Coordination
BACKGROUND
A coordinated combination of a series of motor actions is needed to produce a smooth and accurate movement. This requires integration of sensory feedback with motor output. This integration occurs mainly in the cerebellum.
In the presence of weakness, tests for coordination must be interpreted with caution and are unlikely to be informative if there is significant weakness.
Loss of joint position sense can produce some incoordination (sensory ataxia). This is made substantially worse when the eyes are closed. Joint position sense should be tested before coordination.
WHAT TO DO
Test the gait (see Chapter 4).
In all tests, compare right with left. Expect the right hand to be slightly better (in a right-handed person).
Arms
Ask the patient to hold his arms outstretched and ask him to close his eyes. Tell the patient to keep his arms in this position. Then push his arm up or down suddenly.
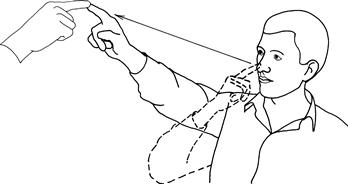
Finger–nose test
Hold your finger out about an arm's length in front of the patient. Ask the patient to touch your finger with his index finger and then touch his nose (Fig. 23.1). When he has done this correctly, ask him to repeat the movement faster. Watch for accuracy and smoothness of movement.
Repeated movements
Ask the patient to pat one hand on the back of the other quickly and regularly (demonstrate).
Ask the patient to twist his hand as if opening a door or unscrewing a light bulb (demonstrate).
Ask the patient to tap the back of his right hand alternately with the palm, and then the back of his left hand. Repeat with the right hand (demonstrate).
Legs
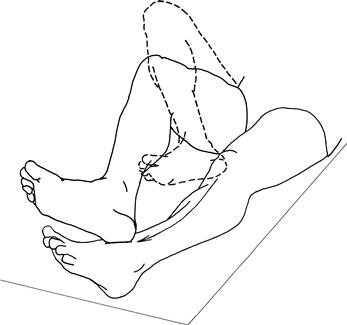
Heel–shin test
The patient is lying down. Ask him to lift his leg and place the point of his heel on his knee, and then run it down the sharp part of his shin (Fig. 23.2) (demonstrate). Watch for accuracy and smoothness of movement.
Ask the patient to tap his feet as if listening to fast music.
Trunk
Ask the patient to sit up from lying without using his hands. Does he fall to one side?
Other tests of cerebellar function
• Speech (Chapter 2).
• Nystagmus (Chapter 10).
• Hypotonia (Chapter 16).
• Pendular reflexes (Chapter 19).
• Tremor (Chapter 24).
WHAT YOU FIND
Repeated movements
• Disorganisation of the movement of the hands and the elbows take wider excursions than expected; irregularity of the movements which are performed without rhythm. Compare the two sides; these changes indicate cerebellar incoordination. Often the abnormality is heard as a slapping sound rather than the normal tapping noise.
 TIP
TIP
Mild upper motor neurone weakness impairs fluency of fast repeated movements. However, the movements will not have a wider excursion than expected.
When there is disorganisation of tapping the hand and then turning it over, this is referred to as dysdiadochokinesia.
Heel–shin test
• Disorganisation of movement with the heel falling off the anterior part of the shin, and the knee falling from side to side.
TIP
The finger–nose and heel–shin tests can be used to test joint position sense. If the movements are accurate with eyes open but are substantially worse when repeated with eyes closed, this indicates impairment of joint position sense.
Trunk
• The patient is unable to sit from lying without falling to one side: truncal ataxia. This is associated with gait ataxia (Chapter 4).
WHAT IT MEANS
• Unilateral incoordination: ipsilateral cerebellar syndrome.
• Bilateral incoordination: bilateral cerebellar syndrome.
• Truncal ataxia, gait ataxia, without limb incoordination: midline cerebellar syndrome.
• Unilateral cerebellar syndrome. Common causes: demyelination, vascular disease. Rare causes: trauma, tumour or abscess.
• Bilateral cerebellar syndrome. Common causes: drugs (anticonvulsants), alcohol, demyelination, vascular disease. Rare causes: hereditary cerebellar degenerations, paraneoplastic disorders, hypothyroidism.
• Midline cerebellar syndrome: lesion of the cerebellar vermis. Causes as for bilateral cerebellar syndrome.