Cranial Nerves V and VII
The Face
BACKGROUND
Facial nerve: VII
Peripheral function can be summarised as ‘face, ear, taste, tear’:
• face: muscles of facial expression and blinking
• ear: stapedius (the muscle that dampens loud noises) and sensory supply to the external auditory meatus and adjacent pinna.
With lower motor neurone (LMN) facial weakness, all muscles are affected.
With upper motor neurone (UMN) facial weakness, the forehead is relatively preserved.
Trigeminal nerve: V
Motor
The trigeminal nerve supplies the muscles of mastication.
What to do
Look at the face generally.
• Is there a general medical syndrome (e.g. hyper- or hypothyroidism, Cushing's disease, acromegaly or Paget's disease)?
• Are there abnormal movements (see Chapter 24)?
FACIAL NERVE: WHAT TO DO
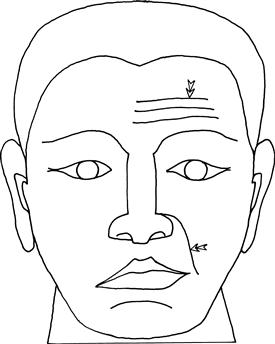
Look at the symmetry of the face.
• Note nasolabial folds and forehead wrinkles (Fig. 11.2).
Ask the patient to:
• show you his teeth (demonstrate)
• close his eyes tightly as if he had soap in them (demonstrate)
– assess the strength by trying to open his eyes with your fingers
Look out for symmetrical movement.
Compare the strength of the forehead and lower face.
In LMN lesions you can see the eye turn upwards on attempted closure—Bell's phenomenon.
Other functions of the facial nerve
Look at the external auditory meatus—the cutaneous distribution of VII. Note any vesicles suggestive of herpes zoster.
Provides taste to the anterior two-thirds of tongue. Taste is rarely tested and requires saline solution and sugar solution. A cotton bud is dipped in the solution and applied to the tongue and the patient is asked to identify it. Test each side of the anterior two-thirds and the posterior one-third.
FACIAL NERVE: WHAT YOU FIND
See Figure 11.3.
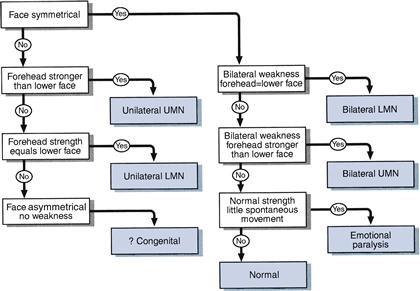
Bilateral facial nerve weakness can be easily missed unless tested for. Think of it if you feel that a patient seems impassive when you talk to him. He may not be depressed; his face might not be able to move!
Failure of the patient to smile when asked to whistle has been noted in patients with emotional paralysis due to parkinsonism: the ‘whistle–smile’ sign.
FACIAL NERVE: WHAT IT MEANS
• Unilateral LMN weakness: lesion of the facial nerve or its nucleus in the pons. Common cause: Bell's palsy. More rarely: pontine vascular accidents, lesions at the cerebellopontine angle, herpetic infections (Ramsay Hunt syndrome—note vesicles in external auditory meatus), Lyme disease, basal meningitis, lesions in its course through the temporal bone, parotid tumours.
• Bilateral LMN weakness: Common causes: sarcoidosis, Guillain–Barré syndrome. Rarer causes: myasthenia gravis can produce bilateral fatigable facial weakness (neuromuscular junction); myopathies can produce bilateral facial weakness (N.B. myotonic dystrophy and fascio-scapulo-humeral dystrophy).
• Unilateral UMN: cerebrovascular accidents, demyelination, tumours—may be associated with ipsilateral hemiplegia (supratentorial lesions) or contralateral hemiplegia (brainstem lesions).
TRIGEMINAL NERVE: WHAT TO DO
Motor
Test muscles of mastication (trigeminal nerve: motor)
Look at the side of the face.
Ask the patient to clench his teeth.
Ask the patient to push his mouth open against your hand.
Jaw jerk.
Sensory
Test facial sensation (trigeminal nerve: sensory). (See Chapter 19 for general comments on sensory testing.)
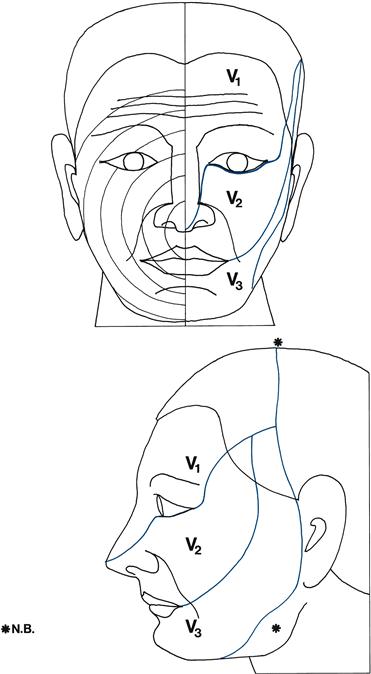
Test light touch and pinprick in each division on both sides:
• V3: lower lip (Fig. 11.1).
Compare one side to the other.
• If abnormal, test temperature.
• If a sensory deficit is found, determine its edges, moving from abnormal to normal.
THE CORNEAL REFLEX (AFFERENT— OPHTHALMIC BRANCH OF V; EFFERENT—VII)
• Ask the patient to look up and away from you. Bring a piece of cotton wool twisted to a point to touch the cornea from the side.
• Watch both eyes blink closed.
• If there is a unilateral facial palsy, the sensation of the cornea can be demonstrated if the opposite eye is watched.
COMMON MISTAKES
• The conjunctiva is touched instead of the cornea (Fig. 11.4).

• Reflex is mildly inhibited in contact lens wearers.
• Cotton wool brought in too quickly acts as a menacing stimulus to provoke a blink.
TRIGEMINAL NERVE: WHAT YOU FIND
Motor
Sensory
• Impairment or loss in one or more divisions on one side (Fig. 11.1): of light touch or pinprick and temperature or both.
• Unilateral facial loss: one or all modalities.
• Muzzle loss of pinprick and temperature.
• Unilateral area of sensory loss not in distribution of whole division.
N.B.
TRIGEMINAL NERVE: WHAT IT MEANS
• Loss of all modalities in one or more divisions:
– Lesion in sensory ganglion: most commonly herpes zoster.
– Lesion of division during intracranial course: V1 cavernous sinus (associated III, IV, VI) or orbital fissure, V2 trauma, V3 basal tumours (usually associated motor V).
• Loss of sensation in all divisions in all modalities:
– Lesion of the Gasserian ganglion, sensory root or sensory nucleus: lesions of cerebellopontine angle (associated VII, VIII), basal meningitis (e.g. sarcoid, carcinoma); trigeminal sensory neuropathy can occur in Sjogren's syndrome.
– With ipsilateral hemisensory loss of light touch: contralateral parietal lobe lesion.
– With no other loss: sensory root lesion in pons.
• Loss of pinprick and temperature with associated contralateral loss of these modalities on the body: ipsilateral brainstem lesion.
• Loss of sensation in muzzle distribution: lesion of descending spinal sensory nucleus with lowest level outermost—syringomyelia, demyelination.
• Area of sensory loss on cheek or lower jaw: damage to branches of V2 or V3 infiltration by metastases.