Chapter 8 Goal Setting in Occupational Therapy
a client-centred perspective
Overview
This chapter focuses on implementing client-centred goal setting, illustrating the process for occupational therapy services. The current standing of goal setting in occupational therapy is presented, underscoring the challenges practitioners face to enact client-centred practice during goal setting. Using as a guide the three phrases of goal setting, (1) identifying client concerns, (2) formulating client-centred goals, and (3) evaluating goal achievement, the knowledge and skills to enact client-centred goal setting are presented, with particular attention to documentation.
Goals and goal setting
‘Humans yearn for the “unattainable” and pursue practical goals; they marshal all possible resources against great odds to reach the most grand, and sometimes the most simple, objectives.’ (Crabtree 2000: 122)
Occupational therapists focus on facilitating a client’s engagement in daily life activities that possess meaning to the client. Essential to the process is client-centred practice, a collaborative approach that respects each client’s perspective, particularly when negotiating goals that become the focus for assessment, intervention and evaluation (Law et al 1995, Sumsion 2000). During negotiation, practitioners and clients explore all daily life activities of concern because even the most mundane and commonplace activities possess the potential for clients to make and express meaning in daily life (Crabtree 2000). Subsequently, goals are identified that express the future state clients hope to experience in regard to their daily life activities.
Although goal setting is common in practice, overwhelming evidence indicates practitioners require additional skill to negotiate and document goals that are client-centred and reflect engagement in daily life activities (Neistadt 1995, Northen et al 1995, Nelson and Payton 1997, Andrew et al 1999, Lund et al 2001, Barclay 2002, Hanna and Rodger 2002, Palmadottir 2003, Eschenfelder 2005). For example, documented goals sometimes reflect the practitioner’s plan, such as Conduct home evaluation & recommend adaptive equipment or Refer to social services for meal programme. Other times, practitioners use the SMART acronym, attempting to ensure goals are Specific, Measurable, Achievable, Realistic and Timely (SMART). Often, though, goals are unclear and not client-centred. How then should practitioners frame goals for intervention?
What are goals?
Most persons think about what they hope to accomplish, whether relatively straightforward tasks, such as tidying the living room, scheduling a dentist appointment, or paying the monthly bills, or more complex activities in which they desire to participate in the future, such as playing the guitar, driving a car, or operating a construction crane. Hopes may focus further in the future, centring on desired roles, such as a partner, parent or employee. Hopes also may reflect a person’s dreams, such as scoring the winning goal during the World Cup or touring the world as a rock star. All of these hopes, though, are often referred to as goals, making little distinction between ‘things to get done today’ and ‘wishful dreams for the future’. These ‘goals’ comprise a continuum, from simple tasks to global aims (Geen 1995) (Figure 8.1). What then along this continuum would be considered a goal during occupational therapy intervention?
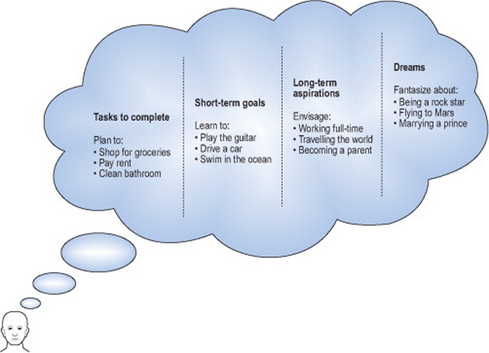
Figure 8.1 A continuum and hierarchy of tasks, goals, aspirations and dreams
Park 2006, with permission
For intervention, a goal is an end-state (an outcome) that expresses what a person hopes to accomplish, is considered attainable, and requires some degree of effort by the client to attain (Schut and Stam 1994, Geen 1995, Quinn and Gordon 2003). Thus, a goal reflects a short-term (but significant) accomplishment rather than a task that is relatively easy to complete or a dream that is unrealistic to attain. Moreover, a goal signifies something in the near future to be accomplished by the person that he or she cannot accomplish now (Quinn and Gordon 2003) and that reflects the attainment of a standard of proficiency within a designated time frame (Locke and Latham 2002).
Benefits of setting goals with clients
Why should practitioners use goal setting? First, they have a professional responsibility to provide individualised services, focusing on the client’s daily life activities of importance (Wallen and Doyle 1996, College of Occupational Therapists 2000, Creek 2003). Client-centred practice is a cornerstone of occupational therapy intervention and as Rebeiro (2000) stated ‘[If] occupational therapy strives to be client-centred, the profession must allow practice to be guided by “client visions”’ (p. 13). Second, focusing on client goals promotes effective use of time and resources (Welch and Foster 2003, Wressle and Samuelsson 2004). Third, actively involving clients during goal setting helps them to understand the focus of intervention (Welch and Foster 2003) and provides a specific direction to intervention (Conneeley 2004). Finally, goals that evolve from client concerns provide a means to identify small changes that are meaningful to clients (Wallen and Doyle 1996) and facilitate the evaluation of outcomes (Wressle et al 2003).
Whilst limited in scope and based in physical rehabilitation, research evidence supports the premise that clients who set goals achieve better outcomes than those who do not (Ponte-Allan and Giles 1999, Wressle et al 2002a). From his review of published research, Wade (1998) concluded reasonable evidence exists that: (a) more behavioural change occurs when goal setting is used; (b) change is more likely to occur when goal setting is reinforced with specific interventions intended to facilitate the desired change; and (c) setting goals may improve long-term effectiveness. Locke and Latham (2002), from their summary of evidence regarding goal setting in the business field, identified the following characteristics:
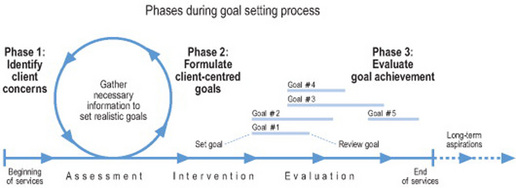
Although successful implementation of goal setting has occurred within occupational therapy services (Rosa and Hasselkus 2005, Sumsion 2005), most research indicates that practitioners need to involve clients more during the goal-setting process and further develop their skills to negotiate and formulate client-centred goals (Northen et al 1995, Neistadt 1995a, Nelson and Payton 1997, Andrew et al 1999, Lund et al 2001, Barclay 2002, Hanna and Rodger 2002, Palmadottir 2003, Eschenfelder 2005). Indeed, the top three barriers to client-centred practice identified by occupational therapists all centred around goals: (a) practitioners and clients identify different goals; (b) practitioners cannot accept clients’ goals due to practitioners’ values and beliefs; and(c) practitioners are uncomfortable allowing clients to choose goals (Sumsion and Smyth 2000). Rosa and Hasselkus (2005) pointedly concluded: ‘[In] spite of the recent professional emphasis on collaborative therapeutic relations … these ideals may continue to elude occupational therapists, perhaps much of the time.’ (p. 206). Given this, how can practitioners successfully implement client-centred goal setting? To address this challenge, this chapter illustrates the process in three phases: (a) identifying client concerns; (b) formulating client-centred goals and (c) evaluating goal achievement (Figure 8.2).
Collaborating with clients: the goal-setting process
‘[T]here [are] two different types of goals: those that were negotiated with the [client] and those that were not.’ (Playford et al 2000: 494)
Client-centred practice and goal setting
Occupational therapists should acknowledge that clients are experts about their lives, capable of indicating what is of importance and concern (Gage 1994, Blackmer 2000, Guidetti and Tham 2002). Everyday, people seek specialists to help resolve problems that they identified as important, for example, enlisting the services of a builder, accountant or lawyer (Sumsion 2006a). This is comparable to a client receiving occupational therapy services – he or she identifies ‘problems’ for which the practitioner can provide specialist advice. Furthermore, the client identifies the problem and the practitioner provides the expertise, similar to the person who identifies (and prioritises) a leaky kitchen tap and hires a plumber to fix it. As Sumsion (2006a) clearly stated: ‘If a therapist cannot accept a person’s right to be a client and all that this right entails then he or she cannot be a client-centred therapist.’ (p. 41).
Practitioners should recognise that clients might identify goals that place them at risk for failure or injury (Law et al 1995). As long as clients are competent to understand the risk or chance for failure and practitioners are not acting in a manner that places clients in perilous circumstances, practitioners should recognise that undertaking such a risk is often a valuable learning experience for clients. Clients’ preferences should be respected as long as realistic concerns do not exist (Blackmer 2000, College of Occupational Therapists 2000).
Practitioners also should consider that client participation during goal setting exists along a continuum – not all clients want to participate equally during the process (Lund et al 2001, Wilkins et al 2001, Palmadottir 2003). Some clients are comfortable sharing their concerns and making decisions whilst others are challenged to make simple choices (Wilkins et al 2001). From research conducted in physical rehabilitation settings, Lund and colleagues (2001) discovered three categories of clients: (a) participants – those who participate in shared decision-making to an extent that meets their need; (b) occasional participants – those who occasionally participate but tend to allow practitioners to make the primary decisions; and (c) relinquishers – those who are not interested in participating and readily accept practitioners’ decisions. Lund and colleagues further discovered that practitioners were inclined to use the same approach for each client, encouraging all clients to participate regardless of a client’s preference. Sumsion (2005), during her review of client-centred practice, revealed further characteristics associated with goal setting: Persons more likely to participate in shared decision-making tend to be younger, more educated, and from a higher social class whilst persons less likely to participate are those with acute and severe illnesses or whose cultural practices sanction decision making by family consensus or the family patriarch.
Phase 1: Identifying client concerns
‘Eliciting and incorporating [clients’] views and setting goals are demanding and potentially time-consuming activities.’ (Parry 2004: 679)
As the practitioner establishes rapport and gathers information about and shares information with the client during the initial assessment, the discussion should evolve to identify what is of concern and important to the client regarding his or her engagement in daily life activities (Park 2006). This process should clearly establish the client’s concerns and priorities; these may not be in agreement, however, with the practitioner, the client’s family, or the reason for the referral (Sumsion 2006b). The objective is to understand the client’s (and others’) perspective. To do so, the practitioner should listen carefully to the client and help the client to identify and clarify his or her concerns.
When identifying concerns, all areas of a client’s engagement in daily life activities, as appropriate, should be explored, including personal care, domestic, productive, play/ leisure, and social activities (Park 2006). The client and practitioner work together to identify specific daily life activities of concern to the client and establish which are priorities. Often, these are the activities considered a challenge by the client and for which a change is desired (Park 2006). Whilst some practitioners have raised concerns about focusing on client ‘problems’ (Halladay 2001, Parry 2004), the intent is not to identify what is wrong; rather, the intent is to listen and solicit areas of concern from the client’s perspective. The practitioner should help the client to identify immediate, realistic concerns with daily life activities. Clients benefit far more if intervention is based in the ‘here and now’ of daily life and targets issues that could be more ‘immediately’ resolved (Park 2006). Questions such as the following can help clients identify specific concerns about their engagement in daily life activities.
Some clients may state their concerns as ‘to go home’ or ‘taking care of myself’. Practitioners should not be satisfied with such general statements and should explore these further (Neistadt 1995). For example, a parent (also considered a client) shares her concern that her child is not performing successfully in school. The practitioner needs to assist the parent to identify specific school activities, such as ‘My daughter doesn’t play with any friends during the break (recess)’ and ‘She takes too much time answering written questions – her handwriting is so laborious’.
Evidence exists that informal means of eliciting clients’ concerns (and goals) are more common than methods based on structured assessments (Neistadt 1995, Wressle et al 2002b, Palmadottir 2003). Although informal discussion is important when establishing therapeutic rapport, practitioners vary in their interview skills and styles; this can affect the quality and extent of information gathered (Neistadt 1995). Because formal interview methods identify a broader range of concerns and lead to more distinct goals (Pollock and Stewart 1998, Bodium 1999, McColl et al 2000, Wressle et al 2002b, 2003, Donnelly et al 2004), practitioners should consider adopting formal methods to elicit client concerns.
Although various methods exist and the choice depends on each situation, the Canadian Occupational Performance Measure (COPM) (Law et al 2005) is a standardised assessment designed to elicit the client’s perspective of problems and priorities with specific daily life activities. The COPM has been used successfully with a variety of clients, including children (and their parents and teachers), adolescents and adults with physical, cognitive and psychosocial health conditions (Carswell et al 2004). Because setting goals requires identifying current ‘problems’ and the COPM prompts clients to consider framing their ‘problems’ in terms of daily life activities, the COPM is well suited to identify client concerns.
During initial discussions with clients, goals should not be the primary focus. Before goals are formulated, the client and practitioner need to possess all necessary information on which to base realistic goals (Law et al 1995, Sumsion 2006b). Moreover, clients (and practitioners) need to appreciate the realities and limitations of existing resources (Sumsion 2006b) and some clients may need to experience their current ‘problems’ in daily life activities before they can identify realistic goals (Chan and Lee 1997, Spencer and Davidson 1998, Bodium 1999, Playford et al 2000, Guidetti and Tham 2002). As Sumsion (2006b) cogently stated: ‘The client-centred approach requires that time and energy be dedicated to the analysis and understanding of the assessment information before the goals are set.’ (p. 26). Therefore, beginning the assessment process by asking a client ‘What do you hope to achieve during occupational therapy?’ or ‘What are your goals for therapy?’ is not recommended (Park 2006). These questions can be difficult to answer, particularly if the client is experiencing the onset of a new health condition, and are more appropriate after the client and practitioner possess a clearer picture of the client’s health condition and potential for change, its effect on the client’s engagement in daily life activities, and the available support and resources.
Sometimes, clients may not be able to participate in a discussion or readily indicate their concerns. Practitioners should make every effort to solicit the viewpoints of principal persons in the client’s life in order to identify potential concerns (and goals) that are in the client’s best interest. Further, every effort should be made to help the client understand the identified concerns and provide an opportunity to agree (or not).
Differences in priorities
Differences of opinion regarding concerns (and goals) will exist amongst practitioners, clients, family members and others; these need to be acknowledged and negotiated (Hanna and Rodger 2002). Although goal setting is client-focused, this does not mean practitioners will always agree with the client’s priorities – at times, the practitioner will need to inform the client that he or she is unable to support the client’s priority. As Parry (2004) stated: ‘Accounting for why it is not…relevant whilst avoiding outright dismissal of a [client’s] stated preference may involve considerable interactional time and effort.’ (p. 675).
Gerard experienced a severe TBI 3 months ago and currently receives community services. When asked about his concerns, Gerard insists he wants to drive again. His practitioner empathises with him but also recognises that Gerard’s concern does not readily convert to a realistic goal that could be achieved over the next 4 months (the anticipated course of intervention). She skilfully shares this perspective with Gerard (without dismissing his long-term aspiration to drive) and continues to collaborate with Gerard to identify concerns that are realistic and potentially achievable over the next 4 months.
Clients and family members may differ in their priorities for intervention. For example, when asked to select which activities should be the focus of intervention, parents tended to prioritise academic tasks such as printing and drawing whereas their children’s preferences leaned more toward self-care and leisure activities (Missiuna and Pollock 2000). When clients and family members do not agree, practitioners need to negotiate an equitable solution before goals can be set, particularly when they propose fostering a client’s ability to engage in desired daily life activities and the client’s family may be more interested in protecting the client from harm, real or imagined (Foye et al 2002).
Phase 2: Formulate client-centred goals
Once a client’s concerns and priorities are identified and sufficient information has been gathered, the practitioner and client work together to identify realistic goals that could be achieved over the course of intervention (Park 2006). To ensure that a goal is client-centred, it should describe a client’s future experience in a specific daily life activity that is relevant and meaningful to the client (Park 2006). Goals should reflect specific daily life activities in which clients need or want to engage, such as safely preparing evening meals, getting dressed in the morning on their own, playing with friends after school at the local park, successfully completing homework on time, engaging in fun social activities at the local leisure centre, or managing their own medications throughout the week. Asking the question, ‘So what difference does performing this activity mean to the person?’ (Randall and McEwen 2000: 1202) can help identify if a goal is client-centred.
Moira, a 34-year-old with learning difficulties, lives with her mother who plans to work an evening shift. Moira remarked that she wants to prepare hot meals when her mother is away. Her mother (whose interests must also be considered) believes that Moira could stay by herself but she does not want her to use the electrical or gas appliances; instead, she wants hot meals to be delivered. The practitioner agrees that Moira could stay by herself but she also believes that Moira has the potential to safely use appliances. If Moira’s mother agrees to Moira preparing hot meals, a goal could be set, such as ‘Moira to safely prepare hot meals at home without supervision’. If Moira’s mother does not agree and arranges for hot meals to be delivered, no goal could be set as no significant change will occur with Moira’s engagement in a daily life activity, particularly as the delivery of hot meals represents a service Moira will receive, not a goal she will achieve. In this case, further negotiation must occur between all three to identify and agree to a client-centred goal for intervention.
Framing goals from the client’s perspective also helps ensure that goals are client-centred. The practitioner should work with the client to ‘match’ the goal to the client’s description of the problem (Parry 2004), and use phrases that reflect common, everyday language. Thus, a goal might state ‘Louvain to sit comfortably in her wheelchair throughout the day with no significant red areas developing on her bottom’ rather than ‘Louvain to prevent development of decubiti whilst in wheelchair’. In this case, the phrase ‘sitting comfortably throughout the day’ is Louvain’s personal perspective of the ‘problem’ and the practitioner ‘translated’ the importance of preventing decubiti into the phrase ‘no significant red areas developing’. Concerns do exist that goals framed from the client’s perspective are not ‘objective’ or ‘measurable’ (Parry 2004). On the contrary, client-centred goals, in addition to being more relevant to clients, are intrinsically more ‘testable’ than conventional goals created using a formula (Quinn and Gordon 2003).
Specific elements of goals
Because client-centred outcomes for intervention focus on persons engaging in daily life activities within various environments (Figure 8.3), goals should reflect this premise. Thus, documented goals should contain three elements: the person, a daily life activity, and a context (Table 8.1).
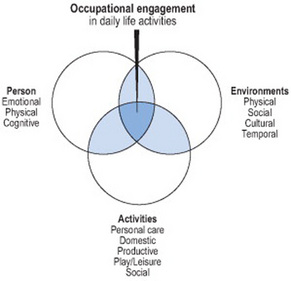
Figure 8.3 Occupational engagement is the interaction between a person, activities and environments.
Park 2006, with permission
Table 8.1 Components and characteristics of client-centred goals
| Components of client- centred goals | Characteristics of goals | |
|---|---|---|
| A PERSONengaging in a specific DAILY LIFE ACTIVITY within a specific CONTEXT |
Client to consistently check for oncoming traffic and wait for traffic lights when crossing road to corner shop throughout the week. |
Person
The person for whom the goal is set and for whom a change is anticipated should always be identified in the goal. Although this most often is the person with a health condition (i.e., the client, service user or patient), the person may be a family member, carer or another person involved in the client’s daily life and with whom the practitioner is working (Park 2006). In many instances, the goal focuses on a carer’s or parent’s ability to care for and interact with the client, such as ‘Mother to safely and with confidence bathe her child each day on her own’ or ‘Carer to help client in and out of bath at home without undue effort and only providing help as necessary’.
Daily life activity
The goal should specify the anticipated ‘level’ of engagement in a specific daily life activity and describe the expected quality of the client’s experience, focusing on the manner in which the client engages in the activity and, as appropriate, the client’s feelings about engaging in the activity. The anticipated activity should be of sufficient challenge given the client’s abilities (Williams et al 1999, Quinn and Gordon 2003) and clearly identify the next ‘level’ of engagement the client might achieve. Practitioners might imagine a client starting on a step (as described later, this reflects the client’s current status) (Figure 8.4). The client and practitioner decide where, on the steps ahead, the client hopes to be in the future – this step represents the goal. In deciding which step ahead is the goal, the magnitude of change is specified – an essential feature of goal setting. To credibly evaluate client outcomes, clients and practitioners need to identify exactly which ‘step’ represents the goal, such as ‘Client to arrive safely on the second step from the top’ or ‘Client to climb steadily halfway up the steps’. One exception does exist – goals may reflect maintenance of a client’s engagement in daily life activities. When improvement is not expected, particularly in the presence of degenerative conditions, goals may focus on maintaining a client’s current status (Cott and Finch 1991, Wallen and Doyle 1996).

Figure 8.4 When setting goals, exactly how ‘far’ a client hopes to ‘go’ (in relation to the starting point) must be explicitly identified.
Park 2006, with permission
Nisha, a 32-year-old woman who experienced the onset of Guillain-Barre syndrome 6 months ago, is unhappy with how she applies her make-up. When asked to elaborate, Nisha shares that she frequently drops items, smears her make-up, gets frustrated with the amount of effort for disappointing results, and often asks for help. Rather than suggest a more conventional goal, such as ‘Nisha to independently apply make-up’, the practitioner collaborates with Nisha, formulating a goal from Nisha’s perspective: ‘Nisha to apply make-up by herself and be pleased with the effort and result’.
Context
The environmental conditions under which the person will engage in the activity should be described. Aspects such as where, with whom, when, or how long may be included, particularly as qualitative differences with a person’s engagement in daily life activities may occur that directly reflect the environment in which the person engages (Park 2006). For example, Aiden, who experiences schizophrenia, will shop for items at the corner shop but is apprehensive about shopping at the nearby superstore and declines to shop there (although he would like to). The goal, ‘Aiden to shop for groceries at super store over the course of a month and feel pleased with accomplishment’, reflects the next level of challenge for Aiden – shopping within a different environment and over a specified time period. Although including contextual information may require additional words, their inclusion enables practitioners to more precisely determine if a goal is achieved (Randall and McEwen 2000).
Identifying current status to assist with goal formation
‘A well-defined problem converted into a goal guides the [intervention] plan and the interventions in a direction that is essential for the [client].’ (Wressle et al 2002a: 34)
When formulating goals with clients, practitioners should identify (and document) the client’s current status in relation to the goal (Table 8.2). Current status is the starting point, a brief description of the ‘problem’ the client is experiencing with the specific daily life activity and that the client and practitioner agree is amendable through intervention (Park 2006). Identifying current status helps to: (a) identify the qualitative features of a client’s experience in daily life activities that will become a target for intervention; (b) ‘quantify’ the expected magnitude of change during intervention; and, (c) determine if the goal was achieved when evaluating the outcome.
Table 8.2 Examples of current status and client-centred goals. After Park 2006, with permission
| Current status | Client-centred goal |
|---|---|
| Client repeatedly washes the same item until prompted to stop and start washing another item, taking an inordinate amount of time to finish washing up | Client to wash up all items on the bench within a reasonable amount of time and without prompting |
| Client is bullied by other ward patients for cigarettes and readily gives them away without protest | When on the ward, client, in an assertive yet considerate manner, to decline to share cigarettes when he does not want to |
| At day care, child often wets himself without indicating he needs to toilet | Throughout the morning, child to consistently indicate (without prompting) need to use toilet before wetting himself |
| Spouse says he is nervous using the hoist at home to move client in/out of bed and declines to use it unless someone else is present | Spouse to safely use hoist to move client in/out of bed and feel confident doing so on his own |
Most often, current status describes the client’s occupational performance, that is, the manner in which the client currently engages in a daily life activity. Essentially, if the client was videotaped participating in the activity, current status would reflect important highlights of the client’s performance that were challenging and which are expected to change during intervention – that is, the occupational ‘problem’ the client is experiencing. Note: This is not the same as the cause of the problem. Current status reflects the client’s experience engaging in a daily life activity, not the reason why he or she is encountering the problem. Moreover, current status may also identify the feelings the client experiences whilst engaging in the activity.
Additional considerations when setting goals
Whilst a client’s performance of specific daily activities is often the primary focus of intervention, the fact a client can perform an activity may not be the only desired outcome. Often, a client’s feelings regarding his or her experience in specific activities are an important outcome to consider and include in the goal. This does not mean, however, the goal reflects a change in the client’s general feelings or mood, such as sadness, happiness, discouragement or joy. Rather, the client’s feelings about his or her experience in a specific daily life activity (termed ‘occupational disposition’) are the focus. For example, Dorothea currently declines to ride the bus to the town centre and conveys she doesn’t feel confident to do so on her own. If the goal were to solely focus on Dorothea’s performance, such as ‘Dorothea to ride the bus independently into town’, an important concern is ignored. Moreover, Dorothea might well ride the bus into the city centre on her own, effectively achieving the stated goal, but feel miserable whilst doing so. Such an outcome would not be acceptable to Dorothea (or the practitioner). Thus, Dorothea’s feelings about her confidence are essential to target during intervention and include in the goal, such as ‘Dorothea to ride the bus into town centre on her own and feel confidence doing so’. If a client’s occupational disposition is neither likely to change over the course of intervention nor of primary concern to the client, a description of the client’s feelings is not required.
Because occupational disposition is difficult to quantify, how can these goals be reliably evaluated? If the goal is formulated such that the client can respond with a simple ‘yes’ or ‘no’ response, the goal can be evaluated (Table 8.3). For example, Oliver experiences extreme anxiety whilst attending community outings and often declines to go (his current status). If the goal was ‘Oliver to be less anxious during community outings’, two concerns exist: (1) The goal does not specify the magnitude of expected change, an essential requirement for goals; and (2) Intervention may well help Oliver experience less anxiety but is this lesser degree acceptable to him? To address these concerns, a goal could be set ‘Whilst attending community outings to the local leisure centre, Oliver to enjoy the outings with a manageable degree of anxiety’. When the goal is reviewed, Oliver can respond with a definitive ‘yes’ or ‘no’ when asked if he enjoyed the outings and if he experienced a manageable degree of anxiety.
Table 8.3 Examples of terms to distinguish the difference in a client’s feelings about experiencing a daily life activity between ‘now’ and in the ‘future’.
| Occupational disposition | |
|---|---|
| Current status | Client-centred goal |
| painfulnot satisfied very anxious, unacceptable anxiety unmanageable anxiety unreasonable amount of timenot confident intolerable, not tolerablenot enjoyable, not funembarrassed | significant reduction in pain satisfied, to client’s satisfaction acceptable degree of anxiety manageable level of anxiety reasonable amount of time confident, reasonably confident tolerable enjoyable, fun not embarrassed |
Park 2006, with permission.
If safety whilst engaging in a daily life activity will be a target of intervention, the client’s risk for personal injury or damage to the environment should be described. For example, when Fiona prepares hot meals in her kitchen, she frequently does not attend to what she is doing, spilling and dropping hot materials and sharp objects. The goal in this case could be ‘Fiona to consistently prepare hot meals with an acceptable degree of risk to her and her partner’. Note: When the goal is evaluated, Fiona and her partner would identify if any safety concerns existed and if these are acceptable.
Practitioners are accustomed to setting goals that focus on amount of assistance, such as ‘Client will be able to dress with minimal assistance’. Is independence the most important factor to the client (Cederfeldt et al 2003)? Or does the notion of independence serve the professional’s need to evaluate progress (Crabtree 2000)? Other factors of equal or greater importance may exist for clients, such as amount of effort, timeliness, efficiency, or the quality of the process or outcome (Park 2006). Setting goals that focus exclusively on independence may not illustrate the meaning of the activity to the client nor indicate important and beneficial qualities that could change during intervention.
Goals may also focus on engaging in a routine of daily life activities as clients may be quite capable of performing an activity but the challenge is sustaining participation over time. For example, Jackson will prepare nutritious meals for a few days in a row but then reverts to his previous habit of eating non-nutritious food. The goal could focus on sustaining a routine of meal preparation, such as ‘Jackson to consistently prepare nutritious and satisfying meals throughout the month’. Table 8.4 provides additional considerations when documenting goals.
Table 8.4 In order to evaluate goals, attention to detail is required whilst documenting.
Additional Considerations When Documenting Goals
| (based on Park 2006, with additional references as noted) | |
| “Word selection is also important in describing change and the measurement of change.” (Sames 2005, p. 92) |
|
| Use the word TO or will; avoid the phrase will be able to | |
| The phrase will be able to is not essential and implies the person can do the activity but might choose not to (Quinn and Gordon 2003, Randall and McEwen 2000) | |
| Current Status When shopping for groceries on his own at the local corner store, client usually returns with 3–4 non-essential items; essential items are frequently not included. |
Client-Centred Goal NO :Client will be able to shop on his own. YES :Over the course of a month, client to shop on his own, consistently returning with essential items and only occasionally 1–2 non-essential items. |
| Ensure goals are clearly understood; avoid professional language | |
| Goals should be stated so that clients understand them. | |
| Current Status When attempting to write her name on lined paper, child holds her pencil with a fisted grasp; her signature is illegible. |
Client-Centred Goal NO:Child to display age-appropriate tripod grasp. YES:Child to neatly write her name on lined paper, using a three-point grasp to hold her pencil. |
| Identify specific goals; avoid goals that are broad | |
| Broad goals do not provide information about specific needs or how to guide intervention most relevant to the client (Forker et al 1999) | |
| Current Status Client has never been employed and is unaware of process to search for and obtain a job. |
Client-Centred Goal NO:Client will obtain a job YES:When applying onsite for a job, client to legibly, thoroughly & accurately complete application by himself. |
| Focus on one activity per goal; avoid including multiple activities | |
| Focusing on one activity makes it easier to monitor change over time. | |
| Current Status Client receives help of one person to get in/out of bed and does so in an unsafe manner. Client receives help of two people to transfer to/from toilet at home. Client receives help of two people to get him in/out of bathtub in a safe manner. |
Client-Centred Goal NO :Client will be able to safely transfer with assistance of one person on/off bed & toilet and in/out of chair & bathtub. YES:Client to receive help of one person to get safely in/out of bed. YES:Client to safely transfer with help of one person on/off toilet. YES:Client to safely transfer with help of one person in/out of bathtub. |
| Focus on client achievements; do not include the intervention plan | |
| Including information about the intervention plan invalidates the goal setting process. Note: Adaptive equipment is not considered an intervention plan; rather, it specifies the manner in which the client will perform the activity. | |
| Current Status Carer doesn’t know how to use bathlift safely with client. |
Client-Centred Goal NO :Carer to be educated to safely use bathlift. YES :Carer, by herself, to safely & confidently use bathlift with client at home. |
| Focus on what clients will do; avoid focusing on a reduction in behaviour | |
| Goals should specify what a client will do, not what he won’t do (Schut & Stam 1994). | |
| Current Status Client frequently hits out at peers and occasionally spits when playing together on the playground. |
Client-Centred Goal NO: Client will not spit whilst playing with peers on the playground. YES: Client to play cooperatively in a socially suitable manner with his peers on the playground. |
| Focus on activity engagement; avoid including information about underlying capacities | |
| Information about a client’s physical, cognitive, or emotional capacity should not be included—a change in capacity is only a means to goal achievement, not an end (Moorhead & Kannenberg 1998). | |
| Current Status Client frequently misses appointments throughout the week and, on occasion, has shown up on the wrong day. |
Client-Centred Goal NO :Client will increase memory to complete appointment diary. YES : Client to arrive to all appointments on time over the course of a month. |
Time frame for realistic goals
As clients and practitioners formulate goals, the time frame of intervention must be considered. To effectively monitor change, goals should reflect accomplishments that clients could realistically achieve whilst receiving intervention; this contrasts with aspirations to be achieved after discharge. To distinguish the difference, short-term goals reflect what might be achieved over the course of intervention and long-term aspirations focus on the client’s life after intervention. When initially discussing goals, clients frequently focus on long-term aspirations. Practitioners should help clients identify ‘smaller’ short-term goals for intervention that subsequently lead to the achievement of long-term aspirations (McClain 2005).
Each short-term goal should reflect an accomplishment that could be potentially achieved within 6 months or less. As such, a review date should be designated, at which time it will be determined if the goal was achieved. Two to five short-term goals may be in ‘play’ at any one time and as goals are achieved, additional ones may be identified. Moreover, short-term goals are not set in stone – some goals may be modified or even abandoned (Hass 1993, Blackmer 2000, Quinn and Gordon 2003, Eschenfelder 2005). As clients gain an understanding of their capacities or re-evaluate the meaningfulness of specific daily life activities, the goal-setting process should accommodate their shifting perspectives.
When asked about his priorities, Raji, a 19-year-old in-patient rehabilitation client with an incomplete C-6 spinal cord injury, identifies one priority is to complete a vocational course and receive a First Diploma in Sport. Because this priority cannot be achieved before discharge, it does not make sense to set a goal that states ‘Client will successfully complete vocational course’. The practitioner, however, acknowledges Raji’s long-term aspiration and together they review the daily life activities required to attend college, such as writing papers, giving presentations and using public transportation. They decide that using a computer to write papers and riding public transportation to college would be meaningful and significant challenges to address. Together, they formulate two goals: ‘Using a computer, Raji to accurately type a 2-page paper within a reasonable time’ and ‘Raji to successfully negotiate the bus from hospital to college, arriving on time and satisfied with effort required’.
Phase 3: Evaluating goal achievement
‘When the client’s need or desired behavior is successfully identified in the [goal], the task of selecting suitable intervention is straightforward’ (McLeod & Robnett 1998: 29).
Although each goal is reviewed at a specified date, to guide and monitor intervention, goals should be referred to regularly during intervention (Cott and Finch 1991, Quinn and Gordon 2003). At the review date, the client and practitioner together should determine if the goal was achieved. All available information can be used to evaluate the outcome, including client self-report, and family members, partners, carers, or other persons can provide relevant information. As well, the practitioner may observe the client in the specified activity, gathering information with which to determine if the goal was achieved. No matter the means, evaluating goal achievement is a collaborative effort between the client and practitioner. It is then the practitioner’s responsibility to document the outcome, providing a complete description such that any reader could compare the outcome to the current status and goal, and conclude if the goal was achieved. Additional information to substantiate why the outcome is important may also be included. Table 8.5 outlines how a client’s current status, goals and outcomes are documented when using client-centred goal setting.
Table 8.5 An example of documentation based on client-centred goal setting. After Park 2006, with permission
Background: Irisa, a retired 72-year-old shopkeeper, lives with her husband of 47 years. Irisa has an extensive history of major depression (her last hospitalisation occurred 2 months ago) and she is currently receiving community services. Her husband is concerned about her favoured activities of preparing meals, attending music group, and taking care of their dog; Irisa expresses hopelessness that she can reclaim her life but identifies it would be nice to help out more around the house and to enjoy life once again.
Documentation
| Current status | Client-centred goals | Client outcomes |
|---|---|---|
| Client requires much encouragement from husband to assist with preparing evening meals. She often declines to help, stating she just can’t do it 01.02.00 |
Irisa to help with preparing evening meals throughout the week with only a bit of encouragement from her husband 01.03.00 |
Irisa reports she helped prepare evening meals with her husband’s occasional encouragement. Irisa’s husband concurs and says he is pleased with the progress 01.03.00 |
| Irisa’s husband prepares lunch for his wife as she will not prepare any food when he is away at work. Irisa says she feels overwhelmed with the prospect of preparing anything to eat 01.02.00 |
For Monday through Friday, Irisa to consistently prepare a satisfying and nutritional lunch 01.04.00 |
Irisa and husband report she prepared four nutritious lunches that she liked. Irisa said she now feels she will continue to make lunch but that occasionally she might not feel like eating 01.04.00 |
| Irisa stays at home during the day and will not attend the twice-weekly music group in which she previously participated 01.02.00 |
Irisa to consistently attend music group twice a week for 2 weeks and enjoy herself 01.05.00 |
Irisa reports she attended 4 music groups over the past 2 weeks and felt good about going 01.05.00 |
| Irisa does not feel able to look after the family dog. The dog is currently living nearby at her daughter’s house 01.05.00 |
Irisa to take care of her dog at her home over the course of a month and feel confident in doing so 01.08.00 |
Although Irisa says she is still apprehensive, she did assume all care for their dog during the past month and would like to continue keeping the dog at home 01.08.00 |
Conclusion
As Welch and Foster (2003) discovered, time and support are needed to assist occupational therapists to incorporate client-centred goal setting into traditional health-care services (and likely others). Goal setting is not just asking clients to identify their goals – it requires practitioners to interlace therapeutic rapport with professional skills to enable clients to find meaning in everyday life activities and to support client efforts to achieve the most ordinary desire and grandest dream. Giving voice to clients through goal setting allows them to experience a key benefit of occupational therapy – engagement in meaningful daily activities to support their health and well-being in everyday life.
Andrew E, McDermott S, Vitzakovitch S, et al. Therapist and patient perceptions of the occupational therapy goal-setting process: A pilot study. Physical & Occupational Therapy in Geriatrics. 1999;17(1):55-63.
Barclay L. Exploring the factors that influence the goal setting process for occupational therapy intervention with an individual with spinal cord injury. Australian Occupational Therapy Journal. 2002;49:3-13.
Blackmer J. Ethical issues in rehabilitation medicine. Scandinavian Journal of Rehabilitation Medicine. 2000;32:51-55.
Bodium C. The use of the Canadian Occupational Performance Measure for the assessment of outcome on a neurorehabilitation unit. British Journal of Occupational Therapy. 1999;62(3):123-126.
Carswell A, McColl MA, Baptiste S, et al. The Canadian Occupational Performance Measure: A research and clinical review. Canadian Journal of Occupational Therapy. 2004;71(4):210-222.
Cederfeldt M, Lundgren Pieree B, Sadlo G. Occupational status as documented in records for stroke inpatients in Sweden. Scandinavian Journal of Occupational Therapy. 2003;10:81-87.
Chan CH, Lee TMC. Validity of the Canadian Occupational Performance Measure. Occupational Therapy International. 1997;4(3):229-247.
College of Occupational Therapists (COT). Code of ethics and professional conduct for occupational therapists. London: COT, 2000.
Conneeley AL. Interdisciplinary collaborative goal planning in a post-acute neurological setting: A qualitative study. British Journal of Occupational Therapy. 2004;67(6):248-255.
Cott C, Finch C. Goal-setting in physical therapy practice. Physiotherapy Canada. 1991;43(1):19-22.
Crabtree J. What is a worthy goal of occupational therapy? Occupational Therapy in Health Care. 2000;12(2/3):111-126.
Creek J. Occupational therapy defined as a complex intervention. London: College of Occupational Therapists, 2003.
Donnelly C, Eng JJ, Hall J, et al. Client-centred assessment and the identification of meaningful treatment goals for individuals with a spinal cord injury. Spinal Cord. 2004;42(5):302-307.
Eschenfelder VG. Shaping the goal setting process in OT: The role of meaningful occupation. Physical & Occupational Therapy in Geriatrics. 2005;23(4):67-81.
Forker JE, Gallagher B, Lewis A. Care planning for the homebound elderly client. Home Health Care Management & Practice. 1999;11(6):42-48.
Foye SJ, Kirschner KL, Wagner LCB, et al. Ethical issues in rehabilitation: A qualitative analysis of dilemmas identified by occupational therapists. Topics in Stroke Rehabilitation. 2002;9(3):89-101.
Gage M. The patient-driven interdisciplinary care plan. Journal of Nursing Administration. 1994;24(4):26-35.
Geen RG. Human motivation: A social psychological approach. Pacific Grove, CA: Brooks/Cole, 1995.
Guidetti S, Tham K. Therapeutic strategies used by occupational therapists in self-care training: A qualitative study. Occupational Therapy International. 2002;9(4):257-276.
Halladay K. Measuring the occupational performance of mental health clients – How hard should we try? OT News. 21, 2001.
Hanna K, Rodger S. Towards family-centred practice in paediatric occupational therapy: A review of the literature on parent–therapist collaboration. Australian Occupational Therapy Journal. 2002;49:14-24.
Law M, Baptiste S, Mills J. Client-centred practice: What does it mean and does it make a difference? Canadian Journal of Occupational Therapy. 1995;62(5):250-257.
Law M, Baptiste S, Carswell A, et al. Canadian Occupational Performance Measure, 4th edn. Ottawa, Ontario: Canadian Association of Occupational Therapists. 2005.
Locke EA, Latham GP. Building a practically useful theory of goal setting and task motivation. American Psychologist. 2002;57(9):705-717.
Lund ML, Tamm M, Bränholm IB. Patients’ perceptions of their participation in rehabilitation planning and professionals’ views of their strategies to encourage it. Occupational Therapy International. 2001;8(3):151-167.
McClain C. Collaborative rehabilitation goal setting. Topics in Stroke Rehabilitation. 2005;12(4):56-60.
McColl MA, Paterson M, Davies D, et al. Validity and community utility of the Canadian Occupational Performance Measure. Canadian Journal of Occupational Therapy. 2000;67(1):22-30.
McLeod K, Robnett R. Psychosocial documentation: Are your objectives functional, measurable and reimbursable? Occupational Therapy in Mental Health. 1998;14(3):21-31.
Missiuna C, Pollock N. Perceived efficacy and goal setting in young children. Canadian Journal of Occupational Therapy. 2000;67(2):101-109.
Moorhead P, Kannenberg K. Writing functional goals. In: Acquaviva JD, editor. Effective documentation for occupational therapy. 2nd edn. Rockville, MD: American Occupational Therapy Association; 1998:75-82.
Neistadt ME. Methods of assessing clients’ priorities: A survey of adult physical dysfunction settings. American Journal of Occupational Therapy. 1995;49(5):428-436.
Nelson CE, Payton OD. The planning process in occupational therapy: Perceptions of adult rehabilitation patients. American Journal of Occupational Therapy. 1997;51(7):576-583.
Northen JG, Rust DM, Nelson CE, et al. Involvement of adult rehabilitation patients in setting occupational therapy goals. American Journal of Occupational Therapy. 1995;49(3):214-220.
Palmadottir G. Client perspectives on occupational therapy services. Scandinavian Journal of Occupational Therapy. 2003;10:157-166.
Park SW. Client-centred, goal-oriented outcome evaluation in occupational therapy [course manual]. London: Harrison Associates, 2006.
Parry RH. Communication during goal-setting in physiotherapy treatment sessions. Clinical Rehabilitation. 2004;18:668-682.
Playford ED, Dawson L, Limbert V, et al. Goal setting in rehabilitation: Report of a workshop to explore professionals’ perceptions of goal setting. Clinical Rehabilitation. 2000;14:491-496.
Pollock N, Stewart D. Occupational performance needs of school-aged children with physical disabilities in the community. Physical & Occupational Therapy in Pediatrics. 1998;18(1):55-68.
Ponte-Allan M, Giles GM. Goal setting and functional outcomes in rehabilitation. American Journal of Occupational Therapy. 1999;53(6):646-649.
Quinn L, Gordon J. Functional outcomes documentation for rehabilitation. St Louis, MO: Saunders, 2003.
Randall KE, McEwen IR. Writing patient-centered functional goals. Physical Therapy. 2000;80(12):1197-1203.
Rebeiro KL. Client perspectives on occupational therapy practice: Are we truly client-centred? Canadian Journal of Occupational Therapy. 2000;67(1):7-14.
Rosa SA, Hasselkus BR. Finding common ground with patients: The centrality of compatibility. American Journal of Occupational Therapy. 2005;59(2):198-208.
Sames KM. Documenting occupational therapy practice. Upper Saddle River, New Jersey: Pearson Prentice Hall, 2005.
Schut HA, Stam HJ. Goals in rehabilitation teamwork. Disability and Rehabilitation. 1994;16(4):223-226.
Spencer JC, Davidson HA. The Community Adaptive Planning Assessment: A clinical tool for documenting future planning with clients. American Journal of Occupational Therapy. 1998;52(1):19-30.
Sumsion T. A revised occupational therapy definition of client-centred practice. British Journal of Occupational Therapy. 2000;63(7):304-309.
Sumsion T. Facilitating client-centred practice: Insights from clients. Canadian Journal of Occupational Therapy. 2005;72(1):13-20.
Sumsion T. Implementation issues. In: Sumsion T, editor. Client-centred practice in occupational therapy: A guide to implementation. Edinburgh, UK: Elsevier; 2006:39-53.
Sumsion T. The client-centred approach. In: Sumsion T, editor. Client-centred practice in occupational therapy: A guide to implementation. Edinburgh, UK: Elsevier; 2006:19-28.
Sumsion T, Smyth G. Barriers to client-centredness and their resolution. Canadian Journal of Occupational Therapy. 2000;67(1):15-21.
Wade DT. Editorial. Evidence related to goal planning in rehabilitation. Clinical Rehabilitation. 1998;12:273-275.
Wallen M, Doyle S. Performance indicators in paediatrics: The role of standardized assessments and goal setting. Australian Occupational Therapy Journal. 1996;43:172-177.
Welch A, Forster S. A clinical audit of the outcome of occupational therapy assessment and negotiated patient goals in the acute setting. British Journal of Occupational Therapy. 2003;66(8):363-368.
Wilkins S, Pollock N, Rochon S, et al. Implementing client-centred practice: Why is it so difficult to do? Canadian Journal of Occupational Therapy. 2001;68(2):70-79.
Williams WH, Evans JJ, Wilson BA. Outcome measures for survivors of acquired brain injury in day and outpatient neurorehabilitation programmes. Neuropsychological Rehabilitation. 1999;9(3/4):421-436.
Wressle E, Samuelsson K. Barriers and bridges to client-centred occupational therapy in Sweden. Scandinavian Journal of Occupational Therapy. 2004;11:12-16.
Wressle E, Eeg-Olofsson A, Marcusson J, et al. Improved client participation in the rehabilitation process using a client-centred goal formulation structure. Journal of Rehabilitation Medicine. 2002;34:5-11.
Wressle E, Marcusson J, Henriksson C. Clinical utility of the Canadian Occupational Performance Measure – Swedish version. Canadian Journal of Occupational Therapy. 2002;69(1):40-48.
Wressle E, Lindstrand J, Neher M, et al. The Canadian Occupational Performance Measure as an outcome measure and team tool in a day treatment programme. Disability and Rehabilitation. 2003;25(10):497-506.