CEMENTUM
After reading this chapter the student will be able to:
• describe the development of cementum and its function on the surface of the root
• describe the nature of and the physical properties of intermediate cementum, cellular cementum, and acellular cementum
• discuss the aging of cementum, the formation of cementicles, and the repair of cementum
OVERVIEW
Cementum, which is the focus of this chapter, has two major functions. It seals the tubules of root dentin and serves as an attachment for periodontal fibers to keep the tooth in its socket. Cementum has the ability to reverse root resorption by means of deposition as it forms a smooth patch on the cemental surface.
Two types of hard tissue cover tooth roots. The first, called intermediate cementum, is a homogenous layer originating from epithelial root sheath cells. The second, called cellular-acellular cementum, is a thicker deposit of a bonelike substance produced by cementoblasts that differentiate from the periodontal ligament fibroblasts. The latter is laid down in increments, usually an acellular layer followed by a cellular layer. Cementum simulates bone by displaying cells within lacunae and cell processes within canaliculi. Cementum also exhibits incremental lines but does not have the vascular and neural filament characteristics of bone. As a result, the cementum has unique characteristics, such as lack of neural sensitivity and a greater ability than bone to resist resorption. Both are important clinical features. Aging cementum exhibits a rough and irregular surface caused by resorption of the cemental surface. This cementum also is associated with free, attached, or embedded cementicles. These oval to round stones are similar to the denticles in pulp. They are calcified bodies that may be embedded, attached to cementum, or free in the periodontal ligament.
ROLE OF CEMENTUM ON THE ROOT SURFACE
The hard tissue that covers the entire root surface is very thin but manages to carry out two important functions. First, it seals the surface of the root dentin and covers the ends of the open dental tubules. Second, perforating fibers of the periodontal ligament become embedded in the cementum. These fibers function as an attachment for the periodontal ligament fibers to the tooth root and aid in maintaining the tooth in its socket. This chapter discusses sealing of the root surface (Fig. 10-1), and Chapter 12 discusses the attachment fibers.

Fig. 10-1 Relation of tooth roots to the periodontium. Cementum is shown on the root apex. It covers entire root surface overlying dentin. (From Avery JK: Oral development and histology, ed 3, Stuttgart, 2002, Thieme Medical.)
 CLINICAL COMMENT
CLINICAL COMMENTCementum can aid in maintaining the teeth in functional occlusion if it is deposited at the apical aspect of the root, especially in patients with chronic bruxism. Because cementum is the slowest growing tissue compared with the other periodontal tissues, it will be the last tissue to be added to the root surface after occlusal loss.
DEVELOPMENT OF CEMENTUM
The first cementum deposited on the root’s surface is called intermediate cementum and is formed by the inner epithelial root sheath cells that formed during root dentin formation. This deposition occurs before the root sheath cell layer disintegrates (Fig. 10-2). Intermediate cementum is situated between the granular dentin layer of Tomes and the secondary cementum that is formed by the cementoblasts. These cementoblasts arise from the periodontal ligament fibroblasts. The thin layer of intermediate cementum is approximately 10 nm thick. After being deposited, this layer mineralizes to a greater extent than the adjacent dentin or the cellular-acellular cementum. Under proper magnification, a thin line of radiopacity is seen covering the root.
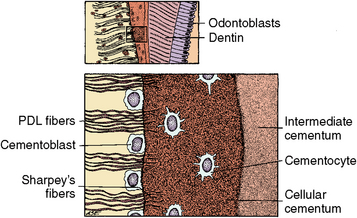
Fig. 10-2 Types of cementum on the root dentin surface. Intermediate cementum on the right overlying dentin cellular cementum in the center of the field and periodontal attachment fibers (PDL) on the left. (From Avery JK: Oral development and histology, ed 3, Stuttgart, 2002, Thieme Medical.)
The cellular-acellular cementum is a specialized hard tissue covering the root surfaces of teeth (see Figs. 10-2 and 10-3). The initial thin layer of this cementum is acellular and is deposited on intermediate cementum. Subsequent layers alternate between cellular and acellular. Thus, cementum is deposited incrementally. Both grossly and histologically, this cementum resembles bone because it is a hard tissue with cells contained in lacunae that exhibit canaliculi (see Fig. 10-2). However, unlike bone, cementum does not contain blood vessels, nerves, or haversian or Volkmann’s canals, which are the nutrient canals containing blood vessels and nerves in bone (see Fig. 10-3).
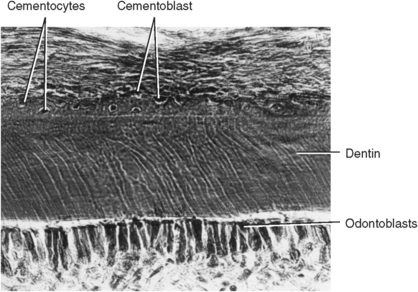
Fig. 10-3 Young cementum deposition on root dentin. Some cementoblasts become enmeshed in cementum matrix and develop into cementocytes living in lacunae. (From Avery JK: Oral development and histology, ed 3, Stuttgart, 2002, Thieme Medical.)
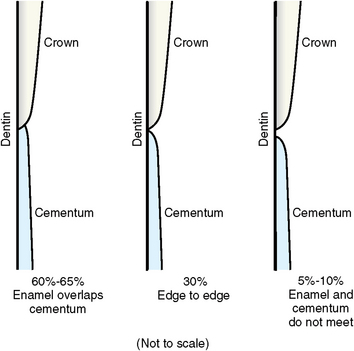
Cementum is limited to the roots of teeth. In 60% of cases, cementum is formed on the cervical enamel for a short distance; in 30% it stops at the cervical line just meeting the enamel; and in 10% a small gap exists between them. This order of frequency is known as OMG, or overlap, meet, and gap (Fig. 10-4 and Table 10-1).
INTERMEDIATE CEMENTUM
Intermediate cementum is a thin, noncellular, amorphous layer of hard tissue approximately 10 μm thick. It is deposited by the inner layer of the epithelial cells of the root sheath. Deposition occurs immediately before the epithelial root cells disintegrate as a sheet and migrate away from the root into the periodontal tissue (see Fig. 10-2). Recently, most authors have used the term intermediate cementum, although some prefer cementoid layer. The latter term is confusing because the initial layer of cementum is called cementoid, like osteoid in bone.
Intermediate cementum is the first layer of hard tissue deposited, and it seals the tubules of dentin. Because of its epithelial origin, intermediate cementum is composed of enamelin protein rather than collagen, which is the protein typical of cellular or secondary cementum. Intermediate cementum is completely formed before deposition of the secondary cementum begins. As an amorphous, noncellular layer, it is similar to the aprismatic enamel layer on the crown surface of teeth. This cementum calcifies to a greater extent than either the adjacent cellular cementum or the dentin and therefore has a harder consistency (see Fig. 10-2).
CELLULAR AND ACELLULAR CEMENTUM
Cementum is deposited directly on the surface of the intermediate cementum at a thickness of about 30 to 60 μm at the cervical region of the crown (see Figs. 10-3 and 10-5). It increases gradually to a thickness of 150 to 200 μm at the root apex (Fig. 10-6).
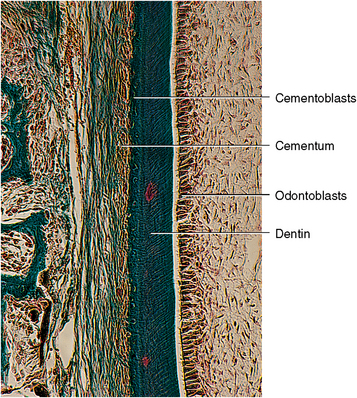
Fig. 10-5 Development of cellular cementum. Epithelial root sheath cells have moved from the root surface of dentin to a position peripheral to the cementum in the periodontal ligament. Cementoblasts are forming cementum along left side of band of dentin and cementum. (From Avery JK: Oral development and histology, ed 3, Stuttgart, 2002, Thieme Medical.)
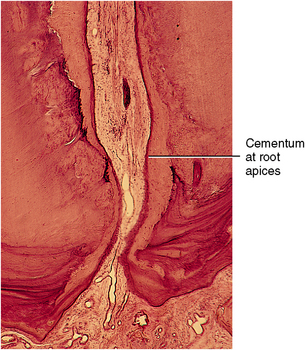
Fig. 10-6 Thick cementum on root apices of an older tooth. Cementum is deposited around apical foramen and is lining the pulpal wall near the apex, constricting the foramen. (From Avery JK: Oral development and histology, ed 3, Stuttgart, 2002, Thieme Medical.)
The cementum appears to be more cellular as the thickness increases, probably to maintain its viability (Fig. 10-7). The thin layer near the cervical region requires no cells to maintain viability because fluids bathe its surface.
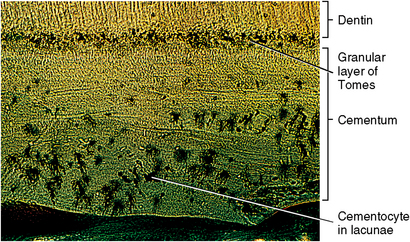
Fig. 10-7 Histology of the granular layer of Tomes and cells in the lacunae in cementum. Cementum near the apex has the greatest number of lacunae. (From Avery JK: Oral development and histology, ed 3, Stuttgart, 2002, Thieme Medical.)
Cementum forms more slowly than the adjacent dentin (see Fig. 10-5). After the inner epithelial root sheath cells stimulate the formation of the root dentin, they deposit the intermediate cementum on the surface of the dentin. These cells then begin to degenerate and migrate from the root surface into the periodontal ligament. Then the cementoblasts, which originate from the periodontal ligament, begin to form increments of cementum along the root surface.
Cementum is always thickest at the apex of the root (see Fig. 10-6). Cementum forms through the deposit in increments of a collagenous matrix that then becomes secondarily mineralized (see Chapter 5). The young matrix is called cementoid, and its formation is similar to that of bone from osteoid and dentin from predentin.
Some cementoblasts become incorporated in the forming cementum along the developing front as cementum continues to form around the cementoblasts (see Figs. 10-7, 10-8 to 10-11). These cells are then termed cementocytes because they reside in lacunae and appear most notably in the thick apical cementum (see Fig. 10-7). The cementocytes found deep in the cementum are polygonal and have fewer organelles (see Fig. 10-9).
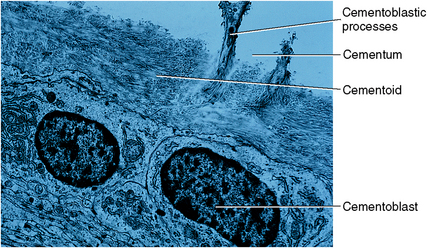
Fig. 10-8 Ultrastructure of cementoblasts on the surface of young cementum. Cementoblasts become cementocytes as their processes (and later their cell bodies) become incorporated in the matrix. (From Avery JK: Oral development and histology, ed 3, Stuttgart, 2002, Thieme Medical.)
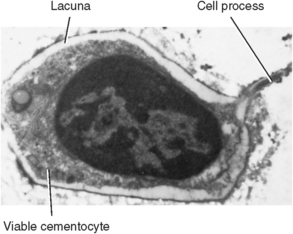
Fig. 10-9 Ultrastructure of cementocyte near the surface of cementum. Cementocytes in this region appear viable and communicate with adjacent cementocytes by gap junctions on their processes. (From Avery JK: Oral development and histology, ed 3, Stuttgart, 2002, Thieme Medical.)
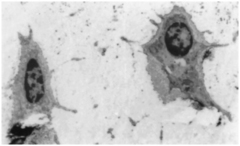
Fig. 10-10 Ultrastructure of two cementocytes lying deep in cementum. These cells contain few organelles and appear to be inactive. (From Avery JK: Oral development and histology, ed 3, Stuttgart, 2002, Thieme Medical.)
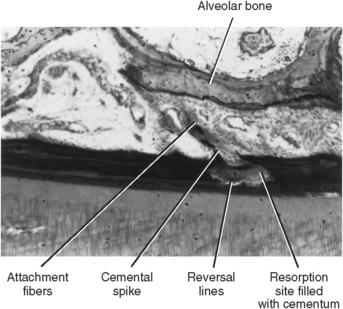
Fig. 10-11 Aging cementum showing projection of cemental spikes into ligament. A reversal line indicates root resorption and anatomic repair. Cementum builds up around bundles of periodontal ligament attachment fibers. (From Avery JK: Oral development and histology, ed 3, Stuttgart, 2002, Thieme Medical.)
Although many blood vessels are near the surface, none actually enters the cementum. In laboratory tests, cementum is slightly more permeable to dyes than bone or dentin. However, the permeability of viable cementum is unknown. Cementum is deposited in increments, resulting in incremental lines similar to those of bone, dentin, and enamel (Fig. 10-12). Cementum has many characteristics of hard tissue, although some elements are absent. Therefore, cementum is not exactly like any other tissue in the human body. A thin layer of acellular cementum covers the cervical half of the root surface to a distance of approximately 20 μm. A deposit of cellular cementum then covers the acellular layer on the cervical root to a total thickness of 50 μm. Cellular cementum is then deposited on the apical root dentin to a thickness of 150 to 200 μm.
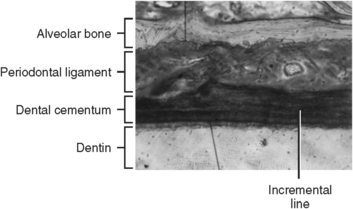
Fig. 10-12 Histology of cementum on the root surface. Horizontal incremental lines in cementum appear similar to those of bone, dentin, or enamel.
Without the presence of nerves, cellular cementum is insensitive to pain, which is an important clinical feature. Cementum is also more resistant to resorption than bone, and the lack of cementum vascularity may be part of the reason.
Deep within cementum, many lacunae appear empty, implying that these cells gradually die. Some of these cells have long processes that lie in canaliculi and are in contact with adjacent cementocytes (see Figs. 10-7 to 10-10). Near the surface of cementum, the cells appear active with organelles such as Golgi’s apparatus, rough-surface endoplasmic reticulum, and mitochondria, which are all associated with protein secretion (see Fig. 10-10). Layers of cellular cementum may alternate with noncellular layers in their formation, although the reason is unknown. Deeper in the cementum, the cells may be less active (see Fig. 10-9).
The collagen fibers formed within the cementum are associated with the cementum’s function on the root’s surface. More superficially, cementum has bundles of noncalcified fibers that are associated with the function of attachment of periodontal fibers. These perforating fibers are called extrinsic fiber bundles of cementum.
PHYSICAL PROPERTIES
As one group of hard connective tissues, cementum contains slightly less mineral than dentin or bone (Table 10-2). It is yellow and can be distinguished from enamel because cementum, unlike enamel, has no luster. Cementum is slightly lighter in color than dentin, which makes it difficult to distinguish between the two. It is softer than dentin, however, which aids in its identification.
AGING OF CEMENTUM
With aging, the relatively smooth surface of cementum becomes more irregular (see Fig. 10-11). This is caused by the calcification of some ligament fiber bundles where they were attached to the cementum. Such occurrences appear on most surfaces of cementum, but to no greater degree near the apical zone. In aging, a continuing increase of cementum in the apical zone may obstruct the apical canal (see Fig. 10-6).
Microscopically, only the lacunae near the surface may have cells that appear viable, whereas deeper lacunae appear empty. Cementum resorption is one characteristic of aging cementum (see Fig. 10-11). Resorption becomes active for a period and then may stop. Deposition of cementum occurs in that period, creating reversal lines. Resorption can also occur in root dentin, and cemental repair can cover this defect (Fig. 10-13).
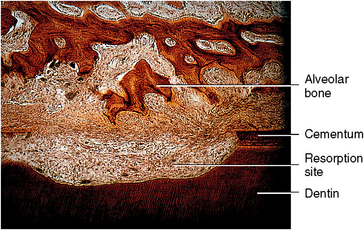
Fig. 10-13 Cemental and dentin resorption with periodontal soft tissue occupying the area. Alveolar bone develops in this space to compensate for root loss. The length of the periodontal fibers is thus maintained. (From Avery JK: Oral development and histology, ed 3, Stuttgart, 2002, Thieme Medical.)
 Consider the Patient
Consider the PatientAn older patient notes that root exposure seems common in her contemporaries. She has also noticed this condition in her son, who has periodontal disease. She asks why this condition is shared by both groups of people.
CEMENTICLES
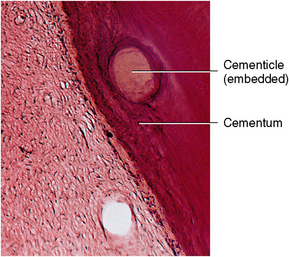
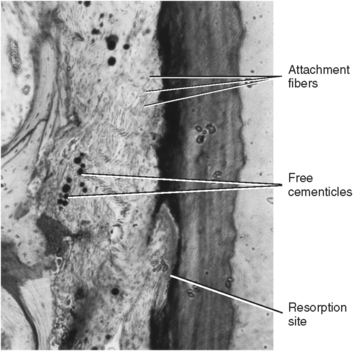
A cementicle is a calcified ovoid or round nodule found in the periodontal ligament. Cementicles may be found singly or in groups near the surface of the cementum (Figs. 10-14 and 10-15). The origin of a cementicle may be a nidus of epithelial cells that are composed of calcium phosphate and collagen in the same amount as cementum (45% to 50% inorganic and 50% to 55% organic). Cementicles may be free in the ligament, attached, or embedded in the cementum (see Figs. 10-14 and 10-15). They are more prevalent along the root in an aging person, although they may also be found at a site of trauma.
CEMENTAL REPAIR
Cemental repair is a protective function of the cementoblasts after resorption of root dentin or cementum. These cells are programmed to maintain a smooth surface of the root. Defects arise because of trauma of various kinds, such as traumatic occlusion, tooth movement, and hypereruption caused by the loss of an opposing tooth. Loss of cementum is accompanied by a loss of attachment fibers to the root surface. When this occurs, repair cementum may be deposited by cementoblasts in the defect. After this happens, the attachment fibers readily appear and are found embedded in the repair cementum (see Fig. 10-11). A cemental deposit means the development of a reversal line. This is seen at the point where resorption stops and deposition begins (Fig. 10-16). In an older individual, the surface cementum no longer exhibits a smooth surface (see Fig. 10-15).
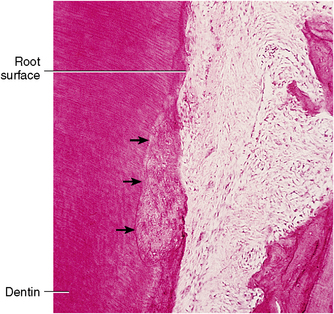
Fig. 10-16 Reversal line in cementum (arrows). The root surface is again smooth as a result of cementum deposit in the resorption area (anatomic repair). (From Avery JK: Oral development and histology, ed 3, Stuttgart, 2002, Thieme Medical.)
Cementum is resistant to resorption in younger tissues. This is the reason that orthodontic tooth movement results in alveolar bone resorption rather than tooth root loss. Cemental repair is an important root protective mechanism.
Discussion: Root exposure is common in both aging and periodontal disease. In either condition, when there is an apical migration of the epithelial attachment, exposure of cementum and dentin occurs. Pain is associated with exposed dentin and cementum because dentinal tubules open into pulp, where nerves are located. Also, cementum is thin or nonexistent on the cervical root. Patients with root exposure should be careful. Root caries is also common in root exposure. This occurs because the exposed cementum and dentin are less resistant to caries than is enamel. The pain decreases in time because pulpal odontoblasts respond to the stimuli of exposed dentinal tubules with deposition of reparative dentin in the pulp underlying this area.
SELF-EVALUATION QUESTIONS
1. What is the origin of intermediate cementum?
2. Where on the root is cementum thinnest and where is it thickest?
3. Name three types of cementicles.
4. Describe the appearance of healed root surfaces.
5. Why is cementum insensitive to pain?
6. What is the function of cementum?
7. What is the origin of cementoblasts and cementocytes?
8. Name two characteristics of aging cementum.
9. What are the percentages that cementum overlaps, meets, or gaps enamel?