Cranial Nerves III, IV, VI
Eye Movements
BACKGROUND
Eye movements can be divided into four types:
• Saccadic eye movements: the rapid movement from one point of fixation to another. You would use a saccadic eye movement to look from the page to someone in the room or if you were told to look up.
• Pursuit eye movements: the slow eye movement used to maintain fixation on a moving object: for example, to maintain eye contact as a person moves across a room.
• Vestibular–positional (vestibulo-ocular reflex) eye movements: the eye movements that compensate for movement of the head to maintain fixation.
• Convergence: the movements that maintain fixation as an object is brought close to the face. These are rarely affected in clinical practice.
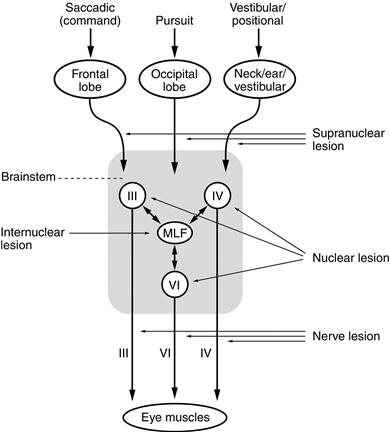
The sites of control of these eye movements differ (Fig. 9.1).
| Type of eye movement | Site of control |
| Saccadic (command) | Frontal lobe |
| Pursuit | Occipital lobe |
| Vestibular–positional | Cerebellar vestibular nuclei |
| Convergence | Midbrain |
In the brainstem, the inputs from the frontal and occipital lobes, the cerebellum and the vestibular nuclei are integrated so that both eyes move together. Important structures are the centre for lateral gaze in the pons and the medial longitudinal fasciculus (MLF), which runs between the nuclei of the III and IV cranial nerves (in the midbrain) and the VI (in the pons).
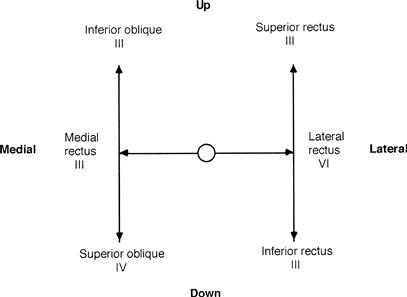
The III, IV and VI cranial nerves then control the following muscles (Fig. 9.2):
Abnormalities can arise at any level (Fig. 9.1):
No double vision (generally):
Double vision:
Internuclear and supranuclear lesions rarely cause double vision.
WHAT TO DO
Look at the position of the head.
Look at the eyes.
• Note ptosis (see Chapter 6).
• Note the resting position of the eyes and the position of primary gaze.
Look at the position of the eyes in primary gaze.
Perform the cover test (Fig. 9.3).
The cover test
What to do
This is a test for latent squint.
Ask the patient to look with both eyes at your right eye, then cover his left eye. Then uncover the left eye rapidly and cover the right eye. Look to see if the left eye has to correct to look back at your eye. Repeat, covering the left eye and watching the right eye.
What you find
If one eye has to correct as it is uncovered, this indicates that the patient has a latent strabismus (squint), which can be classified as divergent or convergent.
Test the eye movements to pursuit
• Hold a pen vertically about 50 cm away from the patient in the centre of his gaze. Ask him to follow it with his eyes without moving his head and to tell you if he sees double. You can hold the chin lightly to prevent head movement.
• Move the pen slowly. Ask the patient to tell you if he sees double:
– up and down at the extreme of lateral gaze.
• Ensure the patient's nose does not prevent the pen being seen at the extreme of lateral gaze.
As you do this, watch the movements of the eyes.
• Do both eyes move through the full range? Estimate the percentage reduction in movement in each direction.
If the patient reports seeing double at any stage:
• Establish if the images are side by side, up and down, or at an angle.
• Establish the direction in which the images are widest apart.
• In this position, briefly cover one eye and ask which image disappears: the inner or outer. Repeat this by covering the other eye (Fig. 9.4).
Test saccadic eye movements
• Face the patient. Hold both your hands out in front of you about 30 cm apart from side to side and about 30 cm in front of the patient.
• Ask the patient to look from one hand to the other.
• Observe the eye movements: are they full, do they move smoothly, do they move together?
• Look particularly at the speed of adduction.
• Then put your hands vertically one above the other, about 30 cm apart and ask the patient to look from one to the other.
• Again observe the eye movements. Do the eyes move at a normal speed and through the full range?
Test convergence
Ask the patient to look into the distance and then look at your finger placed 50 cm in front of him. Gradually bring the eyes in, observing the limit of convergence of the eyes.
Vestibulo-ocular reflex (doll's eye manœuvre)
This test is most commonly used in unconscious patients, when it provides a way of testing eye movements. In conscious patients with limited eye movements on command or pursuit, the test can be used to demonstrate preserved eye movements on vestibulo-positional stimulation, indicating a supranuclear eye movement abnormality.
Ask the patient to look into the distance at a fixed point; turn his head to the left then the right, and flex the neck and extend the neck.
The eyes should move within the orbits, maintaining forward gaze.
WHAT YOU FIND
• The eyes are misaligned in primary gaze:
– The misalignment remains constant in all directions for gaze = convergent or divergent concomitant strabismus (squint).
– One eye is deviated downwards and out, with ptosis = third nerve lesion.
– Eyes aligned in different vertical planes = skew deviation.
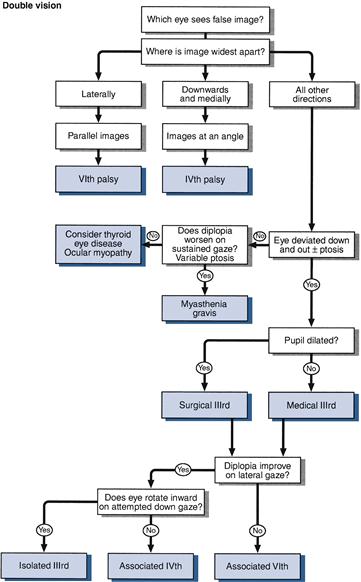
• The patient has double vision (Fig. 9.4):
Try to answer the following questions:
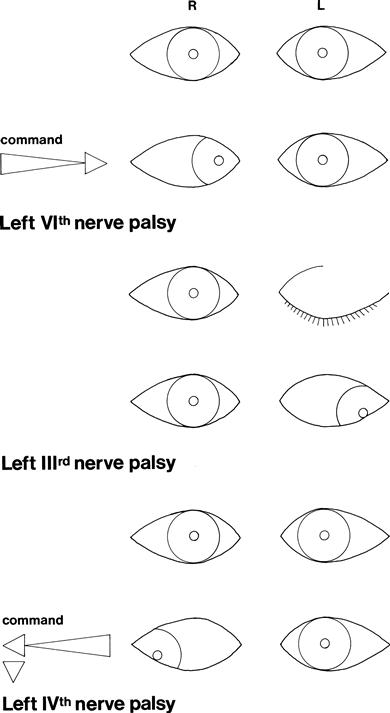
Is there a single nerve (VI, III or IV) deficit (Fig. 9.5)?
– If there is a third nerve deficit, is it medical (pupil-sparing) or surgical (with pupillary dilatation)?
– Is there a combination of single nerves?
– Is it myasthenia or dysthyroid eye disease?
• The patient does not have double vision: Compare movements on command, on pursuit and on vestibular positional testing.
Other common abnormalities:
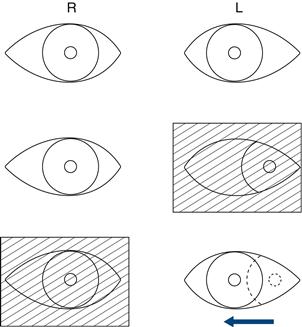
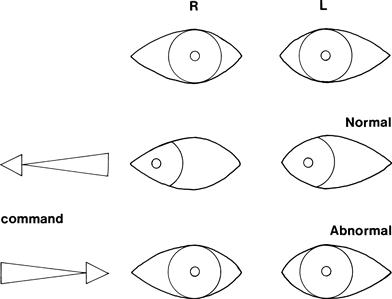
• Patient does not look towards one side = lateral gaze palsy; check response to vestibulo-ocular reflex testing (Fig. 9.6).
• Patient does not look up = upgaze palsy.
• Patient does not look down = downgaze palsy.
• Eyes do not move together, with markedly slowed adduction and with nystagmus in the abducting eye = internuclear ophthalmoplegia with ataxic nystagmus (Fig. 9.7).
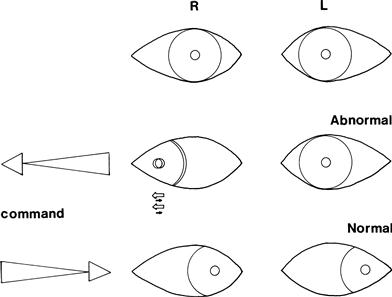
Figure 9.7 Left internuclear ophthalmoplegia. There is nystagmus of the right eye as the eye looks to the right
• Eye movement falls short of target and requires a second movement to fixate = hypometric saccades.
WHAT IT MEANS
• Skew deviation: brainstem lesion. Common causes: stroke, demyelination—look for associated brainstem signs.
• Single cranial nerve palsy (III, IV or VI): lesion along the course of the nerve or a nuclear lesion. Common causes:
– Medical: diabetes mellitus, atherosclerosis. Rarely: vasculitis, Miller–Fisher syndrome (a form of Guillain–Barré syndrome).
– Surgical (N.B. pupil involvement in third nerve palsy): tumour, aneurysm, trauma, a false localising sign or uncal herniation (third nerve).
 TIP
TIP
Posterior communicating aneurysm is a common cause of a surgical third nerve palsy.
• Nuclear lesions: arise from brainstem pathology, including brainstem infarction, multiple sclerosis and, rarely, brainstem haemorrhage and tumour.
• Lateral gaze palsy: can arise from:
– a large frontal or parietal lobe lesion when the patient looks away from the paralysed side (can be overcome by doll's eye manœuvre)
– a pontine lesion when the patient cannot look to the non-paralysed side and there may be other pontine abnormalities (facial weakness); not overcome using doll's eye manœuvre.
• Vertical gaze palsy: lesions in the upper brainstem.
Common causes of lateral and vertical gaze palsies: brainstem infarction, multiple sclerosis, tumour.
• Internuclear ophthalmoplegia = a lesion to the medial longitudinal fasciculus. Common cause: multiple sclerosis. Rarer causes: vascular disease, pontine glioma.
• Supranuclear palsy with preserved positional/vestibular testing: may arise in association with akinetic rigid syndromes (Chapter 24), when it is referred to as the Steele–Richardson syndrome or progressive supranuclear palsy, and may be seen in other degenerative conditions.
• Hypometric saccades: indicate a cerebellar lesion—see Chapter 23.