Chapter 3 Judgement and Decision-Making Skills for Practice
Overview
Why is judgement and decision making important and worthy of inclusion in a book that focuses on Skills for Practice? Few practitioners would contest the notion that they possess knowledge upon which they base their decisions in practice. What the basis of this knowledge is and how they use it in practice is, however, much less clear. Making judgements and decisions are two of the key cognitive tasks used in professional thinking. This chapter teases out how practitioners think in practice, form judgements and make decisions; each of which when made well enables people to take wise action and ultimately enhance the effectiveness of a service’s provision.
The chapter begins by looking at definitions for key terms in the area. It then continues by presenting some of the early occupational therapy studies of clinical reasoning; discussing what this research has told us about the way occupational therapists think, as well as the limitations of the research methods they used. Two related but differing theories of judgement and decision making, that have developed from cognitive psychology, are then presented: cognitive continuum theory and dual process theory. The contribution of each of these theories to practice is examined.
The chapter then considers how practitioners can apply judgement and decision-making skills in practice and exercises are provided to illustrate the challenges and processes of judgement and decision-making tasks. To conclude, the chapter discusses the impact of practitioners’ personal and professional values on judgement and decision making in practice.
Definitions
Researchers studying different cognitive tasks have used a wide variety of terms to describe different types of thinking such as reasoning, judgement, problem solving and decision making (Gale and Marsden 1985). Reasoning implies the drawing of conclusions. Reasoning may be deductive, when the conclusion is logically drawn based on factual information, or inductive, when the conclusion drawn is only possible and needs to be tested in light of further information (Eysenck 1993). A judgement requires a person to consider an item of information or an option and to assign a weight, based on the perceived level of importance. Problem solving involves generating alternatives to select from (see Chapter 10). Decision making occurs when a person makes a selection from possible alternatives that have been considered. In occupational therapy the term ‘clinical reasoning’ tends to be used to cover all these thinking processes but each term can be defined independently and can be used with a distinct meaning.
What tends to clarify the meaning of the terms is understanding the theoretical and methodological orientation of the researcher. Those most interested in the outcome of thinking tend to compare how information has been used with the decision that has been taken. They are most interested in judgement and decision making. Such researchers tend to use quantitative methodologies characteristic of the schools of judgement analysis and decision analysis. They are interested in identification of statistical weightings of judgements or the calculation of the probability that a particular decision has been, or will be, made. Research using judgement analysis has been conducted in occupational therapy by Unsworth (1995, 1996, 1997, 2001), Harries and Harries (2001a, 2001b) and Harries and Gilhooly (2003a, 2003b). To date decision analysis research has not been published in occupational therapy literature.
Researchers more interested in describing the actual processes of thinking, as opposed to the decision outcome, tend to focus their attention on reasoning and problem solving. These latter researchers tend to use qualitative methods such as those informed by phenomenological and ethnographic theories. To date these have accounted for the majority of occupational therapy clinical reasoning research studies.
The early studies*
Joan Rogers used her Eleanor Clark Slagle lecture of 1983 to talk about the ethics, science and art of clinical reasoning. Rogers (1983) defined clinical reasoning as, ‘…the scientific, ethical and artistic dimensions’ of practice (p. 616). Emphasizing that these are inextricably linked.
Later, Mattingly and Fleming (1994) conducted an influential research project of American occupational therapists’ clinical reasoning. It was the first major study to explore the reasoning strategies used by occupational therapists and used an ethnographic and action research approach: interviewing, observing and videoing 17 occupational therapists over a 2-year period (Mattingley and Fleming 1994). The researchers identified reasoning ‘tracks’ or styles and linked these to reasoning strategies. Their findings emphasized that occupational therapists’ reasoning was, ‘largely tacit, highly imagistic and deeply phenomenological’ (Mattingly 1991, p. 797).
Since the work of Mattingly and Fleming (1994), there has been a burgeoning of research in occupational therapy examining the clinical reasoning of occupational therapists (see Fondiler et al 1990, Fleming 1991a, Creighton et al 1995, Alvernick and Sviden 1996, Fortune and Ryan 1996, Fossey 1996, Hagedorn 1996, Munroe 1996, Crabtree and Lyons 1997, Hooper 1997, Chapparo 1999, McKay 1999, Paterson et al 2002, Paterson 2003). This literature has been presented and discussed in greater depth by Patterson and Summerfield-Mann (2006). Whilst there are a few exceptions, the defining characteristics of this body of research are that the methods are qualitative, the sample sizes are generally small, and the participant populations are predominantly north American.
A few key points can be generalized from these and other studies of a similar format in nursing and other professions (Fawcett et al 2001, Sefton 2001, Upshur et al 2001, Rycroft-Malone et al 2004). Generally, these studies view clinical reasoning (or decision making) as being formed of several components including the use of knowledge, self reflection by the clinician (a component of meta cognition), clients’ needs, expectations or desires, and shared decision making. Crucially, the vast majority of these studies view the components of clinical reasoning as being of equal value – like pieces of a jigsaw that are each as important as the other.
Although qualitative approaches were chosen to try to give a holistic understanding of thinking in terms of context, they appear to be limited in terms of their ability to represent the holism of actual thinking. Their lack of validity relates specifically to the difficulty the approaches have in reliably accessing experts’ well-practised intuitive thinking.
Analytical versus intuitive thinking
The first major study of thinking processes in clinical situations was the study of medical problem solving by Arthur Elstein and his colleagues (Elstein et al 1978). Their study used three methods of data collection: direct observation of problem solving using simulated clinical problems, concurrent think aloud and retrospection (whilst viewing video footage). Elstein et al (1978) identified hypothetico-deductive reasoning as the strategy for diagnosis formation in medicine. Occupational therapists also identified hypothetico-deductive reasoning through the ‘occupational dysfunction’ diagnosis (Fleming 1991b). However, when comparing differences between novices and experienced practitioners’ diagnosis formation strategies, Elstein found that there were other forms of thinking (Elstein et al 1990). As experts had the advantage of previous experience they had developed a store of ‘scripts’ (Abernathy and Hamm, 1994). If a client had a familiar problem practitioners used pattern matching to trigger the direct automatic retrieval of an appropriate script. Therefore experts confronted with a familiar problem used a rapid and automatic form of processing that was acknowledged as intuitive reasoning (Abernathy and Hamm 1994).
The more practised in a thinking process a practitioner is, the more intuitive it may become. People are aware of how a motor task such as driving can become partially subconscious; in the same way cognitive tasks can become partially automatic when they have been well practised. It is therefore difficult to verbalize thinking pertaining to a high level of expertise; and post hoc rationalization can reduce the verbalization to a report of a lower-quality thinking process.
Ethnographic and information-processing methods
Ethnographic and information-processing methods appear to have had difficulty in establishing thoughts used in clinicians’ intuitive thinking. These methods have to rely heavily on the reasoner’s awareness of how information has been used to make judgements; they have been limited in their ability to access the more unconscious, rapid and unrecoverable reasoning at the intuitive end of the continuum (Ericsson and Simon 1980). In the early studies intuitive reasoning was not given much attention, for example in the occupational therapists’ study, intuitive reasoning was only nominally identified and described as ‘difficult to map’ (Fleming 1991a).
Whilst these studies were being conducted, other theorists were concurrently drawing into question the efficacy of using verbal reports to access thinking. If intuitive thought was ‘non-recoverable’ the issue of whether decision-makers would have any access into their thinking became apparent (Nisbett and Wilson 1977). With regard to accessing the thinking of experts in particular, verbal reports were recognized by some as inefficient and misrepresentative (Hoffman 1987). Concurrent verbalisations, at best, only got to the content of working memory, or the information attended to (but not necessarily how it is used) and retrospective verbalisations were prone to forgetting and post-hoc rationalisation (Ericsson and Simon 1980). However it is not clear cut. Some recall can be valuable and measures are being taken to maximise the accuracy of recall methods. Unsworth (2004) has begun to use head-mounted video cameras to record occupational therapists’ interventions. This approach has been shown to enhance the accuracy of memory during retrospective recall.
Roberts (1996) and Robertson (1996) recognised the influence of expertise on occupational therapists’ reasoning. The AOFT/AOTA study had focused on hypothetico-deductive strategies in problem identification tasks. These can be verbalised more easily and hence are reported more effectively. Roberts, however, demonstrated that reasoning varied according to the level of expertise and the nature of the task. In her research, 38 practitioners wrote down their thoughts immediately after reading three referral letters. Although some of the reasoning may have been lost before the participant began to write down their thoughts, interesting findings were made. Some practitioners initially used rapid formulations of the issues involved (pattern matchers/heuristic reasoners). They mentioned their recognition of the scenario and recalled previous cases. Others searched for cues and reasoned using various hypotheses, sometimes not reaching any specific formulation. They appeared to have less experience to draw on. The rapid formulators did not show intuitive reasoning exclusively. Evidence of hypothetico-deductive reasoning was also seen when considering some aspects of the case. In these instances participants were thought to have been less familiar with the information. This would concur with the view that reasoning strategies result from interaction between both the experience of the practitioner and the nature of the task.
The value of experience
In Elstein’s 1978 study, differences between novice and expert thinking were explored. They identified that it was the extent of clinical experience in a particular domain that was key to expert thinking. Experts were able to interpret data more accurately when testing hypotheses than novices. This finding had implications for medical education, as contrary to what had been thought, it was not the reasoning strategies themselves that can improve clinicians’ problem solving but the domain-specific knowledge that is important. Pre-registration problem-solving training would, therefore, not create experts: lifelong learning would be necessary to achieve mastery of knowledge domains. Education subsequently made a move away from problem-solving training and toward problem-based learning (Norman and Schmidt 1992). This new method of education increased clinical knowledge through facilitating exposure to clinical case scenarios.
Cognitive continuum theory
In order to better understand why certain thoughts are difficult to access, it is necessary to gain a deeper understanding of how and why differing modes of thought occur. Hammond’s Cognitive Continuum Theory (CCT) can be valuable in understanding these issues (Hammond and Brehmer 1973).
Hammond’s CCT described a range of cognitive modes from intuitive to analytic with quasi-experimental processing as a mid-point. Hammond felt that in more intuitive reasoning, strategies such as pattern recognition and heuristics (rules of thumb) were used: information available (cues) is immediately linked to known patterns (Larkin 1979). This is therefore a largely subconscious, rapid, automated process and is essentially ‘non-recoverable’ (Hammond and Brehmer 1973). At the other end of the continuum, analytical thought occurs. In this mode of thought, hypothetico-deductive reasoning is used: a slower, step-by-step method of thinking that is highly conscious. In hypothetico-deductive thinking, cues are used to generate possible hypotheses and further cues used to test these hypotheses.
Many theorists have agreed that when less practised in a cognitive task, analytical processing is more likely to be used but when more practised in a task, and the information is familiar, intuitive strategies are more likely (Benner 1984, Elstein et al 1990, Norman et al 1994). In addition to the role of expertise, the Cognitive Continuum identified the influence of task characteristics on reasoning strategy. Task characteristics, such as stability and availability of task information are thought to have a strong influence on the possible types of cognitive processing (Shanteau 1992). Therefore the mode of cognitive processing (i.e. thinking) used tends to be a result of the combined effect of level of experience of the practitioner and the characteristics of the task.
Dual-process theories of thinking
Dual-processing theory (Stanovich and West 2003) is a more recent decision-making theory that has developed from cognitive psychology. Whilst bearing similarities to CCT (as both differentiate between intuitive and analytical thinking), there is an important difference in approach. Dual-processing theory posits that the two cognitive systems (the intuitive, which is automatic, holistic and fast; and the analytical, which is deliberate, rational, explicit and slow) are in fact two different systems; not a single continuum as proposed in Hammond’s CCT. Functional magnetic resonance imaging has indicated that these systems are in fact neurologically different (Goel et al 2000). In dual-processing theory, the fast, automatic form of processing is referred to as System 1 (S1) and the slow, deliberate form as System 2 (S2) (Stanovich and West 2000).
Dual-processing theory can be understood in the following way. S1 delivers judgements through largely subconscious reasoning (tacit knowledge) and only the outcome is conscious; whilst, S2 is a highly conscious and logical reasoning process. S2 type reasoning enables practitioners to think about hypothetical situations, analyse potential future possibilities and other features of a situation that are not immediately apparent. S2 type thinking uses central working memory (Gathercole 2003), focuses on one task at a time, and is correlated with general intelligence (Stanovich and West 2000). S2 type reasoning is viewed as having evolved more recently than S1 and, interestingly, is a faculty that only humans have (Evans 2003).
Parallels between the components of clinical reasoning, for instance the work of Mattingly and Fleming (1994), and dual-process theory are easy to make. Concepts such as tacit knowledge and intuitive reasoning appear closely linked to the holistic nature of S1, whilst knowledge and research drawn from an objective basis are more closely associated with the objective reasoning of S2.
Paley et al (2007) drew comparisons between clinical reasoning and empirical knowledge using dual-process theory. Whilst their paper focused on nursing research, the arguments are valid for other areas of health-care research, including occupational therapy. In order to draw comparisons with dual-processing theory they referred to the type of reasoning associated with intuitive reasoning and ‘artful practice’ as N1 and objective knowledge drawn from quantitative research as N2.
Paley et al (2007) however highlight that there is one major difference between the N1/N2 distinction and the S1/S2 distinction; whilst the majority of occupational therapy clinical reasoning literature regards N1 and N2 as equal partners. Cognitive dual-processing theory, on the other hand, emphasises that the principal function of S2 is to override, monitor, suppress the invalid inferences of S1 (Kahneman and Frederick 2002, Evans 2003, Evans and Over 2004). Therefore, while occupational therapy literature, to date, generally views N1 and N2 as equally valid ways of thinking, it is clear that S2 ways of thinking are epistemologically superior.
Heuristics and biases
The heuristics and biases research literature explains why there is a disparity between S1 and S2 ways of thinking (Kahneman et al 1982, Gilovich et al 2002). This research shows that people often make mistakes when the clinical experience (S1) is not controlled by measurable objective evidence (S2). The reasons behind this are outlined in greater detail by Paley et al (2007).
Interestingly S1 type thinking is not only responsible for clinical errors in thinking, but can also explain some academic errors as well. For example how people view and understand scientific research can be compromised by their prior beliefs about its findings (Koehler 1993). Resch et al (2000) and Kaptchuk (2003) have both established that well-designed studies can be dismissed because they either indicate an unconventional intervention is effective, or that a well-respected intervention is ineffective. Conversely poorly designed studies can sometimes be accepted as they appear to support widely held beliefs. This principle is not only restricted to experimental research. Generally any method will be regarded as valid if its conclusions are believed, and as invalid if its conclusions are disagreed with (Fugelsang and Thompson 2000, Roberts and Sykes 2003, Fugelsang et al 2004).
So what does knowledge of S1 and S2 tell us about N1 and N2 types of thinking in occupational therapy? It means that intuitive clinical reasoning is likely to make mistakes (due to S1 type weaknesses in thinking) when it is not corrected by the more structured and objective approach of S2 thinking processes. The impact of thinking errors associated to S1 type thinking are not limited to occupational therapy or nursing, etc. Stanovich (2003) has stated that through such errors, ‘physicians choose less effective medical treatments; people fail to accurately assess risks in their environment; information is misused in legal proceedings; millions of dollars are spent on unneeded projects by government and private industry; parents fail to vaccinate their children; unnecessary surgery is performed; animals are hunted to extinction; billions of dollars are wasted on quack medical remedies; and costly financial misjudgements are made’ (p. 292). Dual-processing theory demonstrates that tacit knowledge and experience (S1/N1) cannot be viewed equally to knowledge that is rigorously researched and empirically based (S2/N2). To continue to view N1 and N2 forms of knowledge as equal, Paley at al (2007) state, is to celebrate the possibility of error in practice.
It could be said that the notion that we should, ‘base our practice on “generalisable evidence” demolishes our traditional practice. Such worldviews urge us to swap our ideas of crafting care around the unique complexity of the individual, for a generalisation about what worked for most people in a study’ (Barker 2000: 332). This is an argument that has proven popular in health-care literature in general and occupational therapy is no exception. The structure of this argument is as follows: ‘Quantitative studies refer to populations; practitioners care for individuals; therefore, quantitative studies are irrelevant to clinical practice. This is similar in form to: epidemiological studies of cancer refer to populations; individuals make decisions; therefore, epidemiological studies are irrelevant to my decision to smoke. Both of these arguments dismiss the concepts of probability and risk, and would make a nonsense of actuarial procedures and insurance. In any case, the experience on which the nurse, [or occupational therapist] draws when working with an individual is also population-based: the population of clients she or her colleagues have previously seen. If the population defined by a research study is irrelevant to the unique individual, so is the population defined by clinical experience’ (Paley et al 2007: 697).
So, how can we use our knowledge of dual-processing theory in practice? S1 is how most practitioners reason, most of the time. But if practitioners use S2 type thinking it will monitor and improve this intuitive form of reasoning (Degani et al 2006). It is this rationale that supports evidence-based practice, helps practitioners to question their judgements about practice and encourages the search for more evidence-based ways of thinking and working.
Three factors, however, inhibit the use of S2 thinking in clinical practice. First, there appears to be a natural resistance to the use of S2 type thinking and there is a general reluctance to accept the idea that practitioners make S1 type errors in reasoning. Secondly, evidence-based decision making and S2 type thinking do not come naturally. And thirdly, S2 type thinking requires time and space – something that challenges everyone (Paley et al 2007).
The idea that intuitive reasoning and holistic practice (S1/N1), is equal in weight and status to scientific evidence (S2/N2), is persuasive. But this should not get in the way of delivering the highest quality services to clients. And to achieve this practitioners need to employ S2 type strategies. There is, of course, no single answer to this issue, but there is one possibility that may offer a solution: the use of conceptual models of practice.
Conceptual models of practice
Within occupational therapy, structured use of conceptual models of practice such as the Canadian Model of Occupational Performance and Engagement (Townsend and Polatjko 2007) or the Model of Human Occupation (Kielhofner 2007) could be viewed as approaches that adopt S2 supervisory functions in practice. Their conscious use ensures that all necessary factors have been considered and given due priority when working with a client. When viewed in the light of the evidence that supports the supervisory nature of S2 over S1, conceptual models such as MOHO and CMOP-E which have evolved through rigorous research, do not provide an illusion of safety as Smith (2006) suggested. They are not a panacea for perfect practice. But they do ensure that the inherent biases and mental shortcuts of practitioners, masquerading under the guise of ‘artful practice’ or clinical reasoning (and which typify S1 type thinking), cannot be carried away unabated, drawing clients into decisions that are ill-considered and lacking in reliable evidence to support their validity.
Conceptual models of practice, as an answer to the dual-processing dilemma, are only one option and their endorsement here should not be taken to suggest that these models are viewed as perfect or infallible. But some do provide an evidence-based structure to follow which limits the possibilities for personal S1 type biases, and conceptual models continue to be researched and refined.
Applying judgement and decision-making skills in practice
Judgement and decisions skills have to be learnt for every stage of the occupational therapy process from referral through to evaluation. Through the use of scenarios as well as real life experience, reasoning skills can be exercised in relation to specific domains. The following examples are designed to improve your reasoning in practice.
Imagine you are an occupational therapist in an adult community mental health team. You may consider taking some general referrals which have been sent to your team and some which have been sent directly to you. These referrals fall into the second category: they have been sent directly to you. Look at the referral in Figure 3.1 and indicate the degree of priority you feel the referral warrants. In practice you would also be likely to see the client before making a fully informed judgement. However, for this task just use your initial impressions of whether you would work with the client. So how much priority would you give it? Put a cross on the line at the bottom of the referral to give your decision.
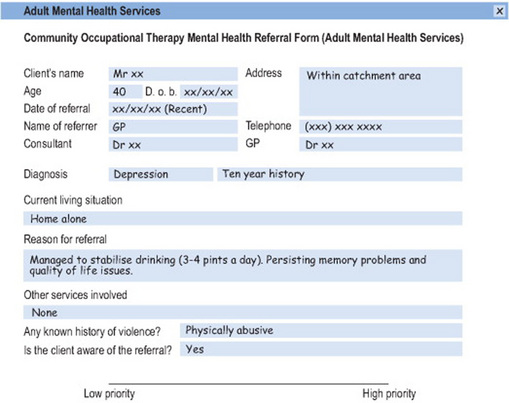
In doing this task you will have decided how much attention to give to the differing types of information. You will have judged how important those types of information are to the decision of prioritisation. You will have used your skills of judgement and decision making. If you have experience of this field the referral may have reminded you of someone similar whom you, or a colleague, have worked with. In that case you may have been influenced by your previous experience. Has any knowledge of current government policy influenced your thinking? For example some governments require services to focus on clients with severe enduring mental health needs. If you do this task with colleagues or fellow students discuss:
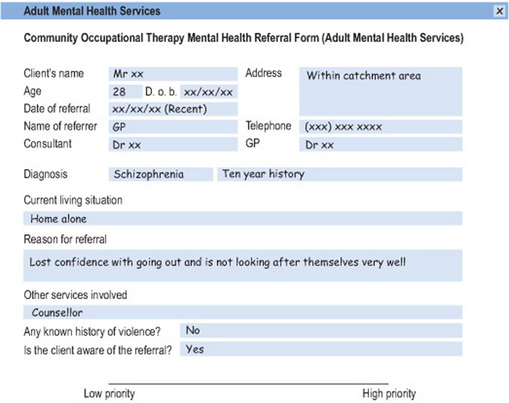
A common comment is that it is difficult to make a decision without knowing what other referrals might look like. This is linked to the phenomenon of calibration. Experience is needed to know how to appropriately calibrate judgements and decisions. So look at this second referral (see Figure 3.2). Go through the same process. Which referral is given higher priority?
In order to learn from those who have experience in the judgements and decisions of their domains we need to study experts in their specific specialities. How would occupational therapists with many years of experience in the field of community mental health make these types of judgements and decisions? Research was conducted in the UK with 40 experienced occupational therapists on 120 referrals of this type. It was found that four different judgement policies were being used. Policies differed according to whether the practitioner aimed to work in a generic or occupationally orientated way (Harries and Gilhooly 2003a). A website has been developed to train novices to follow the occupationally orientated expert judgement policies. The website allows the novice to practise on a set of referrals in order to know how to calibrate their decisions. Training information is then provided about the expert policies and then a second set of referrals is given for prioritisation. Feedback on how the decision maker has done in relation to the expert group is then provided. The training package has been shown to be effective in developing novices’ referral prioritisation skills (Weiss et al 2006) and is a now a freely available evidence-based educational tool to be found at www.priscillaharries.com (Harries 2006). (Email priscilla.harries@brunel.ac.uk for the passwords.)
It is well documented that when experienced, people are better at judging what is important and what is not (Shanteau et al 1991), they are better at balancing the client’s perspective with the realities of the environment and they have a vision of people’s capacity for change. When a practitioner is new to a clinical or social domain it is difficult to make wise judgements or decisions; it is easy to feel overwhelmed as all new information can seem important. Experience is the only way to move forward; each time one moves to a new domain one has to start from the beginning and learn what is important in the new field. This new knowledge facilitates the store of ‘scripts’ in memory (Abernathy and Hamm 1994); these scripts are based on knowledge of similar clients and the narratives that have been heard. Recognition can then be used to pattern match between what has been experienced and any familiar situation which later arises.
Memory and recognition
Research on memory has been conducted to identify how experienced clinicians organise memory ‘chunks’ and how recall mechanisms facilitate recognition of previously encountered scenarios (Norman and Schmidt 1992). Groen and Patel (1985), identified that novice problem solvers reasoned backwards from hypotheses generation to data, whereas experts reason forward using ‘if .… then’ rules (propositional reasoning). It is apparent that to use these propositional rules experts have to draw on their well-structured knowledge bases (Johnson-Laird and Shafir 1993). However when an expert is confronted with an unfamiliar problem they will revert back to methods of hypothesis testing (Elstein et al 1990). The use of scripts should not limit how a practitioner works with people but be used to develop an awareness of what is important to pay attention to and what change is possible.
Values
How someone decides what is important when assigning weights or selecting an option is linked to ones’ personal and professional values and the values of the setting in which the judgements and decisions must be made. In discussing how judgements have been made, values individuals hold can be brought to light. Some of these are from personal experience, some from professional experience. Where practitioners vary in their values, judgements will be made differently. In a health system that promotes parity and adherence to protocol, it is important to get to the core of an individual’s thinking in order to identify thinking methods that result in best practice. Is it more important to help someone with managing self care needs or to gain a work role? Do clients need to socialise? These issues are not black and white and the client themselves or carers are often able to help to focus priorities.
Values inherent in frames of reference and theoretical frameworks
The differing theoretical frameworks that occupational therapists draw on are key to the process of judgement and decision making. These influence how phenomena are viewed and therefore where importance is placed both in terms of what is viewed as an issue that needs addressing and how best that issue might be addressed. They view people from different perspectives and require attention to be given to different aspects of that person. Each frame of reference or theoretical framework has a different value system.
Psychoanalytic, client-centred, cognitive behavioural, biomechanical, developmental, social and occupational frames of reference (see Duncan 2006a) each hold links to what is viewed as important. The client-centred frame of reference for example requires the client to be heavily involved in the decision-making process (see Chapter 4) whereas the biomechanical frame of reference may be more practitioner-led. Psychoanalytical theories require attention to be paid to past experiences whereas cognitive-behavioural theories focus on the here and now. The value systems also vary between the conceptual models of occupational therapy practice. Research from the major conceptual models support their use as being relevant to a multiplicity of needs whether it be a person’s social withdrawal or muscle weakness. And the use of conceptual models of practice does not restrict practitioners from also using a variety of frames of reference (such as the biomechanical, or client-centred frame of reference) depending on the presenting problem. However, not all occupational therapists practice in this way and many select their theoretical basis of practice from a range of frames of reference without necessarily using a conceptual model of practice as an occupational filter (Mallinson and Forsyth 2000). In these cases practitioners aim to select a frame of reference that best fits the client’s need and the context for the intervention; taking into account the strength of the theory’s evidence base and of the cost effectiveness of its use.
Jean was seen at home by the occupational therapist from the community mental health team. The GP had referred the client due to her high anxiety levels, limited IQ and a recent bereavement. Due to her anxiety Jean had also lost her job. During the interview the practitioner noticed how anxious and underweight Jean is. She also observed that there was a lack of food in the house. One aspect that the occupational therapist now wants to assess, through observation and interview, is why Jean is not eating enough to sustain her weight. Depending on the issues that present, the practitioner will choose interventions that are informed by differing theoretical frameworks. Each theory holds differing values which alter the focus of the intervention.
In the above example, Jean is not eating because she may have anorexia nervosa, an occupational therapist may view her needs from a psychoanalytical perspective. Her unresolved emotional conflict could be thought to be the result of prior life experiences. Her withdrawn childlike state could be seen as a sign of emotional underdevelopment. A practitioner could involve the client in projective art, drama therapy and creative group work to facilitate the psychosocial development of her emotional maturity. The ability to express oneself, to develop a sense of self-efficacy and self-esteem would be necessary before Jean will develop the wish to eat. Once partial psychosocial capacity is achieved, the practitioner would add an educational perspective, for example teaching skills in cooking, budgeting, and giving advice as Jean resumes social and work activities.
If however, Jean was not eating because she had severe rheumatoid arthritis, her needs would be viewed from a very different perspective. Her difficulties may be due to the physical weakness, pain and limited range of movement that can cause problems with cutting up food, opening cans and turning on taps. In this case a biomechanical and compensatory perspective may be taken (McMillan 2006). Joint protection advice would be provided to try to reduce the risks of further hand function deterioration. Altering kitchen work surfaces may be suggested, to allow heavy pans to be slid rather than lifted, so that ulna deviation is not exacerbated. Splints may be made by the practitioner to stabilise the radiocarpal and metacarpal phalangeal joints in a functional position. Fatigue management advice may be given to ensure periods of rest are balanced with periods of activity. Equipment such as tap turners, stair rails and elastic shoelaces may be provided to maximise independence and thereby provide some privacy for dressing and bathing occupations. Advice and support to engage in valued leisure or work occupations would also be essential to ensure that Jean has a good quality of life.
If however a client with a physical disability has developed depression as a result of their capacity to cope with their disability, psychological theories may also be needed. Cognitive-behaviour theories would be used to promote positive thinking and to change/challenge cognitive distortions. However, an occupational therapist would not conduct cognitive-behaviour therapy in isolation but would use it alongside occupational engagement (Duncan 2006b). The benefits of engaging in a valued occupation that assists the client to recognise their own skills and potential can help to reinforce positive thinking. The key is to find occupations that are matched to the individual’s capacity and value system, thereby ensuring a sense of self-efficacy and achievement.
Some practitioners and theorists advocate selecting an occupational therapy conceptual model of practice before seeing a client to ensure the occupation focus of the intervention (Forsyth and Kielhofner 2006; see Chapter 7); others do not. Regardless, the reasons for clients’ needs have to be determined before it is known which specific frame of reference will be most valuable in guiding interventions. Some initial assessment is therefore needed before a theoretical frame of reference (such as the biomechanical or cognitive behavioural) is chosen. This will then influence the method of the full assessment and inform which issues need to be explored further. For example if Jean has not been eating through a:
Therefore the way in which practitioners reason using conceptual models of practice and frames of reference can have a significant impact on the judgements and decisions in practice.
Summary
This chapter has highlighted the importance of judgement and decision-making skills in practice. Occupational therapy clinical reasoning literature has been presented and discussed. Two judgement and decision-making models (the CCT and dual-process theory), drawn from cognitive psychology were described and discussed. These models highlight the difference between intuitive reasoning which characterises what is known as ‘artful practice’ and rational reasoning which is a more logical, deliberate and conscious form of reasoning and characterises evidence-based ways of working. Historically the types of knowledge generated through ‘artful practice’ and more evidence-based methods have been looked upon with equal worth within occupational therapy. However both the CCT and dual-process theory highlight the superiority of the judgement and decision making that come from the logical, deliberate method (S2/N2); whilst recognising that most people tend to be naturally intuitive decisions makers in practice (S1/N1). The chapter presented conceptual models of practice as one possibility that could increase the amount of S2 type judgement and decision making in practice. Practical examples were also given to illustrate the complexity of judgement and decision making in practice.
Abernathy CM, Hamm RM. Surgical scripts: master surgeons think aloud about 43 common surgical problems. Philadelphia, PA: Hanley & Belfus, 1994.
Alvervik A, Sviden G. On clinical reasoning: patterns of reflection on practice The Occupational Therapy. Journal of Research. 1996;16(2):98-110.
Barker P. Reflections on caring as a virtue ethic within an evidence-based culture. International Journal of Nursing Studies. 2000;37:329-336.
Benner P. From novice to expert: excellence and power in clinical nursing practice. Menlo Park, CA: Addison-Wesley, 1984.
Chapparo C. Working out: working with Angelica-interpreting practice. In: Ryan SE, McKay EA, editors. Thinking and reasoning in therapy: Narratives from practice. Cheltenham, UK: Stanley Thornes, 1999.
Crabtree M, Lyons M. Focal points and relationships: A study of clinical reasoning. British Journal of Occupational Therapy. 1997;60(2):57-64.
Creighton C, Dijkers M, Bennett N, et al. Reasoning and the art of therapy for spinal cord injury. American Journal of Occupational Therapy. 1995;49:311-317.
Degani JAS, Shafto M, Kirlik A. What makes vicarious functioning work? Exploring the geometry of human-technology interaction. In: Kirlik A, editor. Adaptive Perspectives on Human–Technology Interaction. New York: Oxford University Press; 2006:179-196.
Duncan EAS, editor. Foundations for Practice in Occupational Therapy, 4th edn, Edinburgh, UK: Elsevier/Churchill Livingstone, 2006.
Duncan EAS. The cognitive behavioural frame of reference. Duncan EAS, editor. Foundations for Practice in Occupational Therapy, 4th edn. Edinburgh, UK: Elsevier/Churchill Livingstone. 2006:217-232.
Elstein AS, Shulman LS, Sprafka SA. Medical problem solving: an analysis of clinical reasoning. Cambridge, MA: Harvard University Press, 1978.
Elstein AS, Shulman LS, Sprafka SA. Medical problem solving: a ten year retrospective. Evaluation and the Health Professions. 1990;13(1):5-36.
Ericsson KA, Simon HA. Verbal reports as data. Psychological Review. 1980;87(3):215-251.
Evans J. In two minds: dual-process accounts of reasoning. Trends in Cognitive Science. 2003;7(10):454-459.
Evans J, Over D. If. Oxford, UK: Oxford University Press, 2004.
Eysenck M. Principles of Cognitive Psychology. Hove, UK: Lawrence, 1993.
Fawcett J, Watson J, Neuman B, et al. On nursing theories and evidence. Journal of Nursing Scholarship. 2001;33(2):115-119.
Fleming MH. The therapist with the three-track mind. American Journal of Occupational Therapy. 1991;45(11):1007-1014.
Fleming M.H. Clinical reasoning in medicine compared with clinical reasoning in occupational therapy. American Journal of Occupational Therapy. 1991;45(11):988-996.
Fondiller ED, Rosage LJ, Neuhaus BE. Values influencing clinical reasoning in occupational therapy: An exploratory study. Occupational Therapy Journal of Research. 1990;10:41-55.
Forsyth K, Kielhofner. The Model of Human Occupation: Integrating Theory into Practice and Practice into Theory. 2006. Duncan EAS, editor. Foundations for Practice in Occupational Therapy, 4th edn. Edinburgh, UK: Elsevier/Churchill Livingstone. 2006:69-108.
Fortune T, Ryan S. Applying Clinical Reasoning: A caseload management system for community occupational therapists. British Journal of Occupational Therapy. 1996;59:207-211.
Fossey E. Using the Occupational Performance History Interview: Therapist reflections. British Journal of Occupational Therapy. 1996;59:223-228.
Fugelsang JA, Thompson VA. Strategy selection in causal reasoning: when beliefs and covariation collide. Canadian Journal of Experimental Psychology. 2000;54:13-32.
Fugelsang JA, Stein C, Green A, et al. Theory and data interactions of the scientific mind: evidence from the molecular and the cognitive laboratory. Canadian Journal of Experimental Psychology. 2004;58:86-95.
Gale J, Marsden P. Diagnosis: process not product. In: Sheldon M, Brooke J, Recotr A, editors. Decision-Making in General Practice. Basingstoke, UK: Macmillans, 1985.
Gathercole S, editor. Short-Term and Working Memory. Hove, UK: Taylor and Francis, 2003.
Gilovich T, Griffin D, Kahneman D, editors. Heuristics and Biases: The Psychology of Intuitive Judgement. Cambridge, UK: Cambridge University Press, 2002.
Goel V, Buchel C, Frith C, et al. Dissociation of mechanisms underlying syllogistic reasoning. Neuroimage. 2000;12(5):504-514.
Groen G.J, Patel VL. Medical problem-solving: some questionable assumptions. Medical Education. 1985;19:95-100.
Hagedorn R. Clinical decision making in familiar cases: A model of the process and implications of practice. The British Journal of Occupational Therapy. 1996;59:217-222.
Hammond KR, Brehmer B, editors. Quasi-rational and distrust: implications for international conflict. Human Judgement and Social Interactions. New York: Rineholt & Winston, 1973.
Harries P. Editorial: The development of a web-based tool for training referral prioritization skills. International Journal of Therapy and Rehabilitation. 2006;13(6):777.
Harries PA, Harries C. Studying clinical reasoning, part 1: have we been taking the wrong ‘track’? British Journal of Occupational Therapy. 2001;64(4):164-168.
Harries PA, Harries C. Studying clinical reasoning, Part 2: applying social judgement theory. British Journal of Occupational Therapy. 2001;64(6):285-292.
Harries P, Gilhooly K. Identifying occupational therapists referral priorities in community health. Occupational Therapy International. 2003;10(2):150-164.
Harries P, Gilhooly K. Generic and specialist occupational therapy casework in community mental health. British Journal of Occupational Therapy. 2003;66(3):101-109.
Hoffman RR. The problem of extracting the knowledge of experts from the perspective of experimental psychology. AI Magazine. 1987:53-67.
Hooper B. The relationship between pre-theoretical assumptions and clinical reasoning. American Journal of Occupational Therapy. 1997;51:328-338.
Johnson-Laird PN, Shafir E. The Interaction between reasoning and decision-making: an introduction. Cognition. 1993;49:1-9.
Kahneman D, Frederick S. Representativeness revisited: attribute substitution in intuitive judgment. In: Gilovich T, Griffin D, Kahneman D, editors. Heuristics and Biases: The Psychology of Intuitive Judgment. Cambridge, UK: Cambridge University Press; 2002:46-71.
Kahneman D, Slovic P, Tversky A, editors. Judgment under Uncertainty: Heuristics and Biases. Cambridge, UK: Cambridge University Press, 1982.
Kaptchuk TJ. Effect of interpretive bias on research evidence. British Medical Journal. 2003;326:1453-1455.
Kielhofner G. Model of Human Occupation. Theory and Practice, 4th edn. Baltimore, MD: Lippincott Williams & Wilkins. 2007.
Koehler JJ. The influence of prior belief on scientific judgments of evidence quality. Organizational Behavior and Human Decision Processes. 1993;56:25-28.
Larkin J.H, editor. Information processing and science instruction. Cognitive Process Instruction. Philadelphia, PA: Franklin Institute, 1979.
Mallinson T, Forsyth K. Components of the Occupation Filter. 2006. Duncan EAS, editor. Foundations for Practice in Occupational Therapy, 4th edn. Edinburgh, UK: Elsevier/Churchill Livingstone. 2000:86.
Mattingly C. What is clinical reasoning? American Journal of Occupational Therapy. 1991;45(11):979-986.
Mattingley C, Fleming MH. Clinical reasoning: forms of inquiry in a therapeutic practice. Philadelphia, PA: Davis, 1994.
McKay EA. Lilian and Paula: a treatment narrative in acute mental health. In: Ryan SE, McKay EA, editors. Thinking and reasoning in therapy: Narratives from practice. Cheltenham, UK: Stanley Thornes; 1999:53-64.
McMillan I. Assumptions underpinning a biomechanical frame of reference in occupational therapy. 2006. Duncan EAS, editor. Foundations for Practice in Occupational Therapy, 4th edn. Edinburgh, UK: Elsevier/Churchill Livingstone. 2006:255-276.
Munroe H. Clinical reasoning in community occupational therapy. British Journal of Occupational Therapy. 1996;59(5):196-202.
Nisbett R, Wilson T. Telling more than we can know: verbal reports on mental processes. Psychological Review. 1977;84:231-259.
Norman GR, Schmidt HG. The psychological basis of problem-based learning: a review of the evidence. Academic Medicine. 1992;67(9):557-565.
Norman GR, Trott AL, Brooks LR, et al. Cognitive differences in clinical reasoning related to postgraduate training. Teaching and Learning in Medicine. 1994;6:114-120.
Paley J, Cheyne H, Dalgleish L, et al. Nursing’s ways of knowing and dual process theories of cognition. Journal of Advanced Nursing. 2007;60(6):692-701.
Paterson ML. Professional Practice Judgement Artistry in Occupational Therapy Practice. Australia: The University of Sydney, 2003. Unpublished PhD thesis
Paterson M, Summerfield-Mann L. Clinical Reasoning. Duncan EAS, editor. Foundations for Practice in Occupational Therapy, 4th Edn. Elsevier/Churchill Livingstone. 2006:315-335.
Paterson M, Higgs J, Wilcox S, et al. Clinical reasoning and self-directed learning: Key dimensions in professional education and professional socialisation. Focus on Health Professional Education: A Multi-Disciplinary Journal. 2002;4(2):5-21.
Resch KI, Ernst E, Garrow J. A randomized controlled study of reviewer bias against an unconventional therapy. Journal of the Royal Society of Medicine. 2000;93:164-167.
Roberts AE. Approaches to reasoning in occupational therapy: a critical exploration. British Journal of Occupational Therapy. 1996;59(5):233-236.
Roberts MJ, Sykes EDA. Belief bias and relational reasoning. The Quarterly Journal of Experimental Psychology. 2003;56A(1):131-154.
Robertson L. Clinical reasoning, Part 2: novice/expert differences. British Journal of Occupational Therapy. 1996;59(5):212-216.
Rogers J. Clinical reasoning: The ethics, science, and art. American Journal of Occupational Therapy. 1983;37:601-616.
Rycroft-Malone J, Seers K, Titchen A, et al. What counts as evidence in evidence-based practice? Journal of Advanced Nursing. 2004;47(1):81-90.
Sefton AJ. Integrating knowledge and practice in medicine. In: Higgs J, Titchen A, editors. Practice Knowledge and Expertise. Oxford, UK: Butterworth Heinemann; 2001:29-34.
Shanteau J. Competence in experts: the role of task characteristics. Organizational Behavior and Human Decision Processes. 1992;53:252-266.
Shanteau J, Grier M, Berner E. Teaching decision making skills to student nurses. In: Baron J, Brown RV, editors. Teaching decision making to adolescents. Hillsdale, UK: Lawrence Erlbaum; 1991:185-206.
Smith G. Telling tales – How stories and narratives co-create change. The British Journal of Occupational Therapy. 2006;69(7):304-311.
Stanovich K. The fundamental computational biases of human cognition: heuristics that (sometimes) impair decision making and problem solving. In: Davidson JE, Sternberg RJ, editors. The Psychology of Problem Solving. New York: Cambridge University Press; 2003:291-342.
Stanovich K, West RF. Evolutionary versus instrumental goals: how evolutionary psychology misconceives human rationality. In: Over D, editor. Evolution and the Psychology of Thinking: The Debate. Hove, UK: Psychology Press; 2003:171-230.
Townsend E, Polatajko HJ. Enabling Occupation II: Advancing an Occupational Therapy Vision for Health, Well-being, & Justice through Occupation. Ottawa, Canada: Canadian Association of Occupational Therapists, 2007.
Unsworth CA. Team decision making in rehabilitation. American Journal of Physical Medicine and Rehabilitation. 1996;75:483-484.
Unsworth CA. Studying clinical reasoning. British Journal of Occupational Therapists. 2001;64(6):316-317.
Unsworth CA. Clinical reasoning: How do pragmatic reasoning, worldview and client-centredness Fit? The British Journal of Occupational Therapy. 2004;67(1):10-19.
Unsworth CA, Thomas SA, Greenwood KM. Rehabilitation team decisions on discharge housing for stroke patients. Archives of Physical Medicine and Rehabilitation. 1995;76:331-340.
Unsworth CA, Thomas S.A, Greenwood KM. Decision polarization among rehabilitation team recommendations concerning discharge housing for stroke patients. International Journal of Rehabilitation Research. 1997;20:51-69.
Upshur REG, VanDenKerkhof E, Goel V. Meaning and measurement: an inclusive model of evidence in health care. Journal of Evaluation in Clinical Practice. 2001;7(2):91-96.
Weiss D, Shanteau J, Harries P. People who judge people. Journal of Behavioral Decision Making. 2006;19:441-454.