14 Demonstrating leadership in a mental health setting
Introduction
This chapter looks at the issue of leadership in nursing practice and applies this to mental health settings through reflective learning exercises. In doing so, it considers the importance of leading care through commonly used approaches in mental health settings such as case management. Leadership, case management and partnership working are domains of competence in the Nursing and Midwifery Council (NMC) standards (NMC 2008).
Leadership
A good leader is one who is able to make things happen, to provide inspiration to others to innovate and develop practice (Williamson et al 2008). Delivering good quality care within mental health nursing involves being an effective leader. This section explores what leadership in nursing care is, examines the skills that this involves and considers some situations where you might demonstrate leadership.
Leadership in nursing can be examined from a number of perspectives. First, as Williamson et al (2008) demonstrate, it may be considered for its central role in developing and delivering quality health care and impacting positively on the lives of individuals and families who use services. Lord Darzi (Department of Health (DH) 2008) highlights that strong clinical leadership is the bedrock of empowering both staff and patients in the NHS to ensure high standards of clinical care. In this respect, leadership relates to the development of nursing practice. Kitson (2001) suggests that leadership is about making visions into reality. However, Antrobus and Kitson (1999) highlight that leadership in nursing is also about influencing the health policy that shapes the way in which health care is delivered. This involves developing nursing knowledge and influencing others at a different level, through involvement in regional and national forums, management and research. All forms of leadership involve providing a role model and support to others which helps to promote good nursing care (DH 2006a). The Chief Nursing Officer's review of mental health nursing (DH 2006b) points out that leaders are to be found at every level of an organisation.

Think of someone who you would define as a good leader. This could be someone you have worked with in mental health practice, in previous jobs or a peer. What is it that makes them a good leader? Make a list of what skills, qualities and attributes are important.
Identify how you might be able to incorporate some of these skills/attributes into the delivery of care.
It is common for people to confuse leadership and management. While they share some roles and key skills, this confusion is based on a misunderstanding of the terms and has the potential to inhibit the development of effective leadership in nursing practice. Delivering good quality nursing care involves leadership. Of course those who manage will also be required to be leaders and vice versa, yet it is important that we don't see leadership as a hierarchical concept which is only the remit of those in senior positions in health care.
There is a wealth of literature that examines the similarities and differences between leadership and management. Kotter (1990a,b) highlights that a manager's key role is in dealing with complexity while a leader's role is in creating change (Table 14.1).
Table 14.1 Leadership and management
| Leaders | Managers |
|---|---|
| Define direction Bring people together Inspire and motivate others |
Organise resources and plan Organise staff Control problems |
As a student mental health nurse, particularly during the latter part of your course, there may be a number of activities you are involved in that entail adopting the role of leader.

Make a list of the activities that you have been involved in, in mental health practice where you have shown leadership skills or acted as a leader. It may help you to think about what worked well in these situations and what didn't work so well. This can be used as the basis for a reflective piece or to develop an action plan for continuing to build on your leadership skills. It may also be helpful to revisit what you have produced in this exercise when completing job applications to help you highlight this skill and how you have used it on your practice placement.
Outlined below are a few examples of such areas and a breakdown of the skills and approaches that may assist you in developing leadership in these areas.
Key working (or co-key working)
Facilitating multidisciplinary meetings
This may share some skills with chairing a Care Programme Approach (CPA) review such as good organisational and time management skills. However, there are a few additional areas to consider:
This has provided a brief outline of some activities where as a nursing student or practitioner you may be acting as a leader. The breakdown of these areas provides some insight into the complexity of leadership in clinical care. This list is far from extensive but your involvement in such areas will help you work towards achieving your NMC competencies. The following section considers an example from mental health nursing practice where you may be asked to demonstrate leadership, both as a student and qualified practitioner, and asks you to think about some of the implications of what this involves. It is possible that you have already encountered situations which raise similar issues in your own practice. It may help to think about these in the context of the following scenarios and examine whether you would take a similar course of action again and if your experiences on your course have influenced this at all.
Scenario
Jodie is the deputy team leader on Partridge Unit. She is an experienced professional and your associate mentor. It is 10.00 a.m. and Jodie asks you to accompany her to go around the unit to let the people know that the anxiety management group is about to start. Jodie goes around every room and walks straight in without knocking.
1. What, if any, are your concerns in relation to this scenario?
2. How might the people on the unit feel about Jodie's approach?
Jodie walks into Abhid's room and wakes him up. Abhid returned to the unit at 2.00 a.m. and had disturbed sleep. Abhid shouts at Jodie and becomes angry. Jodie states she is not interested, slams the door and continues around. Jodie walks straight in to Roy's room. He has just returned from the shower and is undressed. Jodie returns to the office and tells Kirsty, a healthcare assistant new to the unit. They giggle about Abhid's reaction and Roy's state of undress.
1. What principle is Jodie disrespecting?
2. What policy and evidence is there that challenges Jodies approach?
You are deeply concerned about Jodie's behaviour. How do you react? Think about this for a moment and then pick one of the options below which most closely represents the course of action that you might take.
A. Ignore your feelings of discomfort and don't say anything.
B. Interrupt Kirsty and Jodie and say you are disgusted with what Jodie did and feel that their behaviour is completely inappropriate.
C. Tell the staff that you have befriended on the unit that you think Jodie was out of order and she doesn't know what she is doing.
D. Discuss your concerns with your mentor and ask them to have a word.
E. Discuss your concerns with your mentor, then meet with Jodie to share how you felt about how she behaved.
Option A
This may well be a common reaction. The scenario identified Jodie as a senior clinician in the team. Some students may not trust their reactions or knowledge of the situation. There may also be a fear that if you were to say anything to Jodie, this could impact on your own assessment and feedback. However, it is possible that not dealing with such feelings of discomfort and ignoring the impact they may have could contribute to the stress and perceived emotional costs of nursing. According to the NMC code, a nurse must act to promote dignity at all times and that poor care is not acceptable (NMC 2008).
Option B
This acknowledges the previous point in terms of highlighting that poor care is unacceptable. However, communicating concerns to Jodie in this manner appears confrontational and has the potential to be shared in an aggressive rather than assertive manner.
Option C
Again this option highlights that you have identified a concern with the manner in which Jodie practised in this particular situation and this may be interpreted as a means for you to access support from other people. Effective team working is supported by open communication and honesty, and reacting in this way has the potential to impact negatively on team working as resentment may build towards Jodie. It also doesn't necessarily provide a good role model for the remainder of the team.
Option D
The literature consistently links quality leadership with both the provision of support but also the need for people who are leaders to be supported (DH 2006a, 2008). This option allows you to raise your concerns about the quality of care being delivered and also gain support. This may be the most appropriate option depending on the context in which poor practice is observed and your own confidence and development.
Option E
Through sharing your views with your mentor, you are able to check out the concerns identified in option A in terms of your own understanding, knowledge and reaction to the situation. This also reflects the requirements of your competencies to participate in supervision and reflect on how your values and emotions impact on your leadership practice. However, leadership is also about maintaining standards and striving for quality. Through addressing your concerns directly with Jodie appropriately and professionally, you are also acting as an advocate for the service users and families who may be under your care. Chapter 13 includes a section on assertiveness. However, these are some suggestions for how the concerns may be broached with Jodie:
1. At the School of Nursing, we recently talked a lot about privacy and I read about essence of care. In relation to this, I was feeling a bit concerned when we didn't knock on Abhid's and Roy's doors to let them know about the anxiety group. Do you think it would have been better if we had asked before going into their rooms?
2. Thank you for your help on Tuesday and I enjoyed getting involved in the preparation for the anxiety group. However, I have not seen Abhid angry before and am a bit worried that us going straight into his room may have upset him. What do you think about how the situation was approached?
Providing constructive criticism, negative feedback or challenging someone's action is difficult at any time. There may be appropriate communication and management channels through which this is best conducted such as through appraisal or management supervision. However, as the scenario above has highlighted, there are times when it may be appropriate to provide that feedback yourself. This is important for effective leadership. As highlighted above, providing this feedback can involve the following:
• Questioning what happened and hearing the other person's side of the story.
• Considering and exploring alternative possibilities.
• Attempting to consider the person's perspective and if they had a rationale for what they did.
A leader's role in creating and managing change is particularly important within nursing (DH 2006a). This is especially relevant within the NHS. Structures and process are often in flux as the health services respond to the changing health needs of the population, developing technology, innovation and resource pressures. Brimblecombe (2009) highlights that it is important for mental health nurses to consider change in line with the values of mental health nursing and the needs and wishes of service users and their families. As a mental health nurse, you may be involved in driving and creating changes within the practice environment. However, change can be unsettling for many so you also have a key role in supporting other members of staff through this process. Changes can be particularly difficult for some people who use services. Therefore, helping the individual deal with this change will be part of leading healthcare delivery.
Williams (2004) reviewed the literature relating to leadership development in organisations and found there were some strategies that were used by effective leaders to enable change to happen. These included the following:
• Identifying others whose opinion is valued/followed in a team.
• Involving people through small groups in implementing a change.
• Developing ways for those involved to share and reflect on their experiences.
• Identifying and employing particular tools and techniques such as following an assessment, planning, implementation and evaluation cycle.
As the first part of this chapter highlighted, there are core areas of nursing practice where leadership is inherent including decision making, innovation and coordinating care. The community is increasingly offering opportunities for newly qualified mental health nurses. Working in this environment often involves working autonomously and effectively managing your own work load. One of the most common methods of organising workloads and delivering care in the community is through case management. The following section explores case management in community care and links this with leadership skills.
Case management
What is case management?
Case management is a means of adapting help to meet individuals’ specific needs by allocating responsibility for assessment and coordination of services with one individual worker or team (Oynett 1998). The core responsibilities of a case manager may be seen to generally reflect the nursing process in terms of assessment, planning, implementation, monitoring and review. There are a number of different models of case management which might structure the particular approach taken within a given team. The aims of case management are to ensure that service users are provided with the services that they need in a coordinated and effective way. Case management is one of the most common ways of leading care in mental health practice.
Case management has emerged from the growth in community-based mental health services. More recently, CPA policy identified the need to integrate the CPA with case management (DH 1999). Community nurses (alongside other professionals) will therefore be acting as care coordinators or case managers for a number of people using services at any one time.
Case management is increasingly being recognised in the wider policy relating to health care and nursing as the most valuable way of organising care delivery in the community. This literature suggests that case management involves clear decision making, articulating a rationale for decisions made and negotiating with other care providers and deliverers (including other organisations). The case management role may also include teaching others, which could be service users, families, students, junior staff or practitioners from other organisations (DH 2004). A socially inclusive approach to care management was emphasised to enable individuals to access or maintain valued roles and activities within the community (DH 2004, 2006c, 2008). Some policies acknowledge that such a role in case management might involve practice development and service improvement (DH 2006b). This is also underpinned by a greater emphasis on the opportunities for nursing leadership, through coordinating (and commissioning) care (DH 2006a).
You are most likely to encounter a case management approach when on placement with a community team such as an older persons' community team, early intervention in pyschosis team, community mental health team or rehabilitation and recovery team (see Ch. 4 for details on these services). While in one or more of these areas, talk to the team members about what they perceive are the benefits and challenges of a case management approach. Additionally, ask them about the skills that they use in order to manage the time and resources that they have for their case loads. After the discussion, consider:
1. What have you learnt from this discussion?
2. What are the implications of this for your future practice?
You might also want to think about what, if any, model of case management outlined below you have observed in the team.
Case management and mental health
Following the development of community-based services for the delivery of mental health care, a number of models of case management have been developed in mental health:
• Standard case management (brokerage and clinical case management).
• Rehabilitation orientated (strengths and rehabilitation models).
• Intensive case management (intensive and assertive models).
The different models of case management have provided some structure to therapeutic activity in specific teams. This reflects the different expectations, philosophies and skills that a professional may use within each approach. For instance, Mueser et al (1998) suggested that clinical case management has had a greater focus on providing education and psychological-based support for service users. The strengths model of case management involves working within the strengths approach, as advocated by Charles Rapp, and accessing community resources. With the possible exception of assertive outreach services within contemporary mental health care, the majority of practitioners might claim to use a number of different models or approaches to inform their practice rather than operate within a specific model of case management.
Evaluation
Case management has helped practitioners establish relationships with individuals living in the community and has therefore been shown to impact on the contact people have with services (Marshall et al 2011). Simpson et al (2003) provide a review of the literature evaluating models of case management. They highlighted some difficulties in drawing definitive conclusions about the benefits of case management due to a lack of robust research studies in the area. However, the paper suggested that the content of sessions between service users and case managers contributes to improvements in outcomes rather than the number of sessions. This is important as one of the challenges that case management has brought is the potentially large case loads that community nurses work with. This requires a practitioner to use effective organisational and time management skills as well as being able to assess, negotiate and prioritise the support both they and others provide to the people they are working with. Ryan et al (1994) found that interventions promoted by the strengths model of case management had a greater effect on promoting social inclusion and improving individuals' skills to live independently than any others.
Working with other organisations
Case management often involves working with organisations that deliver care or social support outside of the NHS. (Chapter 1 introduced multidisciplinary and partnership working in mental health care.) These organisations may be charitable, social or private and could include establishments such as housing associations, hostel providers or hospitals run by private companies. The ability to develop effective partnerships with service users, families and non-statutory organisations has been identified as an essential skill for mental health nurses (DH 2001, 2004, 2006a). There is some differentiation between partnership and interagency working. Interagency working refers to interactions between different organisations for the delivery of care. This may relate to a specific aspect of care delivery or a defined period where professionals coming from different organisations may work together towards a common goal.
Partnership working
What is partnership working?
A partnership is defined as a relationship between parties or more than one agency. The concept of partnership implies an equal relationship. In order for this to be achieved, decisions are made jointly and power is shared. Partnership working is integrated within the delivery of mental health services through the NHS and Community Care Act (1990) which created provisions for health and social care services to work together and to ensure joint working was organised at a more strategic level. Partnerships may include strategic and financial agreement at the level of the commissioning of services. It can also be incorporated into organisational structure. For instance, some trusts are jointly health and social care trusts. In order to ensure effective and efficient partnership working, structures may be joined such as one IT or joint paperwork frameworks (which includes the CPA). However, this doesn't occur in all organisations which can sometimes be a barrier to communication.
Equality can be difficult to achieve within partnerships. This is particularly evident when considering the development of partnership with service users and families where mental health professionals possess more power within the decision-making process. It can also be hard to escape the perceptions of professional hierarchies and the institutional power base that accompanies this when working with establishments outside the NHS.
Different organisations often have different unwritten codes about the way they work and this informs the organisational culture. Each agency may also have specific aims and goals which will ultimately work towards offering good quality care and support to people who use their service but these may differ in their philosophy, structure and language. Understanding and identifying these differences can be really important for a nurse working with other organisations to promote working together efficiently.
Reflecting on your practice experiences so far, identify a situation where you have been involved in decision making in mental health practice (this may be as an observer or as part of the contributions made to an individual's care). Through the development of a reflective piece, examine:
Most decisions in mental health practice, particularly in community settings, involve different professions, service users and people working for different organisations. The section above highlighted the importance of this in terms of the delivery of mental health care. Through this and the reflective exercise, some of the challenges of working in partnership have been recognised.
Effective partnership working is supported by the following:
• Understanding the role and function of teams (both your own and the team that you are working with).
• Understanding professional roles and boundaries.
• Working positively with any difference in aspiration or conflicts of interest.
• A supporting infrastructure.
Learning to work effectively with other agencies is essential within contemporary mental health services.
While on your next placement, identify agencies or organisations that your practice area works with. Make a list.
Pick two organisations and try to arrange an insight visit or opportunity to meet with one of their workers to talk through what their service provides. After this visit, think about:
1. What, if any, are the differences in how the organisation is structured?
2. What is the aim or philosophy of the service? Are there any similarities or differences with that of the NHS?
3. What challenges do the other organisations identify for working with the NHS?
4. How can effective communication between the agencies be promoted?
The activities above may help you to achieve your NMC pre-registration competencies.
Nursing careers
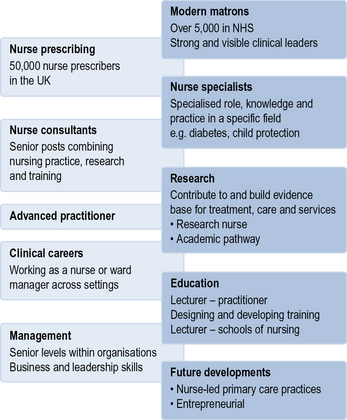
The Chief Nursing Officer's review of mental health nursing expresses a commitment to nursing careers which offer a wide range of options, including leadership, for the provision of excellent care (DH 2006b). This chapter has considered that leadership is part of delivering person-centred effective nursing care (Kitson 2001, DH 2008). However, there are opportunities within nursing to more formally develop the leadership aspect of the role. Figure 14.1 demonstrates some of the career structures that enable this. Nursing is evolving rapidly with new roles and opportunities arising. It is worth exploring the advanced and leadership roles that are linked to your service areas while on placement to keep abreast of developments and explore potential career pathways.
Antrobus S., Kitson A. Nursing leadership; influencing and shaping health policy and nursing practice. Journal of Advanced Nursing. 1999;29(3):746–753.
Brimblecombe N. Leadership and management. In: Callaghan P., Playle J., Cooper L. Mental health nursing skills. Oxford: Oxford University Press, 2009.
Department of Health. Effective care co-ordination in mental health services: modernising the Care Programme Approach. London: HMSO; 1999.
Department of Health. Journey to recovery: the government's vision for mental health care. London: HMSO; 2001.
Department of Health. Ten essential shared capabilities: a framework for the whole mental health workforce. London: HMSO; 2004.
Department of Health. Modernising nursing careers, setting the direction. London: HMSO; 2006.
Department of Health. From values to action: Chief Nursing Officer's review of mental health nursing. London: HMSO; 2006.
Department of Health. Our health, our care, our say: a new direction for community services. HMSO, London: A brief guide; 2006.
Department of Health. High quality care for all: the next stage review. London: HMSO; 2008.
Kitson A. Nursing leadership: bringing caring back to the future. Quality in Health Care. 2001;10:79–84.
Kotter J. A course for change: how leadership differs from management. New York: Free Press; 1990.
Kotter J. What leaders really do. Harvard Business Review. 1990;68(3):103–111.
Marshall M., Gray A., Lockwood A., Green R. Case management for people with severe mental disorders. Cochrane Database of Systematic Reviews. 4, 2011. Art. No.: CD000050. doi:10.1002/14651858.CD000050.pub2
Mueser K., Bond G., Drake R., Resnick S. Models of community care for severe mental illness: a review of research on case management. Schizophrenia Bulletin. 1998;24(1):37–74.
Nursing and Midwifery Council. Code of professional conduct. London: NMC; 2008.
Oynett S. Case management in mental health. London: Chapman Hall; 1998.
Ramsden P. Learning to lead in higher education. London: Routledge; 1998.
Ryan C., Sherman P., Judd C. Accounting for case manager effects in the evaluation of mental health services. Journal of Consulting and Clinical Psychology. 1994;62:965–974.
Simpson A., Miller C., Bowers L. Case management models and the Care Programme Approach: how to make the CPA effective and credible. Journal of Psychiatric and Mental Health Nursing. 2003;10(4):472–483.
Williams S. Evidence of the contribution leadership development for professional groups makes in driving their organisations forward for NHS leadership. Henley: Centre Henley Management College; 2004.
Williamson G., Jenkinson T., Proctor-Childs T. Contexts of contemporary nursing, 2nd ed. Exeter: Learning Matters; 2008.
Brimblecome N. Leadership and management. In: Callaghan P., Playle J., Cooper L. Mental health nursing skills. Oxford: Oxford University Press, 2009.
Department of Health. Modernising nursing careers, setting the direction. London: HMSO; 2006.
Department of Health. From values to action: Chief Nursing Officer's review of mental health nursing. London: HMSO; 2006.
Mental health nursing careers, http://www.nhscareers.nhs.uk/details/Default.aspx?Id=122 (accessed June 2011).
A guide to roles in mental health, http://www.mind.org.uk/help/research_and_policy/whos_who_in_mental_health_a_brief_guide (accessed June 2011).