9 Recovery from surgery
• To ensure that the student understands the need for continuing safety of the patient
• To increase students' awareness of the potential for postoperative complications
• To identify the nursing care and interventions that patients with actual and potential complications will require
• To focus on care in the postoperative recovery stage of patients who have had major surgery requiring a hospital stay
Introduction
A patient's recovery from surgery begins as soon as the actual surgical procedure is completed and the patient leaves the operating theatre. At this stage, the anaesthetist along with the team of nurses and other healthcare practitioners will be responsible for managing the immediate postoperative recovery of the patient. Once the anaesthetist in charge is satisfied that the patient has overcome the immediate effects of the surgery, he/she will decide whether the patient can be transferred safely back to their original ward.
In some cases, due to postoperative needs, the patient may be transferred to a high-dependency unit or intensive care unit. Under some circumstances, such as major chest surgery or prolonged anaesthesia, this will have been predicted and staff in those units will already be prepared to receive the patient.
This chapter focuses on two areas for postoperative recovery: the recovery room in the immediate postoperative period and recovery on the ward for the rest of the postoperative period until discharged home from hospital. Allvin et al (2006) cite studies about ambulatory (day care) surgery where these two areas are added to by a third one (what they call the late phase of postoperative recovery); ‘from discharge until the patients reach preoperative health and well-being’ (2006:553). We discuss this more fully in Chapter 10.
Care of the patient in the recovery room: immediately postoperative
The postoperative stage of patient care begins as soon as the patient is transferred from the theatre to the recovery area/room. These are normally purpose-built rooms set up with the right equipment and resources and staffed by experienced recovery room nurses. Gilmour (2010) cites the view of the Association of Anaesthetists of Great Britain and Ireland (AAGBI) ‘that patients must be observed on a one to one nurse:patient ratio until the patient has regained airway control, is cardiovascularly stable and can communicate’ (AAGBI 2002).
We can therefore identify that the nurse must focus on three areas of physiological monitoring in the immediate postoperative transfer period, namely airway, breathing and circulation. The handover from the theatre nurse/anaesthetist also includes detailed information about the patient, their surgery, their vital signs, any medication already given, any IVs in progress, any catheters or drains and any special instructions regarding their immediate monitoring and management (Gilmour 2010).
Depending on when you undertake this placement, most of you will have been taught some clinical skills in a safe environment such as a clinical skills laboratory at university. The main skills will initially be recording of temperature, pulse and respiration as well as blood pressure. These become vital skills in the immediate postoperative period, both manually and electronically where many patients are recorded by special monitors and equipment which you can observe.

Discuss with your mentor your responsibilities in the immediate care of patients in the recovery room. This is an ideal opportunity to develop not only your clinical skills but also your communication skills in a different environment. Patients are very vulnerable at this time and many will wake up worried about what has happened during surgery. Make sure you focus on learning how to communicate with patients using various senses and also communicate any concerns the patient may experience with your mentor or a qualified member of the recovery team.
Read an up-to-date evidence-based book on clinical skills and postoperative care of the patient and aim to make maximum use of materials for students in the learning environment (see Further Reading list).
Observations in the immediate postoperative period
Amos and Waugh (2007) refer to the priorities of the immediate postoperative recovery as defined by the Scottish Intercollegiate Guidelines Network (2004) as airway, breathing and circulation (see http://www.sign.ac.uk/pdf/sign77.pdf (accessed May 2011)).
Airway
The patient's airway must be kept clear at all times, and initially they may have an airway (Guedal) in place (in situ) to help keep the airway patent and to enable adequate ventilation and breathing.
It is important to ensure that the patient's position is not hampering the airway and, unless contraindicated such as in a total hip replacement where rolling onto their side is not an option, the patient can be nursed in the recovery position – on their side or supine, depending on instructions from the surgical team.
Oxygen is given immediately either with a mask or nasal cannulae, ‘normally at 40%. Contraindications include chronic obstructive airways disease or when a prescribed percentage of oxygen is required. A pulse oximeter is attached to monitor oxygen levels’ (Gilmour 2010:28).
Breathing
It is important to check that the patient's breathing is even and not noisy, which could indicate a possible obstruction, but take into account that ‘complete obstruction is characterised by silence’ (Gilmour 2010:29). It is important to check the skin colour, especially the lips and nail beds, which may indicate cyanosis. (Link this back to preoperative preparation where make up and nail varnish have to be removed – see Ch. 6.)
As well as checking for any airway/breathing obstruction and slow breathing, breathing may also become rapid and the patient might be gasping for breath. Any sudden change you observe must be reported immediately to the qualified nurse responsible for the patient and/or the anaesthetist in order that immediate remedial action can take place.
Circulation
Monitoring of the pulse and blood pressure is an essential observation and some patients will have electronic monitoring of their observations to aid you in maintaining patient safety postoperatively.
As the patient is likely to have wounds and drains, it is important that these are also checked as per instructions, obviously not disturbing any wound dressings while doing so. A dressing saturated with blood requiring additional dressings and packing is an indication that the patient may be haemorrhaging – this will be accompanied by a raised rapid pulse rate and a sudden drop in blood pressure.
If a patient has had a below-the-knee amputation, for example, the surface of the dressing may seem as if there is no increased blood loss despite physical signs of raised rapid pulse rate and dropping blood pressure. If the patient is supine, it is important to also check beneath the leg as blood may be pooling underneath, soaking the sheets rather than the dressing. This is an example from our own experience in nursing practice, with the result that the patient had to be immediately taken back to the operating theatre as a blood vessel required diathermy.
The anaesthetist will have written in the patient's notes the exact postoperative care required with regards to observations and medications, and the medication (prescription) sheet will detail specific postoperative analgesia. Managing a patient's pain is a major aspect of postoperative care, as pain can not only cause the patient some distress but also impact on postoperative physiological responses.
Pain management in the immediate recovery period
Pain is an unavoidable side effect following surgery, but how people cope with this will differ according to gender, age, psychological and cultural factors together with individual coping mechanism (Hughes 2004). The management of pain will already have been discussed with the patient preoperatively unless, of course, the patient was admitted as an emergency, when pain relief will already have commenced.
In the immediate postoperative period in the recovery room, the patient may not easily be able to articulate their pain levels, due to being drowsy or a fear of moving. Other non-verbal cues may be indicative of the need for pain relief, such as restlessness. A study by Heikkinen et al (2005) found that assessment of pain for prostatectomy patients in the recovery room was possible using pain assessment tools even though the patient may be sedated, but that there was inconclusive evidence as to which was best. They maintained that the key issue was ‘the pain is assessed systematically and that both nurse and patient understand the meaning of the assessment’ (2005:598).
Discuss with your mentor whether they use a pain assessment tool in the recovery room and, if yes, agree to use this with a patient under supervision. If a pain tool is not used, discuss why not and how the nurses know if a patient is in pain.
You may choose to consider evaluating pain assessment and management in the immediate postoperative period as a topic for an evidence-based practice assignment or as a presentation to your peers.
Analgesia can be administered via a number of different routes and techniques (Gilmour 2010, Amos & Waugh 2007). These are:
When caring for a patient either pre- or postoperatively, it is important that you familiarise yourself with all of these in order to ensure effective communication and discussion with the patient as well as ensuring evidence-based nursing care delivery. Knowing how each of these work in controlling pain should also be supported by knowing the physiological effects.
Read about the physiology of pain and make notes about the impact of surgery on the body's normal response to pain.
Determine which route for analgesia would be appropriate for a range of surgical situations.
Read Allen D (2005:133–148) (see References) to help you with this activity.
If the surgery is major, it is likely that the route of administration will be the intravenous PCA, given that this avoids use of injections and, importantly, the patient feels in control of their own pain management. The effectiveness of any pain management should be evident when the patient can move more easily and not be afraid to move, as well as being less anxious. In addition, there may be a change in the patient's observations, for example the pulse rate might have been raised and rapid before being given pain relief due to the effect of the pain stressor on the body, and this will stabilise.
Regardless of the extent of the surgical intervention, the patient will experience some degree of pain. It is important at this stage to remember that some patients may not be able to articulate that they are in pain and that physiological signs and symptoms will be the first identification. Continual observation and reassurance by the nurse is essential to the patient's wellbeing. We return to this topic again when the patient has been returned to the ward area.
Managing postoperative nausea and vomiting (PONV)
Following surgery, this remains a common complication (Gibson 2006) and is very distressing for the patient. It may add to any postoperative pain they have due to the ‘retching’ movements during vomiting and the heart rate and blood pressure may be increased (DeLeskey 2009). Anaesthetics used during surgery contribute to this postoperative problem but it can also be a side effect of strong analgesics used postoperatively such as those with an opioid base.
Monitoring the patient for other potential immediate postoperative complications
Two other main potential complications can occur in the immediate recovery period: hypothermia and wound haemorrhage (see above for one possible example affecting the circulatory system).
Wicker and Cox (2010:390) identify three possible causes of hypothermia postoperatively, namely ‘vasodilation or vasoconstriction, a recognised complication following surgery and a large infusion of blood and fluids’. Postoperatively, the patient must be kept warm and they advise that a ‘space blanket’ should be applied and that ‘the room environment should be kept at a warm temperature, above 21 degrees C’ (2010:387). However, patients must not be heated up too quickly either.
Wound haemorrhage can occur in the immediate postoperative recovery period through ‘inadequate wound closure, leaking vascular anastomosis and inadequate homeostasis’ (Wicker & Cox 2010:390) and you need to be careful to observe any wounds for signs of these. Inform your mentor immediately if you notice any signs of haemorrhage at the wound site or other indications (as discussed above) for tachycardia and hypotension.
Patients must be physiologically stable before they leave the recovery room and they must be awake and have normal airway reflexes (Wicker & Cox 2010) (see Box 9.1).
Box 9.1 Discharge from post-anaesthetic recovery
 The patient is fully conscious and can respond to voice or light touch, is able to maintain a clear airway and has a normal cough reflex.
The patient is fully conscious and can respond to voice or light touch, is able to maintain a clear airway and has a normal cough reflex.
Respiration and oxygen saturation are satisfactory (10–20 breaths per minute and SpO2 is > 92%).
The cardiovascular system is stable with no unexplained cardiac irregularity or persistent bleeding. The patient's pulse and blood pressure should approximate to normal preoperative values or should be at a value commensurate with the planned postoperative care.
Pain and emesis should be controlled and suitable analgesic and antiemetic regimens prescribed
Prior to discharge, the recovery staff should record in the notes that patients have met these criteria. If a patient does not meet these criteria, they should be assessed by the anaesthetist responsible either for the procedure or post-anaesthetic recovery with a view to upgrade to level 2 or 3 care (see full document for further details).
Discharge from the post-operative recovery room
The length of time spent in this area will depend on issues such as type of anaesthesia, type of surgery, length of surgery and the postoperative recovery of the patient. The anaesthetist will make that decision based on the recovery nurse's assessment and observations (Smith & Hardy 2007). The ward nurse will receive the handover of the patient from the recovery nurse with a complete report of the surgery, the postoperative care instructions, the current condition of the patient and any medication he/she has been given. Explanations of what is going on will be given to the patient at this time, and many patients will recognise the nurse who has come for them from the ward, especially if it is their named nurse. This is an ideal opportunity for you to undertake a patient transfer back to the ward with your mentor or another member of the ward team.
Care of the patient postoperatively: back on the ward
Once a patient has left the ward for the operating theatre, the bed area is prepared for their return. If the patient's bed has been taken to the recovery room, then he/she will be returning on that bed. The nurse collecting the patient from theatre must take with them a vomit bowl, a pair of gloves (universal precautions), a Guedal airway and a hand-held ventilation Ambu bag (or similar).
Preparation of the bed area in the ward includes checking the oxygen supply (and making sure there is an oxygen mask and proper tubing); checking the suction system/machine and its proper tubing; making sure there is equipment to take blood pressure; and, if necessary, a pulse oximeter to measure oxygen saturation levels. An IV stand may be required if a patient has undergone major surgery as they are most likely to return from the operating theatre with intravenous fluids.

For details about this and a wide range of other excellent perioperative care resources, access the CETL website at City University London:
http://www.cetl.org.uk/learning/tutorials.html (accessed May 2011).
and this linked online resource:
http://www.cetl.org.uk/learning/perioperative-care/player.html (accessed May 2011).
This site has information sheets and video/audio material on all stages of the perioperative care journey and quizzes and tests to check out your learning.
On return to the ward, the nurse takes immediate postoperative observations. Charts are used to record details of temperature, pulse and respiration, fluid balance and, depending on the nature of the surgery, other charts as appropriate.
In patients who have been admitted for day care surgery, the same observations are undertaken on the patient's return, but there will usually not be intravenous fluids to consider as patients having this kind of surgery don't require them.
All observations are recorded on the charts and in the nursing care documentation.
General principles of care in the first 24 hours postoperatively
According to Endacott et al (2009), there are key care steps in the first 24 hours postoperatively and these can be used to help focus on the priorities for the ward nurse on the patient's return from theatre. We return to these in Section 3 where we introduce you to three patients and their perioperative journeys along with learning opportunities that you can pursue in their care.
Steps for postoperative care in the first 24 hours (adapted from Endacott et al 2009)
Step 1: safe transfer and communication
This involves safe transfer of the patient from the recovery room staff to ward staff and return to the ward. Essential information has to be handed over at this time (see above). This is important in order to ensure there is effective communication between care areas but it is also important for patients to know they are going back to the ward and that the surgery is very much over.
Step 2: vital signs and consciousness
Before leaving the operating theatre, all vital signs related to airway, breathing and circulation will have been checked, and these are also checked during transfer and on immediate return to the ward. Consciousness levels are checked as well.
Step 3: early warning score systems
Many of these observations are also included in the early warning score systems (Johnstone et al 2007) which are designed as triggers to indicate a deterioration in a patient's condition. Johnstone et al (2007:221) state that:
As a result of the reduction in the number of acute beds within the NHS trusts, medical and surgical wards are now tending to have a higher number of sicker and more dependent patients … These patients are at greater risk of having a period of critical illness within these general wards and there is a growing recognition that several indicators of acute deterioration are being missed by nurses and doctors.
There are short courses and longer modules that give training in use of these early warning score systems, and Preston and Flynn (2010) identified some key points in their review of the evidence of the effectiveness and use of these tools (see Box 9.2).
Box 9.2 Review of the evidence: observations in acute care – an evidence-based approach to patient safety
1. Doing observations in acute care is crucial for detecting early signs of deterioration.
2. Nurses need a sound knowledge of physiological compensatory mechanisms to facilitate accurate detection of changes in temperature, pulse and respiration, blood pressure, blood glucose levels, neurological function and blood oxygen saturation levels.
3. Recording the respiratory rate is a sensitive indicator of clinical deterioration.
4. Early warning systems, including the Glasgow Coma Scale, are tools to aid identification of patients at risk of adverse clinical situations (cardiac arrest, raised intracranial pressure, sepsis).
5. ALERT (Acute Life-threatening Events – Recognition and Treatment) courses and simulation exercises conducted in a safe environment and development of critical thinking skills that underpin appropriate recognition and reporting of clinical deterioration.
6. Observations should be assessed by a qualified nurse if detection of patient deterioration is to be consistent in acute care.
Determine how many different tools are available in your placement which give an indication of a change in the postoperative status of patients in that area.
Set a learning goal during your placement that you will observe the use of the main early warning score system, and make a contribution to assessing the status of a patient by completing this under the supervision of your mentor.
Step 4: other observations
Endacott et al (2009) recommend checking pulse rate and blood pressure every 15 minutes for the first hour, then every 30 minutes for 2 hours. After that, the observation rate can be increased or reduced according to the patient's condition. At the same time, the skin should be observed for paleness, sweating and peripheral vasoconstriction (cold extremities). Patients who have had surgery will have surgical incisions (wounds) that will need to be observed for blood loss, and sometimes they will leave the recovery room with their external dressing marked for where the blood had been oozing through (this is undertaken carefully so as not to harm the patient). This line around the ‘blood mark’ can then be watched for any increase in size over the first 24 hours. Many surgical procedures, however, do not have large wounds so there is minimal dressing applied and minimal bleeding.
Step 5: major complications
One of the major complications to occur postoperatively is postoperative shock. Gibson (2006:921) makes the following observation with regards to this and its cause:
When the patient returns from theatre to the ward, they require frequent observations for signs of impending shock or haemorrhage. As blood pressure continues to rise, there is a continued risk of reactionary haemorrhage for the first 24 hours. Hypovolaemic shock may also occur due to a slow, continuous loss of fluid; this might be a slowly bleeding vessel or the pooling of fluid in the gastrointestinal tract during the paralytic ileus that occurs as a consequence of surgery. The loss of fluid may be detected as soakage on the dressing or blood in the wound drains, but if the patient is bleeding into a body cavity or losing fluid into the gut it may be less obvious. Distinction should also be made between hypovolaemic shock and other forms of shock, i.e. cardiogenic, septic, anaphylactic and neurogenic.
Undertaking nursing observations as prescribed in this first 24-hour period is therefore vital to detect shock and haemorrhage (see Gibson & Magowan 2011).
Find out what cardiogenic, septic, anaphylactic and neurogenic shock are. Further discussion on these is found later in this book and in the case studies in Section 3.
Patients returning after major surgery may be prescribed intravenous fluids, and sometimes a blood transfusion may be in progress. If the latter, then it is essential to undertake appropriate observations to ensure any adverse reactions to the blood are noted. Transfusion reactions can vary from a mild to a severe life-threatening situation. Symptoms range from a mild fever and pruritus to rigors, tachycardia and respiratory distress – shortness of breath due to anaphylaxis (Oldham et al 2009).
Find out the potential problems associated with a blood transfusion and visit the hospital blood bank to find out the correct procedure for checking out blood for patients. Discuss the procedure with your mentor and ask if you can participate in this activity.
The articles by Gray et al (2008) and Oldham et al (2009) will help you understand the evidence base to changes in blood transfusion practice.
The tutorial on this CETL website is an excellent resource as well:
http://www.cetl.org.uk/learning/blood-transfusion/player.html (accessed December 2011).
Fluid intake and output are also monitored. For many patients, it is difficult to pass urine in the immediate stage postoperatively, not least because many are frightened to move if they have a wound which causes them pain on movement. For some, this problem does not last very long and they will manage to pass urine. If they still haven't passed urine 4–6 hours postoperatively (but their observations regarding circulation and breathing have been satisfactory during this time), this must be reported to the medical staff. If patients have a catheter in situ then it is easier to see if they are passing urine and, most importantly, how much per hour. If the output is less than 4 ml/kg of body weight per hour, this also needs to be reported. It is essential that the function of the kidneys is maintained postoperatively.
Drainage from any wound also needs to be observed as does any fluid loss from a nasogastric tube. If excessive, this needs to be reported as well.
Step 6: pain
Levels of postoperative pain depend on the nature of the surgery and, of course, the individual patient. Whatever the type of surgery, pain levels need to be assessed and recorded and medication given. Pain assessment tools can be useful such as the ‘faces’ scale or a numerical one to rate the level of pain between 0 and 10 where 0 = no pain and 10 = worst pain imaginable (Bell & Duffy 2009).
For patients who have had major surgery, a PCA system may be prescribed and inserted in the operating theatre/recovery room and the patient may already have been made aware of having this in the preoperative phase.
Bell and Duffy (2009:156), however, in their review on the issue of pain assessment and management in surgical nursing found that ‘despite all the research carried out on pain assessment and management, very little has changed in practice’. They conclude that there appears to be two significant barriers to effective practice (although cautioned that it was a multidisciplinary issue to solve), namely ‘the beliefs and attitudes of both patients and nurses towards pain management and nurses' time management’.
Read Bell and Duffy (2009) (see References) and decide if this is a good literature review or not and whether your experience in a surgical placement of any kind can be related to their findings. Discuss with your mentor and share with others in the placement your evidence base for pain assessment and management. This is a valuable topic to explore as pain management extends beyond the boundaries of surgery and the principles of care can be applied to other contexts.
If a patient has a PCA in place, this will have been explained to them preoperatively and they will have been shown the machine. Obviously, if a patient was admitted as an emergency, this would not have been an immediate priority, so a careful explanation of what it is and how to use it will have to be completed by the nurse responsible for the patient's care both in the recovery and ward areas.
Observations of the patient using the PCA will include observing for any adverse effects such as increased sedation, respiratory depression, nausea, pruritus, urine retention and hallucinations/confusion (NHS Quality Improvement Scotland 2004).
The types of medication used postoperatively will depend on the nature of the surgery and immediate postoperative care needs, and will change as a patient progresses postoperatively. The main ones in the immediate postoperative period, if the surgery warrants it, are opioids and antiemetics. Opioids are given intravenously in the recovery room. See Box 9.3 for a description of the rationale and additional information about opioids and the use of a PCA.
Box 9.3 Providing analgesia: use of IV opioids postoperatively
‘This is the ideal route because onset of action is rapid (less than 10 minutes) which is an advantage for patients in acute pain (Scott 2009) … . The IV route of administration is preferred as absorption of an IM [intramuscular] dose may be erratic because of poor blood supply in a recovering postoperative patient. IV opioid patient-controlled analgesia (PCA) is popular in recovery since it allows the patients to titrate small doses of analgesia themselves, according to the pain they feel, giving an accurate level of analgesia. Before commencing PCA, patients require a loading dose of opioid to ensure that pain is controlled with minimal side effects (Chumbley 2009) … . Patients should be educated preoperatively so that they are aware that only they must press the bolus request button, that addiction and overdose are very rare and that the device will make a noise when they request a dose – it is not an alarm to indicate malfunction.’
(From Wicker & Cox 2010:400)
There is a large body of literature available on pain management and control both from nursing and medical professionals. Some helpful resources can be found in the Further Reading section. Further information is also considered below in the section on care after 24 hours.
Step 7: medication
In the immediate postoperative recovery period, it is important to ensure that patients are given the medication they normally take in order to avoid possible side effects from withdrawal. For example, if a patient takes insulin for long-standing diabetes, preoperative and postoperative precautions will be taken. But what happens to the patient's normal medication regimen during surgery if they are unable to eat or drink? In the case of insulin, the patient does not have to be able to eat or drink in order to receive the drug. However, with insulin-dependent diabetes, there are additional and potentially life-threatening issues to take into consideration. The patient's specific needs will be assessed preoperatively and information gained on whether the diabetes is controlled by diet, tablets (hypoglycaemic) or insulin. It may be that a combination of these is being used. It is also important for the anaesthetist to find out whether the patient is suffering from any of the complications of diabetes, such as hypertension, peripheral vascular disease or renal problems, all of which influence the choice of anaesthetic and mode of anaesthesia. Generally, most patients who have diabetes are scheduled to be first on the operating list whenever possible and medication is continued as far as possible on the day of surgery. Following admission to hospital, the patient's sugar level will be monitored closely. See the CETL website for information on how to monitor blood glucose levels: http://www.cetl.org.uk/learning/blood-glucose-monitoring/player.html (accessed June 2011).
Find out from the literature, ward protocols and other information what the pre- and postoperative requirements are for a patient who has diabetes and is insulin dependent.
Identify key areas of pre- and postoperative care and devise a care plan for a patient going for surgery who cannot eat or drink for at least 24 hours postoperatively and 6 hours preoperatively. The information in Box 9.4 will help you with this care plan.
Box 9.4 Diabetes, insulin and perioperative care
General measures for diabetic patients
Regularly monitor blood sugar until the patient's routine is back to normal – eating and drinking normally and taking their usual insulin or oral hypoglycaemic agents. Frequency of blood glucose measurement will depend on the exact situation and trends exhibited by the patient but generally should be done 1–2 hourly preoperatively with increased frequency if the situation is not stable.
Do not discharge any patient home unless certain that the blood sugar is controlled and the patient is able to manage their diabetes.
Hypoglycaemia is an important and life-threatening complication. It may be defined as blood sugar less than 4 mmol/L. It is usually caused by an imbalance of too little food versus too much insulin or oral hypoglycaemia. It may present with sweating, tachycardia, agitation or confusion, fits or unconsciousness. Many diabetic patients will recognise impending hypoglycaemia and will take action to avoid it. If able to eat and drink, give a glass of Lucozade or juice (non-diet) followed by a sandwich or toast. If glucose is less that 2, or the patient is confused, difficult to rouse or unconscious then call immediate medical help. Give 20–50 ml of 50% dextrose IV (repeated if necessary). If the patient is unconscious, attend to the basics of airway, breathing and circulation. If IV access is not available, give glucagon 1 mg intramuscularly.
Any diabetic patient undergoing prolonged fasting (more than one missed meal) requires glucose–potassium–insulin (GKI) or sliding scale management. GKI has been shown to provide better glycaemic control than the sliding scale.
Important note: It is not the responsibility of the student nurse to give the medication specified in this extracted guidance – but you may observe the practice and certainly be able to recognise when a diabetic patient requires professional help. It is important to note that the information here is for general care of any diabetic patient and not for the postoperative period when additional care is required, especially for those taking insulin. The sliding scale refers to the giving of insulin and/or dextrose and potassium separately on a sliding scale of dosage depending on blood glucose levels.
(Adapted from NHS Forth Valley 2009)
Access the CETL website for more information on blood glucose monitoring:
http://www.cetl.org.uk/learning/blood-glucose-monitoring/player.html (accessed December 2011).
Step 8: maintaining observations
It is important to maintain observations as per postoperative instructions, the nature of the surgery and progress of the patient. An increase in pulse and lowering of blood pressure might be caused by blood loss or haemorrhage, possibly due to a blood vessel not being ‘tied off’ or ligated during surgery. This requires a return to the operating theatre. Other indications of excess bleeding could be restlessness and cold and clammy skin in addition to the changes in pulse and blood pressure.
Temperature observation is important in the immediate postoperative period, especially for patients who have had major thoracic or abdominal surgery, due to ‘prolonged surgery and exposure of thoracic or abdominal contents resulting in significant loss of body heat’ (Torrance & Serginson 1999:58).
Observation of respiration rate could show early indication of hypoxia or lack of oxygen, requiring an increase in oxygen given or commencement of oxygen therapy via nasal cannulae or face masks. It is important, however, to note that this is not possible for patients who have chronic obstructive airways disease (COAD) because such patients are used to ‘a low concentration of oxygen for their respiratory drive and in such cases an oxygen concentration that is too high can depress ventilation’ (Torrance & Surginson 1999:58).
It can be seen from this brief insight into postoperative observations the importance of understanding normal physiology in order to understand what happens when changes occur.
Ensure that you read your notes on the normal physiology of body systems prior to your clinical placement and work out what happens if, for example, there is severe and sudden blood loss, or a patient develops a high temperature. Examples of books to read can be found in the Further Reading list. Read the experience of a student nurse whilst on clinical placement and what he learnt about the importance of observations: http://nursingstandard.rcnpublishing.co.uk/students/clinical-placements/professional-development/clinical-learning-curves/appearances-can-be-deceptive-with-a-post-operative-patient (Accessed June 2011)
Step 9: infection control and prevention practices
Preventing infection is one of the most important postoperative care activities, and as such all personnel involved in patient care need to adopt effective and protocol-driven handwashing practices as a normal day-to-day activity rather than just as part of an aseptic technique (see Ch. 8 for handwashing practice in the operating theatre).
Bennallick and King (2009:47) state that ‘infection prevention and control can be defined as a series of strategies and practices that aim to reduce the risk of infection to staff, patients and others where care is delivered’. They point out a number of essential skills that they believe help prevent the transmission of organisms which are associated with healthcare-associated infections, namely (2009:47):
The Department of Health (DH 2010) introduced a new code of practice in 2010 on the prevention and control of infections in health and social care that was implemented on 1 April 2011.
Access this report and consider the implications for organisations such as hospitals and the perioperative environments.
http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_122604 (accessed June 2011).
The consequences of healthcare-associated infection are discussed in this learning resource from CETL:
http://www.cetl.org.uk/learning/healthcare_associated_infections/player.html (accessed June 2011).
Many hospitals had already adopted principles of good practice in the use of antibacterial handwashing gels, with stations placed strategically to ensure that not only staff use these gels but also the general public visiting the hospital environment. Antibacterial handwashing
Make a plan to learn how to develop your competence in each of the areas in the bullet list above. A good clinical skills nursing book can help you with the steps involved, as can the simulated learning environment of the clinical skills laboratory.
Check out the following CETL links for helpful information on some of these practices:
Use and disposal of sharps: http://www.cetl.org.uk/learning/sharps-disposal/player.html (accessed June 2011).
Aseptic technique (also includes disposal of waste and putting on sterile gloves): http://www.cetl.org.uk/learning/aseptic-dressing-technique/player.html (accessed June 2011).
If you have already had experience in the operating theatre, you will have gained skills in putting on gloves, disposing of sharps, dealing with spillages and waste disposal, as well as practising a very specific technique for handwashing. The websites above are excellent resources for learning and testing knowledge on a range of topics connected to a surgical nursing placement as well as other placements you may be allocated to during the course of your study.
gels can also be bought in supermarkets and many people now carry them as part of normal day-to-day practice.
Step 10: essential care in the immediate postoperative period
It is important to ensure that all essential personal care is given postoperatively, but ensuring that specific postoperative instructions relevant to the surgical intervention are not compromised in the process.
One of the problems for patients postoperatively is a dry mouth, caused by not drinking and/or perioperative medication which causes lack of saliva. Maintaining good oral hygiene is essential for the wellbeing of patients until they are able to do this for themselves. If a patient has dentures and is fully conscious, ensure they are cleaned before inserting into the mouth and, if nauseated, the patient may choose to wait until they feel better before wanting them in. Sometimes it helps to have their dentures in so they can speak clearly and be understood. If in doubt about inserting them during the first 24 hours postoperatively, check with a qualified member of staff. The articles by Huskinson and Lloyd (2009) and the Royal College of Nursing (RCN) (Heath et al 2011) (see References) discuss the importance of oral health for patients.
Depending on the severity and nature of the surgery, patients may wish to have their own night clothes to replace their surgical gowns. A wash of the hands and face is also welcomed by many patients if they are fully conscious, making them feel refreshed and ‘normal’ again.
Care of the patient after the first 24 hours postoperatively
The majority of steps highlighted above will continue in one form or another until the patient's discharge home from hospital. We can, however, focus on key postoperative care issues in this section that will help you to care for a patient who has undergone surgery. It is not possible to focus on specific types of surgery here, but we consider broad areas in Section 3 where the principles of practice are considered in more specific contexts and for different types of surgical intervention. We can consider these as actual and potential problems that patients may experience in the postoperative period. Obviously, for patients admitted for emergency surgery, some of these problems become more acute and require more urgent attention. Refer to Chapter 2 for additional material on the following topics, especially the problem-solving exercises.
Re-visit the CETL programme perioperative care resource at:
http://www.cetl.org.uk/learning/perioperative-care/player.html (accessed December 2011).
This includes every stage of the perioperative period and postoperative observations.
Actual and potential problems postoperatively: principles of practice
Management of pain
Pain at some level is a consequence of surgery, the level of pain being dependent on the individual and their tolerance to pain and also to the type and extent of surgery experienced. The physical pain a nurse anticipates a patient will experience from surgery such as removal of the gall bladder via microscopic surgery may be different from the pain she will anticipate a patient may have following major thoracotomy and oesophagectomy. However, as we know, this is not how it may work out in the reality of practice. Consider this quote from McCaffrey (1979:3):
… pain is a subjective experience – the person who helps the patient with pain cannot see or feel what is being treated. Further, psychosocial factors influence responses to pain and even the existence of pain to such an extent that two people exposed to the same potentially painful stimulus may react in opposite ways. Add to this the lack of knowledge about what causes the pain and what may relieve it. Unsurprisingly, the result often is one of disagreement among health professionals and between practitioner and the patient with pain.
Given that McCaffrey wrote this in 1979 (second edition of her classic work from 1972), does her observation still resonate with today's clinical practice? How often have you heard qualified nurses say to patients ‘but you can't be in pain, you had pain relief 2 hours ago and are not due any more for another 2 hours at least’ or the discussion between nurses on the dangers of patients becoming addicted to strong pain relief?
Discuss with your mentor their views on pain management. Consider the various ways in which patients cope with pain in your placement area and consider what the main differences involved in the surgery itself, the medication prescribed and the patient's concerns about pain relief were.
If you can obtain a copy of either McCaffrey's 1972 or 1979 book Nursing Management of the Patient with Pain, consider how her assertions on all aspects of pain management have changed over time. Obviously some of the medication has changed and there is additional research evidence available.
Assessing a patient's pain and managing the pain by various means is one of the main roles of the nurse postoperatively (see Ch. 2).
Management of fluid and electrolyte balance
If a patient has had major surgery, it is likely that he/she will have an intravenous infusion postoperatively in order to replace fluid loss and also prevent dehydration when fluid intake may be restricted and the patient may also not be eating immediately. This requires careful monitoring in terms of the prescribed regimen and for any signs of inflammation at the site of the cannula (Scales 2008). Many patients will also be receiving medications via this infusion. See Box 9.5 for good practice to reduce infection in intravenous therapy. This guidance, however, is for qualified nurses, but if you are a member of the nursing team caring for a patient with an infusion postoperatively, you will undertake many observations related to this good practice alongside your mentor.
Box 9.5 Good practice to reduce infection in intravenous therapy
Wash hands, wear a new pair of non-sterile disposable gloves and use an aseptic non-touch technique for all aspects of IV therapy, including preparation, administration and site care.
Prepare IV fluids and drugs in a designated clean area.
Use pre-mixed solutions and avoid additives to the fluid bags if possible.
Ensure all IV fluid containers are labelled with the date and time they are opened and discard within 24 hours.
Ensure all IV administration sets are labelled with the date and time and change them appropriately: solution sets – change at 72 hours; blood sets – change at 12 hours; lipid-contaning solutions – change at 24 hours.
Administration sets that are disconnected should be discarded.
Add-on devices should be kept to a minimum and changed as recommended by the manufacturer. In general, three-way taps should be changed every 72 hours, bungs (single use, or change at 72 hours if not removed from device) and needleless devices should be changed according to manufacturers' instructions.
Needleless devices should replace the use of bungs to maintain a closed IV system.
All administration ports should be thoroughly decontaminated with 2% chlorhexidine in 70% alcohol and allowed to dry prior to use; they should also be cleaned after use.
IV dressings should be replaced when loose, wet or soiled.
Central vascular access device (VAD) insertion sites should be inspected twice a day and any signs of infection should be reported.
(From Scales 2008:10)
Management of postoperative nausea and vomiting
Postoperative nausea and vomiting (PONV) is also a problem for some patients and can cause stress, discomfort and additional pain (Gilmour 2010). Patients may be responding to the type of anaesthetic given during surgery, postoperative pain or the postoperative pain relief itself. Whatever the cause, it requires immediate response from nurses, something that Jolley (2000) found did not always happen. A more recent audit undertaken by DeLeskey (2009:141) examined whether or not ‘best practice based on best available evidence for the management and treatment of PONV’ was taking place. She found that change in practice was required in a number of areas, based on the six criteria she had selected for the audit (see Box 9.6).
Box 9.6 Six criteria to determine best practice in management and treatment of PONV
1. PONV risk factors are identified and documented before surgery.
2. PONV risk factors are communicated to the anaesthetic/surgical team before surgery.
3. Appropriate PONV treatment is ordered to be given as needed postoperatively.
4. Appropriate PONV prophylaxis is administered as indicated by risk factors.
5. Routine assessment for PONV occurs postoperatively.
6. Appropriate PONV rescue treatment is initiated as needed.
(From DeLeskey 2009:141)
Discuss with your mentor what the current practice is for the management of patients who experience postoperative nausea and vomiting. Use the criteria in Box 9.6 as the basis for this discussion. Observe during your care of postoperative patients how many patients experience nausea and vomiting postoperatively and how it was managed by the surgical team.
Obtain a copy of Jolley (2001) (see References). Read it prior to starting your clinical placement. The article includes a number of ‘Time Out’ questions for the reader as part of continuing professional development. These include some questions related to risk factors and use of antiemetics. Try to answer the questions while reading the article. (If you subscribe to this journal, it also enables you to access a number of resources online which are related to surgical nursing in general).
The management of postoperative nausea and vomiting requires the involvement of the whole surgical team. Ensuring accurate recording of any vomiting together with observation of volume, colour, frequency and timing, however, is the responsibility of the nurse in the team, as is reassuring patients and relieving any distress they may experience. Ensuring you are aware of the evidence-based risk factors as well as the management of PONV enables you to enhance your nursing care of patients in the perioperative period. It is important to note that every patient and various surgical procedures will require a specific response and management, some of which are considered in the case studies in Section 3.
Management of nutrition
Depending on the type of surgery a patient undergoes, as well as their nutritional status when admitted to hospital, managing postoperative nutrition needs is an essential part of a nurse's role. It has been found that many elderly patients, for example, experience malnourishment during a stay in hospital, due in part to a lack of risk assessment or adequate monitoring of what they are eating (see RCN (2009) for an excellent guide to nutrition and older people).
Field and Bjarnason (2002:42) point out the importance of preoperative nutritional assessment and nurses' actions required for patients after abdominal surgery:
Nutritional assessment of ill patients anticipating major surgery is crucial, as deterioration of nutritional status is one of the key factors in surgical outcome. It is important, therefore, to obtain on admission weight, height and BMI [body mass index] score. This assessment can highlight those patients who are underweight and vulnerable on admission. This simple assessment can alert the surgeon to potential postoperative problems. The help and advice of the dietician or nutrition team can then be sought at an early stage.
Obtain a copy of Field and Bjarnason (2002) and compare the practice on your placement with that in the article. Ensuring adequate nutritional intake is as important for day surgery or ambulatory care as it is for major surgery, either planned or emergency.
After major surgery, many patients return to the ward with an intravenous infusion in place in order to ensure adequate and appropriate fluid and electrolyte replacement as well as nutrients essential for postoperative healing and nutrition. The British Association of Parenteral and Enteral Nutrition has developed guidelines for intravenous fluid therapy for adult surgical patients, which includes some basic information regarding the links between physiology and management of patients perioperatively and evidence-based guidance on postoperative fluid and nutrition management (see http://www.bapen.org.uk/pdfs/bapen_pubs/giftasup.pdf (accessed December 2011)).
Management of infection control
Infection control issues have been discussed in Chapters 1–4 in relation to preparation prior to practice placement experience. It is recommended that you re-visit that section as well as the Nursing and Midwifery Council (NMC) essential skills cluster on infection prevention and control.
Postoperatively, the prevention of infection becomes a major nursing management task. It is directly linked to the management of wounds and wound care, but we also need to consider it in the broader context of hospital-acquired infections.
Depending on the type of surgery, you will see many different kinds of wounds, a variety of wound closure techniques, some with wound drains, and a variety of different wound dressings. These are known as surgical wounds, i.e. they are deliberate incisions in the skin which also impact on underlying structures and are usually performed in a clean environment where asepsis is maintained at all times (Pudner 2010). Wound care management postoperatively is aimed at promoting healing and preventing infection (Gibson 2006), and Pudner (2010) identifies five principles of surgical wound management (see Box 9.7).
Examples of different kinds of suturing techniques and drains can be seen in Figures 9.1–9.6.
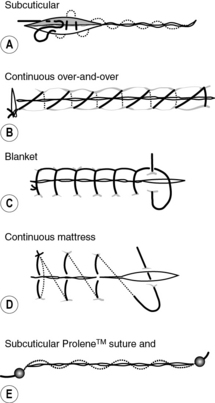
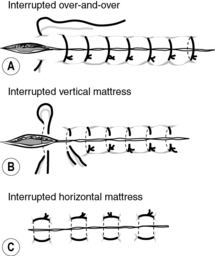
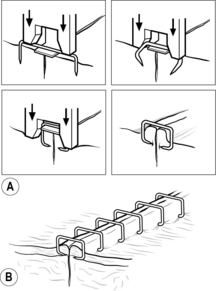
Fig 9.3 (A) Formation of skin staples. (B) Skin staples in situ
(reproduced with permission of Ethicon Ltd)
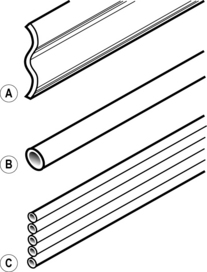
Fig 9.4 Types of passive drain: (A) Corrugated; (B) Penrose; (C) Yeats
(reproduced from Pudner (2010) with permission)
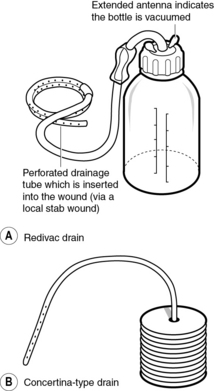
Fig 9.5 Types of active drain: (A) Redivac; (B) Concertina type
(reproduced from Pudner (2010) with permission)
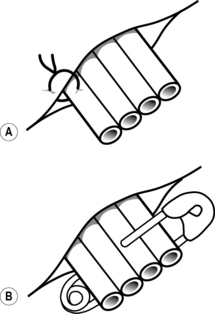
Fig 9.6 Methods of securing a passive drain in place: (A) Yeats drain secured in place with a suture; (B) Yeats drain secured in place by a safety pin
(reproduced from Pudner (2010) with permission)
During your clinical placement, make a list of all the types of wound closure techniques you have seen and ask your mentor if you can first observe the removal of sutures/clips/drains, then gain experience in undertaking this yourself.
When to remove these is dependent on the surgeon's practice and/or the healing progress made by the patient.
Paper to read prior to placement:
Chapter 5 in Pudner (2010) (see References) for further information. It includes an explanation of the knowledge of physiology and how the skin works, which is essential to an understanding of wound healing and infection prevention.
A question often asked is: How do we know if a patient has a wound infection? Reilly (2002) offers the following definition, citing Emmerson et al (1993):
A wound infection should have either a purulent discharge in, or exuding from, the wound, or a painful erythema indicative of cellulitis. Infection should also be considered to be present when there is a fever (> 38°C), tenderness, oedema and an extending margin of erythema, or the patient is still receiving active treatment for a wound which has discharged pus.
It is important that students can undertake aseptic technique, regardless of what type of clinical placement they are undertaking. Watch the video of this technique at the CETL website: http://www.cetl.org.uk/learning/aseptic-dressing-technique/player.html (accessed December 2011).
You may also have similar skills videos at your university – check out the information on your virtual learning environment (such as BlackBoard).
Of course, with many patients now being discharged home from hospital earlier than in the past and after any kind of surgery, the role of the hospital nurse in removal of sutures has altered because this role now belongs to the community health nurse. If you are following a patient pathway or placement learning experience where one of the perioperative areas is your main base or hub, it is a good idea to discuss with your mentor the possibility of visiting a patient you have been caring for once they are discharged home (see Ch. 10).
Personal cleansing and dressing
Personal cleansing and dressing are very important for all patients, in particular the need for correct and appropriate skin care postoperatively. Many patients undergoing surgery are elderly and therefore have additional needs that younger patients don't have.
The symposium paper by Deshi (2010) offers an insight into some of the issues facing the care of elderly patients with co-morbidities (multiple diseases) and weak physiological strength. The paper also focuses on the value of a multidisciplinary approach to caring for an older person undergoing surgery.
Obtain a copy of this paper online and consider its findings for patients in hospital and in the community:
http://www.rcpe.ac.uk/journal/issue/journal_40_4/dhesi.pdf (accessed December 2011).
Older patients, especially those who have multiple health problems, are at risk of developing pressure sores as well, especially if they do not mobilise quickly following surgery. Their skin may be less strong than when they were younger and they may also be on medication which may add to the problem. A preoperative assessment will identify those patients at risk.
Care of the mouth is also important, especially if patients are unable to eat or drink postoperatively, and there is a potential for mouth infections to occur. Some postoperative medications can also cause a dry mouth, especially steroids or oxygen therapy.
Other general personal cleansing and dressing issues involve different cultural and religious needs in relation to postoperative care, and maintaining the dignity of the patient.
A useful document has been published by the Association for Perioperative Practice (AfPP) on this very topic (AfPP 2007). This includes guidance on skin assessment in the perioperative environment, including assessing for cyanosis in darker skin.
Mobilising
Movement is encouraged postoperatively according to the nature of the surgery and the patient pathways for certain health problems (conditions). Apart from the potential to develop pressure ulcers and chest infections, there is the added potential problem of the development of deep vein thrombosis and/or a pulmonary embolism (see the National Institute for Health and Clinical Excellence (NICE 2010) guidelines at: http://www.nice.org.uk/CG92). Patients are mobilised according to the nature of their surgery: an elderly patient, for example, with a fractured femur who has been to theatre for a ‘pin and plate’ will be mobilised very differently to someone who has had an above-the-knee amputation or a total hip replacement.
Consider the practice in your clinical placement with regards to mobilisation of patients postoperatively. If it is an orthopaedic ward, for example, make a list of all the various types of surgery or care given to patients and discuss with your mentor how each patient is normally mobilised after surgery.
Elimination needs
There is a change in patterns of elimination postoperatively, and even patients who have been admitted for ambulatory or day care surgery may stay in hospital because they are unable to pass urine postoperatively and may need catheterisation.
Most patients returning from the operating theatre do not have a catheter in place, but for some types of surgery this is an automatic practice. Examples are major gynaecology surgery, major abdominal surgery or genitourinary surgery.
It is important for patients to pass urine postoperatively to avoid being catheterised and to prevent risk of urinary tract infection.
Urinary retention can be caused by opioids given for postoperative pain, as they act on the bladder's voiding reflex (Kitcatt 2010). They can also cause constipation because they ‘delay gastric emptying and reduce the propulsive contractions in the gut’ (Kitcatt 2010:115).
Paralytic ileus is also a potential problem for patients, especially after major abdominal surgery or surgery to the gastrointestinal tract. It is a term used to describe stasis within the bowel. When the bowel is operated on, the nerve pathways are interrupted, which can result in the temporary loss of peristalsis (Felstead 2007). This means that patients are unable to eat or drink postoperatively as planned due to their bowel not working properly. In cases where there is a paralytic ileus diagnosed, ‘the surgical team will listen for bowel sounds on a daily basis and usually commence the patient on small amounts of water gradually building up to free fluids and full diet over a number of days’ (Felstead 2007:155).
Holland et al (2008) cite Brown's (2002) criteria for determining successful outcomes of postoperative care, which are given in Box 9.8.
Box 9.8 Determining successful outcomes of care postoperatively
1. The patient is free from pain and discomfort, as shown by verbal expression and participation in physical activities and ability to rest and sleep.
2. The fluid intake and electrolyte concentrations are normal for the patient.
3. The patient is taking a nutritionally balanced diet.
4. Urinary and bowel elimination are re-established and normal for the patient.
5. The patient is ambulatory, active and participating in care.
6. The incision is clean, dry and intact.
7. Vital signs are normal for the patient.
8. No manifestations of complications are present.
9. The patient and family demonstrate an understanding of the required care during convalescence and the resources available.
(From Holland et al 2008, citing Brown 2002:190)
Depending on your placement, consider the variance from this standardised list of criteria and what care took place to achieve these outcomes. Discuss as a learning goal with your mentor.
For the majority of patients, this is a normal pattern in terms of measuring a successful postoperative period. Those who develop some of the complications mentioned in this section recover from them, but obviously there are occasions when patients die postoperatively. This may be due to some postoperative complications or to a previously undiagnosed problem which may have led to a cardiac arrest, for example, either in the operating theatre or when returned to the ward.
All surgery carries risk, but if the preoperative assessment has been effective in identifying potential problems and the postoperative care has been managed well and underpinned by an evidence base, then these risks are minimised. The majority of patients are then discharged home from hospital.
Discharge home from hospital
In brief, as this is discussed fully in Chapter 10, planned discharge begins prior to or on admission of the patient for either minor or major surgery. Other agencies may well have to be contacted and follow-up appointments organised. Patients are now discharged home into the care of their GP and the district nursing team. The reduction in hospital stays postoperatively has meant a shift in what happens to patients and their care, with community nurses taking over many postoperative care procedures and continuing to observe for postoperative complications which can still occur and may result in the patient being re-admitted to hospital.
Summary
This chapter has given you a brief insight into the postoperative care of the patient. Given the number and variety of surgical interventions, the presentation has been mainly generic. More explicit examples are explored in Section 3.
Many of the issues discussed here will support your development and achievement of the NMC Essential Skills and Standards for becoming ‘fit for practice’ as a nurse. We return to these in Section 4 when we look at future learning needs, testing what you have learnt through this book and also looking forward to other placements and what you can continue in your ongoing record of achievement (NMC 2010).
Allen D. Sensory receptors and sense organs. Montague S., Watson R., Herbert R.A. Physiology for nursing practice, 3rd ed., Edinburgh: Elsevier, 2005. 133–148
Allvin R., Berg K., Idvall E., Nilsson U. Postoperative recovery: a concept analysis. Journal of Advanced Nursing. 2006;57(5):552–558.
Amos A., Waugh A. Caring for the person having surgery. In: Brooker C., Waugh A. Foundations of nursing practice. Edinburgh: Mosby, 2007. 681–702
Association for Perioperative Practice. Respecting cultural diversity in the perioperative setting. Harrogate: AfPP; 2007.
Bell L., Duffy A. Pain assessment and management in surgical nursing: a literature review. British Journal of Nursing. 2009;18(3):153–156.
Bennallick M., King D. Infection prevention and control, essential skills 4.1. In: Endacott R., Jevon P., Cooper S. Clinical nursing skills – core and advanced. Oxford: Oxford University Press, 2009.
Brown A. The patient undergoing surgery. Walsh M., ed. Watson's clinical nursing and related sciences, sixth ed., London: Baillière Tindall/Royal College of Nursing, 2002. 65–192
DeLeskey K. The implementation of evidence-based practice for the prevention/management of post-operative nausea and vomiting. International Journal of Evidence-Based Healthcare. 2009;7:140–144.
Department of Health. The Health and Social Care Act 2008: code of practice on the prevention and control of infections and related guidance. London: DH; 2010.
Deshi J. Improving outcomes in older people undergoing elective surgery (symposium review). Journal of the Royal College of Physicians. 2010;40:348–353.
Emmerson A.M., Ayliffe G.A.J., Casewell M.W., et al. National prevalence survey of hospital acquired infections. Journal of Hospital Infection. 1993;24:69–76.
Endacott R., Jevon P., Cooper S. Clinical Nursing skills – Core and Advanced. Oxford: Oxford University Press; 2009.
Felstead I. Surgery of the lower gastrointestinal tract. In: McArthur-Rouse F., Prosser S. Assessing and managing the acutely ill adult surgical patient. Oxford: Blackwell, 2007. 145–157
Field J., Bjarnason K. Feeding patients after abdominal surgery. Nursing Standard. 2002;16(48):41–44.
Gibson C. The patient facing surgery. Alexander M., Fawcett J.N., Runciman P.J. Nursing practice hospital and home: the adult, 3rd ed., Edinburgh: Churchill Livingstone, 2006.
Gibson C., Magowan R. The patient undergoing surgery. Brooker C., Nicol M. Alexander's nursing practice, 4th ed., Edinburgh: Churchill Livingstone, 2011.
Gilmour D. Perioperative care. Pudner R., ed. Nursing the surgical patient, 3rd ed., Edinburgh: Baillière Tindall, 2010. 17–34
Gray A., Hart M., Dalrymple K., Davies T. Promoting safe transfusion practice: right blood, right patient, right time. British Journal of Nursing. 2008;17(13):812–817.
Heikkinen K., Salantera S., Kettu M., Taittonen M. Prostatectomy patients' postoperative pain assessment in the recovery room. Journal of Advanced Nursing. 2005;52(6):592–600.
Holland K., Jenkins J., Solomon J., Whittam S. Applying the Roper, Logan and Tierney model in practice. Edinburgh: Churchill Livingstone; 2008.
Hughes S. Principles of post-operative patient care. Nursing Standard. 2004;19(5):43–51.
Huskinson W., Lloyd H. Oral health in hospitalised patients: assessment and hygiene. Nursing Standard. 2009;23(36):43–47.
Johnstone C.C., Rattray J., Myers L. Physiological risk factors, early warning scoring systems and organizational changes. British Association of Critical Care Nurses, Nursing in Critical Care. 2007;12(5):219–224.
Jolley S. Post-operative nausea and vomiting: a survey of nurses' knowledge. Nursing Standard. 2000;14(23):32–34.
Jolley S. Managing postoperative nausea and vomiting. Nursing Standard. 2001;15(40):47–52.
Kitcatt S. Concepts of pain and the surgical patient. Pudner R., ed. Nursing the surgical patient, 3rd ed., Edinburgh: Baillière Tindall, 2010.
McCaffrey M. Nursing management of the patient with pain. Philadelphia: J B Lippincott; 1979. 2nd ed.
NHS Forth Valley. Management of adult patients with diabetes undergoing elective surgery. Falkirk: NHS Forth Valley; 2009.
NHS Quality Improvement Scotland. Postoperative pain management. Edinburgh: NHS Scotland; 2004.
Nursing and Midwifery Council. Standards for pre-registration nursing education. London: NMC; 2010.
Oldham J., Sinclair L., Hendry C. Right blood, right patient, right care: safe transfusion practice. British Journal of Nursing. 2009;18(5):312–320.
Preston R., Flynn D. Key points from a review of the evidence: observations in acute care: evidence-based approach to patient safety. British Journal of Nursing. 2010;19(7):442–447.
Pudner R. Nursing the surgical patient, 3rd ed. Edinburgh: Baillière Tindall; 2010.
Reilly J. Evidence-based surgical wound care on a surgical wound infection. British Journal of Nursing. 2002;11(16):S4–S12.
Royal College of Nursing. Nutrition and older people: essential guide. [Online. Available at:]. RCN: London, 2009. http://rcn-library.rcn.org.uk/uhtbin/cgisirsi/0/0/0/5?searchdata1=a318466{001}/, (accessed December 2011)
Royal College of Nursing. Promoting older people's oral health: essential guide. [Online. Available at:]. RCN: London, 2011. http://nursingstandard.rcnpublishing.co.uk/shared/media/pdfs/OralHealth2011.pdf, (accessed December 2011)
Scales K. Intravenous therapy: a guide to good practice. British Journal of Nursing. 2008;17(19):S4–S12.
Scottish Intercollegiate Guidelines Network. Postoperative management in adults. [Online. Available at:]. SIGN: Edinburgh, 2002. http://www.sign.ac.uk/pdf/sign77.pdf, (accessed December 2011)
Smith B., Hardy D. Discharge criteria: ‘just in case’. Journal of Perioperative Practice. 2007;17(3):102. 104–107
Torrance C., Serginson E. Surgical nursing, twelfth ed. London: Baillière Tindall/Royal College of Nursing; 1999.
Wicker P., Cox F. Patient during recovery. Wicker P., O'Neil J. Caring for the perioperative patient, 2nd ed., Oxford: Wiley-Blackwell, 2010.
European Society of Regional Anaesthesia. Postoperative pain management – good clinical practice. General recommendations and principles for successful pain management. (undated) Online. Available at: http://www.esraeurope.org/PostoperativePainManagement.pdf (accessed May 2011)
Hindle A., Coates A. Nursing care of older people. Oxford: Oxford University Press; 2011.
Holland K., Hogg C. Cultural awareness in nursing and healthcare. London: Arnold; 2010.
Hughes, A., 2009. Pre- and post-operative assessment and care: essential skills. In: Endacott, R., Jevon, P., Cooper, S. (Eds.), Clinical nursing skills – core and advanced. Oxford University Press, Oxford
National Clinical Guideline Centre. Venous thromboembolism: reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital. [Online. Available at:]. NCGC, The Royal College of Physicians: London, 2010. http://www.nice.org.uk/nicemedia/live/12695/47920/47920.pdf, (accessed December 2011)
Razouk K., Harrison L., Taljard F. Perioperative management of diabetic patients undergoing surgery. [Online. Available at: NHS Lanarkshire, 2010. http://www.pdc.nhsscotland.com/PracticeandLearning/PoliciesGuidelines/Policies%20and%20Guidelines/Periop%20Mgmt%20Diabetic%20Patients%20Undergoing%20Surgery.pdf, (accessed June 2011)
RCN guidance for improving transfusion practice: http://www.rcn.org.uk/__data/assets/pdf_file/0009/78615/002306.pdf (accessed December 2011).
Insulin pump therapy (registered users only – RCN membership or a journal subscription): http://nursingstandard.rcnpublishing.co.uk/guides/booklets-and-guides/insulin-pump-therapy (accessed December 2011).
NHS Forth Valley publications: http://www.nhsforthvalley.com/publications/ (accessed December 2011).
NICE guidance on perioperative nutritional support in adults – oral nutrition, enteral tube feeding and parenteral nutrition: http://www.nice.org.uk/nicemedia/live/10978/29981/29981.pdf (accessed December 2011).
Healthcare-associated infections (CETL online site). This session offers explanations by patients and carers of what having a healthcare-associated infection meant to them and how they managed: http://www.cetl.org.uk/learning/healthcare_associated_infections/player.html (accessed December 2011).
NHS Local: Better Health Together information website. This site offers a range of resources for people and their carers (lay and professional) and includes video material of patients talking about some of the issues affecting them.There are also explanations about a wide range of conditions in the section on My Health: http://nhslocal.nhs.uk/my-health/conditions/b/pressure-ulcers/all (accessed December 2011).