Chapter 10 Problem-solving
Introduction
The Chambers dictionary (1994) defines a problem as, ‘a matter difficult to settle or solve’ and problem-solving behaviour as ‘the use of various strategies to overcome difficulties in attaining a goal’ (p. 1366). A problem is generally something that is blocking something from being achieved. It can also be something that occurs when a person does not know how to resolve a situation. In other words, ‘a problem arises when someone wants to do something but either does not know how or is in someway blocked from implementing a known solution. Thus, the problem is the gap that separates individuals from where they are now and where they want to be’ (Robertson 1996: 178). The practical nature of occupational therapy lends itself to naturally take a problem-solving approach to intervention. Consider the following scenarios:
Each of these scenarios present people who are likely to come into contact with occupational therapy and have problems of various forms that they need to resolve.
This chapter is divided into two main sections that present the key ways in which practitioners use problem solving in practice. The first section presents problem solving as a general theoretical approach to practice (Roberts 1996, Robertson 1996, Dutton 2000, Hagedorn 2001). The second section draws on theory from the cognitive behavioural frame of reference (see Duncan 2006) to present how problem solving can also be used as a specific therapeutic intervention.
Problem solving as a theoretical approach in practice
As a theoretical framework for occupational therapy practice, problem solving can be understood as a form of clinical reasoning (Roberts 1996, Paterson and Summerfield-Mann 2006). Dutton (2000) presented problem solving as the practical manifestation of practitioners’ cognitive abilities to break down clients’ difficulties and problems in to small steps. Robertson (1996) examined problem solving in practice and presented it as a form of cognitive information processing. This approach views problem solving as a rational and logical process that describes how practitioners understand a problem and work to solve it (Robertson 1996). Whilst occupational therapists often focus on resolving problems, Robertson (1996) emphasised that it is worth initially spending considerable time to conceptualise how the problem is understood as these ideas will shape the future interventions a practitioner will use to resolve the problem.
Hagedorn (2001) argued that the whole occupational therapy process can be viewed in terms of problem solving and suggested that it entailed the following stages:
Opacich (1991) had, however, already outlined a similar series of stages to describe the occupational therapy process. And although Opacich (1991) considered these in terms of a clinical reasoning process, Paterson and Summerfield-Mann (2006) suggested they can also be viewed in terms of a problem-solving process. Opacich’s (1991) stages are:
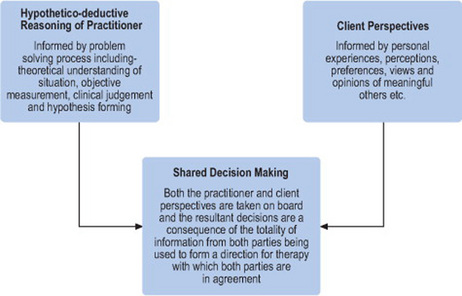
Opacich’s (1991) and Hagedorn’s (2001) approaches to the occupational therapy problem-solving process have clear similarities. Both approaches are essentially forms of hypothetico-deductive reasoning; which is centred on how a professional builds a hypothesis and forms a sequential series of actions. Unsworth (1999) stated that hypothetico-deductive reasoning is an inadequate clinical reasoning strategy to employ on its own as, by its nature, it excludes the interactions that occur between practitioner and clients in practice. However, it can also be argued that the hypothetico-deductive reasoning of the occupational therapy problem-solving process, whilst inadequate in isolation, is essential for practitioners to form an objective perspective of a client’s problem. This understanding can then be shared with the client and, informed by clients’ personal experiences; perceptions; preferences; as well as the views and opinions of meaningful others in the client’s life, can help form a shared decision about the direction of occupational therapy intervention (see Figure 10.1). Chapter 4 describes the challenges of undertaking shared decision making in practice.
Using problem solving as a therapeutic intervention
Problem solving in clinical practice is based on the theoretical foundations of cognitive behavioural therapy. Occupational therapists may find that they use this process intuitively, yet it has a strong theoretical basis (D’Zurilla and Nezu 1999, 2000). Whilst the problem-solving process originally developed within mental health settings, its applications are broad and should not be considered as an intervention for mental health settings alone (see Vignette 10.1). As a therapeutic skill and method of intervention, problem solving has several strengths. It is relatively brief, is applicable to a wide range of issues in differing clinical situations, and aims to empower clients to resolve their own personal issues and challenges without seeking professional assistance in the future.
Vignette 10.1
Leon is a 43-year-old man. He is married to Eleanor and has one son, Theo (aged 15). Leon was diagnosed with a relapsing/remitting form of multiple sclerosis at the age of 31. Initially he had managed to continue to work in his office, however he changed his hours to part-time last year as he was becoming increasingly tired. Ten months ago Leon suffered a further relapse in his condition and has since been off work completely.
Leon’s GP has referred him to see an occupational therapist. The occupational therapist visited Leon at home.
Identifying problems
In discussion, Leon states that he is having a variety of problems and lists them, in no particular order, as follows:
Decide which goals to tackle first
In discussion with Leon, it is agreed to refer to social work to assist with his financial concerns and to focus initially on his fatigue.
Agree goals
Leon wishes to maximize his time awake to look after his self care, and be less tired. Looking after the house is less important to Leon. The following goal is agreed:
Generate possible solutions to meet goals
Leon considers the following potential solutions to meet his goals:
Selecting the best strategy
Leon considers that all possible solutions have worth, and in fact are not mutually exclusive. However, he decides to focus on going to bed no later than 10.30, as he has been reading some information about energy conservation that his general practitioner had given him.
Putting it into action
Leon’s occupational therapist encourages him to put his strategy into action as soon as possible. Eleanor thinks Leon’s plan is a great idea and says she will encourage him to stick to it. Leon himself acknowledges that going to bed sounds easy, but that he is a creature of habit and enjoys watching American police dramas late at night on digital TV. To manage his strategy he will have to change some habits.
Leon’s occupational therapist works with him to develop a wind-down routine for each evening. The aim of this is to help Leon develop new routines and manage his way around the perceived loss of TV. The occupational therapist suggests that Leon could record the programmes he is missing, but Leon dismisses this idea as he says there are so many repeats these days it would not be worthwhile. Instead, Leon decides to switch off the TV at 10pm each evening and spend the last half an hour getting ready for bed.
Reviewing the progress
The practitioner leaves Leon to implement his plan of going to bed earlier and arranges to return in one week’s time. When she returns, Leon reports that he had had a shower six days out of seven and that he had managed to get to bed before 10.30pm four nights out of seven. On discussion Leon agreed that it was not necessary to think of an alternative strategy at this stage: he could see the benefits that going to bed earlier made on his energy conservation the following day and felt confident that he would be able to at least maintain his performance of the previous week, and potentially improve. Together Leon and his practitioner decided to move on and consider the other issues.
Problem solving has been identified as being useful for two types of individual. The first are people who generally cope well, but perhaps due to an illness or the nature of the problem they are facing are not currently coping with a specific situation. The second are individuals who generally find it difficult to deal with life, or may be said to have generally insufficient coping resources (e.g. strong self-esteem, occupationally involved lives, solution-focused mentality, supportive social network, etc.) (Hawton and Kirk 1989). Whilst the problem-solving process can be used with both groups of individuals, it is likely take longer to instil and be successful with the latter population.
There are various situations in which practitioners may use the problem-solving process outlined in this chapter. A specific situation may arise during a session and the occupational therapist may decide that assisting the client to develop a problem-solving strategy would be useful (for example during the break of a social skills group a teenage girl who has anorexia tells her practitioner of her anxiety about going to a friend’s ‘sleep over’ where there will be lots of food). Alternatively, the problems may already be apparent and the practitioner could introduce the concept of the problem-solving process to a client and agree with him/her that it would be useful to focus on problem solving as part of their agreed goals (for example, discussing discharge and return to work with a client who has had an above-knee amputation). Finally, practitioners may find themselves in crisis situations with clients who they may not know well and who are distressed and would benefit from a problem-solving process to assist them to develop solutions for their immediate issues (for example, working in crisis teams, or on the duty desk of a community mental health team). Therefore, regardless of the practice setting that one is working in, problem solving is a skill that should be in every occupational therapist’s repertoire.
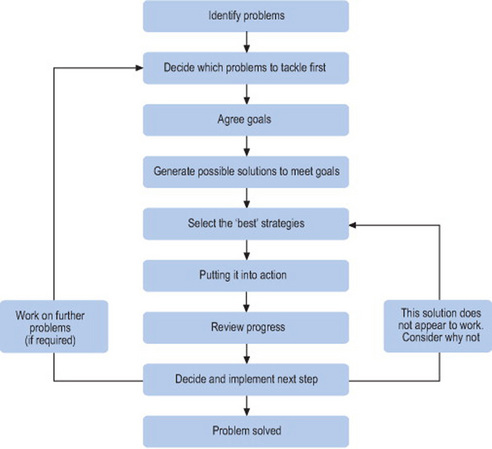
Of course, despite its broad potential for application, problem solving is not the panacea to all situations and is not always an appropriate intervention. There are situations in which problem solving should not be considered. A person who has marked learning difficulties or a severe and enduring mental illness may well be cognitively unable to complete the stages of the problem-solving process (Hawton and Kirk 1989). Similarly an individual who has suffered from a stroke or external head injury may (depending on the nature of the event) be unable to complete the stages of the problem-solving process (see Figure 10.2). And whilst problem solving can be very useful for people experiencing a crisis, in extreme situations (such as in the case of suicidal intent) it is more important to deal with the presenting difficulties, hopelessness and personal disorganisation (thereby ensuring the person’s safety) before attempting to introduce a problem-solving intervention.
The problem-solving process
Identifying problems
The identification of client’s problems is perhaps the most crucial step of problem solving and time should be taken to make sure that all the problems are identified and clearly specified. This is a collaborative process between the practitioner and client (Hawton and Kirk 1989). Identifying problems may seem straightforward, after all clients are unlikely to be seeing an occupational therapist if they did not have any. Often, however, problem identification is not as straightforward as it may first appear. There can be several reasons for this. Clients can present with problems that are unclearly specified (for example ‘difficulty coping at home’, or ‘unhappy on the ward’). In these situations, it is important that the practitioner helps the client to be more specific about the precise nature of the problem. The aim of this process is to help the client be able to specify exactly what the problem is (for example, ‘I am unable to cook dinner for my family and keep the house tidy enough’, or ‘I am finding sharing a living space with strangers very difficult as they want to watch different TV programmes and ask me personal questions I would rather not answer’). Alternatively, clients may present with a range of clinical conditions (such as depression or anxiety, etc.), but be unable to see how these relate to their personal circumstances, or how addressing certain life situations may help their clinical condition. Several strategies can assist clients to become more aware of their underlying problems (Hawton and Kirk 1989):
When the above has been completed and a list of problems has been developed, it is vital that a detailed description of each of the agreed problems is developed. Only then will the practitioner and client be able to set meaningful goals together. Table 10.1 presents an example of a client’s problem list.
Table 10.1 Jack’s problem list
|
2 Frustration at being unable to control his own environment and need for privacy – secondary to problem 1
|
Decide which problems to tackle first
Problem solving is an empowering therapeutic process and ultimately it is up to the client to decide which issue to address first. This should be achieved with support from the practitioner. A client may present a lengthy problem list and it is therefore important that clients prioritise their problems. It is also important that the client commences with a problem that is relatively straightforward to address. An early success in problem solving can increase a client’s self belief and, because success with smaller problems can encourage clients that the bigger ones can also be addressed, maintains motivation for the approach. An example of this can be seen in Jack’s problem list (Table 10.1). Whilst Jack is almost certain to view his continued detention in a secure hospital as his main problem, this is a significant and challenging life issue that is likely to take some time to address and will necessarily involve ‘smaller’ problems to be dealt with first. Helping Jack to achieve his discharge would be better addressed, initially, by supporting him to tackle a more manageable issue (e.g. his boredom) in the present moment. Successfully dealing with that issue may encourage Jack to use a similar problem-solving strategy with other problems and will ultimately support him in his goal of being discharged from hospital.
Agree goals
Having established the priority problems that are going to be addressed, both client and practitioner should then turn their concentration to developing detailed goals to address the identified priority problem. Goal setting in general is discussed in detail elsewhere in this book (see Chapter 8). For the purposes of specific goal setting within the problem-solving process, three key aspects should be kept in mind:
Goals should always be framed in positive terms (for instance what a client will achieve, rather than what they will not do). Setting out goals in this way encourages clients to see that they are moving towards a solution and not avoiding a problem. Goals should be well defined, so that clients know when they have achieved them; well-defined goals are both observable and measurable. Finally, goals need to be realistic, so that they can be achieved. Consider your own experience when you have set personal life goals such as dieting, exercising, etc. Have you ever set unrealistic personal goals? How did you feel when you failed to meet them? Consider what this would be like for some of the clients you work with. To re-emphasise, setting unrealistic goals has the danger of becoming a negative experience for clients and is likely to discourage them from developing their problem-solving skills further.
Generate possible solutions to meet goals
In this stage, the client, with support from their practitioner, lists ways in which their goals could be met. Clients should spend some time on this aspect of the problem-solving process to consider how best to meet their goal. It may be that the most immediate solution is not the best; apart from anything else, it may already have been considered by the client and quite possibly tried before. Strategies for developing lists of possible solutions include brainstorming where the client is asked to write down (or dictate if they have difficulties in writing) all the potential tasks that could result in the target goal being achieved. Clients should be encouraged to list all potential solutions – however implausible. This can lead to a fairly light-hearted component of the session, where a client lets their imagination fly! A side-effect of this process is that the generation of extreme solutions can lead clients to consider possibilities they would otherwise have dismissed (Hawton and Kirk 1989). Once this process has been achieved, clients should list the strengths and weaknesses of each listed solution. Don’t dismiss any idea outright.
At times it may appear that there are two or more equally viable solutions. In such cases it can be useful to generate a list of pros and cons for each solution (Table 10.2). This involves assisting a client to generate and list the advantages and disadvantages of each solution. A further step (which may not always be necessary, but further clarifies the importance of items on the list) involves asking the client to weight each listed item. This is achieved by giving Likert-scale-style ratings to each item listed. The complete pros and cons list therefore gives further information about the potential of a solution by listing both the number of advantages/disadvantages that would result as well as their weight in terms of importance to the client.
Table 10.2 Jack’s pros and cons list, with Likert scale weightings
| Goal: Address boredom: Become more involved in activities in current environment | |
| Potential Solution: Participate three times a week on activities offered to client by occupational therapist |
| Advantages | Disadvantages |
|---|---|
| Will distract me from my current situation (4) | I don’t like the activities that are being offered (8) |
| Will sometimes involve getting out of the ward (7) | I don’t feel like doing anything (2) |
| Will keep my multidisciplinary team happy (2) | I feel scared about meeting different people (3) |
| Will get to meet different people (3) |
Likert scale weighting: 1 = not at all important, 10 = extremely important.
Selecting the ‘best’ strategy
Having developed a list of potential solutions, and where necessary considered their strengths and weaknesses, you then have to decide which strategy is most likely to help solve the problem/achieve the goal. It is important to remember, however, that this is a best-guess scenario. That is, it is the best guess of the person involved (and ideally of all involved) that the strategy selected is the most likely to work. But it remains a process of trial and error; so keep all the potential solutions to hand – the client may yet need to come back and try another!
It is important, however, to choose a strategy that is likely to work. Practitioners should help clients to carefully weigh up the options, balancing the potential of a strategy to succeed with consideration of the personal resources that it requires, and whether a specific strategy is achievable in practice; it may appear the best solution, but if it is not achievable then the client will not be able to carry it out (Figure 10.3). However sometimes the ‘best’ strategy can be very apparent; concrete facts or issues can constrain the options available and the selection of a strategy is therefore limited, or other options may carry too much risk to be realistic in practice.
Putting it into action
Once clients have chosen their strategy, it is time to put it into action. Often this stage is viewed simplistically and skimmed over in problem-solving literature. However, this is the central moment of the problem-solving process; implementing action to solve problems is challenging. The chances are if this were simple clients would already have solved the problem. The fact that a client seeks help to resolve a problem means that, at some level it is difficult. Closer consideration of this stage of the problem-solving process is therefore required.
It is important to understand the factors that can influence clients who are about to put their problem-solving plan into action, and consider ways of supporting them to ensure their greatest chance of success. To do so, practitioners can draw on both the Theory of Planned Behaviour (Ajzen and Manstead 2007), and Task Analysis Theory (Hagedorn 2000).
The Theory of Planned Behaviour
The Theory of Planned Behaviour (Ajzen and Manstead 2007) is a well-established psychological theory that links attitudes with action (behaviour). It can help to inform some of the aspects that make it more likely that a client will be able to undertake their selected problem-solving strategy:
Putting a problem-solving strategy into action is most likely to be successful therefore when it is done quickly, has the social support of meaningful others in the client’s life, and the client believes that what they are about to do is achievable.
Task analysis
Whilst the selected strategy may be the solution to the problem it is usually stated in the form of an overall action (e.g. ‘Go to the gym’). To put the strategy into action requires the task to be broken down into manageable parts: a process known as task analysis. Doing so not only clarifies what has to be carried out, but also makes the task appear more achievable thereby increasing the amount of perceived behavioural control a client has and consequently increasing the chances that it will succeed! Hagedorn (2000) differentiated task analysis from activity analysis (see Chapter 7) as task analysis focuses on larger-scale activities (for example ‘get fit’) whilst activity analysis addresses more focused activities (for example ‘having a bath’).
Hagedorn (2000) presented a six-question system of task analysis that is useful to consider when putting the problem-solving process into action:
Reviewing progress and implementing the next step
Having put the selected strategy into action, both client and practitioner should evaluate how successful it has been. This can normally be easily measured by asking if the client has solved their problem. If the answer to this question is yes, then the process may naturally come to an end; though it can be worth spending some time with the client looking at how to maintain what has been achieved. Alternatively it may be appropriate to select another problem and commence the process again.
If the problem has not been resolved then the client and practititoner should stop and consider why it did not work and what they can learn from the experience: was the strategy wrong, or was it not implemented as planned? Is more time required, or more intensity of whatever was being done? It may be that the answer to these questions is that it was indeed the wrong strategy, but it is worth stopping and taking some time to consider why it did not work. If necessary another strategy can then be selected (taking into account what has been learnt from the last strategy) and the process worked through again. In this way the implementing of strategies to solve problems can be looked on and communicated by the practitioner to the client as a learning process.
Summary
Problem solving is central to occupational therapy practice. It is used both as a theoretical framework to describe the general process of occupational therapy and as a specific technique, based on the cognitive-behavioural frame of reference, that is applicable for use with a wide range of clients.
The problem-solving basis of occupational therapy has been described and presented as a hypothetico-deductive approach (Opacich 1991, Hagedorn 2001) which has been criticised as insufficient for occupational therapy practice (Unsworth 1999). The danger of such criticism is that hypothetico-deductive reasoning may come to be no longer valued within occupational therapy. Instead, this chapter has presented the problem-solving hypothetico-deductive approach as one arm of the decision-making process (see Figure 10.1) and a central component to the process of shared decision making in practice (see Chapter 4).
The problem-solving process was presented as a useful therapeutic skill and intervention. The aim of working through the problem-solving process is twofold: firstly to help clients resolve problems that have proven too challenging to cope with without support. Secondly, to help clients learn the process of problem solving so that they are able to implement it without specific structured support in the future. Whilst routinely associated with working in mental health settings, the problem-solving process is in fact useful in a variety of settings with clients with a range of conditions. Whilst the problem-solving process appears intuitively obvious various factors can be taken into consideration to improve the manner in which this intervention is delivered.
Ajzen I, Manstead ASR, et al. Changing health-related behaviors: An approach based on the theory of planned behavior. In: van den Bos K, Hewstone M, de Wit J, editors. The Scope of Social Psychology: Theory and Applications. New York: Psychology Press; 2007:43-63.
Chambers. The Chambers Dictionary. Edinburgh, UK: Chambers Harrap Publishers, 1994.
Duncan EAS. The Cognitive Behavioural Frame of Reference. Duncan EAS, editor. Foundations for Practice in Occupational Therapy, 4th edn. Edinburgh, UK: Elsevier/Churchill Livingstone. 2006:217-232.
Dutton R. Clinical reasoning in physical disabilities, 2nd edn. Baltimore, MD: Williams and Wilkins. 2000.
D’Zurilla TJ, Nezu AM. Problem-solving therapy: A social competence approach to clinical intervention, 2nd edn. New York: Springer; 1999.
D’Zurilla TJ, Nezu AM. Problem-solving therapies. In Dobson KS, editor: Handbook of cognitive-behavioral therapies, 2nd edn, New York: Guilford, 2000.
Hagedorn R. Foundations for Practice in Occupational Therapy, 3rd edn. Edinburgh, UK: Churchill Livingstone. 2001.
Hagedorn R. Tools for Practice in Occupational Therapy. Edinburgh, UK: Churchill Livingstone, 2000.
Hawton K, Kirk J, et al. Problem-solving. In: Hawton K, Salkovskis PM, Kirk JW, editors. Cognitive behaviour therapy for psychiatric problems: a practical guide. Oxford, UK: Oxford Medical; 1989:406-426.
Opacich KJ. Assessment and informed decision making. In: Christiansen C, Baum C, editors. Occupational Therapy: Overcoming Human Performance Deficits. Slack: Thorofare; 1991:355-374.
Paterson M, Summerfield-Mann L. Clinical reasoning. Duncan EAS, editor. Foundations for Practice in Occupational Therapy, 4th edn. Edinburgh, UK: Elsevier/Churchill Livingstone. 2006:315-335.
Roberts AS. Clinical reasoning in occupational therapy: Idiosyncrasies in content and process. The British Journal of Occupational Therapy. 1996;59(8):372-376.
Robertson LJ. Clinical reasoning. Part 1: The nature of problem solving, a literature review. The British Journal of Occupational Therapy. 1996;59(4):178-182.
Unsworth C. Cognitive and Perceptual Dysfunction: A Clinical Reasoning Approach to Evaluation and Intervention. Philadelphia, PA: FA Davis, 1999.