise that change is hard and is likely to involve some discomfort. However, the therapeutic relationship can provide the safe environment for a person to take these steps provided that they are clear about the rationale and in agreement with aims of the intervention.
Overcoming reduced activity
The impact of low mood on thoughts and feelings is often a decrease in activity. This is due to a combination of unhelpful thought patterns, low energy levels and a lack in feelings of pleasure, achievement or enjoyment. This can impact on the person's day-to-day functioning as initially pleasurable activities become less of a priority and eventually essential tasks become overwhelming. The social isolation which can result from this leads to a loss of support or limits access to help from friends, family or healthcare professionals.
Interventions which aim to address decreased activity involve developing a step-by-step plan of reintroducing aspects of a person's life that they previously enjoyed or are necessary for day-to-day functioning (Martell et al 2001, Hopko et al 2003). This type of intervention is commonly known as behavioural activation. The steps outlined below are a brief introduction to behavioural activation and can inform your approach to working with service users who have decreased activity levels.
Step 1
Discuss the rationale for the intervention and ensure the service user has a clear understanding of the theory which underpins it. It may be helpful to use the Five Areas model to aid this process.
Step 2
Identify how the person is currently coping with their low mood or anxiety. For example, are they:
– adopting unhelpful safety behaviours which provide distraction, reassurance, artificially blocking of emotion or a release of emotions.
It is likely that this behaviour is acting to reinforce or maintain the problem and therefore can become the target for intervention. This information can be gathered by general conversation or by asking the person to keep an activity diary recording what they did, where the activity took place, when they did it and who they did it with, over a 1-week period. This can be a challenging task for people who are experiencing low motivation and may reinforce the perception that they are achieving very little or engaging in limited activities that they enjoy. A person's response to completing the diary will provide valuable information and will often require a level of encouragement and reassurance.
Step 3
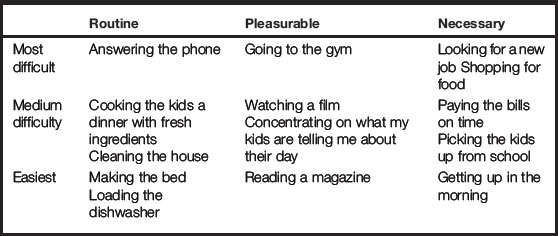
Identify activities that the service user would like to do. These may be activities that they have reduced or given up since they have experienced a change in mood. Once these activities have been listed, they should be categorised into routine, pleasurable and necessary.
Step 4
Organise the list into order of difficulty under the headings most difficult, medium difficulty and easiest. Items from each of the categories above should be included under each of the headings to ensure that activities that are necessary but most difficult are addressed. An example of how this might look is given in Table 11.1.
Step 5
Plan to implement some of the activities identified from each of the categories. Start with the easiest, small and regular activities which can provide quick success and increased motivation to tackle the more challenging activities. A specific plan should be devised to ensure that the service user is clear about what activity is scheduled, when, where and who with. The person's activity should then be recorded in a dairy to enable you both to assess the success of the plan and review it in order to set new goals.
Step 6
Jointly review the achievements in relation to the planned activity under each of the categories. Within the review, you should identify successes, problem solve any barriers to putting plans into action and discuss avoidant behaviours when plans have not been followed through.
Step 7
A return to decreased activity can occur if the person's mood drops further or they do not feel the longer term benefits of their increased activity. Supporting the person to identify early warning signs of decreased activity can help with preventing relapse. It is also essential to discuss the person's expectation of the impact of the intervention. This will involve normalising their responses and reinforcing the service user's achievements. It is unrealistic to assume that they will always feel motivated to complete necessary tasks or that pleasurable activities will always meet their expectations. Therefore it may be helpful to discuss how their reaction is similar to other people who are not experiencing a mental health problem.
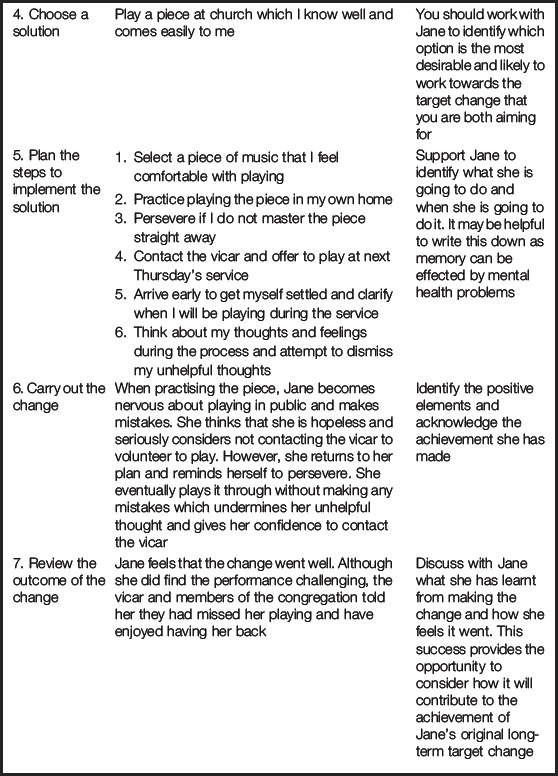
A problem-solving approach has also been advocated as a way of addressing decreased activity levels (Garland et al 2002). In the case study above describing Jane, this will involve considering the stages in Table 11.2.
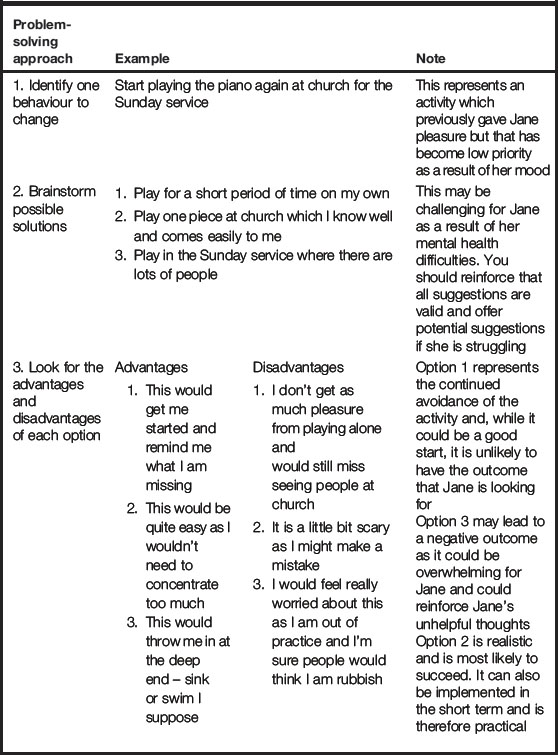
The example given in the table represents a positive outcome arising from a collaborative and well-planned approach. However, if the outcome had been less successful, it could still provide valuable learning and should not be viewed as a failure. The reasons why the plan did not go well can be discussed and a revised plan can be devised which takes into account unforeseen challenges or barriers.
The success arising from this behaviour change is likely to give Jane increased motivation to address other areas of decreased activity and continue to work towards her longer term goals. Applying the same principles will enable her to become practised at approaching problems in this way. In a problem-solving approach it is important to move at a pace that the service user is comfortable with while encouraging them to continually build upon achievements and move forward. This may involve rating the specific problems and broaching the ones which initially feel least challenging and setting time scales for when to address each area.
Overcoming increased anxiety
If a situation is feared, the body will increase levels of adrenaline to help us be alert and responsive to a potential threat. This leads to physical symptoms such as increased heart rate and hyperventilation. This response is commonly known as flight, fight or freeze. Once we feel safe again, the body calms our reactions down and helps us to return to a balanced state.
The most common approach used for helping people to overcome increased anxiety is known as exposure. This is based on the assumption that the more we expose ourselves to anxiety-provoking situations, the more able we are to cope with them. People with increased levels of anxiety will often fear everyday situations such as going to the supermarket or getting on the bus. This may be due to an unhelpful thinking pattern which is underpinning this fear or a misinterpretation of the physical symptoms of anxiety as potentially life threatening. When faced with a feared situation, the person is likely to experience anxiety almost immediately. The body experiences unpleasant physical sensations such as nausea or excess sweating that make the person feel weak. In response to these sensations the person will often attempt to leave (flight) to relieve the anxiety and physical sensations.
Alternatively, when a person is anxious they tend to avoid situations which they perceive as potentially anxiety provoking. Avoidance can be effective in the short term, however in the long term it can lead to an increased and more generalised anxiety as the person's confidence is undermined and their level of activity becomes more and more restricted. This is supported by behavioural theory described in Chapter 3. It can also maintain unhelpful thoughts as the person is not placing themselves in situations where their thoughts can be challenged.
According to conditional learning theory (described in Ch. 3), the best way to respond to these sensations is to stay in the situation long enough for the body to get used to it and to feel safe enough to let the anxiety levels drop. This will teach the body that the situation does not need to be feared and undermine the unhelpful thinking patterns which are contributing to maintaining the problematic response.
The prospect of staying in the situation may feel too challenging for some people and therefore a step-by-step approach may be helpful. This is often known as graded exposure. This requires the service user to define their overall target goal and then to identify related tasks which they can complete which will enable them to gradually develop their resilience to the feared situation. This should start with the least feared option and build up to the most feared. Some people find it helpful to rate these on a scale of 1 to 10. For example:
Least feared:
An alternative approach is known as habituation and involves staying in the anxiety-provoking situation for gradually increasing periods of time. This is particularly helpful if the person believes that their physical symptoms will continue to get worse and may lead to highly distressing outcomes such as fainting, wetting themselves or having a heart attack. The person should be encouraged to rate their anxiety levels during the period of time spent in the situation in order to map the peaks and recognise their increased resilience over time.
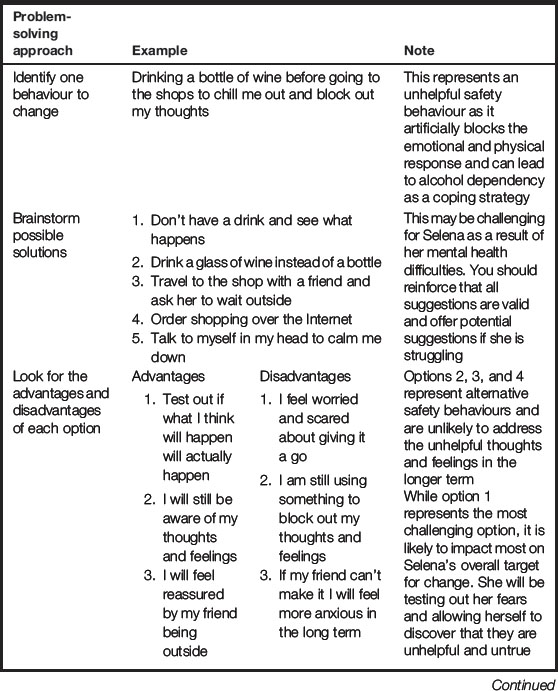
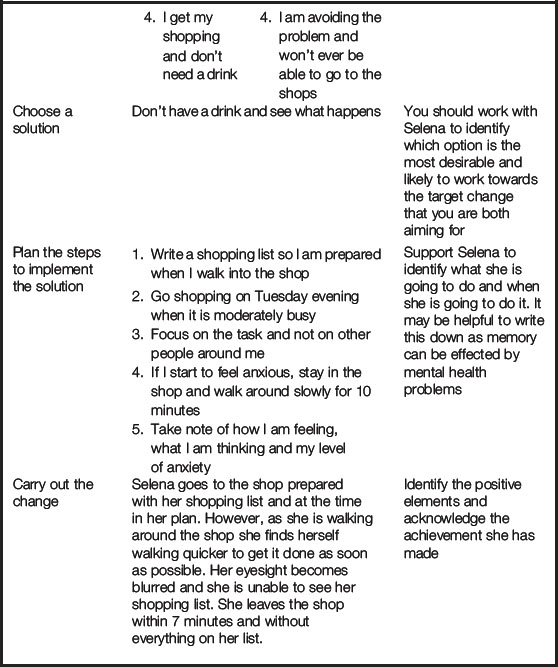
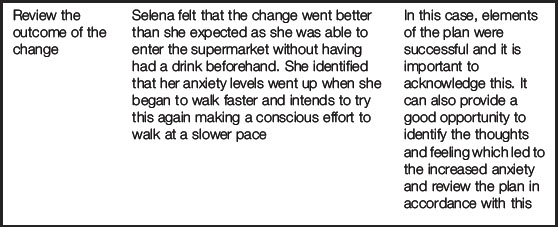
The problem-solving approach advocated by Garland et al (2002) can also be adopted for addressing avoidance or unhelpful safety behaviours arising from feelings of anxiety. Table 11.3 considers Selena's problem with drinking alcohol arising from her attempts to cope with the anxiety she experiences when in the supermarket.
It is important to identify if the person is adopting any safety behaviours to allow them to complete the task or stay in the situation without experiencing anxiety, as this will limit their exposure and prevent them from adapting to the response. For example, they might meet a friend to support them to walk to the bus stop or listen to music to distract themselves from the thoughts and physical sensations. While these may provide short-term relief, they will not address the target goal.
Each of these approaches are examples of behavioural experiments which can be carried out by the service user in between sessions. The outcome should be discussed in depth in order to review challenges, progress and continually move forward. It is also essential to identify how the evidence gained from the experiment is contributing to the evidence for and against the unhelpful thinking pattern and revisit the Five Areas assessment to consider how the associations between each area are influencing the person's progress.
1. Department of Health. Improving access to psychological therapies implementation plan: national guidelines for regional delivery. London: DH; 2008.
2. Garland A., Fox R., Williams C. Overcoming reduced activity and avoidance: a Five Areas approach. Advances in Psychiatric Treatment. 2002;8:453–462.
3. Hopko D.R., Lejuez C.W., Ruggiero K.J., Eifert G.H. Contemporary behavioural activation treatments for depression: procedures, principles and progress. Clinical Psychology Review. 2003;23:699–717.
4. Martell C., Addis M., Jacobson N. Depression in context. Strategies for guided action. New York: Norton; 2001.
Williams C., Garland A. A cognitive-behavioural therapy assessment model for use in everyday clinical practice. Advances in Psychiatric Treatment. 2002;8:172–179.
Williams C., Garland A. Identifying and challenging unhelpful thinking. Advances in Psychiatric Treatment. 2002;8:377–386.
Richards D. Behavioural activation. In: Callaghan P., Playle J., Cooper L. Mental health nursing skills. New York: Oxford University Press, 2009.
Williams C. Overcoming depression. London: Arnold; 2001.
Williams C., Richards P., Whitton I. I'm not supposed to feel like this. London: Hodder and Stoughton; 2002.
Five Areas assessment information, http://www.fiveareas.com/resourcearea/index.php (accessed June 2011).